Summary
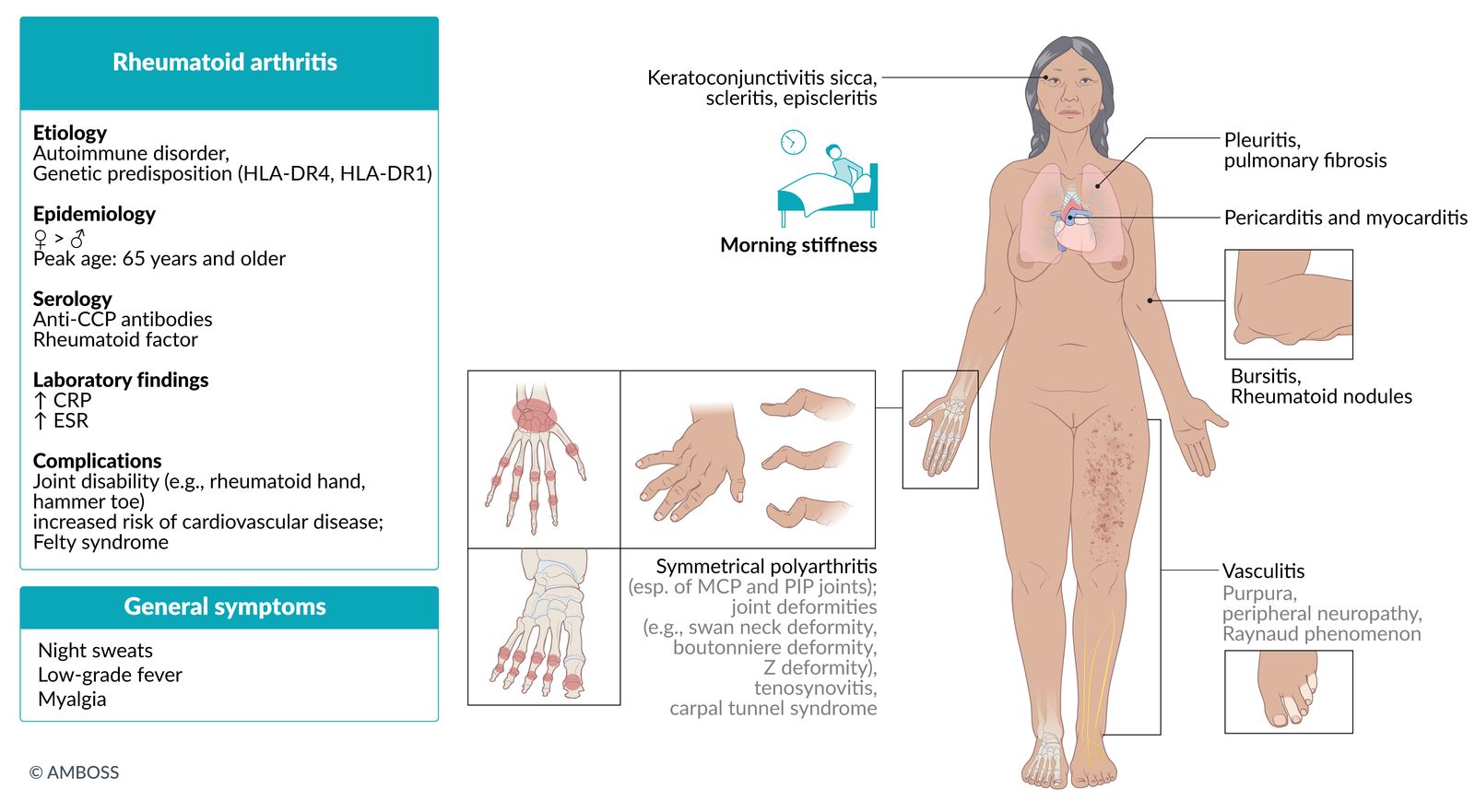
Rheumatoid arthritis (RA) is a chronic, systemic, inflammatory autoimmune disorder that primarily affects the joints (e.g., causes pain, swelling, synovial destruction, deformities), but may also manifest with extraarticular features (e.g., rheumatoid nodules, pulmonary fibrosis). The risk of RA increases with age, and the disease predominantly affects women. The diagnosis is clinical and may be supported by laboratory tests (e.g., rheumatoid factor, anticitrullinated peptide antibodies) and imaging studies (e.g., the presence of synovitis on ultrasound and, later in the disease course, bone erosions and/or joint space narrowing on x-rays). There is no curative therapy for RA but early intervention with disease-modifying antirheumatic drugs (DMARDs) using a treat-to-target strategy can prevent disease progression and RA-related disability.





© AMBOSS

© AMBOSS

© AMBOSS

© AMBOSS

© AMBOSS
Epidemiology
-
Prevalence
- ∼ 0.24% worldwide [1]
- 1% in northern Europe and US [2]
- Sex: : ♀ > ♂ (3:1) [3]
- Peak incidence: : 30–50 years [4]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
- Idiopathic inflammatory autoimmune disorder of unknown etiology
-
Risk factors include: [5]
- Genetic disposition: associated with HLA-DR4 and HLA-DR1 [6]
- Environmental factors (e.g., smoking)
- Female sex hormones: Risk of RA is increased in premenopausal individuals and in the first year postpartum.
- Infection (e.g., periodontitis) [7]
- Obesity
- Family history of RA
“A DRone with 4 propellers and 1 camera:” rheumatoid arthritis is associated with HLA-DR4 and HLA-DR1.
Pathophysiology
- Certain interstitial tissue proteins (e.g. intracellular filament protein vimentin, filaggrin, type II collagen) undergo a posttranslational modification that involves the conversion of arginine to citrulline (citrullination). [8]
- Citrullinated proteins are recognized as foreign by the antigen-presenting cells that present them to CD4+ T cells.
- Activation of CD4+ T cells leads to the following sequences of events: [9]
- IL-4 production → B-cell proliferation and differentiation → production of anticitrullinated peptide antibodies → type II hypersensitivity reaction and type III hypersensitivity reaction
- Migration of CD4+ T cells to synovial joints → secretion of cytokines (IFN-γ, IL-17) → recruitment of macrophages → secretion of cytokines (TNF-α, IL-1, IL-6) → inflammation and proliferation
- Bouts of inflammation, angiogenesis, and proliferation → proliferative granulation tissue with mononuclear inflammatory cells → pannus and synovial hypertrophy → invasion, progressive destruction, and deterioration of cartilage and bone
-
Antibodies against Fc portion of IgG (rheumatoid factor, RF) are produced to aid in removing autoantibodies and immune complexes.
- RF excess triggers formation of new immune complexes and type III HSR
- Individuals with positive RF are more likely to develop extraarticular manifestations. [10]

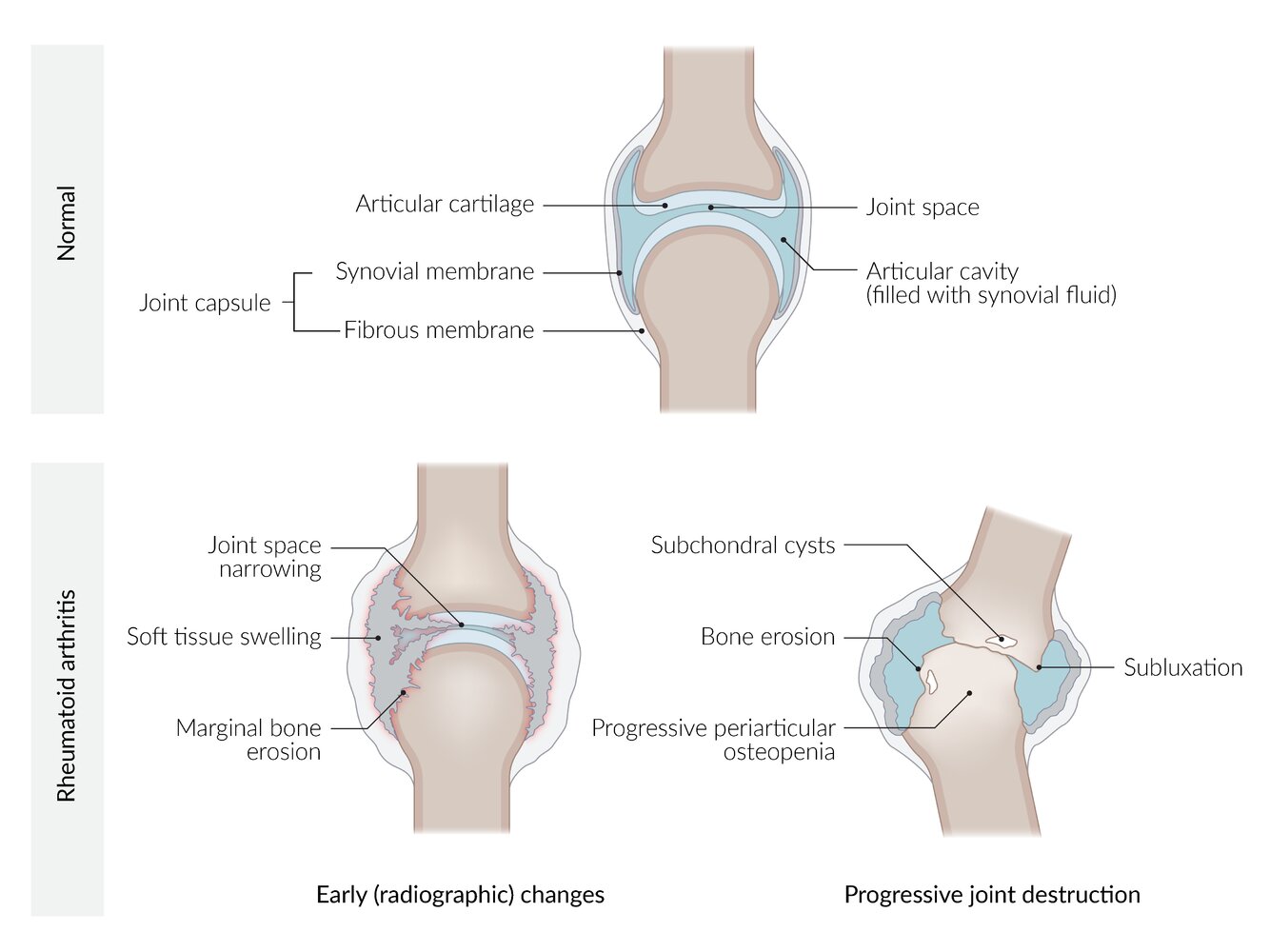
At the initial stage of the disease, there is non-specific inflammation of the synovial tissue, joint swelling, and erosion. Over the course of the disease, a progressive destruction and deterioration of cartilage and bone occurr, followed by a complete joint destruction with malpositioning, loss of mobility, and osteoporosis of the surrounding bones in the end stage of the disease.
© AMBOSS
Clinical features
Articular manifestations [11]
-
Polyarthralgia
- Symmetrical pain and swelling of affected joints (also at rest)
-
Frequently affected joints ; [12]
- Metacarpophalangeal joints (MCP joints)
- Proximal interphalangeal joints (PIP joints)
- Wrist joints
- Knee joints
- Metatarsophalangeal joints (MTP joints)
- Rarely affected: distal interphalangeal joints (DIP joints), first carpometacarpal (CMC) joint, and the axial skeleton (except for the cervical spine)
- Morning stiffness (often > 30 min) that usually improves with activity
-
Joint deformities
-
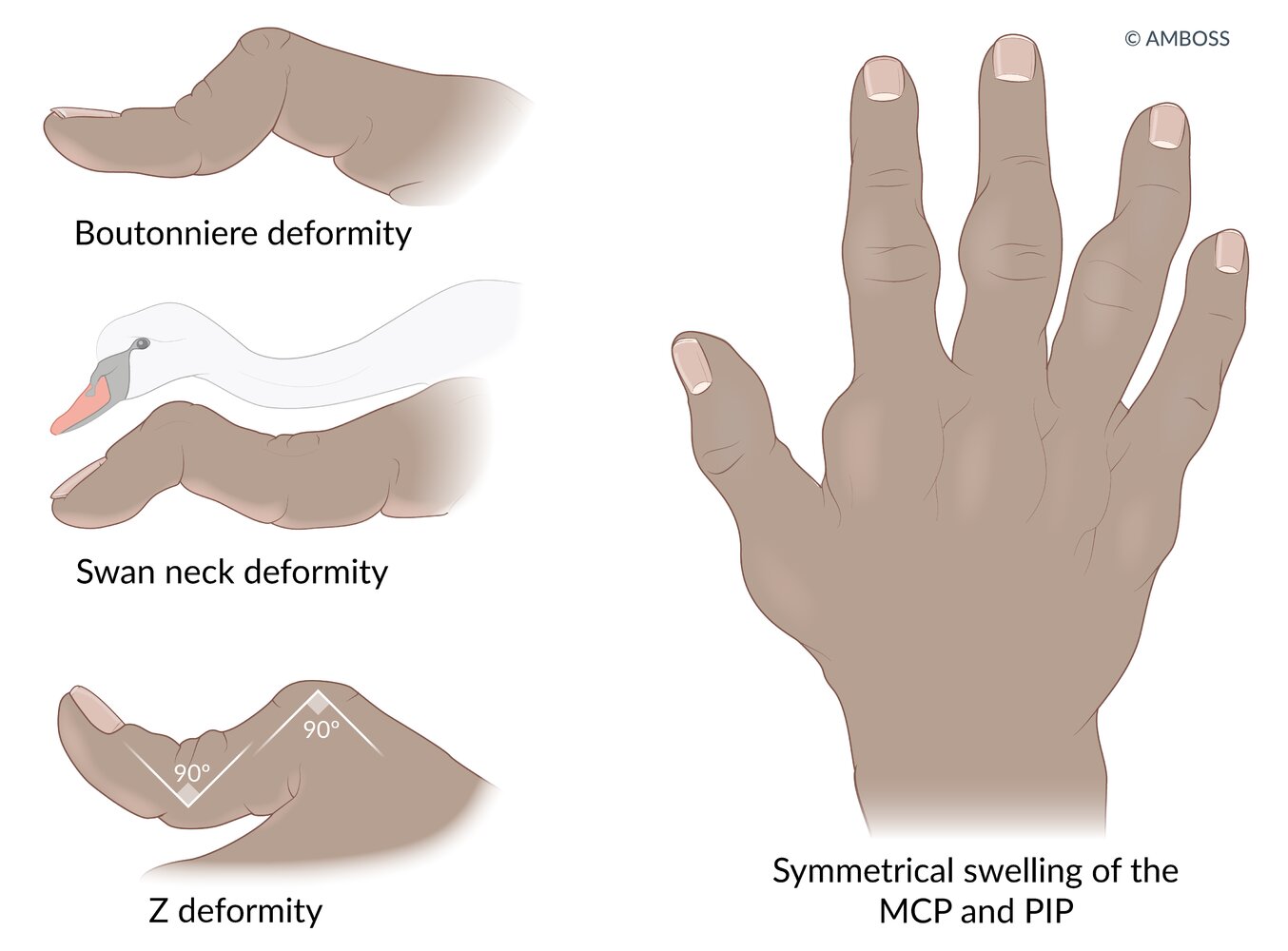
Rheumatoid hand is characteristic and typically manifests with one or more of the following deformities:
- Deepening of the interosseous spaces of the dorsum of hand
- Swan neck deformity: PIP hyperextension and DIP flexion
- Boutonniere deformity: PIP flexion and DIP hyperextension.
- Hitchhiker thumb deformity (Z deformity of the thumb): hyperextension of the interphalangeal joint with fixed flexion of the MCP joint [13]
- Ulnar deviation of the fingers
- Piano key sign: dorsal subluxation of the ulna
- Hammer toe or claw toe
- Atlantoaxial subluxation (see “Rheumatoid arthritis of the cervical spine” below)
-
Rheumatoid hand is characteristic and typically manifests with one or more of the following deformities:
-
Physical examination: compression test (Gaenslen squeeze test)
- Painful compression of hands (or feet) at the level of the MCP joint (metatarsophalangeal joint)
- Painful handshake is an early sign of arthritis
DIP joints are not typically affected in RA.






")
Extraarticular manifestations [14]
-
Constitutional symptoms
- Low-grade fever
- Myalgia
- Malaise
- Fatigue
- Weight loss
- Night sweats
-
Rheumatoid nodules
-
Skin
- Nontender, firm, subcutaneous swellings (2 mm–5 cm)
- Commonly occur in areas exposed to higher pressure, e.g., extensor side of the forearm, bony prominences
-
Lungs
- Typically bilateral and peripheral
- Rheumatoid pulmonary nodules may be accompanied by fibrosis and pneumoconiosis (Caplan syndrome).
-
Skin
-
Lungs
- Pleuritis, pleural effusions
- Interstitial lung disease (e.g., organizing pneumonia) [15]
- Eye: keratoconjunctivitis sicca, scleritis, and episcleritis [16]
- Endocrine and exocrine glands: secondary Sjogren syndrome
-
Hematological
-
Anemia
- Anemia of chronic disease (normocytic anemia)
- NSAIDs and/or steroids → increased risk of GI bleeding → iron deficiency anemia (microcytic anemia)
- Methotrexate → decreased folate level → macrocytic anemia
- Neutropenia
- Splenomegaly
- Large granular lymphocyte leukemia
- Lymphoma
-
Anemia
-
Musculoskeletal
- Tenosynovitis and bursitis
-
Carpal tunnel syndrome
- Typical nocturnal paresthesia of volar hand, thumb, index and middle fingers
- Atrophy of thenar muscles → difficulty making a fist and inability to oppose the thumb
- Tarsal tunnel syndrome
-
Heart
- Pericarditis and myocarditis
- Increased risk of myocardial infarction, stroke, CHF, and atrial fibrillation [17]
-
Vascular
- Peripheral vasculitis, manifests as livedo reticularis
- Raynaud phenomenon
- Purpura
- Vasculitic ulcers
- Necrosing fingertips
- Peripheral neuropathy



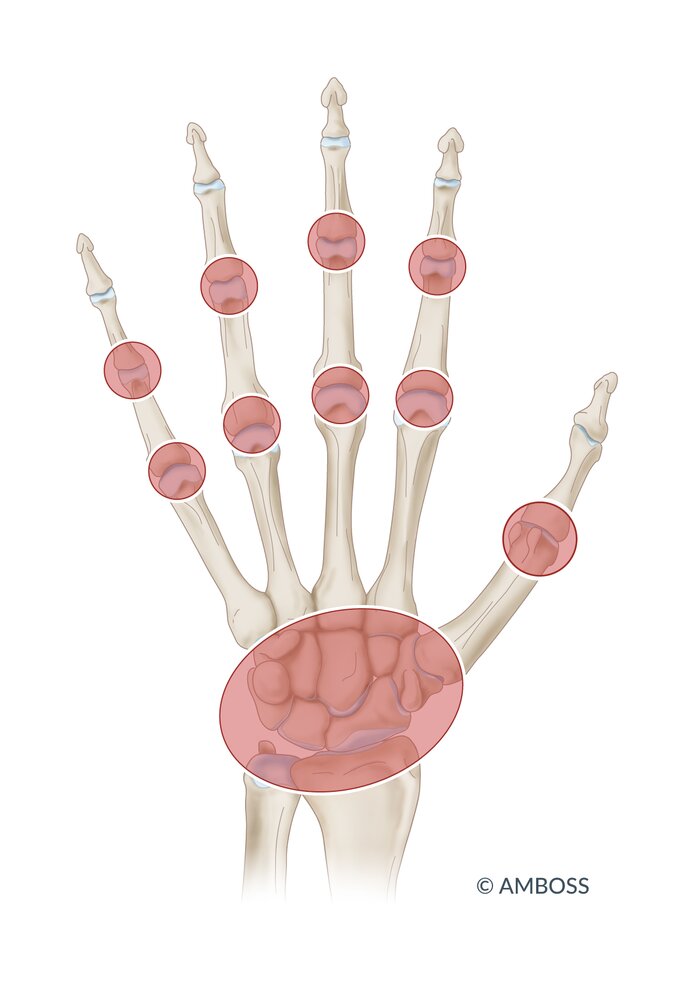
Symmetrical swelling of the metacarpophalangeal, proximal interphalangeal, and wrist joints.
© AMBOSS
© AMBOSS

Proximal interphalangeal joint hyperextension and distal interphalangeal joint flexion
Source: © IMPP

Characteristic appearance of the ring finger with flexed PIP and hyperextended DIP joints
This condition is the result of injury to or slippage of the central band of the extensor digitorum, usually caused by trauma (e.g., sports injury) or chronic inflammatory conditions such as rheumatoid arthritis.
Source: “Boutonnière deformity” by Alborz Fallah, Wikimedia Commons, licensed under CC BY-SA 3.0. Modifications: 90° counterclockwise rotation, converted to PNG file.
{kind=link}

Multiple deformations of the forefoot, in particular of the toes, which show severe lateral deviation and partial overlap. The large toe has deviated laterally and the first metatarsal head has deviated medially (hallux valgus/bunion).
Toes three and five show extension in the metatarsophalangeal joint and flexion in the interphalangeal joint, which is referred to as claw toe.
These findings are characteristic of advanced rheumatoid foot.
© AMBOSS
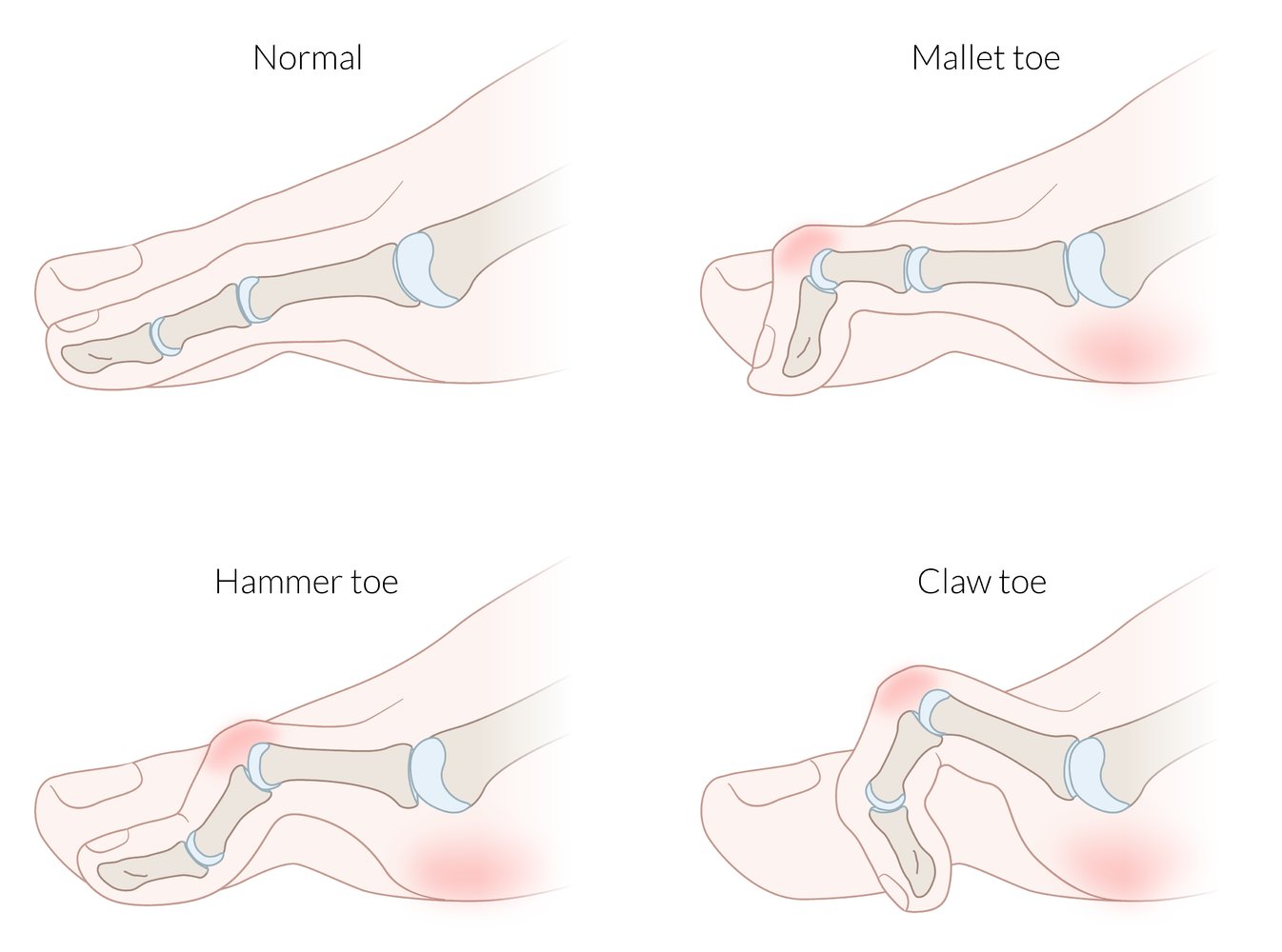
Common deformities of the lesser toes
Hammer toe: PIP flexion; DIP and MTP extension
Claw toe: PIP and DIP flexion; MTP extension
Mallet toe: DIP flexion; PIP and MTP extension
© AMBOSS
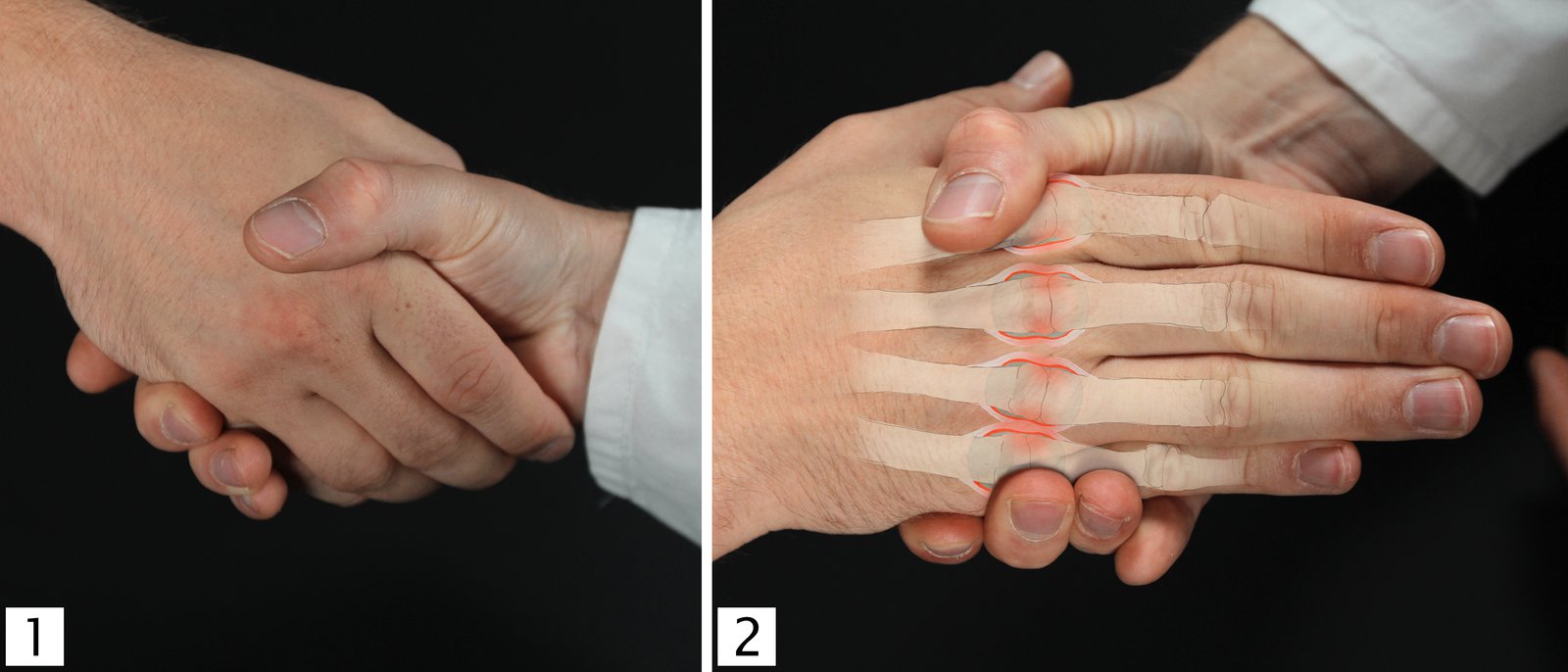
Tenderness on lateral compression of the metacarpophalangeal (MCP) joints can be an early sign of rheumatoid arthritis. This can be tested with a simple handshake when greeting the patient (1), or alternatively using more targeted compression of the hand at the level of the MCP joints (2).
© AMBOSS

A nodule is visible in the palm of this patient's hand.
This appearance is typical of rheumatoid nodules in rheumatoid arthritis.
Created by: Dr. Thomas Rath, Münster. Modifications to original image: Image slightly lightened.

Photograph of the hand of an elderly patient with rheumatoid arthritis (RA)
Multiple erythematous subcutaneous nodules are visible at the metacarpophalangeal, proximal interphalangeal, and distal interphalangeal joints. Involvement of the distal interphalangeal joints and redness are possible but uncommon in patients with RA.
Source: Courtesy of Dr. Gary M. White, MD

© Massachusetts Medical Society. All rights reserved. AMBOSS SE, exclusive licensee.
Pathology
- Synovial pannus formation and bone invasion: pathological layer of proliferative granulation tissue, mononuclear inflammatory cells, and fibroblast-like mesenchymal cells, releasing cytokines and enzymes, which, in turn, damage and invade the surrounding connective tissue [18]
- Synovial lining hyperplasia with mononuclear cell infiltrate
- Perivascular inflammatory infiltrates
- Angiogenesis
- Fibrin deposition on synovial surfaces
- Rheumatoid nodules: central fibrinoid necrosis with palisading histiocytes (epithelioid cells)

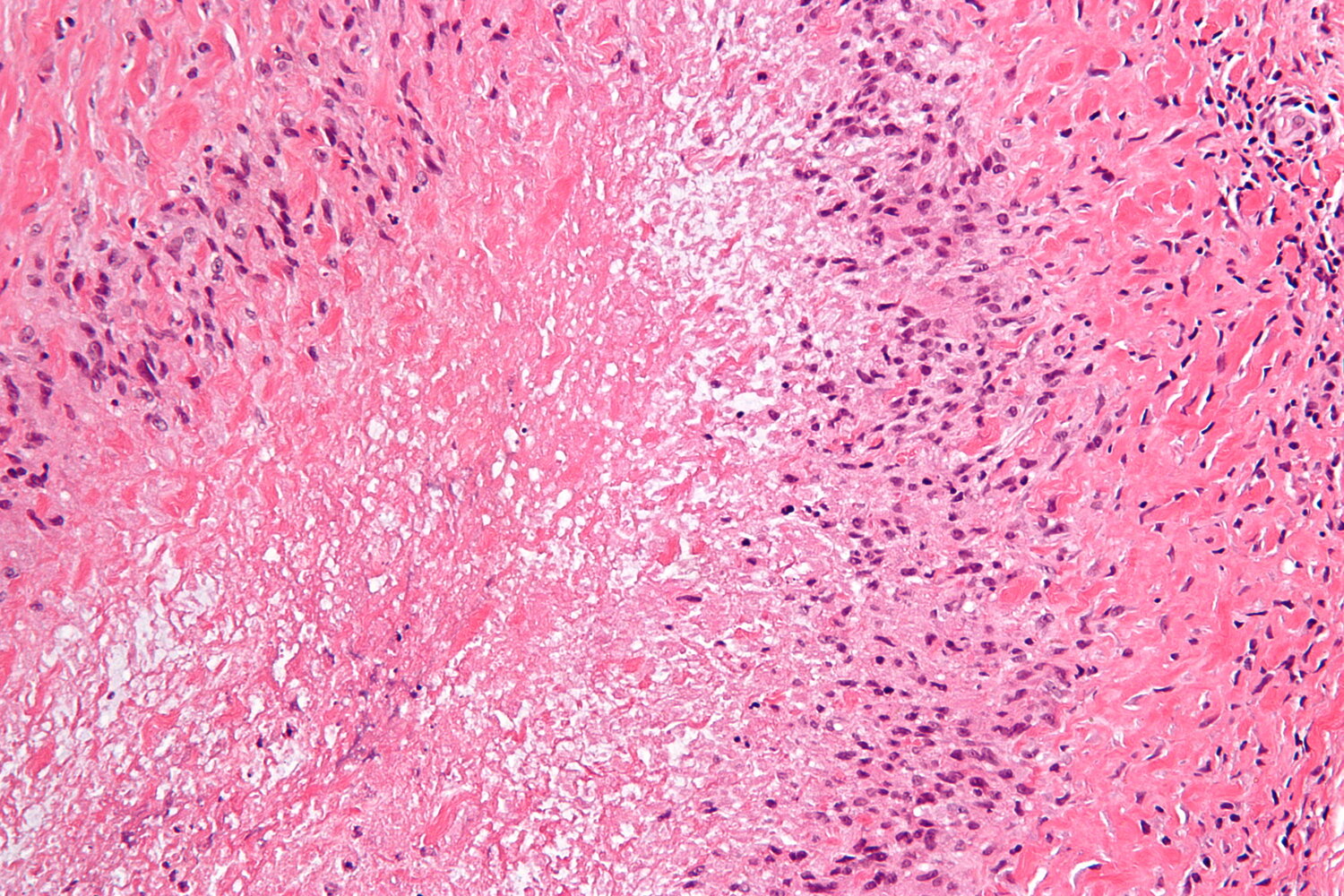
Photomicrograph of a rheumatoid nodule (H&E stain; high magnification)
Fibrinoid necrosis is visible as an accumulation of fibrin (blue overlay). Histiocytes (epithelioid cells) surround the necrotic area (yellow overlay). The outermost granuloma layer shows fibrosis (white overlay) and an abundance of lymphocytes (blue hatched overlay).
Rheumatoid nodules are a typical finding in patients with rheumatoid arthritis.
Source: “Rheumatoid nodule - high mag” by Michael Bonert ("Nephron"), Wikimedia Commons, licensed under CC BY 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
{kind=link}
Subtypes and variants
Rheumatoid arthritis of the cervical spine [12]
RA typically affects the cervical spine early in the course of the disease, while normally sparing the thoracic and lumbar spine. RA of the cervical spine most commonly manifests with atlantoaxial subluxation. Other patterns of instability are atlantoaxial impaction and subaxial subluxation.
Atlantoaxial subluxation
- Definition: a potentially life-threatening complication caused by the inflammatory destruction of the ligaments affecting the atlantoaxial joint and the intervertebral joints
-
Clinical features
- Pain and stiffness of the neck (typically early-morning neck pain at rest)
- Head tilt
- Neurological deficits
- Cervical radiculopathy with peripheral paresthesias of the upper limb
- In some cases, symptoms of high spinal cord compression (see also “Incomplete spinal cord injury”)
- Slowly progressive spastic quadriparesis
- Hyperreflexia or positive Babinski reflex
- Respiratory insufficiency
-
Diagnostics
- Extension and flexion x-rays of the cervical spine
- MRI
- Treatment: surgery if instability or myelopathy are present
Before undergoing general anesthesia, an airway and neck assessment is crucial in patients with RA, as atlantoaxial subluxation may be present, which increases the risk for spinal cord injury. Preoperative flexion-extension radiographs can help to evaluate the position of the cervical vertebra atlas (C1) with regard to the axis (C2).
Felty syndrome [12]
- Definition: a severe subtype of RA characterized by neutropenia and splenomegaly .
- Epidemiology: rare (1–3 % of patients with RA) [19]
-
Clinical features
- Clinical triad consisting of arthritis, splenomegaly, and neutropenia
- Other features
- Skin ulcers of the lower limbs (indicating vasculitis)
- Hepatomegaly
- Fever
- Chest pain (indicating pleuritis or pericarditis)
- Associated with increased risk of non-Hodgkin lymphoma
-
Diagnostics
- Leukopenia with selective neutropenia
- ↑ RF
- ↑ ACPA
-
Treatment
- DMARD: methotrexate
- Alternative: rituximab [20]
- Prompt and aggressive antibiotic treatment for suspected infections
- Consider splenectomy to treat leukopenia and improve the disease course.
- G-CSF (granulocyte-colony stimulating factor) in cases of severe granulocytopenia
- Complications: Neutropenia increases risk of recurrent bacterial infections.
Arthritis, splenomegaly, and neutropenia may suggest Felty syndrome.
Undifferentiated arthritis [7][21][22]
- Definition: symptoms of inflammatory arthritis that are not attributable to trauma or acute inflammatory events; often a transitional state preceding a definitive diagnosis [7][22]
-
Approach to management
- Refer to a rheumatologist for periodical follow-up.
- Management strategies are aimed at preventing progression and can be:
- Nonpharmacological: e.g., smoking cessation, oral health programs [7]
- Pharmacological: DMARDs [23]
-
Prognosis [23]
- Spontaneous remission in approx. 50% of patients
- RA develops in approx. one-third of patients [21]
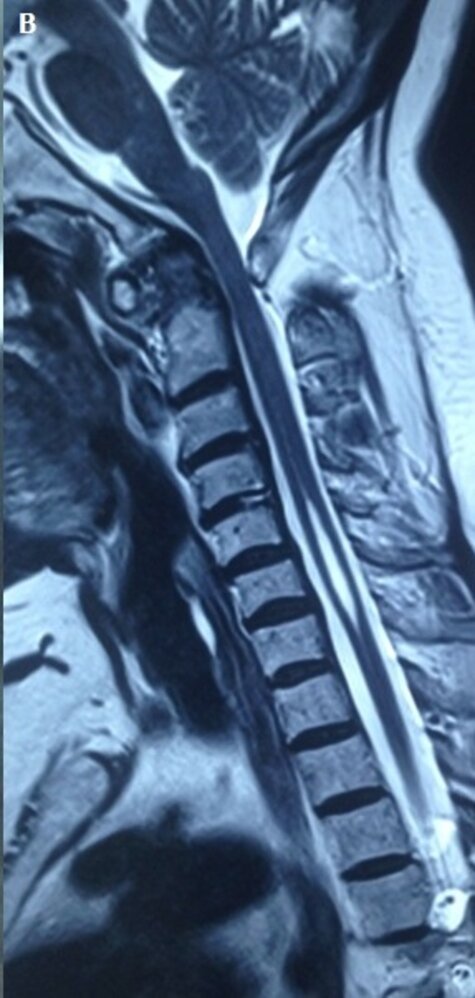
MRI cervical spine (T1-weighted; sagittal view) of a 64-year-old woman with a 12-year history of rheumatoid arthritis and increasing neck pain for 3 months
There are erosive changes to the odontoid process (dens; D). The distance between the dens and the anterior arch of the atlas (A) is widened due to (inflammatory) tissue proliferation ventrally to the dens (green overlay), causing posterior subluxation of the dens. This, in turn, has led to narrowing of the spinal canal between the dens and the posterior arch of the atlas, causing compression of the spinal cord (red overlay).
A syrinx is seen at C5–C7 (yellow overlay).
Source: “Figure 1B, in: Syringomyelia associated to rheumatoid-atlantoaxial subluxation: about a new case” by Kaffel D, Hamdi W, Pan African Medical Journal, licensed under CC BY 4.0. Modifications: Image cropped. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Diagnosis
Approach [7][24][25]
- The diagnosis of RA is clinical.
- Consider RA in patients with arthralgia, joint stiffness, and synovitis lasting ≥ 6 weeks (see “Clinical features”).
- Consider alternative diagnoses in patients with atypical presentations (see “Differential diagnoses”).
- Perform diagnostic studies to further support the diagnosis and help establish disease severity.
- Routine laboratory tests. [7][25]
- X-ray as the initial imaging study
- Consult rheumatology, particularly if the diagnosis is uncertain and when choosing a treatment regimen.
RA is a clinical diagnosis. The 2010 ACR/EULAR classification criteria for RA can help identify RA, but the criteria do not need to be fulfilled in order to establish a diagnosis. [24]
Laboratory studies [7][25]
Routine studies
-
Nonspecific parameters
-
↑ Inflammatory markers
- ↑ CRP and ↑ ESR
- Other acute phase reactants may also be elevated (e.g., ferritin).
- CBC: anemia of chronic disease, thrombocytosis
- TFTs: to rule out an autoimmune thyroid disease, which is common in patients with RA
- Serology: ↑ ANAs in 30–50% of patients with RA [21]
-
↑ Inflammatory markers
-
Specific parameters (serological studies) [7][26]
- Anticitrullinated peptide antibodies; (ACPA), e.g., anticyclic citrullinated peptide (anti-CCP) [27]
- Rheumatoid factor; (RF): IgM autoantibodies against the Fc region of IgG antibodies [21]
- Serological studies may be negative (i.e., seronegative RA)
| Serological testing in rheumatoid arthritis [7][21][26][28] | |||
|---|---|---|---|
| Sensitivity | Specificity | Other | |
| ACPA |
|
|
|
| RF |
|
|
|
| ANA |
|
|
|
Approx. 30% of patients with RA are negative for ACPA and RF. [25]

Additional studies
Additional studies should be considered on an individual basis.
-
Synovial fluid analysis: not routinely recommended [25]
- Indications
- Suspicion of septic arthritis
- Atypical presentation, to rule out differential diagnoses (e.g., gout)
-
Findings are nonspecific [21]
- Cloudy, yellow appearance
- Sterile specimen with leukocytosis (WBC count 5,000–50,000/μL)
- ↑ Neutrophils, granulocytes, and ragocytes
- ↑ Protein level
- Possibly RF
- Indications
-
ASCVD risk assessment [7][25]
- Recommended in all patients with RA, as RA is an ASCVD risk-enhancing factor
- Includes diabetes mellitus screening, screening for lipid disorders, and a risk calculation using the 2013 ACC/AHA pooled cohort equation
ASCVD is the most common cause of premature death in patients with RA; therefore, an ASCVD risk assessment is recommended in all patients with RA.
Imaging studies [25][29][30]
While x-ray is recommended as the initial test, ultrasound and MRI might additionally be necessary to assess joint disease severity.
-
X-ray: initial test
- Studies
- Baseline radiographs of both hands (dorsopalmar view) and feet
- Radiographs of symptomatic joints
-
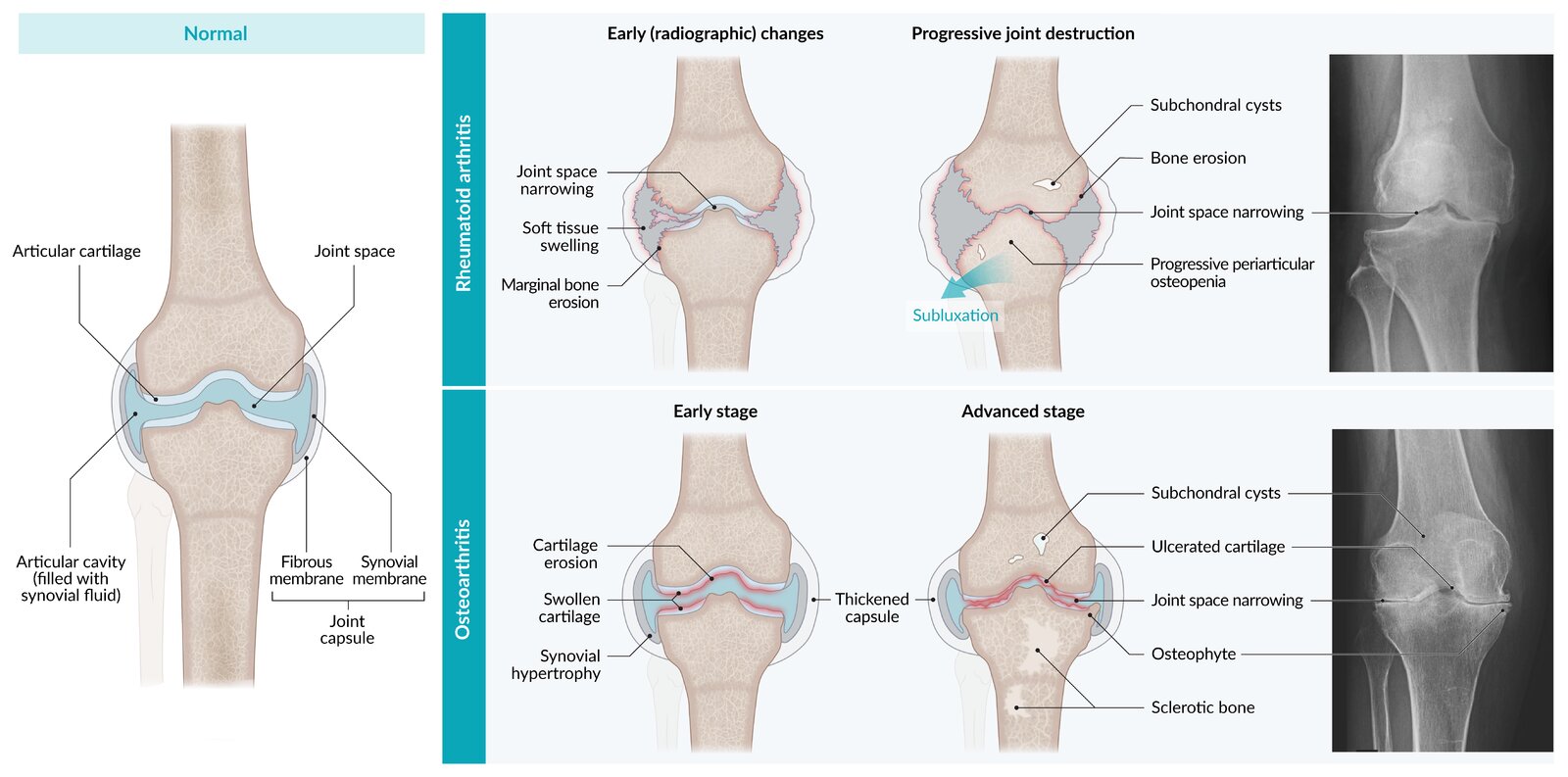
Findings
- Early: soft tissue swelling, osteopenia (juxtaarticular)
- Late: joint space narrowing, marginal erosions of cartilage and bone, osteopenia (generalized), subchondral cysts
- Studies
-
Ultrasound [31]
- Indication: If available, perform on affected joints to detect clinical or subclinical synovitis.
- Supportive findings
- Early signs of inflammation: e.g., subclinical synovitis (synovial hyperemia)
- Synovial proliferation (pannus formation)
- Joint effusion: increased fluid (e.g., pus, blood, inflammatory infiltrate) within the synovial compartment of a joint
- Using contrast can increase the sensitivity of detecting inflammation.
-
MRI of the affected joints (with or without contrast)
- Can help detect early changes in large joints (e.g., subclinical synovitis)
- Consider especially if cervical spine involvement is suspected (see “Atlantoaxial subluxation”).
- Further imaging studies: Perform if extraarticular manifestations are suspected (e.g., a CT scan for interstitial lung disease, an echocardiogram for pericarditis).
Typical RA findings on x-rays may be subtle or absent upon diagnosis in many patients with early RA; therefore, ultrasound or MRI may be more informative, as they have higher sensitivity for detecting early signs of inflammation and erosion.
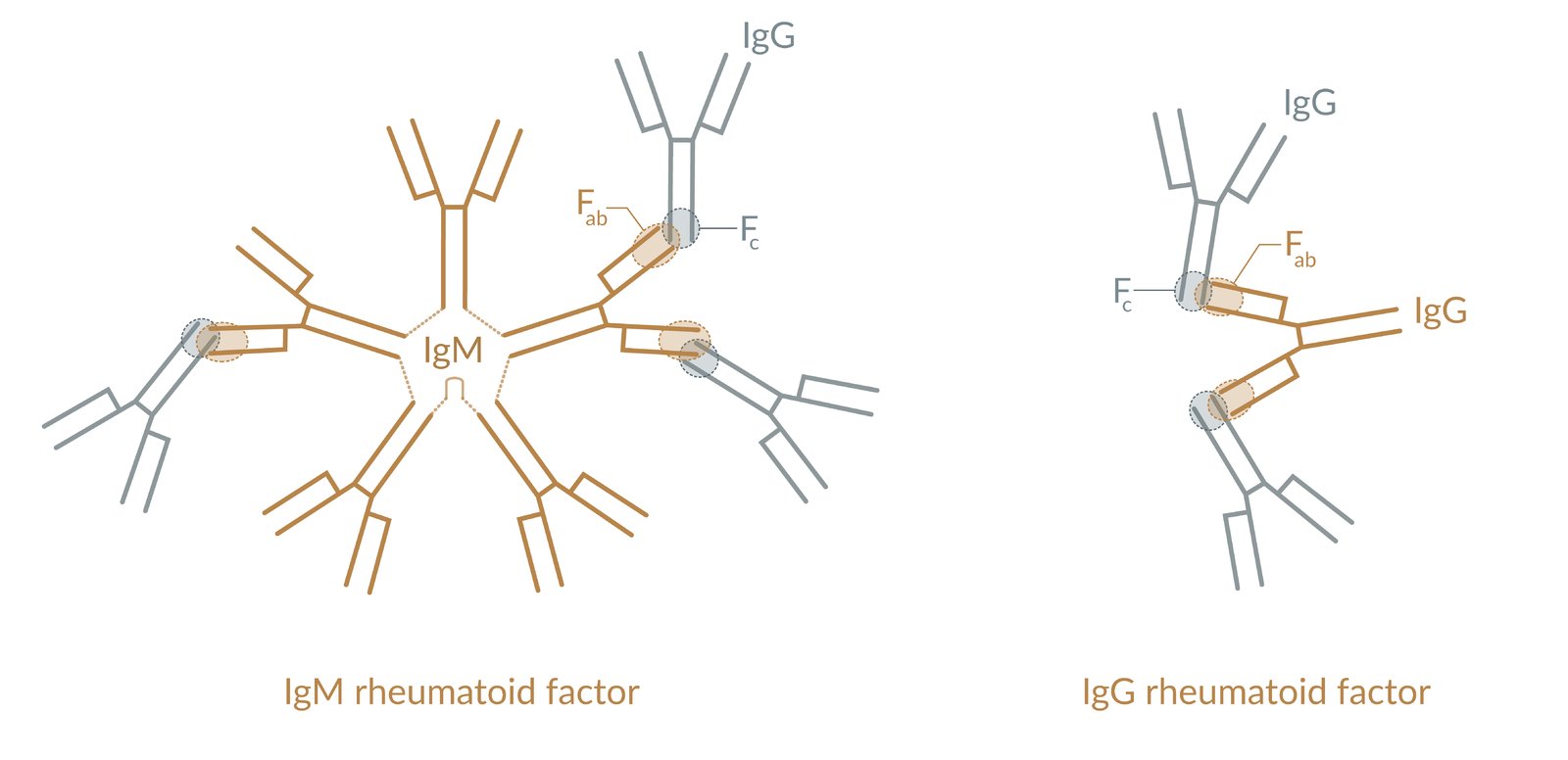
Rheumatoid factors are autoantibodies that bind to the Fc receptor of endogenous immunoglobulin G (IgG) with their Fab receptor. There are different rheumatoid factors, depending on the immunoglobulin isotype that forms the autoantibody. Shown here are the IgM and IgG rheumatoid factor.
© AMBOSS

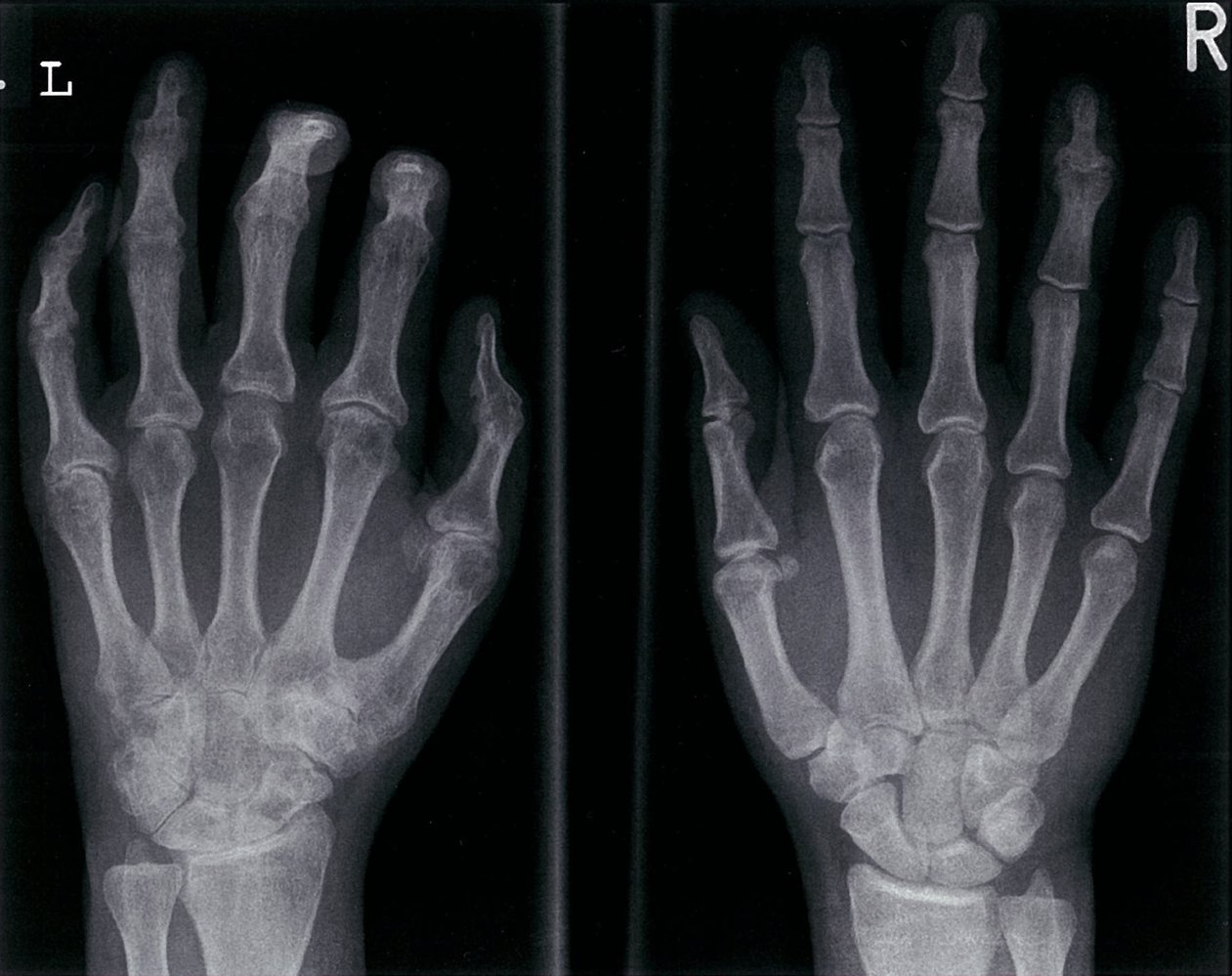
X-ray hands (PA view)
There is generalized periarticular osteopenia (example indicated by green overlay) and narrowing of several metacarpophalangeal and proximal interphalangeal joint spaces (example indicated by green line). The marked deformity of the wrists is the result of numerous carpal, base of metacarpal, and radiocarpal erosions (red lines). Erosive scalloping (example indicated by yellow line) also involves the radioulnar joint.
The radiographic findings are typical of rheumatoid arthritis with advanced wrist involvement.
© AMBOSS. This image was adapted from the image “AsymmetricRheumatoidArthritis” by Golan Levin, Flickr, licensed under CC BY 2.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
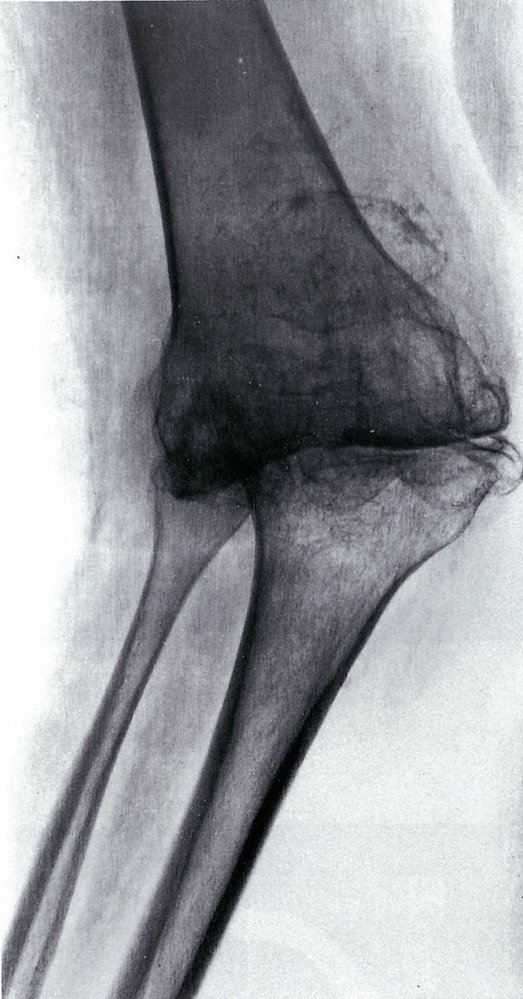
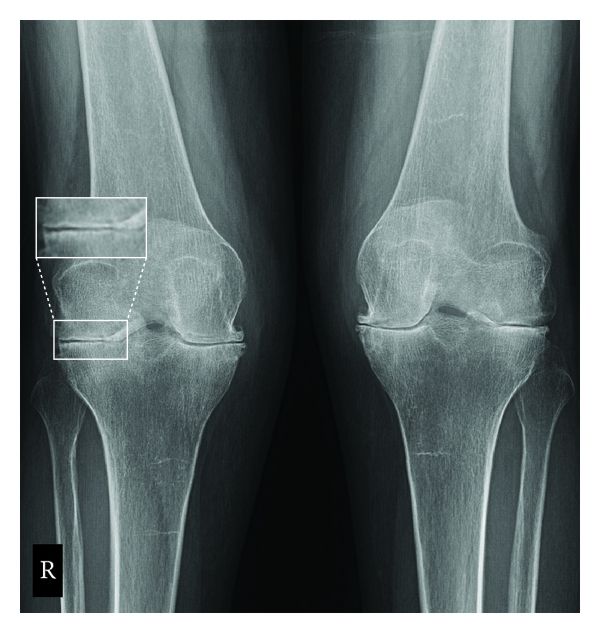
X-ray right knee (AP view)
Diffuse osteopenia is accompanied by uniform joint space narrowing (indicated by the yellow line), severe erosive changes, and valgus deformity. Secondary changes of osteoarthritis can be seen, including osteophytosis (examples indicated by the red overlay) and subchondral sclerosis (green overlay).
Source: © IMPP
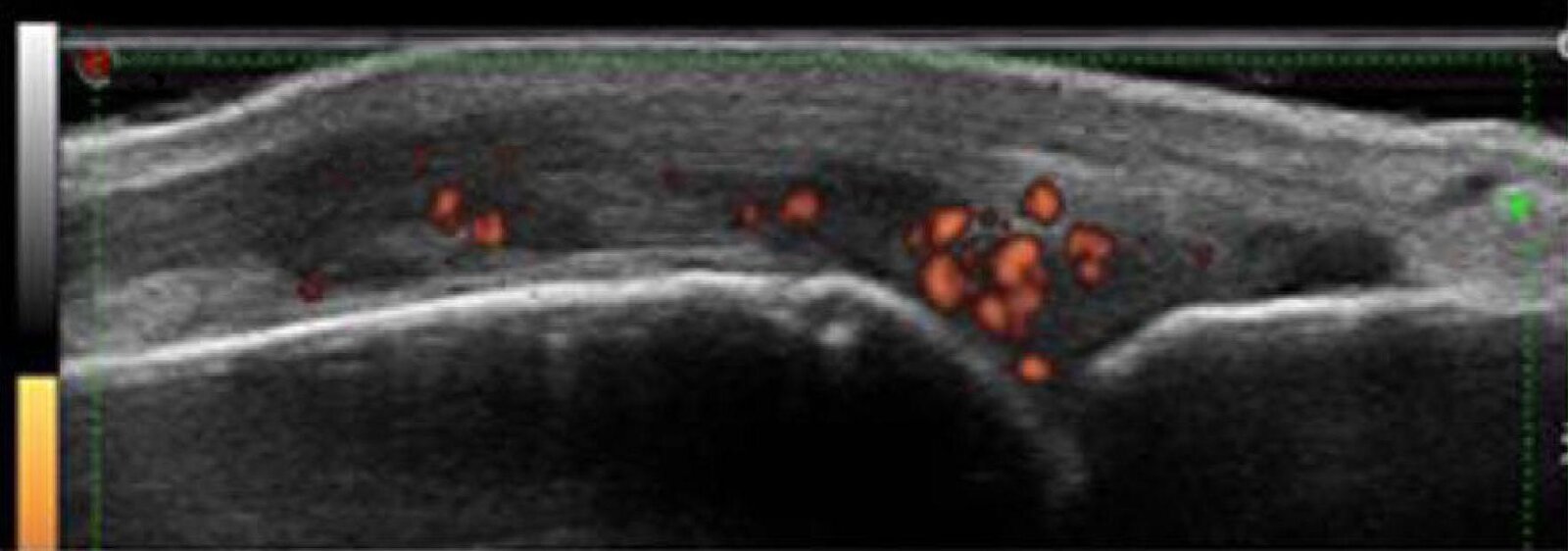
Ultrasound finger (dorsal metacarpophalangeal joint; with power Doppler; longitudinal plane)
Marked hypoechoic synovial proliferation (examples indicated by arrows) is associated with moderate inflammatory activity, seen as vascular enhancement (red) on power Doppler.
Source: “Fig. 1, in: Ultrasound and its clinical use in rheumatoid arthritis: where do we stand?” by Prado AD, Staub HL, Bisi MC, Silveira IG, Mendonça JA, Polido-Pereira J, Fonseca JE, Scielo, licensed under CC BY 4.0. Modifications: -Image was cropped -arrow and letter removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
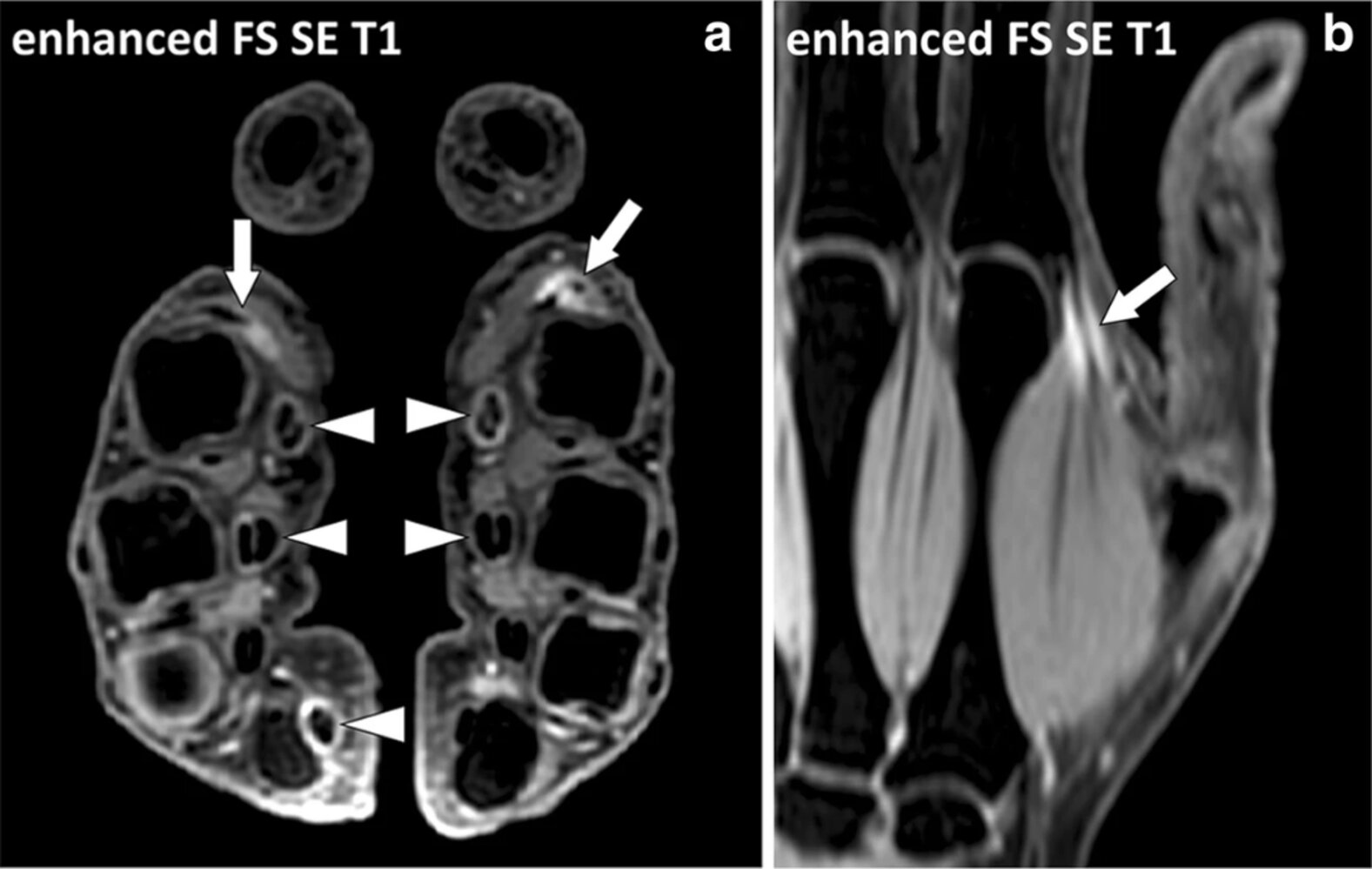
MRI hands (with contrast, fat-suppressed T1-weighted, a: axial plane of both hands, b: coronal plane of the left hand) of a patient with seropositive, non-erosive rheumatoid arthritis
Contrast enhancement in the area of the musculotendinous junction of the interosseus dorsalis I muscle on both sides (arrows) can be seen as a sign of inflammatory changes. In addition, contrast enhancement of the tendon sheaths of the flexor digitorum muscles (arrowheads) indicate a tendovaginitis.
Source: “Fig 21, In: Fasciae of the musculoskeletal system: normal anatomy and MR patterns of involvement in autoimmune diseases” by Kirchgesner T, Demondion X, Stoenoiu M et al., SpringerOpen, licensed under CC BY 4.0.
X-ray right and left knee (PA view)
Joint space narrowing involves both the medial and lateral compartments (arrows and lines). Mild valgus deformity is present bilaterally. Bilateral osteopenia and periarticular erosions (green overlay in magnification) are seen. There is relatively little subchondral sclerosis or osteophyte formation (example indicated by red overlay).
In contrast to osteoarthritis, rheumatoid arthritis typically involves the non-weight-bearing portion of the knee joint. Joint space loss involves all compartments and there is a comparative lack of subchondral sclerosis and osteophytosis. Joint effusion may accompany synovial inflammation.
Source: “Fig. 1, in: Total Knee Arthroplasty Considerations in Rheumatoid Arthritis” by Danoff JR, Moss G, Liabaud A, Geller JA, Hindawi, licensed under CC BY 3.0. Modifications: - magnification added. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
RA activity assessment
Disease activity can be estimated by evaluating a combination of clinical and laboratory features. Disease activity scores may be used to assess RA activity and help guide a treat-to-target strategy (see “Treatment”). The ACR has recommended numerous disease activity scores for clinical practice, including the following: [32]
- Clinical Disease Activity Index
| Clinical Disease Activity Index (CDAI) [7][32][33] | |
|---|---|
| Parameter | Score |
| 28-joint physical examination: swollen joints | 0–28 |
| 28-joint physical examination: tender joints | 0–28 |
| Patient global assessment | 0–10 on a visual analog scale |
| Evaluator global assessment | 0– 10 on a visual analog scale |
Interpretation: add scores
| |
- Simplified Disease Activity Index (SDAI) : includes CDAI parameters plus CRP
- Disease Activity Score with 28-joint count (DAS28) : includes CDAI parameters plus ESR or CRP , but does not include the evaluator global assessment
Consider the influence of concomitant conditions such as fibromyalgia or depression on subjective parameters (i.e., tender joint count and patient or evaluator global assessment) to help prevent patient misclassification.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
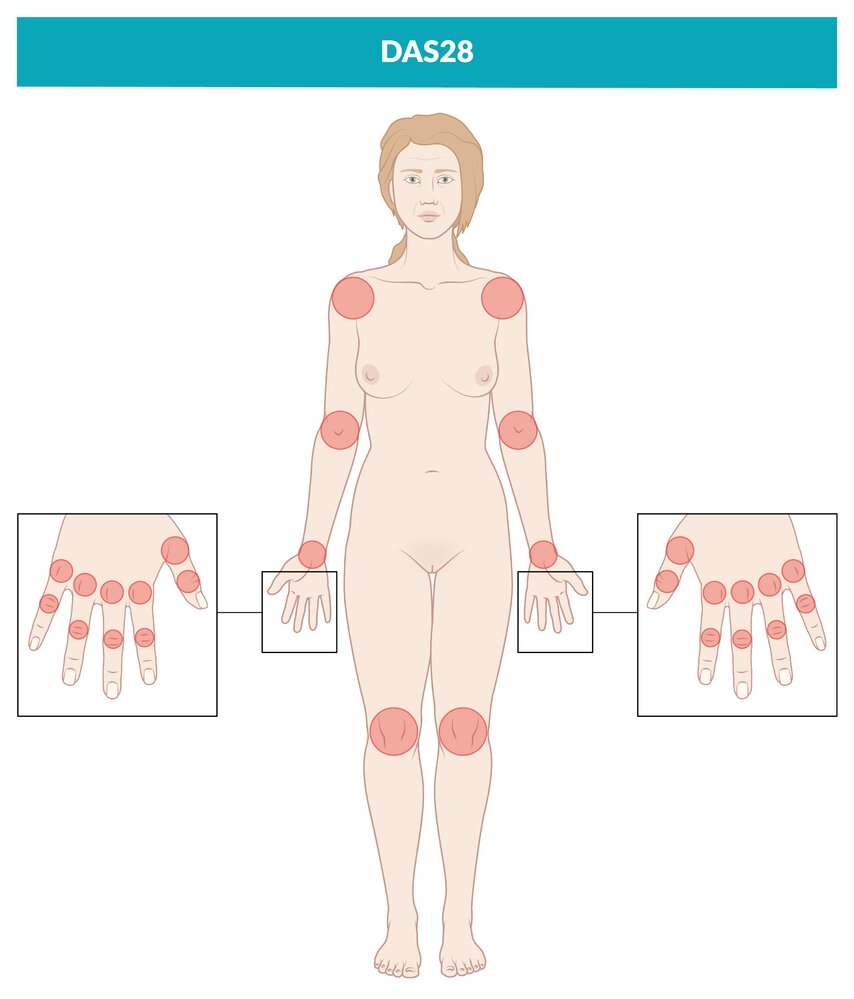
The DAS28 score (Disease Activity Score for the assessment of 28 joints) is used to estimate rheumatoid arthritis disease activity.
The 28 joints included are the interphalangeal joint of the thumb, the 2nd through 5th proximal interphalangeal joints, the 1st through 5th metacarpophalangeal joints, the wrists, elbows, shoulders, and knees.
© AMBOSS
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
Differential diagnoses
| Common causes of chronic arthropathy | |||||
|---|---|---|---|---|---|
| Condition | Rheumatoid arthritis (RA) | Osteoarthritis | Psoriatic arthritis | Gout | Pseudogout |
| Epidemiology |
|
|
|
|
|
| Risk factors |
|
|
|
|
|
| Course of disease |
|
|
|
|
|
| Clinical features |
|
|
|
|
|
|
|
||||
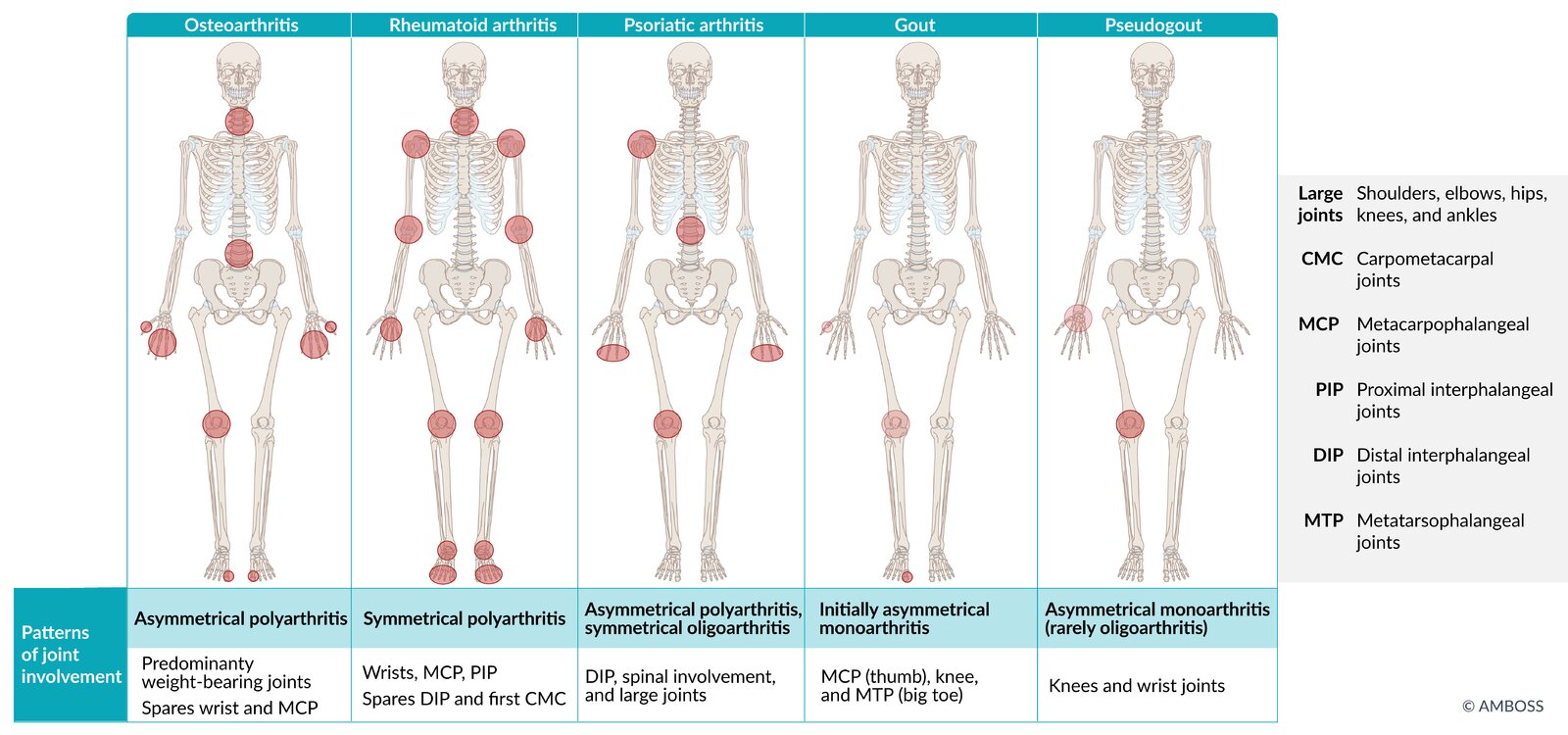
| Symmetry of joint involvement |
|
|
|
|
|
| Pattern of disease |
|
|
|
|
|
| Laboratory findings |
|
|
|
|
|
| Imaging |
|
|
|
|
|
-
Other differential diagnoses
- Autoimmune-related arthritis (e.g., sarcoidosis, SLE, rheumatic fever, mixed connective tissue disease, polymyalgia rheumatica)
- Enteropathic arthritis
- Vasculitides
- Hemochromatosis
- Viral arthritis (e.g., parvovirus B19, hepatitis viruses)
- Lyme arthritis
- Reactive arthritis (post-urethritis, post-enteritis)
- Juvenile idiopathic arthritis
- CPPD disease
- Basic calcium phosphate crystal deposition diseases
- Fibromyalgia
- Soft tissue rheumatic disorders: a group of common nonsystemic focal syndromes characterized by nonarticular pain
- Hypertrophic osteoarthropathy: typically characterized by periosteal reaction in the metaphyses and diaphyses of long bones and associated with lung disease (e.g., lung cancer)
-
Palindromic rheumatism: autoinflammatory and autoimmune disorder [34]
- Characterized by relapsing episodes of joint pain, swelling, and stiffness that typically last 12–72 hours followed by asymptomatic periods lasting days to months
- May progress to RA or other autoimmune conditions (e.g., SLE)









The differential diagnoses listed here are not exhaustive.
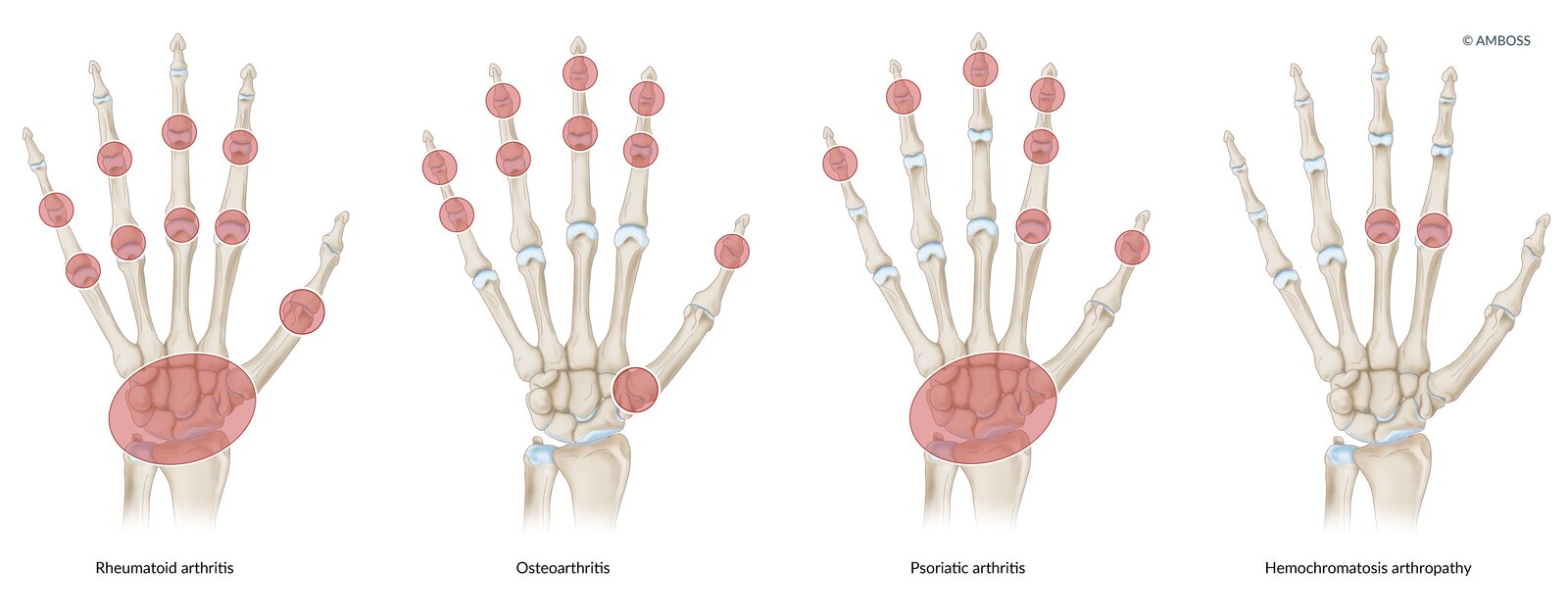
Rheumatoid arthritis: symmetrical swelling of metacarpophalangeal (MCP) and proximal interphalangeal (PIP) joints
Osteoarthritis: PIP, distal interphalangeal (DIP), and first carpometacarpal (CMC) joints
Psoriatic arthritis: DIP and MCP joints, or whole digit (dactylitis)
Hemochromatosis: symmetrical arthropathy of the MCP joint of the second and third digits
© AMBOSS
© AMBOSS
X-ray hands (PA view)
There is generalized periarticular osteopenia (example indicated by green overlay) and narrowing of several metacarpophalangeal and proximal interphalangeal joint spaces (example indicated by green line). The marked deformity of the wrists is the result of numerous carpal, base of metacarpal, and radiocarpal erosions (red lines). Erosive scalloping (example indicated by yellow line) also involves the radioulnar joint.
The radiographic findings are typical of rheumatoid arthritis with advanced wrist involvement.
© AMBOSS. This image was adapted from the image “AsymmetricRheumatoidArthritis” by Golan Levin, Flickr, licensed under CC BY 2.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

X-ray right hand (PA view)
Typical features of osteoarthritis are visible at the first carpometacarpal joint (green circle), including joint space narrowing (blue line), subchondral sclerosis (increase in bone density; green overlay), and marginal osteophytes. A subchondral cyst (geode; red overlay) has formed at the base of the first metacarpal (MC1). Findings of early osteoarthritis also involve several other joints of the hand and wrist (indicated by red arrows).
T: Trapezium
Source: © IMPP
X-ray hands (PA view)
Asymmetric advanced arthritis involves the left hand, with ankylosis of several proximal and distal interphalangeal (PIP and DIP) joints (examples indicated by green overlay) along with multiple flexion deformities. Marginal erosions are present at the bases of the small finger proximal phalanx and thumb distal phalanx (red overlay). Central subchondral erosions and proliferative changes with a gull-wing deformity are seen at the right ring finger DIP joint.
Also shown is an illustration of a pencil-in-cup deformity (not present here), which can occur in psoriatic arthritis and several other inflammatory arthritides.
Advanced degenerative changes additionally involve multiple left carpal and metacarpal joints.
Source: © IMPP

X-ray knee (AP view)
Calcification (green overlay) is seen within the menisci and articular hyaline cartilage of the medial and lateral compartments of the knee.
The chondrocalcinosis was the result of calcium pyrophosphate dihydrate disease (CPPD).
Source: © IMPP

X-ray knees (AP standing view)
Marked bilateral medial compartment joint space narrowing is accompanied by surface irregularity (indicated by red lines), subchondral sclerosis (example indicated by green overlay), and prominent osteophytes (examples indicated by arrowheads). Subluxation of the medial femoral condyles is also seen (indicated by dashed arrows). The lateral compartments show only mild degenerative changes.
Source: “Fig. 3A, in: Arthroscopic cartilage regeneration facilitating procedure for osteoarthritic knee” by Lyu SR, Hsu CC, Lin CW, BMC Musculoskeletal Disorders, licensed under CC BY 2.0. Modifications: Image is cropped, letter "A" is removed, date removed, round metal BBs removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
© AMBOSS
© AMBOSS
Treatment
Approach [7][25][35]
- Initiate acute antiinflammatory treatment with glucocorticoids and NSAIDs for disease flares.
- Long-term treatment
- Initiate treatment with conventional DMARD monotherapy.
- Consider short-term concomitant antiinflammatory treatment.
- Initiate nonpharmacological management.
- Consider surgical treatment in specific cases (e.g., patients with severe joint deformities).
Consult a rheumatologist before initiating treatment.
Acute antiinflammatory treatment [7][25][35]
Temporary (< 3 months) symptomatic treatment with glucocorticoids and/or NSAIDs is indicated for disease flares (i.e., episodes of increased disease activity and symptom worsening). [36]
-
Glucocorticoids
-
Systemic prednisone
- Short-term (i.e., < 3 months) therapy at the lowest effective dose is preferred.
- Longer-term therapy: Only use in patients with highly active RA who do not respond to maximum doses of DMARDs. [7][35]
- See also “Side effects of glucocorticoid therapy” and “Preventing complications of long-term glucocorticoid therapy” in “Glucocorticoids.”
- Intraarticular injections (e.g., with triamcinolone acetonide) can be considered by specialists alongside treatment with DMARDs in patients with predominant symptoms in ≥ 1 medium or large joint.
-
Systemic prednisone
-
NSAIDs and selective COX-2 inhibitors: : relieve symptoms, but do not improve the prognosis
- Ibuprofen
- Diclofenac
- Celecoxib
- Other measures: If a flare occurs due to medication tapering, restart the previous effective treatment regimen.
Glucocorticoids should be used at the lowest effective dose and only for short periods of time to reduce the risk of their many adverse effects (e.g., hypertension, osteoporosis, infections). [25][35]
Long-term pharmacological treatment [7][25][30][35]
Initiation of treatment
- All patients (regardless of baseline disease activity or disease duration): monotherapy with a conventional DMARD
- Consider short-term concomitant use of acute antiinflammatory therapy (i.e., glucocorticoids and/or NSAIDs) for symptom control until the onset of action of DMARDs (e.g., ≥ 6 weeks). [35]
Early administration of DMARDs improves patients' outcomes.
Treat-to-target strategy [30][35]
Long-term treatment is guided by disease activity scoring systems for RA involving clinical and laboratory features, e.g., CDAI. The 2021 ACR guideline does not provide definitions for different stages of disease activity.
- Target at 3 months: ≥ 50% improvement in the disease activity index
- Target at 6 months: low disease activity (or remission)
- Targets not reached: Consult rheumatology to adjust treatment.
A treat-to-target strategy can prevent RA-related disability. [7][30][35]
Do not discontinue all DMARDs in patients who achieve disease remission, as this may trigger a disease flare. [35]
Disease-modifying antirheumatic drugs (DMARDs) [25][30][35]
DMARDs are used as long-term therapy; . They interfere with the inflammatory mechanisms of RA, which can potentially lead to remission. DMARD therapy reduces RA mortality and morbidity by up to 30%. Prevention and monitoring of potential adverse effects are required (see also “Adverse effects” in “Immunosuppressants”). [12]
Synthetic DMARDs
| Synthetic DMARDs for RA [7][30][35] | ||
|---|---|---|
| Drug class | Agent | Important considerations |
| Conventional DMARDs |
|
|
|
|
|
|
|
|
|
|
|
| Targeted DMARDs (JAK inhibitors) |
|
|
Methotrexate monotherapy is strongly recommended over all other synthetic and biologic DMARDs in patients with moderate to high disease activity. [35]
Biologic DMARDs [30]
- Indication: : persistent moderate or severe disease activity after 3 months of conventional DMARD therapy
-
Agents
- TNF-α inhibitors: e.g., adalimumab , infliximab , etanercept (see also “Contraindications to anti-TNF-α treatment”)
- Others: rituximab, anakinra, tocilizumab
-
Adverse effects include:
- Infections
- TB reactivation
- Hepatitis B reactivation
All biologic DMARDs have similar efficacy when combined with MTX. When choosing a biologic DMARD, consider patient preferences, comorbidities, potential adverse effects, and drug availability. [7]
Prevention and monitoring of adverse effects [25][35][37][38]
Perform studies and vaccinations before the initiation of therapy based on the patient's individual risk and potential adverse effects of the prospective agent.
- CBC, liver transaminases, and serum creatinine at baseline
- HCV and HBV serology at baseline
- TB screening (see “Diagnosis of latent TB”): Perform baseline screening in patients who will receive biologic DMARDs or tofacitinib.
-
Vaccinations for patients receiving biologic DMARDs
- Influenza, pneumococcus, and hepatitis B
- Herpes zoster
- Offer contraception counseling, family planning, and information on teratogenicity of pharmacological treatment to all patients. See also “RA in pregnancy.”
Nonpharmacological management [25]
- ASCVD prevention measures are associated with improved outcomes in patients with RA.
- Physical and occupational therapy can improve mobility.
- Heat or cold packs for pain management.
Surgical treatment [25][39]
-
Indications
- Consider in patients with extensive joint deformity.
- Rarely, surgery may be used for symptom control in patients who do not respond to or cannot tolerate the recommended pharmacological regimen.
-
Procedures
- Total joint replacement (e.g., hip joint replacement): Consider in patients with severe joint damage or concomitant osteoarthritis.
- Synovectomy: surgical removal of the synovial tissue
-
Radiation synovectomy: ablation of inflamed synovia via injection of radioactive agents (beta particles) into the synovial cavity of affected joints [40]
- Inhibits synovial growth and fibrosis of the synovia
- May reduce inflammatory activity and pain
- Also indicated in patients with other chronic inflammatory joint diseases (e.g., active arthrosis, psoriatic arthritis) who do not respond to pharmacological treatment
Classification
The ACR/EULAR classification criteria were developed for research purposes and should not be used as diagnostic criteria. These criteria are for targeted use in patients who have at least one joint with clinical synovitis that is not better explained by another cause, e.g. trauma or degenerative joint conditions. [24]
| 2010 ACR/EULAR criteria for the classification of RA [24] | ||||
|---|---|---|---|---|
| Score | Joint involvement (pain or swelling) | Serology | Acute-phase reactants | Symptom duration |
| 0 | ≤ 1 large joint | Negative RF and ACPA | Normal CRP and ESR | < 6 weeks |
| 1 | 2–10 large joints | – | ↑ CRP or ESR | ≥ 6 weeks |
| 2 | 1–3 small joints (with or without large joint involvement) | Low positive RF or ACPA | – | – |
| 3 | 4–10 small joints (with or without large joint involvement) | High positive RF or ACPA | – | – |
| 5 | > 10 joints (including at least one small joint) | – | – | – |
Score: Obtained by adding together the points from each feature Interpretation:
| ||||
The ACR/EULAR classification criteria have high specificity but low sensitivity. Therefore, the purpose of these criteria is to standardize case definitions for enrollment in clinical studies, not to guide practice. [7][24][41]
Complications
Untreated and/or severe cases can result in permanent damage to the joints with stiffening and deformity.
- Complications in the upper limbs: rheumatoid hand deformities (see “Clinical features” above)
-
Complications in the lower limbs
- Baker cyst due to inflammatory joint effusion
- Foot impairment: pes plano‑valgus (flat feet) [42]
-
Other complications
- Muscle weakness
- Vasculitis involving the kidneys
- Amyloid A amyloidosis (AA amyloidosis)
- Septic arthritis [43]
- Osteopenia, osteoporosis, and bone fractures [44]
- Caplan syndrome
 cyst")
We list the most important complications. The selection is not exhaustive.

Dorsomedial view of the knee with swelling in the popliteal fossa indicating popliteal cyst (arrow).
Source: © IMPP
Prognosis
-
Factors associated with poor prognosis
- Cardiovascular disease and infections are the most common causes of death. [12]
- Male sex [45]
- Smoking
- Social factors (e.g., low socioeconomic status, low level of education)
- Presence of extraarticular disease
-
Elevated laboratory values associated with poor prognosis
- CRP
- ESR
- ACPA
- RF
Special patient groups
Rheumatoid arthritis in pregnancy [46][47]
-
General principles
- Pharmacological treatment for patients desiring pregnancy should be adjusted to avoid teratogenicity.
- Advise patients with moderate to high disease activity against pregnancy until they reach disease remission or low activity. See “RA activity assessment.”
- Consider LactMed® and other trusted databases to provide information for patients (see “Tips and Links”).
-
Pharmacological treatment
- Preferred agents: acetaminophen, NSAIDs, glucocorticoids, sulfasalazine
- Alternative agents: TNF-α inhibitors, azathioprine [47]
- Contraindicated agents: methotrexate, leflunomide
- See also “Pharmacological treatment during pregnancy.”
-
Disease course [46]
- Pain decreases in ∼ 60% of patients during pregnancy, and some patients experience remission even in the absence of DMARD therapy.
- Flares may increase in the postpartum period.
Discontinue methotrexate ≥ 3 months before patients attempt conception. [46][47]
Management of RA in patients planning pregnancy involves a multidisciplinary team of specialists (e.g., an obstetrician specializing in high-risk pregnancies, and a rheumatologist).
External Resources
- 2021 American College of Rheumatology Guideline for the Treatment of Rheumatoid Arthritis
- 2019 ACOG Committee Opinion: Immune Modulating Therapies in Pregnancy and Lactation
- 2010 Rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative
- NIH Drugs and Lactation Database (LactMed®)
References
- Cross M, Smith E, et al. "The global burden of rheumatoid arthritis: estimates from the global burden of disease 2010 study". Ann Rheum Dis. 73(7). :1316-22. (2014)
- Hunter TM, Boytsov NN et al. "Prevalence of rheumatoid arthritis in the United States adult population in healthcare claims databases, 2004-2014". Rheumatol Int. 37(9). :1551-1557. (2017)
- Cojocaru M, Cojocaru IM, Silosi I, Vrabie CD, Tanasescu R. "Extra-articular Manifestations in Rheumatoid Arthritis". Maedica (Buchar). (2010)
- Cai Y, Zhang J, Liang J, et al. "The Burden of Rheumatoid Arthritis: Findings from the 2019 Global Burden of Diseases Study and Forecasts for 2030 by Bayesian Age-Period-Cohort Analysis". J Clin Med. 12(4). :1291. (2023)
- Aletaha D, Neogi T, Silman AJ, et al. "2010 Rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative". Arthritis Rheum. 62(9). :2569–2581. (2010)
- Sparks JA. "Rheumatoid Arthritis". Ann Intern Med. 170(1). :ITC1. (2019)
- Aggarwal R, Ringold S, Khanna D, et al. "Distinctions between diagnostic and classification criteria?". Arthritis Care Res (Hoboken). 67(7). :891-7. (2015)
- Smolen JS, Aletaha D, Barton A, et al. "Rheumatoid arthritis". Nature Reviews Disease Primers. 4(1). (2018)
- "Rheumatoid Arthritis Fact Sheet". https://web.archive.org/web/20170421132821/https://www.cdc.gov/arthritis/basics/rheumatoid-arthritis.html. [2017-03-13]
- Kasper DL, Fauci AS, Hauser S, et al. "Harrisons Principles of Internal Medicine ". McGraw-Hill Medical Publishing Division. 19. (2016). ISBN: 9780071802154
- "Hitchhiker thumb deformity". https://radiopaedia.org/articles/hitchhiker-thumb-deformity. [2017-04-10]
- Young A, Koduri G. "Extra-articular manifestations and complications of rheumatoid arthritis". Best Pract Res Clin Rheumatol. 21(5). :907-927. (2007)
- Kim DS. "Interstitial lung disease in rheumatoid arthritis: recent advances". Curr Opin Pulm Med. 12(5). :346-353. (2006)
- Jabs DA, Mudun A, Dunn JP, Marsh MJ. "Episcleritis and scleritis: clinical features and treatment results". Am J Ophthalmol. 130(4). :469-476. (2000)
- Rawla P. "Cardiac and vascular complications in rheumatoid arthritis". Reumatologia/Rheumatology. 57(1). :27-36. (2019)
- Kasper DL, Fauci AS, Hauser SL, et al. "Harrison's Principles of Internal Medicine". McGraw-Hill Education. (2015). ISBN: 9780071802161
- Wegscheider C, Ferincz V, Schöls K, Maieron A. "Felty’s syndrome". Front Med. 10. (2023)
- West SG. "Rheumatology Secrets". Elsevier Mosby. (2014). ISBN: 9780323037006
- Krabben A, Huizinga TWJ, van der Helm-van Mil AHM. "Undifferentiated arthritis characteristics and outcomes when applying the 2010 and 1987 criteria for rheumatoid arthritis". Ann Rheum Dis. 71(2). :238-241. (2011)
- Van der Helm-vanMil AHM, le Cessie S, van Dongen H, et al. "A prediction rule for disease outcome in patients with Recent-onset undifferentiated arthritis: How to guide individual treatment decisions". Arthritis Rheum. 56(2). :433-440. (2007)
- Song YW, Kang EH. "Autoantibodies in rheumatoid arthritis: rheumatoid factors and anticitrullinated protein antibodies". QJM. 103(3). :139-146. (2009)
- Aggarwal R, Liao K, Nair R, Ringold S, Costenbander KH. "Anti-citrullinated peptide antibody assays and their role in the diagnosis of rheumatoid arthritis". Arthritis Care & Research. 61(11). :1472-1483. (2009)
- Slater CA. "Antinuclear Antibody Testing". Arch Intern Med. 156(13). :1421. (1996)
- Jacobson JA, Roberts CC, Bencardino JT, et al. "ACR Appropriateness Criteria ® Chronic Extremity Joint Pain—Suspected Inflammatory Arthritis". J Am Coll Radiol. 14(5). :S81-S89. (2017)
- Aletaha D, Smolen JS. "Diagnosis and Management of Rheumatoid Arthritis". JAMA. 320(13). :1360. (2018)
- Jeka S, Zuchowski P, Dura M, Zwierko B, Waszczak-Jeka M. "The role of ultrasonography in the diagnostic criteria for rheumatoid arthritis and monitoring its therapeutic efficacy". Advances in Clinical and Experimental Medicine. 27(9). :1303-1307. (2018)
- Bresnihan B. "Are synovial biopsies of diagnostic value?". Arthritis Res Ther. 5(6). :271. (2003)
- Sanmartí R, Frade-Sosa B, Morlà R, et al. "Palindromic Rheumatism: Just a Pre-rheumatoid Stage or Something Else?". Front Med. 8. (2021)
- Fraenkel L, Bathon JM, England BR, et al. "2021 American College of Rheumatology Guideline for the Treatment of Rheumatoid Arthritis". Arthritis Care & Research. (2021)
- Bykerk VP, Bingham CO, Choy EH, et al. "Identifying flares in rheumatoid arthritis: reliability and construct validation of the OMERACT RA Flare Core Domain Set". RMD Open. 2(1). :e000225. (2016)
- Singh JA, Saag KG, Bridges SL, et al. "2015 American College of Rheumatology Guideline for the Treatment of Rheumatoid Arthritis". Arthritis Care & Research. 68(1). :1-25. (2015)
- Saag KG, Teng GG, Patkar NM, et al. "American College of Rheumatology 2008 recommendations for the use of nonbiologic and biologic disease-modifying antirheumatic drugs in rheumatoid arthritis". Arthritis & Rheumatism. 59(6). :762-784. (2008)
- Massardo L, Gabriel SE, Crowson CS, O'Fallon WM, Matteson EL. "A population based assessment of the use of orthopedic surgery in patients with rheumatoid arthritis.". J Rheumatol. 29(1). :52-6. (2002)
- Chojnowski MM, Felis-Giemza A, Kobylecka M. "Radionuclide synovectomy – essentials for rheumatologists". Reumatologia. 3. :108-116. (2016)
- Turner DE, Helliwell PS, Emery P, Woodburn J. "The impact of rheumatoid arthritis on foot function in the early stages of disease: a clinical case series". BMC Musculoskelet Disord. 7. :102. (2006)
- "Septic Arthritis". http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement/rheumatology/septic-arthritis/. [2010-08-01]
- Haugeberg G, Ørstavik RE, Kvien TK. "Effects of Rheumatoid Arthritis on Bone". Curr Opin Rheumatol. 15(4). :469-475. (2003)
- Myasoedova E, Davis JM, Crowson CS, Gabriel SE. "Epidemiology of Rheumatoid Arthritis: Rheumatoid Arthritis and Mortality". Curr Rheumatol Rep. 12(5). :379-385. (2010)
- Walther J van Venrooij, Ger J M Pruijn. "Citrullination: a small change for a protein with great consequences for rheumatoid arthritis". Arthritis Res. 2(4). :249. (2000)
- Scott DL, Wolfe F, Huizinga TW. "Rheumatoid arthritis". The Lancet. 376(9746). :1094-1108. (2010)
- van Zeben D, Hazes JM et al. "Clinical significance of rheumatoid factors in early rheumatoid arthritis: results of a follow up study". Ann Rheum Dis. 51(9). :1029-35. (1992)
- Wasserman AM. "Diagnosis and Management of Rheumatoid Arthritis". Am Fam Physician. 84(11). :1245-1252. (2011)
- Alvarez I, Collado J, Daura X, et al. "The rheumatoid arthritis-associated allele HLA-DR10 (DRB1*1001) shares part of its repertoire with HLA-DR1 (DRB1*0101) and HLA-DR4 (DRB*0401)". Arthritis Rheum. 58(6). :1630-1639. (2008)
- England BR, Tiong BK et al. "2019 Update of the American College of Rheumatology Recommended Rheumatoid Arthritis Disease Activity Measures". Arthritis Care Res. 71(12). :1540-1555. (2019)
- Felson DT, Smolen JS, Wells G, et al. "American College of Rheumatology/European League Against Rheumatism provisional definition of remission in rheumatoid arthritis for clinical trials". Arthritis & Rheumatism. 63(3). :573-586. (2011)
- Makol A, Krause M. "Management of rheumatoid arthritis during pregnancy: challenges and solutions". Open Access Rheumatol. :23. (2016)
- American College of Obstetricians and Gynecologists. "ACOG Committee Opinion No. 776: Immune Modulating Therapies in Pregnancy and Lactation". Obstet Gynecol. 133(4). :e287-e295. (2019)
- Whiting PF. "Systematic Review: Accuracy of Anti–Citrullinated Peptide Antibodies for Diagnosing Rheumatoid Arthritis". Ann Intern Med. 152(7). :456. (2010)
- Agha-Abbaslou M, Bensaci AM, Dike O, Poznansky MC, Hyat A. "Adult-Onset Still’s Disease: Still a Serious Health Problem (a Case Report and Literature Review)". American Journal of Case Reports. 18. :119-124. (2017)
- Steinbrocker et al. "Therapeutic criteria in rheumatoid arthritis". JAMA: The Journal of the American Medical Association. 140(8). :659. (1949)