Summary
Pregnancy loss can occur even in previously healthy pregnancies. If it occurs before 20 weeks' gestation (∼ 10% of pregnancies), it is called miscarriage or spontaneous abortion. If it occurs after 20 weeks' gestation, it is called stillbirth or intrauterine fetal demise. There is no widely accepted definition of recurrent pregnancy loss, but it often refers to ≥ 2 losses before viability. The majority of spontaneous abortions are due to fetal aneuploidy. Other common causes of spontaneous abortion are maternal disease, trauma, and congenital anomalies. Stillbirth can be caused by maternal disease, placental disorders, umbilical cord complications, or fetal congenital anomalies. In many cases, the cause of spontaneous abortion or stillbirth is unknown. The management of pregnancy loss depends on the week of gestation and clinical presentation and may involve medication-induced evacuation of the pregnancy, surgical evacuation of the pregnancy, or expectant management. After a spontaneous abortion, the products of conception should undergo histopathological examination. Similarly, fetal autopsy should be offered after a stillbirth in order to determine the underlying cause and address any modifiable etiologies.
See also “Counseling on pregnancy loss” and “Induced abortion.”
Overview
| Types of pregnancy loss [1] | |||
|---|---|---|---|
| Type [2][3] | Definition | Findings | Treatment |
| Threatened abortion |
|
|
|
| Inevitable abortion |
|
|
|
| Missed abortion |
|
|
|
| Incomplete abortion |
|
|
|
| Complete abortion |
|
|
|
| Stillbirth |
|
|
|

© AMBOSS
Spontaneous abortion
Definitions [1][2]
-
Spontaneous abortion (miscarriage)
- Spontaneous loss of pregnancy before 20 weeks' gestation [2][4]
- If gestational age is unknown: spontaneous loss of pregnancy with fetal weight < 350 g) [2][4]
- Early pregnancy loss: spontaneous loss of pregnancy before 13 weeks' gestation (i.e., during the first trimester)
- See also “Recurrent pregnancy loss.”
Etiology [1]
Causes of spontaneous abortion include:
-
Maternal
- Abnormalities of the reproductive organs
- Septate uterus
- Uterine leiomyomas
- Uterine adhesions
- Cervical incompetence
- Systemic diseases
- Including diabetes mellitus, hyperthyroidism, hypothyroidism, genetic disorders, infections, hypercoagulability (see “Recurrent pregnancy loss”)
- Abnormalities of the reproductive organs
-
Fetoplacental
- Chromosomal abnormalities account for up to half of all spontaneous abortions.
- Congenital anomalies
- Anembryonic pregnancy
-
Miscellaneous
- Trauma
- Iatrogenic (e.g., amniocentesis or chorionic villus sampling)
- Environmental (exposure to toxins such as drugs or maternal smoking during pregnancy)
- Unknown
Clinical features [3][5]
- Vaginal bleeding
- Abdominal pain or cramping
- Loss of pregnancy symptoms (e.g., breast tenderness, nausea)
- Size-date discrepancies in gestational age assessment
- Absence of fetal cardiac activity
Diagnostics [2][3][6]
General principles
- The diagnosis of spontaneous abortion is based on a combination of the following:
- Clinical evaluation to assess for active bleeding, retained POC, and whether the cervical os is dilated
- Ultrasound to assess for sonographic signs of intrauterine pregnancy and fetal cardiac activity
- Supportive diagnostics, including serum β-hCG, CBC, and blood typing
- Ectopic pregnancy must be excluded (see “Diagnostics for ectopic pregnancy”).
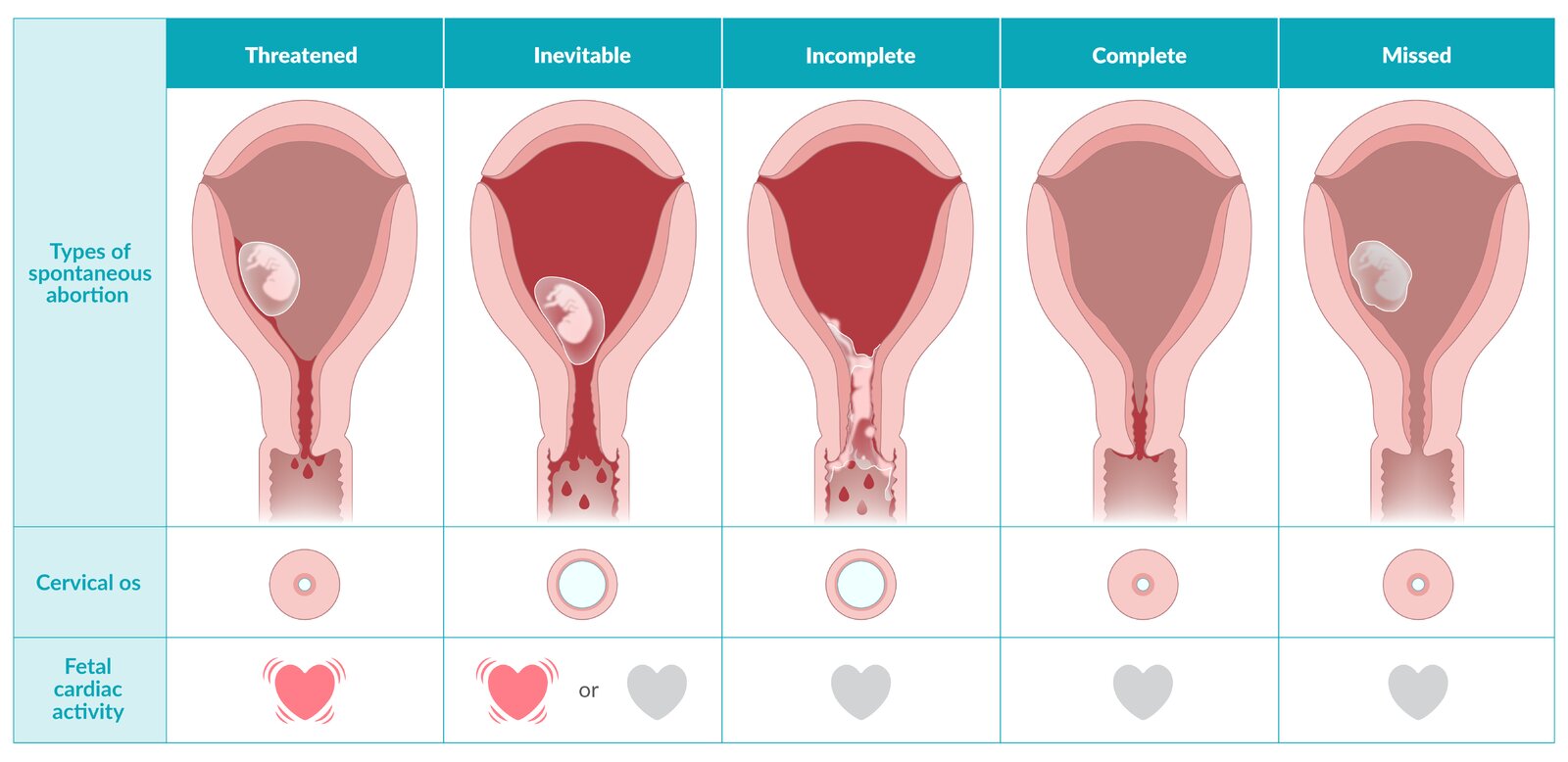
| Features of spontaneous pregnancy loss [3] | ||||
|---|---|---|---|---|
| Type | Vaginal bleeding | Fetal cardiac activity | Products of conception (POC) | Cervical os |
| Threatened abortion |
|
|
|
|
| Inevitable abortion |
|
|
|
|
| Missed abortion |
|
|
|
|
| Incomplete abortion |
|
|
|
|
| Complete abortion |
|
|
|
|
Diagnostic confirmation of fetal death prior to treatment is essential to avoid compromising a viable pregnancy.
Consider the diagnosis of septic abortion in patients with clinical features of pregnancy loss and fever. [7]
Clinical evaluation
- Bimanual pelvic examination: Assess for size-date discrepancies and signs of ectopic pregnancy (e.g., adnexal mass or tenderness).
-
Speculum examination
- Assess for cervical dilatation and retained POC.
- Confirm that the source of bleeding is uterine.
In stable patients after a resolved episode of mild to moderate vaginal bleeding, pregnancy viability may be assessed by ultrasound without a bimanual or speculum examination. [5]
Ultrasound
-
Fetal heart rate auscultation with Doppler monitor [8]
- Performed routinely during prenatal visits after 10–12 weeks' gestation
- Absence of fetal heart sounds should raise suspicion of spontaneous abortion.
-
Transvaginal ultrasound (TVUS): to look for sonographic signs of intrauterine pregnancy (IUP)
- Diagnostic modality of choice to verify the presence of a viable IUP [9]
-
TVUS findings of pregnancy failure include:
- Absence of fetal cardiac activity when crown-rump length is ≥ 7 mm [2]
- Gestational sac ≥ 25 mm without an embryo
- Previously visualized IUP not observed (empty uterus) [2]
- For the technique, see “POCUS for early pregnancy.”
Perform a pelvic ultrasound on pregnant patients who present to the emergency department with abdominal pain or vaginal bleeding, regardless of β-hCG levels. [10]
Laboratory studies
- Serial serum β-hCG: : Downtrending levels suggest a failed pregnancy. [11][12][13]
-
Additional studies
- CBC: to assess for blood loss anemia and determine baseline in patients with persistent bleeding
- Blood typing: to determine maternal Rh blood group
β-hCG levels above the discriminatory zone threshold without visualization of an intrauterine pregnancy on ultrasound should raise concern for spontaneous abortion or ectopic pregnancy. [14]
Management [2][3][5]
Approach
-
Clinically unstable patients
- Immediate hemodynamic support and stabilization (see “ABCDE approach”)
- Urgent OB/GYN consult for emergency surgical uterine evacuation
-
Stable patients
- Threatened abortion: expectant management
- Inevitable, incomplete, or missed abortion: expectant management, medical evacuation, or surgical evacuation
- Complete abortion: no intervention needed
- Inconclusive ultrasound findings: close follow-up with serial β-hCG measurements and repeat TVUS [6]
-
All patients
- If there is concern for septic abortion, obtain blood cultures, start broad-spectrum antibiotics, and consult OB/GYN.
-
Anti-D immunoglobulin for Rh(D)-negative patients [15]
- Consider for all patients with vaginal bleeding.
- Indicated after surgical evacuation
- Provide counseling on pregnancy loss and arrange for follow-up.
Consult OB/GYN for emergency surgical evacuation for miscarriage complicated by heavy bleeding, hemodynamic instability, or septic abortion.
Threatened abortion
- Expectant management: Symptoms will resolve or progress to inevitable, incomplete, or complete abortion.
- Advise the patient to avoid strenuous physical activity. [2]
- Prescribe as-needed oral analgesics (e.g., acetaminophen). [6]
- Educate patients on what to expect if tissue expulsion occurs and provide return precautions.
- Repeat pelvic ultrasound in one week.
Inevitable abortion, incomplete abortion, or missed abortion
Management of uncomplicated spontaneous abortions depends mostly on patient preference.
-
Expectant management (option for women ≤ 12 weeks gestation) [2]
- Watchful waiting as long as patient remains stable (i.e., no fever or significant hemorrhage) [2][5]
- The patient can choose to pursue surgical or medical evacuation at any time during the process. [3]
-
Medical evacuation
- Misoprostol is used to induce cervical ripening and expulsion of the products of conception.
- When available, pretreatment with mifepristone 24 hours prior is recommended. [2]
- See “Medical abortion” for details and regimens.
-
Surgical evacuation
- Indicated for septic abortion, heavy bleeding, or if there are maternal comorbidities
- Options
- First trimester: vacuum aspiration or dilation and curettage [2][3][6]
- Second trimester: dilation and evacuation
- Complications include uterine perforation, hemorrhage, endometritis, and/or intrauterine adhesions.
-
Additional measures and follow-up
- In patients managed expectantly or with medical evacuation:
- Prescribe as-needed oral analgesics (e.g., NSAIDs).
- Instruct patient on what to expect when tissue expulsion occurs. [3][5]
- Provide detailed return precautions
- Advise that surgical evacuation may be needed if complete expulsion is not achieved.
- Schedule follow-up to document resolution of pregnancy: e.g., with serum β-hCG and/or ultrasound. [2][3]
- In patients managed expectantly or with medical evacuation:
Instruct patients managed expectantly or with medical evacuation to seek medical attention without delay for heavy bleeding, fever, or any other concerning symptom.
Complications
See also “Complications of induced abortion.”
-
Septic abortion [7]
- Definition: an infection of the placenta and fetus before 20 weeks' gestation which is inevitably associated with fetal death
- Etiology
- Complication of missed, inevitable, or incomplete abortion
- Vaginal and/or uterine instrumentation
- Prolonged vaginal bleeding
-
Clinical features of septic abortion
- Fever
- Abdominal and/or pelvic pain
- Purulent vaginal discharge and/or bleeding
- Uterine tenderness
- Septic shock
- Management
- Broad-spectrum antibiotics with anerobic coverage (e.g., piperacillin-tazobactam ) [7]
- Source control: surgical evacuation of uterine cavity
- See also “Management of sepsis.”
-
Retained products of conception
- Tissue derived from a fertilized egg (e.g., fetus, placenta) that remains in the mother's body after delivery, pregnancy loss, or termination of pregnancy [16]
- Can result in the release of thromboplastin into systemic circulation → disseminated intravascular coagulation
- Endometritis
Prevention
- Minimize risk with treatment of maternal disease and adequate prenatal care.
- See also “Recurrent pregnancy loss.”
© AMBOSS
Acute management checklist
- Unstable patients: Initiate immediate hemodynamic support and consult OB/GYN urgently.
- Provide analgesia as needed.
- Evaluate for features of spontaneous pregnancy loss.
- Perform TVUS to assess for sonographic signs of IUP and fetal cardiac activity.
- Consider additional diagnostics (serum β-hCG, CBC, blood type).
- Threatened abortion: Educate patients and discharge with follow-up.
- Inevitable, incomplete, or missed abortion: Consult OB/GYN for further management.
- Septic abortion: Initiate broad-spectrum antibiotics and consult OB/GYN urgently.
Recurrent spontaneous abortion
This section only addresses recurrent pregnancy loss prior to 20 weeks' gestation, i.e., spontaneous abortions. Recurrent stillbirths may involve additional diagnostics and management.
Definitions [17]
Recurrent spontaneous abortion is defined as multiple spontaneous abortions. It may be further classified into either: [18][19][20][21]
- Primary recurrent spontaneous abortion: All prior pregnancies have ended in miscarriage.
- Secondary recurrent spontaneous abortion: The affected individual has had at least one live birth.
Etiology [17][20][21]
- Any cause of spontaneous abortion
- Common causes for recurrent spontaneous abortions include: [18][22][23]
- Chromosomal abnormalities
- Antiphospholipid syndrome
- Uterine structural abnormalities
- Hormonal and metabolic conditions
-
Risk factors include:
- Advanced parental age (especially maternal age > 40 years) [20]
- Number of prior pregnancy losses [17]
- Abnormal BMI (overweight or underweight) [24]
The most common treatable cause of recurrent pregnancy loss is antiphospholipid syndrome. [17]
The cause of recurrent pregnancy loss is not identified in more than half of affected individuals. [17][18]
Diagnosis [17][18][20][21]
Following a recurrent spontaneous abortion, send products of conception for genetic analysis and arrange further evaluation in consultation with appropriate specialists.
-
Clinical evaluation
- A detailed history
- Physical examination, including a pelvic exam
-
Laboratory tests: to evaluate for underlying medical conditions and chromosomal abnormalities [22]
-
All patients
- Antiphospholipid antibodies
- Diagnostics for hypothyroidism [18][20][21][25]
- Genetic analysis [22]
- Patients with indications
- Screening for diabetes mellitus
- Diagnostics for hyperprolactinemia
-
All patients
-
Imaging to detect uterine structural abnormalities [22][26]
- All patients: ultrasound pelvis (most common), sonohysterography [20][21][22]
- Patients with indications: MRI pelvis, hysteroscopy (most invasive)
Routine evaluation for inherited thrombophilia in individuals with recurrent pregnancy loss is not recommended. [18][20]
Management [17][18][23]
Refer all patients to a multidisciplinary team for appropriate management, which includes:
- Treatment of underlying conditions (e.g., treatment of hypothyroidism, management of antiphospholipid syndrome, surgery for structural abnormalities); see also “Medical conditions that affect pregnancy”
- Genetic counseling and possible preimplantation genetic testing
- Preconception counseling on diet and lifestyle changes [17]
- Counseling to address any psychosocial impacts
- Pharmacotherapy if additional indications are present (not used routinely)
- Vaginal progesterone [2][17][23]
- Low-dose aspirin [27]
Pregnant individuals with antiphospholipid syndrome should receive thromboprophylaxis for APS during pregnancy to prevent pregnancy loss. [28][29]
Stillbirth
Definition [30]
- Fetal death after 20 weeks' gestation (also known as intrauterine fetal demise) [2][4]
- If gestational age is unknown: death of a fetus weighing ≥ 350 g [2][4]
Etiology [30][31]
-
Maternal
- Fetal-maternal hemorrhage (FMH)
- Diabetes mellitus
- Hypertensive pregnancy disorders (especially if complicated by placental insufficiency or placental abruption)
- Uterine rupture
- Advanced age
- Heavy smoking
-
Fetoplacental
- Intrauterine growth restriction (which is most commonly due to placental insufficiency)
- Placental abnormalities (e.g., placental abruption, vasa previa)
- Infection (especially following premature rupture of membranes)
- Chromosomal abnormalities
- Congenital malformations
- Umbilical cord complications (nuchal cord or knot leading to fetal vascular compromise)
- Fetal hydrops
-
Miscellaneous
- Unknown (in some studies, more than half of all stillbirths were of unknown etiology)
- Environmental (exposure to toxins such as drugs or maternal smoking during pregnancy)
Clinical features [32]
- Absence of fetal movements and cardiac activity
- Delivery of a fetus with no signs of life
Diagnostics [30]
- Ultrasonography: to confirm absence of fetal cardiac activity
-
Evaluation of underlying cause: indicated in all cases
- Maternal and family history
- Maternal Kleihauer-Betke test or flow cytometry [30]
- Examination of the placenta, fetal membranes, and umbilical cord
- Fetal autopsy
- Genetic analysis (e.g., fetal karyotype)
Management [30][32]
- All patients: Obtain an OB/GYN consult.
-
Timing of delivery: Spontaneous labor usually begins within 2 weeks of intrauterine fetal death.
- Maternal health risk (i.e., preeclampsia, sepsis, placental abruption, or membrane rupture): Expedite delivery.
- No maternal health risk: Deliver or consider short-term expectant management according to patient preference.
-
Method of delivery
- Spontaneous or induced vaginal delivery (e.g., with vaginal misoprostol or oxytocin infusion) is usually safer than cesarean delivery. [30]
- Cesarean delivery may be considered based on patient preference and maternal condition.
- Dilation and evacuation may be considered as an alternative during the second trimester.
-
Supportive measures: Also see “Counseling on pregnancy loss.”
- Express empathy and acknowledge patient grief.
- Provide privacy and emotional support.
- Offer contact between parents and the stillborn baby after delivery. [32][33]
- Administer anti-D immunoglobulin to Rh(D)-negative patients. [15]
- Offer parents a fetal autopsy to determine the cause of death.
- See also “Postpartum care following stillbirth or neonatal death.”
Complications
- Retained products of conception
- Endometritis
External Resources
- 2020 ACOG/SMFM Obstetric Care Consensus: Management of Stillbirth
- 2018 ACOG Practice Bulletin No. 200: Early Pregnancy Loss
- 2018 ACR Appropriateness Criteria First Trimester Vaginal Bleeding
- 2016 ACEP Clinical Policy: Initial Evaluation and Management of Patients Presenting to the ED in Early Pregnancy
- Guttmacher Institute Overview of Abortion Laws
- 2012 American Society for Reproductive Medicine committee opinion on evaluation and treatment of recurrent pregnancy loss
- 2022 European Society of Human Reproduction and Embryology (ESHRE) guideline on the management of recurrent pregnancy loss
- 2023 Royal College of Obstetricians and Gynaecologists guideline on recurrent miscarriage
- 2024 ACOG Clinical Expert Series Evaluation of Recurrent Pregnancy Loss
References
- Beckmann CRB. "Obstetrics and Gynecology". Lippincott Williams & Wilkins. (2010). ISBN: 0781788072
- American College of Obstetricians and Gynecologists Committee on Practice Bulletins—Gynecology. "ACOG Practice Bulletin No. 200: Early Pregnancy Loss (reaffirmed 2025)". Obstet Gynecol. 132(5). :e197-e207. (2018)
- Prine LW, MacNaughton H. "Office management of early pregnancy loss". Am Fam Physician. 84(1). :75-82. (2011)
- Blencowe H, Hug L, Moller A, You D, Moran A. "Definitions, terminology and standards for reporting of births and deaths in the perinatal period: International Classification of Diseases (<scp>ICD</scp>‐11)". International Journal of Gynecology & Obstetrics. 168(1). :1-9. (2024)
- Jurkovic D, Overton C, Bender-Atik R. "Diagnosis and management of first trimester miscarriage". BMJ. 346(jun19 2). :f3676-f3676. (2013)
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904
- Eschenbach DA. "Treating Spontaneous and Induced Septic Abortions". Obstet Gynecol. 125(5). :1042-1048. (2015)
- Zolotor AJ, Carlough MC. "Update on prenatal care". Am Fam Physician. 89(3). :199-208. (2014)
- Brown DL, Packard A, Maturen KE, et al. "ACR Appropriateness Criteria® First Trimester Vaginal Bleeding". J Am Coll Radiol. 15(5). :S69-S77. (2018)
- Hahn SA, Promes SB, Brown MD, et al. "Clinical Policy: Critical Issues in the Initial Evaluation and Management of Patients Presenting to the Emergency Department in Early Pregnancy". Ann Emerg Med. 69(2). :241-250.e20. (2017)
- Barnhart K, Franasiak J, and the Committee on Practice Bulletins—Gynecology. "ACOG Practice Bulletin No. 191: Tubal Ectopic Pregnancy". Obstet Gynecol. 131(2). :e65-e77. (2018)
- Hendriks E, Rosenberg R, Prine L. "Ectopic Pregnancy: Diagnosis and Management". Am Fam Physician. 101(10). :599-606. (2020)
- Van Mello NM, Mol F, Opmeer BC, et al. "Diagnostic value of serum hCG on the outcome of pregnancy of unknown location: a systematic review and meta-analysis". Hum Reprod Update. 18(6). :603-617. (2012)
- Hendriks E, MacNaughton H, MacKenzie MC. "First Trimester Bleeding: Evaluation and Management". Am Fam Physician. 99(3). :166-174. (2019)
- American College of Obstetricians and Gynecology Committee on Practice Bulletins—Obstetrics. "Practice Bulletin No. 181: Prevention of Rh D Alloimmunization (reaffirmed 2024)". Obstet Gynecol. 130(2). :e57-e70. (2017)
- Guarino A, Di Benedetto L, Assorgi C, Rocca A, Caserta D. "Conservative and timely treatment in retained products of conception: a case report of placenta accreta ritention". Int J Clin Exp Pathol. 8(10). :13625-9. (2015)
- American College of Obstetricians and Gynecologists. "Management of Stillbirth: Obstetric Care Consensus No, 10". Obstet Gynecol. 135(3). :e110-e132. (2020)
- Reddy UM, Goldenberg R, Silver R, et al. "Stillbirth Classification—Developing an International Consensus for Research". Obstet Gynecol. 114(4). :901-914. (2009)
- Tsakiridis I, Giouleka S, Mamopoulos A, Athanasiadis A, Dagklis T. "Investigation and management of stillbirth: a descriptive review of major guidelines". J Perinat Med. 50(6). :796-813. (2022)
- Hennegan JM, Henderson J, Redshaw M. "Contact with the baby following stillbirth and parental mental health and well-being: a systematic review". BMJ Open. 5(11). :e008616. (2015)
- Dimitriadis E, Menkhorst E, Saito S, Kutteh WH, Brosens JJ. "Recurrent pregnancy loss". Nat Rev Dis Primers. 6(1). (2020)
- Practice Committee of the American Society for Reproductive Medicine. "Evaluation and treatment of recurrent pregnancy loss: a committee opinion". Fertil Steril. 98(5). :1103-1111. (2012)
- Practice commitee of the American Society for Reproductive Medicine. "Definitions of infertility and recurrent pregnancy loss: a committee opinion". Fertil Steril. 113(3). :533-535. (2020)
- "ESHRE Guideline on the management of recurrent pregnancy loss". https://web.archive.org/web/20240820194629/https://www.eshre.eu/Guidelines-and-Legal/Guidelines/Recurrent-pregnancy-loss. [2023-02-01]
- Regan L, Rai R, Saravelos S, Li T. "Recurrent Miscarriage Green‐top Guideline No. 17". BJOG. 130(12). (2023)
- de Assis V, Giugni CS, Ros ST. "Evaluation of Recurrent Pregnancy Loss". Obstet Gynecol. (2024)
- Chester MR, Tirlapur A, Jayaprakasan K. "Current management of recurrent pregnancy loss". The Obstetrician & Gynaecologist. 24(4). :260-271. (2022)
- Ng KYB, Cherian G, Kermack AJ, et al. "Systematic review and meta-analysis of female lifestyle factors and risk of recurrent pregnancy loss". Scientific Reports. 11(1). (2021)
- Barbhaiya M, Zuily S, Naden R, et al. "The 2023 ACR/EULAR Antiphospholipid Syndrome Classification Criteria". Arthritis Rheumatol. 75(10). :1687-1702. (2023)
- Wall DJ, Reinhold C, Akin EA, et al. "ACR Appropriateness Criteria® Female Infertility". J Am Coll Radiol. 17(5). :S113-S124. (2020)
- ACOG Committee on Obstetric Practice. "ACOG Committee Opinion No. 743: Low-Dose Aspirin Use During Pregnancy". Obstet Gynecol. 132(1). :e44-e52. (2018)
- Tektonidou MG, Andreoli L, Limper M, et al. "EULAR recommendations for the management of antiphospholipid syndrome in adults". Ann Rheum Dis. 78(10). :1296-1304. (2019)
- Schreiber K, Sciascia S, de Groot PG, et al. "Antiphospholipid syndrome". Nat Rev Dis Primers. 4(1). (2018)