Summary
Psoriasis is a common chronic inflammatory skin disorder affecting individuals with an underlying genetic predisposition. Triggering events (e.g., infection, medication) can lead to disease manifestation. Psoriasis typically manifests as sharply demarcated, erythematous, scaly, pruritic plaques, most commonly occurring on the scalp, presacral region, and extensor surfaces of the knees and elbows; however, any area of the skin may be affected. Other common clinical findings include arthritis, generally affecting the fingers and lower spine, and nail involvement (e.g., pitting, discoloration). The size, location, and severity of psoriasis lesions vary depending on the subtype. The diagnosis is primarily clinical, based on the patient's symptoms, history, and the presence of any specific signs (e.g., the Auspitz sign); a biopsy is rarely indicated. Mild psoriasis can be treated with topical agents such as corticosteroids, whereas moderate to severe disease requires systemic therapy (e.g., phototherapy, biologic agents).
Epidemiology
- Prevalence: ∼ 2% of the US population [1][2][3]
-
Age of onset: : can present at any age; typically shows bimodal age distribution [1][4]
- Early onset psoriasis: (∼ 75% of cases): before 40 years of age
- Late onset psoriasis (∼ 25% of cases): after 40 years of age; usually mild
Epidemiological data refers to the US, unless otherwise specified.
Etiology
- Genetic predisposition: most likely determined via polygenic inheritance [5]
-
Trigger factors [6]
-
Infectious
- Infections of the upper respiratory tract caused by β-hemolytic streptococci
- Staphylococcal infections
- HIV
- Mechanical irritation
- Drugs; (e.g., beta-blockers, chloroquine, lithium, interferon)
-
Infectious
Pathophysiology
The mechanism causing the immune response is not yet well understood.
-
Increased proliferation of keratinocytes
- Acanthosis: thickening of the epidermis
- Parakeratosis: retention of nucleated keratinocytes in the stratum corneum
- T cells secrete cytokines, which mediate an inflammatory response.
References:[7]
Clinical features
The disease course is typically relapsing, with symptom-free intervals.
Cutaneous lesions [2]
- Well-demarcated, erythematous plaques and/or papules with silver-white scaling
- Typically, a few single lesions initially appear, often becoming confluent. [2]
- Located mainly on the scalp, trunk, elbows, and knees (extensor surfaces), but any area of the skin may be affected.
- Pruritus in ∼ 80% of cases (typically mild, but may be severe in some cases) [8]
-
Characteristic features may be present.
-
Auspitz sign ; [2]
- Small pinpoint bleeding when scales are scraped off
- Removal of the scales exposes the dermal papillae, which leads to bleeding.
- Koebner phenomenon: Physical stimuli or skin injury (e.g., trauma, scratching, irritating clothing) can lead to the appearance of psoriatic skin lesions on previously unaffected skin (isomorphic response). [2]
-
Auspitz sign ; [2]








Cutaneous variants [2]
- Plaque psoriasis: most common variant; characterized by symmetrically distributed, thick, scaly, erythematous lesions
-
Guttate psoriasis
- Lesions the size of drops of water
- May develop into plaque psoriasis
- Occurs mainly in children and adolescents after streptococcal infection
-
Erythrodermic psoriasis
- Generalized erythematous lesion with diffuse scaling
- May lead to severe illness with fever and dehydration
- Inverse psoriasis: : mainly affects skin folds and flexural creases of large joints (flexural psoriasis)
-
Pustular psoriasis
- High correlation with HLA-B27
-
Generalized pustular psoriasis (most common subtype)
- Generalized erythroderma, confluent white pustules over the entire body, involvement of the oral mucosa and tongue
- Relapsing course with pronounced malaise (fever, weakness, chills); may be fatal
Plaque psoriasis is the most common psoriasis variant (accounts for ∼ 80–90% of psoriasis cases). [2]
Erythrodermic and generalized pustular psoriasis can lead to severe, life-threatening illness, which must be treated as a medical emergency. [2]











Nail involvement [2]
Present in ∼ 50% of cases [9]
- Nail pitting: small, round depressions in the nail
- Brittle nails: nail dystrophy with crumbling of the nail
- Onycholysis: partial and mostly distal separation of the nail plate
- Oil drop sign (or salmon spot): well-circumscribed, yellow-red discoloration of the nail [9]
Clinical features vary depending on the cutaneous variant. Erythema, thickening, and scaling are present in most variants. [2]

Multiple erythematous, partially confluent plaques with silver-white scaling are visible on the extensor and flexor sides of the legs.
Source: © IMPP

Multiple round, sharply demarcated, scaly, erythematous plaques are visible on the arms and trunk.
This appearance is typical of guttate psoriasis, a subtype of psoriasis.
Source: “Figure 76, In: Atlas of Paediatric HIV Infection” by Regina E. Oladokun, Rannakoe J. Lehloenya, Carol Hlela et.al., Openbooks, licensed under CC BY-ND 4.0.
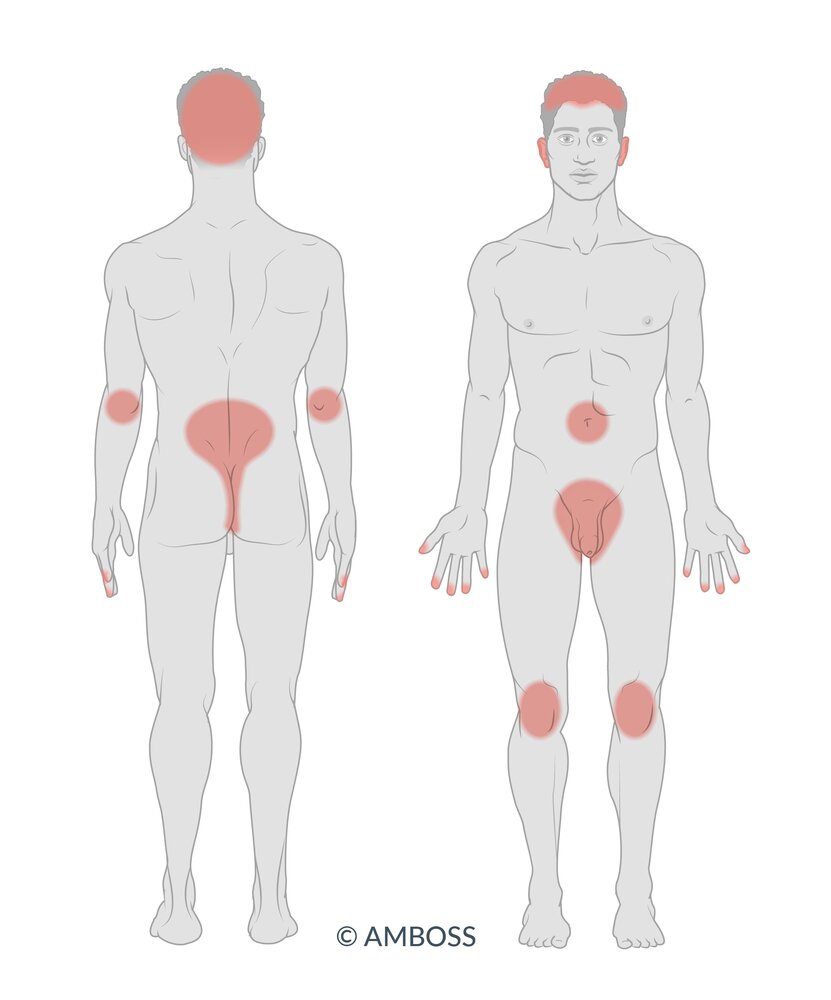
Psoriasis typically manifests on the scalp, trunk, the extensor surfaces of the elbows and knees, and near the groin and buttocks, but any area may be affected. Typical nail findings include nail pitting, onycholysis, brittle nails, and oil drop sign.
© AMBOSS

Erythrosquamous, partially confluent plaques with coarse scaling are visible along the hairline over an area of up to approx. 2 cm under the hairline.
These findings are characteristic of psoriasis capitis.
Source: © IMPP

There are several large, erythematosquamous plaques with silver-white scaling on the back and the extensor sides of the upper limbs.
These features are characteristic of plaque psoriasis.
Source: © IMPP

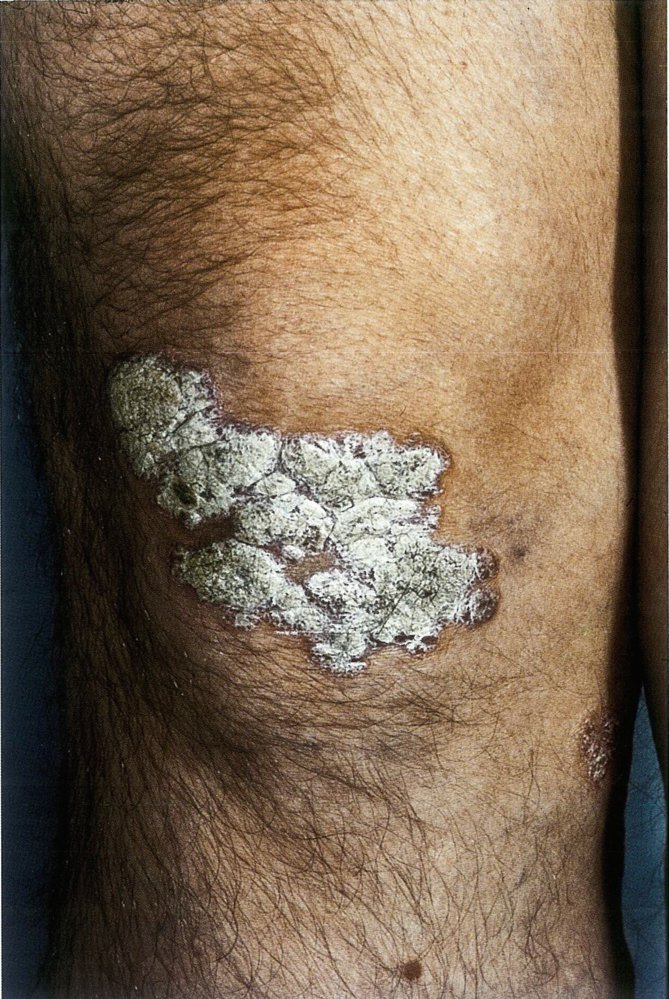
Erythematosquamous plaques with silver-white scaling and surrounding erythema are visible over the extensor surface of the knee.
Source: © IMPP

Erythematous plaques and scales are visible on the lower leg and knee. There are areas of pinpoint bleeding (Auspitz sign; indicated by arrowheads) where scales have been scraped off on the left-hand side of the lowest lesion.
These findings are consistent with psoriasis.
Source: “Psoriasis am Unterschenkel” by Medinfektion, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}

© Massachusetts Medical Society. All rights reserved. AMBOSS SE, exclusive licensee.
Multiple sharply demarcated erythematosquamous plaques with coarse, silver-white scaling are visible on the extensor sides of the lower arms and elbows.
Source: "ID#: 4053", CDC/ Richard S. Hibbets, Centers for Disease Control and Prevention (CDC) licensed under Public Domain
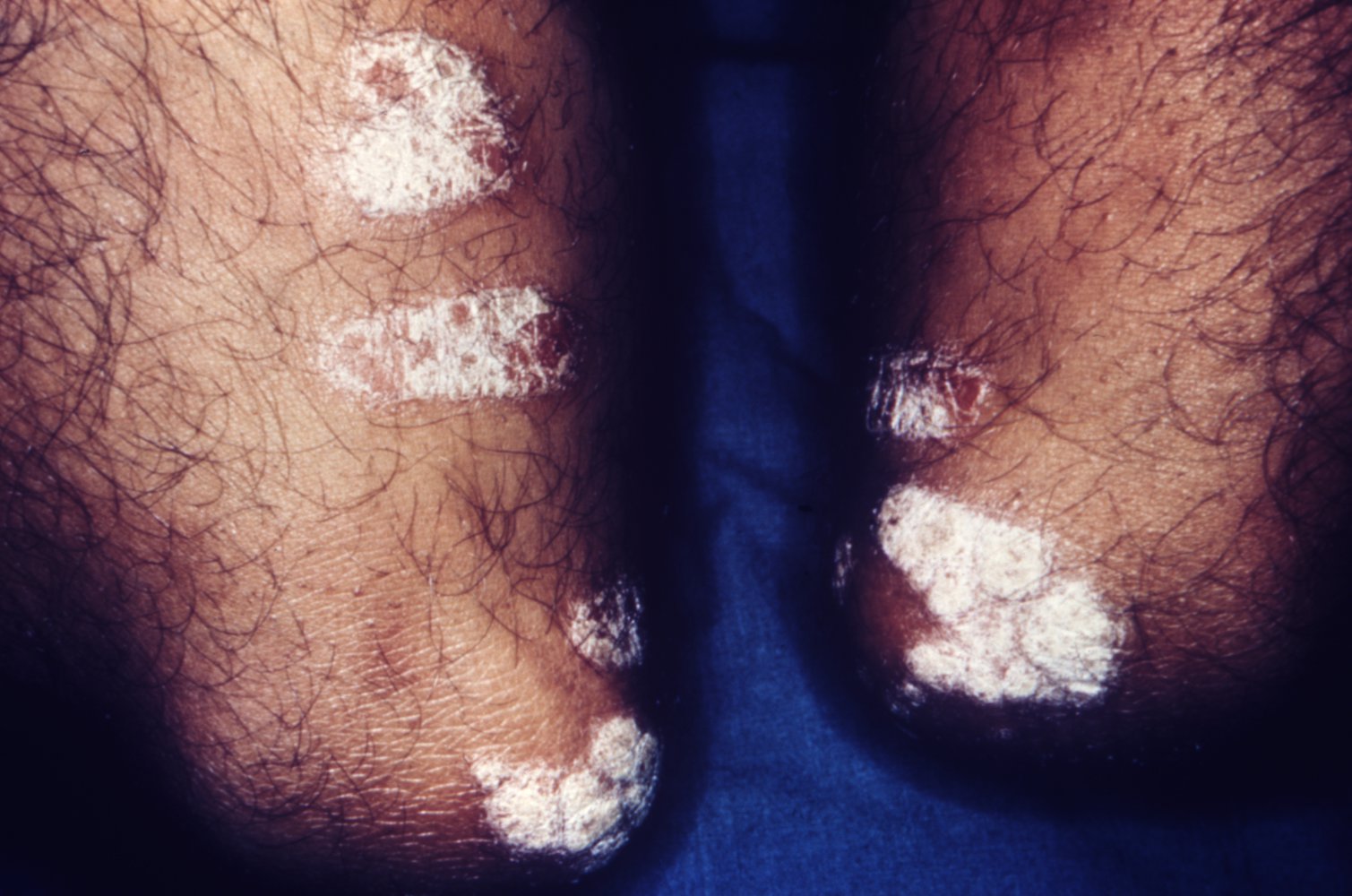
Multiple sharply demarcated confluent plaques covered with hard, coarse, silver-white scaling are visible over the extensor surface of the knee.
This is the characteristic appearance of plaque psoriasis.
Source: © IMPP

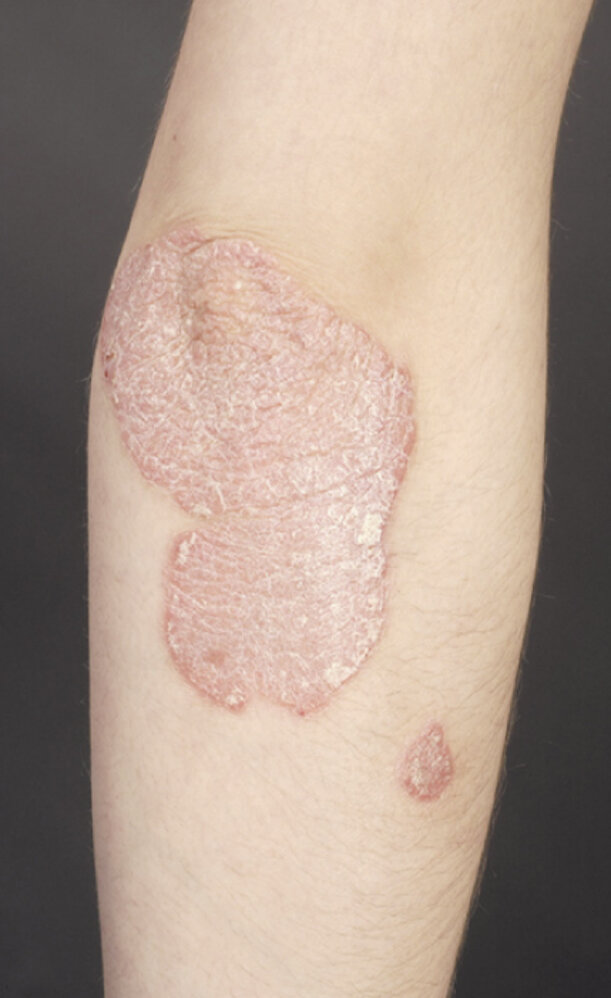
Confluent erythematous plaques with silver-white scaling are visible on the extensor surface of the upper limb.
Source: “File:Psoriasis 002.jpg” by Jacopo188, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}

Multiple small scaly erythematous lesions are visible.
This appearance is typical of guttate psoriasis and is most often precipitated by group A streptococcal infection.
Source: “Psoriasis_en_gouttes_enfant_4.jpg” by Gzzz, Wikimedia Commons, licensed under CC BY-SA 4.0.
{kind=link}

The skin over the patient's back appears erythematous, with slight superficial scaling.
This appearance suggests erythrodermic psoriasis, but other causes of erythroderma also should be ruled out.
Source: “Figure 3: Erythrodermic psoriasis.” by Karaca S, Inci R, Journal of Infectious Diseases and Therapy, licensed under CC BY 4.0.

57-year-old man with a long-standing history of psoriatic arthritis, two weeks after stopping all medications
The upper body and feet show severe erythroderma, generalized diffuse yellow scaling, and nail involvement.
These features represent a generalized exfoliative dermatitis, caused by an outbreak of erythrodermic psoriasis, which was precipitated here by medication cessation.
Source: “Fig. 1a and b, in: Erythrodermic Psoriasis Causing Uric Acid Crystal Nephropathy” by Ellis J, Lew J, Brahmbhat S, Gordon S, Denunzio T, Case Reports in Medicine (Hindawi), licensed under CC BY 4.0. Modifications: image cropped.

Erythematosquamous plaques with silver-white scaling are visible at the margin of the intergluteal cleft. Small individual plaques are distributed across the buttocks.
These findings are consistent with inverse psoriasis.
Source: "ID#: 4049", CDC/ Dr. Gavin Hart, Centers for Disease Control and Prevention (CDC) licensed under Public Domain

White pustules (red overlays with white dashed outlines) on an erythematous base (green overlays) are visible on the palm, thumb, and little finger.
Source: © IMPP
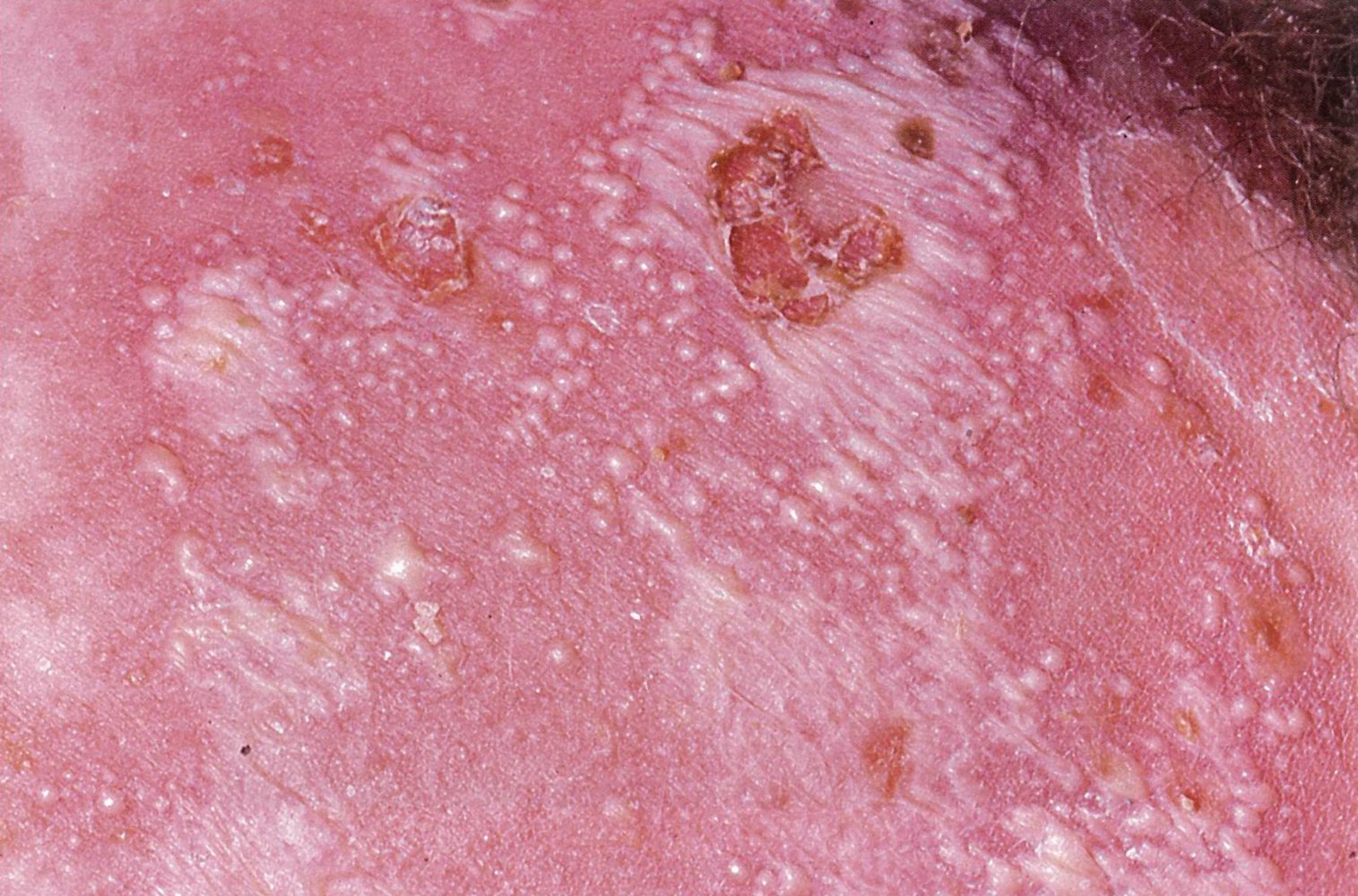
White, confluent pustules with a diameter of 2–3 mm on an erythrodermic base, some with erosion, are visible.
This appearance suggests generalized pustular psoriasis, but diagnosis should be confirmed by pathology.
Source: © IMPP
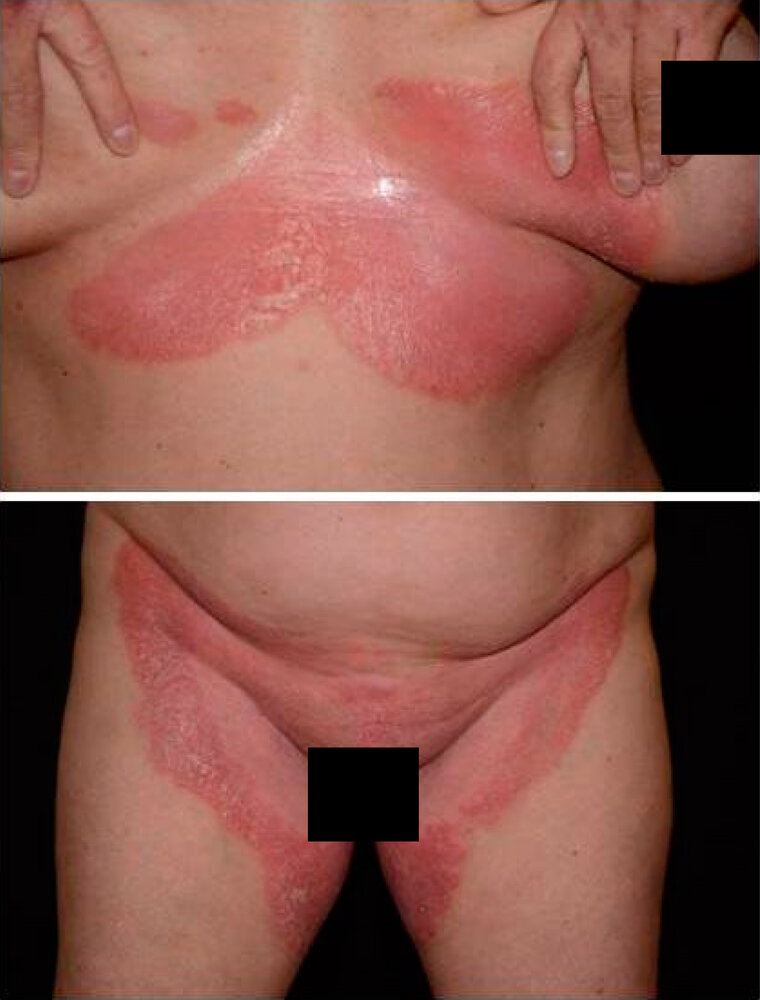
There are erythematous, well-demarcated plaques with superficial desquamation affecting intertriginous areas, specifically the inframammary region and inguinal folds. The lesions are bright red with a shiny, smooth surface and subtle scaling at the periphery.
This presentation is consistent with inverse psoriasis.
Source: “Figure 1, in: Genetic Investigation of Inverse Psoriasis” by Anikó Göblös, Emese Varga, Katalin Farkas, Kristóf Árvai und Lajos Kemény, Life 11, no. 7, licensed under CC BY 4.0. Modifications: The image has been cropped..

Multiple, small round depressions are seen in the nails.
This appearance is caused by the presence of parakeratotic cells (cells with impaired keratinization) in the nail matrix. Over time, these cells grow into the nail plate from the nail matrix, where they erupt from the horny layer, leaving small visible depressions.
Source: © IMPP

The middle finger shows numerous superficial, round depressions (nail pits; examples indicated by arrowheads) caused by deficient keratinization. Both the ring and the middle finger show distal separation of the nail plate (onycholysis; green overlay). The index finger appears mostly normal.
Nail pitting and onycholysis are typical features of psoriasis with nail involvement.
Source: Courtesy of Dr. Gary M. White, MD

Fingernails of the right hand show widespread pitting (resulting from parakeratosis within the nail plate) and onycholysis (i.e., distal separation of the nail plate).
These are common features of psoriatic nails.
© Massachusetts Medical Society. All rights reserved. AMBOSS SE, exclusive licensee.
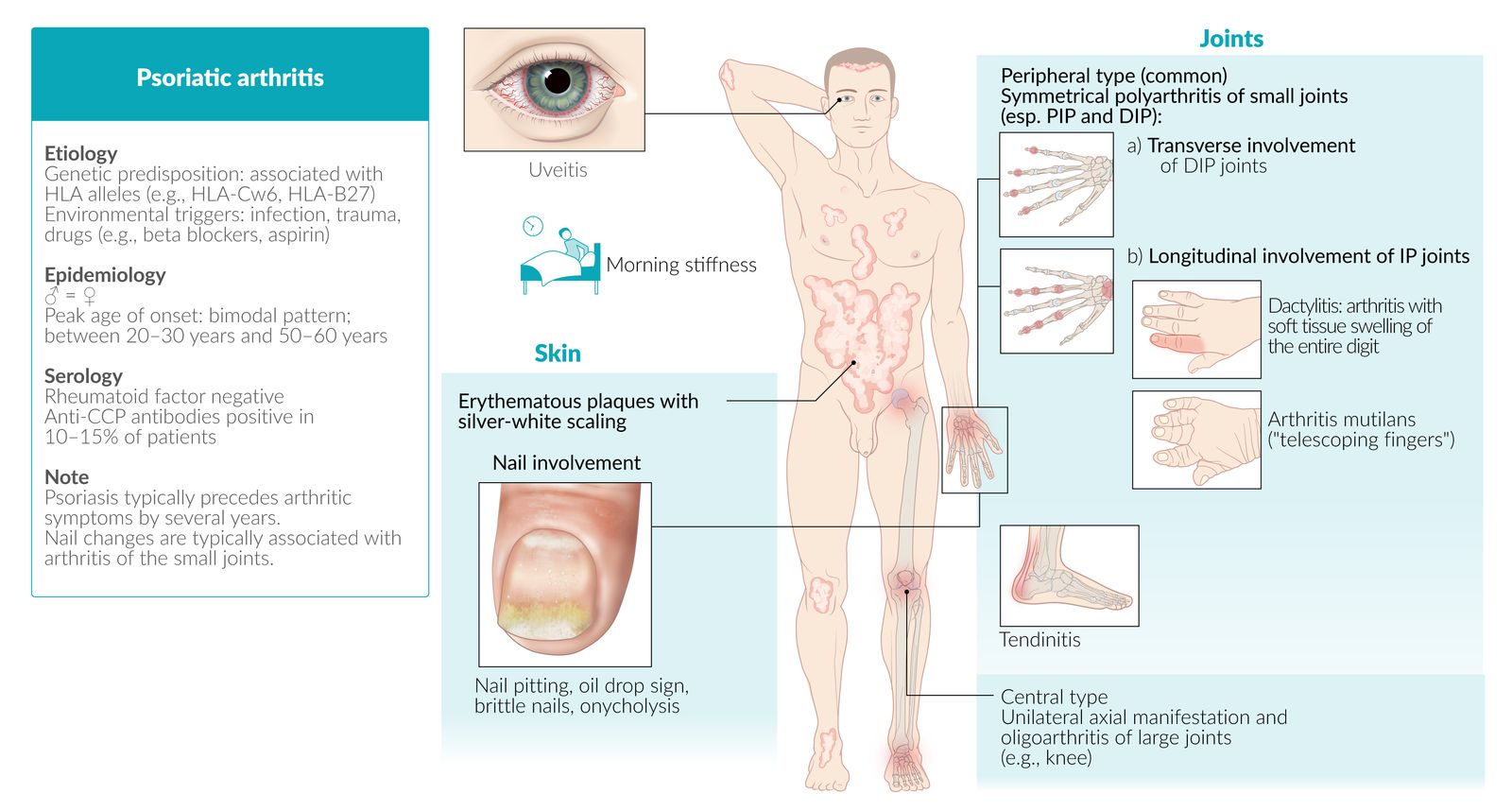
Psoriatic arthritis


Definition
Psoriatic arthritis (PsA) is a type of inflammatory arthritis that primarily affects the hands, feet, and/or spine and occurs in up to 30% of patients with psoriasis. [10]
Psoriasis and PsA can occur together or alone
Clinical features [10][11]
Arthritis [10][11]
Multiple patterns may be present.
- Oligoarthritis; (typically asymmetric; ≤ 4 joints affected)
- Polyarthritis (symmetric; similar appearance to rheumatoid arthritis)
- Involvement of distal and proximal interphalangeal joints (DIP and PIP); often occurs in conjunction with other subtypes [10]
- Arthritis mutilans: destruction of interphalangeal joints through bone resorption, resulting in the collapse of the soft tissue of the affected area (e.g., telescoping fingers or “opera glass hand”)
- Axial involvement (spine and sacroiliac joints); often occurs in conjunction with other subtypes


")




Accompanying features [10]
- Enthesitis, e.g., of the calcaneal tendon or the plantar fascia [10]
- Dactylitis: inflammation and swelling of the fingers and/or toes (“sausage digits”) [10]
- Tenosynovitis
- Nail involvement (e.g., pitting, onycholysis) [2][10]
- Uveitis [10]
In PsA, patterns of joint involvement can change over time and vary widely between patients. Oligoarthritis tends to be more common at onset, while polyarthritis may develop in later stages. [10]


Diagnostics [10][11]
General principles
- Diagnosis is mainly clinical, based on patient and family history and clinical features.
- lmaging studies can support the diagnosis and help estimate severity.
- Laboratory studies are usually obtained as a part of the inflammatory arthritis workup.
- Consult rheumatology for all patients.
Imaging studies [10][11]
-
X-ray of the affected area (e.g., hands, spine)
- Supportive findings include:
- Fingers: pencil-in-cup deformity of DIP joints
- Spine: syndesmophytes, asymmetric paravertebral ossification, unilateral sacroiliitis
- May appear normal in early disease, especially in patients with axial involvement
- Supportive findings include:
-
Further studies
- Doppler ultrasound: may show early erosions, synovitis, and enthesophytes
- MRI: may show focal erosions, synovitis, and/or bone marrow edema




Laboratory studies [10]
Laboratory studies may be obtained to rule out other diagnoses but are not typically required to make a diagnosis of PsA.
- Inflammatory markers: ↑ ESR, ↑ CRP [10]
- BMP: ↑ uric acid
-
Serology
- HLA-B27: present in ∼ 25% of patients [10]
- ACPA and rheumatoid factor: negative in ∼ 95% of patients [10]
Rheumatoid factor is typically negative in patients with PsA, which can help rule out differential diagnoses of inflammatory arthritis. [10]
Classification criteria
These classification criteria are not diagnostic but can provide guidance in clinical practice. [10]
| Classification criteria for psoriatic arthritis (CASPAR) [10][12] | ||
|---|---|---|
| Criteria | Score | |
| Clinical features |
|
2 |
|
1 | |
|
1 | |
|
1 | |
| Diagnostic studies |
|
1 |
|
1 | |
| Interpretation A total score of ≥ 3 points indicates PsA. | ||
Management of psoriatic arthritis [11][13]
General principles
- Treatment depends on disease severity and the presence of certain features and/or comorbidities.
- A treat-to-target approach with a target of remission or low disease activity is recommended. [13]
- Consult a rheumatologist before starting pharmacotherapy.
Pharmacological treatment [11][13]
-
Disease-modifying antirheumatic drugs (DMARDs): mainstay of treatment for most patients with PsA.
- Conventional DMARDs, e.g., methotrexate, sulfasalazine, leflunomide
- Targeted synthetic DMARDs, e.g., apremilast, tofacitinib
-
Biologic DMARDs, e.g.:
- TNF-α inhibitors (first line), e.g., etanercept, adalimumab, infliximab
- IL-17 inhibitors, e.g., secukinumab, ixekizumab
- IL-12/23 inhibitors, e.g., ustekinumab
- Abatacept
-
NSAIDs, e.g., naproxen, indomethacin:
- May be trialed as initial treatment in patients with very mild disease (limited evidence of efficacy)
- Preferred over DMARDs in certain patients, e.g., those with axial disease or predominant enthesitis [11]
- Can also be prescribed for symptomatic relief
- Intraarticular glucocorticoids: used for symptomatic relief
Systemic glucocorticoids are not commonly used in PsA because of concerns that tapering too rapidly may induce a flare of cutaneous disease. [11]
Supportive management [13]
- Encourage lifestyle modifications.
- Smoking cessation
- Low-impact physical activity
- Maintaining a healthy weight
- Recommend physical therapy and occupational therapy.
© AMBOSS

© AMBOSS
The distal and proximal interphalangeal joints of the finger or the entire finger (sausage digit) are especially affected.
© AMBOSS
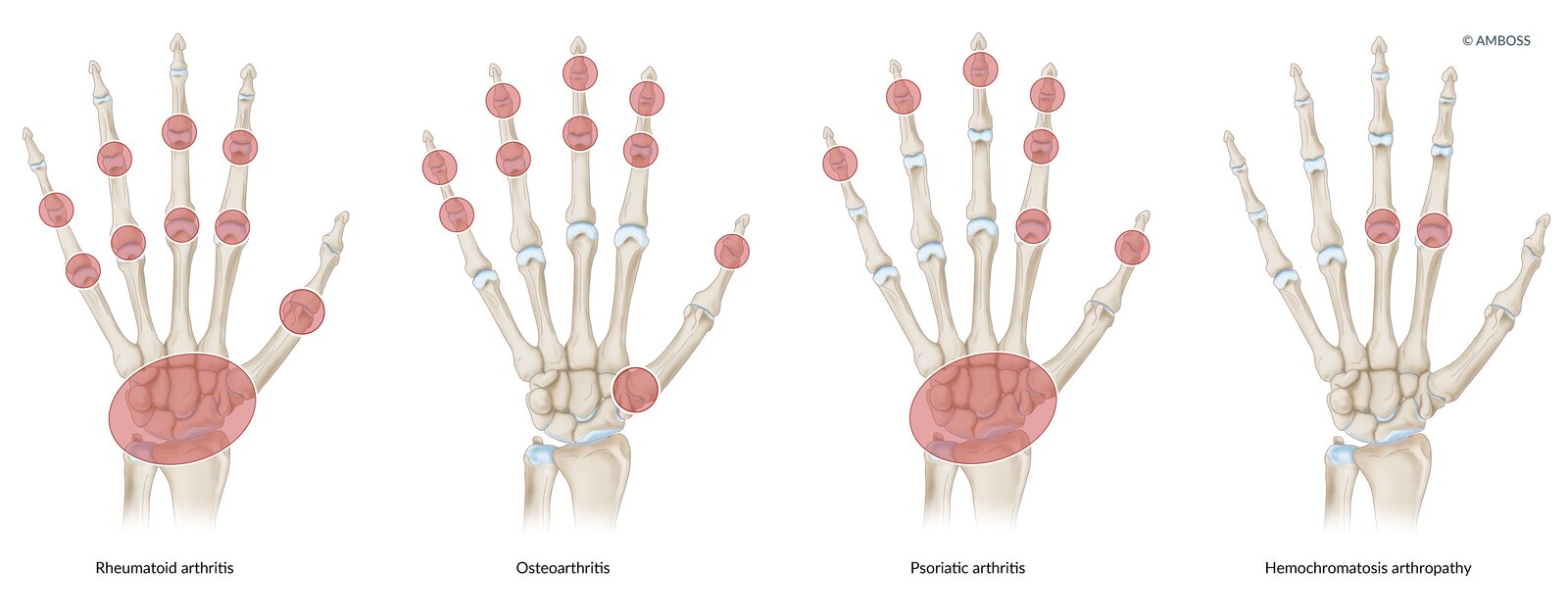
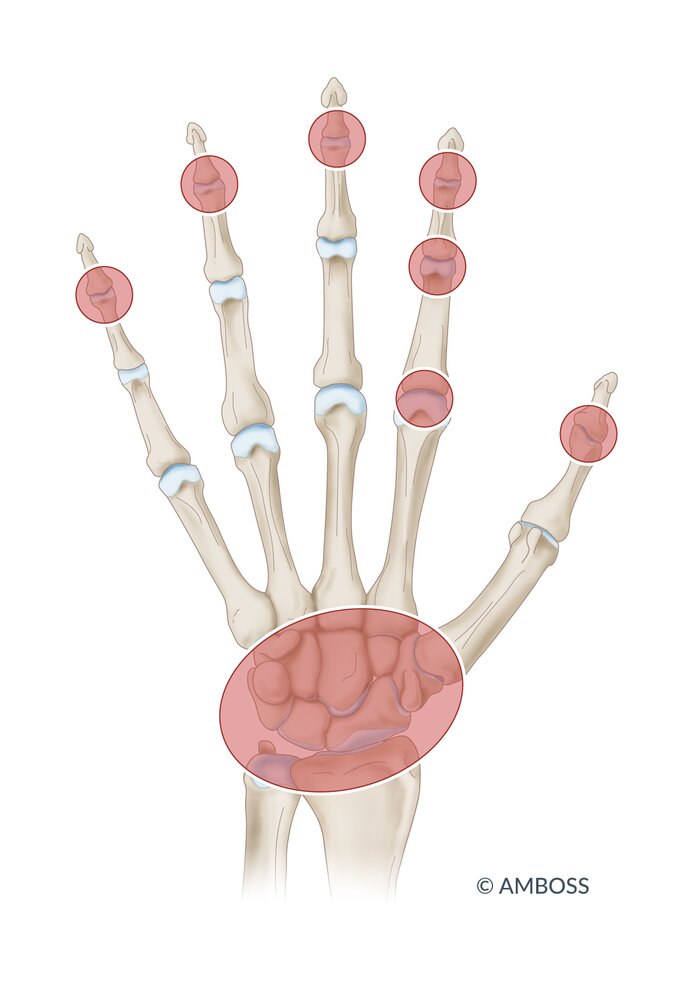
Rheumatoid arthritis: symmetrical swelling of metacarpophalangeal (MCP) and proximal interphalangeal (PIP) joints
Osteoarthritis: PIP, distal interphalangeal (DIP), and first carpometacarpal (CMC) joints
Psoriatic arthritis: DIP and MCP joints, or whole digit (dactylitis)
Hemochromatosis: symmetrical arthropathy of the MCP joint of the second and third digits
© AMBOSS

Hands of an adult female
The nail of the third digit of the right hand shows distinct signs of onycholysis (the other digits have artificial nails). There is dactylitis of the second and fifth digit of the right hand and the thumb of the left hand. A Boutonniere deformity can also be seen in the second digit of the right hand.
These are typical findings of psoriatic arthritis.
Source: Courtesy of Dr. Gary M. White, MD

Erythematous swelling on the proximal interphalangeal joint of the fifth digit and on the interphalangeal joint of the thumb. Nail involvement (nail dystrophy with an oil drop sign and pitted nails) is also evident.
Source: © IMPP

The fingers are grossly shortened and each phalangeal segment has telescoped into the proximal phalangeal segment.
This is the characteristic appearance of arthritis mutilans, which is an end-stage deformity caused by destructive erosive arthritides, such as psoriatic arthritis, rheumatoid arthritis, and gout.
Source: © IMPP
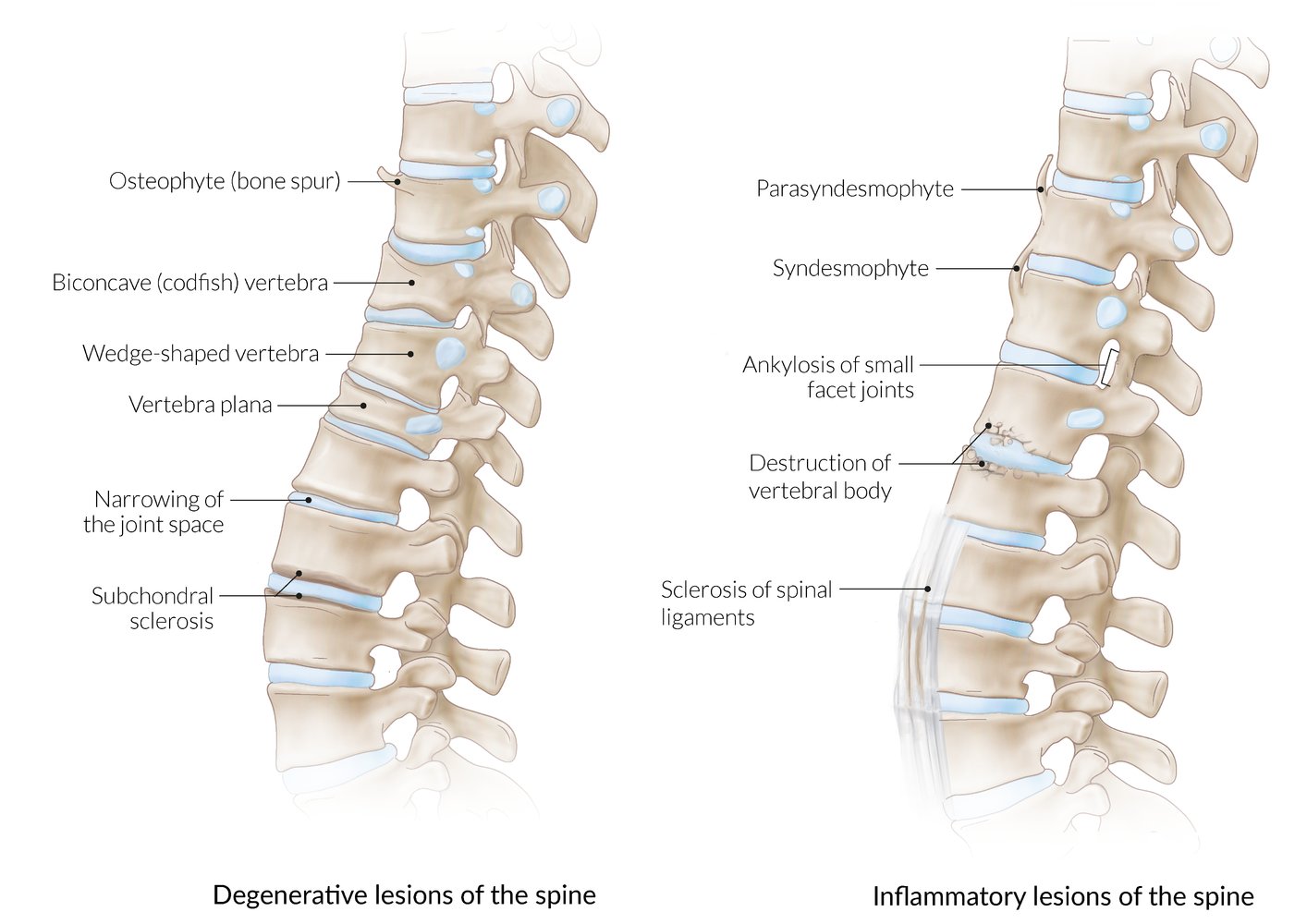
Degenerative lesions result from wear and tear and are associated with older age. Inflammatory lesions occur in diseases such as ankylosing spondylitis and psoriasis.
If there is subchondral erosion or destruction of the vertebral body, consider bacterial infection or a tumor as possible etiologies.
© AMBOSS

Right foot of a patient with psoriatic arthritis
The fourth toe appears swollen and hyperemic, and the distal end of the second toe is also swollen. No superficial trauma, axial deviation, or dislocation of the toes is visible. The rest of the foot, including the toenails, appears normal.
Source: © IMPP

Enthesitis of the Achilles tendon in psoriatic arthritis
Source: © IMPP

The entire left index finger of this patient with psoriatic arthritis is swollen.
This appearance is typical of dactylitis, which can be caused by a variety of conditions, including spondyloarthropathies, infections, and sickle cell disease.
Source: © IMPP
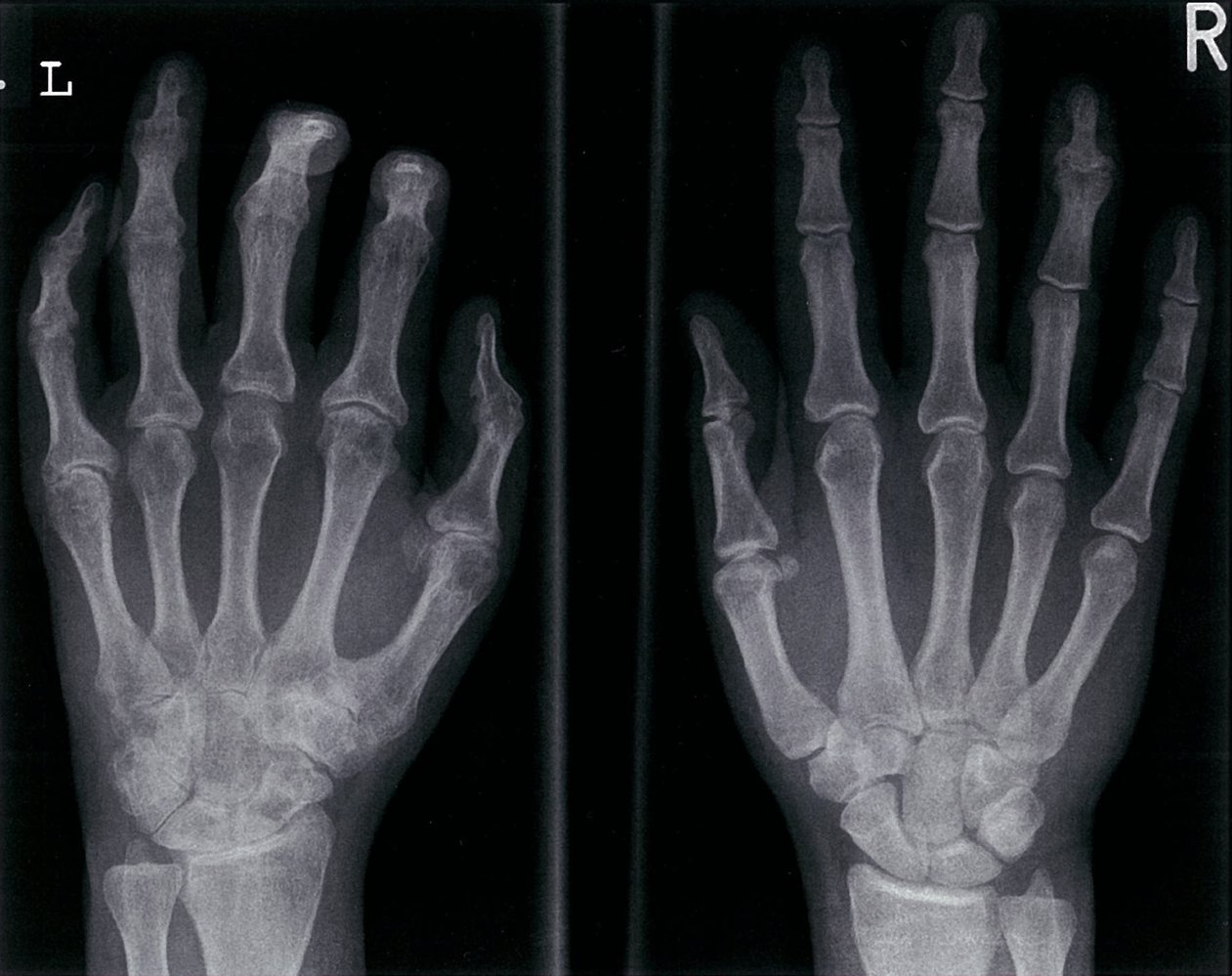
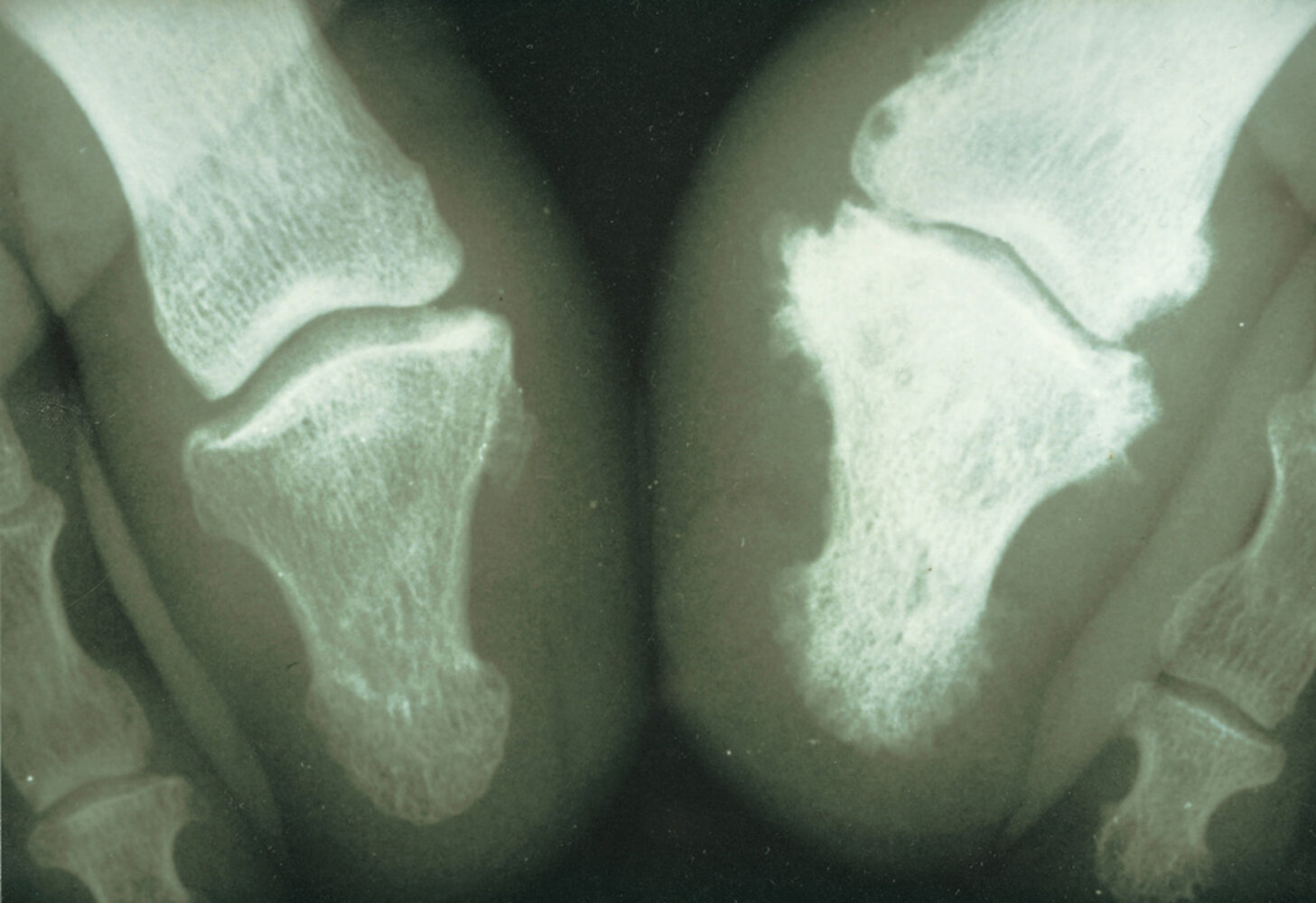
X-ray hands (PA view)
Asymmetric advanced arthritis involves the left hand, with ankylosis of several proximal and distal interphalangeal (PIP and DIP) joints (examples indicated by green overlay) along with multiple flexion deformities. Marginal erosions are present at the bases of the small finger proximal phalanx and thumb distal phalanx (red overlay). Central subchondral erosions and proliferative changes with a gull-wing deformity are seen at the right ring finger DIP joint.
Also shown is an illustration of a pencil-in-cup deformity (not present here), which can occur in psoriatic arthritis and several other inflammatory arthritides.
Advanced degenerative changes additionally involve multiple left carpal and metacarpal joints.
Source: © IMPP

Anteroposterior x-ray of the lumbar spine:
1. Syndesmophytes: e.g., between L3 and L4 (example shown on the left).
2. Parasyndesmophytes : e.g., right lateral of L2–L3
Source: © IMPP
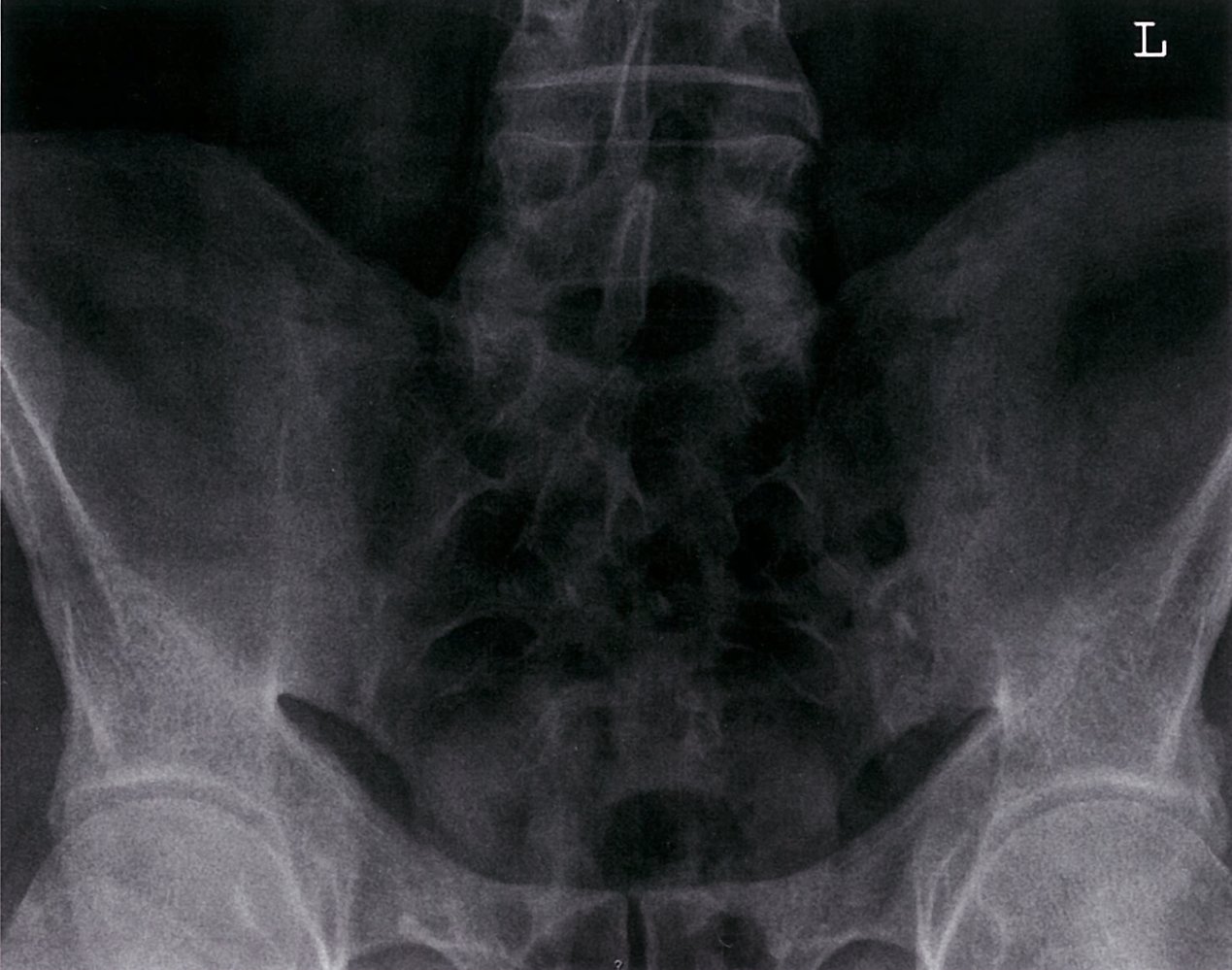
Anteroposterior sacroiliac joint:
1. Fusion of the sacroiliac joints in line with ankylosis
2. Subchondral sclerosis of both acetabular roofs
Source: © IMPP
Diagnosis
Psoriasis is a clinical diagnosis based on patient and family history and thorough skin examination.
Approach [2][14]
- Consult a dermatologist to confirm the diagnosis.
- Skin biopsy is not routinely required for diagnostic confirmation.
- Perform an ASCVD risk assessment. [2]
- Evaluate for comorbidities including psoriatic arthritis, IBD, MDD, and anxiety.
All patients with psoriasis should be evaluated for psoriatic arthritis, as early diagnosis improves outcomes and the presence of psoriatic arthritis influences treatment decisions. [2]
Skin biopsy [15]
- Indications: Consider only if clinical presentation is atypical.
-
Supportive findings
- Acanthosis and parakeratosis
- Thickening of the stratum spinosum, thinning of the stratum granulosum
- Munro microabscesses: accumulation of neutrophils in the stratum corneum surrounded by parakeratosis
Differential diagnoses
| Differential diagnosis of scaling | ||
|---|---|---|
| Disorder | Lesion | Distribution |
| Psoriasis |
|
|
| Atopic dermatitis |
|
|
| Seborrheic dermatitis |
|
|
| Pityriasis rubra pilaris |
|
|
| Erythroderma [16] |
|
|


")



The differential diagnoses listed here are not exhaustive.
Multiple round, sharply demarcated, scaly, erythematous plaques are visible on the arms and trunk.
This appearance is typical of guttate psoriasis, a subtype of psoriasis.
Source: “Figure 76, In: Atlas of Paediatric HIV Infection” by Regina E. Oladokun, Rannakoe J. Lehloenya, Carol Hlela et.al., Openbooks, licensed under CC BY-ND 4.0.

Papulovesicular erythema and hyperpigmentation are visible on the popliteal fossae of both legs
Source: © IMPP

Dark, lichenified lesions with excoriations are visible on this patient's left arm and leg. The skin appears dry and coarse.
These findings are consistent with inflammatory lesions of atopic dermatitis in skin of color.
Source: “Figure 69b, in: Atlas of Paediatric HIV Infection” by Regina E. Oladokun, Rannakoe J. Lehloenya, Carol Hlela et.al., Openbooks, licensed under CC BY-ND 4.0.

Photograph of the scalp of a 2-month-old
Yellow, scaling plaques on erythematous skin extend over the scalp.
This appearance in an infant is consistent with infantile seborrheic dermatitis.
Source: “Infant (2 months old) with cradle cap” by LepoRello, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}

Well-defined erythema with peripheral scaling is visible on this child's neck. Fine, whitish scaling is also visible behind the ear.
The location of these lesions is typical of infantile seborrheic dermatitis.
Source: “Figure 67f, In: Atlas of Paediatric HIV Infection” by Regina E. Oladokun, Rannakoe J. Lehloenya, Carol Hlela et.al., Openbooks, licensed under CC BY-ND 4.0.
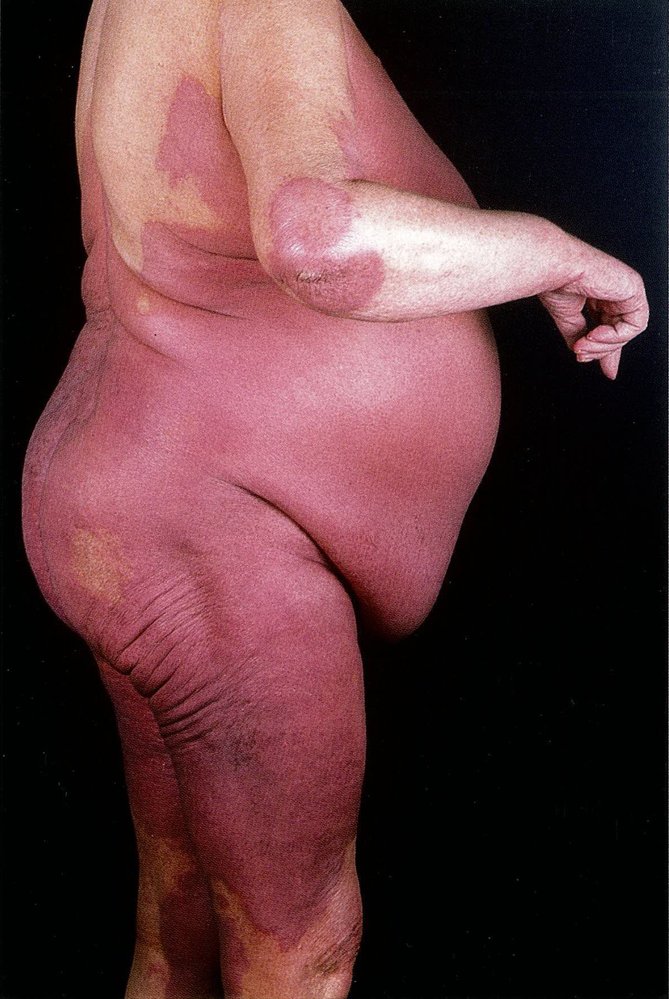
Erythema and thickening of the skin can be seen across the trunk, proximal lower limbs, and over the right elbow.
This is the typical appearance of erythroderma (exfoliative dermatitis), which may be idiopathic or occur secondary to a drug reaction or systemic disease (e.g., psoriasis, atopic dermatitis).
Source: © IMPP

Back of a 68-year-old patient showing generalized erythematosquamous skin.
Source: © IMPP
Treatment
The following recommendations apply to the treatment of plaque psoriasis ; consult a specialist before initiating treatment.
Approach to patients with psoriasis[2][14][17]
Treatment depends on disease severity, comorbidities, and patient preference.
-
All patients
- Assess disease severity: e.g., based on estimated body surface area (BSA) affected.
- Provide supportive care.
-
Mild psoriasis (below 3–5% BSA involvement)
- Topical pharmacotherapy (e.g., corticosteroids, calcipotriene, retinoids) and/or targeted phototherapy
- Systemic agents if treatment response is insufficient
-
Moderate to severe psoriasis (above 3–5% BSA involvement)
- Systemic pharmacotherapy
-
And/or phototherapy
- Narrowband UVB therapy
- PUVA therapy
- Consider adjunctive topical pharmacotherapy.
All patients with plaque psoriasis and concomitant psoriatic arthritis require systemic treatment. [2]


Topical pharmacotherapy [2][17]
Topical pharmacotherapy is the mainstay of mild psoriasis treatment.
-
Topical corticosteroids (first-line: )
- Face, neck, or skin folds (i.e., areas with sensitive/thin skin): low-potency (e.g., hydrocortisone 1%)
- Scalp, trunk, and extremities
- Medium-potency (e.g., triamcinolone 0.1%)
- High-potency (e.g., fluocinonide 0.05%)
-
Topical calcineurin inhibitors (off-label use ): e.g., tacrolimus 0.03 % or 0.1%, or pimecrolimus 1%
- Alternative to steroids for areas with sensitive/thin skin
- May be used for maintenance after > 4 weeks of steroid use
-
Additional therapy: the following agents may be used in combination with topical corticosteroids
- Vitamin D analogues: e.g., calcipotriene/calcipotriol
- Keratolytics: retinoids (e.g., tazarotene), or salicylic acid
- Tar preparations, e.g., 1% coal tar lotion
- Anthralin
Commonly used combinations include topical corticosteroids plus either vitamin D analogues or keratolytic agents. Combination therapy increases efficacy and may cause fewer adverse effects than monotherapy.
Systemic pharmacotherapy [18][19]
-
Principles of systemic therapy
- Management should be specialist guided
- Before therapy initiation, obtain baseline laboratory studies (e.g., BMP, CBC, liver chemistries).
- Adjunctive topical pharmacotherapy may be added after a careful review for possible interactions.
-
Common indications
- Moderate to severe psoriasis
- Mild psoriasis with insufficient response to topical agents
-
Treatment options
-
Biologics
- IL-17 inhibitors, e.g., brodalumab, secukinumab
- IL-23 inhibitors, e.g., ustekinumab , guselkumab
- TNF-α inhibitors, e.g., etanercept, adalimumab, infliximab
- Other medications
- Methotrexate PLUS folic acid to reduce the adverse effects
- Cyclosporine
- Apremilast
-
Biologics
Supportive care [17]
- Provide topical treatment with ointments (e.g., petroleum jelly) and moisturizers to prevent moisture loss.
- Counsel on reducing alcohol consumption and smoking cessation.
- Provide management for any comorbid mental health conditions (e.g., MDD, anxiety).
Alcohol consumption and tobacco use are associated with increased disease severity and ASCVD risk. [14]
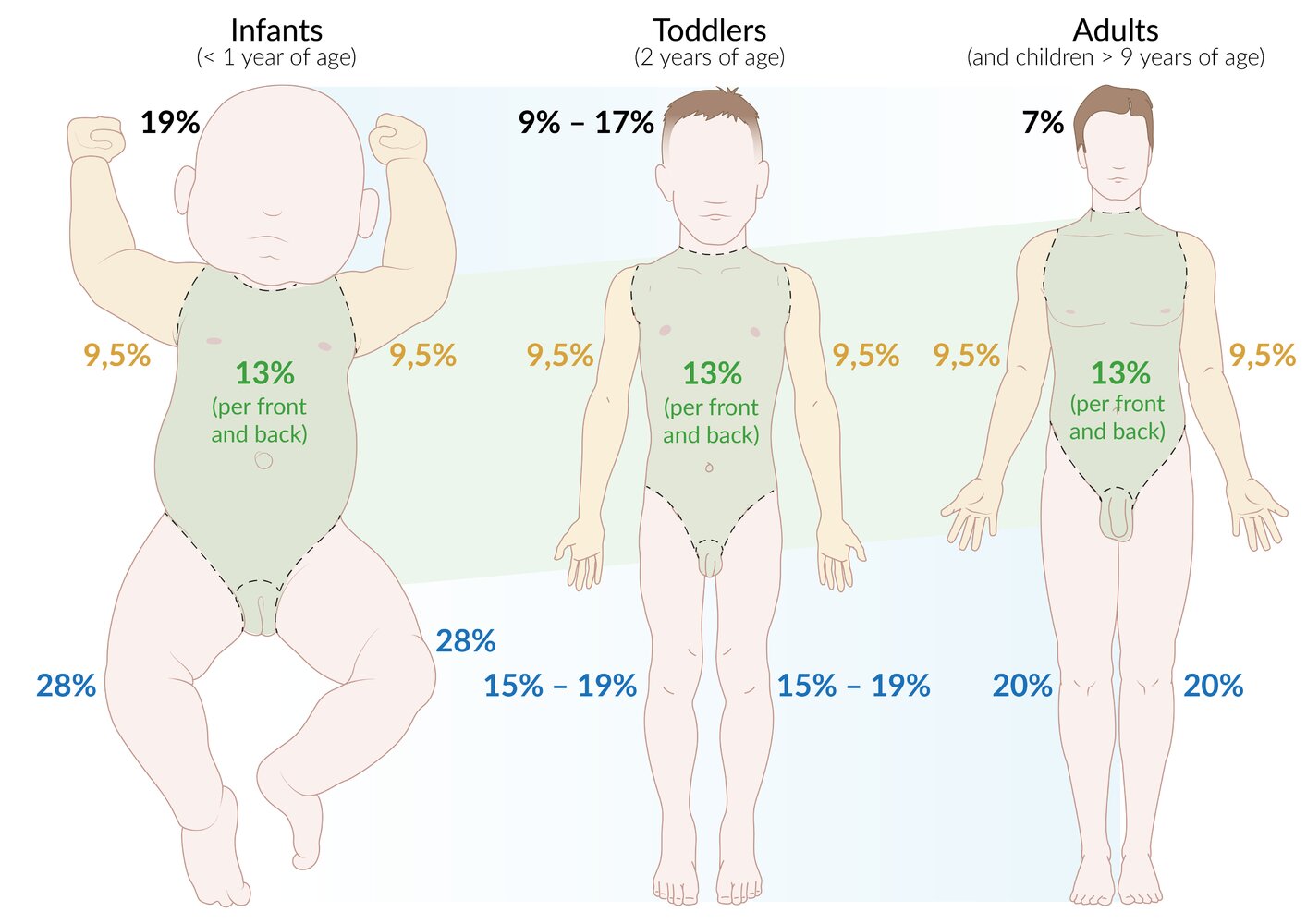
Representation of development from infant to toddler to adulthood (according to Wallace rule of nines). The regions of the body that occupy the same percentage of the total body surface area throughout development are indicated in green, whereas regions of the body in which the relative proportion of the total body surface area varies with age are depicted in blue.
© AMBOSS
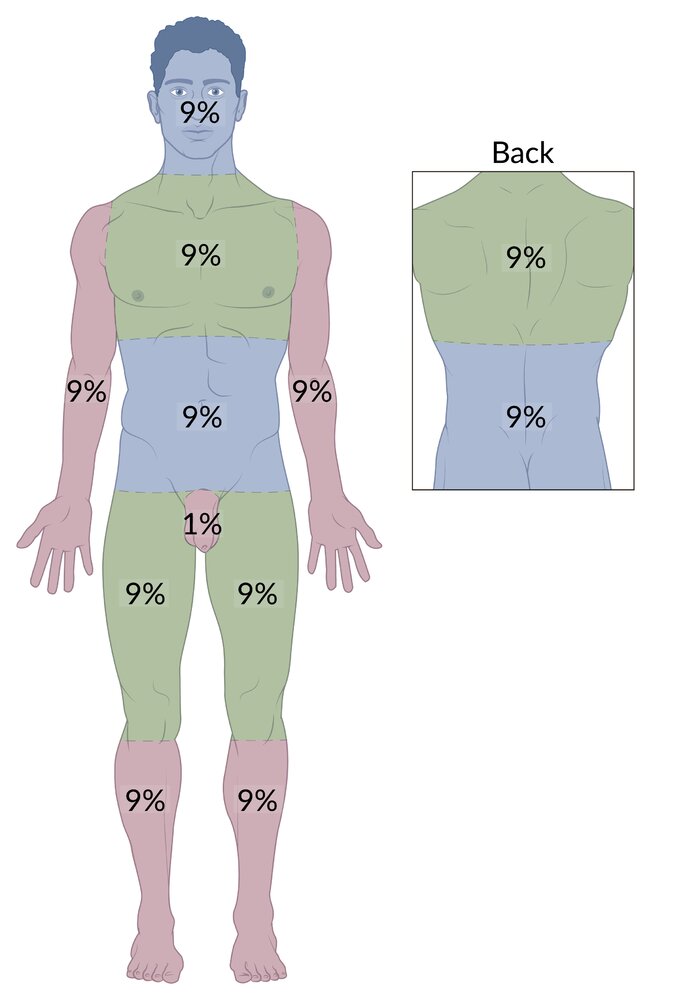
The entire body surface of an adult can be divided into 11 regions, each comprising approximately 9% of the total body surface area. The external genitalia accounts for the remaining 1%. The rule of nines is used to quickly estimate the total body surface area affected by burns in adults.
© AMBOSS
Complications
Increased risk of other comorbidities:
- Metabolic syndrome
- Cardiovascular diseases (hypertension, coronary heart disease, myocardial infarction, stroke)
- Chronic kidney disease
We list the most important complications. The selection is not exhaustive.
Prognosis
- Lifelong disease, usually benign
- Patients may experience remissions of varying lengths; acute episodes of exacerbation possible.
- Psoriasis is associated with depression and a decreased quality of life.
Prevention
- Avoidance of nicotine and alcohol
- Regular physical activity
External Resources
- 2018 ACR/NPF Guideline for the Treatment of Psoriatic Arthritis
- 2021 AAD–NPF Guidelines for the Treatment of Psoriasis with Topical Therapy and Alternative Medicine Modalities
- 2019 AAD-NPF Guidelines for the Treatment of Psoriasis with Biologics
- 2019 AAD-NPF Guidelines for the Treatment of Psoriasis with Awareness and Attention to Comorbidities
References
- Langley RGB. "Psoriasis: epidemiology, clinical features, and quality of life". Ann Rheum Dis. 64(suppl_2). :ii18-ii23. (2005)
- Armstrong AW, Read C. "Pathophysiology, Clinical Presentation, and Treatment of Psoriasis". JAMA. 323(19). :1945. (2020)
- Parisi R, Symmons DP, Griffiths CE, Ashcroft DM. "Global epidemiology of psoriasis: a systematic review of incidence and prevalence". J Invest Dermatol. 133(2). :377-385. (2013)
- Queiro R, Tejón P, Alonso S, Coto P. "Age at disease onset: a key factor for understanding psoriatic disease". Rheumatology. 53(7). :1178-1185. (2013)
- Hüffmeier U, Lascorz J, Becker T et al. "Characterisation of psoriasis susceptibility locus 6 (PSORS6) in patients with early onset psoriasis and evidence for interaction with PSORS1". J Med Genet. 46(11). :736–744. (2009)
- Feldman SR. "Epidemiology, Clinical Manifestations, and Diagnosis of Psoriasis". UpToDate. UpToDate. https://www.uptodate.com/contents/epidemiology-clinical-manifestations-and-diagnosis-of-psoriasis. [2015-12-09]
- Lowes MA, Suárez-Fariñas M, Krueger JG. "Immunology of psoriasis". Annu Rev Immunol. 32. :227-255. (2014)
- "Pruritus severity in patients with psoriasis is not correlated with psoriasis disease severity". http://www.jaad.org/article/S0190-9622(13)01012-8/abstract. [2014-02-01]
- Rosso Schons KR, Faccin Knob C, Murussi N, et al. "Nail psoriasis: a review of the literature". An Bras Dermatol. 89(2). :312-317. (2014)
- Elmets CA, Leonardi CL, Davis DMR, et al. "Joint AAD-NPF guidelines of care for the management and treatment of psoriasis with awareness and attention to comorbidities". J Am Acad Dermatol. 80(4). :1073-1113. (2019)
- Jacobi A, Prinz JC. "Autoimmune Diseases of the Skin". Springer Science & Business Media. :327. (2005). ISBN: 9783211206867
- Davis MDP. "Erythroderma in Adults". UpToDate. UpToDate. https://www.uptodate.com/contents/erythroderma-in-adults. [2016-09-21]
- Elmets CA, Korman NJ, Prater EF, et al. "Joint AAD–NPF Guidelines of care for the management and treatment of psoriasis with topical therapy and alternative medicine modalities for psoriasis severity measures". J Am Acad Dermatol. 84(2). :432-470. (2021)
- Menter A, Strober BE, Kaplan DH, et al. "Joint AAD-NPF guidelines of care for the management and treatment of psoriasis with biologics". J Am Acad Dermatol. 80(4). :1029-1072. (2019)
- Menter A, Gelfand JM, Connor C, et al. "Joint American Academy of Dermatology–National Psoriasis Foundation guidelines of care for the management of psoriasis with systemic nonbiologic therapies". J Am Acad Dermatol. 82(6). :1445-1486. (2020)
- Ritchlin CT, Colbert RA, Gladman DD. "Psoriatic Arthritis". N Engl J Med. 376(10). :957-970. (2017)
- FitzGerald O, Ogdie A, Chandran V, et al. "Psoriatic arthritis". Nat Rev Dis Primers. 7(1). :59. (2021)
- Taylor W, Gladman D, Helliwell P, et al. "Classification criteria for psoriatic arthritis: Development of new criteria from a large international study". Arthritis Rheum. 54(8). :2665-2673. (2006)
- Singh JA, Guyatt G, Ogdie A, et al. "2018 American College of Rheumatology/National Psoriasis Foundation Guideline for the Treatment of Psoriatic Arthritis". Arthritis & Rheumatology. 71(1). :5-32. (2018)
- Inamadar AC, Palit A, Ragunatha S. "Textbook of Pediatric Dermatology". JP Medical Ltd. (2014). ISBN: 9351520838
- Hertl M. "Autoimmune Diseases of the Skin: Pathogenesis, Diagnosis, Management". Springer Science & Business Media. (2011). ISBN: 3211992251