Summary
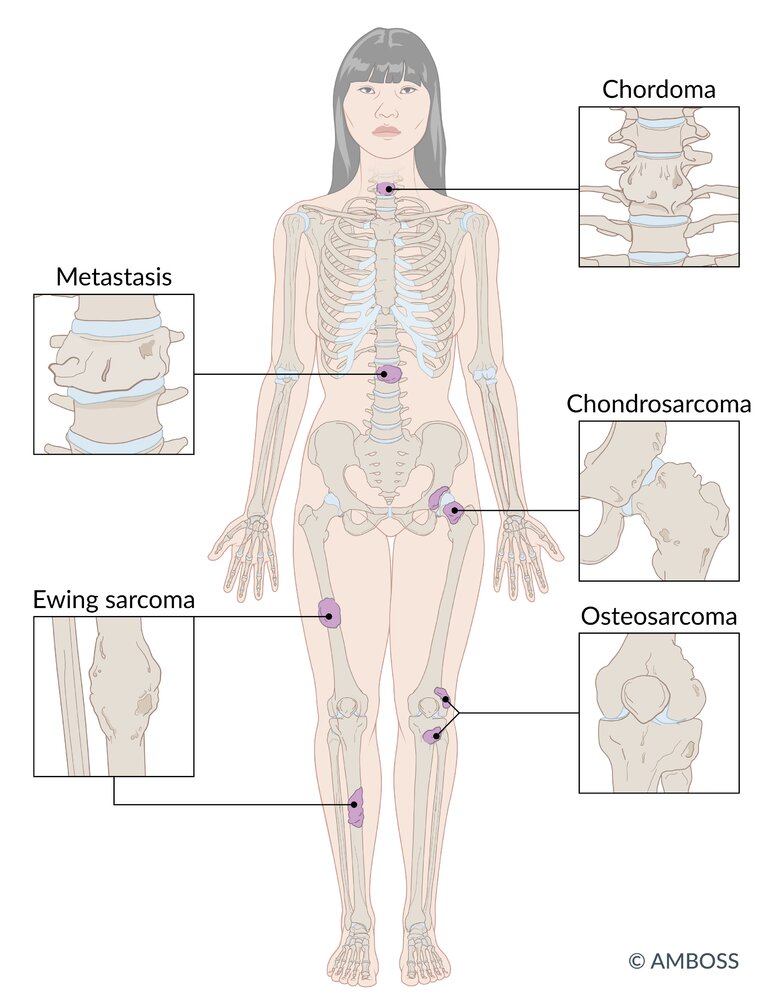
Primary malignant bone tumors are rare malignant tumors that arise from native bone tissue, such as osteoblasts, chondrocytes, and mesenchymal stem cells. Osteosarcoma and Ewing sarcoma are the most common types in children and adolescents, while chondrosarcoma is most common in adults. Initial manifestations typically include localized pain and swelling, which may become apparent after an injury to the site. Primary malignant bone tumors may metastasize hematogenously to the lungs and skeletal system; regional spread and skip lesions may also occur. X-ray is the preferred initial diagnostic test. Characteristic radiographic features include a focal lytic and/or sclerotic lesion, typically with an aggressive periosteal reaction. If a primary malignant bone tumor is suspected, prompt specialist referral (e.g., to orthopedic oncology) is recommended for diagnostic confirmation on biopsy, staging, and further management. When feasible, complete surgical excision of the primary tumor is preferred. Ewing sarcoma, unlike other primary malignant bone tumors, is also responsive to definitive radiotherapy. Combination chemotherapy and adjuvant radiation therapy are often indicated for the management of osteosarcoma and Ewing sarcoma but are generally less effective in the management of chondrosarcoma. Long-term surveillance for early detection of recurrence is recommended.
Overview
Types of primary malignant bone tumors
| Overview of primary malignant bone tumors | |||
|---|---|---|---|
| | Osteosarcoma [1] | Ewing sarcoma [1] | Chondrosarcoma [2][3] |
| Age group |
|
|
|
| Typical location of primary tumor |
|
|
|
| Characteristic x-ray findings |
|
|
|
| Treatment of localized disease |
|
|
|
| Five-year survival rate |
|
|
|





Clinical features [1][6]
-
Localized pain
- Intermittent at first; progresses to pain at rest [7]
- May worsen at night
- May manifest after minor trauma
- Localized swelling, sometimes associated with tenderness and erythema
- B symptoms may be present, especially in patients with Ewing sarcoma.
- Decreased range of motion if the tumor is near a joint
- Altered gait (e.g., limp) [8]
- Pathological fractures may be the presenting symptom.
Primary bone tumors often present insidiously with intermittent symptoms. Maintain a low threshold to evaluate persistent or recurrent bone pain or swelling. [1]
Diagnostic approach to suspected primary malignant bone tumors [1][6][9]
- Obtain a comprehensive medical history and perform a thorough physical examination.
- Consider common differential diagnoses of bone pain.
- Obtain an x-ray of the area of interest (initial test of choice).
- Symptomatic bone lesion identified on x-ray:
- Patients aged < 40 years: Refer to specialist (e.g., orthopedic oncology) for further evaluation, including: [1]
- Additional imaging (e.g., MRI ± CT of primary site; CT chest, FDG-PET/CT, and/or bone scan to evaluate for metastases)
- Staging (prior to obtaining a biopsy)
- Confirmation of diagnosis with incisional biopsy or core needle biopsy [1]
- Patients aged ≥ 40 years: Perform diagnostic evaluation for bone metastases as indicated.
- Patients aged < 40 years: Refer to specialist (e.g., orthopedic oncology) for further evaluation, including: [1]
- Normal or equivocal findings on x-ray but high clinical suspicion for primary malignant bone tumor:
- Obtain an MRI without or without and with IV contrast of the area of interest. [9]
- Consider referral to specialist (e.g., orthopedic oncology).
- Consider supportive laboratory studies (e.g., CMP with calcium, ALP, LDH, CBC, ESR, CRP). [7]
- Refer for genetic counseling and testing in selected patients (e.g., patients with hereditary cancer syndromes, family history of bone sarcoma).
Staging of a suspected primary malignant bone tumor should be performed by a specialist before biopsy. [1]
In individuals aged < 40 years, the likelihood of a bone lesion being a primary malignant bone tumor is high. [1]
Differential diagnosis of bone pain [1][7]
- Growing pains
- Musculoskeletal injury (e.g., stress fractures)
- Osteomyelitis
- Avascular necrosis
- Acute gout
-
Benign bone tumors, e.g.:
- Osteochondroma
- Giant cell tumor of the bone
- Aneurysmal bone cysts
- Chondroblastoma
- Langerhans cell histiocytosis
- Bone metastasis
- Multiple myeloma
- Paget disease of bone
- Hyperparathyroidism
Management [1][6]
- When feasible, complete surgical excision of the primary tumor is preferred. [1]
- Ewing sarcoma is also responsive to definitive radiotherapy.
- Additional treatment (e.g., neoadjuvant and adjuvant chemotherapy, radiation therapy) varies based on specific cancer type; see respective sections for details.
- Refer patients planning for chemotherapy for fertility consultation.
- In successfully treated patients, long-term surveillance is necessary to monitor for recurrence and post-treatment complications.
- See "Principles of cancer care" for general management strategies for patients with cancer.
© AMBOSS

X-ray of the right femorotibial joint (AP view) of a 17-year-old male patient
A sclerotic outgrowth of the bone (green overlay) surrounded by osteolytic destruction of medullary and cortical bone (red overlay) is visible on the medial metaphysis of the femur.
The periosteum over the lesion is noncontinuous (dashed line), indicating rapid growth of the bone lesion.
This appearance of a mixed osteosclerotic and osteolytic lesion in the metaphyses of long bones is characteristic of osteosarcoma.
Source: © IMPP
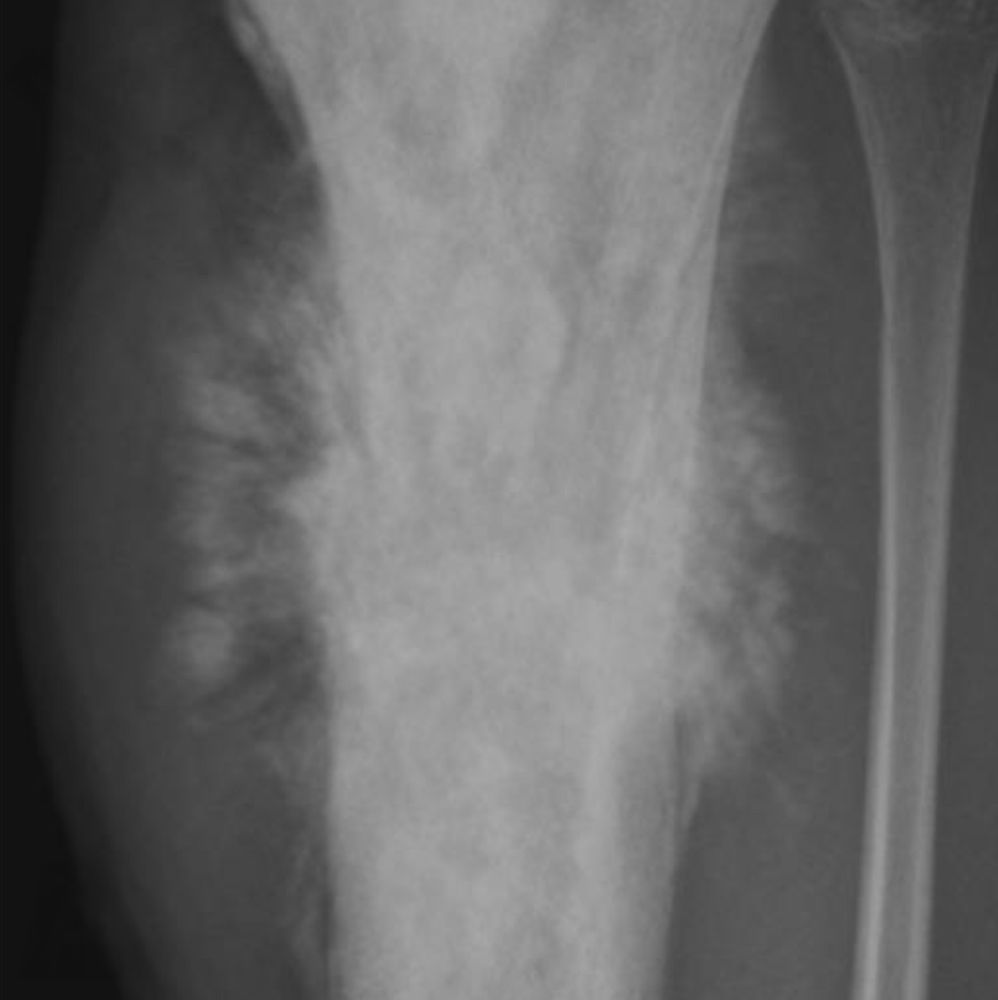
X-ray tibia (left; AP view)
A mixed density osteoblastic (sclerotic; S) and osteolytic (lucent; L) lesion that replaces most of the proximal tibia shows a permeative pattern of destruction with cortical breakthrough. The aggressive tumor is accompanied by periosteal elevation that has created a triangular area of new bone (Codman triangle; yellow overlay). Linear bony spicules radiate outward and resemble rays of the sun (sunburst pattern; examples indicated by blue lines).
A Codman triangle is seen in the setting of an aggressive bone lesion when only the edge of the raised periosteum ossifies. Sunburst periosteal reaction, another sign of aggressive periostitis, occurs when the periosteum is unable to form organized layers and Sharpey fibers are stretched.
Source: “Fig. 1A, in: Multimodal Imaging of Osteosarcoma: From First Diagnosis to Radiomics” by Cè M, Cellina M, Ueanukul T, et al, MDPI cancers, licensed under CC BY 4.0. Modifications: letter and arrow removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

X-ray knee and lower leg (lateral view) of a child with Ewing sarcoma
A lytic permeative lesion (green overlay) in the proximal tibial diaphysis has a wide zone of transition. It is accompanied by lamellated periosteal reaction that results in an onion skin appearance (red overlay).
Illustration: comparison of radiographic patterns of bone destruction
Source: “Ewing sarcoma tibia child” by Michael Richardson, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.

X-ray calcaneus (lateral view) of a 58-year-old patient with a calcaneal chondrosarcoma
A large lytic lesion (green overlay) is visible in the posterior calcaneus. The lesion contains a few small calcifications (arrowheads).
Chondrosarcomas can occur at any age, although they most commonly occur in people > 50 years of age. About half of cases are lytic on x-ray and contain calcifications.
Source: “Fig 1A, In: Delayed Reconstruction by Total Calcaneal Allograft following Calcanectomy: Is It an Option?” by Degeorge B, Dagneaux L, Forget D, Gaillard F, Canovas F, Hindawi, licensed under CC BY 4.0. Modifications: removal of the letter A in the upper left corner. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Osteosarcoma
Epidemiology
- Most common primary bone malignancy in children and adolescents [1]
-
Peak incidence [1]
- Primary osteosarcoma: 10–14 years of age
- Secondary osteosarcoma: individuals aged > 65 years
- Sex: ♂ > ♀ [6]
Etiology [1][6][10]
Osteosarcoma is a malignant, osteoid-forming bone tumor arising from mesenchymal stem cells (osteoblasts).
-
Primary osteosarcoma arises spontaneously in previously healthy bones.
- Idiopathic
-
Increased incidence in individuals with genetic cancer syndromes, e.g.:
- Hereditary retinoblastoma
- Li-Fraumeni syndrome
-
Secondary osteosarcoma arises in previously abnormal or diseased bone, e.g.:
- Paget disease of bone
- Radiation injury
- Bone infarction
Sites of involvement [1][6]
- Primary tumor: metaphyses of long bones (particularly distal femur, proximal tibia, and proximal humerus)
-
Metastases
- Hematogenous spread: lungs (most common), skeletal system
- Regional spread: along the involved bone, forming skip lesions
Primary osteosarcoma typically arises from the metaphyseal region (near the growth plate) during periods of rapid skeletal growth. [1][6]
Diagnostics [1]
See “Diagnostic approach to suspected primary malignant bone tumors.”
-
X-ray findings [11]
- Osteolytic and osteosclerotic lesions in the metaphyseal region
- Aggressive periosteal reactions: sunburst appearance, Codman triangles, hair-on-end appearance
- Laboratory findings: : ↑ ALP, ↑ LDH, ↑ ESR ,↑ CRP [12]
-
Histology findings [13]
- Pleomorphic, malignant osteoblasts that produce osteoid
- Osteosarcomas always feature woven bone matrix (in contrast to chondrosarcomas and fibrosarcomas).




Remember to wear your SOCK (Sunburst, Osteosarcoma, Codman, Knee region).
Treatment [1]
-
Localized disease
- All patients with resectable disease: surgery (wide excision or amputation)
-
High-grade disease
- Neoadjuvant and/or adjuvant chemotherapy [1]
- Adjuvant radiotherapy may be considered. [1]
- Metastatic disease: Treatment options are chemotherapy, surgery (metastasectomy and excision of the primary tumor), and/or radiotherapy.
- Surveillance: Long-term follow-up with the treating oncologist is recommended. [1]
Prognosis
- Aggressive course [1]
- Primary osteosarcoma 5-year survival rate of ∼ 60% for localized disease [5]
- Secondary osteosarcoma: poor prognosis (less responsive to treatment) [6]
X-ray of the right femorotibial joint (AP view) of a 17-year-old male patient
A sclerotic outgrowth of the bone (green overlay) surrounded by osteolytic destruction of medullary and cortical bone (red overlay) is visible on the medial metaphysis of the femur.
The periosteum over the lesion is noncontinuous (dashed line), indicating rapid growth of the bone lesion.
This appearance of a mixed osteosclerotic and osteolytic lesion in the metaphyses of long bones is characteristic of osteosarcoma.
Source: © IMPP

X-ray right knee (AP and lateral views) of a patient with osteosarcoma
An ill-defined cloud-like lesion with a wide zone of transition (green overlay) is seen in the distal femur. An aggressive type of periosteal reaction known as a Codman triangle (C) is visible medially. Additional aggressive periosteal reaction seen posteriorly has produced a sunburst pattern (S).
Source: © IMPP
X-ray tibia (left; AP view)
A mixed density osteoblastic (sclerotic; S) and osteolytic (lucent; L) lesion that replaces most of the proximal tibia shows a permeative pattern of destruction with cortical breakthrough. The aggressive tumor is accompanied by periosteal elevation that has created a triangular area of new bone (Codman triangle; yellow overlay). Linear bony spicules radiate outward and resemble rays of the sun (sunburst pattern; examples indicated by blue lines).
A Codman triangle is seen in the setting of an aggressive bone lesion when only the edge of the raised periosteum ossifies. Sunburst periosteal reaction, another sign of aggressive periostitis, occurs when the periosteum is unable to form organized layers and Sharpey fibers are stretched.
Source: “Fig. 1A, in: Multimodal Imaging of Osteosarcoma: From First Diagnosis to Radiomics” by Cè M, Cellina M, Ueanukul T, et al, MDPI cancers, licensed under CC BY 4.0. Modifications: letter and arrow removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
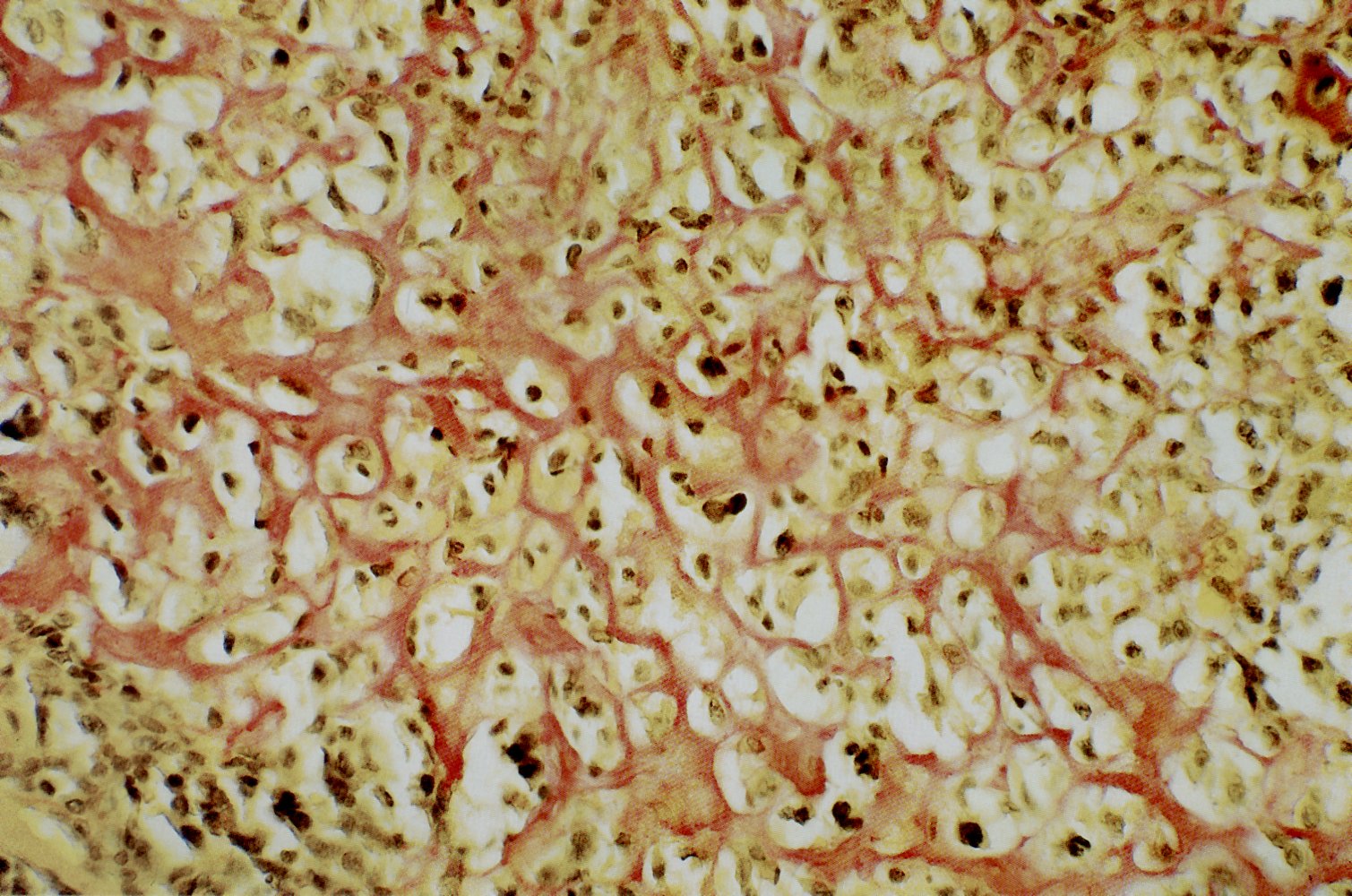
Microscopic image of the bone marrow of the lateral epicondyle of the femur (van Gieson's stain)
The atypical, polymorphic, mesenchymal cells (green overlay), which synthesize the reticular osteoid (blue overlay), are characteristic for osteosarcoma.
Source: © IMPP
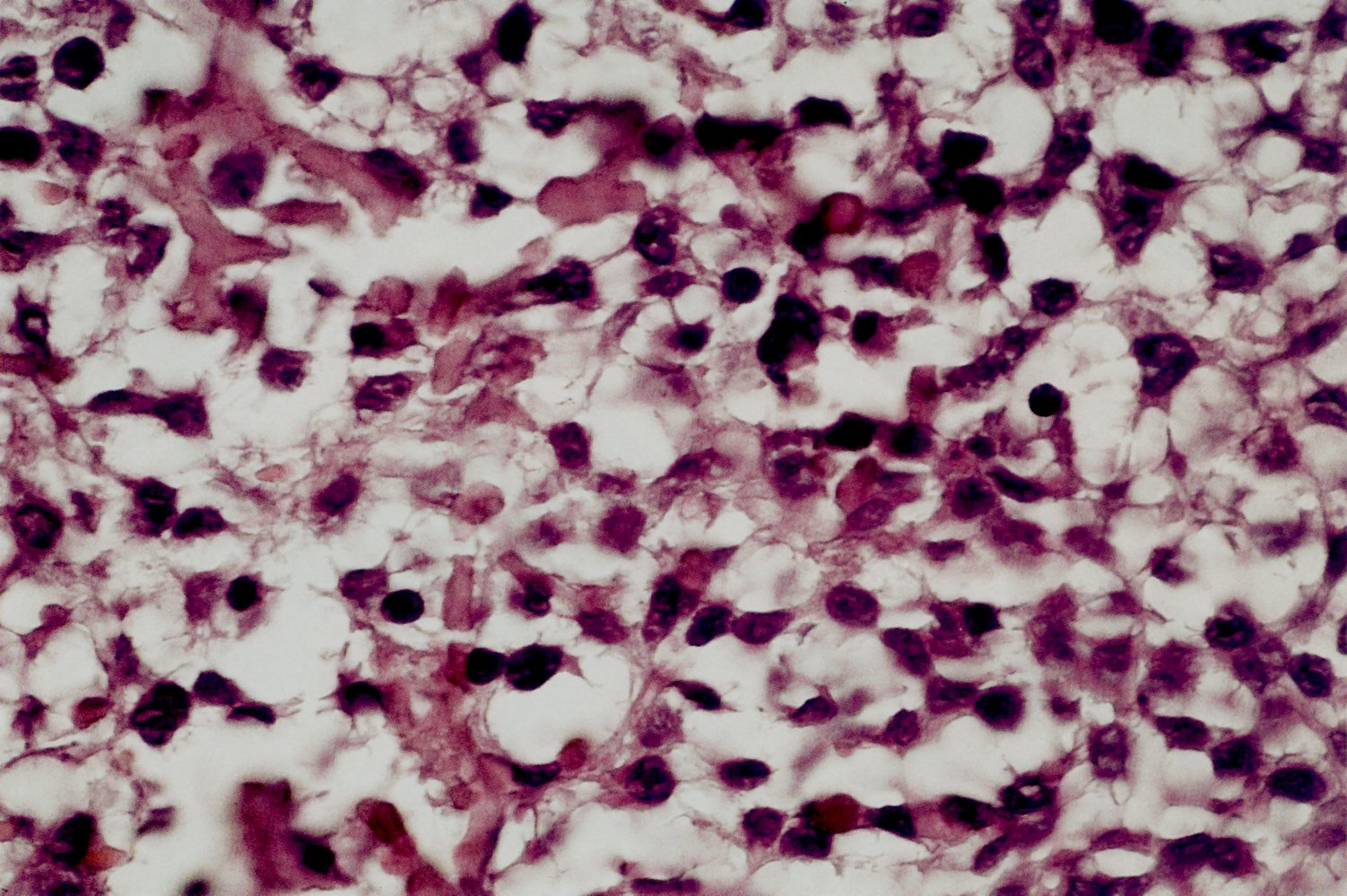
H&E stain of the bone marrow from the lateral epicondyle of the femur: atypical, polymorphic, mesenchymal cells that synthesize the osteoid. This finding is characteristic of osteosarcoma.
Source: © IMPP
Photomicrograph of a bone biopsy specimen
Abundant osteoid (appearing as eosinophilic, glassy material) forms a coarse, lacelike pattern around pleomorphic osteoblasts, which show signs of malignant transformation (i.e., multiple nuclei). Necrotic trabeculae can be seen.
Some areas of the lesion show pericellular calcification, resulting in the characteristic “chicken wire” appearance (which is characteristic of chondroblastoma).
This histopathologic appearance indicates an osteosarcoma with both osteoblastic and chondroblastic parts.
Source: © IMPP
Ewing sarcoma
Epidemiology [6][14]
- Second most common primary bone tumor in children and adolescents, after osteosarcoma
- Age: peak incidence between 10 and 20 years [14]
- Sex: ♂ > ♀
- Ethnicity: most common in White individuals
Etiology [1]
Ewing sarcoma is a highly malignant bone tumor of unclear lineage.
- May arise from neuroectodermal cells or mesenchymal stem cells [6][15]
- Associated with chromosomal fusion and translocation of the EWSR1 gene (chromosome 22) with other genes, most commonly FLI1 (chromosome 11)
Sites of involvement [1][4][6]
-
Primary tumor
- Most commonly affects diaphyses of long bones (particularly femur, tibia, fibula, and humerus), the pelvis, and bones of the chest wall
- May occur in other bones and may arise from extraosseous tissue
- Metastases: most commonly to lungs, skeletal system, and bone marrow
Diagnostics [4][6]
See “Diagnostic approach to suspected primary malignant bone tumors.”
-
X-ray findings
- Lytic bone lesions with extensive bone destruction (moth-eaten appearance) [7]
- Aggressive periosteal reaction, typically lamellated (onion skin appearance) or Codman triangles
- Laboratory findings: ↑ LDH, leukocytosis, ↑ ESR [1][16]
- Histology findings: anaplastic small blue round cell tumor; tumor cells resemble lymphocytes and differential diagnoses include lymphoma
-
Genetic and/or molecular studies (on the biopsy sample): to distinguish Ewing sarcoma from other small blue round cell tumors
- Chromosomal translocation t(11;22); (q24;q12), which leads to expression of fusion protein EWS-FLI1, is present in ∼ 85% of patients with Ewing sarcoma. [1]
- Ewing sarcoma cancer cells strongly express CD99, a cell surface gycoprotein.
Features of Ewing sarcoma (localized pain, swelling, and erythema; B symptoms; leukocytosis) can mimic those of osteomyelitis. [17]
“Ew, did you feed on 22 onions?”: Ewing sarcoma, diaphysis, femur region, chromosome 22, onion skin appearance.

Treatment [1]
-
Localized disease
- Initial treatment in all patients: neoadjuvant chemotherapy [1]
- Stable or improved disease after initial treatment: either of the following to achieve local control [1]
- Surgery (wide excision or amputation), with adjuvant chemotherapy and with or without adjuvant radiotherapy [1]
- Definitive radiotherapy with adjuvant chemotherapy
- Progressive disease after initial treatment: Palliative approaches may be required.
- Metastatic disease: Treatment options include surgery or definitive radiotherapy with adjuvant chemotherapy, or palliative approaches.
- Surveillance: Long-term follow-up with the treating oncologist is recommended. [1]
Unlike most primary malignant bone tumors, Ewing sarcoma is radiosensitive. Definitive radiotherapy is a treatment option when surgical excision is not feasible. [1]
Prognosis [1][4]
- Extremely aggressive; early metastases
- Usually responsive to chemotherapy
- 5-year survival rate of ∼ 70% for localized disease[4]
X-ray knee and lower leg (lateral view) of a child with Ewing sarcoma
A lytic permeative lesion (green overlay) in the proximal tibial diaphysis has a wide zone of transition. It is accompanied by lamellated periosteal reaction that results in an onion skin appearance (red overlay).
Illustration: comparison of radiographic patterns of bone destruction
Source: “Ewing sarcoma tibia child” by Michael Richardson, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. Alberto Perez Bouza
Chondrosarcoma
Epidemiology
- Most common primary malignant bone tumor in adults [1]
- Age: usually > 50 years [1]
- Sex: ♂ > ♀ [2][6]
Etiology [2][3]
Chondrosarcoma is a malignant bone tumor arising from chondrocytes. [6]
- Primary chondrosarcoma
- Arises in previously healthy bone
- Unknown etiology
- Secondary chondrosarcoma: malignant transformation of a benign cartilage tumor (e.g., osteochondroma, enchondroma)
Sites of involvement [2]
- Primary tumor: most commonly arises in the intramedullary cavity of long bones (particularly the proximal and distal femur and distal tibia) and pelvis
-
Metastases
- Less likely in low-grade disease; in high-grade disease, most commonly to lung and bone
- Skip lesions may be caused by regional spread.
Diagnostics [2][3]
See “Diagnostic approach to suspected primary malignant bone tumors.”
-
X-ray findings [18]
- Mixed osteolytic and osteosclerotic lesions
- Intralesional calcifications; characteristic of cartilaginous tumors (rings-and-arcs calcifications) [2]
- Endosteal scalloping
- High-grade tumors: cortical bone destruction (moth-eaten appearance) and cortical breach with infiltration of soft tissue
-
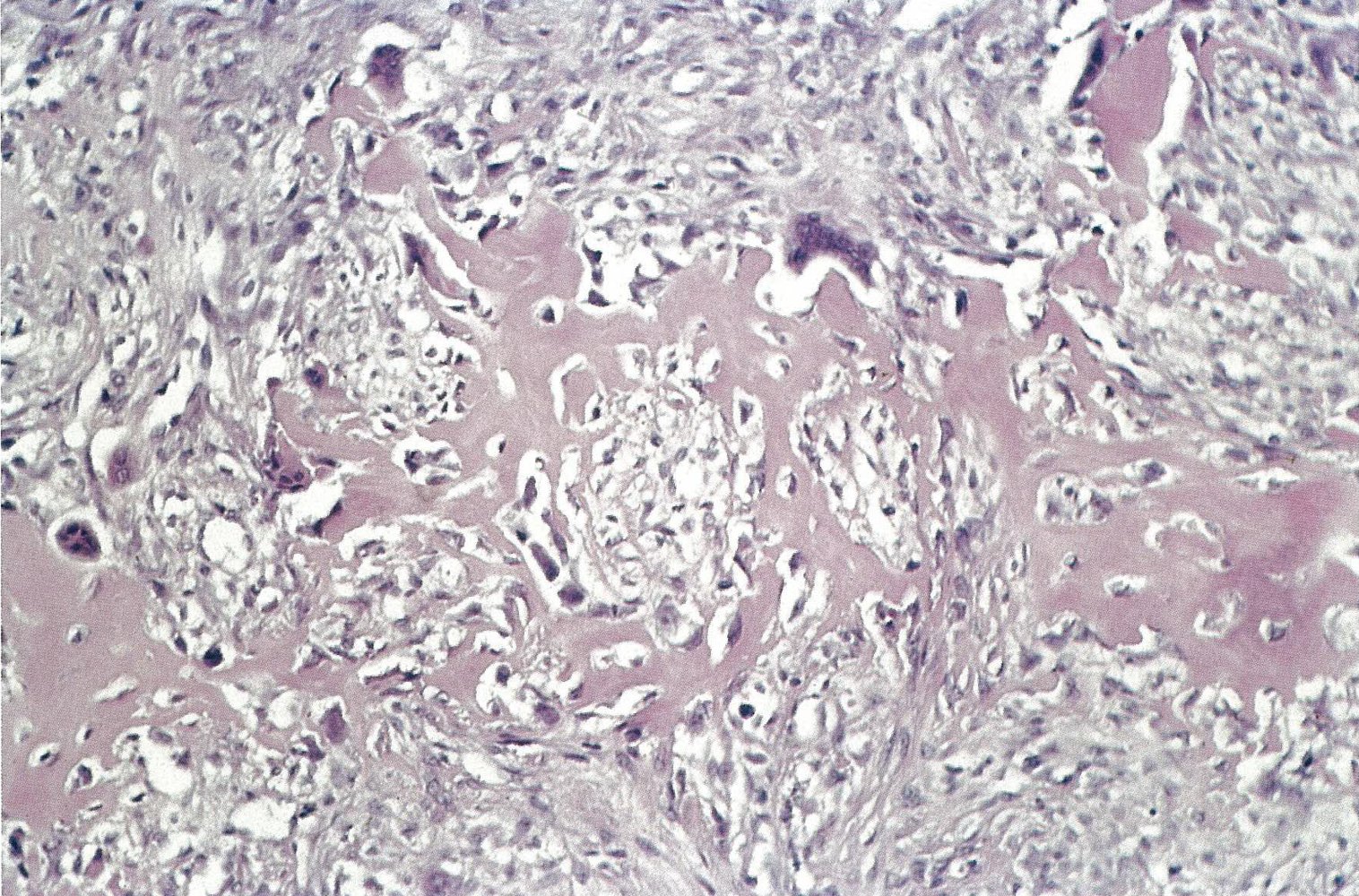
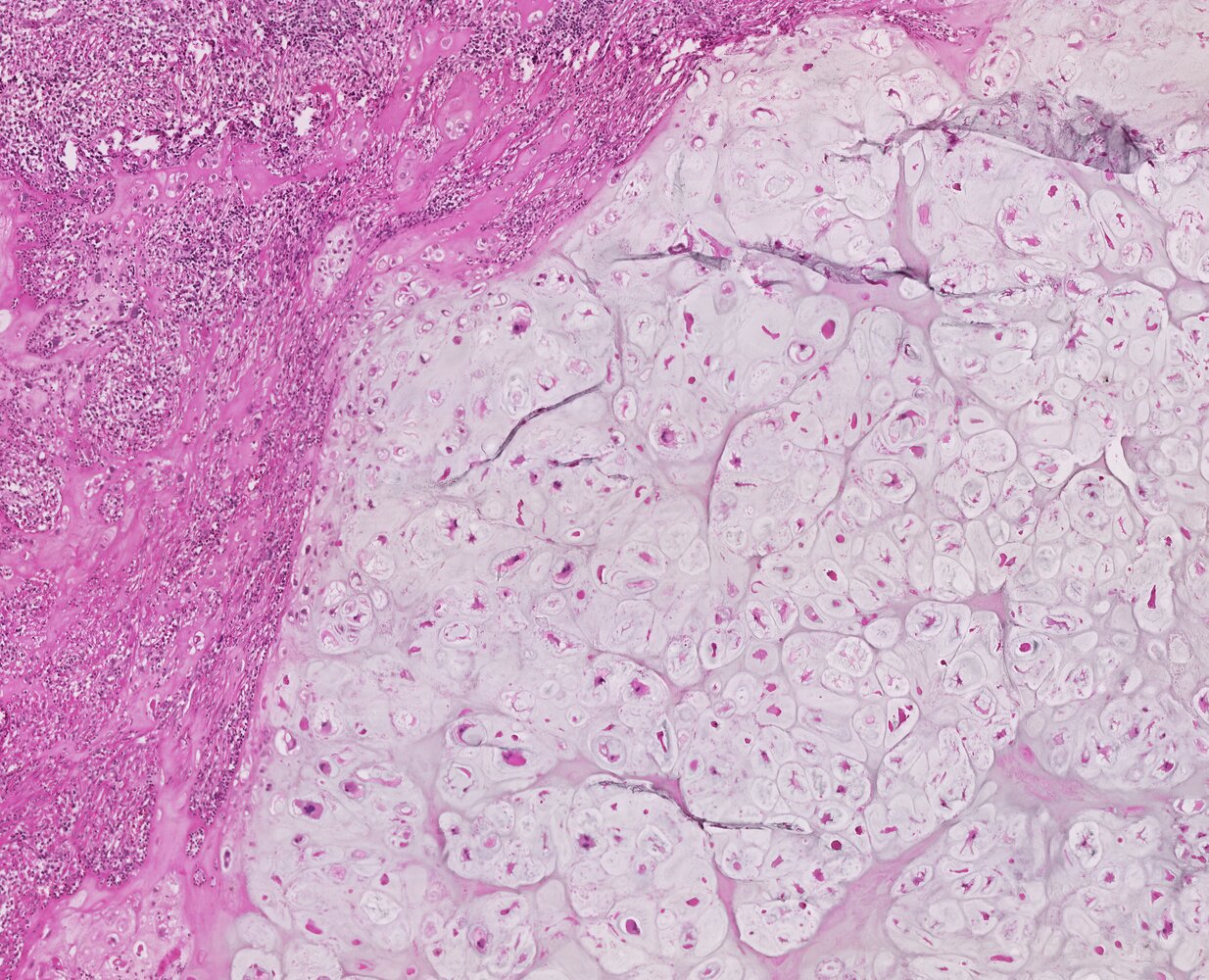
Histopathology findings [19]
- Malignant chondrocytes
- Lobulated appearance (hyaline cartilage nodules with peripheral calcification )


")



Treatment [3]
- Definitive treatment: surgery (complete resection)
- Radiation and chemotherapy
- Usually ineffective
- Can be considered as adjuvant therapy for high-grade chondrosarcomas and metastatic disease
- Radiotherapy may be used when complete surgical resection is not feasible (e.g., spine chondrosarcoma).
- Long-term surveillance with the treating physician is recommended.
Prognosis
-
5-year survival rates [2]
- Low-grade disease: 90%
- High-grade and/or metastatic disease: ∼ 30%
- Late recurrences are possible. [1]

X-ray of the pelvis (AP view)
Osteolytic zone in the left acetabulum (green overlay).
Source: © IMPP
X-ray calcaneus (lateral view) of a 58-year-old patient with a calcaneal chondrosarcoma
A large lytic lesion (green overlay) is visible in the posterior calcaneus. The lesion contains a few small calcifications (arrowheads).
Chondrosarcomas can occur at any age, although they most commonly occur in people > 50 years of age. About half of cases are lytic on x-ray and contain calcifications.
Source: “Fig 1A, In: Delayed Reconstruction by Total Calcaneal Allograft following Calcanectomy: Is It an Option?” by Degeorge B, Dagneaux L, Forget D, Gaillard F, Canovas F, Hindawi, licensed under CC BY 4.0. Modifications: removal of the letter A in the upper left corner. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
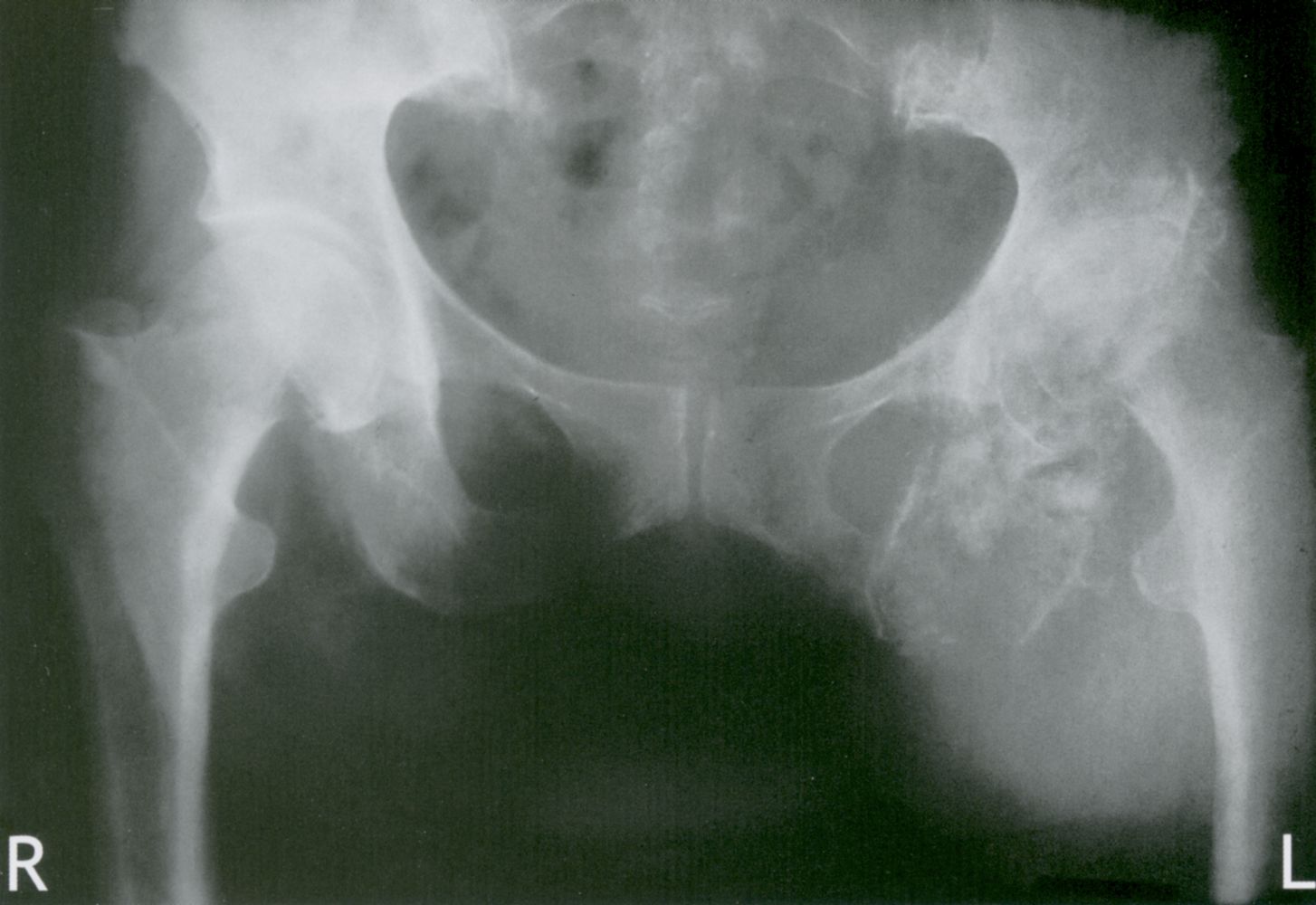
X-ray hips (AP view) of a patient with left hip pain, swelling, gait instability, and restriction of movement
A mixed lytic (example indicated by blue overlay) and sclerotic (examples indicated by yellow overlay) lesion in the left hemipelvis is accompanied by a large soft tissue component (ST). Indistinct margins and areas of cortical destruction (arrowhead) suggest an aggressive lesion.
Further evaluation confirmed the diagnosis of chondrosarcoma.
White dashed line: lesion margin
Source: © IMPP
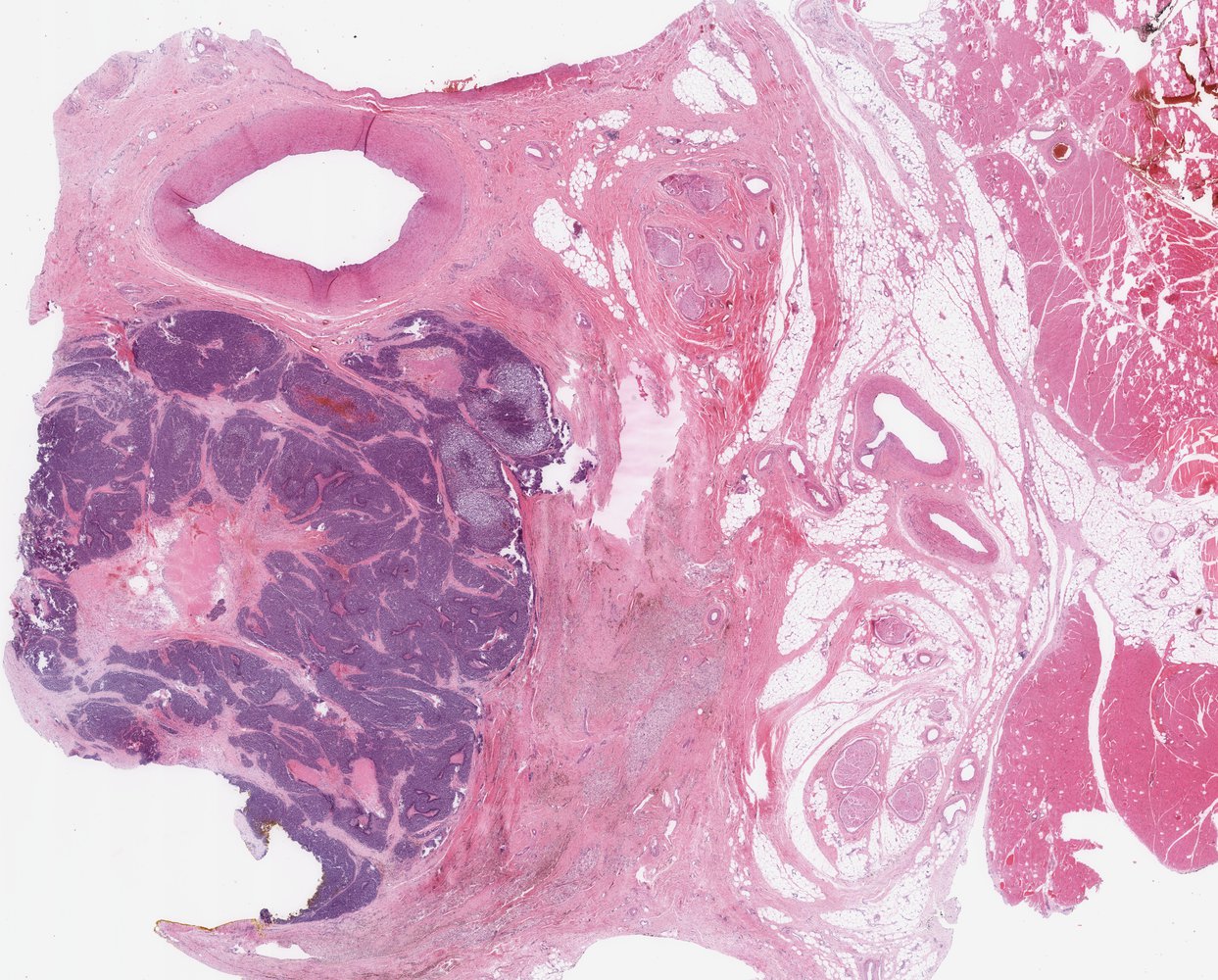
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Blue overlays: examples of calcifications; yellow outlines: examples of lobulations; arrowheads: examples of enlarged nuclei
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. Alberto Perez Bouza
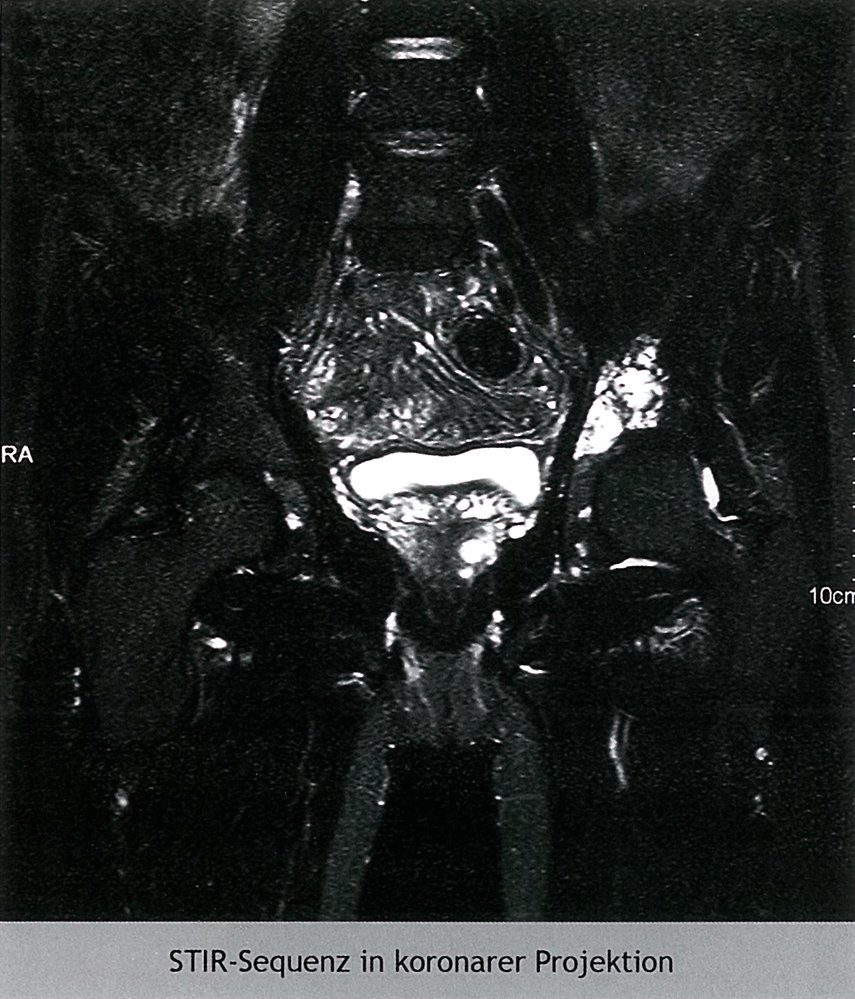
Coronal short tau inversion recovery (STIR) MRI of the pelvis
An intraosseous, hyperintense tumor (green overlay) can be seen in the left acetabular region.
Source: © IMPP
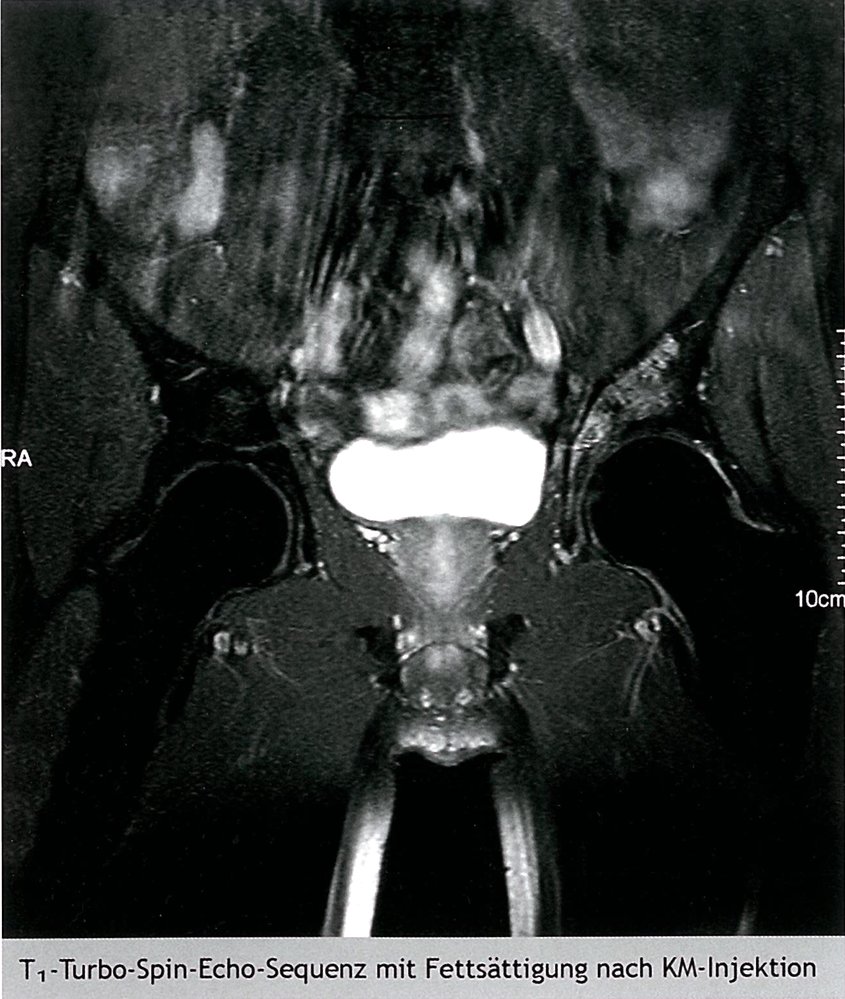
Coronal T1 weighted, fat saturated MRI of the pelvis after IV contrast agent administration: intraosseous, hyperintense tumor in the left acetabular region
Source: © IMPP
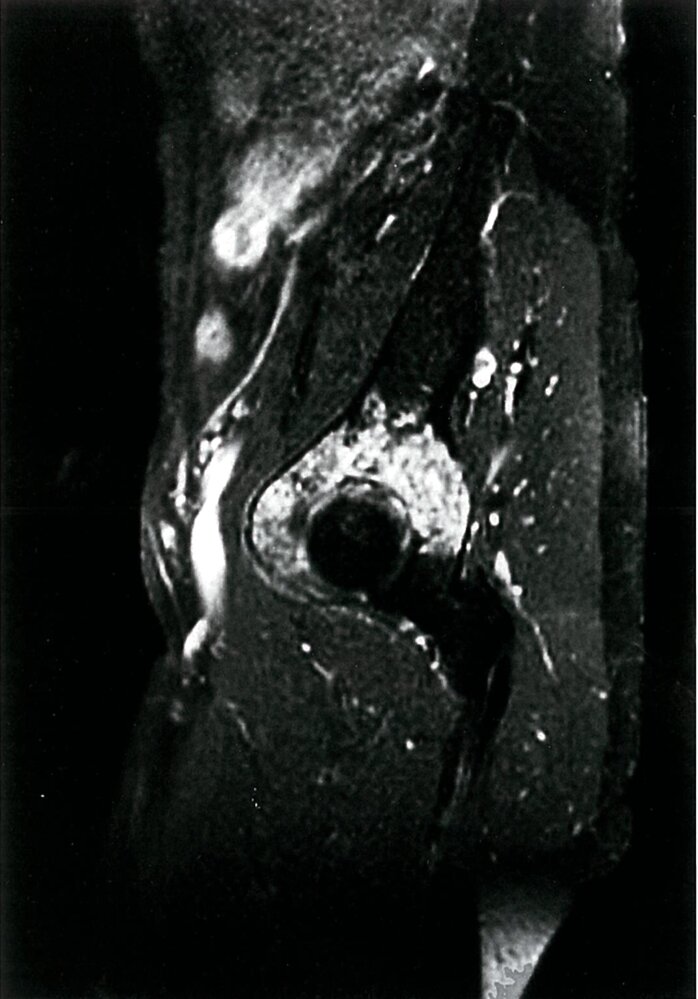
MRI hip (T1 fat saturated; sagittal view; with contrast)
There is diffuse heterogeneous enhancement of the acetabulum (green overlay).
This region of abnormal enhancement was found to be a chondrosarcoma, a malignant cartilaginous tumor. Distinguishing between benign cartilaginous tumors, such as enchondromas, and low-grade chondrosarcoma can be challenging on imaging alone, and a biopsy may be required. The chondrosarcoma in this example does not demonstrate any definitive features of malignancy apart from its large size and would be difficult to differentiate from an enchondroma on imaging alone.
Source: © IMPP
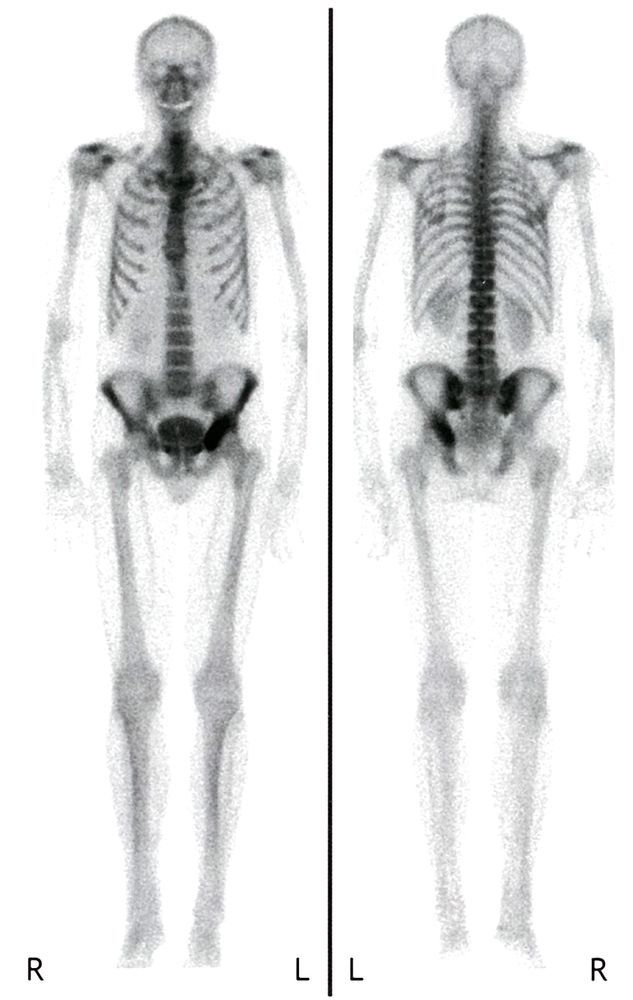
Bone scan (Tc-99m-MDP, whole body) of a patient with a history of chondrosarcoma of the pelvis
Intense uptake of radiopharmaceutical (indicated by black arrowheads) is visible in the region of the mass in the left ischium.
Chondrosarcomas frequently display intense uptake on bone scintigraphy.
Source: © IMPP
Chordoma
- Description: extremely rare malignancy of the spine and skull
- Epidemiology: typically develops in patients around 50 years
- Localization: sacral spine (∼ 50%) and skull base (∼ 35%) [20]
- Treatment: surgery
References:[21]
External Resources
References
- Biermann JS, Hirbe A, Ahlawat S, et al. "Bone Cancer, Version 2.2025, NCCN Clinical Practice Guidelines In Oncology". J Natl Compr Canc Netw. 23(4). (2025)
- Ferguson JL, Turner SP. "Bone Cancer: Diagnosis and Treatment Principles". Am Fam Physician. 98(4). :205-213. (2018)
- Laranga R, Focaccia M, Evangelista A, et al. "Bone Infarct-Associated Osteosarcoma: Epidemiologic and Survival Trends". Oncol Res Treat. 45(6). :326-335
- Nguyen JC, Baghdadi S, Pogoriler J, et al. "Pediatric Osteosarcoma: Correlation of Imaging Findings with Histopathologic Features, Treatment, and Outcome". RadioGraphics. 42(4). :1196-1213. (2022)
- Jettoo P, Tan G, Gerrand C, Rankin K. "Role of routine blood tests for predicting clinical outcomes in osteosarcoma patients". J Orthop Surg (Hong Kong). 27(2). (2019)
- Beird H, Bielack S, Flanagan A, et al. "Osteosarcoma". Nat Rev Dis Primers. 8(1). (2022)
- Meltzer P, Helman L. "New Horizons in the Treatment of Osteosarcoma". New England Journal of Medicine. 385(22). :2066-2076. (2021)
- "Ewing Sarcoma and Undifferentiated Small Round Cell Sarcomas of Bone and Soft Tissue Treatment". https://web.archive.org/web/20251030120015/https://www.cancer.gov/types/bone/hp/ewing-treatment-pdq#_70. [2024-11-27]
- Patrick P. Lin, Yongxing Wang, Guillermina Lozano. "Mesenchymal Stem Cells and the Origin of Ewing's Sarcoma". Sarcoma. 2011. :1-8. (2011)
- Riggi N, Suvà M, Stamenkovic I. "Ewing’s Sarcoma". New England Journal of Medicine. 384(2). :154-164. (2021)
- Plant J, Cannon S. "Diagnostic work up and recognition of primary bone tumours: a review". EFORT Open Rev. 1(6). :247-253. (2016)
- Bernstein M, Kovar H, Paulussen M, et al. "Ewing's Sarcoma Family of Tumors: Current Management". Oncologist. 11(5). :503-519. (2006)
- McCarville MB, Chen JY, Coleman JL, et al. "Distinguishing Osteomyelitis From Ewing Sarcoma on Radiography and MRI". AJR Am J Roentgenol. 205(3). :640-50; quiz 651. (2015)
- Gazendam A, Popovic S, Parasu N, Ghert M. "Chondrosarcoma: A Clinical Review". Journal of Clinical Medicine. 12(7). :2506. (2023)
- Weinschenk RC, Wang WL, Lewis VO. "Chondrosarcoma". J Am Acad Orthop Surg. 29(13). :553-562. (2021)
- Chaabane S, Bouaziz MC, Drissi C, Abid L, Ladeb MF. "Periosteal Chondrosarcoma". American Journal of Roentgenology. 192(1). :W1-W6. (2009)
- Murphey M, Walker E, Wilson A, et al. "From the archives of the AFIP: imaging of primary chondrosarcoma: radiologic-pathologic correlation". Radiographics. 23(5). :1245-1278. (2003)
- Tenny S, Varacallo M. "Chordoma". StatPearls. (2020)
- "Chordoma". https://rarediseases.org/rare-diseases/chordoma/
- Morancie NA, Helton MR. "Evaluating the Child With a Limp". Am Fam Physician. 107(5). :474-485. (2023)
- Expert Panel on Musculoskeletal Imaging, Ahlawat S, Lenchik L, et al. "ACR Appropriateness Criteria® Suspected Primary Bone Tumors: 2024 Update". J Am Coll Radiol. 22(5S). :S440-S454. (2025)