Summary
Renal cell carcinoma (RCC), which originates from the renal tubular epithelium, is the most common renal malignancy in adults. Most cases are sporadic, but some hereditary disorders are also associated with the development of RCC. Major risk factors for RCC include smoking, acquired cystic disease of the kidney, nephrolithiasis, and long-term acetaminophen use. In the majority of cases, RCC is diagnosed following an incidental finding on imaging, and most patients are asymptomatic. Rarely, patients may present with the classic triad of flank pain, hematuria, and a palpable abdominal mass. Patients may also present with anemia, weight loss, and/or paraneoplastic manifestations such as hypercalcemia and hypertension. The primary imaging modality is an abdominal ultrasound, or CT or MRI with contrast. Most RCC tumors are resistant to radiotherapy and classical chemotherapeutic agents. Surgical resection is first-line treatment in nonmetastatic disease, and immunotherapy and targeted therapy, e.g., vascular endothelial growth factor (VEGF) and mammalian target of rapamycin (mTOR) inhibitors, are used in metastatic RCC. Patients with early-stage RCC with tumor growth limited to the kidney have a very good prognosis.
Epidemiology
- Prevalence: most common malignancy of the renal parenchyma (70% of renal cancers in adults are renal cell carcinoma)
-
Incidence [1]
- In 2020, an estimated 73,750 new cases will be diagnosed in the US.
- ♂ > ♀ (∼ 2:1)
- Peak incidence between 55 and 74 years
- Median age at diagnosis: 64 years
")
")
Epidemiological data refers to the US, unless otherwise specified.
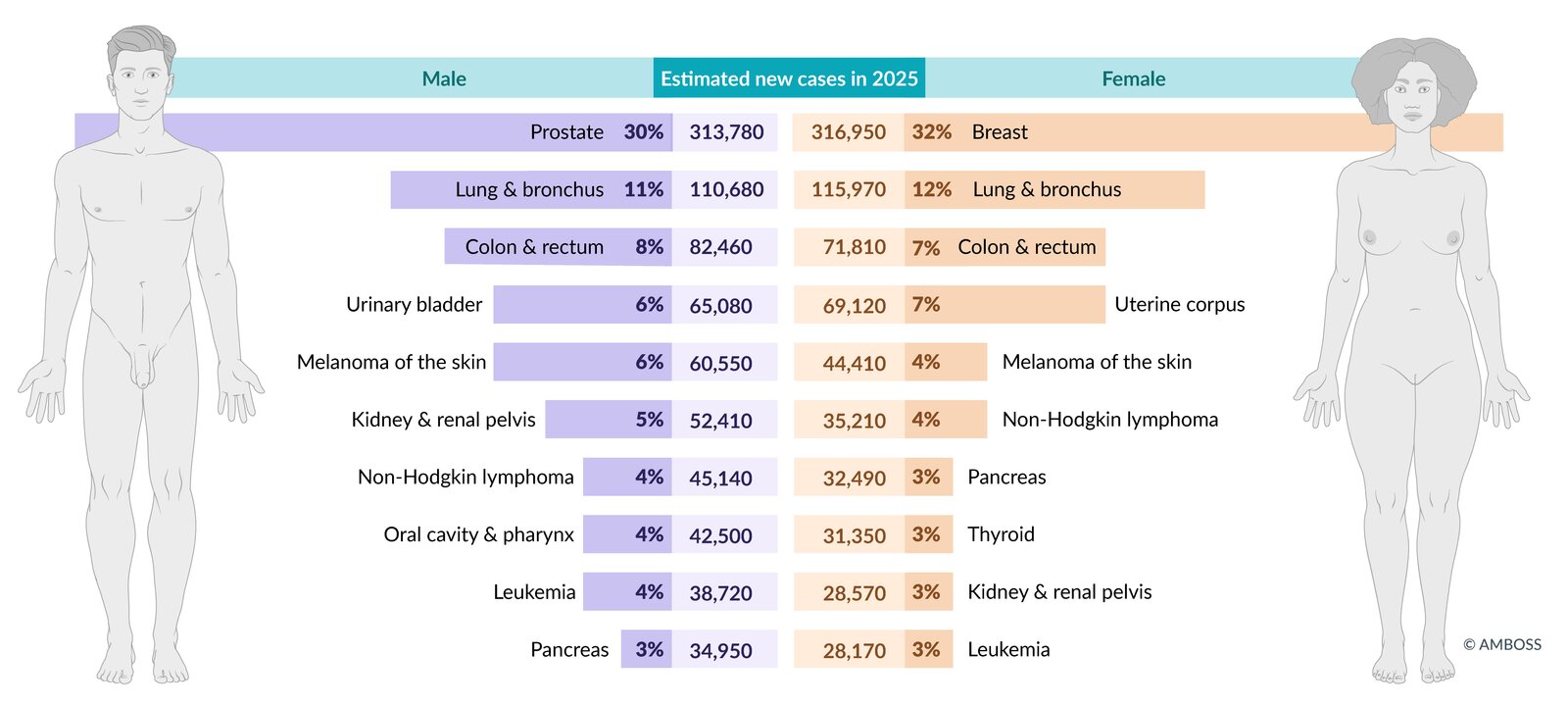
Estimated incidence of the most common cancers in the US in total figures and as a percentage of total cancer incidence (excluding non-melanoma skin cancers and in-situ carcinoma, except urinary bladder). Figures are prospective estimates of the American Cancer Society for 2025.
© AMBOSS. Data source: Cancer Facts & Figures 2024, American Cancer Society, access date 06/28/24 (https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2024/2024-cancer-facts-and-figures-acs.pdf)
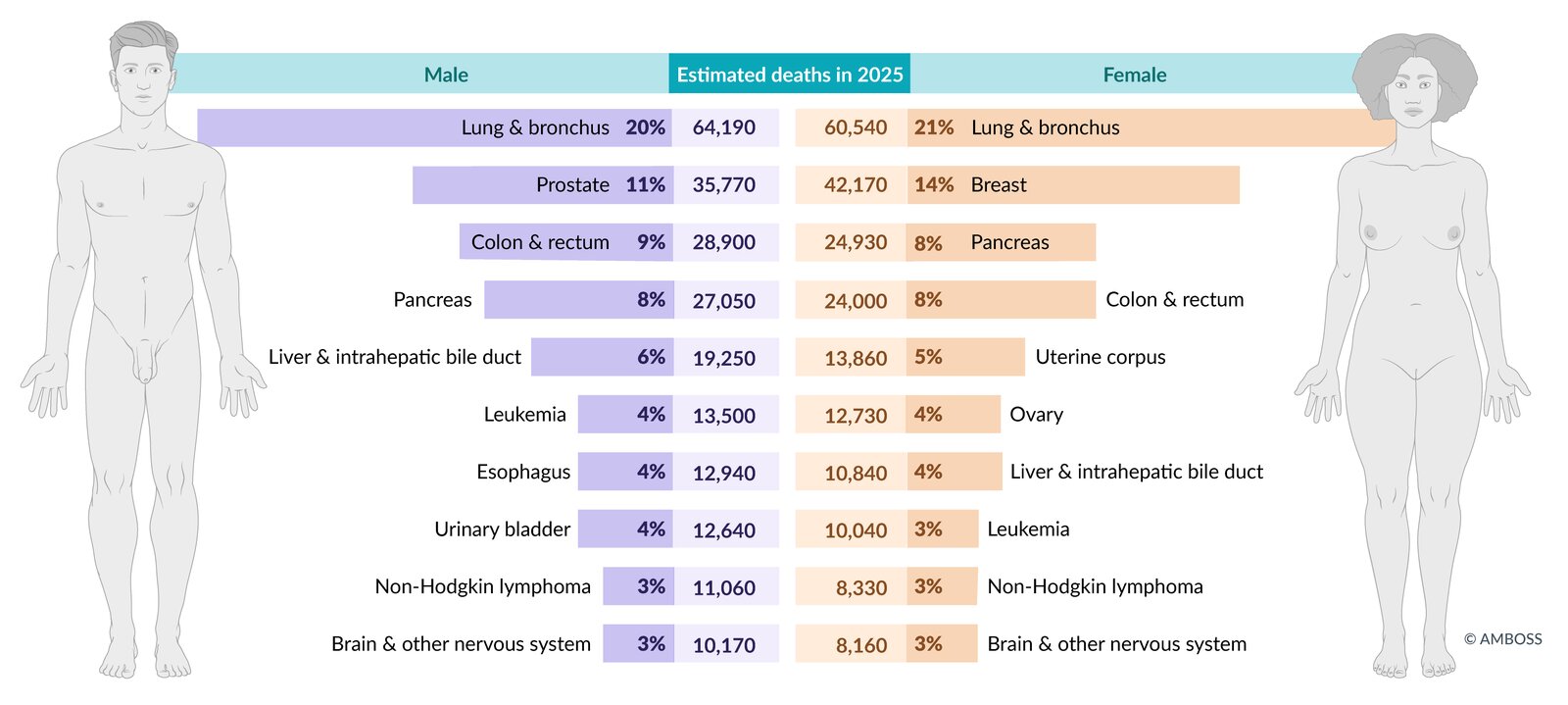
Estimated mortality from the most common cancers in the US in total figures and as a percentage of total cancer mortality. Figures are prospective estimates of the American Cancer Society for 2025.
© AMBOSS. Data source: Cancer Facts & Figures 2024, American Cancer Society, access date 06/28/24 (https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2024/2024-cancer-facts-and-figures-acs.pdf)
Etiology
Overview
- Most renal cell carcinomas (RCCs) occur sporadically.
- Approx. 4% of renal cell carcinomas are associated with hereditary factors.
- Both forms show structural alterations of the short arm of chromosome 3 (3p) and subsequent alterations of the VHL gene.
Risk factors for sporadic RCC [2][3]
-
Lifestyle
- Smoking
- Obesity
-
Associated conditions
- Sickle cell disease
- Acquired cystic kidney disease [4]
- Renal pelvic stones
- Hypertension
- Immunodeficiency
- Chronic hepatitis C infection
-
Substance exposure
-
Occupational exposure to:
- Cadmium
- Asbestos
- Petroleum by-products such as trichloroethylene (a degreasing agent)
- Chemotherapeutic agents (e.g., cisplatin) during childhood
- Chronic analgesic use (acetaminophen, aspirin)
-
Occupational exposure to:
Hereditary renal cell carcinomas [3]
- Von Hippel-Lindau syndrome: Approx. 40% of patients with VHL syndrome develop renal cell carcinomas (usually clear cell RCC).
-
Tuberous sclerosis
- ∼ 5% of people with tuberous sclerosis develop renal cell carcinomas (usually clear cell RCC).
- RCC that is associated with tuberous sclerosis occurs more commonly in women.
-
Birt-Hogg-Dube syndrome
- Inherited autosomal dominant condition caused by a mutation in the folliculin (FLCN) gene on chromosome 17
- Characterized by the following symptoms:
- Skin lesions: fibrofolliculomas, benign hamartomatous tumors of hair follicles
- Lung cysts
- Renal cell carcinoma (usually chromophobic RCC or oncocytic RCC)
-
Hereditary leiomyomatosis and renal cancer syndrome (HLRCC)
- Autosomal dominant condition caused by a mutated fumarate dehydrogenase gene located on chromosome 1
- Characterized by cutaneous and uterine leiomyomas
- 15% develop type 2 papillary RCC
-
Hereditary papillary renal cell carcinoma (HPRCC)
- Autosomal dominant condition with a high penetrance
- Caused by activating mutations of the MET proto-oncogene located on the long arm of chromosome 7
- Usually associated with type 1 papillary RCC
- Succinate dehydrogenase deficiency: autosomal dominant condition associated with pheochromocytomas, extra-adrenal paragangliomas, and renal cell carcinoma.
Hereditary renal cell carcinomas are autosomal dominant and tend to affect patients at a younger age than sporadic renal cell carcinomas.
Clinical features
-
Overview
- Usually asymptomatic in the early stages
- Patients become symptomatic when the tumor has reached a large size (usually > 10 cm) and/or if metastases are present.
-
Constitutional symptoms
- Weight loss, fatigue
- Fever, night sweats
- Anemia
-
Symptoms caused by primary tumor
- Hematuria
- Flank pain
- Palpable renal mass
- Symptoms of local spread and metastatic disease: see “Complications” below
The classical triad of renal cell carcinoma consists of hematuria, flank pain, and a palpable flank mass. However, only 10–15% of patients present with all three components of the triad and > 25% present with one or more atypical symptoms related to paraneoplastic syndromes and/or disseminated disease. [5]
Staging
TNM classification (8th Edition, 2017)
| Overview of TNM classification | |
|---|---|
| TNM | Tissue invasion |
| T1 |
|
| T2 |
|
| T3 |
|
| T4 |
|
| N0 |
|
| N1 |
|
| M0 |
|
| M1 |
|


AJCC staging (8th Edition, 2017)
| Overview of AJCC stages | |
|---|---|
| AJCC stage | TNM |
| Stage I |
|
| Stage II |
|
| Stage III |
|
| Stage IV |
|
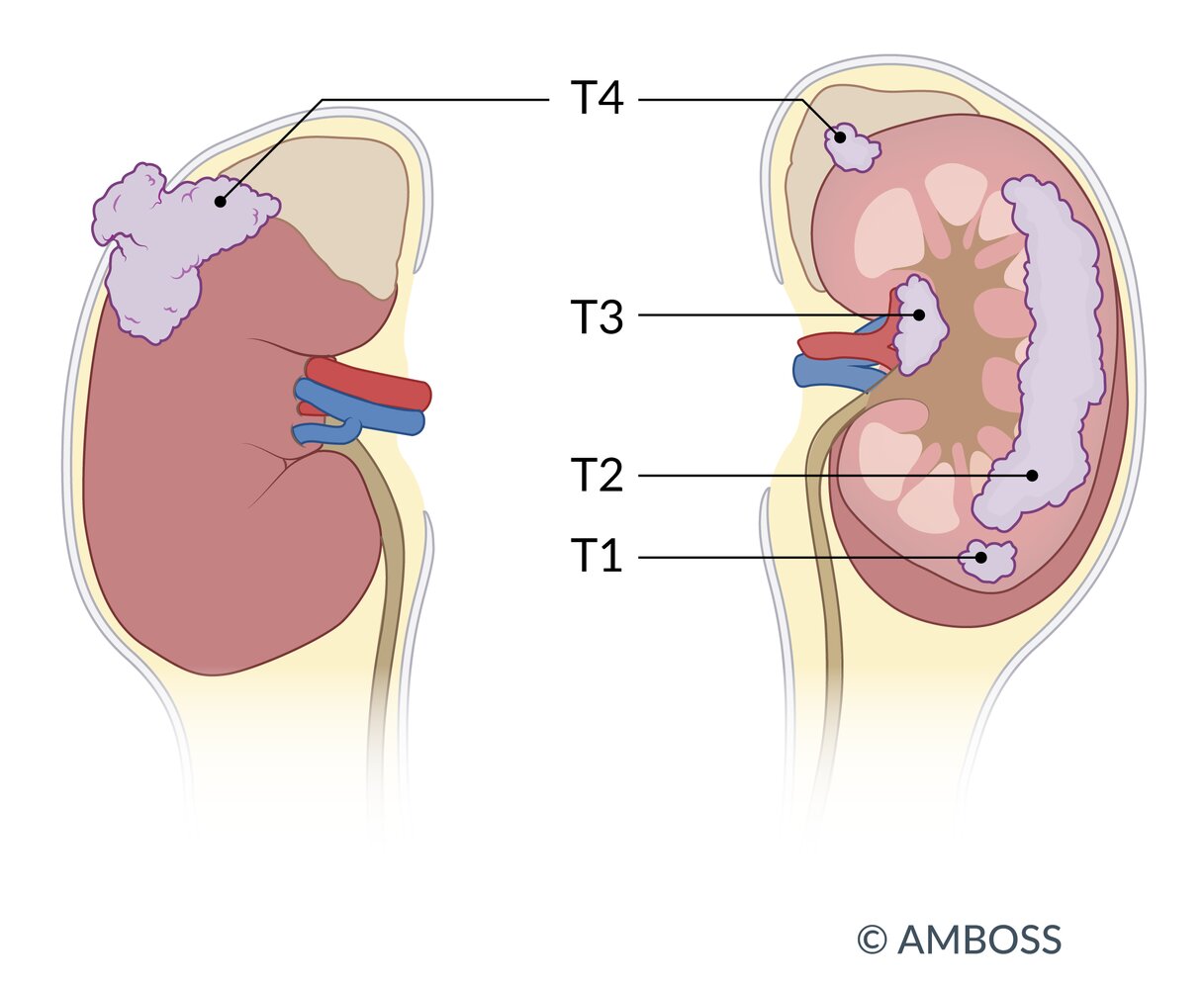
T1: tumor limited to the kidney; tumor size < 7 cm (T1a: < 4 cm; T1b: 4–7 cm)
T2: tumor limited to the kidney; tumor size > 7 cm, (T2a: 7–10 cm; T2b: > 10 cm)
T3: tumor extends into major veins or perinephric tissues but not into the ipsilateral adrenal gland or beyond the Gerota fascia
T4: tumor invades beyond the Gerota fascia or the ipsilateral adrenal gland
© AMBOSS
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
Diagnosis
Approach [6][7]
Most renal masses are detected incidentally on imaging performed for another indication or to evaluate nonspecific symptoms.
- Obtain additional imaging in patients with an indeterminate mass. [8]
- Preferred: CT or MRI abdomen (with IV contrast)
- Alternative: ultrasound abdomen (with IV contrast)
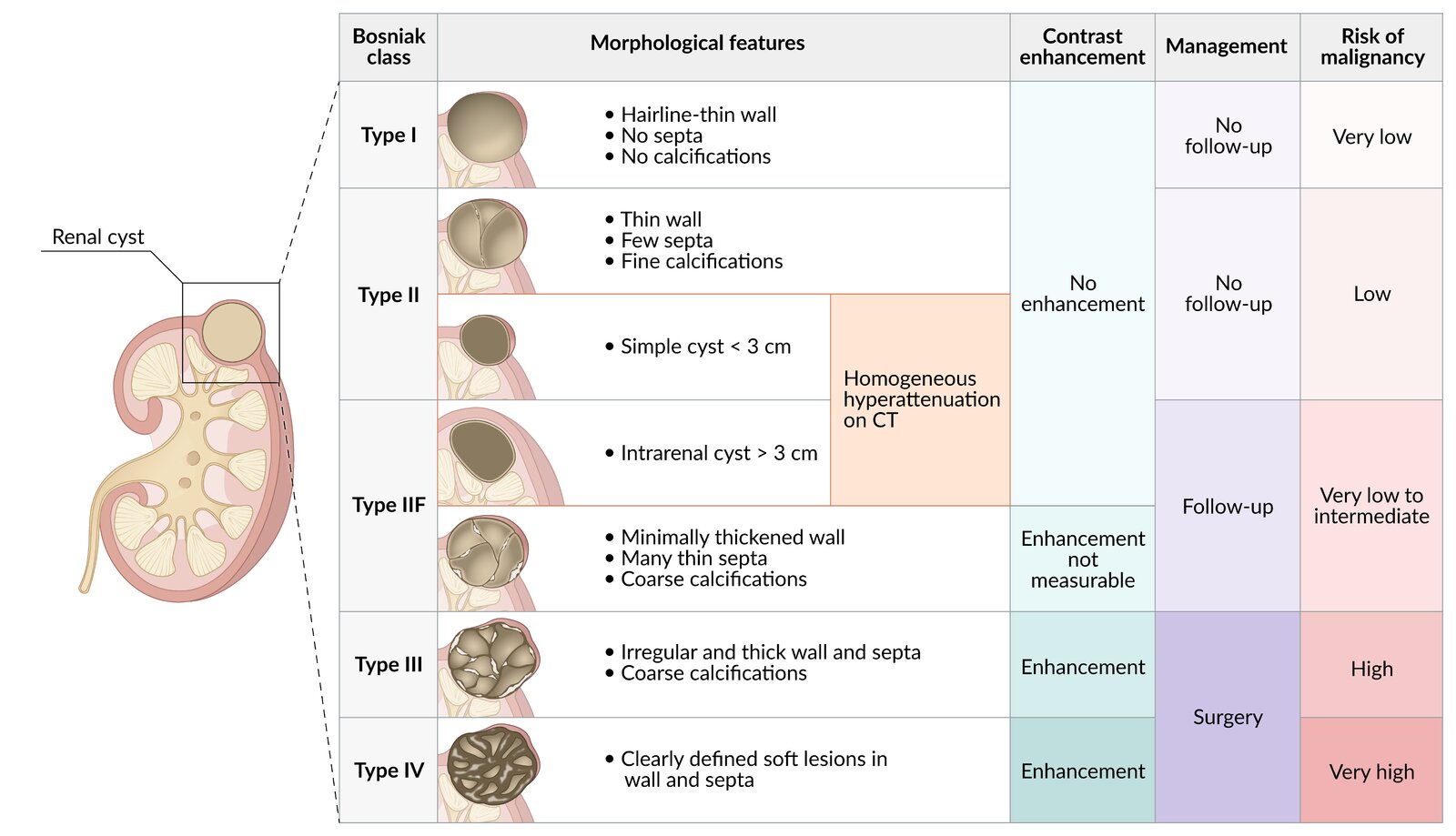
- Pursue workup based on imaging findings (e.g., repeat imaging for Bosniak IIF cystic mass).
Hematuria may be the initial presentation of RCC. Patients ≥ 35 years of age with asymptomatic microhematuria, and all patients with gross hematuria in the absence of a UTI, should be referred to urology. [7]
Imaging
- Overview: Most renal masses are detected incidentally on imaging performed for another indication or to evaluate nonspecific symptoms.
-
Indications
- Characterization of lesions (e.g., size, regular or irregular walls).
- Identification of lymph node and/or renal vein involvement. [9][10]
-
Modalities and characteristic findings: Abdominal CT, MRI, or ultrasound (with IV contrast) are first-line modalities. ; [6][8]
- CT abdomen (with IV contrast; multiphase renal protocol)
- Lesion(s) with thickened irregular walls, calcification, and variable enhancement [10][11][12]
- Distorted renal outline
-
MRI abdomen (with IV contrast; multiphase renal protocol) [8][9]
- May be preferred for the assessment of small lesions (< 1.5 cm) and Bosniak IIF or III cystic renal masses
- Can provide additional information on IVC invasion if findings are unclear on a CT scan [9]
-
Ultrasound abdomen (with IV contrast)
- Preferred study in patients with contraindications to iodinated contrast for CT and gadolinium-based contrast for MRI.
- Can identify renal lesion(s) with variable echogenicity [10]
- CT abdomen (with IV contrast; multiphase renal protocol)
| Workup based on imaging findings [6][7][10] | |
|---|---|
| Findings | Next steps |
|
|
|
|
|
|

")
")
")


Metastatic evaluation
These may be considered in consultation with a urologist.
-
CT or MRI chest (with IV contrast): indicated in patients with large tumors [15][16]
- May reveal pulmonary cannonball metastases [17]
- Other common metastatic sites: bone, lymph nodes, liver [18]
- Bone scan: may be indicated in patients with bone pain and/or ↑ ALP [9]
- CT or MRI head: indicated in patients with neurological signs or symptoms [15]
- Other modalities: Metastases may be an incidental finding on initial imaging, e.g., abdominal ultrasound.

Laboratory studies and urinalysis
-
Urinalysis
- Can show frank and microscopic hematuria [19]
- Measure albumin:creatinine ratio if proteinuria is detected. [6]
-
Laboratory studies [6][14][19]
-
CBC
- Abnormal hemoglobin levels
- ↑ WBC and/or ↑ platelets [20][21][22]
-
CMP
- Hypercalcemia
- ↑ AST, ALT, and/or ALP
- ↑ BUN:creatinine ratio
-
CBC
Further investigations
- Renal mass biopsy: only required if it may alter the management or is requested by the patient. [6][23]
- Split renal function [9]
Refer patients ≤ 46 years of age with renal malignancy and those with multifocal or bilateral renal masses or other findings suggestive of familial RCC for genetic counseling. [6]
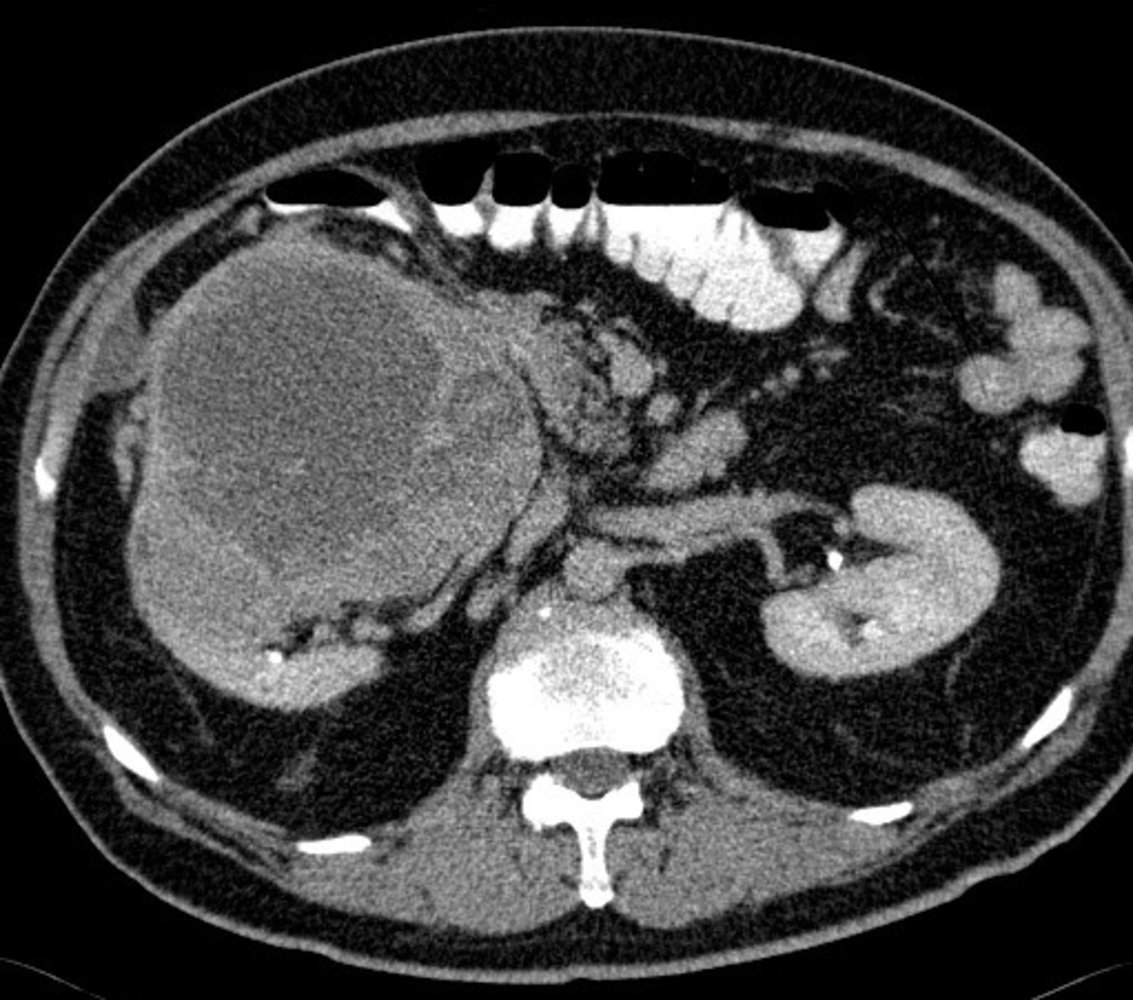
CT abdomen (with oral and IV contrast; axial plane) of patient with a history of renal cell carcinoma
A large mass with peripheral enhancement (blue overlay) and central necrosis (yellow overlay) arises from the mid pole of the right kidney.
A: abdominal aorta; C: colon; K: left kidney; P: pancreas
Our great thanks to Dr. Kissig (Center for Diagnostic and Interventional Radiology, Hedwigshöhe, St. Hedwig, Berlin, and St. Josefs Hospital, Potsdam) for kindly providing this image.
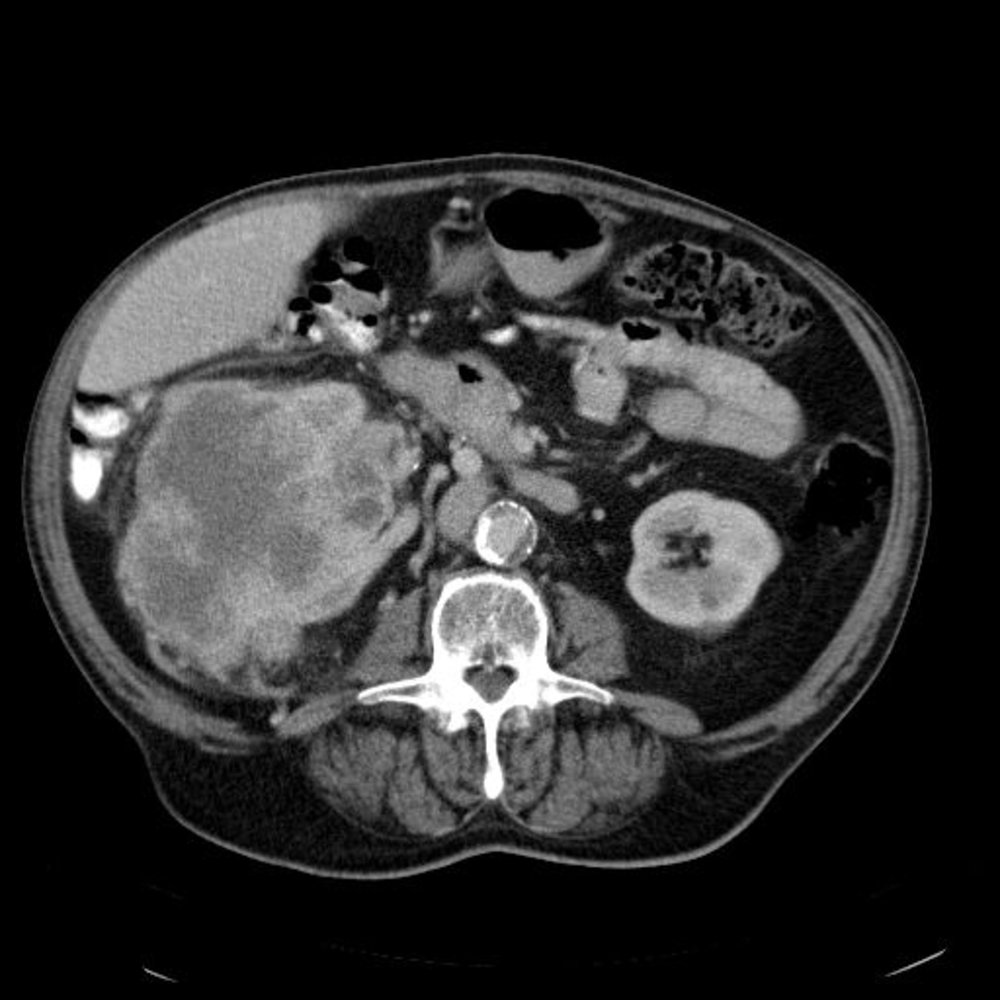
CT abdomen (with oral and IV contrast; axial plane) of a patient with history of renal cell carcinoma
A large mass with peripheral enhancement (blue overlay) and central necrosis (yellow overlay) arises from the mid pole of the right kidney. Soft tissue density (red overlay) visible in the perinephric space raises concern for extracapsular extension.
A: calcified abdominal aorta; C: colon; K: left kidney, L: liver
Our great thanks to Dr. Kissig (Center for Diagnostic and Interventional Radiology, Hedwigshöhe, St. Hedwig, Berlin, and St. Josefs Hospital, Potsdam) for kindly providing this image.
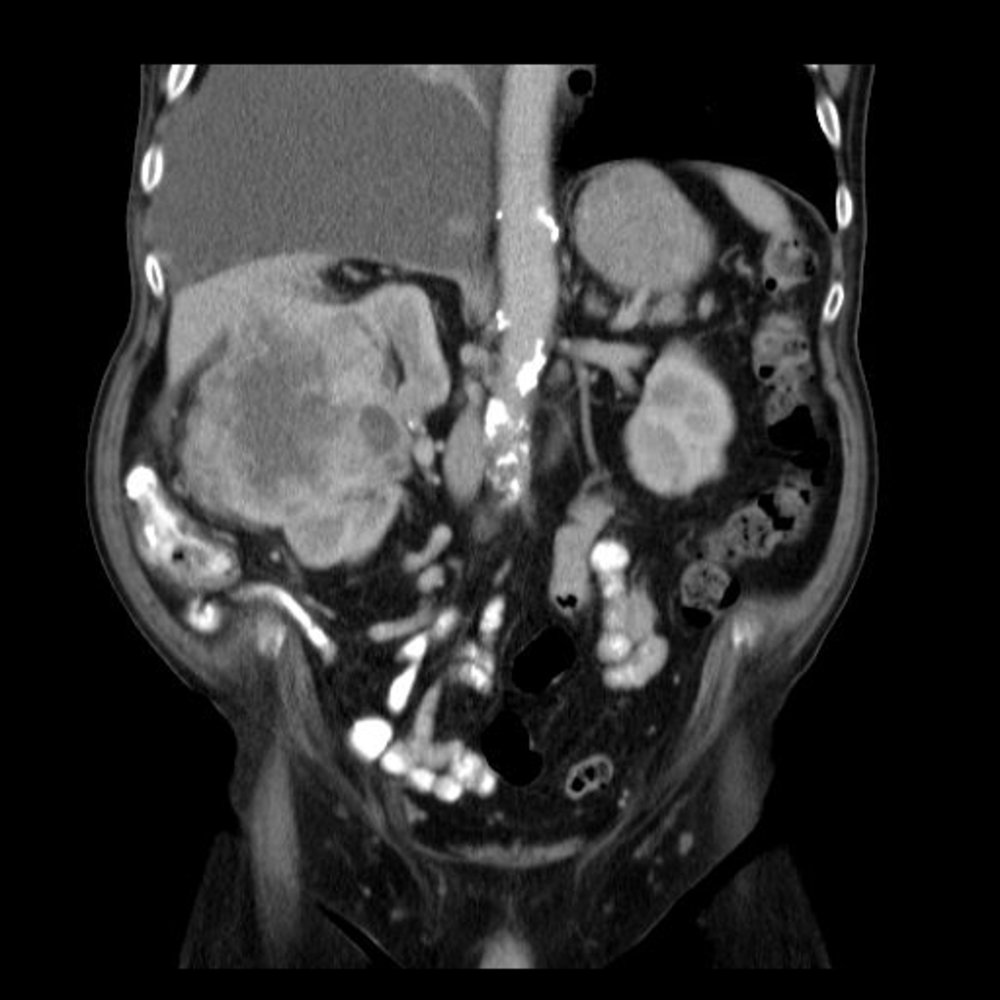
CT abdomen (with oral and IV contrast; coronal plane) of patient with a history of renal cell carcinoma
A large mass with peripheral enhancement (blue overlay) and central necrosis (yellow overlay) arises from the mid pole of the right kidney. Soft tissue density (red overlay) visible in the perinephric space raises concern for extracapsular extension. A large pleural effusion (outline) accompanied by passive atelectasis (green overlay) depresses the right hemidiaphragm.
A : calcified abdominal aorta; C: colon; K: left kidney; L: liver
Our great thanks to Dr. Kissig (Center for Diagnostic and Interventional Radiology, Hedwigshöhe, St. Hedwig, Berlin, and St. Josefs Hospital, Potsdam) for kindly providing this image.

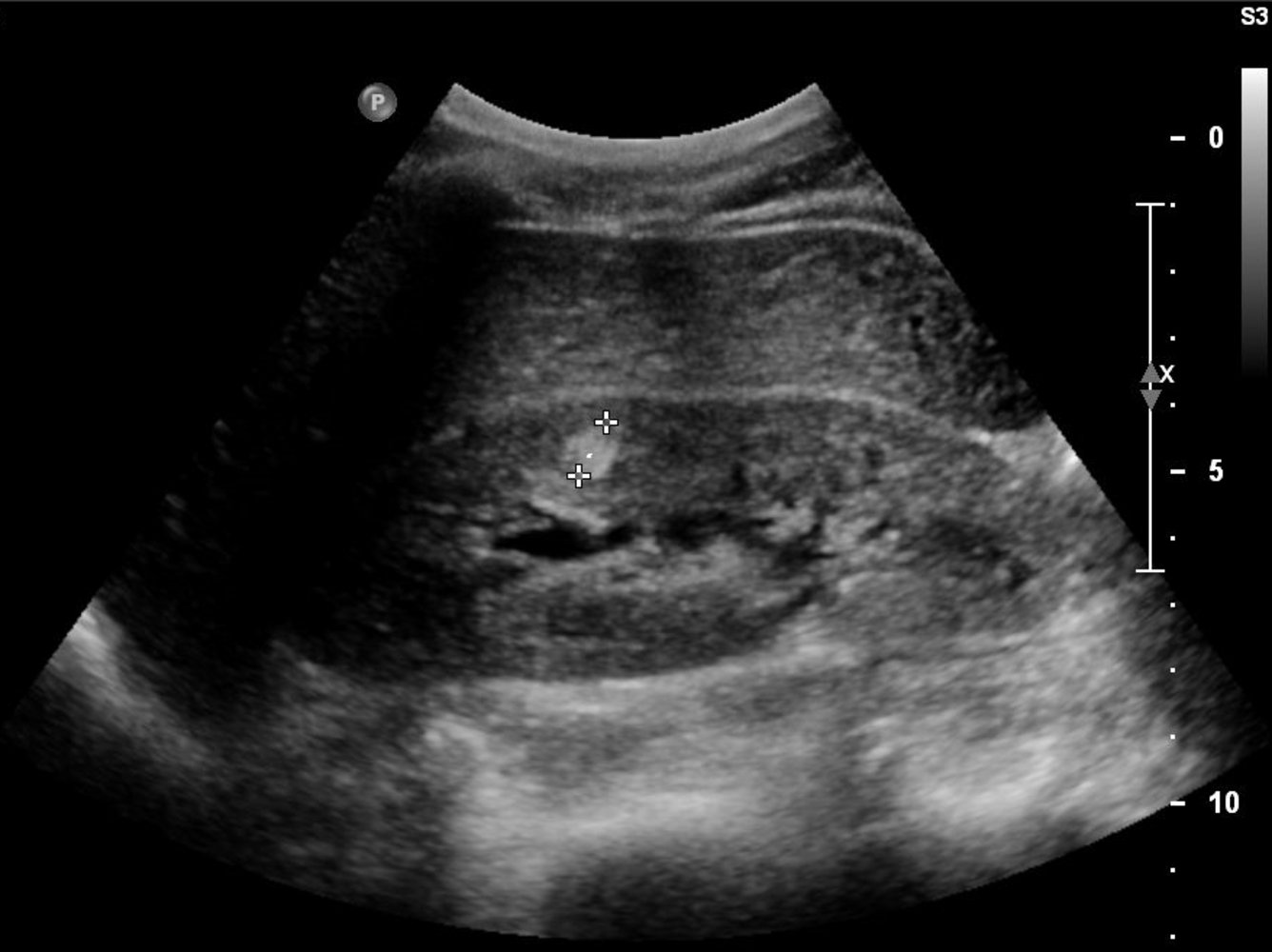
Ultrasound kidney (longitudinal plane)
An irregular heterogeneous hypoechoic mass involves the lower pole renal cortex and the adjacent region of the collecting system. There is no posterior acoustic enhancement to indicate a cystic component.
The differential for a hypoechoic solid renal mass includes both benign and malignant tumors as well as several non-tumorous lesions. The most common tumor is renal cell carcinoma. Further imaging would be necessary for a definitive diagnosis and would typically include CT and possibly MRI and/or biopsy.
Outline: kidney
Our great thanks to Albertinen Krankenhaus, Hamburg, Germany, for kindly providing this case.

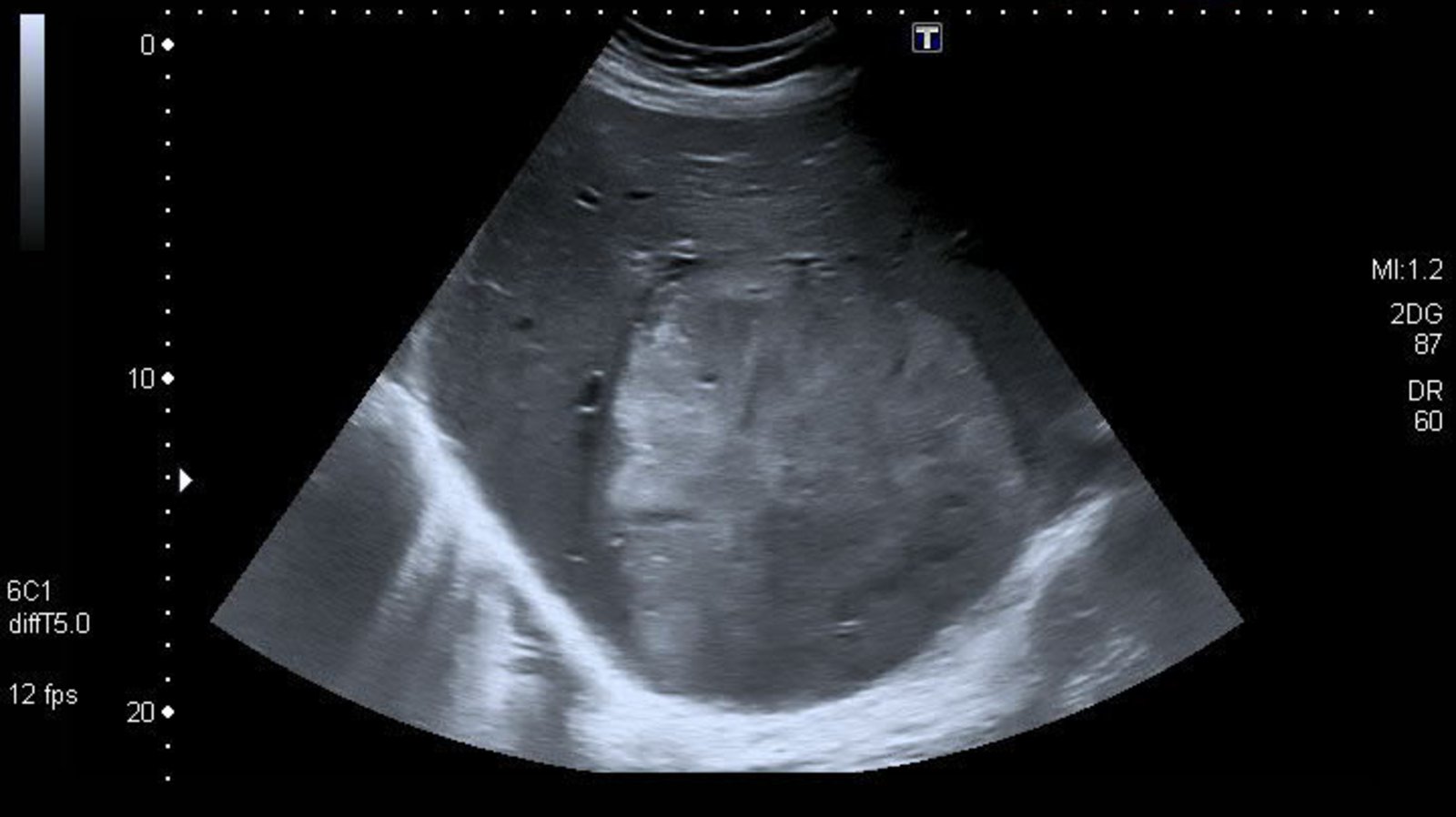
Ultrasound right kidney (longitudinal plane; imaged from flank)
A large circumscribed complex mass contains heterogeneous and hypoechoic regions that indicate central necrosis. Contrast-enhanced CT, MRI, or ultrasound could be performed to further characterize the lesion.
Edge artifact obscuring part of the margin is due to the scattering and refraction of the ultrasound beam by the curved surface.
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
© AMBOSS
Ultrasound liver (transverse plane) of patient with renal cell carcinoma
A large, lobulated, heterogenous mass (green overlay) is slightly echogenic relative to the background liver parenchyma. The mass abuts the diaphragm (dashed line).
The ultrasound pattern of renal cell carcinoma metastases is variable, e.g., solid or partially cystic; homogeneous, heterogeneous, or targetoid; and hypoechoic, isoechoic, or hyperechoic.
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
Pathology
Renal cell carcinomas are adenocarcinomas that usually arise from the epithelial cells of the proximal convoluted tubule.
| Overview of the most important types of renal cell carcinoma [24][25] | |||||
|---|---|---|---|---|---|
| Clear cell renal cell carcinoma | Non-clear cell renal cell carcinomas | ||||
| Papillary (chromophilic) RCC | Chromophobe RCC | Oncocytic RCC | Collecting duct carcinoma (Bellini duct carcinoma) | ||
| Relative frequency |
|
|
|
|
|
| Cell of origin |
|
|
|
||
| Etiology |
|
|
|
|
|
| Macroscopic appearance |
|
||||
| Microscopic appearance |
|
|
|
|
|
| Prognosis |
|
|
|
|
|
Rule of 3: A mutation in the VHL (von Hippel-Lindau) gene on chromosome 3 causes RCC (renal cell carcinoma).




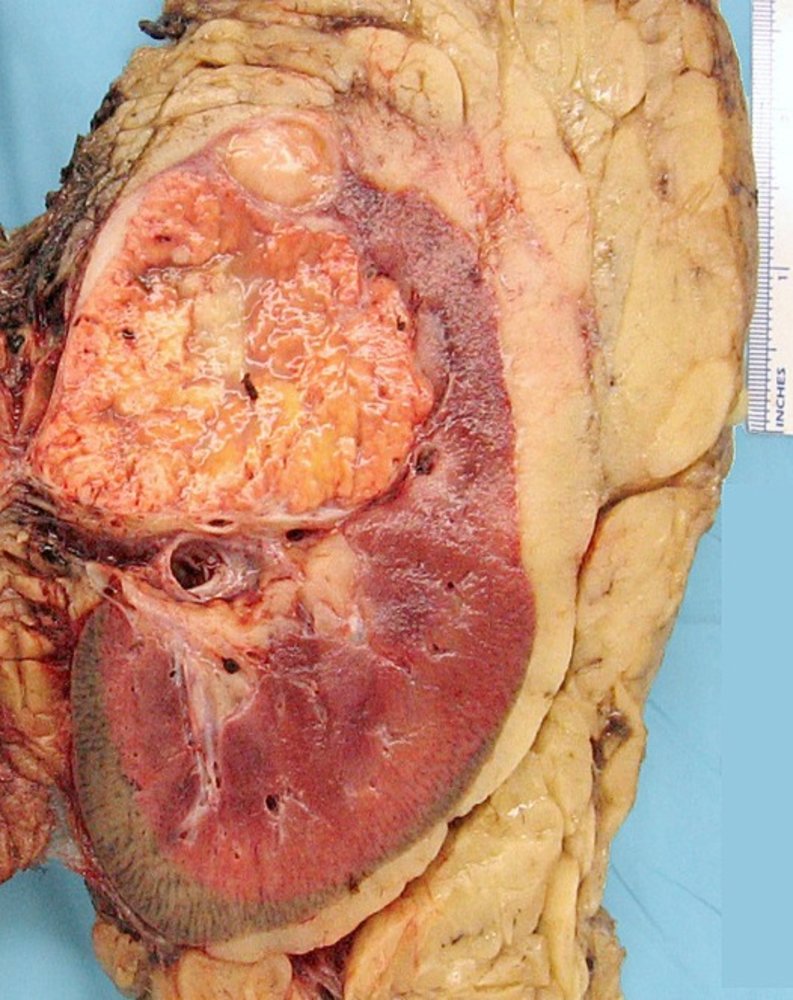
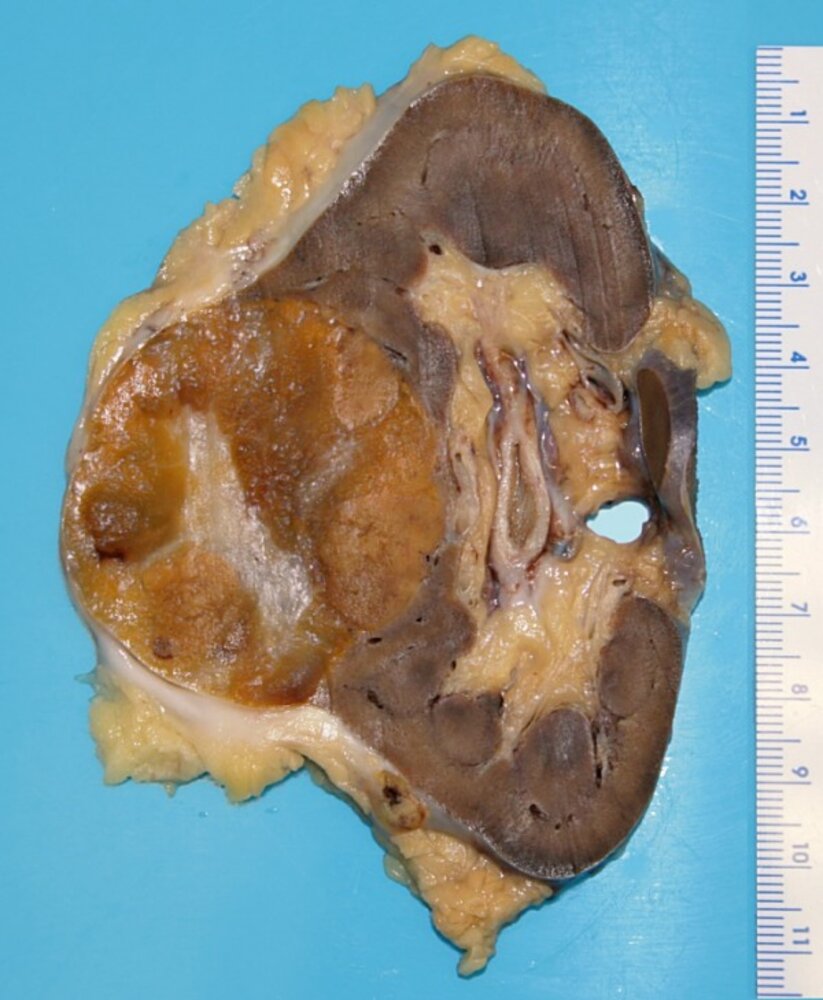
Photograph of a nephrectomy specimen
A large, yellow mass (green overlay) is visible infiltrating the top half of the kidney (K).
Source: “Kidney cancer” by Emmanuelm, Wikimedia Commons, licensed under CC BY 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
{kind=link}
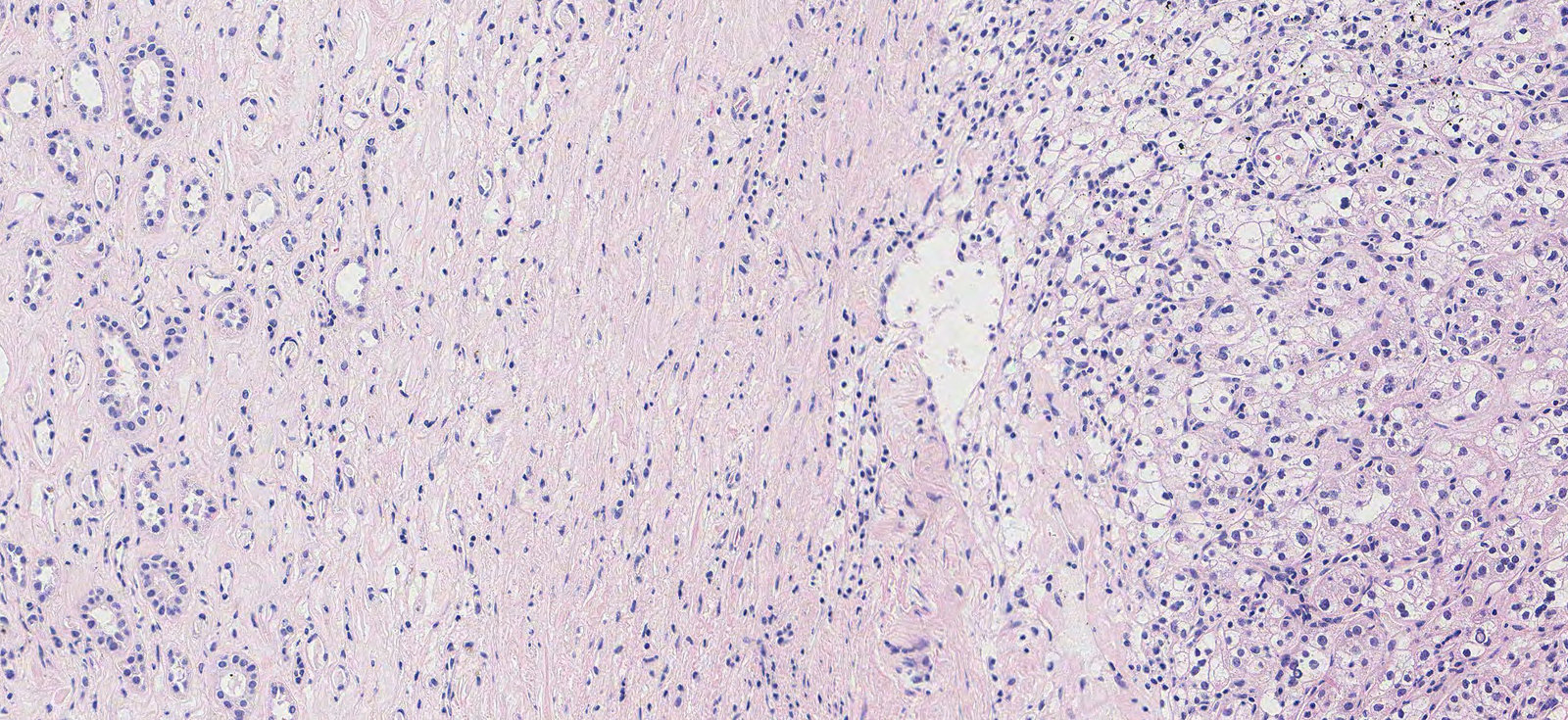
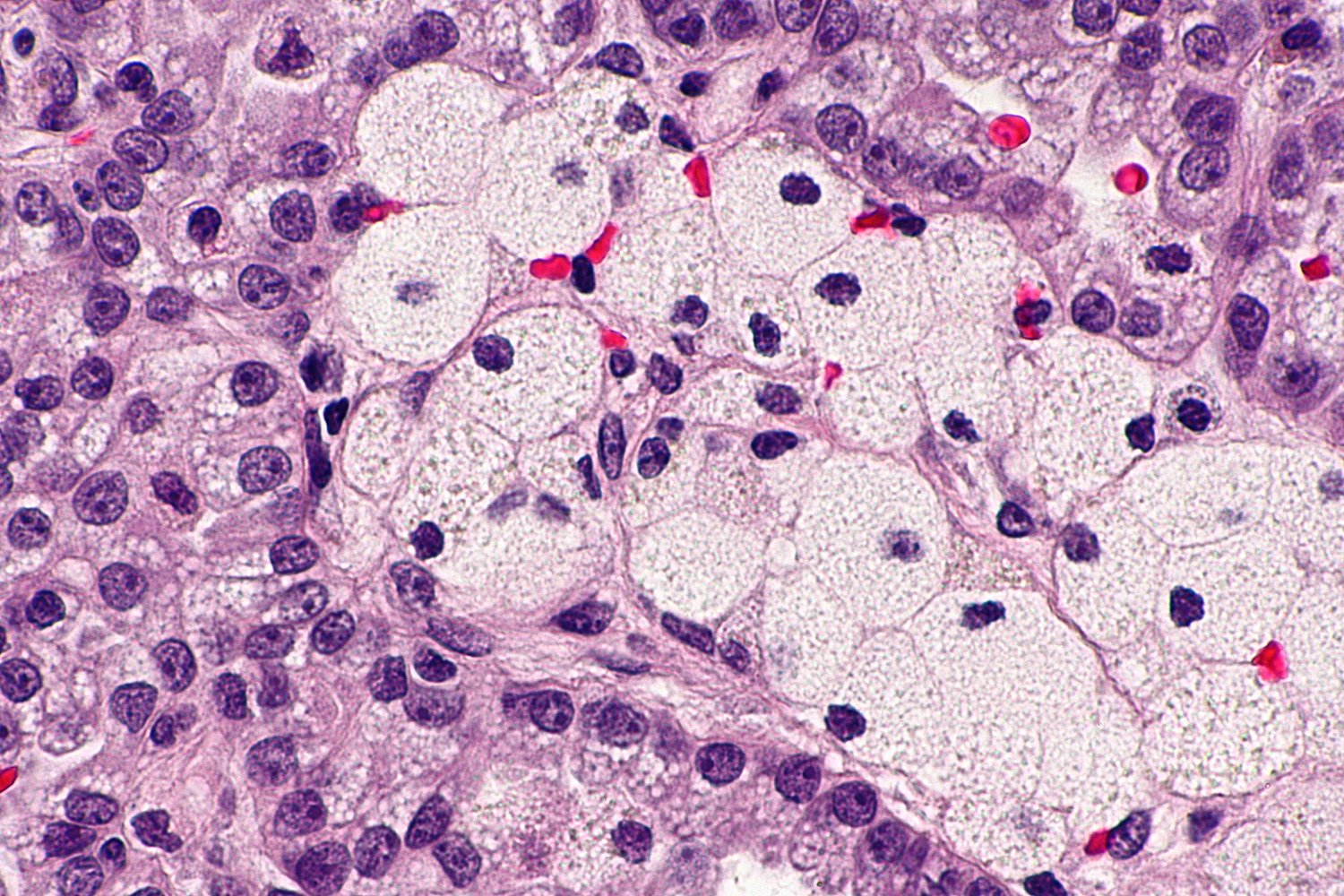
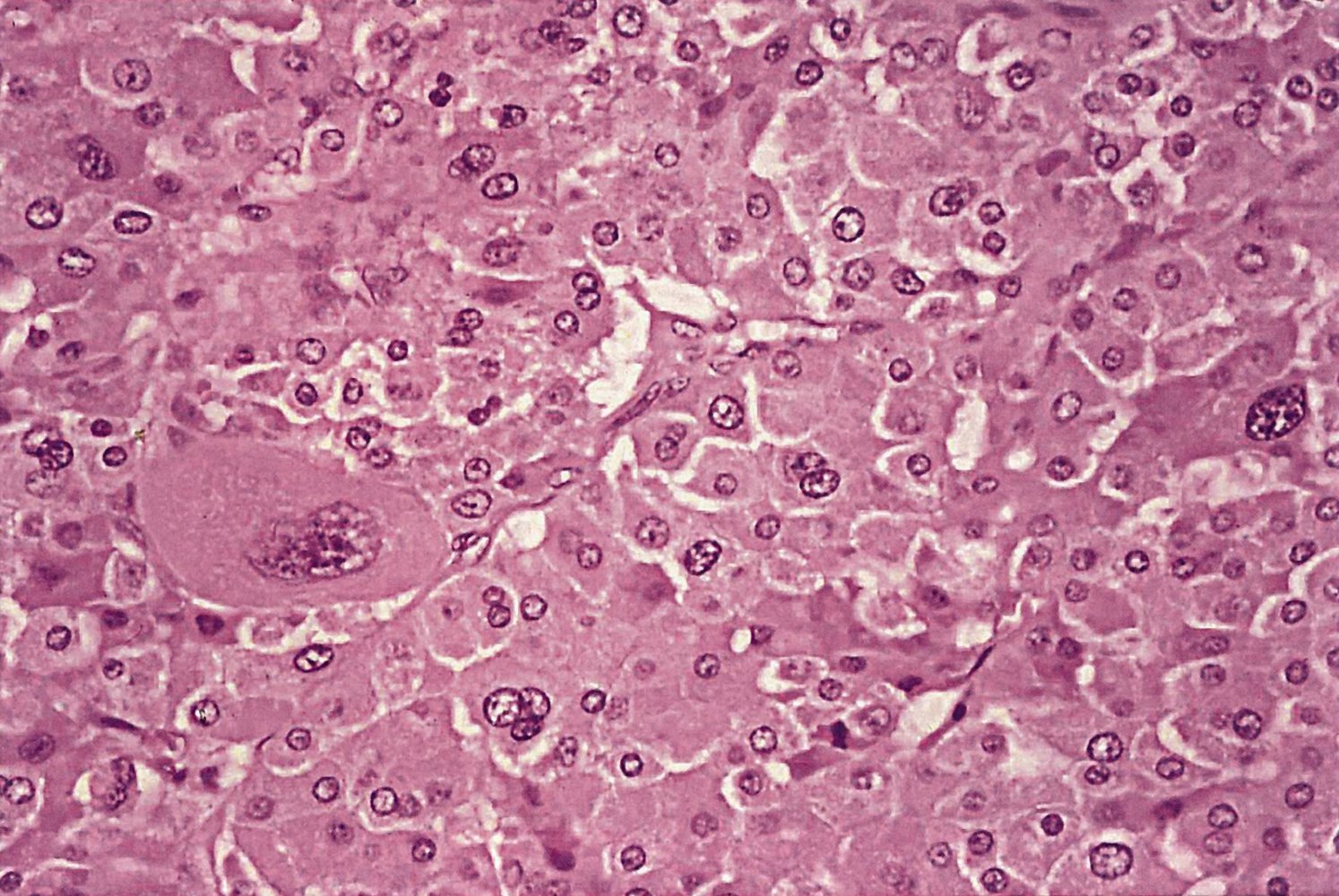
Photomicrograph of kidney tissue (H&E stain, 350x magnification)
The renal tubules (black circles) can be seen within the renal parenchyma on the left. The tumor cells have spread beyond the renal capsule (faded area) and have an enlarged cytoplasm that appears clear due to high lipid and glycogen content.
This is the typical histological appearance of clear cell renal cell carcinoma.
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. med. Alberto Perez Bouza, Facharzt für Pathologie
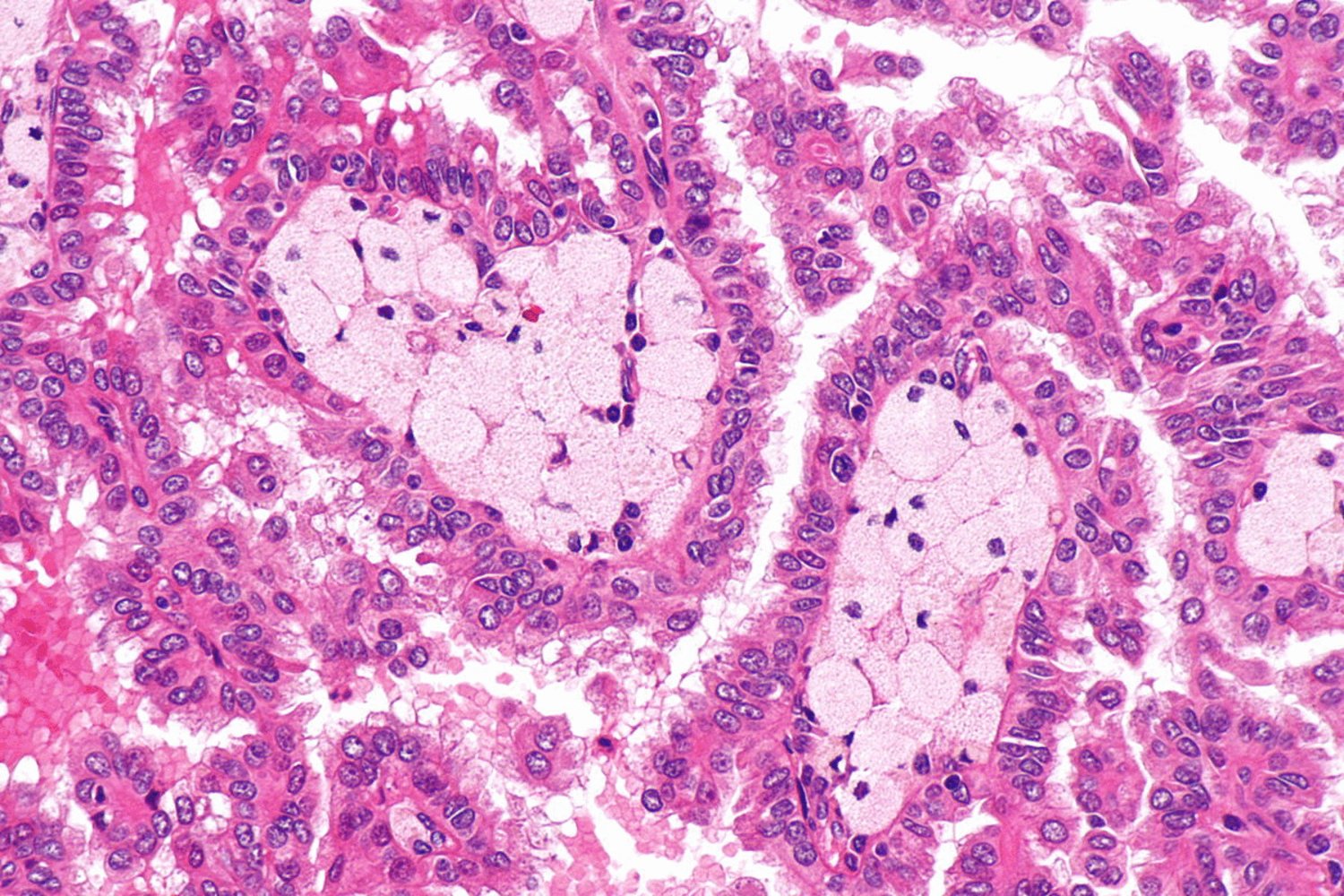
Photomicrograph of renal tissue (H&E stain; very high magnification)
Two cross-sectioned papillae are visible in the center of the image. The papillae are lined by large cells with abundant eosinophilic cytoplasm arranged in pseudostratified layers (examples indicated by yellow arrowheads). Foamy histiocytes (green overlay) are present in the fibrovascular core of the papillae.
Distinct papillary formation within renal tissue is characteristic of papillary renal cell carcinoma.
Source: “Papillary renal cell carcinoma -- very high mag” by Michael Bonert ("Nephron"), Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
Photomicrograph of a kidney biopsy specimen (H&E stain; high magnification)
A large papilla in cross-section is visible, lined by large cells with abundant eosinophilic cytoplasm arranged in pseudostratified layers (examples indicated by yellow arrowheads). Foamy histiocytes (green overlay) can be seen in the central fibrovascular core of the papilla.
This appearance of distinct papillary formation within renal tissue is characteristic of papillary renal cell carcinoma.
Source: “Papillary renal cell carcinoma - 2 -- very high mag” by Michael Bonert ("Nephron"), Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
Differential diagnoses
Malignant renal masses
- Renal cell carcinoma
- Metastasis from extrarenal tumors
- Urothelial carcinoma of the renal pelvis (∼ 8% of renal tumors)
- Other rare primary malignancies
- Lymphomas
- Soft tissue sarcomas
- Neuroendocrine neoplasms
All renal masses > 1 cm in size are presumed to be renal cell carcinoma and treated as such.
Benign renal masses
Angiomyolipoma [26]
- Definition: benign renal tumors that arise from perivascular epithelioid cells and consist of blood vessels, smooth muscle, and mature fat cells
-
Epidemiology
- Most common benign renal tumor
- Sex: ♀ > ♂ (4:1)
-
Etiology
- Sporadic
- Associated with the following syndromes:
- Tuberous sclerosis (TSC)
- Sporadic lymphangioleiomyomatosis
-
Clinical features
- Mostly asymptomatic
- Large angiomyolipomas may present with the following symptoms:
- Hematuria
- Retroperitoneal hemorrhage
- Impaired renal function
- Symptoms of tuberous sclerosis may be present.
-
Diagnostics
- Abdominal ultrasound: round, well-circumscribed, highly echogenic (similar echogenicity to renal pelvis) renal tumor often located near the renal capsule
-
Abdominal CT
- Tumor with macroscopic fat deposits
- No calcification
-
Pathology
- Classic angiomyolipomas: slow growing tumors
-
Epithelioid angiomyolipomas
- Greater number of epithelioid cells
- Acidophilic and granular cytoplasm
- Less fat than classic type
- Treatment: Surgical resection of the tumor is indicated for angiomyolipomas that measure > 4 cm in diameter.



Oncocytoma
- Definition: benign epithelial tumor arising from the intercalated tubular cells in the collecting duct
-
Clinical features
- Painless hematuria
- Abdominal mass
- Flank pain
-
Pathology
- Macroscopy: smooth, clearly defined brown tumor with central radial scar
- Microscopy
- Large acidophilic cells
- Excessive amount of mitochondria → acidophilic, granular cytoplasm without perinuclear clearing (unlike chromophobe RCC)
-
Treatment
- Often resected in order to exclude RCC
- Surveillance
- Nephrectomy in case of increase in tumor size
- Prognosis: Oncocytomas are not invasive, but they may transform into a malignant oncocytic RCC.



Others
- Renal abscess
- Renal cysts (e.g., polycystic kidney disease)
- Metanephric adenoma
- Granulomatous renal disease (e.g., renal tuberculosis, xanthogranulomatous pyelonephritis)
The differential diagnoses listed here are not exhaustive.

Ultrasound kidney (longitudinal plane; imaged from flank)
A sharply demarcated, hyperechoic, rounded lesion (blue overlay) is seen within the upper pole renal cortex.
This appearance is typical of a fat-rich angiomyolipoma, although some renal cell carcinomas can also exhibit hyperechogenicity.
Outline: margin of kidney; RSF: renal sinus fat; Yellow overlay: acoustic enhancement
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
Ultrasound of the right kidney in a transhepatic longitudinal section: There is a sharply demarcated, hyperechoic lesion (red area) in the parenchyma of the right kidney (white circled area), which is most likely an angiomyolipoma. The cranial portion of the kidney (white broken line) is indistinguishable as a result of acoustic attenuation (green area) by a rib (R). (Li = liver)
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
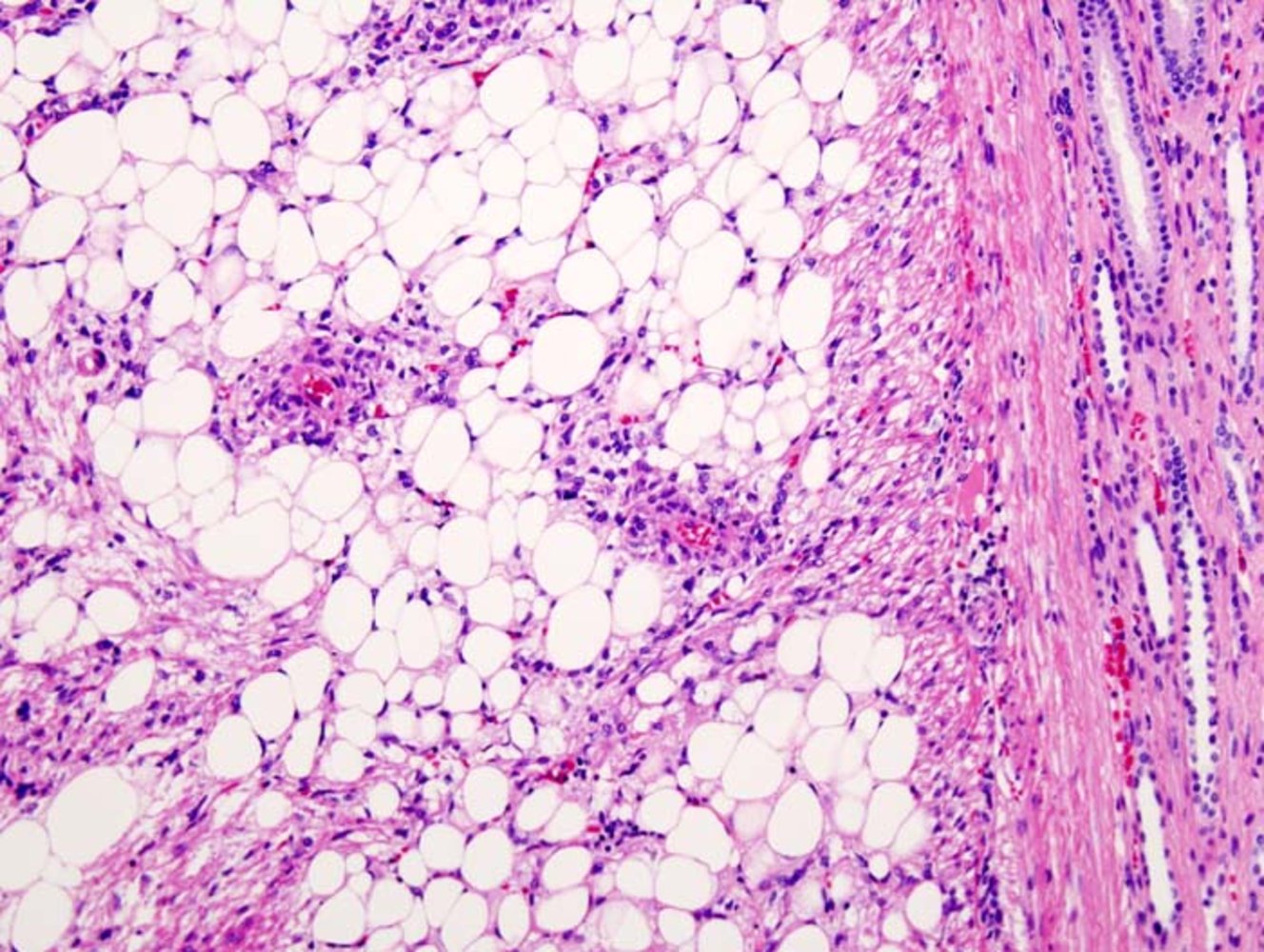
Photomicrograph of a kidney biopsy specimen (H&E stain; high magnification)
Numerous mature adipocytes are visible, identifiable as large clear cells with a thin layer of eosinophilic cytoplasm and a peripherally placed basophilic nucleus (examples indicated by black arrowheads). Thick-walled blood vessels (green overlay) are scattered among the adipocytes. Bundles of transversely cut and longitudinally cut smooth muscle cells (red overlay) are visible on the right, and renal tubular architecture is visible on the extreme right.
The presence of mature adipocytes, blood vessels, and smooth muscle cells within the renal parenchyma is characteristic of renal angiomyolipoma.
Source: “Histopathologic image of renal angiomyolipoma. Nephrectomy specimen. H & E stain.” by KGH, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
.jpg){kind=link}
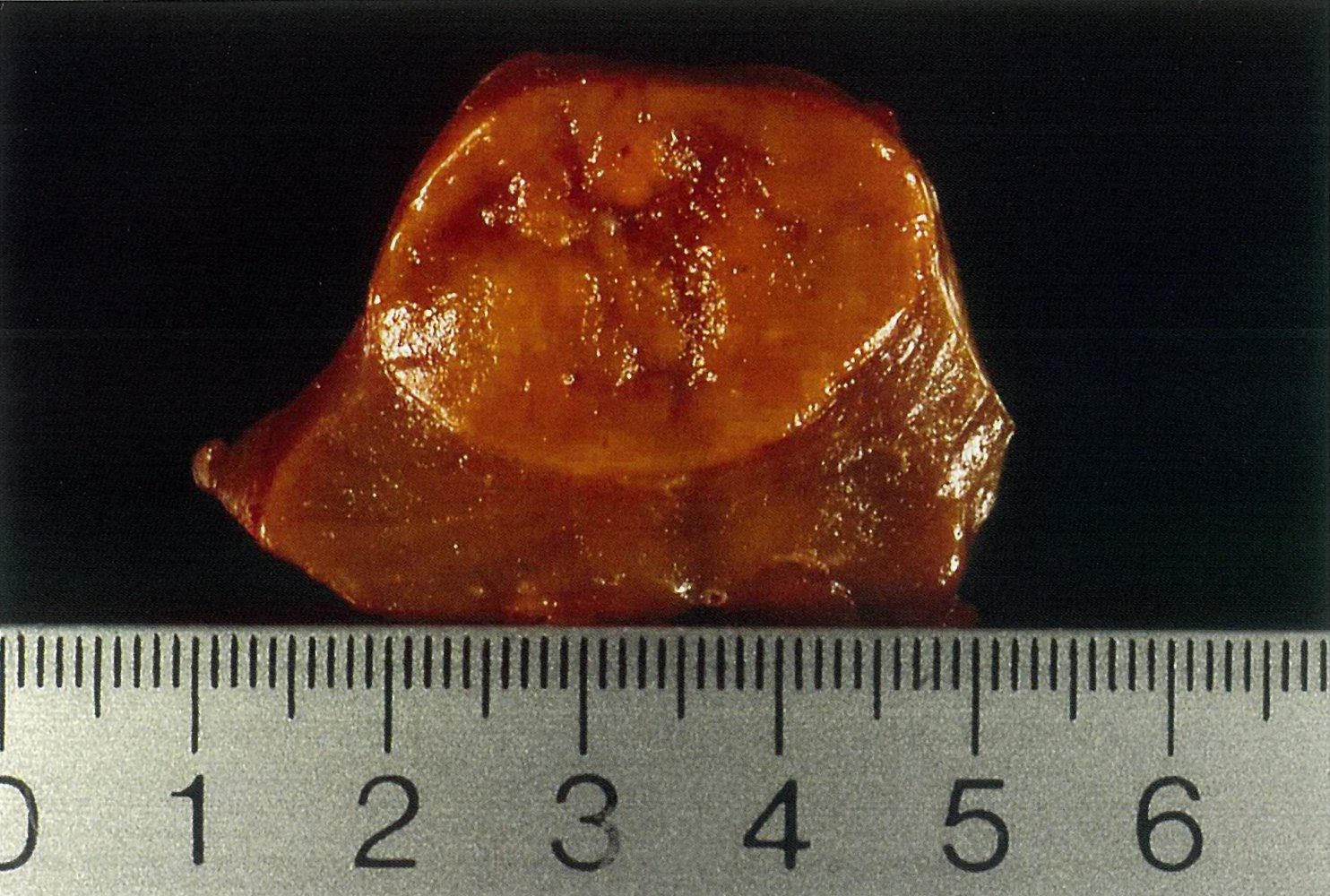
Light brown, well-circumscribed renal tumor with a central radial scar.
Source: © IMPP
Gross pathology specimen of a kidney (sagittal section)
A well-circumscribed, mahogany-brown tumor (green overlay) with a central scar (hatched green overlay) is visible.
These findings are characteristic of a renal oncocytoma.
Source: “Renal oncocytoma” by Emmanuelm, Wikimedia Commons, licensed under CC BY 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
{kind=link}
Photomicrograph of a renal tumor tissue specimen (H&E stain; 400x magnification)
A solid nest of tumor cells (without formation of glands or other structures) can be seen. The large tumor cells have a granular eosinophilic cytoplasm (examples indicated by arrowheads). Two atypical cells with hyperchromatic, pleomorphic nuclei (green overlay) are also visible.
This is the characteristic appearance of a renal oncocytoma. It is a benign condition, even if a few degenerative cells with suspicious atypia are seen.
Source: © IMPP
Treatment
Approach
-
Local or locoregional disease: curative treatment intent ; [19][27]
- Standard of care: nephrectomy (partial or radical) [6]
- Consider adrenalectomy, lymph node dissection, and adjuvant therapy with sunitinib. [6]
-
Metastatic disease: mostly palliative treatment intent but may be curative for patients with a solitary metastasis or oligometastatic disease [9] [19]
- Targeted and/or immunotherapy
- In selected patients, surgery (i.e., cytoreductive nephrectomy, metastasectomy) or other local therapies (e.g., embolization) [28]
-
Consider active surveillance for patients with: [23]
- Solid masses < 2 cm
- Complex masses that are predominantly cystic
- Limited life expectancy
- High surgical risk
Surgery [6]
The following applies to patients with solid renal masses or renal cysts with Bosniak classification III or IV. The approach may be open, robotic, or laparoscopic.
-
Partial nephrectomy: Only the mass and some surrounding renal tissue are removed; the rest of the kidney is spared. [6]
- Absolute indications: patients with a T1a renal mass , a solitary kidney, bilateral masses, familial RCC, preexisting chronic kidney disease, or proteinuria [27]
- Relative indications: patients who are young and/or have a longer life expectancy, multifocal masses, or comorbidities that impact renal function
-
Radical nephrectomy
- Removal of the entire kidney along with the adrenal gland and surrounding perinephric fat, with or without lymph node dissection
- Preferred in patients with increased oncological risk [6]
Medical therapy [19][28]
| Agents for the treatment of renal cell carcinoma | ||
|---|---|---|
| Drug type | Examples | |
| Targeted therapy [28][29] | VEGF receptor tyrosine kinase inhibitors |
|
| Anti-VEGF antibodies |
|
|
| mTOR inhibitors |
|
|
| Immunotherapy | Anti-PD-1 antibodies |
|
| Anti-CTLA-4 antibodies |
|
|
| Cytokines |
|
|
- Regimens vary (e.g., axitinib combined with pembrolizumab) and are determined by risk level. [28][30]
Other
-
Radiochemotherapy
- Radiation therapy is not typically used because RCC is usually radioresistant. [28][31]
- Conventional chemotherapy is not used to treat RCC because RCC is highly resistant to most chemotherapeutic agents. [19]
-
Local therapies [6][27]
- Thermal ablation (e.g., cryoablation): may be appropriate for patients with tumors ≤ 3 cm and/or high surgical risk
- Embolization of the primary tumor and/or metastases: for symptom control in patients with nonresectable disease [9]
Many RCC tumors are also resistant to chemotherapy due to the expression of multidrug resistance protein 1 (MDR-1) by tumor cells. [9][32]
Complications
Complications caused by paraneoplastic syndromes
- Secondary hypercortisolism: due to ectopic ACTH release
- Secondary polycythemia: due to ectopic erythropoietin (EPO) secretion
- Hypertension: due to the release of renin
- Hypercalcemia: due to the release of PTHrP (parathyroid hormone-related protein)
- Leukemoid reaction: due to bone marrow stimulation
-
Limbic encephalitis [33]
- Memory loss
- Psychosis
- Depression
Paraneoplastic RCC: Polycythemia (EPO), Renin (hypertension), hyperCalcemia (PTHrP) and hyperCortisolism (ACTH).
Complications caused by local spread
-
Varicocele
- Rare, classically associated with left-sided RCC
- Malignant cells grow inside the left renal vein and occlude the ostium of the left gonadal vein.
-
Budd-Chiari syndrome: caused by involvement of the IVC
- Lower limb edema
- Ascites
- Hepatic dysfunction
Complications caused by metastatic disease
-
Overview
- Spread beyond the renal capsule affects the lymph nodes of the renal hilum and para-aortic nodes.
- Hematogenous spread occurs via renal vein and IVC.
-
Pulmonary metastases: most common site of metastases
- Hemoptysis
- Dyspnea
-
Bone metastases: second most common site of metastases
- Bone pain
- Pathological fractures
Reactive amyloidosis [34]
- Epidemiology: RCC accounts for 25 to 42% of all reported AA amyloidosis cases caused by solid organ malignancies.
-
Clinical features
- Nephrotic syndrome [35][36]
- Primary adrenal insufficiency
- Hepatosplenomegaly
- Malabsorption
We list the most important complications. The selection is not exhaustive.
Prognosis
Survival of kidney cancer patients
- Overall prognosis is determined by the anatomic extent of the disease (stage of cancer at diagnosis) and the histopathology of the tumor.
- Targeted therapies have significantly prolonged survival time.
- Early stage RCC with tumor growth limited to the kidney generally has a good prognosis.
| 5-year survival of kidney cancer patients [37] | ||
|---|---|---|
| SEER stage | Description | 5-year survival rate |
| Localized |
|
|
| Regional |
|
|
| Distant |
|
|
| All stages combined |
|
|
Increased awareness and screening (e.g., ultrasound) of high-risk patients in recent years has led to earlier tumor detection and improved the prognosis of RCC.
Motzer score [38]
Overview
- Used to determine prognosis of patients with stage IV (distant) disease
- A point is assigned for each of the following criteria.
- Based on the resulting score, the prognosis of the metastatic RCC patient is estimated.
- High scores are associated with a poorer prognosis.
Instrument
| Motzer score | ||
|---|---|---|
| Parameter | Description | |
| Karnofsky performance status | < 80% | < 80%: 1 point |
| > 80%: 0 points | ||
| Hemoglobin level | ♀ < 12 g/dL | < 12 g/dL: 1 point |
| > 12.0 g/dL: 0 points | ||
| ♂ < 13.5 g/dL | < 13.5 g/dL: 1 point | |
| > 13.5 g/dL: 0 points | ||
| ↑ LDH (> 1.5 times the upper normal limit) | > 420 U/L | > 420 U/L: 1 point |
| < 420 U/L: 0 point | ||
| ↑ Serum calcium | > 10 mg/dL (> 2.5 mmol/L) | > 10 mg/dL (> 2.5 mmol/L): 1 point |
| < 10 mg/dL (< 2.5 mmol/L): 0 points | ||
| Time from diagnosis to systemic treatment | < 1 year | < 1 year: 1 point |
| > 1 year: 0 points | ||
Interpretation
| Motzer score interpretation | ||
|---|---|---|
| Points | Risk | Median survival |
| 0 |
|
|
| 1–2 |
|
|
| ≥ 3 |
|
|
External Resources
- 2021 AUA Guidelines for Evaluation, Management, and Follow-up of Renal Mass and Localized Renal Cancer (Part I)
- 2021 AUA Guidelines for Evaluation, Management, and Follow-up of Renal Mass and Localized Renal Cancer (Part II)
- 2019 ESMO clinical practice Guidelines for Management of RCC
- EAU Guidelines on Renal Cell Carcinoma
References
- "Key Statistics About Kidney Cancer". https://www.cancer.org/cancer/kidney-cancer/about/key-statistics.html. [2020-02-01]
- Cheng G, Xie L. "Alcohol intake and risk of renal cell carcinoma: a meta-analysis of published case-control studies". Archives of Medical Science. 4. :648-657. (2011)
- "Risk Factors for Kidney Cancer". https://www.cancer.org/cancer/kidney-cancer/causes-risks-prevention/risk-factors.html. [2020-02-01]
- "Acquired Cystic Kidney Disease". https://www.niddk.nih.gov/health-information/kidney-disease/acquired-cystic-kidney-disease. [2015-08-01]
- "Renal cell carcinoma". https://radiopaedia.org/articles/renal-cell-carcinoma-1. [2017-02-15]
- Campbell SC, Clark PE, Chang SS, et al. "Renal Mass and Localized Renal Cancer: Evaluation, Management, and Follow-Up: AUA Guideline: Part I". J Urol. 206(2). :199-208. (2021)
- Gray RE, Harris GT. "Renal Cell Carcinoma: Diagnosis and Management.". Am Fam Physician. 99(3). :179-184. (2019)
- Wang ZJ, Nikolaidis P, Khatri G, et al. "ACR Appropriateness Criteria® Indeterminate Renal Mass". J Am Coll Radiol. 17(11). :S415-S428. (2020)
- Ljungberg B, Bensalah K, Canfield S, et al. "EAU Guidelines on Renal Cell Carcinoma: 2014 Update". Eur Urol. 67(5). :913-924. (2015)
- van Oostenbrugge TJ, Futterer JJ, Mulders PFA. "Diagnostic Imaging for Solid Renal Tumors: A Pictorial Review". Kidney Cancer. 2(2). :79-93. (2018)
- Freire M, Remer EM. "Clinical and Radiologic Features of Cystic Renal Masses". AJR Am J Roentgenol. 192(5). :1367-1372. (2009)
- Johnson PT, Horton KM, Fishman EK. "How Not to Miss or Mischaracterize a Renal Cell Carcinoma: Protocols, Pearls, and Pitfalls". AJR Am J Roentgenol. 194(4). :W307-W315. (2010)
- Silverman SG, Pedrosa I, Ellis JH, et al. "Bosniak Classification of Cystic Renal Masses, Version 2019: An Update Proposal and Needs Assessment". Radiology. 292(2). :475-488. (2019)
- Palapattu GS, Kristo B, Rajfer J. "Paraneoplastic syndromes in urologic malignancy: the many faces of renal cell carcinoma.". Rev Urol. 4(4). :163-70. (2002)
- Vikram R, Beland MD, Blaufox MD, et al. "ACR Appropriateness Criteria Renal Cell Carcinoma Staging". J Am Coll Radiol. 13(5). :518-525. (2016)
- Chan J, Albretson J. "Causes of isolated recurrent ipsilateral sixth nerve palsies in older adults: a case series and review of the literature". Clinical Ophthalmology. :373. (2015)
- Brufau BP, Cerqueda CS, Villalba LB, et al. "Metastatic Renal Cell Carcinoma: Radiologic Findings and Assessment of Response to Targeted Antiangiogenic Therapy by Using Multidetector CT". Radiographics. 33(6). :1691-1716. (2013)
- Gong J, Maia MC, Dizman N, Govindarajan A, Pal SK. "Metastasis in renal cell carcinoma: Biology and implications for therapy". Asian J Urol. 3(4). :286-292. (2016)
- Hsieh JJ, Purdue MP, Signoretti S, et al. "Renal cell carcinoma". Nat Rev Dis Primers. 3(1). (2017)
- Sole K. "Thrombocytosis predicts mortality in patients with renal cell carcinoma". Nat Rev Urol. 3(5). :240-240. (2006)
- Wang Y-C, Yang S, et al. "Renal Cell Carcinoma Producing Granulocyte Colony-stimulating Factor". J Formos Med Assoc. 105(5). :414-417. (2006)
- Fox P, Hudson M, Brown C, et al. "Markers of systemic inflammation predict survival in patients with advanced renal cell cancer". Br J Cancer. 109(1). :147-153. (2013)
- Campbell SC, Uzzo RG, Karam JA, et al. "Renal Mass and Localized Renal Cancer: Evaluation, Management, and Follow-up: AUA Guideline: Part II". J Urol. 206(2). :209-218. (2021)
- Vos N, Oyen R. "Renal Angiomyolipoma: The Good, the Bad, and the Ugly". Journal of the Belgian Society of Radiology. 102(1). (2018)
- Escudier B, Porta C, Schmidinger M, et al. "Renal cell carcinoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up". Ann Oncol. 30(5). :706-720. (2019)
- Dutcher JP, Flippot R, Fallah J, Escudier B. "On the Shoulders of Giants: The Evolution of Renal Cell Carcinoma Treatment—Cytokines, Targeted Therapy, and Immunotherapy". Am Soc Clin Oncol Educ Book. :418-435. (2020)
- Zarrabi K, Wu S. "Current and Emerging Therapeutic Targets for Metastatic Renal Cell Carcinoma". Curr Oncol Rep. 20(5). (2018)
- Massari F, Rizzo A, Mollica V, et al. "Immune-based combinations for the treatment of metastatic renal cell carcinoma: a meta-analysis of randomised clinical trials". Eur J Cancer. 154. :120-127. (2021)
- Tselis N, Chatzikonstantinou G. "Treating the Chameleon: Radiotherapy in the management of Renal Cell Cancer". Clinical and Translational Radiation Oncology. 16. :7-14. (2019)
- Walsh N, Larkin A, Kennedy S, et al. "Expression of multidrug resistance markers ABCB1 (MDR-1/P-gp) and ABCC1 (MRP-1) in renal cell carcinoma". BMC Urol. 9(1). (2009)
- Harrison JW, Cherukuri R, Buchan D. "Renal Cell Carcinoma Presenting with Paraneoplastic Hallucinations and Cognitive Decline from Limbic Encephalitis". J Gen Intern Med. 30(7). :1037-1040. (2015)
- Babu A, Lachmann H, Pickett T, Boddana P, Ludeman L. "Renal cell carcinoma presenting as AA amyloidosis: a case report and review of the literature.". CEN case reports. 3(1). :68-74. (2013)
- Ahmed M, Solangi K, Abbi R, Adler S. "Nephrotic syndrome, renal failure, and renal malignancy: an unusual tumor-associated glomerulonephritis". J Am Soc Nephrol. 8(5). :848-852. (1997)
- Woodrow G, Innes A, Ansell ID, Burden RP. "Renal cell carcinoma presenting as nephrotic syndrome". Nephron. 69(2). :166-169. (1995)
- "Survival Rates for Kidney Cancer". https://www.cancer.org/cancer/kidney-cancer/detection-diagnosis-staging/survival-rates.html. [2020-02-01]
- Robert J. Motzer, Madhu Mazumdar, Jennifer Bacik, et al. "Survival and Prognostic Stratification of 670 Patients With Advanced Renal Cell Carcinoma". Journal of Clinical Oncology. 17(8). :2530-2530. (1999)
- Kumar V, Abbas AK, Aster JC. "Robbins & Cotran Pathologic Basis of Disease". Elsevier Saunders. (2014). ISBN: 9781455726134
- "What Is Kidney Cancer?". https://www.cancer.org/cancer/kidney-cancer/about/what-is-kidney-cancer.html. [2020-05-05]