CME information and disclosures
To see contributor disclosures related to this article, hover over this reference: [1]
Physicians may earn CME/MOC credit by reading information in this article to address a clinical question, then completing a brief evaluation in which they identify their question and report the impact of any information learned on their clinical practice.
AMBOSS designates this Internet point-of-care activity for a maximum of 0.5 AMA PRA Category 1 Credit(s)™. Physicians should claim only credit commensurate with the extent of their participation in the activity.
For answers to questions about AMBOSS CME, including how to redeem CME/MOC credit, see “Tips and Links” at the bottom of this article.
Quick guide
Related Quick guide: Dyspnea
Diagnostic approach
- ABCDE survey
- Targeted clinical evaluation
- ABG
- CBC
- BMP
- 12-lead ECG
- BNP
- Troponin
- D-dimer
- Bedside imaging: chest x-ray, lung and cardiac POCUS
Initiate stabilization before definitive diagnostic confirmation.
Red flag features
- Signs of imminent respiratory arrest
- Signs of airway compromise
- Severe altered mental status
- Hemodynamic instability
- Exhaustion, inability to maintain respiratory effort
Management checklist
- IV access
- Pulse oximetry
- Cardiac telemetry
- Respiratory support (e.g., supplemental oxygen, NIPPV, rescue breaths)
- Perform rapid sequence intubation if clinical status does not improve.
- Treat rapidly reversible causes of respiratory failure.
- Tension PTX: needle decompression, chest tube
- Opioid overdose: naloxone
- Flash pulmonary edema: NIPPV, nitrates if SBP > 90 mm Hg (e.g., nitroglycerin )
- Cardiogenic pulmonary edema: loop diuretics (e.g., furosemide OR bumetanide )
- Foreign body: Back blows/chest thrusts/Heimlich; prepare for laryngoscopy/bronchoscopy.
- Anaphylaxis: IM epinephrine
- Asthma or COPD exacerbation: nebulized bronchodilators, IV glucocorticoids
- Ascertain code status.
- Begin treatment for suspected underlying cause (e.g., empiric antibiotics for CAP).
- Consult ICU early.
Summary
Respiratory failure is the acute or chronic inability of the respiratory system to maintain gas exchange (PaO2 < 60 mm Hg, PaCO2 > 50 mm Hg). Causes can be extrapulmonary (e.g., CNS depression due to narcotic overdose) as well as pulmonary (e.g., acute exacerbation of COPD). Respiratory failure can be classified as hypoxemic (type 1) or hypercapnic (type 2). Clinical features of hypoxemia include respiratory distress, cyanosis, tachycardia, and altered mental status. Clinical features of hypercapnia include hypoventilation, headache, warm extremities, and asterixis. Diagnostics include arterial blood gas analysis and possibly chest imaging to detect the underlying disease. Treatment includes supportive measures (oxygen delivery and/or ventilator support) and treatment of the underlying condition. Complications may arise due to prolonged hypoxemia and can affect various organs (e.g., renal/heart failure, brain damage).
For children, see "Respiratory distress and failure in children."
Definitions
-
Respiratory failure: the acute or chronic inability of the respiratory system to maintain adequate gas exchange [2]
- Hypoxemic respiratory failure: defined as a < 60 mm Hg (< 8 kPa)
- Hypercapnic respiratory failure: defined as a > 50 mm Hg (> 6.7 kPa)
- Hypoxemic and hypercapnic respiratory failure can occur together.
- Respiratory arrest: the complete cessation of breathing in patients with a pulse [3]
- Respiratory distress: A clinical syndrome associated with breathing disorders (See “Clinical features of respiratory distress.”)
Classification
By gas exchange abnormality
| Types of respiratory failure [2] | ||
|---|---|---|
| Type 1 (hypoxemic respiratory failure) | Type 2 (hypercapnic respiratory failure) | |
| Definition |
|
|
| PaO2 |
|
|
| PaCO2 |
|
|
Patients may present with mixed hypoxemic and hypercapnic respiratory failure.
By duration [4]
- Acute respiratory failure: develops over minutes to hours as a result of an acute illness or insult
- Chronic respiratory failure: longstanding respiratory failure resulting from chronic illness (e.g., COPD, ILD, obesity hypoventilation syndrome)
In patients with hypercapnia, a normal pH suggests chronic CO2 retention while a low pH raises concern for acute or acute-on-chronic CO2 retention, which requires immediate intervention (see also “Respiratory acidosis.”)
Etiology
This section lists causes of respiratory failure and respiratory arrest by type and mechanism. See “Etiology of dyspnea” for a system-based approach.
Respiratory failure and respiratory arrest share the same causes and patients with respiratory failure can quickly decompensate into respiratory arrest.
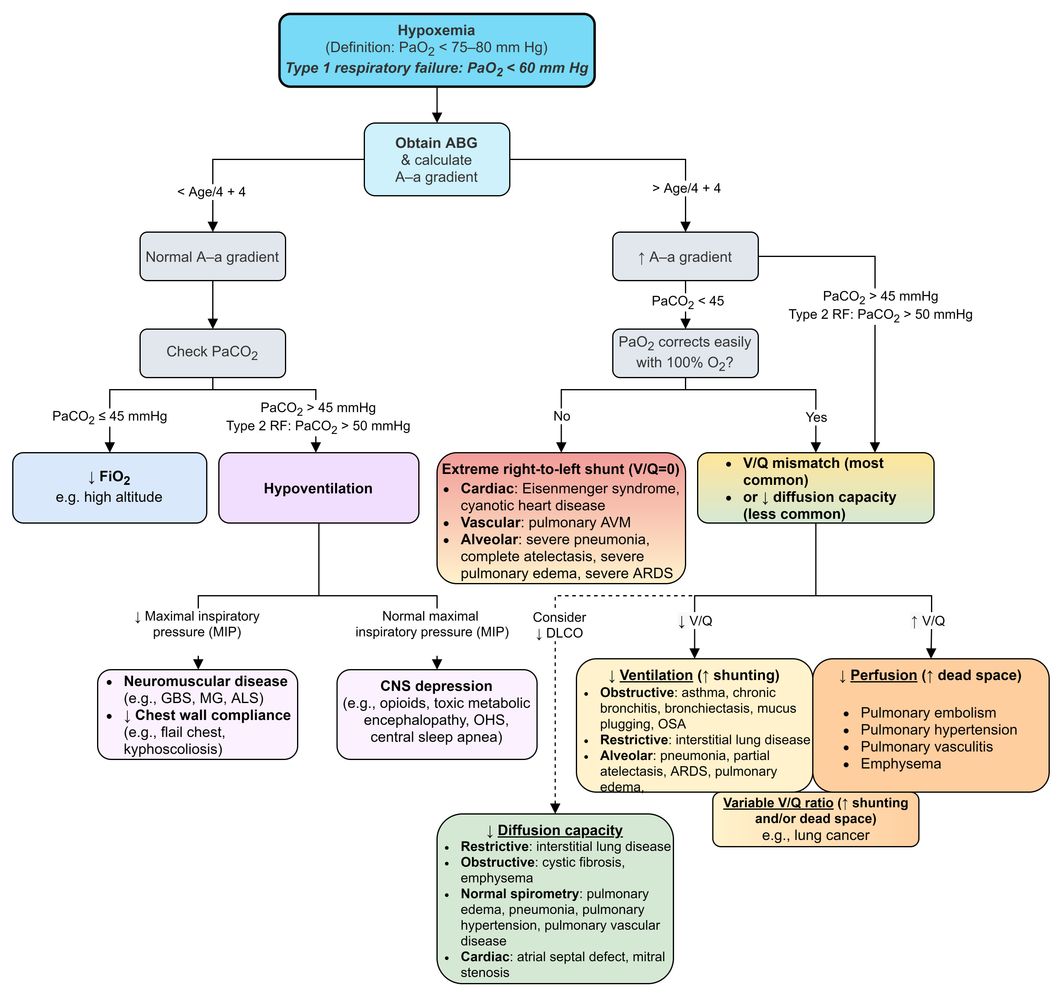
Causes of hypoxemia [5]
- Impaired alveolar diffusion (e.g., due to pulmonary edema, severe pneumonia, pulmonary hemorrhage , idiopathic pulmonary fibrosis)
-
Right-to-left shunt
- Pulmonary right-to-left shunt (e.g., due to ARDS, pulmonary contusions/hemorrhage, lung collapse, tension pneumothorax)
- Intracardiac right-to-left shunt (e.g., due to Eisenmenger syndrome)
- V/Q mismatch (e.g., due to severe pneumonia, pulmonary edema, pulmonary embolism, atelectasis)
- Decreased FiO2 (e.g., due to asphyxiant gas exposure, high altitude illness)
- Hypoventilation (see “Causes of hypercapnia”) [5]
Causes of hypercapnia [5]
Hypercapnia may be caused by decreased ventilation (hypoventilation) resulting from any of the following:
-
Airway obstruction and/or increased physiologic dead space due to:
- Lung diseases: e.g., AECOPD, acute asthma exacerbation, bronchiolitis, aspiration, bronchiectasis, cystic fibrosis
- Upper airway obstruction: e.g., laryngospasm, angioedema, anaphylaxis, tumors, croup, epiglottitis, diphtheria, drowning, OSA
- CNS depression (e.g., due to opioid intoxication, benzodiazepine intoxication, barbiturate intoxication, TBI, cerebral herniation, stroke, inhalant-related disorders)
- Respiratory muscle weakness (e.g., due to myasthenia gravis, Guillain-Barré syndrome, myopathies, ALS, high cervical spinal cord injury, poliomyelitis)
- Decreased chest wall compliance (e.g., due to rib fractures, tetanus, seizures, fibrothorax; , obesity hypoventilation syndrome, circumferential burns)
- Electrolyte disturbances (e.g., anorexia nervosa)
Increased O2 consumption and/or CO2 production (e.g., due to severe sepsis, toxic shock syndrome, cardiogenic shock, multiorgan dysfunction) may contribute to respiratory failure.
Clinical features
By affected system
-
Respiratory: clinical features of respiratory distress
- Dyspnea
- Increased respiratory drive: tachypnea, hyperventilation
-
Increased work of breathing (increased respiratory effort)
- Nasal flaring
- Grunting
- Pursed lips
- Respiratory accessory muscle use
- Intercostal, subcostal, and/or suprasternal retractions
- Tripod positioning
- Paradoxical breathing
- Other clinical features of hypoxemia: agitation, cyanosis
- Inability to lie flat
- Airway: clinical features of airway compromise
- CNS: altered respiratory drive
By underlying process
-
Clinical features of hypoxemia
- Tachypnea, dyspnea
- Cyanosis
- Pleuritic chest pain
- Tachycardia, arrhythmia
- Altered mental status: e.g., confusion, somnolence, agitation
-
Clinical features of hypercapnia
- Hypopnea
- Headache, daytime sleepiness
- Anxiety
- Warm extremities
- Papilledema
- Asterixis
- Coma
- Paralytic ileus
-
Clinical features of the underlying condition
- Fever, e.g., due to sepsis, pneumonia
- Cough, e.g., due to pneumonia, COPD
- Chest pain, e.g., due to pneumonia, pulmonary embolism
- Signs of general muscle weakness, e.g., due to myasthenia gravis, Guillain-Barré syndrome, myopathies, ALS
- Pain on inspiration, e.g., due to rib fracture
- CNS depression, e.g., due to opioid use
Recognize signs of imminent or ongoing respiratory arrest (e.g., gasping, inspiratory stridor, decreased respiratory rate, cyanosis, absent chest rise, or acute oxygen desaturation) and treat it immediately if present.
Initial management
This section outlines the management of acute respiratory failure. For the management of chronic respiratory failure, see articles on specific causes, e.g., “COPD” and “Interstitial lung disease.”
Approach [6]
- Use ABCDE approach including IV access, pulse oximetry, and cardiac monitoring.
- Provide immediate respiratory support tailored to the underlying cause and severity of respiratory failure.
- Ascertain code status early if feasible.
- Identify and treat rapidly reversible causes of respiratory failure.
- Perform focused clinical evaluation.
- Obtain initial diagnostics: e.g., ABG, routine laboratory studies, ECG, CXR, POCUS
- Consider advanced diagnostic testing based on initial findings.
- Treat the underlying cause of respiratory failure.
Respiratory support
- Airway management: Secure the airway if clinical features of airway compromise are present.
- Rescue breaths: indicated immediately for patients in respiratory arrest
-
Oxygen therapy
- Indicated for SpO2 < 95%
- Consider HFNC for hypoxemic respiratory failure.
-
Mechanical ventilation [7]
- Consider indications for NIPPV and indications for invasive mechanical ventilation.
- Choose an appropriate ventilation strategy.
-
Adjust mechanical ventilator parameters as needed to correct hypercapnia and/or hypoxemia.
- ↑ Respiratory rate and/or ↑ tidal volume → ↑ ventilation
- ↑ FiO2 and/or ↑ PEEP → ↑ oxygenation
- See “Improving ventilation in mechanically ventilated patients” and “Improving oxygenation in mechanically ventilated patients” for further details.
Treatment of rapidly reversible causes of respiratory failure
- Tension pneumothorax: emergency chest decompression and chest tube placement
- Opioid-induced respiratory failure: naloxone
- Flash pulmonary edema: NIPPV, vasodilators for AHF
- Foreign body aspiration: maneuvers to dislodge an aspirated FB, emergency airway procedures for FBA
- Anaphylaxis: IM epinephrine
- Angioedema: C1 esterase inhibitor
- Status asthmaticus: bronchodilators, corticosteroids, magnesium
A-a gradient: alveolar-arterial gradient
ABG: arterial blood gas analysis
ALS: amyotrophic lateral sclerosis
ARDS: acute respiratory distress syndrome
AVM: arteriovenous malformation
CNS: central nervous system
DLCO: diffusing capacity of the lung for carbon monoxide
FiO2: fraction of inspired oxygen
GBS: Guillain-Barré syndrome
MG: myasthenia gravis
OHS: obesity hypoventilation syndrome
OSA: obstructive sleep apnea
PaCO2: partial pressure of carbon dioxide in arterial blood
PaO2: partial pressure of oxygen in arterial blood
RF: respiratory failure
V/Q mismatch: ventilation-perfusion mismatch
V/Q ratio: ventilation-perfusion ratio
© AMBOSS
Diagnosis
Respiratory failure and respiratory arrest are clinical diagnoses. ABG analysis, rapid laboratory studies, and bedside imaging can help identify the type of respiratory failure and guide treatment of the underlying cause.
Respiratory failure and arrest require immediate management, i.e., prior to diagnostic confirmation.
Initial investigations [6]
-
ABG: for diagnostic confirmation
- Alveolar-arterial gradient (A-a gradient): ([Patm - 47] × FiO2 - [PaCO2/0.8]) - PaO2
- Normal A-a gradient: hypoventilation or ↓ oxygen uptake
- ↑ A-a gradient: V/Q mismatch or shunting
- ↑ CO2 and ↓ pH: acute hypercapnia (see “Initial blood gas analysis”)
- CBC: to assess for anemia
- BMP: to assess for metabolic and electrolyte derangements
- ECG
- Consider the following based on clinical suspicion:
- BNP: to assess for acute heart failure
- Troponin: to assess for myocardial infarction
- D-dimer: to assess for pulmonary embolism
ABG analysis is key to diagnosing and classifying respiratory failure.
Bedside imaging [6]
- CXR: to assess for chest wall, pleural, and/or lung lesions (e.g., trauma, ARDS, pneumonia, pneumothorax, atelectasis, pleural effusion)
- POCUS: to assess lung, pleura, heart, pericardium, and deep veins (See “Lung POCUS” and “Focused cardiac ultrasound.”)
POCUS may help to quickly identify pneumothorax, pulmonary edema, pleural effusions, heart failure, cardiac tamponade, or the presence of DVT and/or signs of acute right heart strain suggesting pulmonary embolism.
Advanced diagnostic testing [6]
- CT chest: for detailed pulmonary evaluation (e.g., trauma, ARDS, tumor, pleural effusion, pneumonia)
- CTA chest: for suspected pulmonary embolism
- Echocardiography: for suspected heart failure, cardiac tamponade, or signs of right heart strain suggesting pulmonary embolism or pulmonary hypertension
- CT head: for suspected head trauma or stroke
- CO-oximetry: to assess for carbon monoxide toxicity or methemoglobinemia

A-a gradient: alveolar-arterial gradient
ABG: arterial blood gas analysis
ALS: amyotrophic lateral sclerosis
ARDS: acute respiratory distress syndrome
AVM: arteriovenous malformation
CNS: central nervous system
DLCO: diffusing capacity of the lung for carbon monoxide
FiO2: fraction of inspired oxygen
GBS: Guillain-Barré syndrome
MG: myasthenia gravis
OHS: obesity hypoventilation syndrome
OSA: obstructive sleep apnea
PaCO2: partial pressure of carbon dioxide in arterial blood
PaO2: partial pressure of oxygen in arterial blood
RF: respiratory failure
V/Q mismatch: ventilation-perfusion mismatch
V/Q ratio: ventilation-perfusion ratio
© AMBOSS
Click on the overlay icon below the taskbar on the left to toggle the overlay on and off.
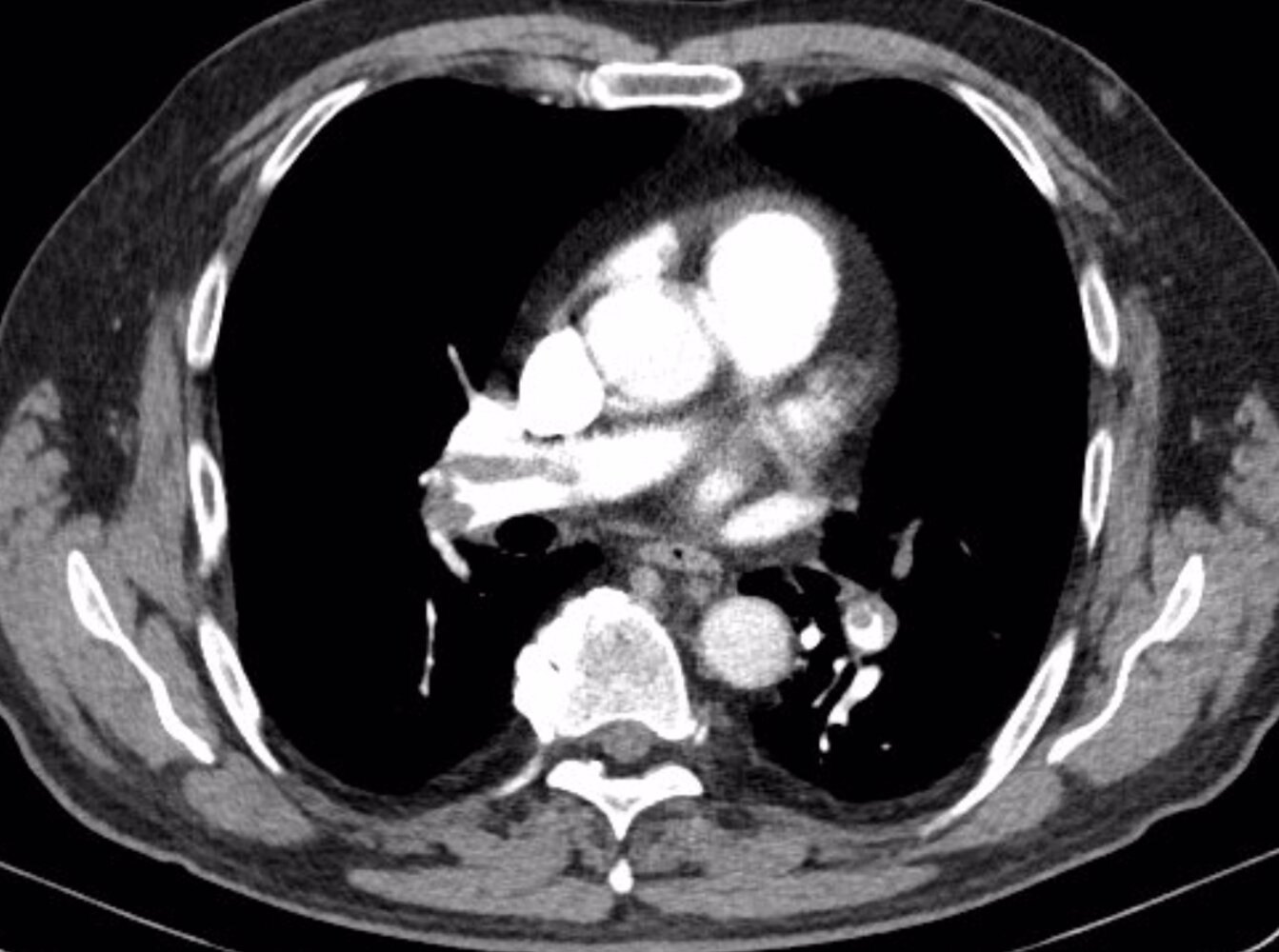
CT chest (with contrast; axial plane, lung window; axial plane, mediastinal window; coronal plane, mediastinal window) of a patient with shortness of breath, post-circulatory collapse, elevated D-dimer (5,086 ug/L; normal < 5), and normal C-reactive protein (CRP; < 3.0 mg/L)
Multiple intraluminal filling defects in the right and left pulmonary arteries and their lobar, segmental, and subsegmental branches represent pulmonary emboli of different age. The acute emboli are seen as central filling defects, whereas the older emboli are eccentric and show irregular thickening of the arterial wall.
Right ventricular and atrial enlargement, septal flattening, and contrast reflux into the hepatic veins are evidence of right ventricular strain. The causes of ground glass opacification in the left upper lobe and misty mesentery with nodes in the upper abdomen are not readily evident. Incidental findings include a hypodense cyst within a small, irregular left kidney and slight deformity of the right sixth rib from a previous fracture.
Our great thanks to Nándor Faluhelyi (University of Pécs, Medical School) for kindly providing this image.
Treatment
Treatment of the underlying cause of respiratory failure
The following is a nonexhaustive list of common causes of respiratory failure. See also “Rapidly reversible causes of respiratory failure.”
| Common causes of respiratory failure and their management | ||
|---|---|---|
| Suggestive features | Cause-specific management | |
| Upper airway causes of respiratory failure |
|
|
| Pulmonary causes of respiratory failure |
|
|
| Cardiac causes of respiratory failure |
|
|
| Toxic and metabolic causes of respiratory failure |
|
|
| CNS causes of respiratory failure |
|
|
Monitoring and disposition [6]
- Admit to the ICU for close monitoring and ongoing respiratory and/or hemodynamic support.
- Monitor respiratory and hemodynamic parameters.
- Follow serial ABGs.
- Consider repeating laboratory studies and/or chest imaging if the patient's clinical status changes.
- See also “Monitoring of mechanical ventilation.”
Complications
- Pulmonary: e.g., irreversible lung scarring after pulmonary embolism or pneumonia, ventilator dependence
- Cardiac: : e.g., arrhythmias, heart failure, cardiac arrest
- Neurological: : e.g., hypoxic brain injury, irreversible brain damage, brain death
- Renal: e.g., acute renal failure
- Gastrointestinal: e.g., stress ulcer, ileus
- Nutritional: e.g., hypoglycemia, electrolyte disturbances
- Other: hypoxic damage to other organs
We list the most important complications. The selection is not exhaustive.
Related One-Minute Telegram
- One-Minute Telegram 108-2024-2/3: Is 24/7 oxygen necessary for severe hypoxemia?
Interested in the newest medical research, distilled down to just one minute? Sign up for the One-Minute Telegram in “Tips and links” below.
External Resources
References
- Walls R, Hockberger R, Gausche-Hill M. "Rosen's Emergency Medicine". Elsevier Health Sciences. (2018). ISBN: 9780323354790
- Roberts JR. "Roberts and Hedges' Clinical Procedures in Emergency Medicine and Acute Care". Elsevier. (2018). ISBN: 9780323354783
- Schneider J, Sweberg T. "Acute Respiratory Failure". Crit Care Clin. 29(2). :167-183. (2013)
- "Contributor Disclosures - Respiratory failure and arrest. None of the individuals in control of the content for this article reported relevant financial relationships with ineligible companies. For details, please review our full conflict of interest (COI) policy:"
- Shebl E, Burns B. "Respiratory Failure". StatPearls. (2021)
- Kleinman ME, Brennan EE, Goldberger ZD, et al. "Part 5: Adult Basic Life Support and Cardiopulmonary Resuscitation Quality". Circulation. 132(18 suppl 2). :S414-S435. (2015)
- Kasper DL, Fauci AS, Hauser SL, et al. "Harrison's Principles of Internal Medicine". McGraw-Hill Education. (2015). ISBN: 9780071802161