Quick guide
Diagnostic approach
- Focused clinical evaluation, including comprehensive skin examination
- CBC
- CMP
- See “Diagnostics for rash.”
Routine laboratory studies are seldom required for rashes that appear benign, but are necessary in severely ill patients.
Management checklist
- Don PPE.
- Isolate patients with fever and petechial rash and use droplet precautions.
- For life-threatening rash, establish IV and consult dermatology urgently.
- Supportive care for symptom relief
- Manage the underlying cause.
- Admit patients with vital sign abnormalities, systemic infection or syndrome, electrolyte abnormalities, inability to maintain PO intake.
Red flag features
- Fever
- Severely ill appearance
- Hypotension
- Severe pain
- Mucosal lesions
- Extremes of age
- History of immunosuppression
- Recently initiated medication
Life-threatening causes
- Toxic epidermal necrolysis
- Stevens-Johnson syndrome
- Necrotizing fasciitis
- Meningococcal septicemia
- Toxic shock syndrome
- Disseminated intravascular coagulation
- Anaphylaxis
- Rocky Mountain spotted fever
- DRESS
- Pemphigus vulgaris
Summary
Rash is a common presenting symptom with many different causes. A systematic approach is necessary to identify life-threatening conditions and reach a definitive diagnosis. Initial management steps include evaluating for red flags for a life-threatening rash and characterizing the rash based on its basic morphology, e.g., petechial or purpuric, erythematous, maculopapular, annular, or vesiculobullous. The cause of rash can often be identified clinically, but specific testing may be required based on the presumptive diagnosis. Management is specific to the condition. Although most rashes can affect individuals of any age, some are more common in childhood (e.g., pediatric viral exanthems).
For details on rashes or lesions due to localized infection, see “Overview of skin and soft tissue infections.”
Etiology
Petechial and purpuric rashes
Febrile or severely ill patients
-
Palpable lesion
- Meningococcal septicemia
- Disseminated gonococcal infection
- Acute bacterial endocarditis
- Rocky Mountain spotted fever (RMSF)
- IgA vasculitis
-
Nonpalpable lesion
- Thrombotic thrombocytopenic purpura (TTP)
- Purpura fulminans
- Acute leukemia [3]
Afebrile patients
- Palpable lesion: vasculitis
- Nonpalpable lesion: idiopathic thrombocytopenia (ITP)



Erythematous rashes
Febrile or severely ill patients
-
Positive Nikolsky sign
- Staphylococcal scalded skin syndrome (SSSS)
- Stevens-Johnson syndrome (SJS)
- Toxic epidermal necrolysis (TEN)
-
Negative Nikolsky sign
- Toxic shock syndrome (TSS)
- Kawasaki disease
- Scarlet fever
Afebrile patients
- Positive Nikolsky sign: Toxic epidermal necrolysis
-
Negative Nikolsky sign
- Anaphylaxis
- Histamine fish poisoning
- Medication flushing syndrome, e.g., vancomycin, niacin
- Alcohol flush reaction

Maculopapular rashes
Febrile or severely ill patients
-
Central distribution
- Measles
- Viral exanthem
- Lyme disease
- Drug reaction with eosinophilia and systemic symptoms (DRESS syndrome)
-
Peripheral distribution
- Erythema multiforme
- Meningococcal septicemia
- RMSF
- Syphilis
- Lyme disease
Afebrile patients
-
Central distribution
- Drug reaction
- Pityriasis rosea
-
Peripheral distribution
- Scabies
- Atopic dermatitis
- Bed bugs [4]

Vesiculobullous rashes
See “Overview of blistering skin diseases.”
Febrile or severely ill patients
-
Diffuse distribution
- Varicella
- Disseminated intravascular coagulation (DIC)
- Disseminated gonococcal infection
- Smallpox
-
Localized distribution
- Necrotizing fasciitis
- Hand foot and mouth disease
Afebrile patients
-
Diffuse distribution
- Bullous pemphigoid
- Pemphigus vulgaris
-
Localized distribution
- Herpes zoster
- Contact dermatitis
- Burns
- Dyshidrotic eczema


Annular skin lesions [5]
- Tinea infections
- Nummular dermatitis
- Erythema marginatum
- Erythema multiforme
- Fixed drug eruption
- Granuloma annulare
- Subacute cutaneous lupus erythematosus

Skin plaques and scaling lesions [6]
- Psoriasis
- Seborrheic dermatitis
- Cutaneous lichen planus
- Pityriasis rubra pilaris
- Mycosis fungoides
- Erythroderma
- Tinea infections
- See also “Differential diagnosis of scaling.”

Urticaria [7]
See also “Type I hypersensitivity reaction.”
- Acute (< 6 weeks): viral infection, drug reactions, or food allergens
-
Chronic (≥ 6 weeks)
- Spontaneous urticaria
- Chronic inducible urticaria

Childhood rashes [8][9]
See also “Differential diagnosis of infectious rashes in childhood.”

Common causes
- Roseola infantum
- Pityriasis rosea
- Scarlet fever
- Erythema infectiosum
- Hand foot and mouth disease
- Nonbullous impetigo
- Atopic dermatitis
- Contact dermatitis
- Exanthematous cutaneous reaction [10][11]
- Scabies
- Tinea infections
Less common causes
- Varicella zoster (chickenpox)
- Measles
- Rubella
- Erysipelas
- SSSS
- SJS/TEN
- Acute generalized exanthematous pustulosis
- DRESS
- RMSF

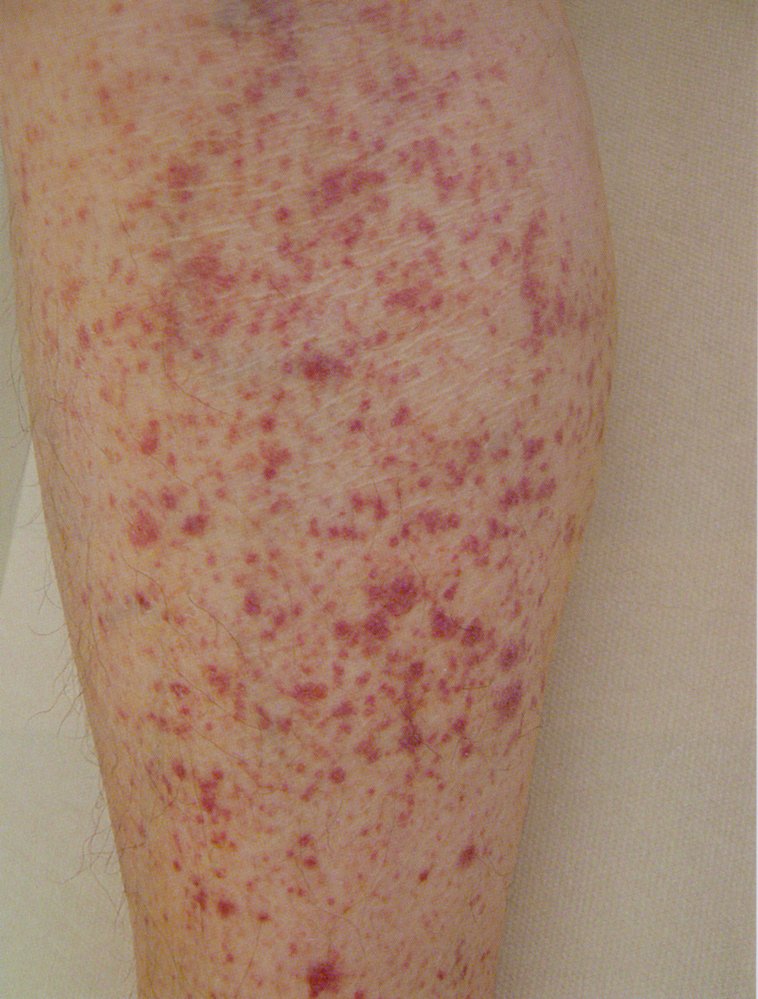
Photograph of the leg of an 18-year-old male patient
Multiple well-defined erythematous skin lesions (purpura) are visible. Some purpura have coalesced to form ecchymoses. Examination revealed the purpura to be palpable and nonblanchable.
The tetrad of purpura, arthritis, abdominal pain, and kidney impairment is typical of IgA vasculitis. Histopathology is required to confirm the diagnosis of IgA vasculitis.
Source: “Purpura” by Hektor, Wikimedia Commons, licensed under CC BY-SA 3.0.

Bluish-red, round or oval maculae (approx. 0.2 mm–1 cm in diameter) are distributed over the right lower leg. There is also an irregularly shaped macula of the same color lateral to the patella (approx. 4 × 2 cm in diameter).
This appearance is characteristic of purpura.
Source: © IMPP
The lower leg displays numerous red spots, each about the size of a pinhead, that do not blanch or disappear when pressed. These are indicative of petechial hemorrhages related to thrombocytopenia.
Source: © IMPP

Erythema of the skin is visible, especially on the patient's cheeks and nose. This symptom usually resolves within minutes after treatment. Vancomycin flushing reaction is not a true allergic reaction, but rather a rate-dependent hypersensitivity reaction. It can be avoided by slow infusion.
Source: “Figure 1, in: Red Man Syndrome with Oral Vancomycin: A Case Report” by Fray Arroyo-Mercado, Aleksandr Khudyakov, Gurasees S. Chawla, Onix Cantres-Fonseca, and Isabel M. McFarlane, American Journal of Medical Case Reports, licensed under CC BY 4.0.

Dark red, large maculopapular, partially confluent exanthema on patient's back.
Combined with the characteristic clinical features, this finding indicates measles.
Source: Courtesy of Dr. Gary M. White, MD

Chest of a child
Multiple vesicles filled with clear fluid on an erythematous base are visible.
This clinical finding is called "dewdrops on a rose petal," and it is classically seen in varicella (chickenpox).
Source: Courtesy of Dr. Gary M. White, MD

A diffuse rash is seen in various stages of lesion evolution (starry-sky appearance), with mainly ruptured vesicles and crusted erosions seen here.
These findings are typical for chickenpox.
This image is an adaptation. Source of original image: Wikimedia Commons. Original title: “Waterpokken”. Created by: Postertjack. Licensed under Public Domain. Modifications to original image: Pixelation of the orbital area.

A round, well demarcated erythematous lesion with central scaling is visible. The border is raised with several pustules visible.
These features are characteristic of tinea corporis.
Source: "ID#: 2938", CDC/ Dr. Lucille K. Georg, Centers for Disease Control and Prevention (CDC) licensed under Public Domain

Well-demarcated erythematosquamous plaques and silver-white scaling are visible over the extensor side of both lower legs.
These findings are characteristic of psoriasis.
Source: © IMPP

Erythematous, confluent plaques typical of urticaria that cover most of the skin on the antecubital fossa and the ventral side of the forearm.
Source: “EMminor2010” by James Heilmann, MD, Wikimedia Commons, licensed under CC BY-SA 3.0.
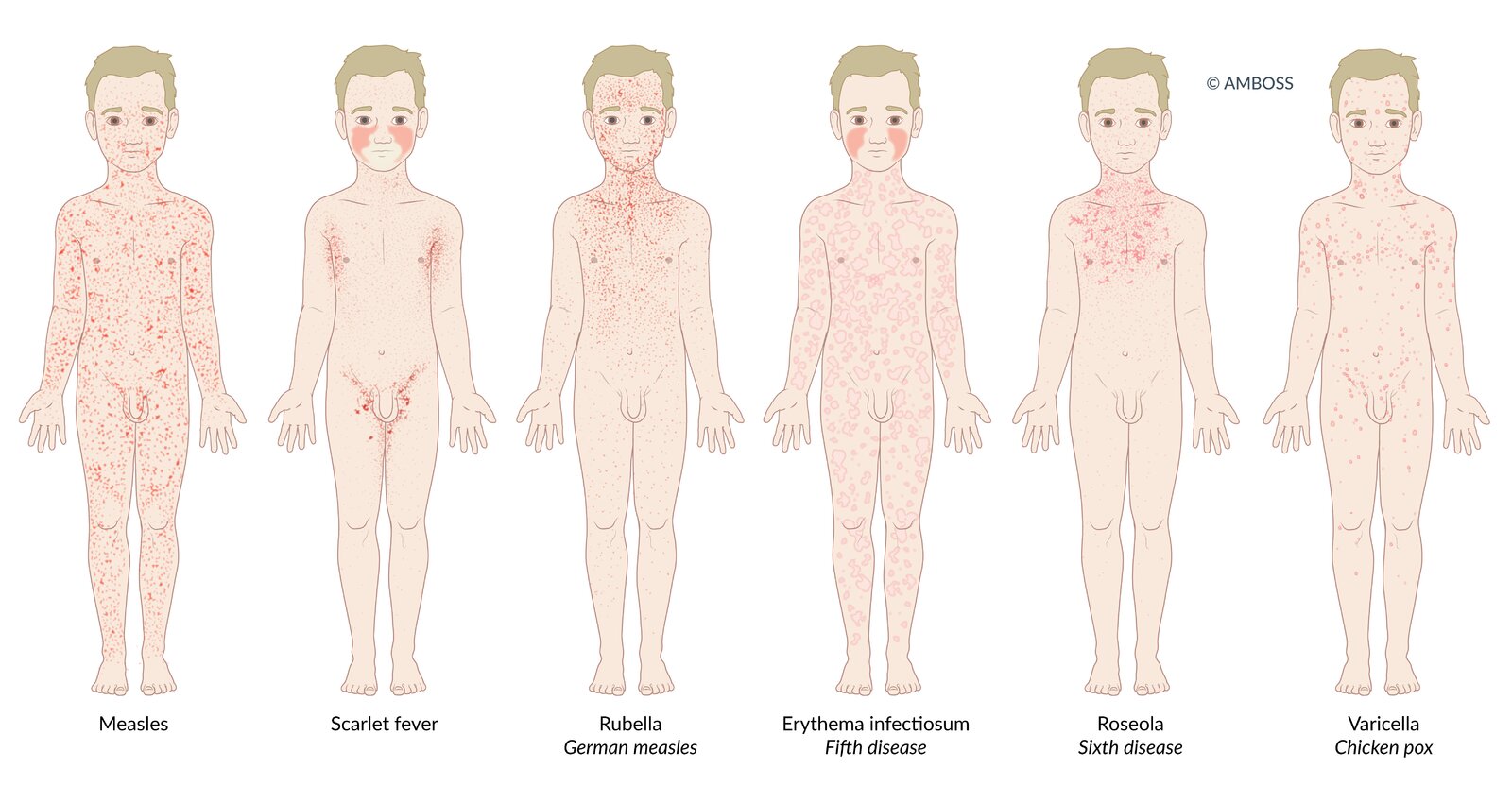
Many infectious diseases in children present with a rash (exanthem). The distribution and morphological characteristics of the exanthem allow the diseases to be differentiated from one another.
Measles: Patients present with a dark red, erythematous, maculopapular, partially confluent exanthem, which spreads from behind the ears to the rest of the body.
Scarlet fever: Patients present with a fine, light red rash with sandpaper-like texture. The exanthem begins on the neck or trunk and disseminates to the whole body. Cheeks may be flushed with perioral pallor. In flexural areas (e.g., axilla and groin), the rash may be more pronounced and linear petechiae (Pastia lines) may be present.
Rubella (German measles): Patients typically present with a nonconfluent, pink, maculopapular exanthem, which begins on the face and spreads to the trunk and extremities.
Erythema infectiosum (fifth disease): A confluent, maculopapular rash appears only in ¼ of patients. It may take on a lace-like, reticular appearance over time. Additionally, patients present with diffuse redness of the face with perioral sparing (slapped-cheek rash).
Roseola infantum (sixth disease): 3-7 days of high fever are followed by a sudden decrease in temperature and development of a patchy, blanching rose-pink maculopapular rash. The rash originates on the trunk, and may spread to the face and extremities.
Varicella (chickenpox): The exanthem affects the whole body, typically spreading to the scalp as well. Various stages of the rash occur simultaneously, which leads to the characteristic clinical finding known as “starry sky.”
© AMBOSS
Initial management
Approach [1][2][12]
- Don PPE as appropriate, e.g., contact precautions.
- Isolate patients with fever and petechial rash and escalate PPE to droplet precautions.
- Identify patients with red flags for a life-threatening rash.
- Initiate continuous monitoring and place IV access in severely ill patients.
- Consult dermatology urgently.
- Initiate treatment for life-threatening causes of rash immediately.
- Perform a focused clinical evaluation.
- Narrow the differential diagnosis based on the morphology of the rash (see “Etiology”).
- Obtain appropriate diagnostic testing.
- Begin supportive and definitive treatment.
Fever and petechial rash may indicate meningococcal septicemia.
Red flags for a life-threatening rash [2]
- Fever
- Severely ill appearance, e.g., lethargy, cyanosis, mottled extremities, hypoventilation or hyperventilation
- Hypotension
- Mucosal lesions
- Severe pain
- Extremes of age
- History of immunosuppression
- Recently initiated medication
Life-threatening causes of rash
- Pemphigus vulgaris
- SJS/TEN
- DRESS
- TSS
- Meningococcal septicemia
- RMSF
- Necrotizing fasciitis
Disposition [4]
Admit patients with any of the following:
- Hypotension
- High fever or hypothermia
- Systemic infection or underlying condition requiring inpatient management
- Significant fluid and electrolyte abnormalities
- Inability to maintain oral intake
Clinical evaluation
The differential diagnosis of a rash can be quickly narrowed using basic morphology and associated clinical findings. [1][2]
Focused history [2][8][12]
Rash characteristics
- Onset
- Duration
- Progression
Associated symptoms
- Fever
- Pruritus
- Pain at rash site
- Arthralgias
Exposures
- New medications
- Recent travel
- Occupation
- Change in personal care products
- Sexual history
- Sick contacts
- Recent bites
Focused examination [2][4][12]
General physical examination
- Overall condition, e.g., mental status and vital signs
- Lung auscultation
- Cardiac auscultation
- Lymphadenopathy
Skin examination
See “Primary skin lesions” and “Secondary skin lesions” for describing and documenting rashes.
-
Rash morphology
- Petechiae or purpura
- Erythema
- Maculopapular rash
- Vesiculobullous rash
-
Lesion characteristics
- Palpable or nonpalpable
- Blanchable
- Positive or negative Nikolsky sign
Always have the patient disrobe and ensure that the entire body is examined, including mucus membranes and genitalia.
Diagnosis
Laboratory studies [4][12]
Routine laboratory studies are seldom required for rashes that appear benign, but are necessary in severely ill patients.
-
CBC
- Thrombocytopenia, e.g., in vasculitis
- Leukocytosis suggests infection or severe inflammatory disease.
-
CMP
- Electrolyte and acid-base abnormalities suggest severe disease.
- Abnormal LFTs may indicate hepatitis, e.g., in severe drug reactions.
-
Serology, antibody, and antigen testing
- Rapid strep test: often positive in scarlet fever
- EBV serology: positive in infectious mononucleosis
- Monospot test: positive in infectious mononucleosis, but may be false positive
- VDRL or FTA-ABS: diagnostic for syphilis
- Rickettsia antibody panels
- Lyme antibody testing
- ANCA: for suspected autoimmune conditions, e.g., eosinophilic granulomatosis with polyangiitis
- Cultures: CSF for meningococcal septicemia, blood cultures for endocarditis
Dermatologic studies
- Punch biopsy: for uncertain diagnosis or suspected autoimmune condition
- Tzanck smear: in vesicular lesions; diagnostic for pemphigus vulgaris, HSV infection, and chickenpox
- Vesicle or pustule cultures: for suspected bacterial, fungal, or viral infections
- Patch test: for suspected contact dermatitis, allergic dermatitis
- KOH prep: for suspected fungal infections
Petechial and purpuric rashes
The lesions of a petechial or purpuric rash do not blanch when pressure is applied.
| Common causes of petechial and purpuric rashes [2][3][13] | ||||
|---|---|---|---|---|
| Images | Distinguishing features | Diagnostic findings | Management | |
| Meningococcal septicemia |
|
|
|
|
| Acute bacterial endocarditis |
|
|
|
|
| RMSF |
|
|
|
|
| Disseminated gonococcal infection |
|
|
|
|
| IgA vasculitis |
|
|
|
|
| TTP |
|
|
|
|
| ITP |
|
|
|
|
| Vasculitic syndromes |
|
|
|
|







Unexplained purpura in a child, especially on the trunk, ears, or face, may indicate child abuse. [3]

Purple nonblanching macules of various sizes, consistent with purpura (larger macules) and petechiae (smaller macules), are visible.
These findings are consistent with purpura in Waterhouse-Friderichsen syndrome.
Source: © IMPP

There are multiple raised nodular lesions on the palm and palmar aspects of the first and second digits. The lesions appear dark brown, indicating subcutaneous hemorrhages.
This is the typical appearance of Osler nodes.
Source: “Osler Nodules Hand” by Roberto J. Galindo, Wikimedia Commons, licensed under CC BY-SA 4.0.

Multiple erythematous macules are visible on the thenar eminence and the base of the thumb.
These Janeway lesions are typically caused by septic microembolisms secondary to infective endocarditis.
Source: “Janeway lesion” by Warfieldian, Wikimedia Commons, licensed under CC BY-SA 4.0.

Multiple, partly confluent, macules are visible on this patient's forearm.
This rash is suggestive of Rocky Mountain spotted fever (RMSF), a tick-borne disease caused by Rickettsia rickettsii bacteria. The distal extremities are usually affected first; the rash then spreads toward the proximal extremities and the trunk (the face, however, is usually spared).
Source: "ID#: 1962", CDC, Centers for Disease Control and Prevention licensed under Public Domain

Source: "ID#: 2848", CDC/Dr. Thomas F. Sellers, Public Health Image Library (PHIL) licensed under Public Domain

Multiple well-defined erythematous skin lesions (purpura) are distributed on the shin of this pediatric patient. Some purpura have coalesced to form ecchymoses.
Purpura may be palpable and nonblanchable on examination.
Source: “Figure 1, in: Henoch-schonlein purpura associated with primary active epstein barr virus infection: a case report” by B. Karakayali, S. Yilmaz, D. Çakir et al., The Pan African Medical Journal, licensed under CC BY 4.0.
The lower leg displays numerous red spots, each about the size of a pinhead, that do not blanch or disappear when pressed. These are indicative of petechial hemorrhages related to thrombocytopenia.
Source: © IMPP
Bluish-red, round or oval maculae (approx. 0.2 mm–1 cm in diameter) are distributed over the right lower leg. There is also an irregularly shaped macula of the same color lateral to the patella (approx. 4 × 2 cm in diameter).
This appearance is characteristic of purpura.
Source: © IMPP

Multiple, partially confluent, round circular maculae (purpura) can be seen on both lower legs and thighs.
This is a common cutaneous symptom of cryoglobulinemic vasculitis.
Source: © IMPP
Diffuse erythematous rashes
Erythematous rashes manifest as diffuse redness that blanches with pressure.
| Common causes of erythematous rashes [2][4] | ||||
|---|---|---|---|---|
| Images | Distinguishing features | Diagnostic findings | Management | |
| SSSS |
|
|
|
|
| TEN and SJS [15] |
|
|
|
|
| TSS |
|
|
|
|
| Scarlet fever rash |
|
|
|
|
| Anaphylaxis |
|
|
|
|
| Histamine fish poisoning [16] |
|
|
|
|
| Flushing reaction [17][18] |
|
|
|
|

")


")

Perioral, cervical and axillary reddening of the skin is visible, resulting in a scalded appearance on this child's face. In some areas, the superficial epidermal layer is detached (e.g., on the chin). On the right side of the neck, several flaccid blisters can be seen. The lips appear dry, with several rhagades in the corners of the mouth.
Source: Courtesy of Dr. Gary M. White, MD

The trunk and arm show generalized, widespread, extensive necrosis with purple and red erythema, as well as yellow-white exudation. Spots of hemorrhagic, subepidermal tissue can also be seen.
These characteristic findings are distinctive for TEN, a severe form of Stevens-Johnson syndrome (SJS).
Source: “Figure 89: Extensive epidermal necrolysis; in : Atlas of Pediatric HIV Infection” by Regina E. Oladokun; Rannakoe J. Lehloenya; Carol Hlela et al., Openbooks, licensed under CC BY-ND 4.0.


The typical scarlet-colored, fine, maculopapular exanthem of scarlet fever is seen on the right arm. Flushed cheeks and perioral pallor are also evident.
Source: “Scarlet Fever” by Badobadop, Wikimedia Commons, licensed under CC BY-SA 3.0. Modifications: Pixelated eyes.
Erythematous, confluent plaques typical of urticaria that cover most of the skin on the antecubital fossa and the ventral side of the forearm.
Source: “EMminor2010” by James Heilmann, MD, Wikimedia Commons, licensed under CC BY-SA 3.0.

Multiple annular, erythematous, well-demarcated, slightly elevated plaques are visible.
This appearance is consistent with urticaria. Urticaria appears soon after exposure to an antigen and disappears within a few hours. The lesions are caused by mast-cell degranulation in the superficial dermis.
Our great thanks to Milena Koreng for kindly providing this image.
Erythema of the skin is visible, especially on the patient's cheeks and nose. This symptom usually resolves within minutes after treatment. Vancomycin flushing reaction is not a true allergic reaction, but rather a rate-dependent hypersensitivity reaction. It can be avoided by slow infusion.
Source: “Figure 1, in: Red Man Syndrome with Oral Vancomycin: A Case Report” by Fray Arroyo-Mercado, Aleksandr Khudyakov, Gurasees S. Chawla, Onix Cantres-Fonseca, and Isabel M. McFarlane, American Journal of Medical Case Reports, licensed under CC BY 4.0.
Maculopapular rashes
The mixture of flat and raised discolored areas that define a maculopapular rash may also be the early stage of a petechial, purpuric, or vesiculobullous rash.
| Common causes of maculopapular rashes [2][4] | ||||
|---|---|---|---|---|
| Images | Distinguishing features | Diagnostic findings | Management | |
| Measles |
|
|
|
|
| Kawasaki disease |
|
|
|
|
| Secondary syphilis |
|
|
|
|
| Viral exanthem |
|
|
|
|
| Cutaneous drug reactions [10][11] |
|
|
|
|
| Scabies |
|
|
|
|
| Atopic dermatitis |
|
|
|
|
| Pityriasis rosea |
|
|||




")
")



Meningococcal septicemia, RMSF, and Stevens-Johnson syndrome are life-threatening conditions that may also cause a maculopapular rash.
Dark red, large maculopapular, partially confluent exanthema on patient's back.
Combined with the characteristic clinical features, this finding indicates measles.
Source: Courtesy of Dr. Gary M. White, MD
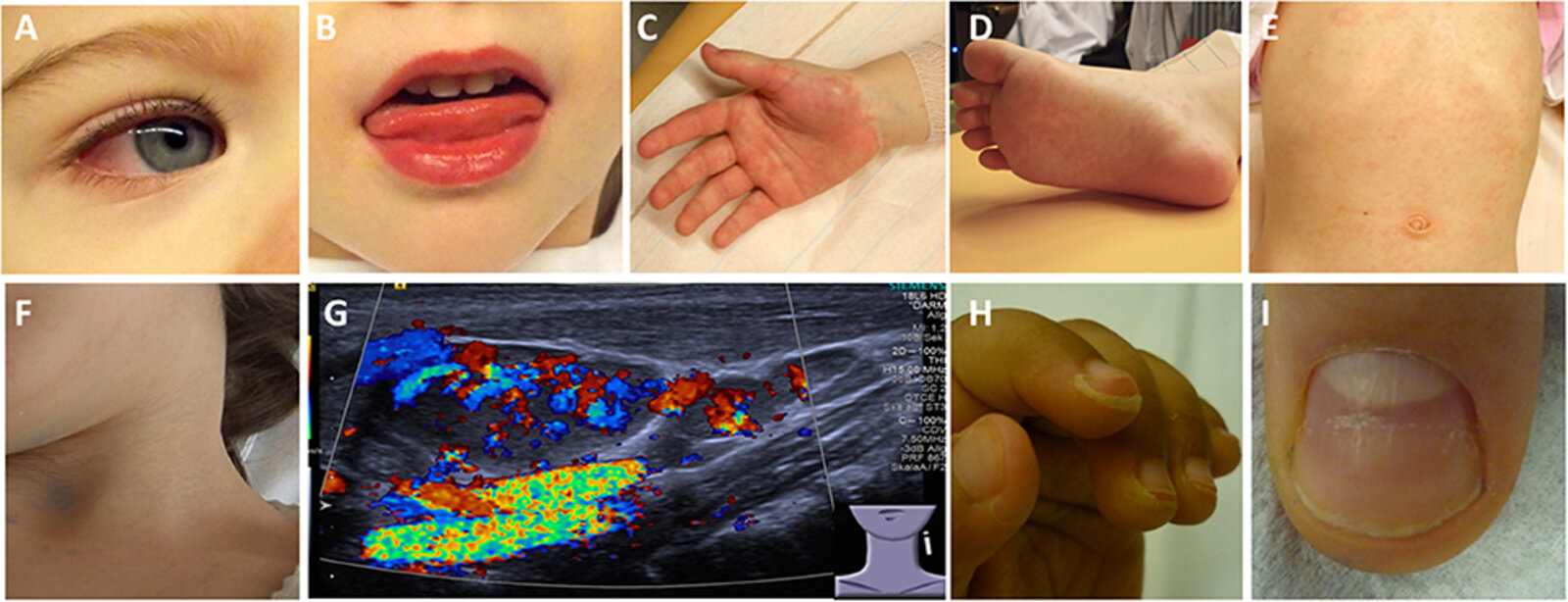
(A) Bilateral, nonpurulent conjunctivitis
(B) Stomatitis with bright red lips
(C) Erythema and edema of the hands
(D) Erythema and edema of the feet
(E) Truncal rash
(F) Cervical lymphadenopathy
(G) Ultrasound of an enlarged cervical lymph node: increased perfusion
(H) Desquamation of fingertips
(I) Deep grooves in the nail (Beau lines)
Source: “Figure 2, in: Kawasaki Disease” by C. M. Hedrich, A. Schnabel, T. Hospach, Frontiers in Pediatrics, licensed under CC BY 4.0.

An erythematous maculopapular rash with scaling is visible on the left palm.
A rash with this appearance typical for secondary syphilis.
Source: © IMPP

Partially confluent and partially scaling red papules and macules of ∼2–5 mm diameter are visible on the palms and wrists.
This appearance is typical of secondary syphilis.
Source: © IMPP

Photograph of the back of a young child:
This child shows a generalized, macular, pale, and fine-spotted rash. In this case, the child presented with signs and symptoms of a cold. The physical findings together with the history indicate the presence of a nonspecific virus exanthema, most commonly triggered by enteroviruses.
© AMBOSS
Many infectious diseases in children present with a rash (exanthem). The distribution and morphological characteristics of the exanthem allow the diseases to be differentiated from one another.
Measles: Patients present with a dark red, erythematous, maculopapular, partially confluent exanthem, which spreads from behind the ears to the rest of the body.
Scarlet fever: Patients present with a fine, light red rash with sandpaper-like texture. The exanthem begins on the neck or trunk and disseminates to the whole body. Cheeks may be flushed with perioral pallor. In flexural areas (e.g., axilla and groin), the rash may be more pronounced and linear petechiae (Pastia lines) may be present.
Rubella (German measles): Patients typically present with a nonconfluent, pink, maculopapular exanthem, which begins on the face and spreads to the trunk and extremities.
Erythema infectiosum (fifth disease): A confluent, maculopapular rash appears only in ¼ of patients. It may take on a lace-like, reticular appearance over time. Additionally, patients present with diffuse redness of the face with perioral sparing (slapped-cheek rash).
Roseola infantum (sixth disease): 3-7 days of high fever are followed by a sudden decrease in temperature and development of a patchy, blanching rose-pink maculopapular rash. The rash originates on the trunk, and may spread to the face and extremities.
Varicella (chickenpox): The exanthem affects the whole body, typically spreading to the scalp as well. Various stages of the rash occur simultaneously, which leads to the characteristic clinical finding known as “starry sky.”
© AMBOSS

Ventral upper body of a patient presenting with a pruritic rash following the administration of amoxicillin
A diffuse rash composed of several fine erythematous papules is visible. This rash, known as a morbilliform rash because it resembles the rash seen in measles, is typical of a drug reaction.
© AMBOSS

Dorsal upper body of a patient presenting with a pruritic rash following the administration of amoxicillin
A diffuse rash composed of several fine erythematous papules is visible. This rash, known as a morbilliform rash because it resembles the rash seen in measles, is typical of a drug reaction.
© AMBOSS

Multiple erythematous papules (partially excoriated) are visible in the interdigital folds and on the dorsal aspect of the hand and fingers.
© AMBOSS

Multiple papules with excoriation are visible on this patient's trunk, esp around the umbilicus, around which the skin appears lichenified.
These findings together with pruritus are suggestive of scabies.
© AMBOSS

Erythema and excoriations on the wrist of the left hand.
Source: © IMPP
Vesiculobullous rashes
Vesiculobullous rashes are composed of multiple fluid-filled lesions caused by a disorder of the epidermal-dermal junction.
| Common causes of vesiculobullous rashes [2][4] | ||||
|---|---|---|---|---|
| Images | Distinguishing features | Diagnostic findings | Management | |
| Varicella |
|
|
|
|
| Shingles |
|
|
|
|
| Necrotizing fasciitis [19] |
|
|
|
|
| Hand, foot, and mouth disease [20] |
|
|
|
|
| Bullous pemphigoid [21][22] |
|
|
|
|
| Pemphigus vulgaris [21][22] |
|
|
|
|
| Bullous impetigo |
|
|
|
|
| Contact dermatitis |
|
|
|
|








See also “Autoimmune blistering diseases” and “Skin and soft tissue infections.”
Disseminated gonococcal infection, acute generalized exanthematous pustulosis, and smallpox may have a vesiculobullous appearance.
Chest of a child
Multiple vesicles filled with clear fluid on an erythematous base are visible.
This clinical finding is called "dewdrops on a rose petal," and it is classically seen in varicella (chickenpox).
Source: Courtesy of Dr. Gary M. White, MD

Asymmetrical, red, vesicular lesion in the area of the right scapula, indicating reactivation of varicella-zoster virus (VZV).
Source: © IMPP

Posterolateral aspect of the left thigh, gluteal region, and popliteal fossa
There is significant diffuse edema and erythema across the entire visible region, with well-defined areas of necrosis, desquamation, and hemorrhagic bullae.
These features are strongly suggestive of necrotizing fasciitis, a rapidly progressive infection of the skin, subcutaneous tissue, and superficial and deep fascia that requires urgent debridement.
Source: “Figure 1, in: Late diagnosed necrotizing fasciitis as a cause of multiorgan dysfunction syndrome: A case report” by Smuszkiewicz P, Trojanowska I, Tomczak H, BMC Cases Journal, licensed under CC BY 2.0.

Source: “Hand foot and mouth disease” by Gzzz, Wikimedia Commons, licensed under CC BY-SA 4.0.

Multiforme lesions and serous fluid-filled blisters of various sizes are visible over the entire anterior aspect of the patient's body. Marked erythema is also present.
These findings are consistent with bullous pemphigoid.
Source: © IMPP

Multiple ruptured blisters with surrounding erythema are visible. A single intact blister can be seen in the center of the image.
This finding is suggestive of pemphigus vulgaris, but histopathology is required to confirm the diagnosis.
Source: Courtesy of Dr. Gary M. White, MD

Flaccid bullae and gray-white plaques are visible on the oral mucosa. The plaque can be scraped off, causing deep red erosions.
These findings are consistent with pemphigus vulgaris.
Source: "ID#: 12573", CDC/ Dr. J. Lieberman; Dr. Freideen Farzin, Univ. of Tehran, Centers for Disease Control and Prevention (CDC) licensed under Public Domain

Multiple vesicles, some of which have already ruptured and formed brown crusts, are visible on the gluteal region of this infant. The lesions in bullous impetigo are easily confused with the polymorphic rash of secondary syphilis.
Source: "ID#: 5154", CDC, Centers for Disease Control and Prevention licensed under Public Domain

Upper body of a man presenting with a severely pruritic rash after getting a henna tattoo on the right arm
An erythematous papulovesicular rash is visible over the chest and arms. The rash is most severe around the henna tattoo, which appears markedly erythematous.
This is the typical appearance of allergic contact dermatitis.
Source: © IMPP
Annular skin lesions
| Overview of annular skin lesions | ||||||||
|---|---|---|---|---|---|---|---|---|
| Images | Etiology | Location | Characteristics | |||||
| Erythema migrans |
|
|
|
|
||||
| Tinea corporis |
|
|
|
|
||||
| Erythema marginatum |
|
|
|
|
||||
| Nummular dermatitis |
|
|
|
|
||||
| Granuloma annulare |
|
|
|
|
||||
| Urticaria |
|
|
|
|
||||
| Erythema multiforme (EM) |
|
|
|
|
||||
| Fixed drug eruption |
|
|
|
|
||||
| Pityriasis rosea |
|
|
|
|
||||
| Discoid lupus |
|
|
|
|
||||


")











 in pityriasis rosea")



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}

A large, primary lesion with circular erythema and central clearing on the posterior side of the right upper arm is visible.
This clinical picture is typical of erythema migrans (stage-I Lyme disease).
Illustration: Bull's eye sign
Source: "ID#: 9875", CDC/ James Gathany, Centers for Disease Control and Prevention (CDC) licensed under Public Domain

A round, homogeneous area of erythema with a diameter of approx. 14 cm can be seen on the right shoulder of this patient diagnosed with Lyme disease.
The circular expanding lesion forming around a tick bite is highly suggestive of erythema migrans, which is characteristic of Lyme disease.
Source: "ID#: 14482", Centers for Disease Control and Prevention licensed under Public Domain

Four round, erythematous plaques with central clearing and raised, scaly borders are visible on this patient's arm.
Source: © IMPP

Multiple circular patches with raised borders, peripheral scaling, and central clearing are visible on this child's upper abdomen.
These findings are distinctive of tinea corporis, which is also called "ringworm" because of its characteristic presentation.
Source: “Figure 41a: Tinea corporis (trunk); in: Atlas of Pediatric HIV Infections” by Regina E. Oladokun; Rannakoe J. Lehloenya; Carol Hlela et al., Openbooks, licensed under CC BY-ND 4.0.

Left upper arm of a child diagnosed with acute rheumatic fever (ARF)
Erythematous plaques with areas of central clearing are visible on the ventral aspect of the forearm.
This is characteristic of erythema marginatum, the characteristic annular erythema occuring in 10% of attacks of acute rheumatic fever in children, caused by group A streptococcus.
Source: “Erythema marginatum” by Adsie, Wikimedia Commons, licensed under CC BY-SA 4.0. Modifications: image has been cropped.
{kind=link}

Upper ankle region with a round, red-brown, scaly plaque.
Nummular eczema is usually associated with severe pruritus. Tinea corporis should be considered as a differential diagnosis.
Source: Courtesy of Dr. Gary M. White, MD

Multiple round, erythematous, scaly plaques are visible on this child's lower legs.
Source: “Figure 8, in: The spectrum of skin diseases in a rural setting in Cameroon (sub-Saharan Africa)” by A.Z. Bissek, E.N. Tabah, E. Kouotou et al., BMC Dermatology, licensed under CC BY 2.0.

Photograph of the dorsum of the hand
Ring-shaped lesions are visible over the 2nd and 4th knuckles.
On closer inspection, each ring is composed of multiple non-scaly mildly erythematous papules and nodules, some of which are skin-colored.
Each lesion has a central clearing.
These non-scaly annular lesions are characteristic of granuloma annulare, an idiopathic, benign, non-contagious cutaneous lesion.
Source: © IMPP

Hypopigmented, nonscaly papules are visible on the patient's chin. The lesions coalesce to form arciform or annular patterns.
These lesions are characteristic of granuloma annulare. The absence of scaling distinguishes this feature from tinea corporis.
Source: “Figure 16, in: Clinical Manifestations of Sarcoidosis and Granulomatous Disorders” by Suchibrata Das, IntechOpen, licensed under CC BY 3.0.

Multiple well-defined, erythematous, partially confluent lesions with raised serpiginous borders and central clearing are visible.
This is the characteristic appearance of urticaria, which typically has an acute onset, is highly pruritic, and transient.
Source: © IMPP

Multiple well-defined lesions can be seen on the back of the hand. The lesions consist of concentric rings with an outer erythematous zone, a paler intermediate zone, and a darker violaceous center, consistent with target lesions. Some of the lesions show central blistering.
This presentation is typical of erythema multiforme.
Source: © IMPP

Multiple circular lesions with a central papule and raised edges (also called “target lesions”), surrounded by a lighter edematous area, are visible on the anterior aspect of the thighs.
This is the typical appearance of erythema multiforme.
Source: Courtesy of Dr. Gary M. White, MD

Multiple, heterogeneous, and mostly bullous lesions with characteristic, slight erythematous rims around a hyperpigmented center are visible.
While blisters and/or ulcerations of the damaged skin may not always occur, the rest of the highlighted findings are still suspicious for a fixed drug eruption.
Source: “Figure 94 c: Classic round pigmented {...}; in: Atlas of Pediatric HIV Infection” by Regina E. Oladokun; Rannakoe J. Lehloenya; Carol Hlela et al., Openbooks, licensed under CC BY-ND 4.0.

A secondary rash after primary plaque formation (not shown) can be seen on the back of this patient. The secondary eruption of pityriasis rosea is usually episodic and distributed along Langer lines.
Source: © IMPP

The primary plaque (located on the trunk) in this image is the initial and largest lesion in pityriasis rosea. The surface shows irregular scaling.
Source: "ID#: 5506", CDC/ Dr. Sellars, Centers for Disease Control and Prevention (CDC) licensed under Public Domain

Bilateral diffuse, oval-shaped plaques with scaly collarettes are visible on this child's back and face.
Source: “Figure 1, in: Atypical Pityriasis rosea in a black child: a case report” by Sergio Vano-Galvan, Dong-Lai Ma, Alejandro Lopez-Neyra, Bibiana Perez, Ernesto Muñoz-Zato, Pedro Jaén, Cases Journal, BioMed Central Ltd., licensed under CC BY 3.0.

Multiple annular (discoid), sharply demarcated, erythematous plaques, 0.5–3 cm in diameter with central atrophy and scaling are visible underneath the right ear. Additional scaly plaques are located on the lobe, helix, and antihelix of the ear.
These are the characteristic features of discoid lupus erythematosus (DLE), a chronic, scarring variant of cutaneous lupus erythematosus. DLE lesions are typically pruritic and have a propensity to first appear on the face and neck.
Source: © IMPP

Back of a patient with Takayasu arteritis
Several annular (discoid), sharply-demarcated, erythematous lesions can be seen. The center of the lesions appears atrophic.
These are characteristic features of discoid systemic lupus erythematosus.
Source: “Figure 1, in: Takayasu’s Arteritis with Systemic Lupus Erythematosus: A Rare Association” by Dhrubajyoti Bandyopadhyay, Vijayan Ganesan, Debarati Bhar, Diptak Bhowmick, Sibnarayan Sasmal, Cankatika Choudhury, Sabyasachi Mukhopadhyay, Adrija Hajra, Manas Layek, Partha Sarathi Karmakar, Hindawi, licensed under CC BY 3.0.
Mimics
Skin nodules [23][24]
A skin nodule is an elevated cystic or solid lesion > 1 cm in diameter.
- Sebaceous hyperplasia
- Epidermal inclusion cysts
- Dermatofibroma
- Acrochordon
- Rheumatoid nodules
- Nonmelanoma skin cancer
- Chancre
- Leprosy

Cutaneous ulcers [25]
Cutaneous ulcers are rounded or irregularly shaped discontinuities in the skin caused by loss of the epidermis and some portion of the dermis.
- Chronic venous disease
- Peripheral artery disease
- Collagen vascular disease
- Vasculitides
- Pyoderma gangrenosum
- Necrobiosis lipoidica
- Decubitus ulcer


A nodule is visible in the palm of this patient's hand.
This appearance is typical of rheumatoid nodules in rheumatoid arthritis.
Created by: Dr. Thomas Rath, Münster. Modifications to original image: Image slightly lightened.

Left lower leg
Typical features of chronic venous insufficiency, including purpura jaune d'ocre, atrophie blanche, lipodermatosclerosis, and an active venous ulceration are present.
There is impaired microcirculation of the vessels due to venous stasis. The findings indicate CEAP class C6 disease.
Source: “Chronic venous insufficiency Stadium (III)” by Abdullah Sarhan, Wikimedia Commons, licensed under CC BY-SA 4.0.
.JPG){kind=link}
References
- Higgins JC, Maher MH, Douglas MS. "Diagnosing Common Benign Skin Tumors". Am Fam Physician. 92(7). :601-7. (2015)
- Brinkman D, Roche L, Ullah K, O’Connor TM. "Multiple cutaneous nodules as the presenting sign of small cell lung cancer". BMJ Case Rep. 2013(may22 1). :bcr2013009160-bcr2013009160. (2013)
- Panuncialman J, Falanga V. "Unusual Causes of Cutaneous Ulceration". Surg Clin North Am. 90(6). :1161-1180. (2010)
- McCollough M. "The Algorithmic Approach to the Unidentified Rash". Springer International Publishing. :215-240. (2018). ISBN: 9783319756226
- Santistevan J, Long B, Koyfman A. "Rash Decisions: An Approach to Dangerous Rashes Based on Morphology". J Emerg Med. 52(4). :457-471. (2017)
- Thomas AE, Baird SF, Anderson J. "Purpuric and petechial rashes in adults and children: initial assessment". BMJ. :i1285. (2016)
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904
- Trayes KP, Savage K, Studdiford JS. "Annular Lesions: Diagnosis and Treatment". Am Fam Physician. 98(5). :283-291. (2018)
- Gisondi P, Bellinato F, Girolomoni G. "Topographic Differential Diagnosis of Chronic Plaque Psoriasis: Challenges and Tricks". J Clin Med. 9(11). :3594. (2020)
- Schettini N, Corazza M, Schenetti C, Pacetti L, Borghi A. "Urticaria: A Narrative Overview of Differential Diagnosis". Biomedicines. 11(4). :1096. (2023)
- Allmon A, Deane K, Martin KL. "Common Skin Rashes in Children". Am Fam Physician. 92(3). :211-6. (2015)
- James G. Dinulos. "What's new with common, uncommon and rare rashes in childhood". Curr Opin Pediatr. 27(2). :261-266. (2015)
- Khan DA. "Cutaneous drug reactions". J Allergy Clin Immunol. 130(5). :1225-1225.e6. (2012)
- Segal AR, Doherty KM, Leggott J, Zlotoff B. "Cutaneous Reactions to Drugs in Children". Pediatrics. 120(4). :e1082-e1096. (2007)
- Ely JW, Seabury Stone M. "The generalized rash: part II. Diagnostic approach". Am Fam Physician. 81(6). :735-9. (2010)
- Antonov D, Kamarashev J, Kazandjieva J, Neykova T, Tsankov N. "The rash that becomes purpuric, petechial, hemorrhagic, or ecchymotic". Clin Dermatol. 38(1). :3-18. (2020)
- Hussain A, Gray C, Marlowe S, et al. "Unconventional Rocky Mountain Spotted Fever Presentation From Kentucky: A Compelling Case Report and Literature Review". Cureus. (2023)
- Zimmerman D, Dang NH. "Stevens–Johnson Syndrome (SJS) and Toxic Epidermal Necrolysis (TEN)". Springer International Publishing. :267-280. (2019). ISBN: 9783319745879
- Feng C, Teuber S, Gershwin ME. "Histamine (Scombroid) Fish Poisoning: a Comprehensive Review". Clin Rev Allergy Immunol. 50(1). :64-69. (2015)
- Shrivastava S, Shrivastava S. "Vancomycin Flushing Syndrome: A Case Report". Cureus. (2024)
- Brooks PJ, Enoch MA, Goldman D, Li TK, Yokoyama A. "The Alcohol Flushing Response: An Unrecognized Risk Factor for Esophageal Cancer from Alcohol Consumption". PLoS Med. 6(3). :e1000050. (2009)
- Fatimah L, Kiat H, En Natalie Y. "Necrotizing fasciitis: How reliable are the cutaneous signs?". J Emerg Trauma Shock. 10(4). :205. (2017)
- Saguil A, Kane SF, Lauters R, Mercado MG. "Hand-Foot-and-Mouth Disease: Rapid Evidence Review". Am Fam Physician. 100(7). :408-414. (2019)
- Meijer JM, Diercks GFH, de Lang EWG, Pas HH, Jonkman MF. "Assessment of Diagnostic Strategy for Early Recognition of Bullous and Nonbullous Variants of Pemphigoid". JAMA Dermatol. 155(2). :158. (2019)
- Di Lernia V, Casanova DM, Goldust M, Ricci C. "Pemphigus Vulgaris and Bullous Pemphigoid: Update on Diagnosis and Treatment". Dermatol Pract Concept. :e2020050. (2020)