Summary
Prostate cancer is one of the most common cancers that affect men, especially those > 50 years of age. Typically, prostate cancer has an indolent course and is usually discovered while still localized in the prostate. This allows many patients to undergo monitoring for progression rather than active treatment, preventing unnecessary treatment-related adverse effects. Prostate cancer is typically diagnosed and monitored using prostate-specific antigen (PSA) testing, multiparametric MRI (mpMRI), and guided biopsy. Once the decision to treat has been made, therapeutic options include radical prostatectomy, radiation therapy, androgen deprivation therapy (ADT), and chemotherapy. Since all treatment options may adversely affect the patient's quality of life, shared decision-making with the patient is strongly encouraged in all current guidelines. Symptomatic management may be preferable in patients with significant comorbidities or limited life expectancy, as further treatment is unlikely to be life-prolonging.
Epidemiology
- Incidence: most common cancer in men in the US, following skin cancer (i.e., melanoma and nonmelanoma combined) [1]
- Mortality: in 2020, second leading cause of cancer deaths in men in the US (after lung cancer)
")
")
Epidemiological data refers to the US, unless otherwise specified.
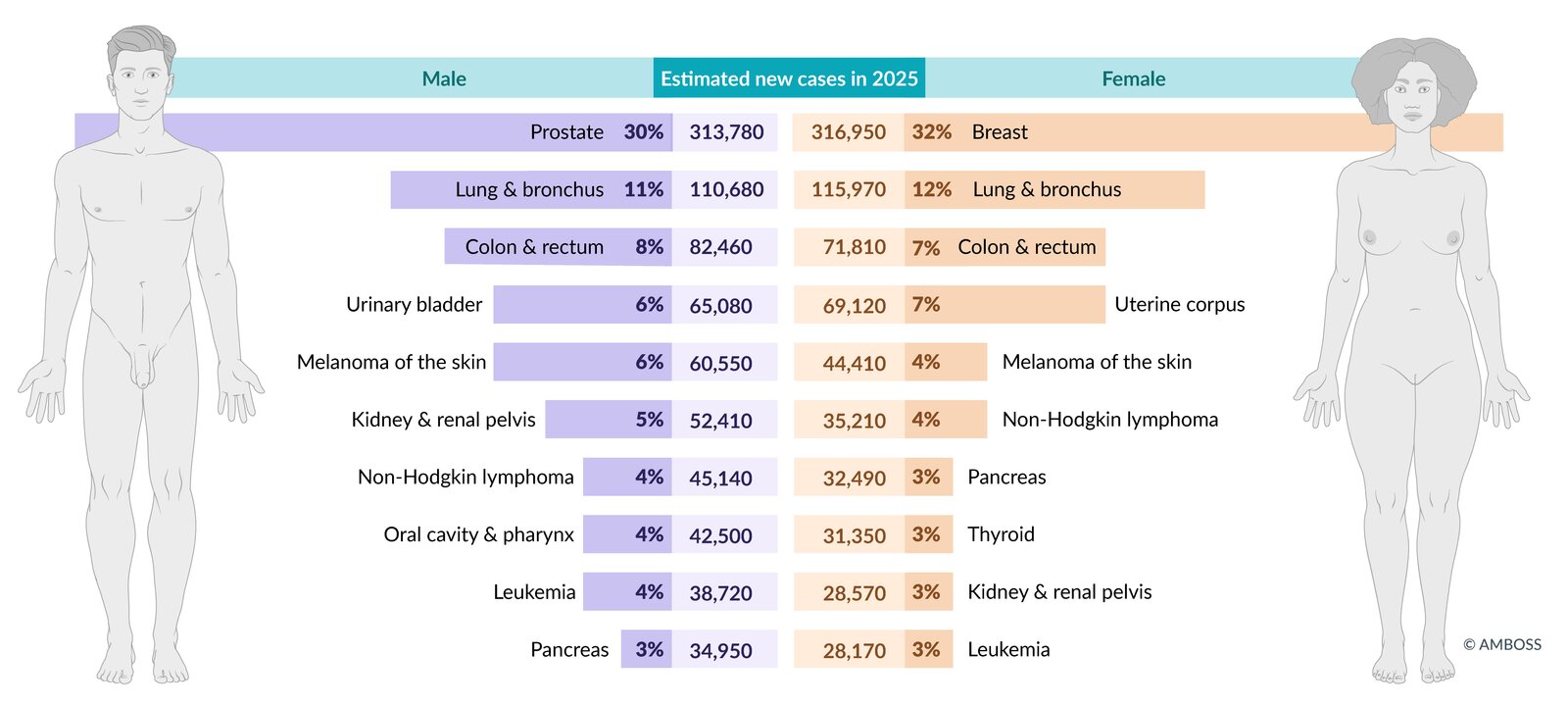
Estimated incidence of the most common cancers in the US in total figures and as a percentage of total cancer incidence (excluding non-melanoma skin cancers and in-situ carcinoma, except urinary bladder). Figures are prospective estimates of the American Cancer Society for 2025.
© AMBOSS. Data source: Cancer Facts & Figures 2024, American Cancer Society, access date 06/28/24 (https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2024/2024-cancer-facts-and-figures-acs.pdf)
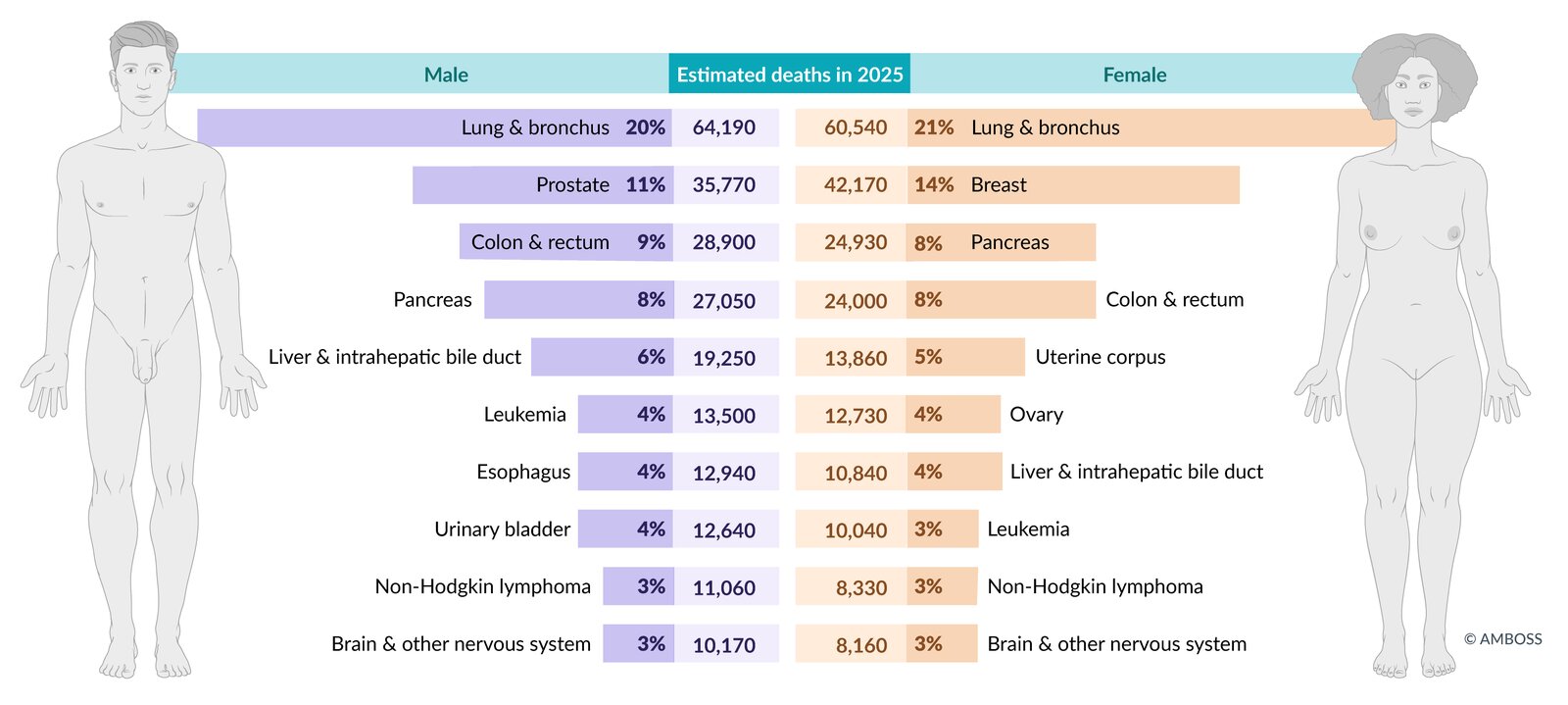
Estimated mortality from the most common cancers in the US in total figures and as a percentage of total cancer mortality. Figures are prospective estimates of the American Cancer Society for 2025.
© AMBOSS. Data source: Cancer Facts & Figures 2024, American Cancer Society, access date 06/28/24 (https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2024/2024-cancer-facts-and-figures-acs.pdf)
Risk factors
- Advanced age (> 50 years) [1][2]
- Family history
- African-American descent
- Genetic disposition (e.g., BRCA2, Lynch syndrome)
- Dietary factors: high intake of saturated fat, well-done meats, and calcium
Advanced age is the main risk factor for prostate cancer. Sexual activity and benign prostatic hyperplasia (BPH) are not associated with prostate cancer.
References: [3][4]
Clinical features
Symptoms
-
Typically asymptomatic
- Early prostate cancers are typically detected during screening tests.
- Some prostate cancers are found incidentally (incidental prostate cancer).
- Patients may present with features of complicated lower urinary tract symptoms (LUTS), including: [5]
- Urinary retention
- Hematuria
- Incontinence
- Flank pain (due to hydronephrosis)
-
Advanced prostate cancer can manifest with:
- Constitutional symptoms: fatigue, loss of appetite, clinically significant unintentional weight loss
- Features of metastatic disease; examples include:
- Bone pain (due to bone metastasis, especially in the lumbosacral spine)
- Neurological deficits (e.g., due to vertebral fracture causing spinal cord compression)
- Lymphedema (caused by obstructing metastases in the lymph nodes)
Digital rectal examination (DRE) [6][7][8]
A DRE should be performed in individuals with elevated serum PSA levels; and as part of the comprehensive evaluation of male LUTS. DRE has a low positive predictive value for detecting prostate cancer and should not be performed as the sole screening modality.
- May be normal; in early disease or if the cancer is located in areas of the gland that are not palpable on DRE [9]
-
Features suggestive of prostate cancer include:
- Localized indurated nodules on an otherwise smooth surface
- Prostatomegaly, lobar asymmetry, obliteration of the sulcus
- Hard nontender nodules
Most prostate cancers are located in the peripheral zone (posterior lobe) of the prostate. In contrast, BPH occurs in the transitional zone of the prostate.
Even patients with advanced prostate cancer may have a normal DRE; if clinical suspicion is high, continue diagnostic evaluation for prostate cancer!
")
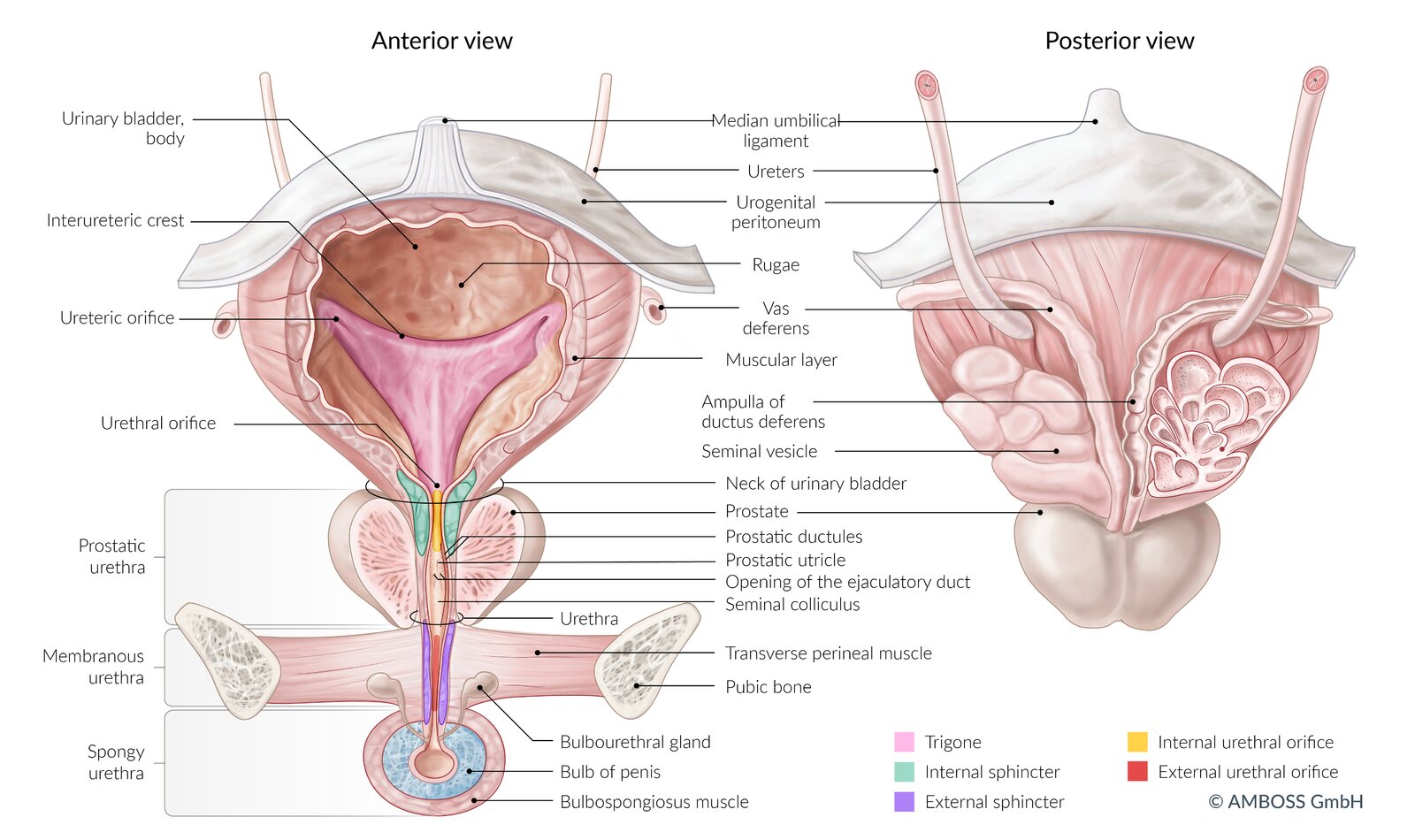
Left: ventral view of the bladder, urethra, prostate, and penis (coronal section)
Right: dorsal view of the bladder, seminal vesicles, terminal ureters, and prostate
The coronal section of the seminal vesicle and vas deferens is depicted on the right.
© AMBOSS
Diagnosis
Approach
The following content is related to diagnosing prostate cancer in symptomatic patients or those with a positive screening test. Screening for prostate cancer in asymptomatic individuals is detailed separately.
- Suspect prostate cancer in patients with elevated PSA levels detected on routine screening and/or abnormal findings on DRE.
- Consider adjunctive PSA testing (e.g., free PSA:total PSA ratio, PSA density, urinary prostate cancer antigen 3 levels) before performing a biopsy.
- Confirm the diagnosis on image-guided prostate biopsy.
- Stage prostate cancer to determine the appropriate management and prognosis.
Prostate-specific antigen (PSA) levels
PSA is a serine protease produced only in the prostate gland and, therefore, is an organ-specific marker. It is not cancer-specific however, as levels may also be elevated in benign conditions. [10]
-
Indications
- Suspected prostate cancer
- Monitoring for recurrence following treatment of prostate cancer
- Screening for prostate cancer (controversial).
-
Interpretation [11][12]
- Total PSA levels
- PSA < 2.5 ng/mL: Prostate cancer is unlikely.
- PSA 2.5–4 ng/mL: Prostate cancer is possible in symptomatic patients. [13]
-
> 4 ng/mL: Prostate cancer is likely. [12]
- PSA 4–10 ng/mL (moderately elevated PSA): ∼ 25% chance of prostate cancer
- PSA > 10 ng/mL: > 50% chance of prostate cancer
- Free PSA (unbound) : Free PSA levels are lower in prostate cancer than in normal prostate tissue or benign disease.
- Total PSA levels
- Other causes of elevated total PSA: BPH, UTI, prostatitis, prostatic trauma or manipulation (including DRE) [14]
A PSA level ≤ 4 ng/mL does not exclude prostate cancer!
5-alpha reductase inhibitors (5-ARIs) can suppress PSA production, resulting in spuriously low PSA levels. This should be taken into consideration in patients on long-term 5-ARIs (e.g., for BPH). [15][16]
Inflammation, manipulation of the prostate, and other malignant and benign prostate diseases may lead to a false-positive PSA result!
Urinalysis [17][18]
- Should be performed as part of the initial workup of LUTS and to rule out differential causes of elevated PSA
- Urinalysis is typically normal in patients with prostate cancer.
- Pyuria and/or bacteriuria in a patient with LUTS indicate a UTI or prostatitis.
Initial imaging
-
mpMRI of the prostate [19][20]
- Becoming the preferred imaging modality for suspected prostate cancer [19][21]
- Additional indications include:
- Guidance of prostate biopsy
- Clinical suspicion of prostate cancer despite negative transrectal ultrasound (TRUS) or TRUS-guided biopsy
- Initial staging of confirmed prostate cancer
- Active surveillance and follow-up
- Transrectal ultrasound of the prostate: predominantly used to guide prostate biopsy if there is clinical suspicion of prostate cancer [22][23]

Prostate biopsy
- Indication: : clinical suspicion of prostate cancer after shared decision-making with a patient whose life expectancy is ≥ 10 years [8][24]
-
Important considerations: Consider the following to minimize unnecessary biopsies. [8]
- Adjunctive PSA tests
- Free PSA:total PSA ratio of < 10–20% suggests a high probability of prostate cancer. [25]
-
PSA density [26]
- Calculated by dividing total PSA by prostate volume (as determined on imaging)
- A low PSA density (< 0.08 ng/mL/cc) suggests that clinically significant cancer is unlikely.
- mpMRI of the prostate (if not already performed)
- Presence of risk factors for prostate cancer
-
Prostate cancer antigen 3 gene (PCA3) levels in urine [27]
- The PCA3 gene is expressed more frequently in cancerous tissue than in normal prostate tissue.
- Increased PCA3 expression in a urine sample taken after DRE suggests a high probability of prostate cancer. [7]
- Adjunctive PSA tests
-
Technique
- Prophylactic antibiotics to prevent prostatitis: recommended for transrectal biopsy; consider before transperineal biopsy
- Anesthesia: local anesthesia, nerve blocks, procedural sedation, or general anesthesia
- Under image guidance (TRUS-guided or MRI-guided), several biopsy cores are obtained from the prostate via the transperineal or transrectal approach. [28][29]
-
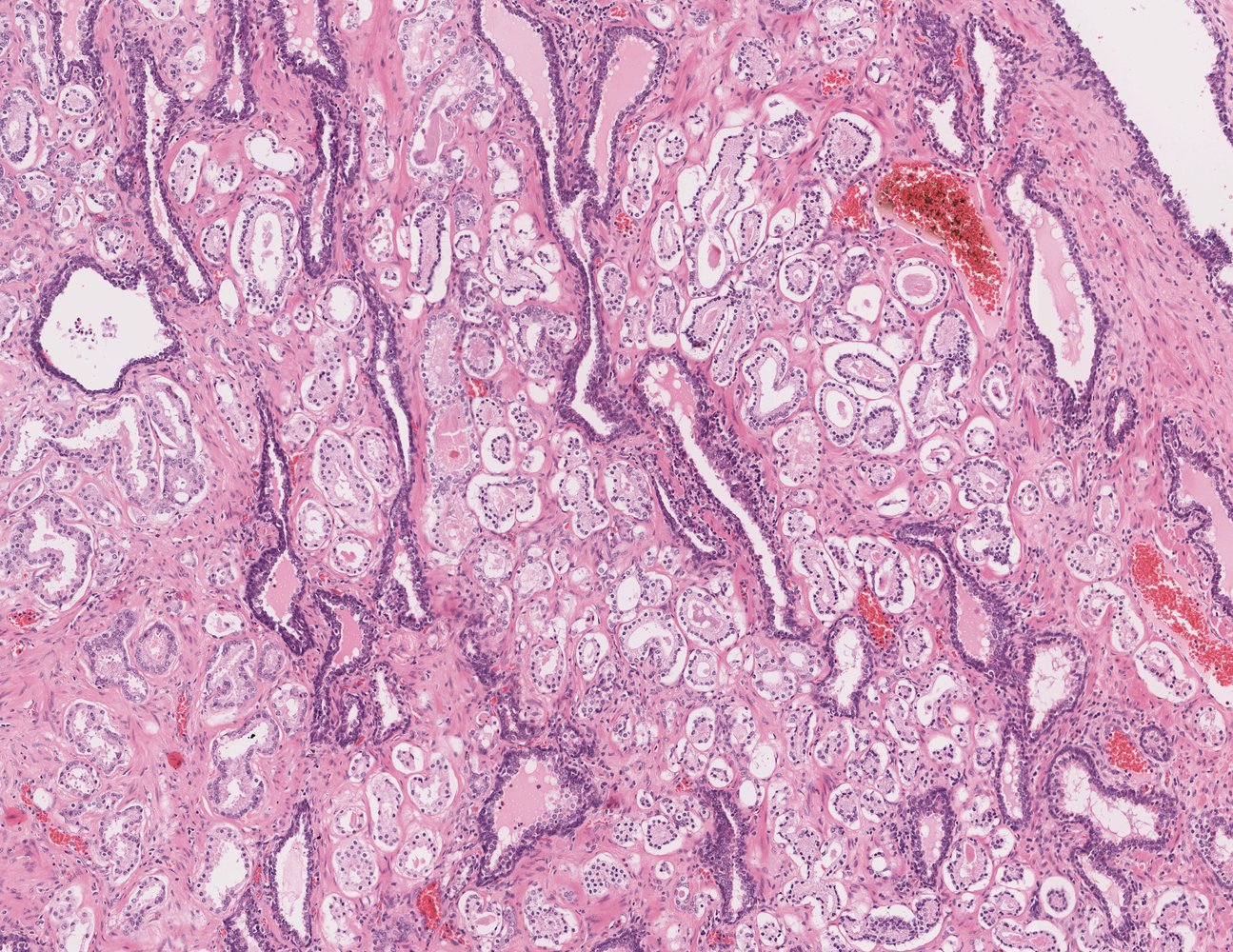
Findings: adenocarcinoma ; [30][31]
- Gleason grade (Gleason pattern): depending on the degree of differentiation of tumor cells and stromal invasion, tumors are graded from 1 (well-differentiated) to 5 (poorly differentiated)
- Gleason score (ranges from 2 to 10): the sum of the two most prevalent Gleason grades [32]
- Grade groups: prognostic categories based on the Gleason score that are used to guide management [31]

")

Gleason score and grade groups are used to grade the metastatic potential of prostate adenocarcinoma based on gland-forming differentiation.
Evaluation of tumor extent [21][22][33]
- mpMRI provides information on local tumor extent (e.g., tumor size and volume).
- Additional imaging to assess for local tumor extent and metastasis to guide management: [21]
- Recommended in patients with intermediate or high-risk prostate cancer (i.e., patients with > 10 ng/mL and an unfavorable grade group
- Not routinely recommended for patients with low or very low-risk prostate cancer (i.e., patients with PSA < 10 ng/mL, a favorable grade group, and low tumor burden in biopsy cores)
-
Cross-sectional imaging (CT, MRI, or PET-CT scan) is recommended to identify: ; [34][35]
- The spread of cancer beyond the prostatic capsule
- Pelvic and distal lymph node involvement
- Hepatic and osseous metastasis
-
Assessment of bone metastases
- Serum alkaline phosphatase may be elevated in bone metastases.
- Bone scintigraphy (technetium-99m) is the standard study for detecting bone metastases. [22]
- PET scan is more sensitive than bone scintigraphy and may become the new standard. [22][36]
- X-rays (e.g., spinal x-ray) may be appropriate to evaluate undifferentiated bone pain or if pathological fractures are suspected.
mpMRI is the preferred method for detecting local tumor extent (including recurrent prostate cancer) and PET-CT is preferred to evaluate for metastatic disease. [34][35]
Skeletal metastases are the most common nonnodal sites of metastasis in prostate cancer. Vertebral metastases commonly occur due to the spread of malignant cells through the Batson vertebral venous system. Skeletal metastases are predominantly osteoblastic but osteolytic metastases can also occur.
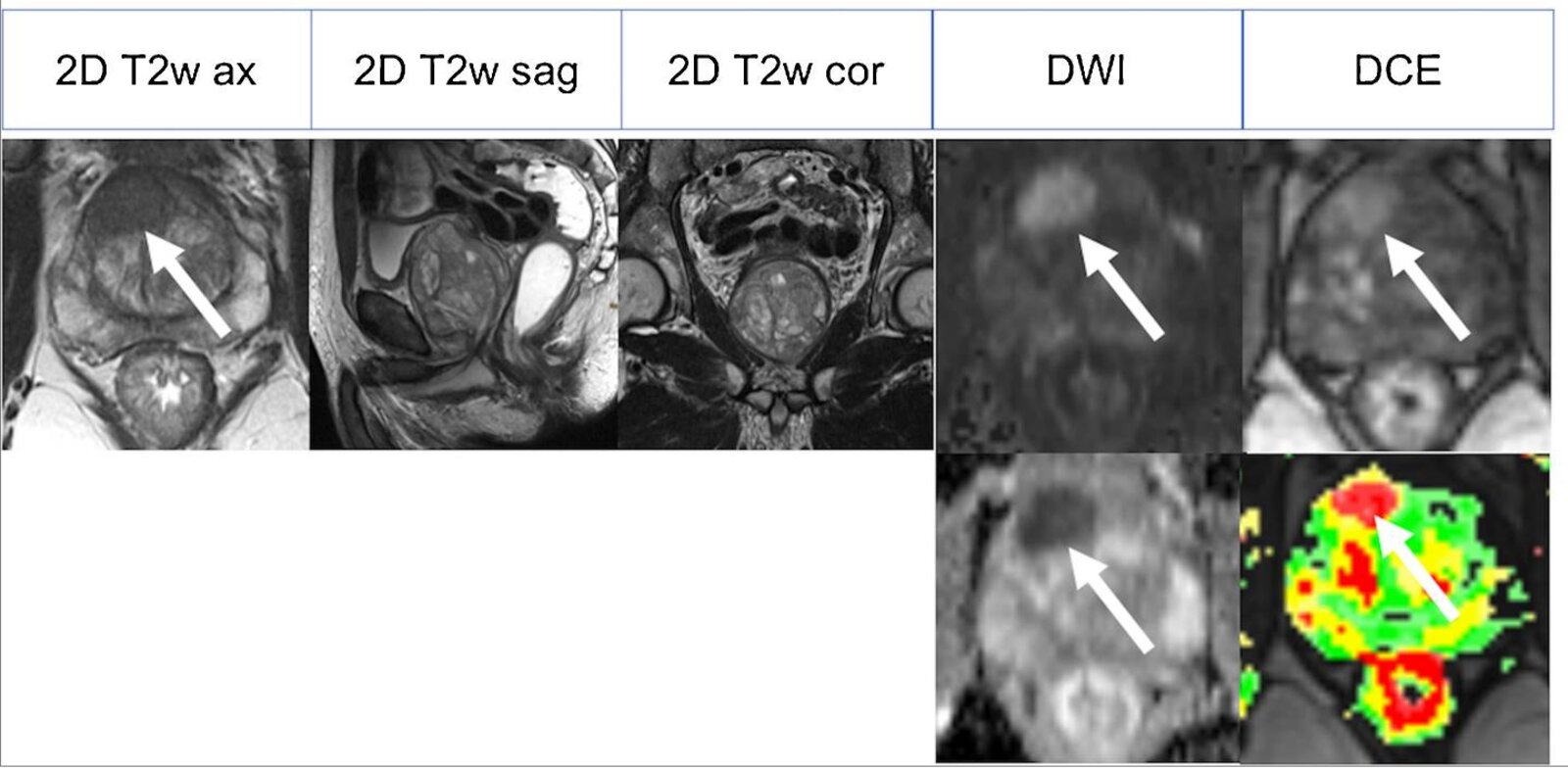
MRI prostate gland (multiparametric; T2-weighted, 3 planes; diffusion-weighted imaging (DWI), axial plane; dynamic contrast-enhanced (DCE), axial plane) of a patient with prostate carcinoma
The prostate gland (green overlay) is enlarged and elevates the bladder floor (red overlay). A hypointense lesion (arrow) is seen in the right anterior transitional zone on the axial T2-weighted sequence. It is hyperintense on DWI and hypointense to the corresponding ADC map (bottom). It shows marked contrast enhancement on the DCE images.
Source: “Fig 5, In: 3D T2-weighted imaging to shorten multiparametric prostate MRI protocols” by Polanec SH, Lazar M, Wengert GJ et al., SpringerLink, licensed under CC BY 4.0. Modifications: image cropped. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
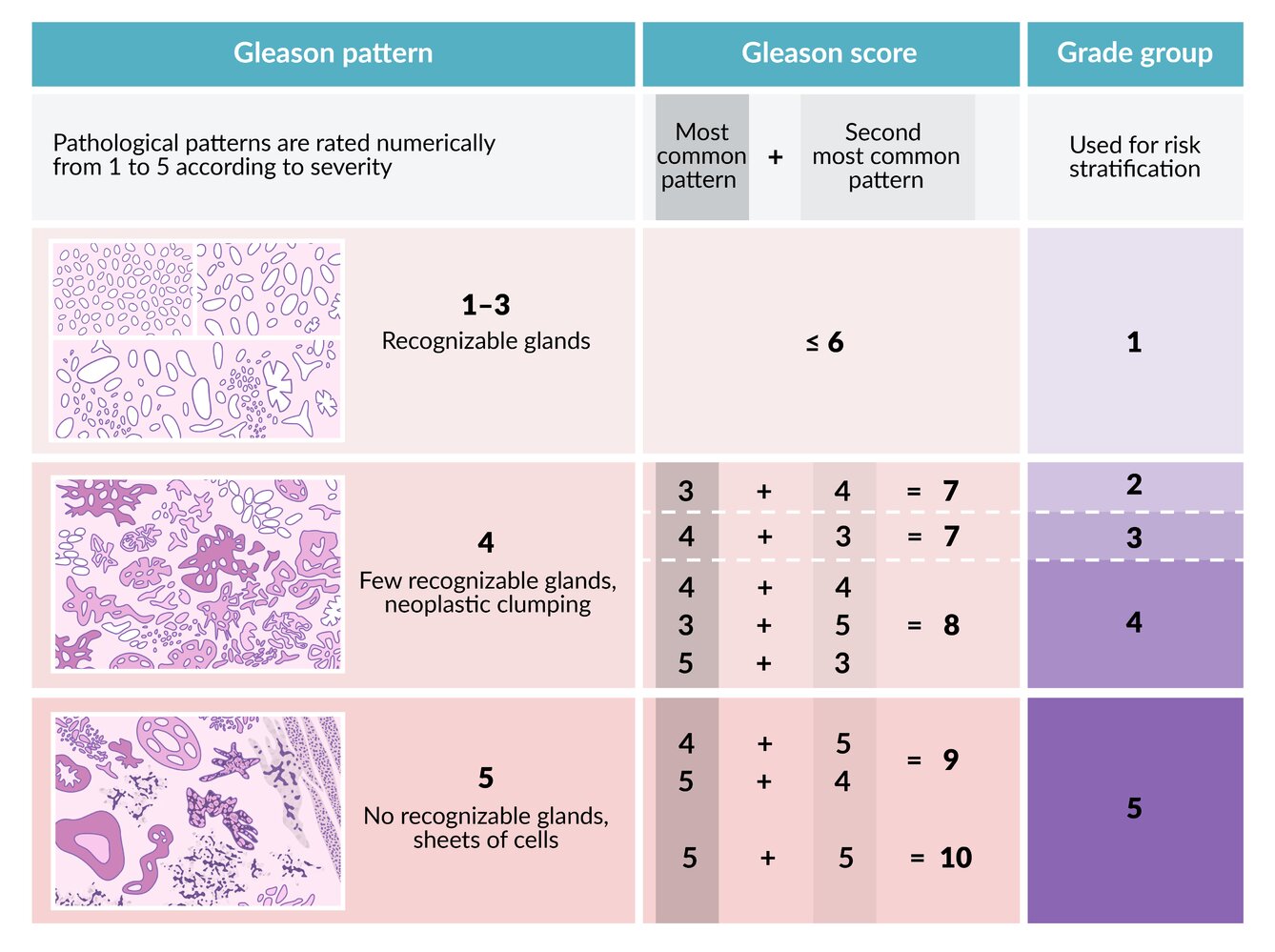
The pathological patterns of prostate CA in a biopsy sample are rated numerically according to severity. The scores of the most common and second most common patterns are added to obtain the Gleason score. This score is then used to determine the grade group, which is used for risk stratification.
© AMBOSS
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. Alberto Perez Bouza
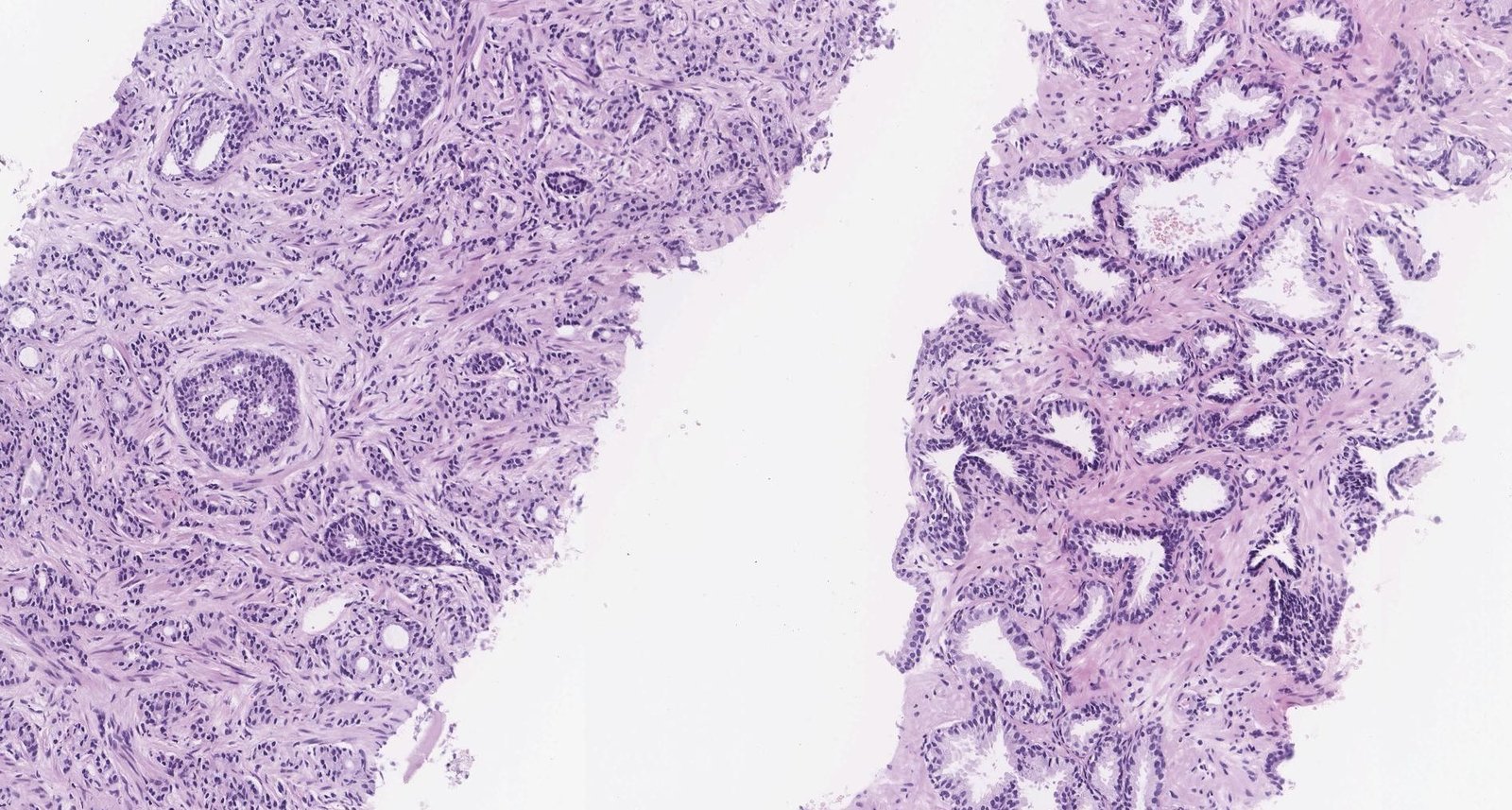
Photomicrograph of a prostate punch biopsy specimen (H&E stain; low magnification)
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. Alberto Perez Bouza

X-ray pelvis (AP view) of a patient with prostate cancer:
Numerous sclerotic metastases are seen throughout the pelvis, lumbar spine, and proximal femurs (examples indicated by green overlay). Also seen is avascular necrosis (osteonecrosis) of the right hip, with marked fragmentation of the femoral head (indicated by red overlay) and superior subluxation of the femur (asymmetry indicated by dashed lines).
Source: “Figure 1d, in: When the tumour is not the culprit: avascular necrosis of the hip in a patient with castration-resistant prostate cancer” by E. Chan, G. Chan, L. Ehrlich et al., MDPI - Current Oncology, licensed under CC BY 4.0. Modifications: Original image was made up of 4 images, Image enlarged. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Staging
The TNM staging system is based on American Joint Committee on Cancer recommendations (see “Grading and staging” in “General oncology”). Broadly, prostate cancer is divided into the following clinical stages. [21][37][38]
-
Localized prostate cancer
- Tumor confined to the prostate (T1–T2) or tumor with extracapsular extension (T3a)
- And no evidence of lymph node involvement or metastasis (i.e., N0, M0)
-
Locally advanced prostate cancer [39]
- Extension to the seminal vesicles (T3b) or adjacent periprostatic tissue (T4)
- Or regional lymph node involvement (N1) [38]
- And no evidence of distant metastases (M0)
-
Metastatic prostate cancer
- Involvement of lymph nodes outside the true pelvis (M1a)
- Or spread to nonnodal regions (M1b–c)
- Most common site: bone (M1b), especially the vertebrae
- Less common sites: lungs, liver, and adrenal glands (M1c)
Risk stratification of localized prostate cancer
All patients with confirmed prostate cancer undergo staging; patients with disease localized to the prostate additionally undergo risk stratification prior to treatment.
| Risk stratification of localized prostate cancer [21] | ||
|---|---|---|
| Risk category | Criteria | |
| Very low |
|
|
| Low |
|
|
| Intermediate |
|
|
| High |
|
|
Staging classifies prostate cancer as localized or advanced; risk category stratifies localized disease.
Management
Approach [21][33]
Management options for prostate cancer depend on the cancer stage, presence of high-risk features, and the patient's life expectancy. The impact of potential adverse effects of treatment on quality of life should be discussed with the patient prior to treatment initiation.
- Estimate the patient's life expectancy.
- Limited life expectancy (≤ 5 years): Consider watchful waiting (asymptomatic patients) or palliative ADT (symptomatic patients). [21]
- Life expectancy > 5 years: Manage according to cancer stage.
-
Stage prostate cancer to determine if it is localized, locally advanced, or metastatic.
-
Localized prostate cancer: Stratify risk based on the histological grade group and pretreatment PSA levels.
- Low or very low-risk prostate cancer: Consider active surveillance.
- Intermediate or high-risk prostate cancer: radical prostatectomy OR radiotherapy in combination with ADT
- Locally advanced prostate cancer: ADT PLUS androgen synthesis inhibitor PLUS radiation therapy
-
Metastatic prostate cancer
- Management is similar to that of locally advanced prostate cancer.
- Antiandrogens or chemotherapy can be considered instead of androgen synthesis inhibitors.
-
Localized prostate cancer: Stratify risk based on the histological grade group and pretreatment PSA levels.
- Anticipate and manage treatment-related complications (e.g., osteoporosis, pathological fractures, erectile dysfunction).
- Schedule follow-ups to assess response to therapy.
Watchful waiting [21]
-
Indications: recommended approach if all of the following apply
- Limited life expectancy (≤ 5 years)
- Slow-growing tumor (i.e., low-risk or intermediate-risk localized tumors)
- Asymptomatic or minimal symptoms
-
Method
- Regular monitoring with scheduled DRE and serum PSA levels (less intensive follow-up than active surveillance).
- Initiate definitive management according to cancer stage only when symptoms occur.
Active surveillance [21][40]
-
Indications [21]
- Very low-risk and low-risk localized prostate cancers in patients with a life expectancy > 5 years
- May be considered in favorable intermediate-risk localized prostate cancer
-
Method
- Regular monitoring with scheduled DRE, PSA, prostate biopsies, and mpMRI
- Initiate definitive management according to cancer stage if disease progression is demonstrated.
Androgen deprivation [33][41]
Androgen deprivation therapy (ADT)
- Definition: therapy designed to decrease testosterone production by the testes
-
Indications
- Locally advanced and metastatic prostate cancer: primary treatment modality
- High-risk localized prostate cancer: alternative to radical prostatectomy
-
Options
-
Medical castration: decreases pituitary stimulation of androgen production by the testes
- Gonadotropin-releasing hormone (GnRH) agonists (e.g., leuprolide)
- Gonadotropin-releasing antagonist (e.g., degarelix)
- GnRH receptor antagonist (e.g., relugolix)
- Surgical castration: bilateral orchiectomy
-
Medical castration: decreases pituitary stimulation of androgen production by the testes
-
Adverse effects
- Increased risk of osteoporosis and fractures
- Sexual dysfunction: loss of libido, erectile dysfunction
- Change in body image: gynecomastia, weight gain, decreased penile and testicular size
- Change in body composition: increased body fat, decreased muscle mass
- Increased cardiovascular and metabolic risk
- Anemia
Androgen synthesis inhibitors and androgen receptor antagonists [42]
- Indication: adjunct to ADT in locally advanced and metastatic prostate cancer
-
Androgen synthesis inhibitors
- Mechanism of action: inhibition of CYP17 gene products (including 17α-hydroxylase and 17,20-lyase) → inhibits androgen synthesis in the adrenal glands, testis, and tumor tissue
- Commonly used agent: abiraterone
-
Specific adverse effects:
- Increased production of mineralocorticoids: hypertension, hypokalemia, cardiac arrhythmias
- Inhibition of glucocorticoid production: adrenal insufficiency
- Important consideration
- Glucocorticoids should be coadministered to avoid adrenal insufficiency.
- Glucocorticoids further increase bone fragility associated with androgen deprivation and aging.
-
Androgen receptor antagonists (antiandrogen therapy)
- Mechanism of action: displaces androgens from androgen receptors
- Commonly used agents: apalutamide and enzalutamide (second-generation antiandrogens) [43]
Initiate prophylaxis against treatment-induced osteoporosis and fractures in all patients on androgen deprivation and/or glucocorticoids.
First-generation antiandrogens (flutamide and bicalutamide) are used only for the short-term management of a testosterone flare. [43]
Radiation therapy [21][44]
-
Indications
- Localized prostate cancer: primary treatment option
- Metastatic prostate cancer, high-risk localized prostate cancer, local recurrence following prostatectomy: as an adjunct to androgen deprivation
- After prostatectomy: adjuvant therapy if adverse features are detected
- Options: brachytherapy; and/or external beam radiation therapy (EBRT)
-
Complications
- Radiation proctitis, enteritis (e.g., diarrhea),
- Cystitis, urethritis, and urinary incontinence
- Erectile dysfunction [45]
- Increased risk of rectal cancer [46]
Radical prostatectomy [21]
-
Indications
- Localized prostate cancer in patients who are not candidates for active surveillance
- Following unsuccessful primary radiation therapy (salvage prostatectomy) [47]
-
Technique
- Removal of the entire prostate gland, including the prostatic capsule, the seminal vesicles, and the vas deferens [21]
- Pelvic lymph node dissection may be performed during prostatectomy.
- Important consideration: PSA levels should drop to undetectable levels after a successful prostatectomy.
- Complications: erectile dysfunction; , urinary incontinence; , infertility [45]
Radical prostatectomy involves the removal of the vas deferens, resulting in infertility.
Chemotherapy [33]
- Indication: Consider as an adjunct to ADT in patients with metastatic prostate cancer.
- Commonly used agent: docetaxel (a cytotoxic agent)
Management of bone health [48][49][50]
Prostate cancer patients are at an increased risk of skeletal features due to osteoporosis (treatment-induced and age-related) and bone metastases. [33]
Prophylaxis against treatment-induced osteoporosis and fractures
- Indications: patients on ADT, antiandrogens, and/or glucocorticoids
-
Method
- Optimize bone health (see “Treatment of osteoporosis” for details).
- Assess fracture risk
- Assess bone mineral density (e.g., DEXA scan)
- Assess of 10-year fracture risk (e.g., using tools such as FRAX®)
- Consider osteoclast inhibitors (e.g., bisphosphonates, denosumab) in patients at high risk of a skeletal-related event.
- See “Pharmacotherapy for osteoporosis” for details and dosages.
Management of skeletal events [51]
- Pain due to skeletal metastases: Consider EBRT.
- Acute skeletal pain: urgent x-rays to assess for pathological fractures
- New neurological symptoms: urgent MRI spine to identify spinal cord compression (see “Acute back pain” for details)
Patients with known vertebral metastatic disease and new neurological symptoms must have an urgent MRI to rule out spinal cord compression.
Follow-up
-
Monitor serum total PSA levels. [52]
- Every 6 months for the first 5 years, then annually for patients who have had definitive local therapy
- Every 3–6 months for patients on ADT
- Consider assessing PSA velocity (PSA doubling time); a significant rise or short doubling time suggests a recurrence. [11]
- Arrange further studies for patients with abnormal PSA values.
- After radical prostatectomy: Any measurable PSA value should prompt evaluation for recurrence.
- After radiation therapy: Any rise in PSA from nadir should prompt evaluation for recurrence. [52]
- Annual DRE: to monitor for prostate cancer recurrence and rectal cancer [46]
Screening
General principles [53]
Given the indolent nature of prostate cancer and the significant potential for treatment-related decline in quality of life, patients should be educated on the risks and benefits of participating in screening and undergoing treatment if cancer is detected. For patients with a limited life expectancy, neither screening nor treatment may be appropriate. [21][54]
-
PSA screening is controversial as it has:
- A high false-positive rate [53]
- A high detection rate of clinically insignificant cancers (leading to overdiagnosis) [53]
- Minimal or no effect on prostate cancer-related mortality. [55][56][57]
- Patient harm may occur as a result of testing and/or treatment initiated by a positive PSA screening test.
Because of the low benefit and potential risk associated with PSA screening, patients should be involved in the decision to screen for prostate cancer. [6]
Screening recommendations [54][58]
- Recommendations for screening are based on age and life expectancy and differ between the USPSTF and AUA. [54][58]
- USPSTF: Offer screening to all individuals between 55 and 69 years.
-
AUA
- Offer screening to all individuals aged 45–69 years.
- Consider initiating screening at age 40 years for individuals with risk factors for prostate cancer.
- Screening is not recommended for patients with a life expectancy < 10 years. [58]
Screening modalities [6][58]
-
PSA level remains the standard screening tool.
- The PSA threshold for referral and biopsy is based on age. [58]
- Lower thresholds are used in:
- Patients receiving a 5-ARI [59]
- Patients receiving gender-affirming hormone therapy (see “Preventive health care of transgender individuals”)
- DRE is not recommended as the sole screening tool for prostate cancer. [60]
- A screening interval of 2 years (or more) is recommended.
Prognosis
- The most important prognostic indicator for prostate cancer is the histological grade (i.e., grade group or Gleason score). [38]
- Broadly, patients with cancer confined to the prostate and pretreatment PSA levels < 10 ng/mL have a favorable prognosis. [21][61]
| Grade groups for prostate cancer [31][62] | ||
|---|---|---|
| Grade group | Gleason score [32] | 5-year survival after radical prostatectomy |
| 1 | ≤ 6 | 96% |
| 2 | 3 + 4 = 7 | 88% |
| 3 | 4 + 3 = 7 | 63% |
| 4 | 4 + 4 = 8 | 48% |
| 5 | 9 or 10 | 26% |
|
||
|
||
|
Differential diagnoses
- Benign prostatic hyperplasia
- Prostatitis
- Other tumors of the prostate
The differential diagnoses listed here are not exhaustive.
Related One-Minute Telegram
- One-Minute Telegram 136-2025-3/3: Long game, small (survival) gain after 23 years of PSA screening
- One-Minute Telegram 126-2025-1/3: A second set of AIs for prostate MRI
- One-Minute Telegram 100-2024-2/3: Less is more with low-risk prostate cancer
- One-Minute Telegram 72-2023-3/3: Aggressive therapy may not be the key to survival for localized prostate cancer
Interested in the newest medical research, distilled to just one minute? Sign up for the One-Minute Telegram in the “Tips and links” below.
External Resources
- Subscribe to the One-Minute Telegram
- 2021 AUA Advanced Prostate Cancer: AUA/ASTRO/SUO Guideline
- 2019 AUA Adjuvant and Salvage Radiotherapy After Prostatectomy: ASTRO/AUA Guideline
- 2017 AUA Clinically Localized Prostate Cancer: AUA/Astro/SUO Guideline
- US Preventive Services Task Force Recommendations (Prostate cancer)
References
- "Key Statistics for Prostate Cancer". https://www.cancer.org/cancer/prostate-cancer/about/key-statistics.html. [2017-01-05]
- Philip J, Mathew J. "Penile metastasis of prostatic adenocarcinoma: Report of two cases and review of literature". World J Surg Oncol. 1(1). :16. (2003)
- Stevermer JJ, Fink KS. "Counseling Patients About Prostate Cancer Screening". Am Fam Physician. 98(8). :478-483. (2018)
- "2018 review of the 2013 AUA guideline on the early detection of prostate cancer". https://web.archive.org/web/20210604081830/https://www.auanet.org/guidelines/guidelines/prostate-cancer-early-detection-guideline. [2018-01-01]
- Streicher J, Meyerson BL, Karivedu V, Sidana A. "A review of optimal prostate biopsy: indications and techniques". Therapeutic advances in urology. 11. :1756287219870074
- Wernert N. "The peripheral zone of the prostate is more prone to tumor development than the transitional zone: Is the ETS family the key?". Molecular Medicine Reports. (2011)
- Saini S. "PSA and beyond: alternative prostate cancer biomarkers". Cell Oncol (Dordr). 39(2). :97-106. (2016)
- Javaeed A, Ghauri SK, Ibrahim A, Doheim MF. "Prostate-specific antigen velocity in diagnosis and prognosis of prostate cancer - a systematic review". Oncology Reviews. 14(1). (2020)
- Gretzer MB, Partin AW. "PSA Levels and the Probability of Prostate Cancer on Biopsy". Eur Urol. 1(6). :21-27. (2002)
- Carter HB. "Prostate cancers in men with low PSA levels--must we find them?". N Engl J Med. 350(22). :2292-4. (2004)
- Lechevallier E, Eghazarian C, Ortega J-C, Roux F, Coulange C. "Effect of digital rectal examination on serum complexed and free prostate-specific antigen and percentage of free prostate-specific antigen". Urology. 54(5). :857-861. (1999)
- Sarkar RR, Parsons JK, Bryant AK, et al. "Association of Treatment With 5α-Reductase Inhibitors With Time to Diagnosis and Mortality in Prostate Cancer". JAMA internal medicine. 179(6). :812-819. (2019)
- Gratzke C, Bachmann A, Descazeaud A, et al. "EAU Guidelines on the Assessment of Non-neurogenic Male Lower Urinary Tract Symptoms including Benign Prostatic Obstruction". Eur Urol. 67(6). :1099-1109. (2015)
- Abdelmoteleb H, Jefferies ER, Drake MJ. "Assessment and management of male lower urinary tract symptoms (LUTS)". International Journal of Surgery. 25. :164-171. (2016)
- Coker TJ, Dierfeldt DM. "Acute bacterial prostatitis: diagnosis and management". Am Fam Physician. 93(2). :114-120. (2016)
- "Standard Operating Procedure for Multiparametric Magnetic Resonance Imaging in the Diagnosis, Staging and Management of Prostate Cancer 2019". https://www.auanet.org/guidelines/guidelines/mri-of-the-prostate-sop. [2019-09-01]
- Bjurlin MA, Carroll PR, Eggener S, et al. "Update of the Standard Operating Procedure on the Use of Multiparametric Magnetic Resonance Imaging for the Diagnosis, Staging and Management of Prostate Cancer". J Urol. 203(4). :706-712. (2020)
- "Clinically Localized Prostate Cancer: AUA/ASTRO/SUO Guideline (2017)". https://www.auanet.org/guidelines/guidelines/prostate-cancer-clinically-localized-guideline. [2017-01-01]
- Coakley FV, Oto A, Alexander LF, et al. "ACR Appropriateness Criteria ® Prostate Cancer—Pretreatment Detection, Surveillance, and Staging". Journal of the American College of Radiology. 14(5). :S245-S257. (2017)
- Harvey CJ, Pilcher J, Richenberg J, Patel U, Frauscher F. "Applications of transrectal ultrasound in prostate cancer". Br J Radiol. 85 Spec No 1. :S3-17. (2012)
- Wasson JH, Bubolz TA, Yao GL, Barry MJ. "Prostate biopsies in men with limited life expectancy". Eff Clin Pract. 5(3). :137-42
- Walz J, Haese A, Scattoni V, et al. "Percent free prostate-specific antigen (PSA) is an accurate predictor of prostate cancer risk in men with serum PSA 2.5 ng/mL and lower". Cancer. 113(10). :2695-2703. (2008)
- Aminsharifi A, Howard L, Wu Y, et al. "Prostate Specific Antigen Density as a Predictor of Clinically Significant Prostate Cancer When the Prostate Specific Antigen is in the Diagnostic Gray Zone: Defining the Optimum Cutoff Point Stratified by Race and Body Mass Index". J Urol. 200(4). :758-766. (2018)
- Ploussard G, Haese A, Van Poppel H, et al. "The prostate cancer gene 3 (PCA3) urine test in men with previous negative biopsies: does free-to-total prostate-specific antigen ratio influence the performance of the PCA3 score in predicting positive biopsies?". BJU Int. 106(8). :1143-1147. (2010)
- Chang DTS, Challacombe B, Lawrentschuk N. "Transperineal biopsy of the prostate—is this the future?". Nature Reviews Urology. 10(12). :690-702. (2013)
- Islam M, Da Silva RD, Gustafson D, et al. "A Comparison of Infectious Outcomes Between In-office Transperineal Prostate Biopsies Without Antibiotic Prophylaxis and Transrectal Prostate Biopsies". J Urol. 203(Supplement 4). (2020)
- "Prostate cancer types". https://www.cancercenter.com/cancer-types/prostate-cancer/types. [2020-11-05]
- Gordetsky J, Epstein J. "Grading of prostatic adenocarcinoma: current state and prognostic implications". Diagn Pathol. 11(1). (2016)
- "Prostatic Adenocarcinoma: Gleason Grading (Modified Grading by ISUP)". https://web.archive.org/web/20210705111204/https://www.auanet.org/education/auauniversity/education-products-and-resources/pathology-for-urologists/prostate/adenocarcinoma/prostatic-adenocarcinoma-gleason-grading-%28modified-grading-by-isup%29
- "Advanced Prostate Cancer: AUA/ASTRO/SUO Guideline". https://web.archive.org/web/20210702115211/https://www.auanet.org/guidelines/guidelines/advanced-prostate-cancer. [2021-01-01]
- Panebianco V, Barchetti F, Musio D, et al. "Advanced Imaging for the Early Diagnosis of Local Recurrence Prostate Cancer after Radical Prostatectomy". Biomed Res Int. 2014. :1-12. (2014)
- Bhargava P, Ravizzini G, Chapin BF, Kundra V. "Imaging Biochemical Recurrence After Prostatectomy: Where Are We Headed?". AJR Am J Roentgenol. 214(6). :1248-1258. (2020)
- Poulsen MH, Petersen H, Høilund-Carlsen PF, et al. "Spine metastases in prostate cancer: comparison of technetium-99m-MDP whole-body bone scintigraphy, [18F]choline positron emission tomography(PET)/computed tomography (CT) and [18F]NaF PET/CT". BJU Int. 114(6). :818-823. (2014)
- Buyyounouski MK, Choyke PL, McKenney JK, et al. "Prostate cancer - major changes in the American Joint Committee on Cancer eighth edition cancer staging manual". CA Cancer J Clin. 67(3). :245-253. (2017)
- Frendl DM, FitzGerald G, Epstein MM, et al. "Predicting the 10-year risk of death from other causes in men with localized prostate cancer using patient-reported factors: Development of a tool". PLoS ONE. 15(12). :e0240039. (2020)
- Epstein JI, Egevad L, Amin MB, et al. "The 2014 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma". Am J Surg Pathol. 40(2). :244-252. (2016)
- Fenton JJ, Weyrich MS, Durbin S, et al. "Prostate-Specific Antigen–Based Screening for Prostate Cancer". JAMA. 319(18). :1914. (2018)
- Grossman DC, Curry SJ, et al. "Screening for Prostate Cancer". JAMA. 319(18). :1901. (2018)
- Schröder FH, Hugosson J, Roobol MJ, et al. "Screening and Prostate-Cancer Mortality in a Randomized European Study". N Engl J Med. 360(13). :1320-1328. (2009)
- Martin RM, Donovan JL, Turner EL, et al. "Effect of a Low-Intensity PSA-Based Screening Intervention on Prostate Cancer Mortality". JAMA. 319(9). :883. (2018)
- Pinsky PF, Prorok PC, Yu K, et al. "Extended mortality results for prostate cancer screening in the PLCO trial with median follow-up of 15 years". Cancer. 123(4). :592-599. (2017)
- Wei JT, Barocas D, Carlsson S, et al. "Early Detection of Prostate Cancer: AUA/SUO Guideline Part I: Prostate Cancer Screening". J Urol. 210(1). :46-53. (2023)
- Etzioni RD, Howlader N, Shaw PA, et al. "Long-term effects of finasteride on prostate specific antigen levels: results from the prostate cancer prevention trial". J Urol. 174(3). :877-881. (2005)
- Halpern JA, Oromendia C, Shoag JE, et al. "Use of Digital Rectal Examination as an Adjunct to Prostate Specific Antigen in the Detection of Clinically Significant Prostate Cancer". J Urol. 199(4). :947-953. (2018)
- Skolarus TA, Wolf AMD, Erb NL, et al. "American Cancer Society prostate cancer survivorship care guidelines". CA Cancer J Clin. 64(4). :225-249. (2014)
- Baxter NN, Tepper JE, Durham SB, Rothenberger DA, Virnig BA. "Increased risk of rectal cancer after prostate radiation: A population-based study". Gastroenterology. 128(4). :819-824. (2005)
- American Joint Committee on Cancer. "AJCC Cancer Staging Manual". Springer International Publishing. (2018). ISBN: 9780996826297
- Payne H. "Management of locally advanced prostate cancer". Asian J Androl. 11(1). :81-7. (2009)
- Chen RC, Rumble RB, Loblaw DA, et al. "Active Surveillance for the Management of Localized Prostate Cancer (Cancer Care Ontario Guideline): American Society of Clinical Oncology Clinical Practice Guideline Endorsement". J Clin Oncol. 34(18). :2182-2190. (2016)
- "Initial Treatment of Prostate Cancer, by Stage". https://www.cancer.org/cancer/prostate-cancer/treating/by-stage.html. [2016-03-11]
- Sharifi N. "Androgen Deprivation Therapy for Prostate Cancer". JAMA. 294(2). :238. (2005)
- Lowrance WT, Breau RH, Chou R, et al. "Advanced Prostate Cancer: AUA/ASTRO/SUO Guideline PART I". J Urol. 205(1). :14-21. (2021)
- Pisansky TM, Thompson IM, Valicenti RK, D’Amico AV, Selvarajah S. "Adjuvant and Salvage Radiotherapy after Prostatectomy: ASTRO/AUA Guideline Amendment 2018-2019". J Urol. 202(3). :533-538. (2019)
- "National Institute for Health and Care Excellence (NICE) Guidance: Prostate cancer: diagnosis and management". https://www.nice.org.uk/guidance/ng131. [2019-05-09]
- Stephenson AJ, Eastham JA. "Role of Salvage Radical Prostatectomy for Recurrent Prostate Cancer After Radiation Therapy". J Clin Oncol. 23(32). :8198-8203. (2005)
- Lowrance WT, Breau RH, Chou R, et al. "Advanced Prostate Cancer: AUA/ASTRO/SUO Guideline PART II". J Urol. 205(1). :22-29. (2021)
- Hussain A, Tripathi A, Pieczonka C, et al. "Bone health effects of androgen-deprivation therapy and androgen receptor inhibitors in patients with nonmetastatic castration-resistant prostate cancer". Prostate Cancer Prostatic Dis. 24(2). :290-300. (2020)
- Brown JE, Handforth C, Compston JE, et al. "Guidance for the assessment and management of prostate cancer treatment-induced bone loss. A consensus position statement from an expert group". Journal of Bone Oncology. 25. :100311. (2020)
- Parker C, Castro E, Fizazi K, et al. "Prostate cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up". Ann of Oncol. 31(9). :1119-1134. (2020)
- Jahn JL, Giovannucci EL, Stampfer MJ. "The high prevalence of undiagnosed prostate cancer at autopsy: implications for epidemiology and treatment of prostate cancer in the Prostate-specific Antigen-era". International Journal of Cancer. 137(12). :2795-2802. (2015)
- Kasper DL, Fauci AS, Hauser SL, et al. "Harrison's Principles of Internal Medicine". McGraw-Hill Education. (2015). ISBN: 9780071802161
- "Prostate Cancer Risk Factors". https://www.cancer.org/cancer/prostate-cancer/causes-risks-prevention/risk-factors.html. [2020-06-09]