Summary
Rabies is a neurotropic virus transmitted through the bite of an infected animal. The virus enters via the animal saliva, traveling along peripheral nerves to the central nervous system (CNS). The onset of nonspecific flu-like symptoms begins after an incubation period of 4–12 weeks, progressing to acute rabies encephalitis. Clinical features include fever, hydrophobia, hypersalivation, stupor, and mania, followed by coma and death resulting from respiratory and circulatory collapse. Paralytic rabies, a less common form, manifests with ascending paralysis that resembles Guillain-Barré syndrome. Rabies is preventable with rabies postexposure prophylaxis (PEP) and proper wound care but is almost always fatal once symptoms appear. Rabies preexposure prophylaxis (PrEP) is recommended for those at increased risk of exposure (e.g., veterinarians and travelers to endemic areas).
Epidemiology
- Found in animal reservoirs in most countries throughout the world
- Considerable divide between developed and developing countries in terms of human deaths due to rabies
- Incidence worldwide: ∼ 60,000 people die of rabies each year. [1]
- Incidence in the US: Three people on average die of rabies each year.

Epidemiological data refers to the US, unless otherwise specified.
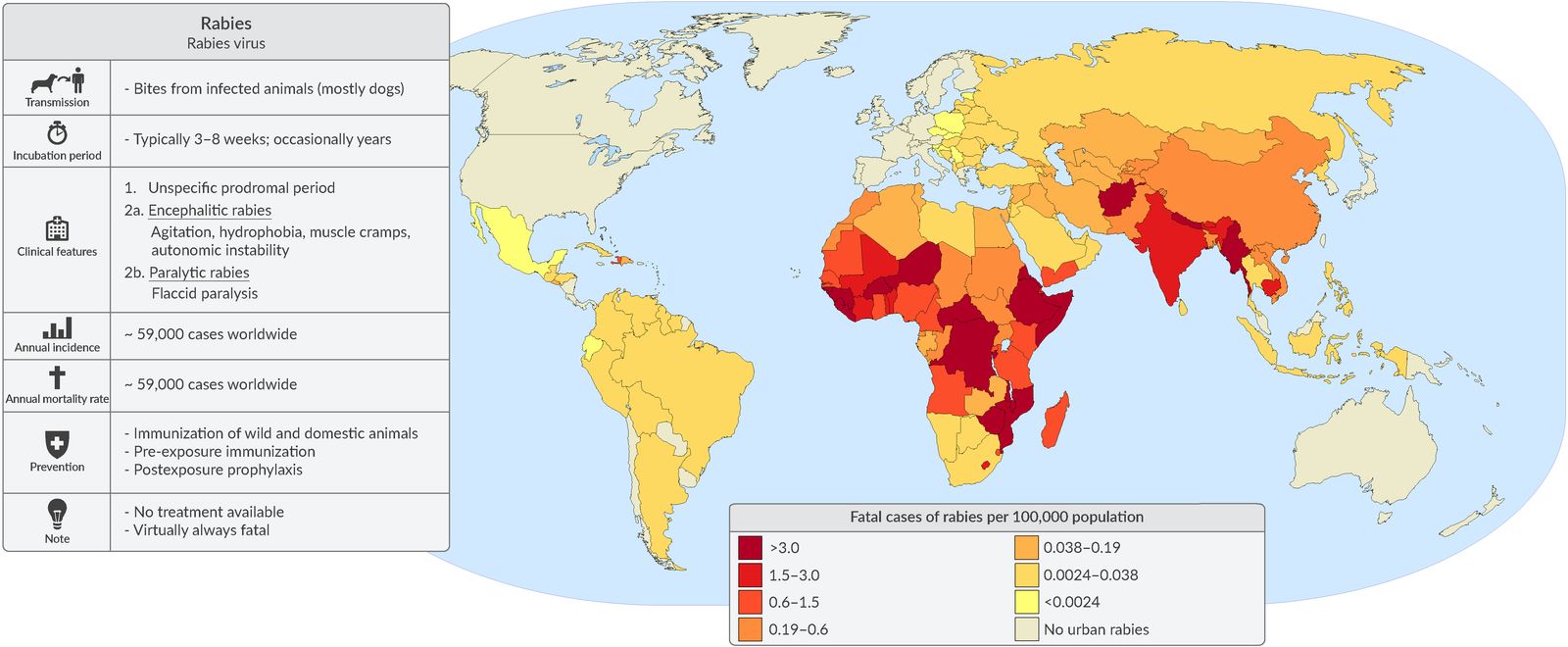
The high mortality rate of rabies in developing countries is attributed to a lack of vaccination programs for animals and postexposure prophylaxis being unaffordable or unavailable.
© AMBOSS. Map based on: Hampson et al.: Estimating the Global Burden of Endemic Canine Rabies. In: PLOS Neglected Tropical Diseases. 9, 2015, doi:10.1371/journal.pntd.0003709.
Etiology
-
Pathogen
- Rabies is caused by several different members of the Rhabdoviridae family.
- Rhabdoviruses are rod or bullet shaped
- Genus: Lyssavirus
- ssRNA
-
Transmission [2]
- Most common animal reservoir worldwide: dogs (≥ 90%)
- Most common animal reservoirs in the US: bats, raccoons, skunks, and foxes
- Spread through saliva of rabid animal after bite injury
- Via aerosols (e.g., bat caves); rare


This dog is salivating and there is froth at its mouth because infection with the rabies virus causes difficulty swallowing. Other symptoms in animals include abnormal behavior, nervousness, weight loss, paralysis, and epileptic seizures.
Source: "ID#: 2626", CDC, Centers for Disease Control and Prevention licensed under Public Domain
Pathophysiology
-
Rabies virus binds the ACh receptor of peripheral nerves in the bite wound → migrates retrogradely along the axonal microtubules (using motor protein dynein) → enters the CNS → infects the brain [3]
- Diencephalon, hippocampus, and brainstem are involved first
- Causes acute, progressive, and fatal encephalitis → encephalitic rabies
- Causes ascending flaccid paralysis → paralytic rabies
Clinical features
General
- Incubation period: 4–12 weeks average [1]
-
Prodromal symptoms
- Flu-like symptoms (e.g., fever, malaise)
- Pain, paresthesia, and pruritus near the bite site
Encephalitic rabies (∼ 80% of cases) [2]
- Hydrophobia: Rabies patients experience involuntary, painful pharyngeal muscle spasms when trying to drink; later on in the disease, the sight of water alone may provoke nausea or vomiting.
-
CNS symptoms
- Anxiety, agitation, and combativeness alternating with calm periods
- Confusion and hallucinations
- Photophobia
- Fasciculations
- Seizures
- ↑ Muscle tone and reflexes with nuchal rigidity
- Autonomic symptoms (e.g., hypersalivation, hyperhidrosis)
- Coma and death within days to weeks of the development of neurological symptoms
Paralytic rabies (∼ 20% of cases) [2]
- Flaccid paralysis, gradually ascending and spreading from bite wound [4]
- Paraplegia and loss of sphincter tone
- Respiratory failure and death
The pathognomonic feature of rabies is hydrophobia due to pharyngeal muscle spasm. This may present along with agitation, strange behavior, mental status changes, and possibly foaming at the mouth.
Diagnosis
Suspect rabies in patients with potential exposure and clinical features of rabies.
Antemortem diagnosis [2]
Several tests using multiple specimens must be performed because virus and antibody detection vary throughout disease. Identifying rabies virus antigen or nucleic acid confirms the diagnosis. [2]
- Required specimens: serum, saliva, CSF, and skin biopsy [2]
-
Laboratory studies [2]
- RT-PCR to detect rabies RNA
- Cell culture to isolate rabies virus
- Direct fluorescent antibody staining for viral antigen in skin biopsy
-
Indirect fluorescent antibody testing
- Serum antibodies detected in individuals who are not immunized and did not receive rabies PEP indicate a rabies infection
- Antibodies in the CSF regardless of the immunization history indicate a rabies infection
- Virus neutralization test
- Rabies CSF analysis: lymphocytic pleocytosis, ↑ protein, normal or ↑ glucose [5][6]
If a case of rabies is suspected in the US, contact the state health department and CDC to determine if testing is necessary and what specimens are required.
Postmortem diagnosis
-
Postmortem brain tissue autopsy
- Immunofluorescent staining of viral antigen in infected CNS tissue
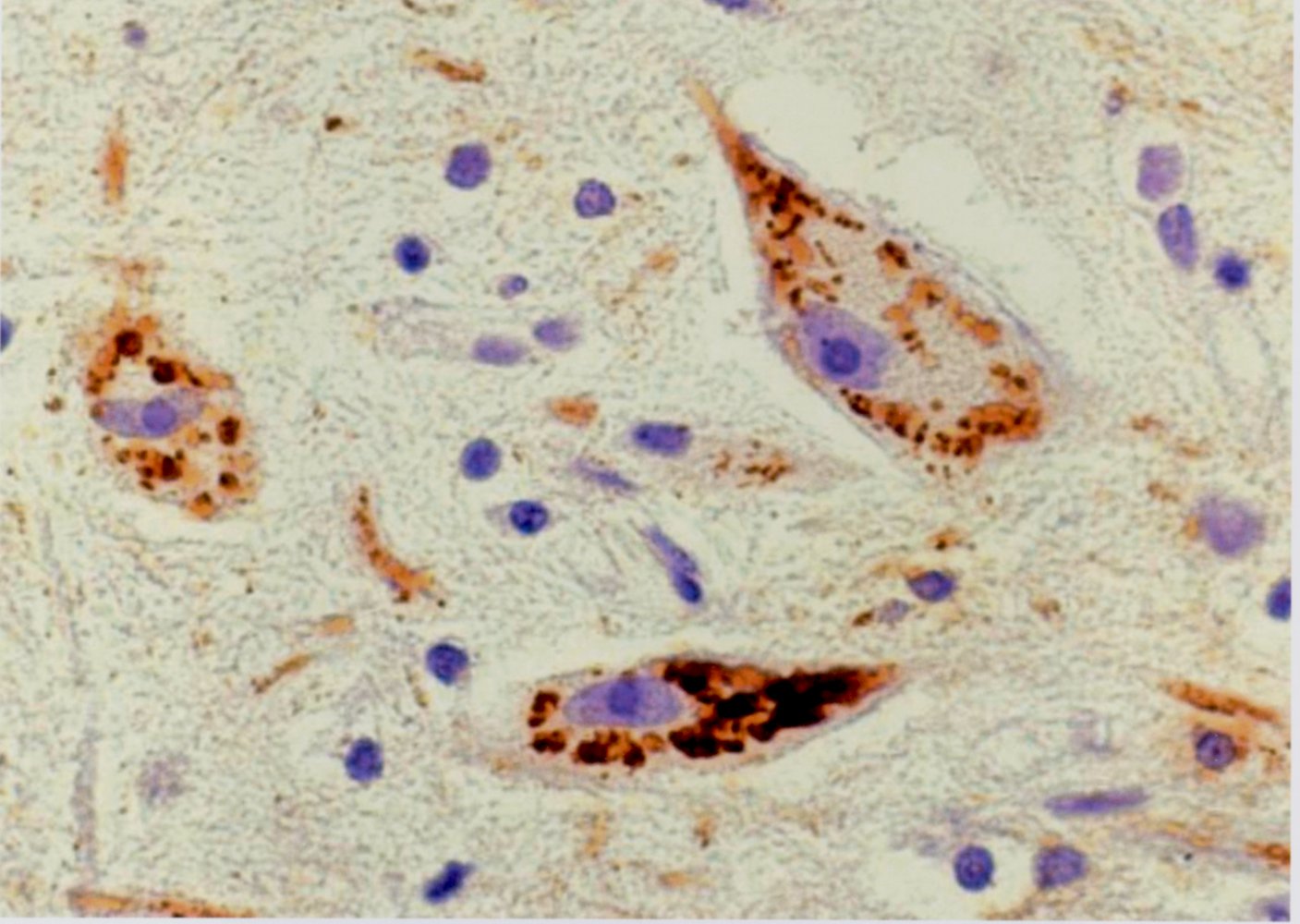
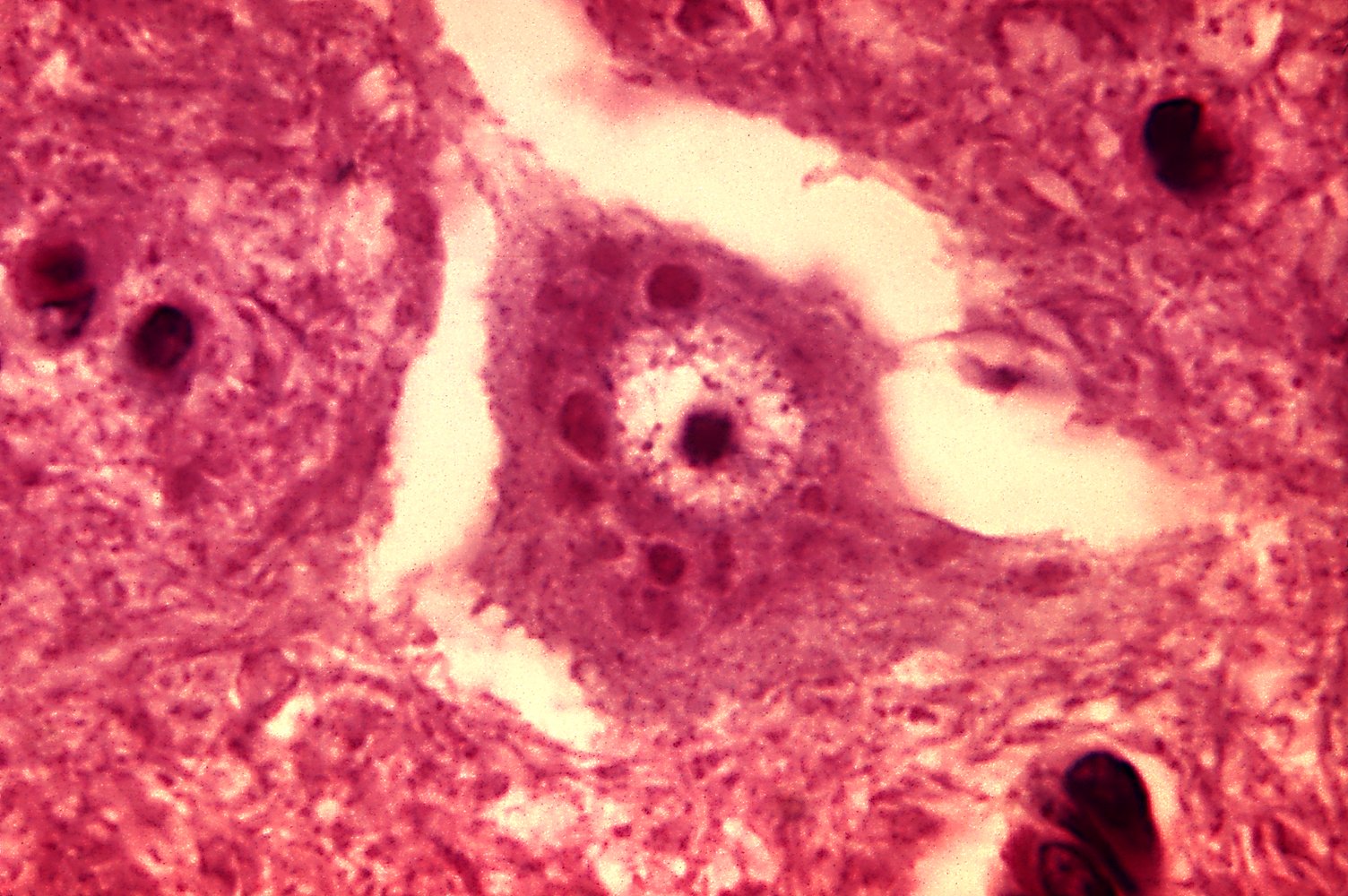
- Histopathological findings: Negri bodies (eosinophilic cytoplasmic inclusion bodies typically found in the cerebellum and hippocampus)



Photomicrograph of autopsy specimen of brain tissue (H&E stain)
Negri bodies (examples indicated by green arrows) are eosinophilic intracytoplasmic inclusion bodies present within the cell bodies and axons of neurons infected by the rabies virus. Although the presence of Negri bodies is pathognomonic of rabies, their absence does not rule out infection.
Source: © IMPP
Photomicrograph of brain tissue (H&E stain; high magnification)
A pyramidal cell (green overlay) is visible in the center of the image. The distinct eosinophilic intracytoplasmic inclusions within the pyramidal cells are Negri bodies (examples indicated by black arrowheads and white dashed outlines).
Negri bodies are most commonly found within the pyramidal cells of hippocampus and the Purkinje cells of patients infected by the rabies virus. Although the presence of Negri bodies is pathognomonic of rabies, their absence does not rule out infection.
Source: "ID#: 3377", CDC/ Dr. Daniel P. Perl, Centers for Disease Control and Prevention licensed under Public Domain Further notes: Public Health Image Library (PHIL); ID: 3377
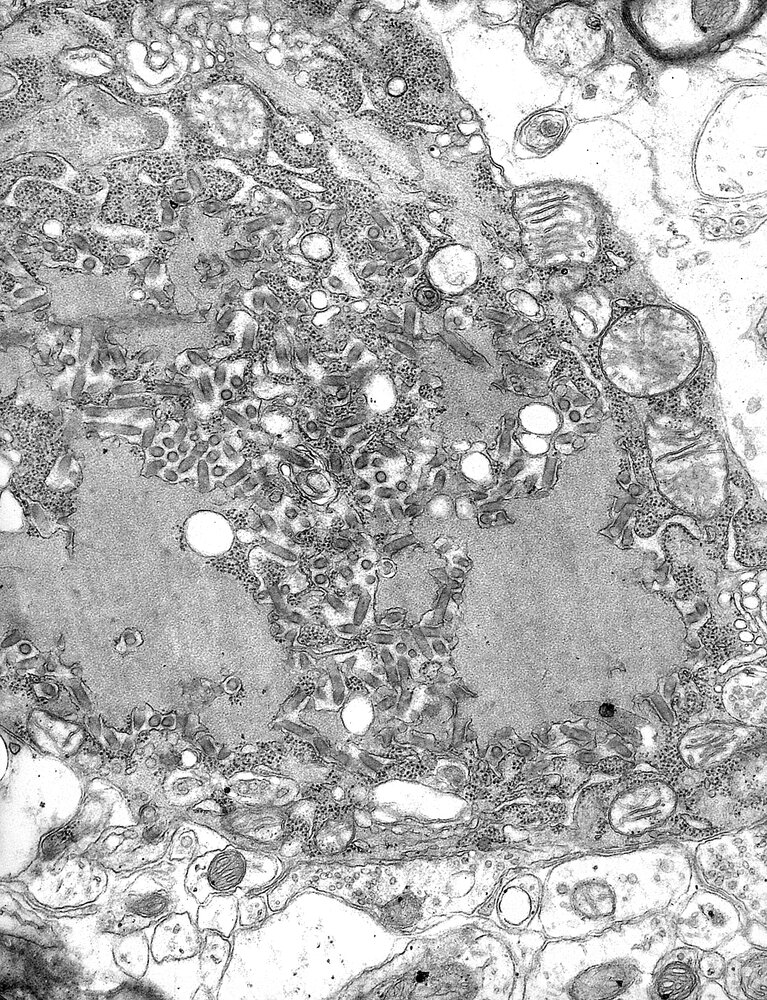
Electron micrograph of cell with rabies virions
The rabies virions can be identified by their bullet-shaped appearance (examples indicated by green overlay). They can bud from Negri bodies, which are pathognomonic inclusions within the cell (example indicated by red hatched overlay).
This image is an adaptation. Source of original image: Centers for Disease Control and Prevention. Original title: “ID#1876”. Created by: CDC/ Dr. Fred Murphy. Licensed under Public Domain. Modifications to original image: Overlays added.
Treatment
For management of individuals with potential rabies exposure, see “Rabies PEP.”
- Symptomatic rabies is almost universally fatal. [2]
- Patients are managed with palliative care (e.g., pain management, sedation).
Prevention
- Avoiding animal bites is the most effective way to prevent rabies infection. [2]
- Consider rabies PrEP for individuals at increased risk of rabies exposure.
- For potential rabies exposure, consider rabies PEP based on rabies risk assessment.
Rabies preexposure prophylaxis
-
Indications: individuals at increased risk of rabies exposure, e.g., [6][7]
- Occupational exposures (e.g., veterinarians)
- Recreational exposures (e.g., spelunkers)
- Travelers to endemic areas
- Immunization schedule: See “Vaccines before travel.”
Rabies PEP is still required for patients exposed to rabies who previously received rabies PrEP. [2]
Rabies postexposure prophylaxis
Recommendations in this article are consistent with the CDC and ACIP guidelines for rabies PEP. [8][9] Consider following the WHO guidelines for rabies PEP in resource-limited settings. [10]
Approach [6]
- Manage bite wounds (e.g., with irrigation, debridement).
- Perform a rabies risk assessment based on the source and nature of exposure.
- Administer rabies PEP if required.
- Follow local protocols for animal observation, testing, and reporting requirements.
- Inform the patient when to return for subsequent rabies vaccinations.
Rabies risk assessment [6][8]
Wild animal bites
-
High-risk animals (e.g., bats, raccoons, skunks, foxes, other carnivores) and monkeys
- Animal is not present: Administer rabies PEP.
-
Animal is present: Contact the local health department for expedited animal rabies testing.
- Positive: Administer rabies PEP.
- Negative: No rabies PEP is necessary.
- If results cannot be obtained expeditiously, initiate rabies PEP and discontinue if negative.
- Low-risk animals (e.g., rodents, lagomorphs): No rabies PEP is necessary.
Any suspicion of a bat bite (e.g., waking up with a bat in the room) warrants the administration of rabies PEP, even if there is no evidence of a bite. [2]
Domestic animal bites
-
Dogs, cats, ferrets
- Animal is not present: Administer rabies PEP.
-
Animal is present: Confine and observe the animal for 10 days.
-
Animal becomes symptomatic
- Administer rabies PEP.
- Contact the local health department for expedited animal rabies testing.
- If animal rabies testing is negative, discontinue rabies PEP.
- Animal remains asymptomatic: No rabies PEP is necessary.
-
Animal becomes symptomatic
- Other domestic animals: Consult the local health department.
Rabies PEP regimens [2]
Unvaccinated patients [6][8][9]
-
Rabies immune globulin (RIG) [2]
- Infiltrate as much RIG as feasible into and around the wound.
- Inject the remaining RIG at a site distant from the site of vaccine administration.
-
PLUS inactivated rabies vaccine [2]
- Administer on days 0, 3, 7, and 14.
- Immunosuppressed patients: Administer an additional dose on day 28.
Unvaccinated patients require passive immunization (i.e., RIG) and active immunization (i.e., rabies vaccine).
Vaccinated patients [6][7]
An individual is considered vaccinated against rabies if they have previously completed rabies PrEP, rabies PEP, or they have partially completed the rabies vaccination series and have positive rabies antibody titers. [2]
- Inactivated rabies vaccine on days 0 and 3 [2]
- RIG is not required.
External Resources
References
- "Rabies Fact Sheet". https://web.archive.org/web/20250417140301/https://www.who.int/en/news-room/fact-sheets/detail/rabies. [2024-06-05]
- "CDC Yellow Book 2024: Rabies". https://web.archive.org/web/20250206222103/https://wwwnc.cdc.gov/travel/yellowbook/2024/infections-diseases/rabies. [2024-05-03]
- Poisson N, Gaudin Y, Jacob Y, et al. "Molecular basis for the interaction between rabies virus phosphoprotein P and the dynein light chain LC8: dissociation of dynein-binding properties and transcriptional functionality of P". J Gen Virol. 82(11). :2691-2696. (2001)
- Mader EC, Maury JS, Santana-gould L, et al. "Human Rabies with Initial Manifestations that Mimic Acute Brachial Neuritis and Guillain-Barré Syndrome". Clin Med Insights Case Rep. 5. :49-55. (2012)
- Petersen B, Rupprecht C. "Non-Flavivirus Encephalitis". InTechOpen. (2011)
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904
- Manning SE, Rupprecht CE, Fishbein D, et al. "Human rabies prevention--United States, 2008: recommendations of the Advisory Committee on Immunization Practices.". MMWR Recomm Rep. 57(RR-3). :1-28. (2008)
- "Use of a Reduced (4-Dose) Vaccine Schedule for Postexposure Prophylaxis to Prevent Human Rabies: Recommendations of the Advisory Committee on Immunization Practices". https://web.archive.org/web/20241217125753/https://www.cdc.gov/mmwr/preview/mmwrhtml/rr5902a1.htm. [2010-03-09]
- World Health Organization. "WHO Expert Consultation on Rabies: Third Report". World Health Organization. (2018). ISBN: 9789241210218
- "Use of a Modified Preexposure Prophylaxis Vaccination Schedule to Prevent Human Rabies: Recommendations of the Advisory Committee on Immunization Practices". https://web.archive.org/web/20241217090052/https://www.cdc.gov/mmwr/volumes/71/wr/mm7118a2.htm. [2022-05-06]