Summary
Regional anesthesia involves the injection of local anesthetic agents around nerves in the peripheral nervous system or central nervous system to achieve reversible numbing of pain conduction in the corresponding innervated tissue. Regional anesthesia can be divided into peripheral nerve blocks, neuraxial anesthesia (i.e., spinal anesthesia, epidural anesthesia), and intravenous regional anesthesia.
See also “Local anesthesia” and “Local anesthetic agents.”
Overview
- Goal: used prior to certain medical procedures to reduce pain. [1]
- Types of anesthetic agents: See “Local anesthetic agents.”
-
General contraindications to regional anesthesia
- Absolute: allergy to a class of anesthetic
- Relative
- Active inflammation or infection at the injection site
- Coagulopathy
- Neurological deficits in the area of distribution
-
Types
- Peripheral nerve blocks
- Neuraxial anesthesia (i.e., epidural anesthesia, spinal anesthesia)
- Intravenous regional anesthesia (Bier block): a local anesthetic agent is injected intravenously into an extremity that has been separated from the central circulation with a tourniquet and exsanguinated by compression to provide an anesthetized, bloodless surgical field
Peripheral nerve block
Definition [1]
Injection of local anesthetic agents around nerves in the peripheral nervous system to achieve reversible numbing of pain conduction in the corresponding innervated tissue
Indications [1]
General
- Nonthoracoabdominal surgery or minor procedures (e.g., closed reductions)
- Wound repair in which infiltration anesthesia may distort the anatomy
- Large area of anesthesia required
- Postoperative pain control
Head, neck, and thorax
| Common nerve blocks of the head, neck, and thorax [1] | ||
|---|---|---|
| Type | Targeted nerves | Clinical applications |
| Maxillary nerve block |
|
|
| Mandibular nerve block |
|
|
| Intercostal block |
|
|
| Penile block [2][3] |
|
|
Use a local anesthetic agent without epinephrine for regional anesthesia of the penis. [2]

Upper extremity
| Common nerve blocks of the upper extremities [1] | ||
|---|---|---|
| Type | Targeted nerves or plexus | Clinical applications |
| Brachial plexus block |
|
|
| Elbow or wrist block |
|
|
| Digital block See also “Lower extremity.” |
|
|




Lower extremity
| Common nerve blocks of the lower extremities [1] | ||
|---|---|---|
| Type | Targeted nerves | Clinical applications |
| Femoral block (three-in-one block) |
|
|
| Fascia iliaca block |
|
|
| Sciatic block |
|
|
| Ankle block |
|
|
| Digital block |
|
|

")
")
Contraindications
See “General contraindications to regional anesthesia.”
Procedure [1]
- Injection site: varies based on the target nerve
-
Approach
- Single injection
- Continuous administration via a catheter
-
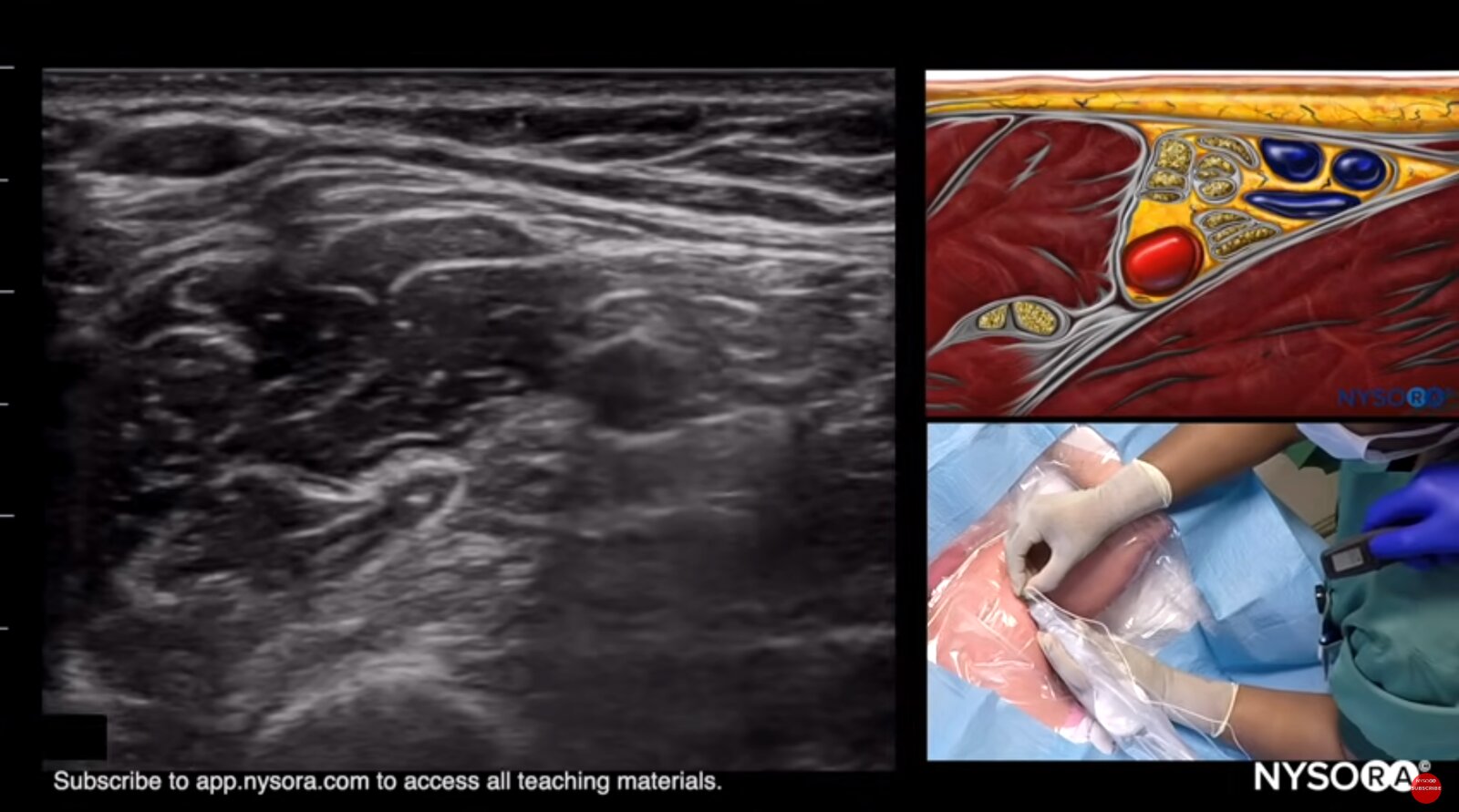
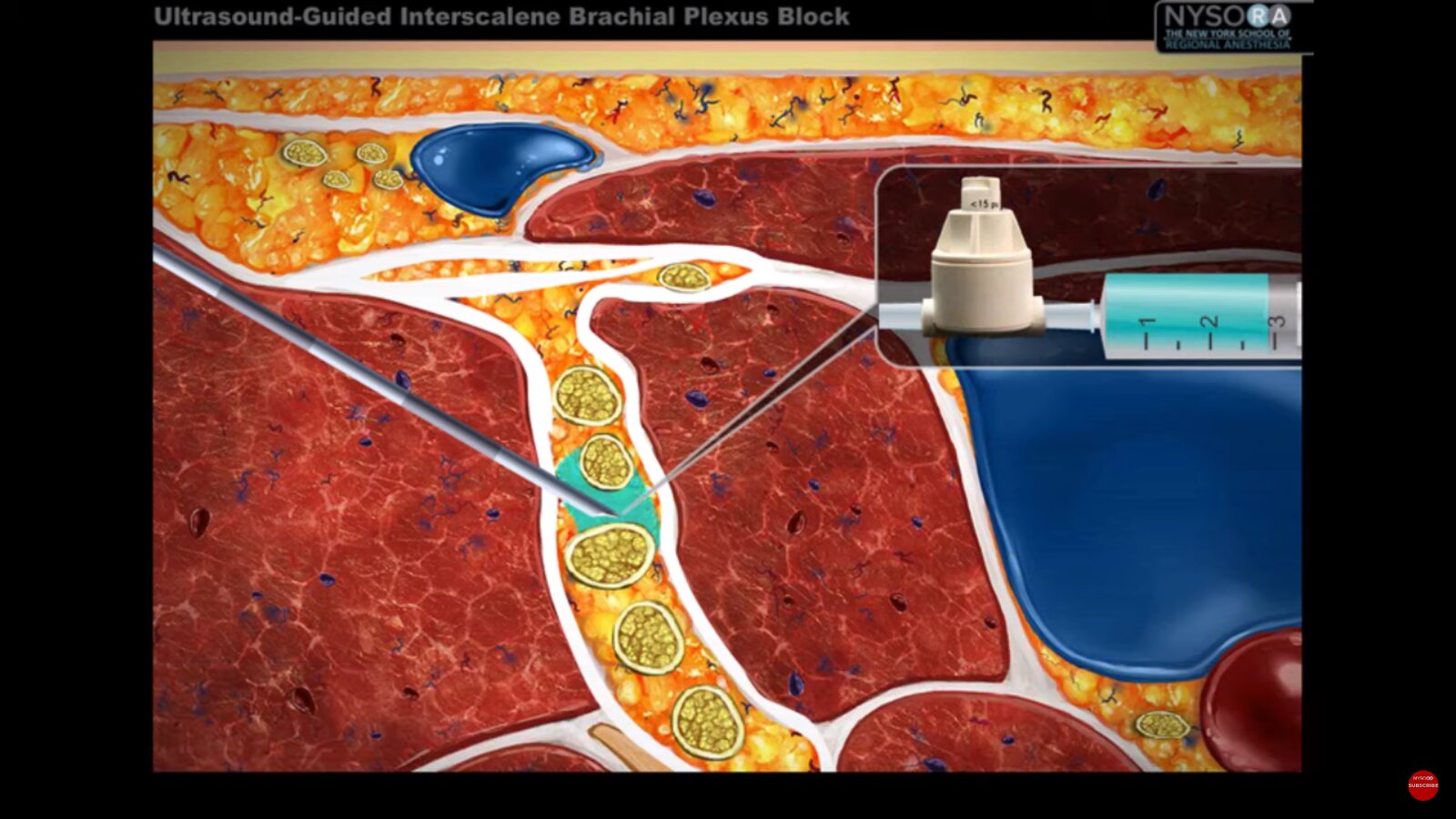
Technique: varies based on the target nerve
- Place the patient in a position that allows easy access to the target nerves.
- Perform skin preparation and maintain a sterile field.
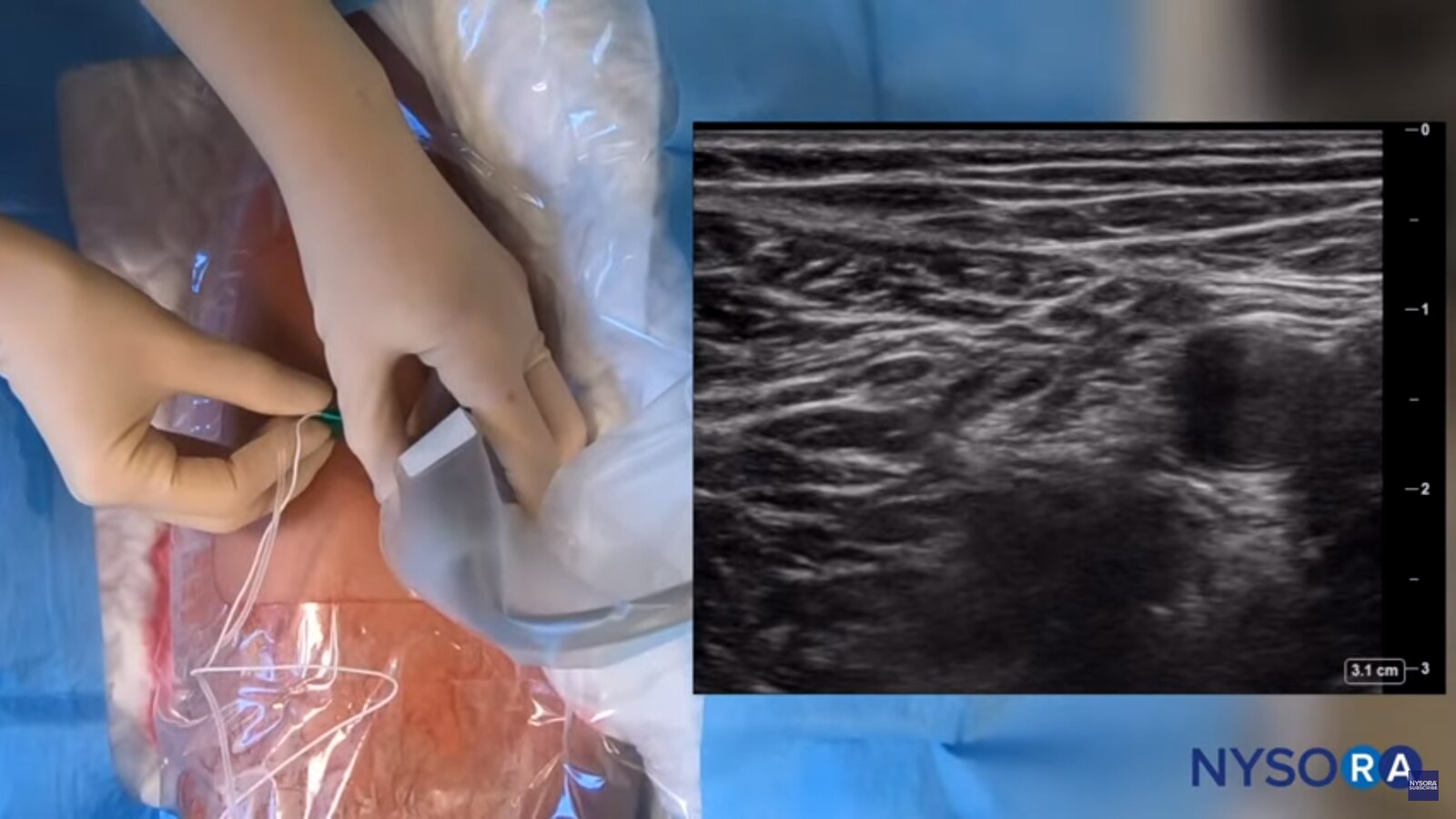
- Identify the targeted nerve using anatomical landmarks and/or:
- Ultrasound
- Nerve stimulation test
- Inject the local anesthetic agent around the target nerve.





Complications
See “Complications of regional anesthesia.”
Peripheral nerve blocks do not carry the risks associated with general anesthesia (e.g., respiratory depression, aspiration) and neuraxial anesthesia (e.g., CSF leak syndrome, urinary retention). [1]
Avoid discharging patients after major nerve blocks until sensation and function have returned to baseline levels to reduce the risk of secondary injury. [1]
Monitor for delayed-onset LAST, especially if high doses of local anesthetic agents were used.
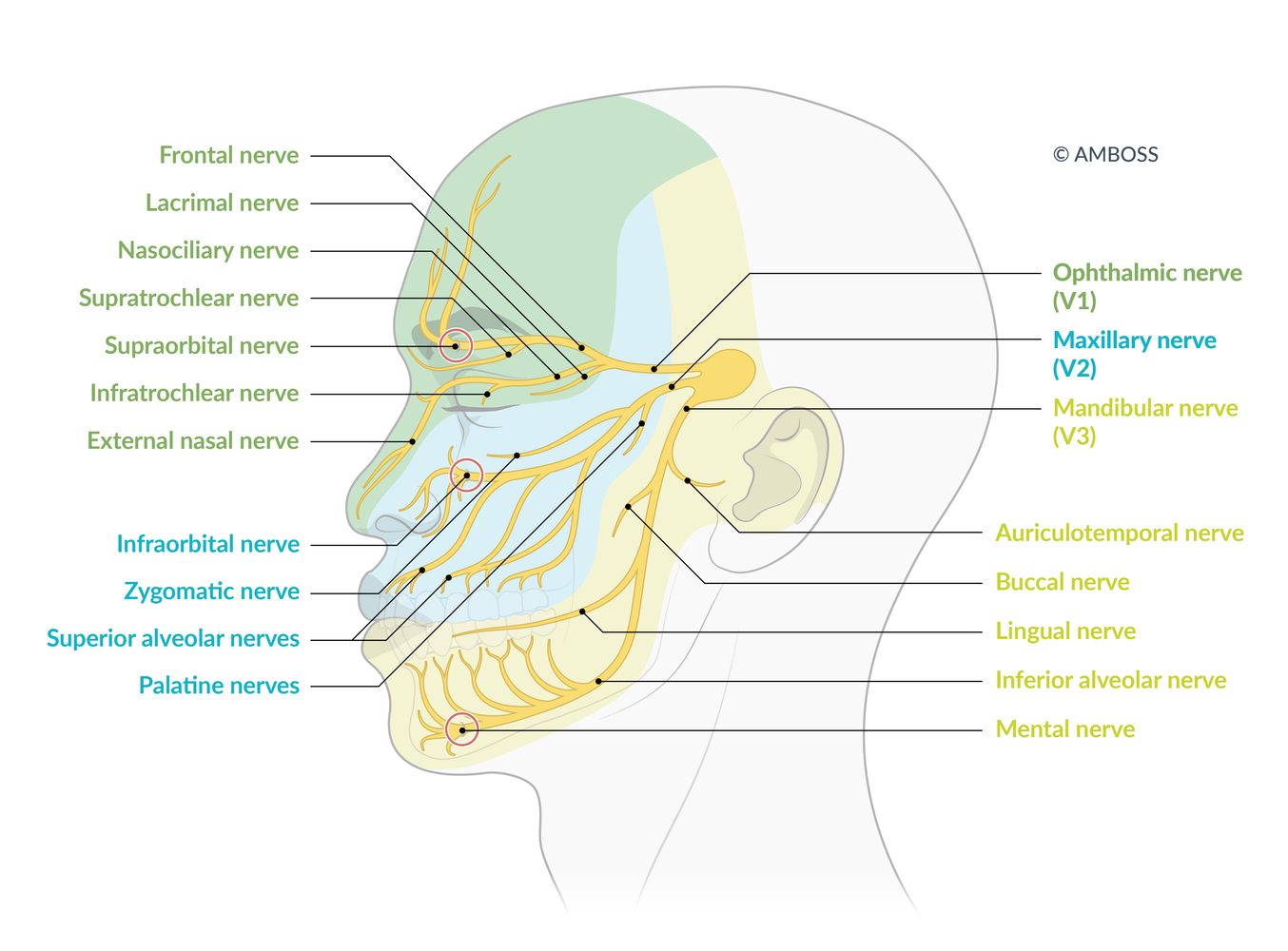
Illustrated are the 3 main branches of the trigeminal nerve (V1–V3), the areas in which they supply sensory innervation, and their subsidiary branches. The terminal superficial branches of V1–V3 are, respectively, the supraorbital, infraorbital, and mental nerves, which exit the skull at their eponymous foramina (marked with red circles). These exit points are clinically relevant as injection points for a superficial trigeminal nerve block.
© AMBOSS
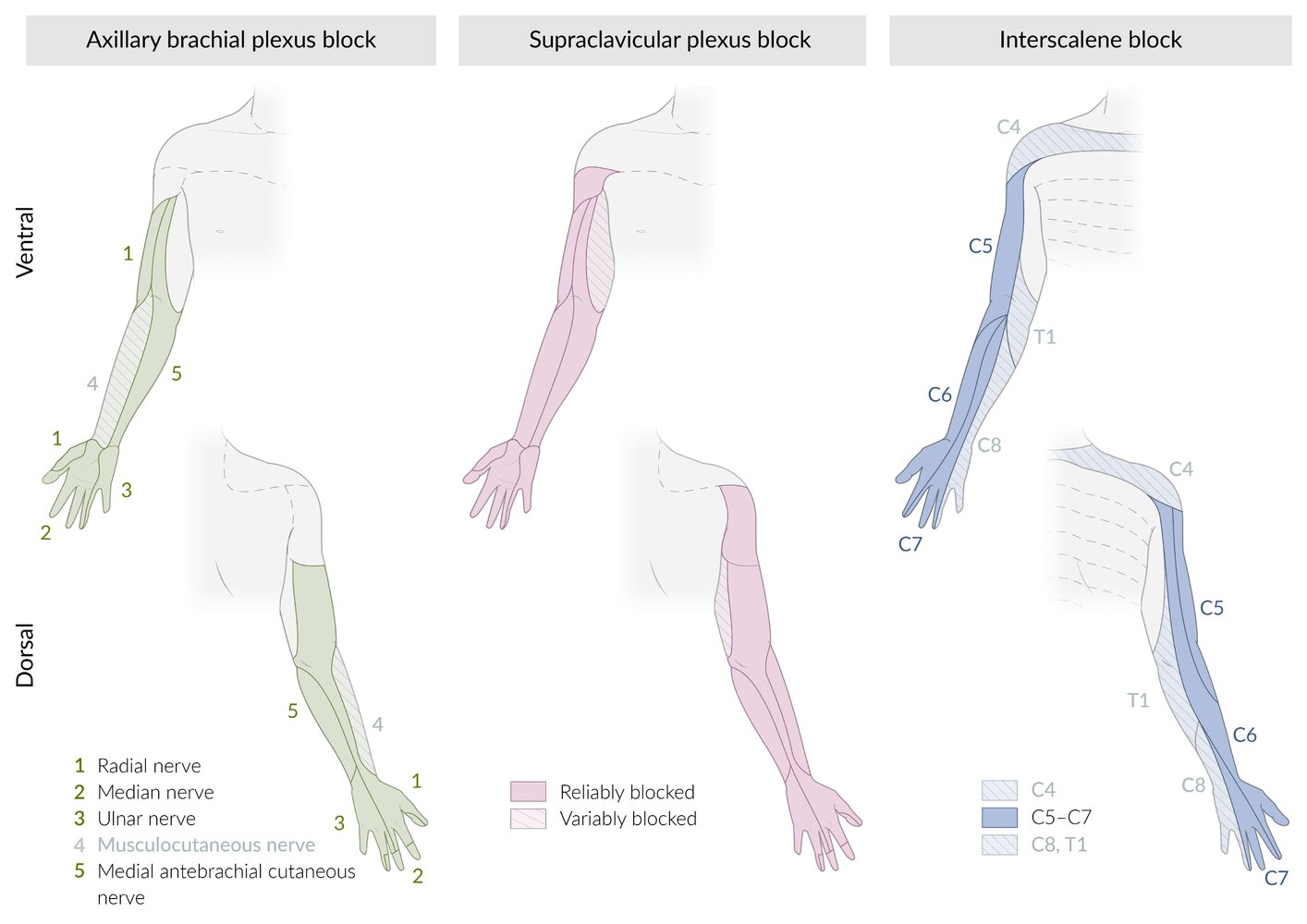
Dermatomal distributions affected by selected brachial plexus blocks
Left: The axillary brachial plexus block anesthetizes the terminal branches of the brachial plexus, providing reliable anesthesia to the solid green dermatomes. Depending on the technique used, the musculocutaneous nerve (hatched dermatome) may also be blocked.
Middle: The supraclavicular plexus block anesthetizes the trunks of the brachial plexus, providing reliable anesthesia to the solid pink dermatomes. The hatched region, innervated by the medial brachial cutaneous nerve (originating from the brachial plexus) and the intercostobrachial nerve (originating from the second intercostal nerve), is not reliably blocked.
Right: The interscalene block reliably anesthetizes nerve roots C5–C7 of the brachial plexus (solid blue dermatomes). Anesthesia to nerve roots C4, C8, and T1 (hatched dermatomes) may vary depending on the technique used and patient anatomy.
© AMBOSS
© AMBOSS
© AMBOSS
© AMBOSS
© AMBOSS
© AMBOSS
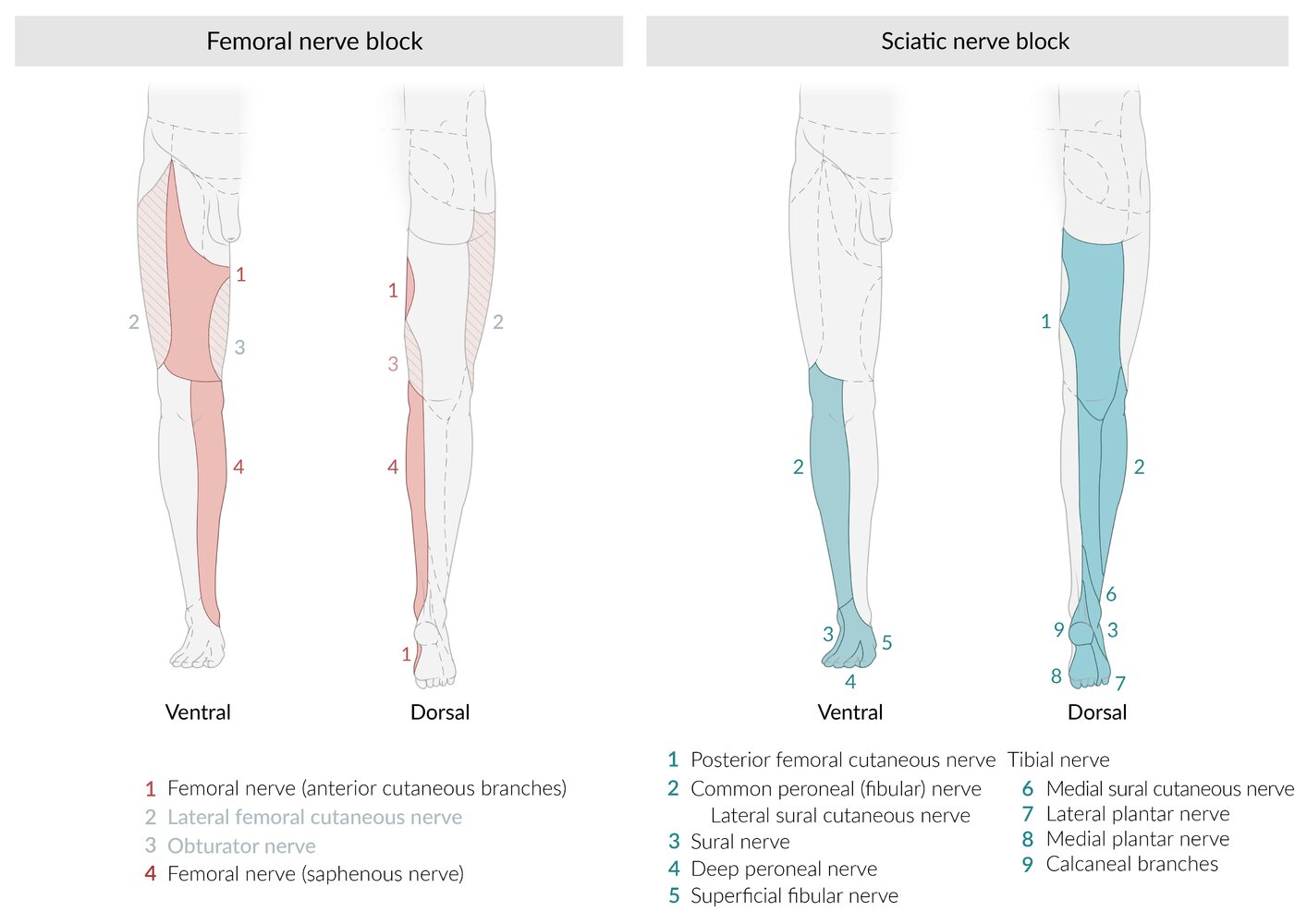
Dermatomal distributions affected by femoral and sciatic nerve blocks
Left: The femoral nerve block anesthetizes the entire region innervated by the femoral nerve (solid red dermatomes). Depending on the technique used, the lateral femoral cutaneous and obturator nerves may also be blocked (hatched dermatomes); this variation of the femoral nerve block is sometimes referred to as a “3-in-1 block.”
Right: The sciatic nerve block anesthetizes the entire region innervated by the sciatic nerve and its branches (blue dermatomes 2–9). Depending on the technique used, the posterior femoral cutaneous nerve (blue dermatome 1) may also be blocked.
© AMBOSS


Epidural anesthesia
Definition [4]
- Local anesthetics with or without opioids and alpha-adrenergic agonists are injected into the epidural space and act on the spinal nerve roots.
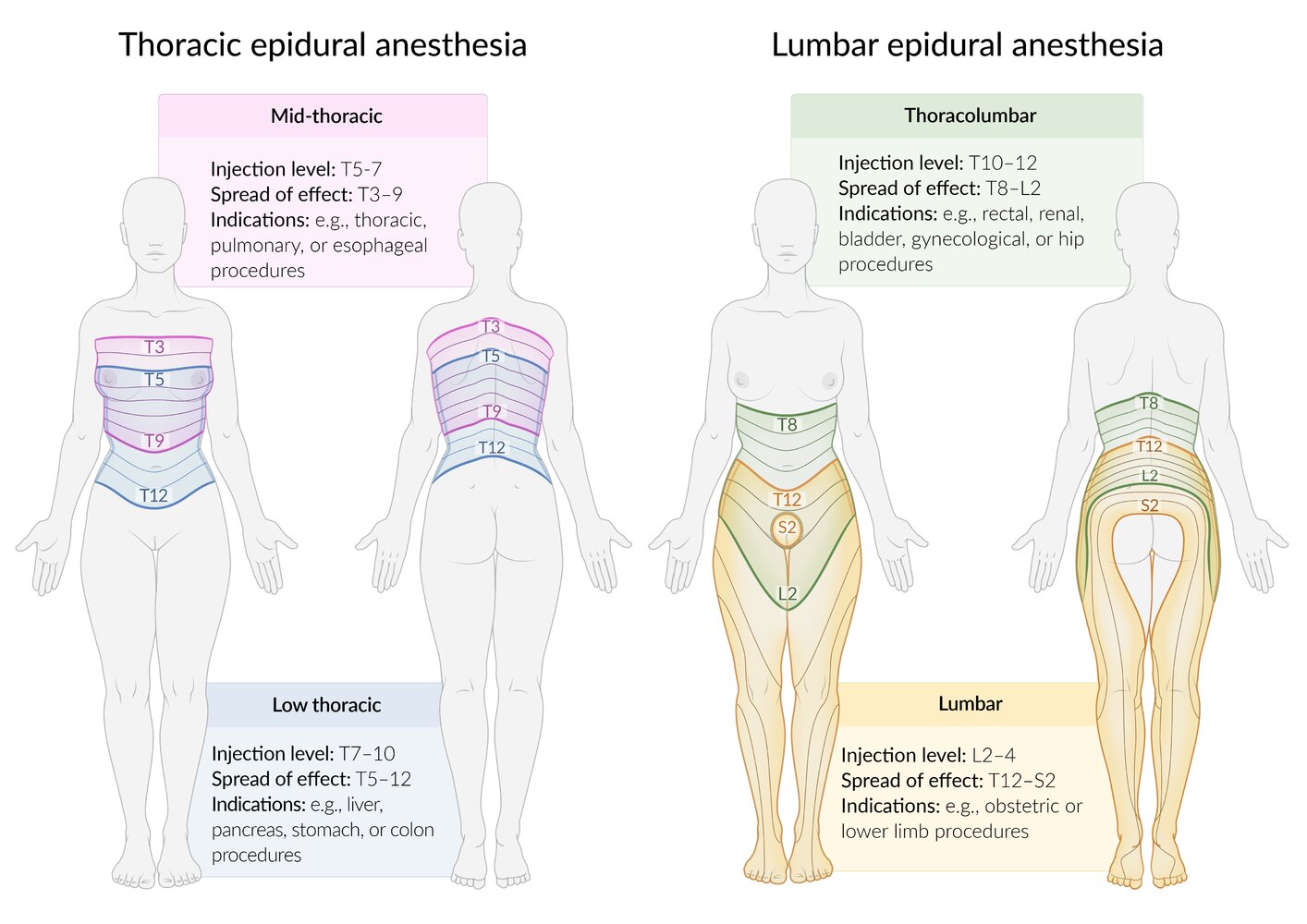
- Epidural anesthesia blocks several nerve roots around the site of injection and barely affects the function of the nerve roots above and below (segmental anesthesia).
Indications [4]
- Used for a variety of surgeries of the lower body (e.g., cesarean delivery, hernia repair, appendectomy, prostate and bladder surgeries, knee surgery)
- During labor
- Perioperatively
- Chronic pain management (e.g., spinal stenosis, disk herniation)
Contraindications [4]
See also “General contraindications to regional anesthesia.”
-
Absolute
- Uncorrected hypovolemia
- Increased intracranial pressure
- Infection at the puncture site
-
Relative
- Coagulopathy
- Spinal deformities
- Sepsis, systemic bacteremia, amniotic infection syndrome
- Neurological deficits caused by, e.g., disk prolapse, paraplegic syndrome, and multiple sclerosis
Procedure [4]
- Injection site
- May be performed at any vertebral level (cervical, thoracic and lumbar spine)
- Needle inserted into the epidural space between the ligamentum flavum and dura mater
- Approaches to inject the local anesthetic
- Catheter placement, which has the advantage of repeated/continuous administration of anesthetic drugs (most commonly performed)
- Single-shot technique

: materials and patient positioning")
: procedure")
Complications
See “Complications of regional anesthesia” and “Complications of neuraxial anesthesia.”
© AMBOSS
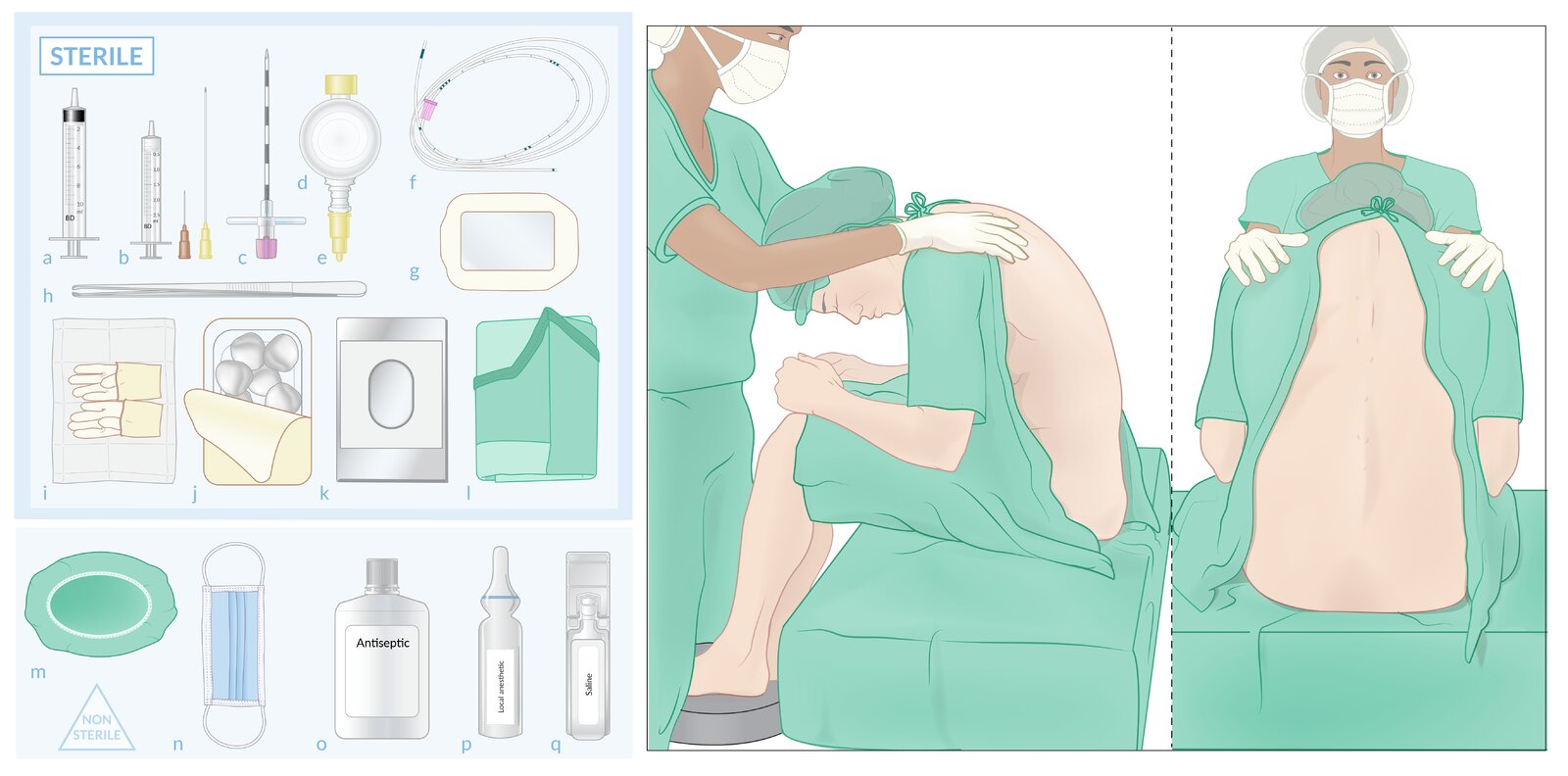
Sterile materials (upper left)
(a) Loss-of-resistance syringe
(b) Syringe with needles for superficial and deep local anesthesia
(c) Epidural needle
(d) Epidural filter with (e) adapter
(f) Epidural catheter
(g) Transparent dressing
(h) Surgical foreceps
(i) Gloves
(j) Surgical swabs
(k) Fenestrated surgical drape
(l) Surgical gown
Nonsterile materials (lower left)
(m) Surgical cap
(n) Surgical mask
(o) Antiseptic
(p) Local anesthetic
(q) Saline solution (to test loss of resistance)
Patient positioning (right): The patient is seated close to the edge of the bed, to bring their back as close as possible to the clinician performing the procedure. The feet rest on a stool. The patient is asked to hunch over, which flexes the spine and so widens the space between the spinous processes (without leaning forward, which increases lumbar lordosis). The arms may rest directly on the thighs or be propped up on pillows resting on the thighs. An assistant (wearing a surgical cap, mask, and non-sterile gloves) supports the patient in this position. The injection site and surrounding area should be fully visible and accessible.
© AMBOSS
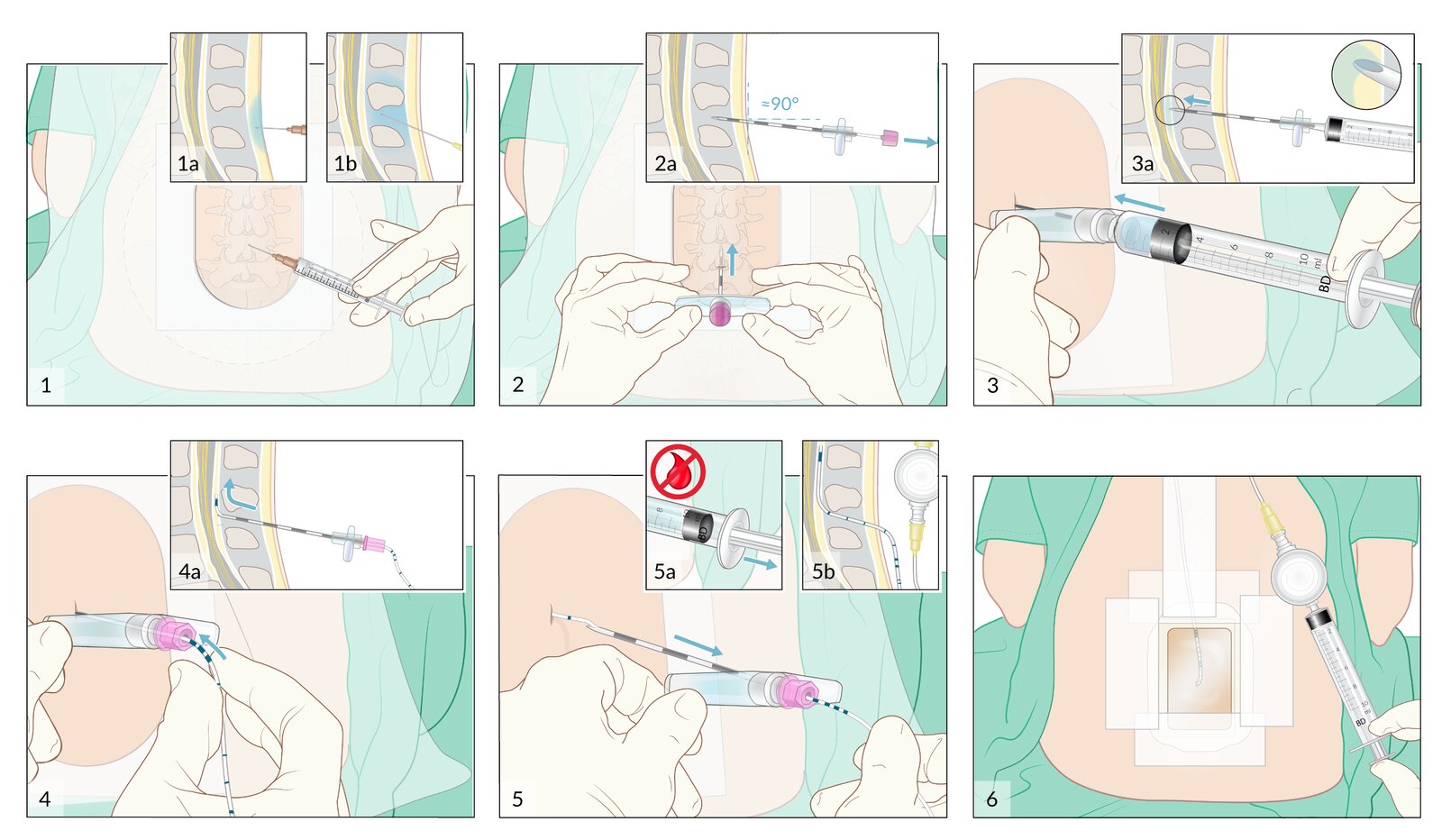
The injection site may be at any vertebral level (cervical, thoracic, and lumbar). This illustration shows a midline approach, but a paramedian approach is also possible.
(1) Local anesthetic is infiltrated into the subcutaneous tissue (1a) and interspinous ligament (1b).
(2) The epidural needle is inserted, angled slightly cephalad with the bevel orientated cephalad. Once the needle has been advanced by about 2–3 cm into the interspinous ligament, the stylet is removed and a loss-of-resistance syringe filled with saline is attached.
(3) The needle is advanced while applying constant, gentle pressure on the syringe plunger. After passing through the ligamentum flavum and entering the epidural space, a sudden loss of resistance is felt and the saline is more easily injected (3a); at this point, advancement is stopped.
(4) The syringe is removed and the epidural catheter is inserted through the needle to its correct depth (puncture depth + 4–6 cm). The tip of the catheter must always be advanced cephalad (4a); therefore, the bevel of the needle must remain facing cephalad.
(5) The epidural needle is removed, taking care to maintain the epidural catheter at the correct depth. At this time, aspiration is attempted from the catheter (5a: this should return neither blood nor CSF), and an epidural filter is attached (5b).
(6) The puncture site is covered with a transparent dressing and the catheter is secured to the patient's back with adherent dressings. A test dose is then administered.
© AMBOSS
Spinal anesthesia
Definition
- Local anesthetics with or without opioids and alpha-adrenergic agonists are injected into the cerebrospinal fluid (CSF) in the lumbar spine and act directly on the spinal cord
-
Combined spinal and epidural anesthesia (CSE)
- Combines the advantages of spinal anesthesia (rapid action, motoric block) with the advantages of epidural anesthesia (favorable post-operative pain management via an epidural catheter)
- Plays a major role in obstetrics and orthopedics.
Indications
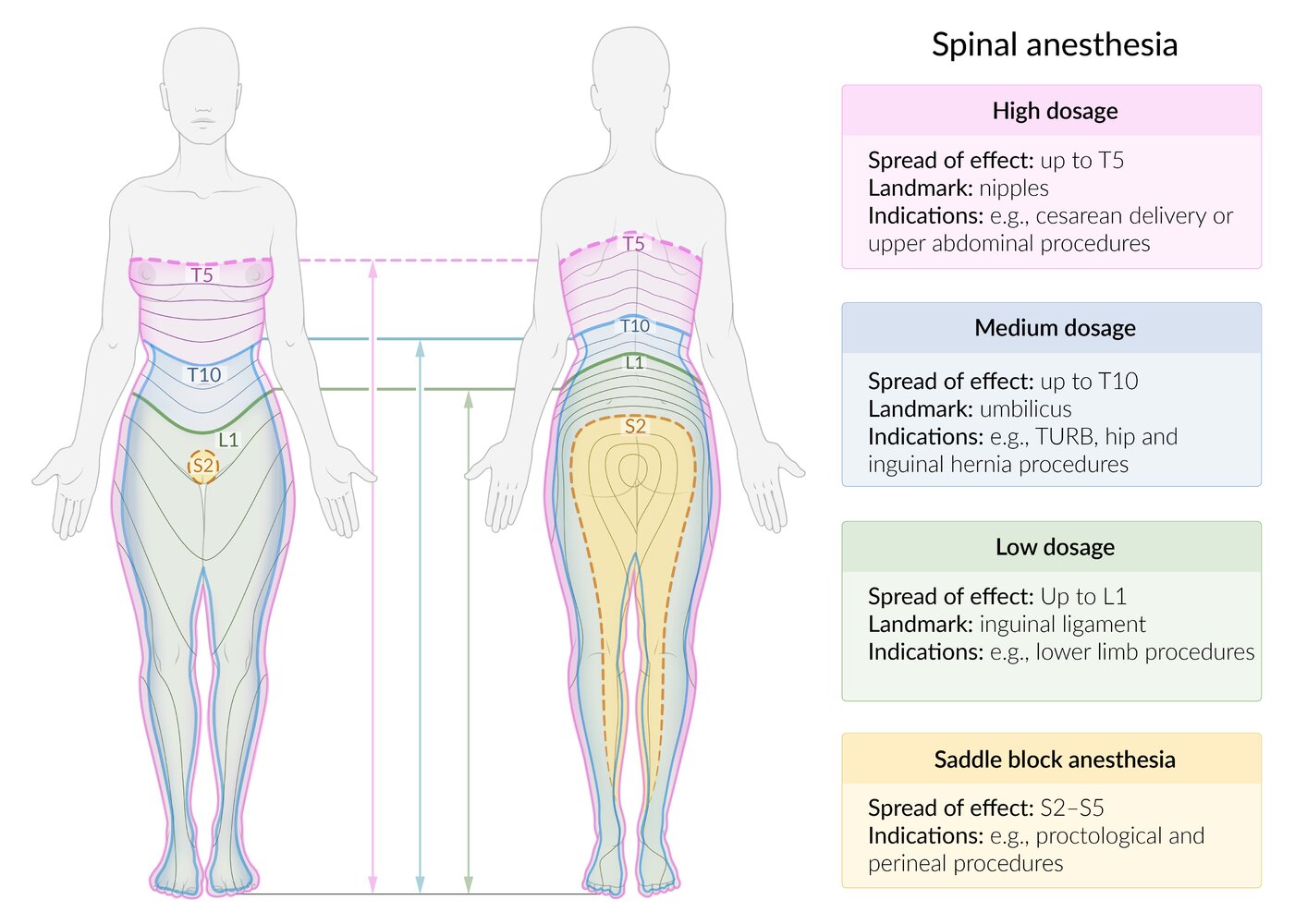
Used for a variety of lower extremity, lower abdominal, pelvic, and perineal procedures (e.g., cesarean delivery, hip and knee replacement), e.g:
- Cesarean delivery: T4–6 (mamillary line)
- Pelvic, urethral, and renal pelvic surgery: T6–8 (xiphoid)
- Transurethral surgery including stretching of the bladder, vaginal birth, hip surgery: T10 (navel)
- Transurethral surgery without stretching of the bladder: L1 (inguinal ligament)
- Knee and foot surgery: L2/3
- Perineal surgery: S2–5
Contraindications
See “Contraindications” in “Epidural anesthesia.”
Procedure
-
Injection site
- Injection usually performed below L2 to avoid damage to the spinal cord
- Needle inserted into subarachnoid space between the arachnoid and pia mater
- Approach: almost always single-shot technique


: materials and patient positioning")
: procedure")

Complications
See “Complications of regional anesthesia” and “Complications of neuraxial anesthesia.”
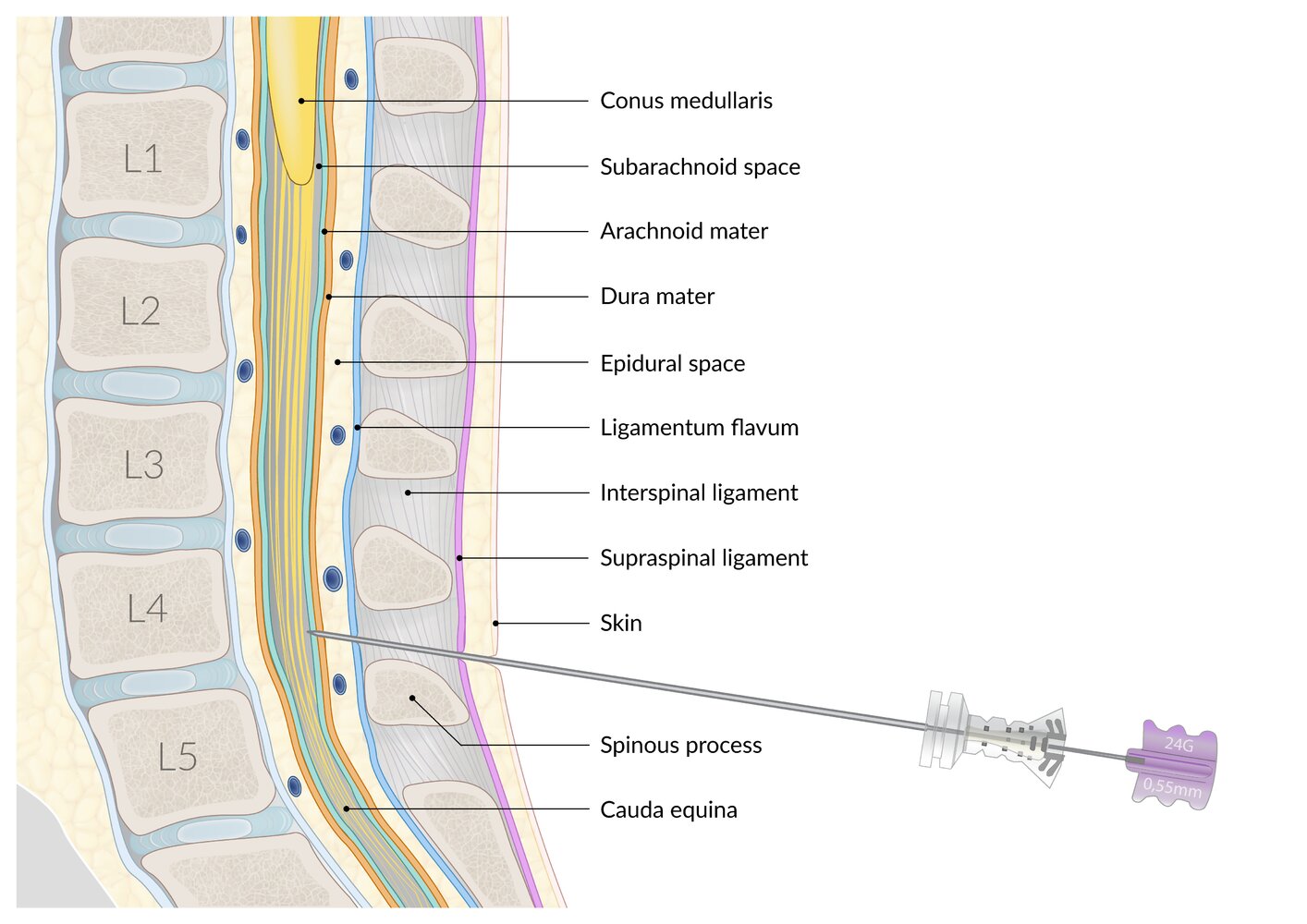
For lumbar puncture (including spinal anesthesia) the spinal needle is typically inserted in the L3-4 or L4-5 interspace and directed toward the umbilicus.
© AMBOSS
© AMBOSS

Sterile materials (upper left)
(a) Gloves
(b) Surgical swabs
(c) Fenestrated surgical drape
(d) Surgical gown
(e) Needle for local anesthesia
(f) Introducer needle
(g) Spinal needle
(h) Plaster
(i) 2 ml syringe
(j) 5 ml syringe
Nonsterile materials (lower left)
(k) Surgical cap
(l) Surgical mask
(m) Antiseptic
(n) Local anesthetic.
Patient positioning (right): The patient is seated close to the edge of the bed, to bring their back as close as possible to the clinician performing the procedure. The feet rest on a stool. The patient is asked to hunch over, which flexes the spine and so widens the space between the spinous processes (without leaning forward, which increases lumbar lordosis). The arms may rest directly on the thighs or be propped up on pillows resting on the thighs. An assistant (wearing a surgical cap, mask, and non-sterile gloves) supports the patient in this position. The injection site and surrounding area should be fully visible and accessible.
© AMBOSS
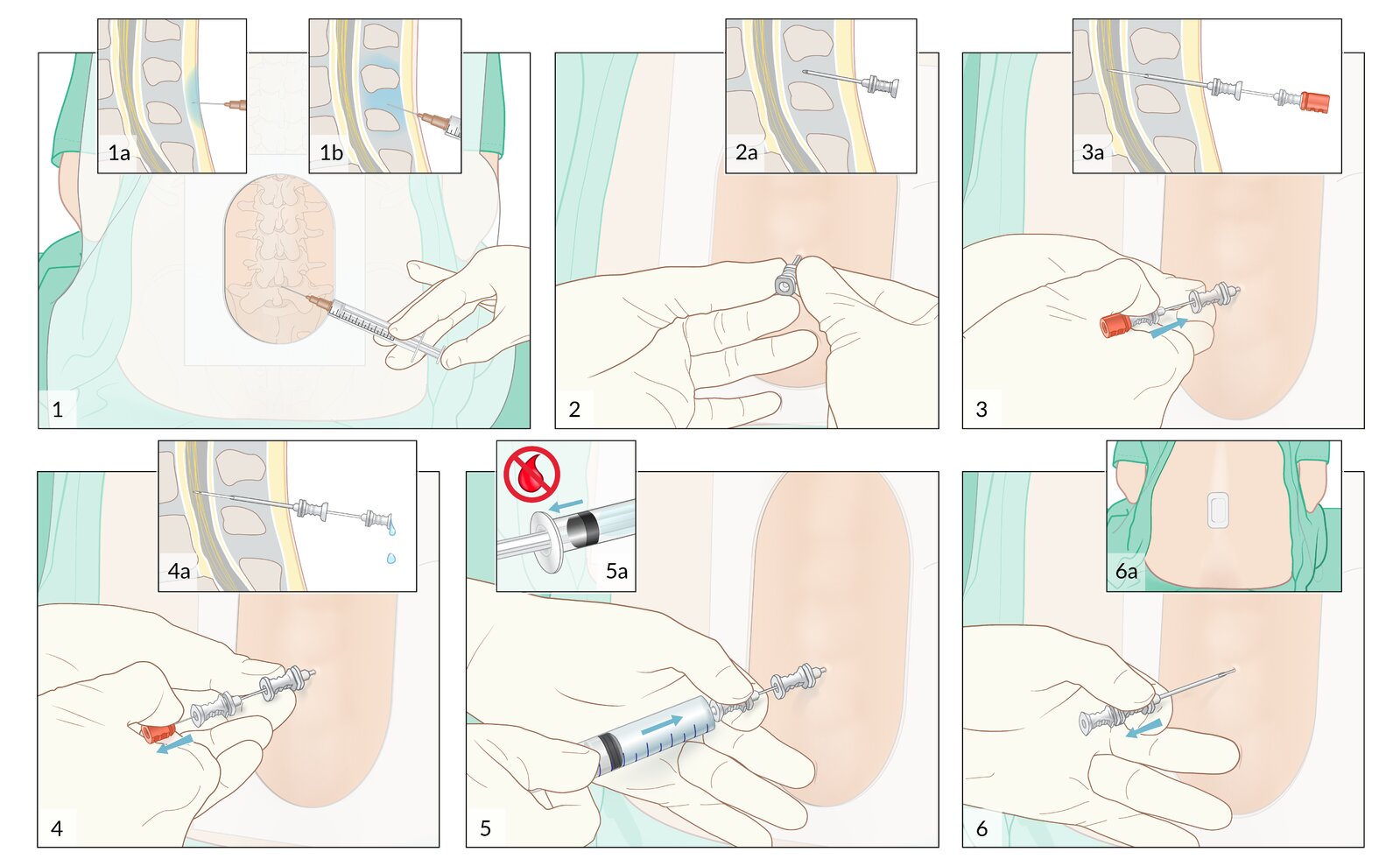
The injection site is usually at L3/L4 or L4/L5. This illustration shows a midline approach, but a paramedian approach is also possible.
(1) Local anesthetic is infiltrated into the subcutaneous tissue (1a) and interspinous ligament (1b).
(2) The introducer needle is inserted (slightly cephalad) into the interspinous ligament.
(3) The spinal needle is inserted through the introducer needle and through the ligamentum flavum, epidural space, dura- and arachnoid mater into the subarachnoid space (3a). The perforation of the dura mater may result in an audible and/or palpable click.
(4) The stylet is removed while stabilizing the introducer and spinal needles with the other hand. If positioned correctly, cerebrospinal fluid (CSF) will drip from the outer opening of the spinal needle (4a).
(5) A syringe with local anesthetic is connected to the spinal needle. A small amount of CSF is aspirated to ensure correct positioning; this should not be bloody (5a). Following this confirmation, the local anesthetic is slowly injected, while continuously monitoring the patient for signs of complications.
6) The introducer and spinal needles are removed together, and a sterile plaster is applied (6a).
© AMBOSS
© AMBOSS
Complications
See also “Adverse effects of local anesthetic agents.”
Complications of regional anesthesia [1]
- Nerve injury
- Local anesthetic systemic toxicity
- Hematoma
- Infection
- Secondary injury
Complications of neuraxial anesthesia [5][6][7]
- CSF leak syndrome
- Spinal epidural hematoma; and spinal epidural abscess
- Meningitis
-
Hypotension
- Pathophysiology: sympathetic blockade causes vasodilation and decreases venous return → reduced cardiac output
- Clinical features: hypotension, dizziness, lightheadedness, and nausea shortly after administering anesthetic
- Diagnostics: clinical diagnosis
- Treatment: IV fluid resuscitation + small doses of epinephrine
- Sympathetic block → peripheral vasodilation, bradycardia, and hypotension (Bezold-Jarisch reflex) → relative hypovolemia
- Postoperative urinary retention
- Back pain
- Anterior spinal artery syndrome
- Conus medullaris syndrome
Total spinal anesthesia [8]
- Definition: complete spinal space affected by local anesthetic drug
- Pathophysiology: drug overdose during spinal block or accidental spinal anesthesia during epidural block (intrathecal injection) → excessive cranial spread of the local anesthetic drug → inhibition of the intercostal respiratory muscles and sympathetic block → bradycardia and hypotension → reduced perfusion of the brainstem → total spinal anesthesia → circulatory and respiratory arrest
-
Clinical features
- Hypotension and cardiac decompensation
- Apnea
- Loss of consciousness
- Mydriasis (dilated pupils), fixed pupils
-
Prophylaxis: correct catheter placement
- Negative aspiration test: Aspiration of blood indicates a perforated blood vessel or intravascular placement of the catheter. Aspiration of CSF may be caused by catheter insertion into the intrathecal space.
- Intrathecal test dose injection : Numb legs point to a misplaced catheter.
-
Therapy
- Immediate intubation unless already performed
- Stabilization of BP via fluid resuscitation and catecholamines
We list the most important complications. The selection is not exhaustive.

MRI cervical spine (T2-weighted; sagittal plane) of a 58-year-old patient on long-term warfarin therapy presenting with acute tetraplegia
A region of heterogeneous signal lies along the posterior aspect of the spinal canal (indicated by arrows), between the dura and vertebral canal, representing a hematoma. The hematoma displaces the spinal cord anteriorly and compresses it, most prominently between the levels of C3 and C7. At the level of C7, there is an oval area of hyperintense signal within the spinal cord (arrowhead), representing myelopathic change (injury to the spinal cord).
Source: “Fig. 1, in: Anti-coagulation Drug Warfarin Contributes to Severe Adverse Outcomes in Prolonged Unsupervised Use: A Double-edged Sword” by Ordookhanian C, Kaloostian SW, Kaloostian PE, Cureus, licensed under CC BY 3.0. Modifications: Arrows have been removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
References
- Roberts JR. "Roberts and Hedges' Clinical Procedures in Emergency Medicine and Acute Care". Elsevier. (2018). ISBN: 9780323354783
- Turnbull DK, Shepherd DB. "Post-dural puncture headache: pathogenesis, prevention and treatment". Br J Anaesth. 91(5). :718-729. (2003)
- "Clinical Relevance of the Bezold–Jarisch Reflex". http://anesthesiology.pubs.asahq.org/article.aspx?articleid=1943118. [2003-05-01]
- Schrock SD, Harraway-Smith C. "Labor analgesia.". Am Fam Physician. 85(5). :447-54. (2012)
- Asfaw G, Eshetie A. "A case of total spinal anesthesia". International Journal of Surgery Case Reports. 76. :237-239. (2020)
- Sandeman DJ, Dilley AV. "Ultrasound guided dorsal penile nerve block in children.". Anaesth Intensive Care. 35(2). :266-9. (2007)
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904
- Ronald D. Miller, Manuel Pardo (Jr.). "Basics of Anesthesia". Elsevier Health Sciences. (2011). ISBN: 9781437716146
- Agabegi SS, Agabegi ED. "Step-Up To Medicine". Wolters Kluwer Health. (2015). ISBN: 9781496306142