Summary
Pyelonephritis is an infection of the renal pelvis and parenchyma that is usually associated with an ascending bacterial infection of the bladder. It occurs more commonly in women and risk factors include pregnancy and urinary tract obstruction. Patients typically present with flank pain, costovertebral angle tenderness, fever, and other features of cystitis (e.g., dysuria, frequency). Urinalysis shows pyuria and bacteriuria. Urine cultures should be taken in all patients before initiating treatment to identify the pathogen and possible antibiotic resistance. Early empiric antibiotic treatment is essential to avoid renal complications and urosepsis. Definitive treatment depends on the drug sensitivities of the causative pathogen and the patient's clinical profile (e.g., possible comorbidities).
See also “Urinary tract infections.”
Etiology
- Usually caused by an ascending bacterial infection of the bladder (cystitis)
- Less commonly due to hematogenous spread of infection to the kidney (e.g., infectious endocarditis)
-
Pathogens
-
Gram-negative bacteria
- Escherichia coli (∼ 75–90% of cases; leading cause of pyelonephritis)
- Pseudomonas aeruginosa
- Klebsiella pneumoniae
- Proteus mirabilis
-
Gram-positive bacteria
- Enterococcus faecalis
- Staphylococcus aureus
- Staphylococcus saprophyticus [2]
- Candida infection (especially in immunocompromised patients) is possible
-
Gram-negative bacteria
-
Risk factors for pyelonephritis
- Most common in women because they have shorter urethras
- Pregnancy
-
Urinary tract obstruction (potentially leading to pyonephrosis)
- Foreign bodies (e.g., indwelling urinary catheters or other urologic instrumentation)
- Anatomical abnormalities (e.g., benign prostatic hyperplasia, vesicoureteral reflux, nephrolithiasis, ureteral strictures)
- Cystitis
- Recent administration of antibiotics (possible antibiotic resistance)
- Immunosuppression; (e.g., HIV, diabetes mellitus)
- Renal transplant [3][4]
Classification
The terminology used for classifying pyelonephritis is somewhat controversial and serves primarily to estimate the risk of atypical or antibiotic-resistant pathogens.
- Uncomplicated pyelonephritis: pyelonephritis in an immunocompetent, nonpregnant female with normal genitourinary anatomy and renal function [5][6][7][8]
-
Complicated pyelonephritis: pyelonephritis associated with any of the following risk factors for complications: [6][8]
- Failure of outpatient therapy
- Sepsis
- Male sex
- Age > 60 years
- Urinary tract abnormalities (e.g., obstruction, indwelling catheter)
- History of surgery to the urinary tract or kidneys
- Hospital-acquired infection
- Renal impairment
- History of nephrolithiasis
- Immunosuppression and/or severe comorbidities (e.g., diabetes mellitus, chronic corticosteroid use)
- Pregnancy
Clinical features
- Fever, chills
- Flank pain
- Costovertebral angle tenderness: pain upon percussion of the flank (usually unilateral, may be bilateral)
- Dysuria as well as other symptoms of cystitis (e.g., frequency, urgency)
- Weakness, nausea, vomiting (diarrhea may also be present)
- Possible abdominal or pelvic pain
Suspect pyelonephritis in any patient presenting with fevers, chills, and flank pain, irrespective of lower urinary tract symptoms.
Pyelonephritis symptoms may overlap with those of other life-threatening causes of flank pain (see “Differential diagnosis of pyelonephritis”).


© AMBOSS
Diagnosis
Approach
- Pyelonephritis is a clinical diagnosis that is supported by positive urine culture.
- Routine diagnostic workup should include blood cultures (2 sets), urinalysis with microscopy, and urine culture with susceptibilities.
- Check CBC, BMP for signs of sepsis and organ dysfunction.
- Consider imaging in patients with suspected complicated pyelonephritis or treatment failure.
Laboratory tests
-
Urinalysis [6]
- Nonspecific findings of UTI
- Pyuria (positive esterase on dipstick test)
- Leukocyturia (WBCs > 5/hpf)
- Bacteriuria
- Positive nitrites on dipstick test indicate bacteria that convert nitrates to nitrites. [9]
- Hematuria (including microhematuria)
- Other findings
- WBC casts; : rare finding, but considered to be a strong indicator for pyelonephritis [6][10]
- Urine pH of ≥ 7.5–8.0: associated with urease-producing organisms [1][11][12]
- Epithelial cells > 5/hpf: suggests contamination.
- Gram stain: direct visualization of bacteria (seldom performed)
- Nonspecific findings of UTI
-
Urine culture with susceptibilities
- Perform in all patients with suspected pyelonephritis to determine the pathogen and any associated drug resistance.
- ≥ 105 colony-forming units/mL suggests bacterial infection (See “Urine culture” for more details.) [13][14]
- Blood cultures (2 sets): should be performed in all patients with suspected complicated pyelonephritis
- Urine pregnancy test in women of childbearing age
-
Additional blood tests
- CBC: leukocytosis
- Inflammatory markers: ↑ CRP, ESR
- BMP: may be normal or show elevated BUN and creatinine
Collect urine and blood cultures before administering empiric antibiotic therapy.
 test strip")



Imaging [15]
Indications
- Imaging is not routinely indicated in patients with suspected acute uncomplicated pyelonephritis.
- Imaging serves to identify obstruction, abscess, or emphysematous pyelonephritis.
- Consider in the following situations: [1]
- Complicated pyelonephritis
- Sepsis or septic shock
- Known or suspected nephrolithiasis [16]
- New decline in eGFR to < 40
- Recurrent pyelonephritis [5]
- No response to therapy within 2 days
CT is the imaging study of choice for assessing patients with suspected complicated pyelonephritis and ruling out differential diagnoses.
In the emergency department, renal POCUS may be helpful for quickly identifying hydronephrosis, but it does not preclude the need for CT in patients who require imaging. [17]
CT abdomen and pelvis with and without IV contrast [18]
Modality of choice in nonpregnant patients who need imaging
-
CT findings in pyelonephritis
- Renal parenchyma may appear normal (early) or edematous (hypodense areas)
- Infected parenchyma may be visible as; wedge-shaped areas of streaky contrast enhancement (striated nephrogram). [18]
-
CT findings in urinary tract obstruction
- Hydroureter, hydronephrosis
- Nephrolithiasis, urolithiasis (well-defined hyperintensities)
-
Other findings that may be present
- Congenital abnormalities of the renal tract
- Abscess: intra-or extraparenchymal hypodense areas with peripheral contrast enhancement
- Emphysematous pyelonephritis: presence of gas within the renal parenchyma, collecting system or perinephric space [19]
- Hemorrhage in the parenchyma (hyperdense areas)



Ultrasound of the kidneys and bladder [18]
- Indications: patients with contraindications to CT scan (e.g., allergy to contrast)
-
Findings supportive of pyelonephritis
- Renal enlargement
- Loss of corticomedullary differentiation
- Edema (hypoechoic regions)
- Hemorrhage (hyperechoic regions) in the parenchyma
- Abscess: thick-walled hypoechoic region
-
Findings supportive of urinary tract obstruction
- Hydroureter, hydronephrosis
- Thickened bladder wall
- High bladder residual volume
- Prostate enlargement
- Disadvantages: low sensitivity compared to CT, particularly in early acute infections [18]


MRI abdomen and pelvis
- Indications
- Patients with contraindications to CT
- Pregnancy [18]
- Findings: similar to CT scan (See “CT abdomen and pelvis with and without IV contrast.”) [18]

Additional imaging modalities
The following are rarely used, as CT, MRI, and ultrasound are more widely available.
-
Intravenous pyelogram (IVP)
- Indications: suspected obstruction or congenital abnormality [20]
- Characteristic findings [18]
- Enlarged kidney
- Striated nephrogram
- Delayed nephrogram and delayed calyceal opacification time [21]
- Dilation or effacement of the collecting duct
-
DMSA scan [18]
- Indications: children with suspected pyelonephritis [22]
- Characteristic findings: Acute pyelonephritis is visible as focal or global areas of decreased uptake.
-
Additional imaging to consider
- Voiding cystourethrogram: used to diagnose vesicoureteral reflux [23]
- Urodynamic testing: to exclude neurogenic bladder or subvesical obstruction

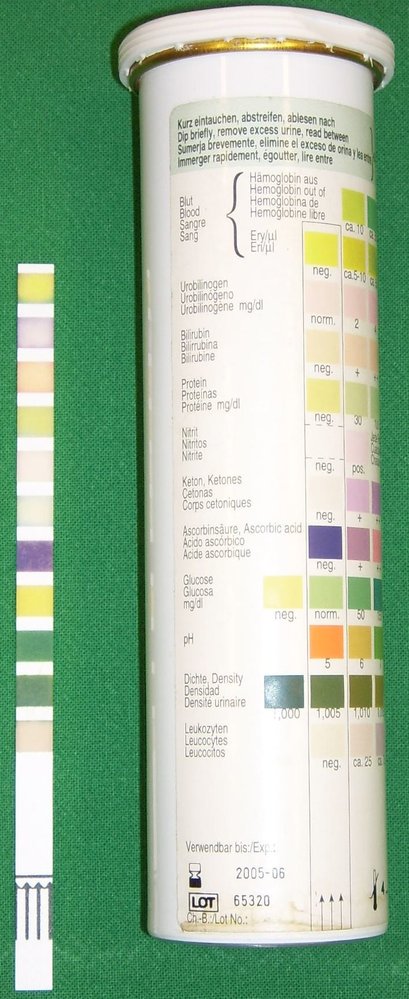
Left: test strip following immersion in urine
Right: test strip packaging with instructions on how to interpret findings
Source: “Urine Quicktest” by Uwe Gille, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}
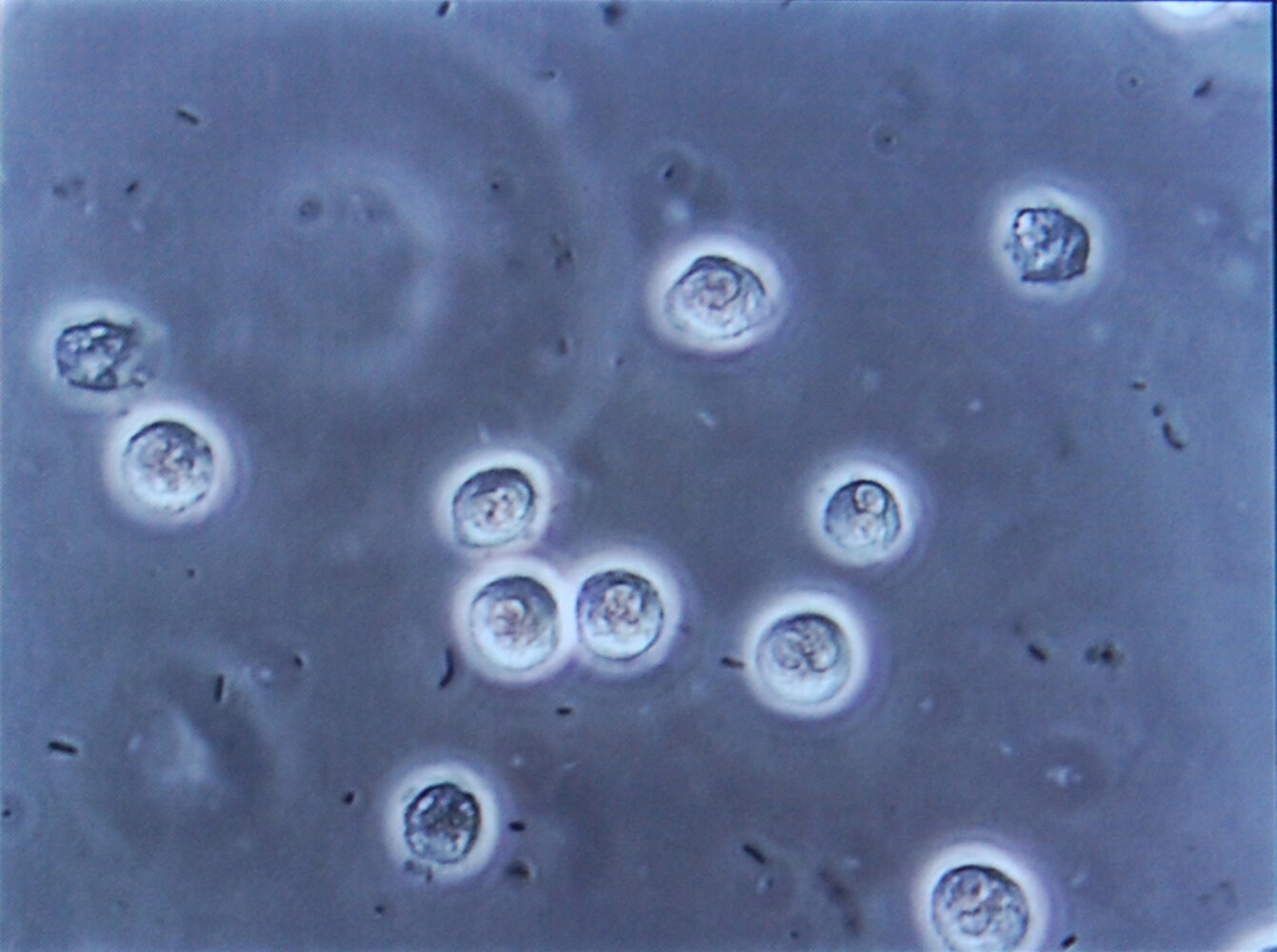
Photomicrograph of a urine specimen (high magnification)
Multiple white blood cells (large, light-colored structures) and bacteria (small black structures) are visible.
The presence of white blood cells (pyuria) and bacteria (bacteriuria) in the urine is characteristic of urinary tract infection.
Source: “Bacteriuria pyuria 4” by Steven Fruitsmaak, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}
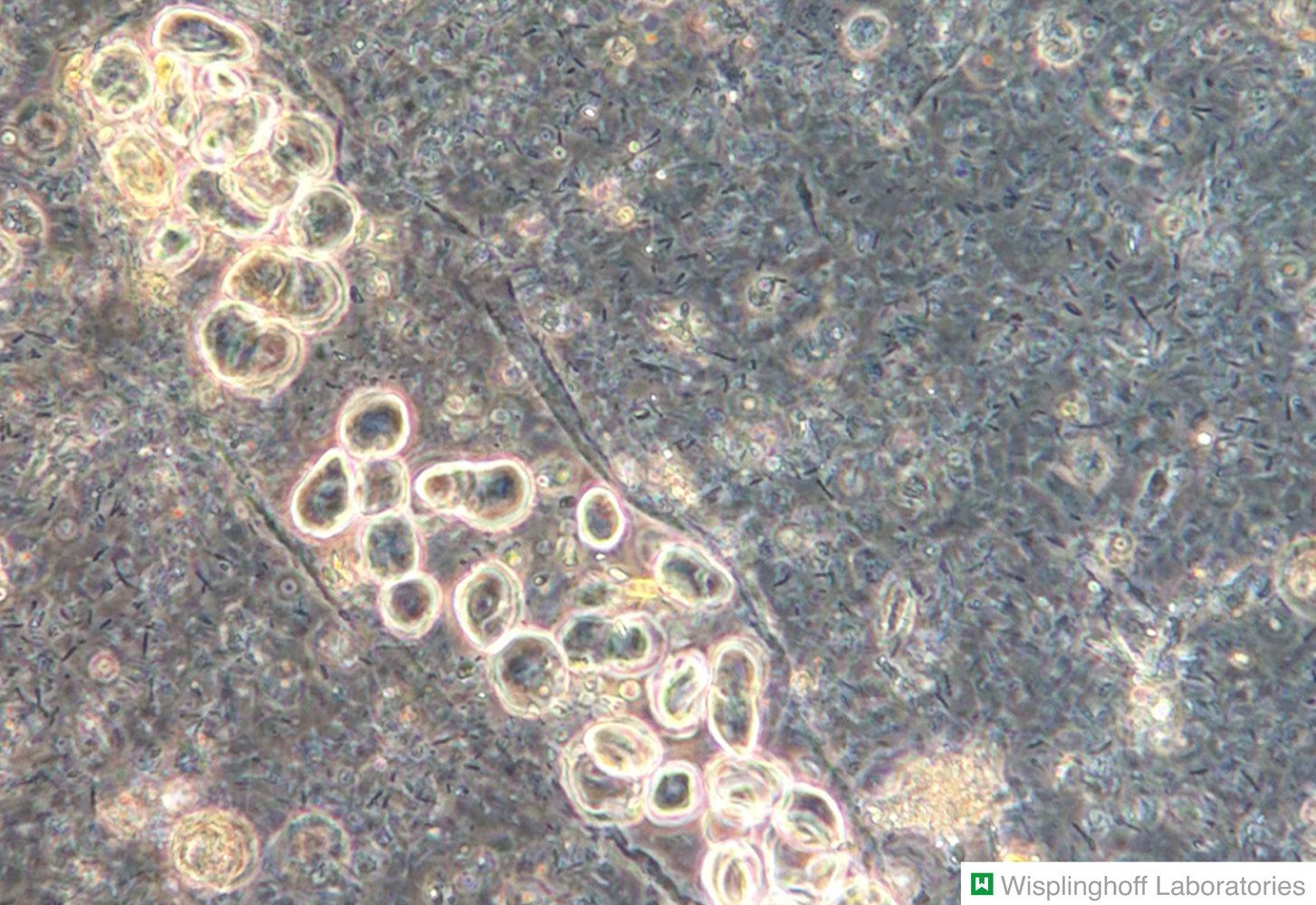
Photomicrograph of urine sediment (phase-contrast microscopy; high magnification)
White blood cell (WBC) casts (blue overlay) contain leukocytes (examples outlined in yellow) that are compressed in a matrix. Sharp margins are characteristic of WBC casts, differentiating them from randomly assembled leukocyte conglomerates.
Our great thanks to Dr. Wisplinghoff (Dr. Wisplinghoff's laboratory) for kindly providing this image.

Photomicrograph of urine sediment (phase-contrast microscopy; high magnification)
The granular cast in the center of the image is comprised of a hyaline matrix (green overlay) with large droplets of plasma proteins embedded within.
Granular casts can be an indication of proteinuria (e.g., in glomerulonephritis or pyelonephritis). However, they may also be present in healthy individuals (e.g., after severe physical stress).
Our great thanks to Dr. Wisplinghoff (Dr. Wisplinghoff's laboratory) for kindly providing this image.
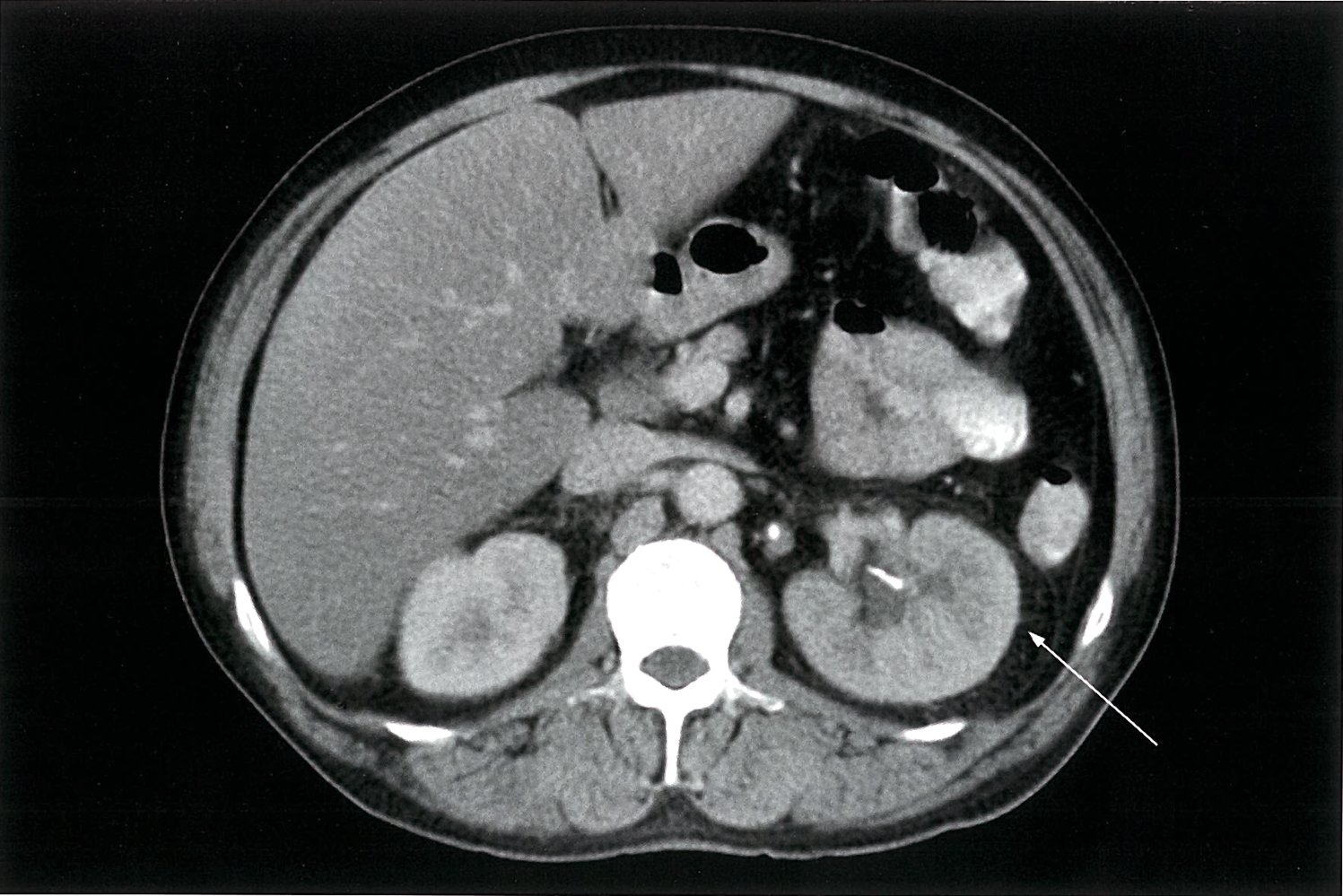
CT abdomen (with IV contrast; venous phase; axial plane) of a patient with acute pyelonephritis
The left ureter and renal pelvis are slightly dilated (red overlay) and contain hyperdense calculi (white arrowheads). The left kidney is larger than the right and the left renal parenchyma (green overlay) shows reduced contrast enhancement. There is also perinephric stranding (yellow overlay and white arrow), which is an important sign of renal inflammation or obstruction.
V: inferior vena cava; A: aorta
Source: © IMPP
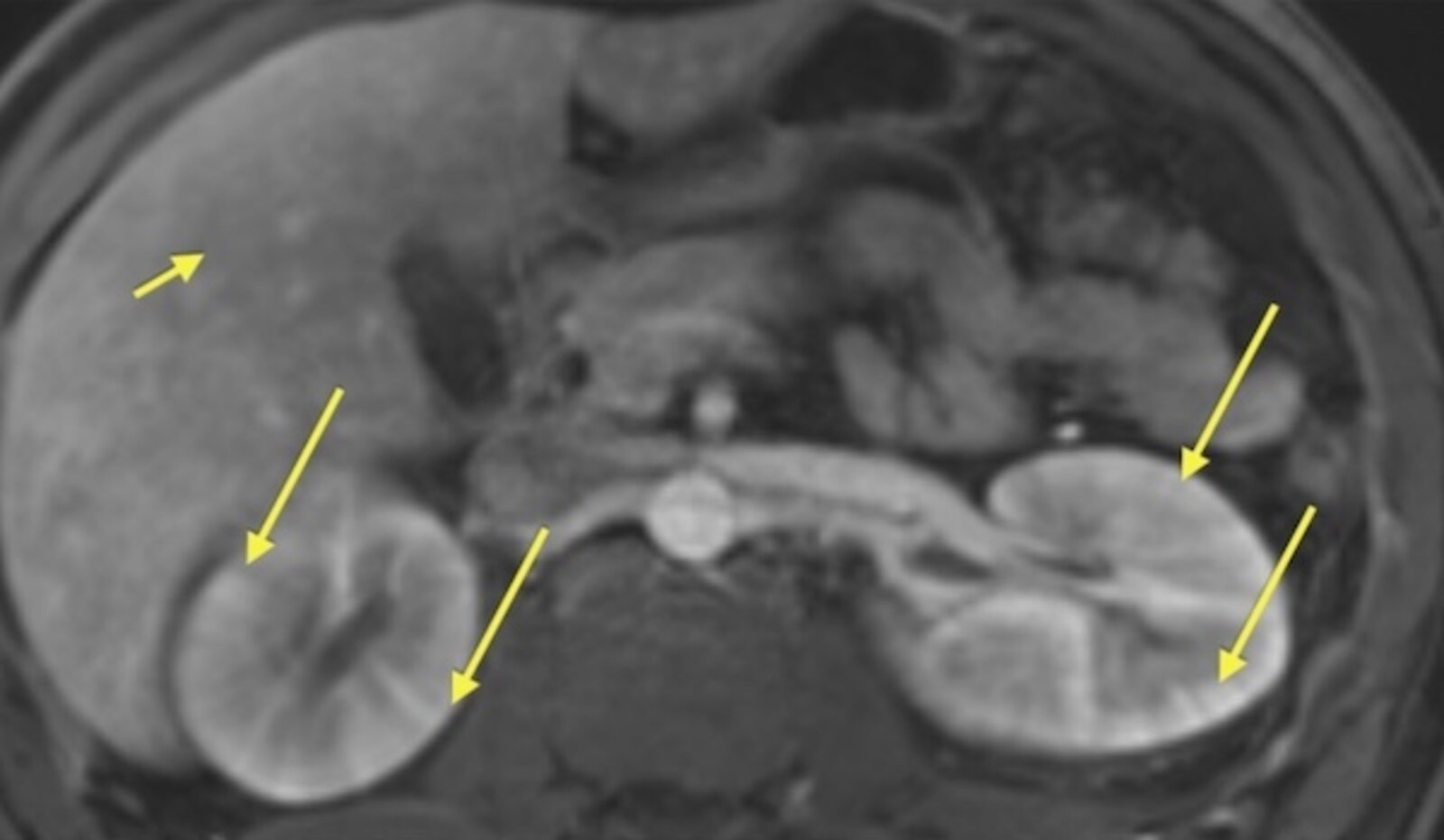
MRI abdomen (kidneys; T1-weighted fat-saturated; with contrast; arterial phase)
Alternating high- and low-attenuation linear bands (striations; arrows) radiate through the cortex and medulla of the kidney parallel to the axes of tubules and collecting ducts.
A striated nephrogram can result from stasis and concentration of contrast in edematous or necrotic renal tubules.
Source: “Figure 3, in: Allergic Interstitial Nephritis Manifesting as a Striated Nephrogram” by Irfan Moinuddin, Erika Bracamonte, Bijin Thajudeen, Amy Sussman, Machaiah Madhrira, and James Costello, Case Reports in Medicine, licensed under CC BY 3.0.

CT abdomen and pelvis (without contrast; coronal plane) of a patient with a history of neurogenic bladder and recurrent urinary infections
The renal calyces, pelves, and ureters are dilated (green overlay), with normally concave (cup-shaped) renal calyces appearing convex (club-shaped; examples indicated by arrowheads). Thinning of the renal parenchyma (examples indicated by white dashed lines on the parenchymal edge) suggests that the dilatation is chronic rather than acute. Marked thickening of the bladder wall (red overlay) is likely responsible for chronic ureteral obstruction.
Source: “Figure 3: Computed tomography (coronal view) confirmed moderately severe bilateral hydronephrosis and hydroureter” by Subramanian Vaidyanathan, Fahed Selmi, Kottarathil Abraham Abraham, Peter Hughes, Gurpreet Singh & Bakul Soni, Patient Safety in Surgery Journal, licensed under CC BY 2.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

CT abdomen (without contrast; axial plane)
The rounded hyperdense structure (red arrow) medial to the left kidney is a ureteral calculus. Mild dilatation of the ureter (green overlay) is also visible. An additional, very small calculus (red overlay) is present in a dilated calyx.
K: kidney
Source: “Midureterstonehydro” by James Heilman, MD, Wikimedia Commons, licensed under CC BY-SA 3.0. Modifications: arrow removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
Ultrasound kidney (longitudinal plane)
The renal sinus and cortex (C) are not well differentiated from one another. Much of the central kidney is replaced by a poorly marginated area of hyperechogenicity (green overlay).
Source: “Figure 26, in: Ultrasonography of the Kidney: A Pictorial Review” by Kristoffer Lindskov Hansen, Michael Bachmann Nielsen, Caroline Ewertsen, Diagnostics, licensed under CC BY 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

Ultrasound left kidney (longitudinal plane)
The calyces (green overlay) are dilated and have lost their normal cup-shaped appearance. Flattening of papillae and blunting of fornices can be seen. Where visible, the renal cortical parenchyma is not thinned.
RP: renal parenchyma; Arrowheads: hyperechoic renal sinus
Source: “Ultrasonographic picture taken from a patient with left ureteral stone with hydronephrosis, created in Taiwan” by morning2k, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
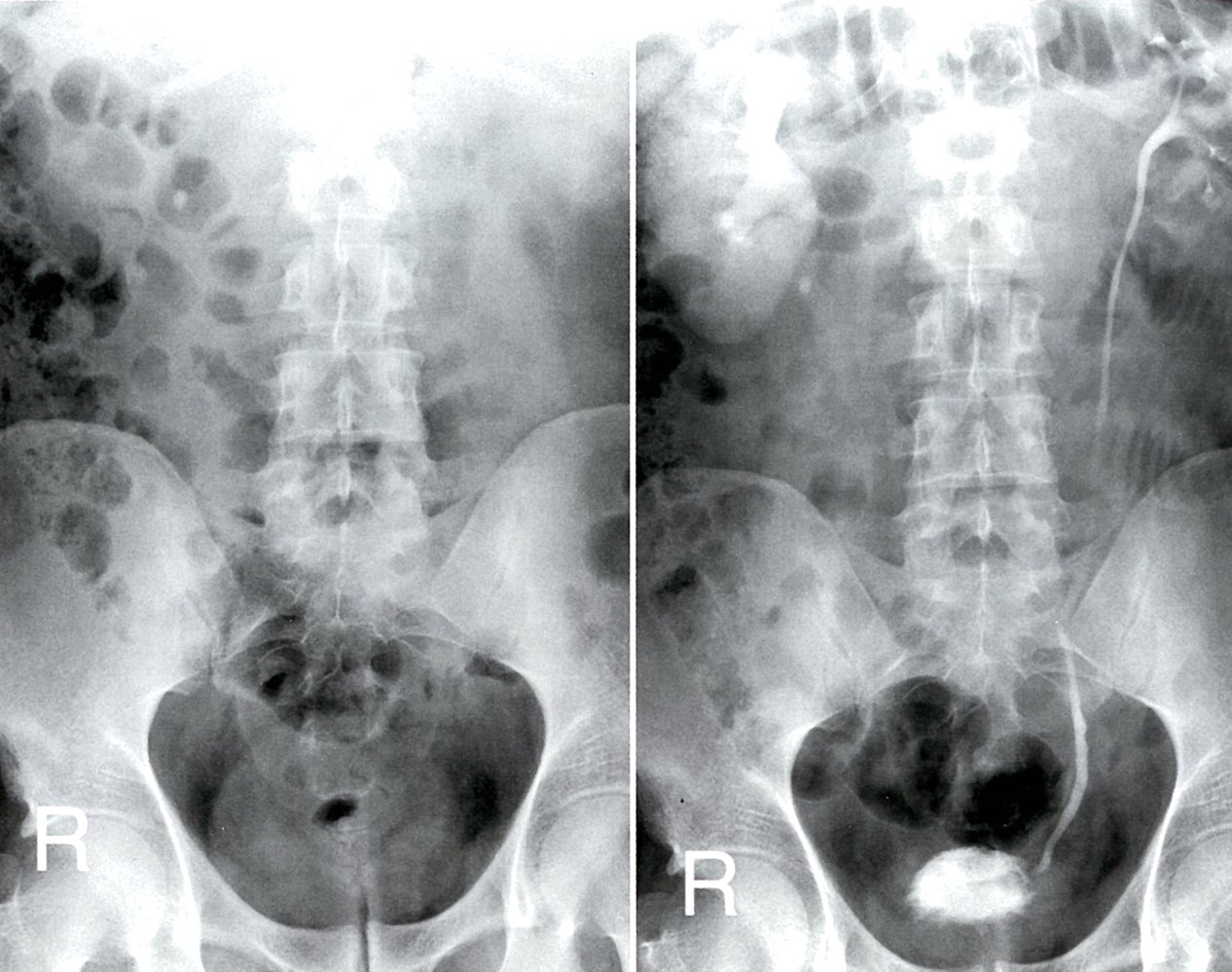
Excretory urography (AP view; left: pre-contrast; right: 2.5 hours post-contrast)
A calcification medial to the lower pole of the right kidney on the pre-contrast radiograph (red overlay) is shown post-contrast to be an obstructing proximal ureteral calculus (UC; red overlay). The right kidney is enlarged, with persistent enhancement (green overlay). There is pelvicaliectasis and poor contrast-filling of the right ureter (region indicated by dashed lines). The left renal collecting system is normal (purple overlay).
RP: renal pelvis, U: ureter; UB: urinary bladder
Source: © IMPP
Pathology
-
Acute pyelonephritis
- Most commonly affects the cortex (spares glomeruli and vessels)
- Purulent inflammation of the interstitium with destruction of the parenchyma, the renal tubules, and, in some cases, the renal pelvis
-
Histology
- Neutrophilic infiltration of the renal tubules and the interstitium
- Sparing of the glomeruli and intrarenal vessels
-
Chronic pyelonephritis
- Chronic inflammatory changes with rough, asymmetric scarring and fibrosis of the corticomedullary junction
- Blunted calyces from recurrent urinary reflux
- Histology: eosinophilic casts in the tubules that resemble thyroid tissue with coloid (thyroidization of the kidney)
-
Xanthogranulomatous pyelonephritis
- A rare form of chronic pyelonephritis characterized by chronic destructive granuloma formation
- Associated with Proteus mirabilis and Escherichia coli infections
- Large, irregular, yellow-orange masses on gross examination of the kidney (may be mistaken for a true renal neoplasm)
- Histology: granulomatous tissue with lipid-laden foamy macrophages and multinucleated giant cells



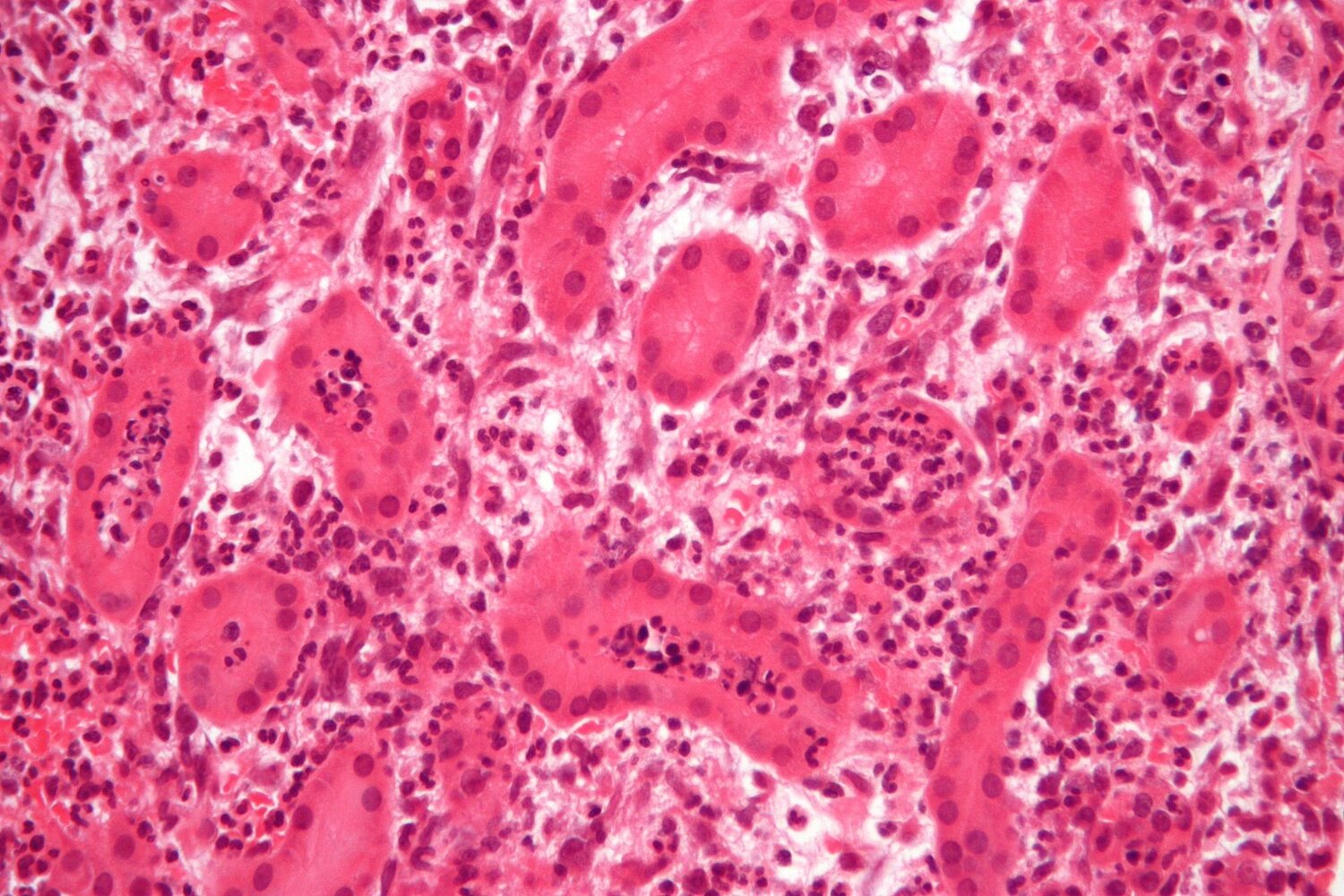
Photomicrograph of a renal tissue biopsy specimen (H&E stain, very high magnification)
Areas of neutrophilic infiltration are visible throughout the renal interstitium (example indicated by hatched green overlay), especially in the tubules (example indicated by green overlay), which appear dilated.
These findings suggest acute pyelonephritis.
Source: “Acute pyelonephritis - 2 - very high mag” by Nephron, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}

Macroscopic preparation of a kidney specimen
There are multiple irregular areas of fibrosis.
This is the typical appearance of fibrosis in chronic pyelonephritis.
Source: © IMPP
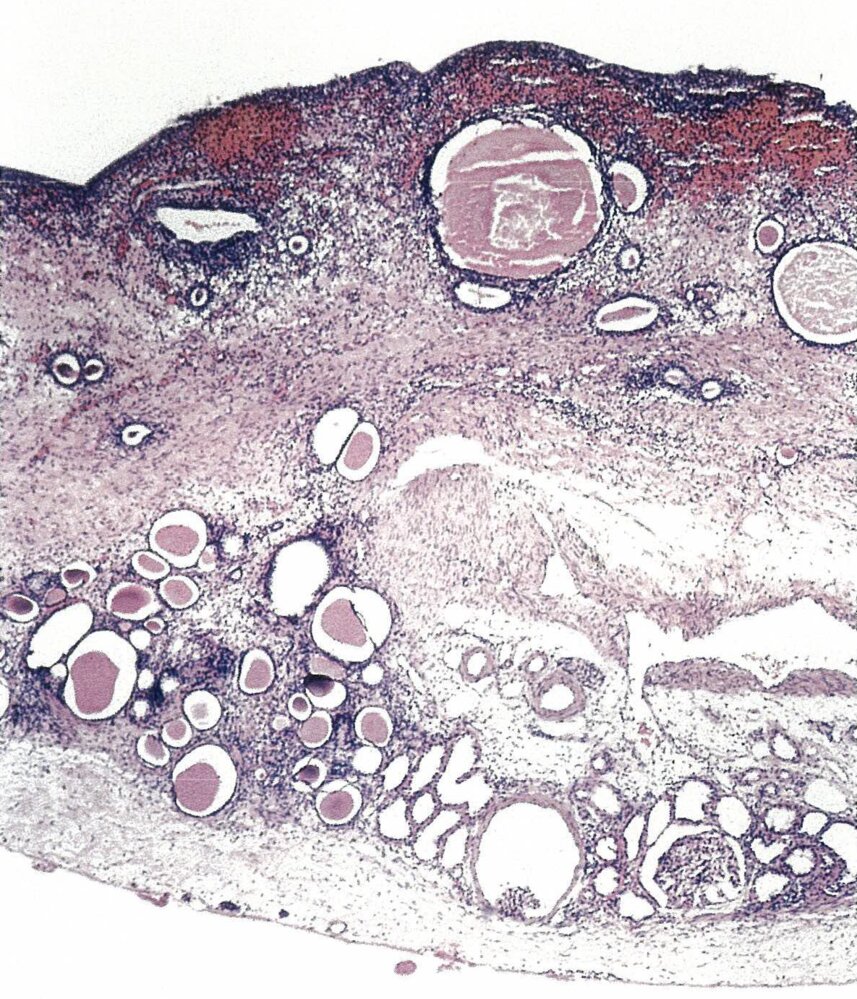
Photomicrophraph (H&E stain, 150x magnification) of an autopsy kidney specimen of a 60-year-old patient with prostate and bladder carcinoma
A chronic interstitial infilitrate (highlighted red) is seen in scarred fibrous tissue (highlighted green) replacing most of the renal parenchyma. Tubules are partly atrophic with flattened epithelia (arrowheads) or cystically dillated with colloid-like luminal material (so-called tubular “thyroidization” because of it's resemblance of thyroid follicles). A single normal glomerulum (marked "G") can be seen. The overall reduced thickness of the parenchyma speaks for a dilated renal pelvis and an obstructive problem (e. g. by tumor or after radiation).
These findings are consistent with chronic pyelonephritis.
Source: © IMPP
Differential diagnoses
See also “Differential diagnoses of acute abdomen” and “Differential diagnoses of acute back pain.”
-
Other kidney and urinary tract disorders
- Lower UTIs
- Renal colic
- Renal vein thrombosis
- Renal infarct
-
Other intraabdominal, retroperitoneal, and pelvic disorders
- Psoas abscess
- Splenic infarct or abscess
- Retroperitoneal hematoma or infection
- Acute cholecystitis
- Appendicitis
- Diverticulitis
- Pelvic inflammatory disease
- Endometriosis
-
Disorders outside the abdomen, pelvis, and retroperitoneum
- Musculoskeletal disorders (e.g., spinal, paraspinal)
- Pleural empyema
- Pulmonary infarct
- Shingles
The differential diagnoses listed here are not exhaustive.
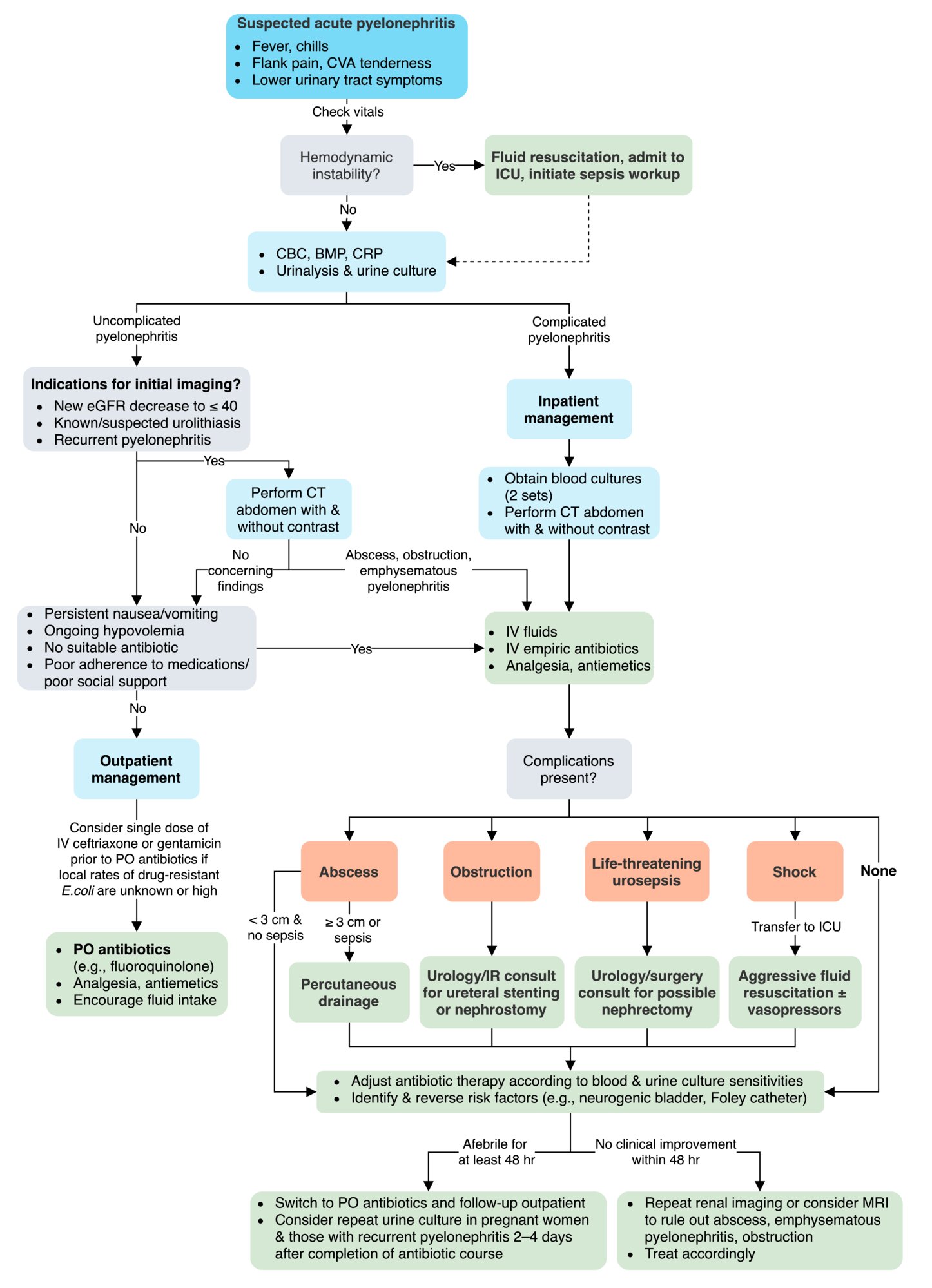
Treatment
Antibiotic therapy, source control, and supportive care are the mainstays of treatment of pyelonephritis. The choice of empiric antibiotic regimen should be guided by the risk of infection with resistant organisms (i.e., complicated vs. uncomplicated pyelonephritis) and antibiotics should be tailored as soon as culture results become available. Consider specialist consultation in cases of complicated pyelonephritis, especially if urinary tract obstruction is suspected.

Uncomplicated pyelonephritis [5][7][24]
-
Empiric antibiotic therapy for uncomplicated pyelonephritis [24]
- Most patients can be treated with an oral fluoroquinolone (e.g., ciprofloxacin; , levofloxacin ) for 5–7 days [1][24][25]
- Alternatives
- Trimethoprim/sulfamethoxazole , for 10–14 days (only recommended if susceptibility is known) [1]
- Amoxicillin/clavulanate for 10–14 days [24]
- Cefpodoxime for 10–14 days [24]
- Consider a single dose of a broad-spectrum parenteral antibiotic prior to the administration of oral antibiotics, especially when the local rates of drug-resistant E. coli are unknown or known to be > 10%. [1][24]
- Ceftriaxone
- OR gentamicin [24][25]
-
Supportive care
- Encourage the patient to drink adequate amounts of fluids.
- Consider an IV fluid bolus in patients with dehydration. [1]
- Analgesia for pain (see “Pain management”) [1]
- Antiemetics in patients with nausea and vomiting (e.g., ondansetron ) [1]
-
Additional considerations
- Outpatient treatment is generally appropriate.
-
If there is no response within 48 hours of starting empiric antibiotic therapy:
- Consider imaging to evaluate for urinary tract obstruction or formation of renal abscess (see “Diagnostics”).
- Check urine culture results and adjust treatment accordingly. [1]
- Repeat urine culture (i.e., “test for cure”) is not routinely indicated. [5]
A single dose of a broad-spectrum parenteral antibiotic prior to the administration of oral antibiotics is recommended when local rates of E. coli resistance are > 10% (or unknown) or if trimethoprim/sulfamethoxazole is used empirically.
Complicated pyelonephritis [5][7][24]
Patients with complicated acute pyelonephritis should be admitted to the hospital and started on parenteral empiric antibiotic therapy as soon as possible. [1]
- The choice of empiric antibiotic therapy should be decided based on:
- Clinical severity (i.e., presence of sepsis)
- The presence of risk factors for infection with multidrug-resistant bacteria [1]
- Age ≥ 65 years
- Recent stay in hospital or long-term care facility
- Recent antibiotic use
- Indwelling urinary tract devices
- Known abnormalities of the urological tract or urinary tract obstruction
- Previous resistant infection
- Recent travel to an area with high antibiotic resistance (e.g., Asia, Mexico)
| Empiric antibiotic therapy for complicated pyelonephritis [1][24][26] | ||
|---|---|---|
| Patient characteristics | Antibiotic regimens to consider | |
| Not severely ill and no risk factors for multidrug-resistant bacterial infection |
|
|
| Severely ill (i.e., septic) and/or with risk factor(s) for multidrug-resistant gram-negative bacterial infection |
|
|
| Enterococcus or MRSA suspected |
|
|
Fluoroquinolone monotherapy should be avoided in severely ill patients with complicated pyelonephritis due to the high prevalence of fluoroquinolone-resistant pathogens!
-
Supportive care
- Analgesics as needed (see “Pain management”)
- Antiemetics as needed
-
Additional considerations
- Aggressive IV resuscitation for patients with sepsis (see “IV fluid therapy”)
- Source control: Consider imaging to identify urinary obstruction (see “Diagnostics” above).
- Specialist consultations
- Urology consultation if renal abscess or obstruction is present/suspected
- Nephrology consultation in patients with AKI, electrolyte derangements, need for hemodialysis
- Critical care consultation if septic shock is present
-
Management of complications
-
Abscess
- Abscess < 3 cm and no signs of sepsis: no drainage necessary
- Abscess ≥ 3 cm and/or signs of sepsis present: percutaneous drainage of abscess
- Life-threatening urosepsis: urology/surgery consultation for possible nephrectomy [27][28]
- Shock: aggressive fluid resuscitation, vasopressors (see “Shock”)
- Urinary tract obstruction: emergent urology and IR consultation for ureteral stenting or percutaneous nephrostomy
-
Abscess
-
Subsequent management
- Duration of antibiotic therapy: 10–14 days [24]
- Antibiotic therapy should be adjusted once blood and urine culture sensitivity reports are available.
- Consider repeat urine culture in pregnant women and those with recurrent pyelonephritis 2–4 days after completion of the antibiotic course. [5][29]
- Identify and treat the underlying cause.
Patients with concurrent urinary tract obstruction are at very high risk of clinical deterioration and require immediate intervention to remove the obstruction.
Admission criteria [1]
Consider inpatient management if any of the following are present:
- Complicated pyelonephritis
- Potential difficulties in following outpatient care and follow-up instructions
- No suitable oral antibiotic
- Ongoing hypovolemia
- Persistent nausea and vomiting
© AMBOSS
Acute management checklist
Uncomplicated pyelonephritis [5][7][24][25]
- Check urinalysis and order urine culture with susceptibilities (ideally before administering antibiotics).
- Consider a single initial dose of broad-spectrum empiric IV antibiotics.
- Start empiric oral antibiotic therapy.
- Encourage oral hydration.
- Consider inpatient admission if there is concern for a complicated course.
- Follow up on urine culture results and narrow antibiotic regimen accordingly.
Complicated pyelonephritis [5][7][24]
- Obtain blood cultures (2 sets) and urine culture with susceptibilities (ideally before administering antibiotics).
- Start parenteral empiric antibiotic therapy for complicated pyelonephritis.
- Establish source control: Check imaging to evaluate for an abscess and/or obstruction.
- Identify and treat sepsis.
- IV fluid therapy
- Identify and treat any urinary tract obstruction.
- Treat the underlying cause.
- Follow up on urine culture results and narrow antibiotic regimen accordingly.
- Inpatient admission
Complications
- Urosepsis, septic shock
- Perinephric abscess; , renal abscess
- Renal papillary necrosis
-
Emphysematous pyelonephritis [18]
- Rare form of pyelonephritis characterized by gas formation within and around the kidney
- Most common in patients with poorly controlled diabetes or immunodeficiency
- Typically caused by E. coli or K. pneumoniae
- Treatment includes IV antibiotics, percutaneous drainage, and, in some cases, nephrectomy.
- Recurrent bacterial pyelonephritis
- If recurrence is caused by the same organism despite adequate treatment, then prolong the course of antibiotics for 6 weeks.
- If a new pathogen is identified, change antibiotics accordingly and treat for 2 weeks.
- Atrophic kidneys
- End-stage renal disease (ESRD): if both kidneys are affected, the patient has a single kidney, or the other kidney has been damaged by a different pathology
Rule out urosepsis in elderly patients with altered mental status!
We list the most important complications. The selection is not exhaustive.
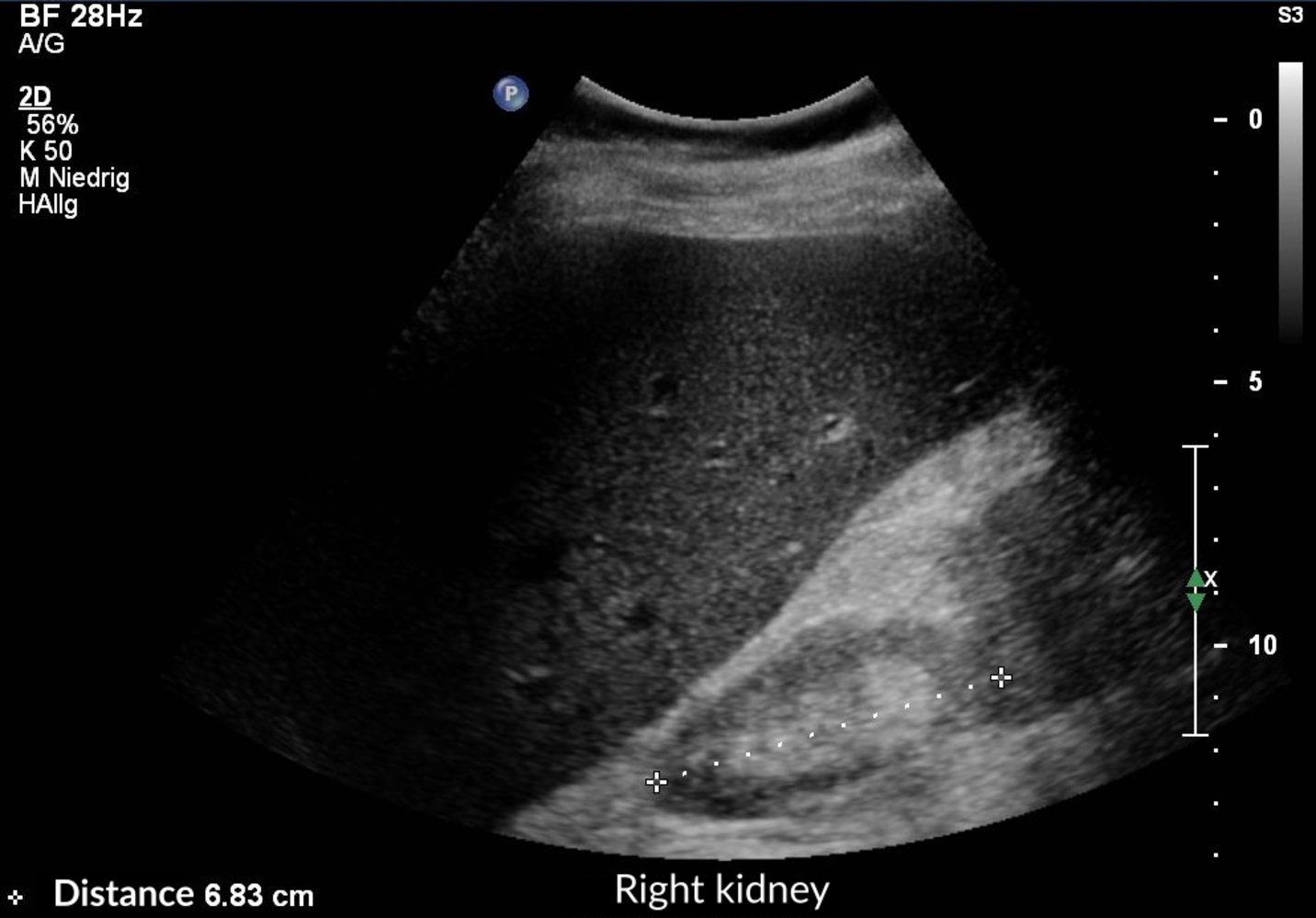
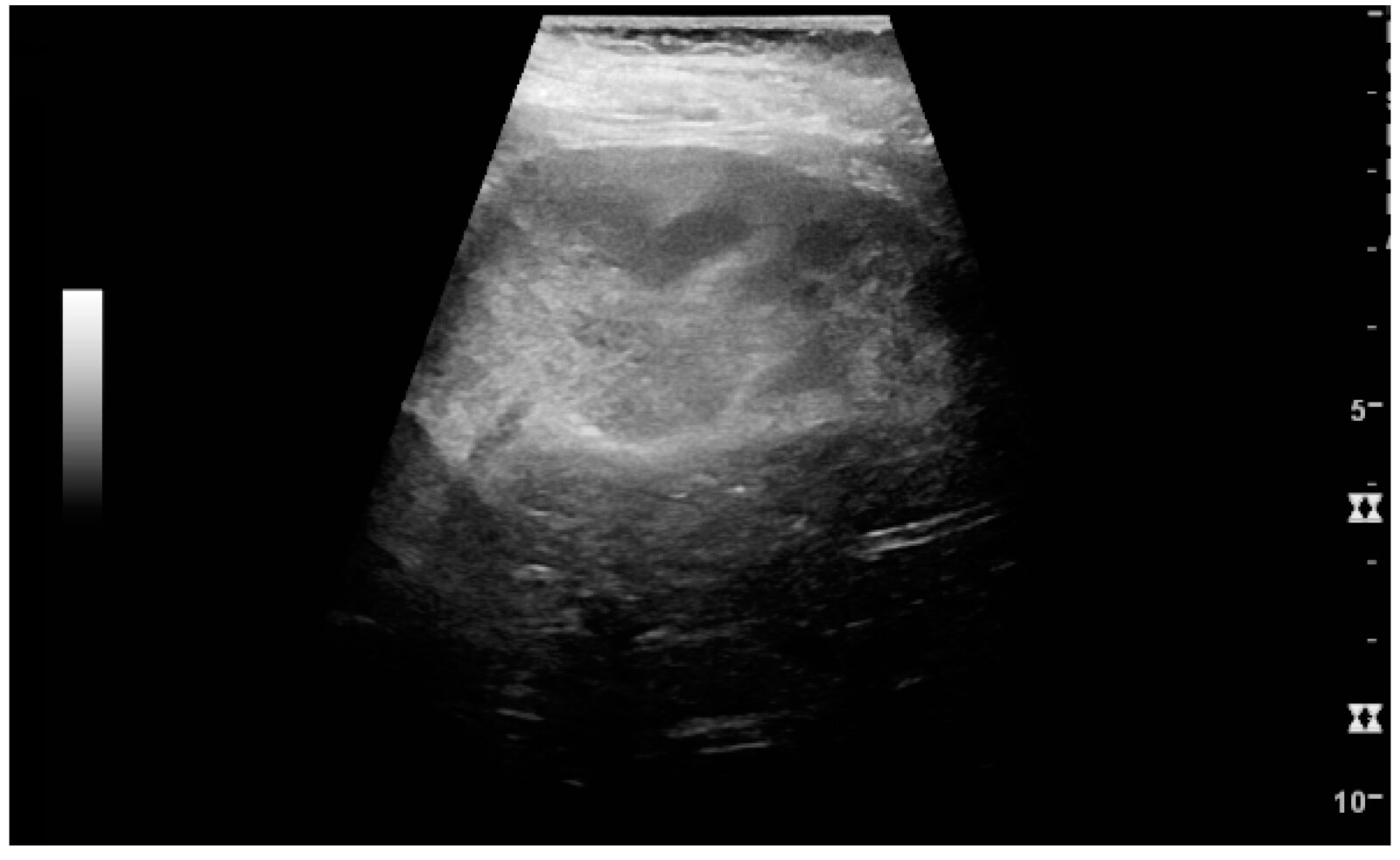
Ultrasound of the right kidney (transhepatic longitudinal view): very small sized kidney (green overlay) with a diameter of approx. 7 cm. The normal kidney size of an adult is approximately 10–12 cm (L = liver).
Our great thanks to Dr. Kissig (Center for Diagnostic and Interventional Radiology, Hedwigshöhe, St. Hedwig, Berlin, and St. Josefs Hospital, Potsdam) for kindly providing this image.
Special patient groups
Pyelonephritis in pregnancy [1][24]
-
Epidemiology
- The risk of pyelonephritis is increased during pregnancy.
- As many as one-third of pregnant women with asymptomatic bacteriuria will progress to develop pyelonephritis (if left untreated).
- One of the most common complications of pregnancy, with potentially severe consequences for both mother and fetus [1]
- Diagnosis: See “Diagnostics” above; use ultrasound or MRI for imaging. [30]
-
Treatment [1][24]
-
Hospitalization is recommended; definitive indications for hospitalization are: [31]
- Signs of sepsis
- Dehydration (e.g., due to vomiting)
- Contractions
-
A third- or fourth-generation cephalosporin for 7–10 days, such as:
- Cefotaxime
- Ceftazidime
- Cefepime
- In severe pyelonephritis (immunocompromised patients or poor urine output), consider one of the following for 10–14 days:
- Piperacillin/tazobactam
- Meropenem
- Ticarcillin
- Parenteral broad-spectrum antibiotics are recommended at least until the patient is afebrile, after which transition to oral antibiotics (e.g., penicillins, cephalosporins) is possible. [31]
- See “Antibiotics during pregnancy” for additional drugs and dosages.
-
Hospitalization is recommended; definitive indications for hospitalization are: [31]
- Secondary prevention: Monthly urine culture or prophylactic nitrofurantoin until 4–6 weeks postpartum is recommended, as the recurrence rate of pyelonephritis in pregnancy is 25%. [32]
All asymptomatic cases of bacteriuria during pregnancy must be treated to prevent the development of pyelonephritis.
Avoid fluoroquinolones, trimethoprim/sulfamethoxazole, and aminoglycosides in pregnant women!
Acute pyelonephritis in children
See "Urinary tract infection in children and adolescents."
Chronic pyelonephritis
- Description: a consequence of recurrent or persistent acute pyelonephritis
-
Predisposing factors
- Vesicoureteric reflux
- Urinary tract obstruction (e.g., nephrolithiasis, neurogenic bladder)
-
Clinical features
- Nonspecific (mild fever, anorexia, malaise)
- Abdominal or flank pain
-
Diagnostics
- Urinalysis: pyuria, proteinuria, WBC casts
- Imaging (ultrasound, intravenous urogram): corticomedullary scarring (mainly upper pole), blunt/clubbed renal calyces
- Biopsy: thyroidization of the kidney (see ''Pathology'')
-
Treatment
- Treat the underlying cause.
- Antibiotics
External Resources
References
- Johnson JR, Russo TA. "Acute Pyelonephritis in Adults". N Engl J Med. 378(1). :48-59. (2018)
- Ferri FF. "Ferri's Clinical Advisor 2018 E-Book: 5 Books in 1 (Ferri's Medical Solutions)". Elsevier. :1779. (2017). ISBN: 9780323280495
- Lee JR, Bang H, Dadhania D, et al. "Independent Risk Factors for Urinary Tract Infection and for Subsequent Bacteremia or Acute Cellular Rejection". Transplantation. 96(8). :732-738. (2013)
- Ariza-Heredia EJ, Beam EN, Lesnick TG, et al. "Impact of urinary tract infection on allograft function after kidney transplantation". Clin Transplant. 28(6). :683-690. (2014)
- Ramakrishnan K, Scheid DC. "Diagnosis and management of acute pyelonephritis in adults". Am Fam Physician. 71(5). :933-942. (2005)
- Simerville JA, Maxted WC, Pahira JJ. "Urinalysis: a comprehensive review". Am Fam Physician. 71(6). :1153-62. (2005)
- Colgan R, Williams M. "Diagnosis and Treatment of Acute Pyelonephritis in Women". Am Fam Physician. (2011)
- Hesse, Albrecht. "Urinary Stones". Karger Medical and Scientific Publishers. (2009). ISBN: 9783805591492
- Van Nieuwkoop C, Hoppe BPC, Bonten TN, et al. "Predicting the Need for Radiologic Imaging in Adults with Febrile Urinary Tract Infection". Clin Infect Dis. 51(11). :1266-1272. (2010)
- Jameson JL, Fauci AS, Kasper DL, et al. "Harrison's Principles of Internal Medicine, Twentieth Edition (Vol.1 & Vol.2)". McGraw-Hill Education / Medical. (2018). ISBN: 9781259644030
- Colgan, Williams. "Diagnosis and Treatment of Acute Uncomplicated Cystitis". American Family Physician. (2011)
- Nikolaidis P, Dogra VS, Goldfarb S, et al. "ACR Appropriateness Criteria® Acute Pyelonephritis". J Am Coll Radiol.. 15(11). :S232-S239. (2018)
- Williams M. "Comprehensive Hospital Medicine". Elsevier Health Sciences. (2007). ISBN: 9781416002239
- Colgan R, Williams M, Johnson JR. "Diagnosis and treatment of acute pyelonephritis in women.". Am Fam Physician. 84(5). :519-526. (2011)
- Walls R, Hockberger R, Gausche-Hill M. "Rosen's Emergency Medicine". Elsevier Health Sciences. (2018). ISBN: 9780323354790
- Craig WD, Wagner BJ, Travis MD. "Pyelonephritis: Radiologic-Pathologic Review". Radiographics. 28(1). :255-276. (2008)
- Ubee SS, McGlynn L, Fordham M. "Emphysematous pyelonephritis.". BJU Int. 107(9). :1474-8. (2011)
- Das CJ. "Multimodality imaging of renal inflammatory lesions". World Journal of Radiology. 6(11). :865. (2014)
- Amery A, Fagard R, Lijnen P, Staessen J. "Hypertensive Cardiovascular Disease: Pathophysiology and Treatment". Springer Science & Business Media. (2012). ISBN: 9789400974760
- Lee J, Woo BW, Kim HS. "Prognostic Factors of Renal Scarring on Follow-up DMSA Scan in Children with Acute Pyelonephritis". Child Kidney Dis. 20(2). :74-78. (2016)
- Dunnick R, Sandler C, Newhouse J. "Textbook of Uroradiology". Lippincott Williams & Wilkins. (2012). ISBN: 9781451171617
- Gupta K, Hooton TM, Naber KG, et al. "International Clinical Practice Guidelines for the Treatment of Acute Uncomplicated Cystitis and Pyelonephritis in Women: A 2010 Update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases". Clin Infect Dis. 52(5). :e103-e120. (2011)
- Murphy JE, Lee MW-L. "PSAP 2018 Book 1: Infectious Diseases". American College of Clinical Pharmacy. (2018). ISBN: 9781939862600
- Gupta K, Hooton TM, Naber KG, et al. "Executive Summary: International Clinical Practice Guidelines for the Treatment of Acute Uncomplicated Cystitis and Pyelonephritis in Women: A 2010 Update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases". Clin Infect Dis. 52(5). :561-564. (2011)
- "EAU Guidelines on Urological Infections- Limited update 2019". https://uroweb.org/wp-content/uploads/EAU-Guidelines-on-Urological-infections-2019.pdf. [2019-03-01]
- Berger I, Wildhofen S, Lee A, et al. "Emergency nephrectomy due to severe urosepsis: a retrospective, multicentre analysis of 65 cases". BJU Int. 104(3). :386-390. (2009)
- Kalra O, Raizada A. "Approach to a Patient with Urosepsis.". J Glob Infect Dis. 1(1). :57-63. (2009)
- Matuszkiewicz-Rowińska J, Małyszko J, Wieliczko M. "State of the art paper Urinary tract infections in pregnancy: old and new unresolved diagnostic and therapeutic problems". Arch Med Sci. 1. :67-77. (2015)
- Smith A, Nikolaidis P, Khatri G, et al. "ACR Appropriateness Criteria® Acute Pyelonephritis: 2022 Update". J Am Coll Radiol. 19(11). :S224-S239. (2022)
- Delzell JE Jr, Lefevre ML. "Urinary tract infections during pregnancy". Am Fam Physician. 61(3). :713-21. (2000)
- Abraham G, Reddy YNV, George G. "Diagnosis of acute pyelonephritis with recent trends in management". Nephrol Dial Transplant. 27(9). :3391-3394. (2012)
- Cohen J, Powderly WG, Opal SM. "Infectious Diseases". Elsevier Health Sciences. (2016). ISBN: 9780702063381
- Fulop T. "Acute Pyelonephritis". WebMD. http://emedicine.medscape.com/article/245559-workup#c1. [2016-09-08]
- Lohr JW. "Chronic Pyelonephritis". WebMD. https://emedicine.medscape.com/article/245464-overview. [2015-12-06]
- Colgan R, Williams M, Johnson JR. "Diagnosis and treatment of acute pyelonephritis in women.". Am Fam Physician. 84(5). :519-526. (2011)
- Munar MY, Singh H. "Drug dosing adjustments in patients with chronic kidney disease.". Am Fam Physician. 75(10). :1487-1496. (2007)
- "American College of Radiology ACR Appropriateness Criteria® Acute Pyelonephritis". https://acsearch.acr.org/docs/69489/Narrative/. [2018-01-01]