Summary
Preterm labor is defined as regular uterine contractions and cervical changes before 37 weeks' gestation. Preterm birth is defined as live birth between 20 0/7 weeks and 36 6/7 weeks' gestation. Risk factors for preterm labor include a previous preterm birth, a short cervical length during pregnancy, and multiple gestations. Diagnosis is usually based on the presence of regular contractions, cervical effacement, and/or rupture of membranes. The risk of impending delivery may be assessed by cervical length ultrasonography and fetal fibronectin test. Management depends on gestational age and can include tocolysis, antenatal steroids to improve fetal lung maturity, and magnesium sulfate for fetal neuroprotection. Tocolytics may be used for short-term prolongation of pregnancy to allow time for steroids and magnesium sulfate to take effect and for transportation to an appropriate hospital. Fetal complications of preterm birth include intraventricular hemorrhage, neonatal respiratory distress syndrome, and necrotizing enterocolitis. Strategies for prevention of preterm birth include reduction in modifiable risk factors, screening for short cervical length, and management of cervical insufficiency and short cervical length (e.g., with progesterone supplementation).
Definitions
- Preterm labor: regular uterine contractions with cervical effacement, dilation, or both before 37 weeks' gestation [1]
-
Preterm birth
- Live birth between 20 0/7 weeks' and 36 6/7 weeks' gestation
- WHO subcategories [2]
- Extremely preterm (< 28 weeks)
- Very preterm (28 to < 32 weeks)
- Moderate to late preterm (32 to < 37 weeks)
Epidemiology
- Complications of preterm birth are the leading cause of death in children < 5 years of age worldwide. [2]
- About half of patients who deliver prematurely are diagnosed with preterm labor. [1]
- Preterm birth rate in the US: ∼ 12% of all live births [3][4]
- African-American women are 50% more likely to give birth prematurely compared to white women.
Epidemiological data refers to the US, unless otherwise specified.
Etiology
The exact mechanisms underlying premature labor are not well understood, but certain risk factors have been identified. [5][6]
Nonmodifiable risk factors
- History of preterm birth (greatest risk factor)
- Cervical insufficiency
- History of cervical surgery (e.g., conization)
- Short cervical length
- Multiple gestations
- Polyhydramnios
- Preterm premature rupture of membranes (PPROM)
-
Antepartum hemorrhage caused by:
- Placenta previa
- Placental abruption
- Uterine anomalies (e.g., anomalies of Mullerian duct fusion, uterine fibroids)
- Black individuals of non-Hispanic origin [7]
- Congenital abnormalities of the fetus [8]
Modifiable risk factors
-
Maternal and fetal conditions
- Infections (e.g., urinary tract infections, STIs, vaginal infections )
- Trauma (e.g., intimate partner violence) [9]
- Hypertensive pregnancy disorders (e.g., preeclampsia, HELLP syndrome)
- Diabetes mellitus, gestational diabetes
-
Lifestyle and environmental factors
- Smoking
- Substance use (e.g., heavy alcohol use, heroin, cocaine)
- Maternal or fetal stress
- Maternal age (≤ 18 years, > 35 years) [10]
- Low maternal prepregnancy weight
- Short interval between pregnancies (< 18 months) [5]
Clinical features
- Regular uterine contractions and associated symptoms of labor (e.g., lower back pain)
- Loss of mucus plug (bloody show)
- Cervical effacement and/or cervical dilation
- Rupture of membranes
- See “First stage of labor.”
To decrease the risk of infection, avoid digital cervical examinations until PPROM has been ruled out. [5][11]
Diagnosis
The diagnosis of preterm labor is made clinically based on preterm contractions and cervical changes. The presence of risk factors for preterm labor can help establish the diagnosis. Fetal fibronectin levels and cervical length measurements can help assess the risk of impending delivery.
Initial evaluation [1][5]
- Evaluate for clinical features of preterm labor.
- Determine gestational age.
- Perform sterile speculum examination.
- Evaluate for cervical effacement and/or cervical dilation. [5]
- Assess for rupture of membranes, e.g. by performing the fern test.
- Obtain vaginal swabs for additional laboratory studies.
- Perform fetal status assessment.
Laboratory studies [1][5]
-
Cervicovaginal fetal fibronectin (fFN) test
- Used to help differentiate between true preterm labor and false labor [5]
- Elevated levels in cervical secretions are associated with an increased risk of preterm delivery. [5][12]
- To rule out infections:
- Prenatal screening for group B Streptococcus (GBS)
- STI screening, if indicated (see “Indications for third-trimester STI screening”)
- Urinalysis and urine culture
Ultrasound [5][13]
- Transvaginal ultrasound: Cervical length > 3 cm indicates a low likelihood of delivery within 14 days. [5]
-
Obstetric ultrasound
- Identifies fetal, placental, or maternal anatomical abnormalities
- Measures fetal gestational age and weight
- Confirms fetal position and fetal presentation
- Determines amniotic fluid index
As cervical length and fetal fibronectin levels each have a low positive predictive value, neither should be used in isolation to assess the risk of preterm delivery. [1]
Treatment
Approach [1][5]
-
All patients < 37 weeks' gestation
- Consult OB/GYN to determine the appropriate management.
- Administer group B streptococcus prophylaxis, if indicated (see “GBS prophylaxis considerations in preterm labor”).
- Prepare for immediate care for the newborn and possible neonatal resuscitation.
- If necessary, initiate transfer to a hospital able to provide maternal and neonatal care.
-
34 0/7 to 36 6/7 weeks' gestation
- Proceed with normal labor and delivery.
- Consider steroids for induction of fetal lung maturity.
-
< 34 weeks' gestation
- Consider tocolysis to inhibit uterine contractions in consultation with OB/GYN.
- Administer steroids for induction of fetal lung maturity.
- Administer antibiotic prophylaxis for PPROM.
-
< 32 weeks' gestation
- Administer magnesium sulfate for fetal neuroprotection.
- Administer steroids for induction of fetal lung maturity.
Activity restriction, including bed rest, is not routinely recommended and may result in adverse outcomes. [1][14]
Tocolysis [1][5][15]
Overview
- Definition: administration of tocolytics to inhibit uterine contractions [16]
- Goal: prolonging pregnancy to allow for induction of fetal lung maturity and/or transfer to another medical center, if necessary
- Duration: up to 48 hours
-
Contraindications
- Maternal-specific drug contraindications
- Nonreassuring fetal cardiotocography
- Intrauterine fetal demise
- Chorioamnionitis
- Antepartum hemorrhage with hemodynamic instability
- Severe preeclampsia or eclampsia
- Lethal fetal anomaly
Do not delay labor by administering tocolytics if there is evidence of fetal demise, abruption, eclampsia, or intrauterine infection. [17]
Long-term use of tocolytics does not prevent preterm birth and does not improve neonatal outcomes. [1]
Options
| Tocolytics [1][18][19] | ||
|---|---|---|
| Medication | Maternal adverse effects | Fetal adverse effects |
| Nifedipine (calcium channel blocker) |
|
|
| Indomethacin (NSAID) |
|
|
| Terbutaline (beta-2 adrenergic agonist) |
|
|
| Magnesium sulfate |
|
|
There are no FDA-approved tocolytic drugs; all agents are used off-label.
Induction of fetal lung maturity [1][21]
- Definition: administration of antenatal steroids to promote the production of surfactant and thereby improve neonatal survival and fetal lung maturity
-
Indications
- Patients at 34 0/7 to 36 6/7 weeks' gestation if:
- Steroids not previously given
- No evidence of chorioamnionitis
- Delivery anticipated between 24 hours and 7 days
- Patients at 24 0/7 to 33 6/7 weeks' gestation
- Initial course: all patients at risk of delivery within 7 days
- Second course: patients at risk of delivery within 7 days whose prior course was > 14 days ago
- Patients at 34 0/7 to 36 6/7 weeks' gestation if:
-
Options (off-label use)
- Betamethasone [1]
- Dexamethasone [1]
Fetal neuroprotection
- Definition: administration of antenatal magnesium sulfate to reduce the risk and severity of neurological disorders (e.g., cerebral palsy) [1]
- Indication: preterm labor at < 32 weeks' gestation [5]
- Dosing: Follow local protocols. [1]
Antibiotics [1][22]
- Not recommended for the prevention of preterm delivery
-
Antibiotics are indicated for:
- GBS prophylaxis
- PPROM antibiotic prophylaxis
Acute management checklist
- Determine gestational age.
- Sterile speculum examination to evaluate cervix and exclude PPROM
- Fetal status assessment
- Rule out infections: urinalysis and culture, prenatal GBS screening, STI screening (if indicated)
- Consider fFN test and cervical length measurement.
- Consult OB/GYN and/or consider transfer to an appropriate facility.
- GBS prophylaxis, if indicated
- 34 0/7 to 36 6/7 weeks' gestation: Proceed with normal labor and delivery.
- < 34 weeks' gestation
- Consider tocolysis.
- Steroids for induction of fetal lung maturity
- Antibiotics for PPROM
- < 32 weeks' gestation: Consider fetal neuroprotection.
Complications
Pulmonary and cardiovascular
- Neonatal respiratory distress syndrome
- Patent ductus arteriosus (PDA)
- Bronchopulmonary dysplasia (BPD)
Neurological complications of prematurity
Periventricular leukomalacia (PVL)
- Definition: symmetrical, periventricular injury of cerebral white matter (necrosis and cystic formation) caused by ischemia and/or infection
- Epidemiology: mainly affects premature infants
- Clinical features: features of spastic cerebral palsy, intellectual impairment, and visual disturbances
- Diagnostics: brain imaging using ultrasound, cranial CT, or MRI
Intraventricular hemorrhage (IVH) [23]
- Definition: Bleeding into the ventricles from the germinal matrix, a highly vascularized region within the subventricular zone of the brain from which cells migrate out during brain development.
-
Etiology: associated with a number of risk factors
- Birth weight < 1500 g and delivery before 32 weeks' gestation due to the fragility of the germinal matrix and/or impaired autoregulation of blood pressure
- Maternal chorioamnionitis
- Hypoxia during or after birth
-
Pathophysiology
- Immaturity of the basal lamina and lack of astrocytic glial fibrillary acidic protein within the germinal matrix leads to abnormal cerebral autoregulation.
- Alterations in an infant's blood pressure (e.g., during birth, intubation) → failure of cerebral autoregulation to compensate for the change in blood pressure → rupture of and bleeding from vessels in the germinal matrix → rupture of ependyma → blood flows into the ventricles
-
Clinical features
- Usually occurs within the first days of life (up to day 5)
- Most infants are asymptomatic, but saltatory (for several days) or, more rarely, catastrophic (over minutes to hours) courses are also possible.
- Lethargy, hypotonia, irregular respirations, seizures, bulging anterior fontanelle
- Cranial nerve abnormalities (e.g., pupils react sluggishly to light) and changes in eye movement (e.g., roving eye movements)
- Signs of acute blood loss (e.g., anemia, tachycardia)
-
Diagnostics
-
Cranial ultrasound: allows grading of IVH based upon the location and extent to assess severity [24]
- Grade I: bleeding confined to germinal matrix and ≤ 10% of the ventricular area
- Grade II: 10–50% of the lateral ventricle volume occupied by germinal matrix and IVH
- Grade III: > 50% of the lateral ventricle volume occupied by germinal matrix and IVH, ventricular distortion
- Periventricular hemorrhagic infarction: hemorrhagic infarction in periventricular white matter ipsilateral to IVH
- Since most patients are asymptomatic, screening ultrasounds are routinely performed in infants with a birth weight < 1500 g and delivery before 30 weeks' gestation. [25]
-
Cranial ultrasound: allows grading of IVH based upon the location and extent to assess severity [24]
-
Treatment
- Supportive
- Lumbar puncture, diuretics, and/or ventriculoperitoneal shunt in severe IVH
Other
- Cerebral palsy
- Learning disabilities
- Developmental delays
- ADHD
Homeostasis
-
Hypothermia of prematurity [26]
- Definition: impaired ability to produce an adequate body temperature due to a high surface area: volume ratio
- Clinical features: body temperature < 36.5°C (< 97.7°F), lethargy, cyanosis
- Treatment: rewarming in an incubator or radiant warmer
- Apnea, bradycardia
- Hypoglycemia, hyperglycemia
Other
-
Anemia of prematurity
- Definition: impaired ability to produce adequate erythropoietin (EPO)
- Clinical features: usually asymptomatic, possible symptoms include tachycardia, poor weight gain, increased episodes of apnea
- Pathophysiology: onset of breathing and closure of ductus arteriosus → ↑ tissue oxygenation → ↓ erythropoiesis
- Diagnostics: should be suspected in premature infants with low hemoglobin, hematocrit, and reticulocyte count
- Treatment: iron supplementation, blood transfusions (severe cases)
- Retinopathy of prematurity (ROP)
- Necrotizing enterocolitis (NEC)
- Infection and sepsis (e.g., neonatal sepsis, neonatal pneumonia)
Morbidity and mortality in preterm infants increase with decreasing birth weight and gestational age.
")

")
We list the most important complications. The selection is not exhaustive.
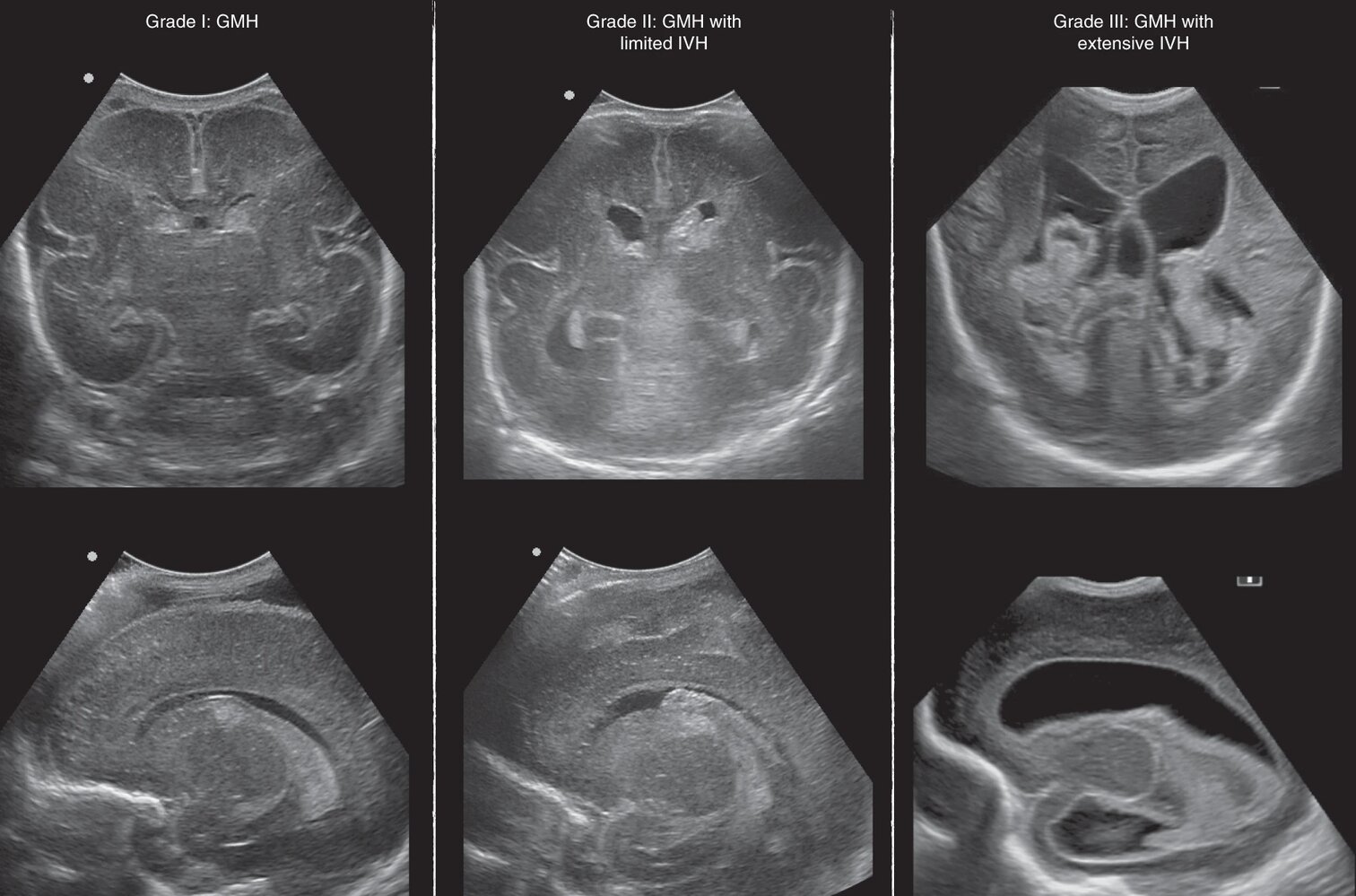
Ultrasound head (top row: coronal plane; bottom row: parasagittal plane) of a newborn
The first column shows bleeding confined to the subependymal germinal matrix (red overlay), which is consistent with grade 1 IVH.
The second column shows blood occupying less than 50% of the left lateral ventricle (red overlay), with no enlargement of the lateral ventricles (yellow overlay) or the cavum septi pellucidi (green overlay). In addition, the choroid plexus is clearly demarcated (blue overlay). Together, these findings are consistent with grade 2 IVH.
The third column shows blood occupying more than 50% of the lateral ventricles (red overlay) with enlargement of the cavum septi pellucidi (green overlay) and both lateral ventricles (yellow overlay). This appearance is consistent with grade 3 IVH.
These features suggest impaired progressive posthemorrhagic ventricular dilatation (PHVD) due to associated impairment of CSF circulation, which is a potential complication of high-grade IVH.
Source: “Figure 3, in: Cranial ultrasound findings in preterm germinal matrix haemorrhage, sequelae and outcome” by A. Parodi, P. Govaert, S. Horsch et al., Pediatric Research, licensed under CC BY 4.0. Modifications: Image cropped. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

© AMBOSS

Preterm infant born at 23 weeks of gestation with approximate weight of 500 g. The immature skin is very thin, transparent, and sensitive.
© AMBOSS
Prevention
Primary prevention [7][27]
- Address risk factors for preterm labor for all patients, including:
- Screening for hypertensive pregnancy disorders
- Screening for gestational diabetes
- Screening for infections (see “Prenatal screening for medical comorbidities”)
- Counseling on smoking cessation
- For singleton pregnancies: Manage cervical insufficiency and short cervical length, e.g., vaginal progesterone and/or cervical cerclage. [5]
- The following measures are not recommended due to a lack of efficacy: [7]
- Screening for and prophylactic treatment of bacterial vaginosis in asymptomatic individuals [28]
- Prophylactic intramuscular progesterone [27]
- Activity restrictions (e.g., bed rest)
Screening
Evaluation for short cervical length can identify individuals at increased risk for preterm birth.
| Screening for short cervical length [5][7][27] | |||
|---|---|---|---|
| Screening modality and interval | Follow-up of abnormal results | ||
| Singleton pregnancy | History of preterm birth |
|
|
| No history of preterm birth |
|
|
|
| Multiple pregnancy [27] | |||
External Resources
- 2023 ACOG Practice Advisory: Updated Clinical Guidance for the Use of Progesterone Supplementation for the Prevention of Recurrent Preterm Birth
- 2022 WHO Recommendation on Tocolytic Therapy for Improving Preterm Birth Outcomes
- 2022 WHO Recommendations on Antenatal Corticosteroids for Improving Preterm Birth Outcomes
- 2021 ACOG Practice Bulletin No. 234: Prediction and Prevention of Spontaneous Preterm Birth
- 2016 ACOG Practice Bulletin No. 171: Management of Preterm Labor
References
- American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins. "Practice Bulletin No. 171: Management of Preterm Labor". Obstetrics & Gynecology. 128(4). :e155-e164. (2016)
- "Preterm Birth Fact Sheet". http://www.who.int/mediacentre/factsheets/fs363/en/. [2016-11-01]
- "Reproductive Health - Preterm Birth". https://web.archive.org/web/20170513085140/https://www.cdc.gov/reproductivehealth/maternalinfanthealth/pretermbirth.htm. [2016-11-10]
- Carmen Giurgescu, Amelia Banks, Barbara L. Dancy, Kathleen Norr. "African American Women's Views of Factors Impacting Preterm Birth". MCN: The American Journal of Maternal/Child Nursing. 38(4). :229-234. (2014)
- Rundell K, Panchal B. "Preterm Labor: Prevention and Management". Am Fam Physician. 95(6). :366-372. (2017)
- Goldenberg RL, Culhane JF, Iams JD, et al. "Epidemiology and causes of preterm birth". Lancet. 371(9606). :75-84. (2008)
- ACOG. "Prediction and Prevention of Spontaneous Preterm Birth, Practice Bulletin 234". Obstet Gynecol. 138(2). :e65-e90. (2021)
- Honein MA, Kirby RS, Meyer RE, et al. "The Association Between Major Birth Defects and Preterm Birth". Matern Child Health J. 13(2). :164-175. (2008)
- Jafari Kafiabadi M, Sabaghzadeh A, Khabiri SS, et al. "Orthopedic Trauma During Pregnancy; a Narrative Review". Arch Acad Emerg Med. 10(1). :e39. (2022)
- Cavazos-Rehg PA, Krauss MJ, Spitznagel EL, et al. "Maternal Age and Risk of Labor and Delivery Complications". Matern Child Health J. 19(6). :1202-1211. (2014)
- "Updated Clinical Guidance for the Use of Progesterone Supplementation for the Prevention of Recurrent Preterm Birth". https://web.archive.org/web/20230726180510/https://www.acog.org/clinical/clinical-guidance/practice-advisory/articles/2023/04/updated-guidance-use-of-progesterone-supplementation-for-prevention-of-recurrent-preterm-birth. [2023-04-01]
- Owens DK, Davidson KW, et al. "Screening for Bacterial Vaginosis in Pregnant Persons to Prevent Preterm Delivery". JAMA. 323(13). :1286. (2020)
- AIUM, ACR, ACOG, et al. "AIUM-ACR-ACOG-SMFM-SRU Practice Parameter for the Performance of Standard Diagnostic Obstetric Ultrasound Examinations". J Ultrasound Med. 37(11). :E13-E24. (2018)
- Owens R. "Intraventricular Hemorrhage in the Premature Neonate". Neonatal Network. 24(3). :55-71. (2005)
- Bassan H. "Ultrasonographic Features and Severity Scoring of Periventricular Hemorrhagic Infarction in Relation to Risk Factors and Outcome". Pediatrics. 117(6). :2111-2118. (2006)
- Hand IL, Shellhaas RA, Milla SS. "Routine Neuroimaging of the Preterm Brain". Pediatrics. 146(5). :e2020029082. (2020)
- Demtse AG, Pfister RE, Nigussie AK, et al. "Hypothermia in Preterm Newborns: Impact on Survival". Global Pediatric Health. 7. :2333794X2095765. (2020)
- Lauder J, Sciscione A, Biggio J, Osmundson S. "Society for Maternal-Fetal Medicine Consult Series #50: The role of activity restriction in obstetric management". Am J Obstet Gynecol. 223(2). :B2-B10. (2020)
- Vogel JP, Ramson J, Darmstadt GL, et al. "Updated WHO recommendations on antenatal corticosteroids and tocolytic therapy for improving preterm birth outcomes". The Lancet Global Health. 10(12). :e1707-e1708. (2022)
- Haas DM, Caldwell DM, Kirkpatrick P, McIntosh JJ, Welton NJ. "Tocolytic therapy for preterm delivery: systematic review and network meta-analysis". BMJ. 345(oct09 2). :e6226-e6226. (2012)
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904
- Caritis S. "Adverse effects of tocolytic therapy". BJOG. 112. :74-78. (2005)
- Lamont RF, Jørgensen JS. "Safety and Efficacy of Tocolytics for the Treatment of Spontaneous Preterm Labour". Curr Pharm Des. 25(5). :577-592. (2019)
- Yokoyama K, Takahashi N, Yada Y, et al. "Prolonged maternal magnesium administration and bone metabolism in neonates". Early Hum Dev. 86(3). :187-191. (2010)
- ACOG. "Committee Opinion No. 713: Antenatal Corticosteroid Therapy for Fetal Maturation". Obstetrics & Gynecology. 130(2). :e102-e109. (2017)
- Kenyon S, Boulvain M, Neilson JP. "Antibiotics for preterm rupture of membranes". Cochrane Database Syst Rev. (2003)
- American College of Obstetricians and Gynecologists. "Prelabor Rupture of Membranes: ACOG Practice Bulletin, Number 217". Obstet Gynecol. 135(3). :e80-e97. (2020)
- van Baaren GJ, Vis JY, Wilms FF, et al. "Predictive Value of Cervical Length Measurement and Fibronectin Testing in Threatened Preterm Labor". Obstet Gynecol. 123(6). :1185-1192. (2014)
- Coutinho CM, Sotiriadis A, Odibo A, et al. "ISUOG Practice Guidelines: role of ultrasound in the prediction of spontaneous preterm birth". Ultrasound Obstet Gynecol. 60(3). :435-456. (2022)