Summary
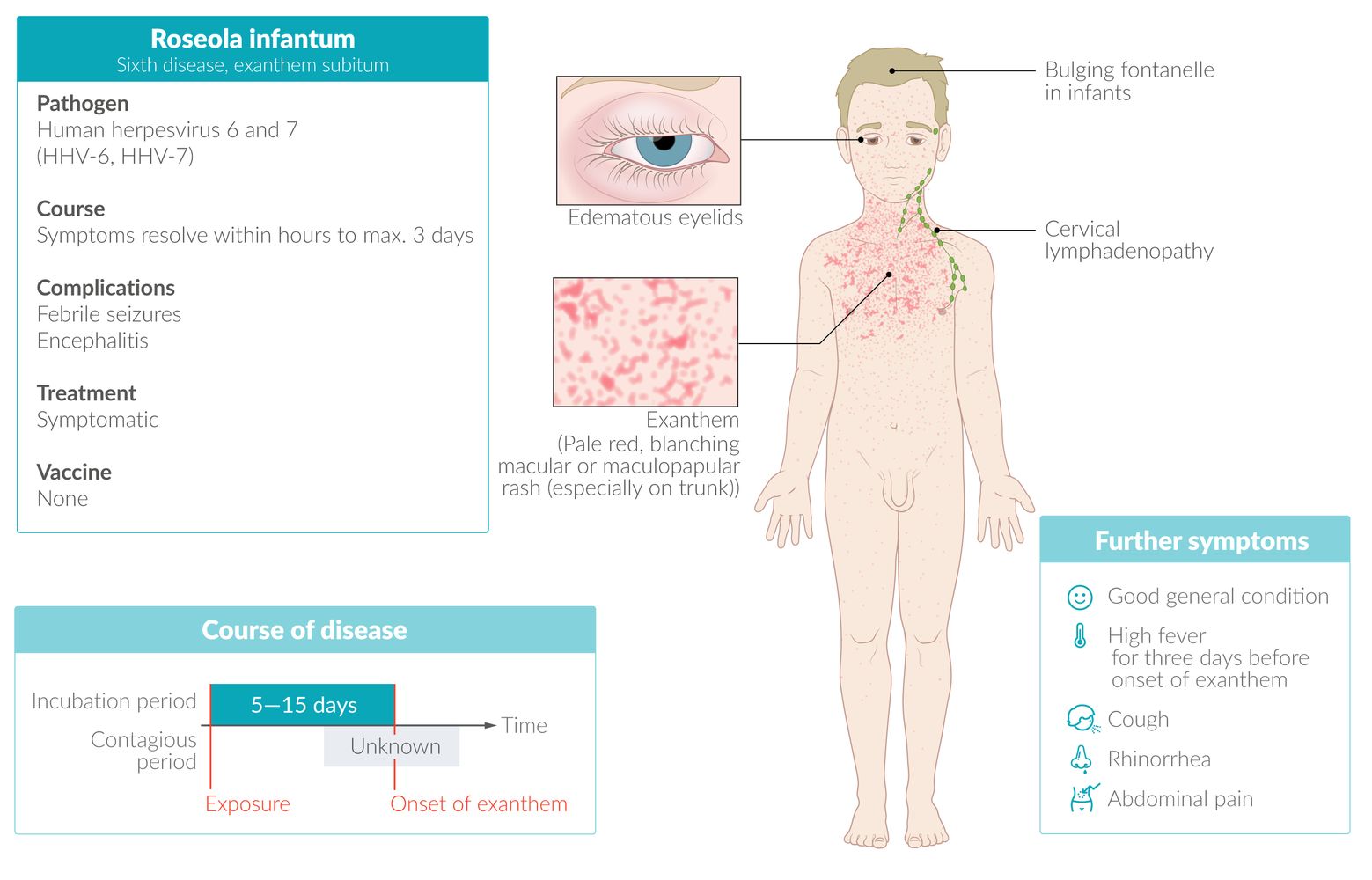
Roseola infantum is an infectious disease most commonly caused by human herpesvirus 6 (HHV-6). It occurs most frequently in children between 6 months and 2 years of age. Roseola infantum is characterized by abrupt onset and resolution of high fever lasting approx. three days, followed by the sudden manifestation of a patchy, nonpruritic rash with macules and papules that starts on the trunk and sometimes spreads to the face and extremities. Roseola infantum is diagnosed clinically; laboratory tests are not typically recommended. The course is self-limited, but symptomatic treatment may be considered. Febrile seizures are the most common complication of infection.
Epidemiology
- Most frequent in infants and young children [1]
- Peak incidence: 6 months to 2 years [1]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
-
Pathogen
- HHV-6 (and in rare cases HHV-7)
- Humans are the sole hosts.
- Route of transmission: droplet infection (e.g., saliva)
- Incubation period: 5–15 days
References:[2][3]
Clinical features
Children with roseola infantum usually appear well. Rarely, children present with complications of roseola infantum (e.g., encephalitis). [1][4][5]
Prodrome [1][5]
-
Fever
- Abrupt onset of high fever, in some patients > 39.5°C
- Lasts ∼ 3 days (up to 7 days)
- Febrile seizures are a potential complication of roseola infantum.
- Cervical and/or occipital lymphadenopathy
- Inflamed tympanic membranes
- Nagayama spots: papular enanthem on the uvula and soft palate [6]
- Cough
- Rhinorrhea
- Fussiness and irritability [6]
- Gastrointestinal symptoms (e.g., diarrhea)
- Edematous eyelids and conjunctivitis [6][7]
More than 75% of HHV-6 infections do not cause roseola infantum; the most common manifestations of HHV-6 infection are fever and rhinorrhea. [1]
Exanthem phase [1][5]
- Rash typically manifests after sudden resolution of fever
- Lasts 1–2 days [6]
-
Patchy macular and papular exanthem that:
- Is rose-pink in color
- Blanches upon pressure
- Is nonpruritic (in contrast to drug rash)
- Originates on the trunk and sometimes spreads to the face and extremities
")
 fact sheet")
The alternative names for roseola infantum, “three-day fever” and “exanthem subitum” (from Latin: “subitus” = sudden), reflect the two phases of the disease: three days of high fever followed by a sudden rash. [6]

Photograph of a 1-year-old child with recent febrile illness
A patchy, nonpruritic, blanching, erythematous rash with macules and papules can be seen on the trunk and arms. Symptoms manifested one day after the fever resolved.
These features are consistent with roseola infantum.
Source: "Sestamalattia", Emiliano Burzagli, Wikimedia Commons licensed under Public Domain
{kind=link}
© AMBOSS
Diagnosis
- Usually a clinical diagnosis [1][5]
- Consult infectious diseases for consideration of confirmatory studies (e.g., serology, NAAT) in patients with: [1][6]
- Severe complications
- Immunocompromise
Laboratory studies are not required but (if performed) may show leukopenia, thrombocytopenia, and elevated transaminases. [6]
Differential diagnoses
- Other infectious rashes in childhood
- Drug-induced skin reaction
- Bacterial meningitis


The differential diagnoses listed here are not exhaustive.
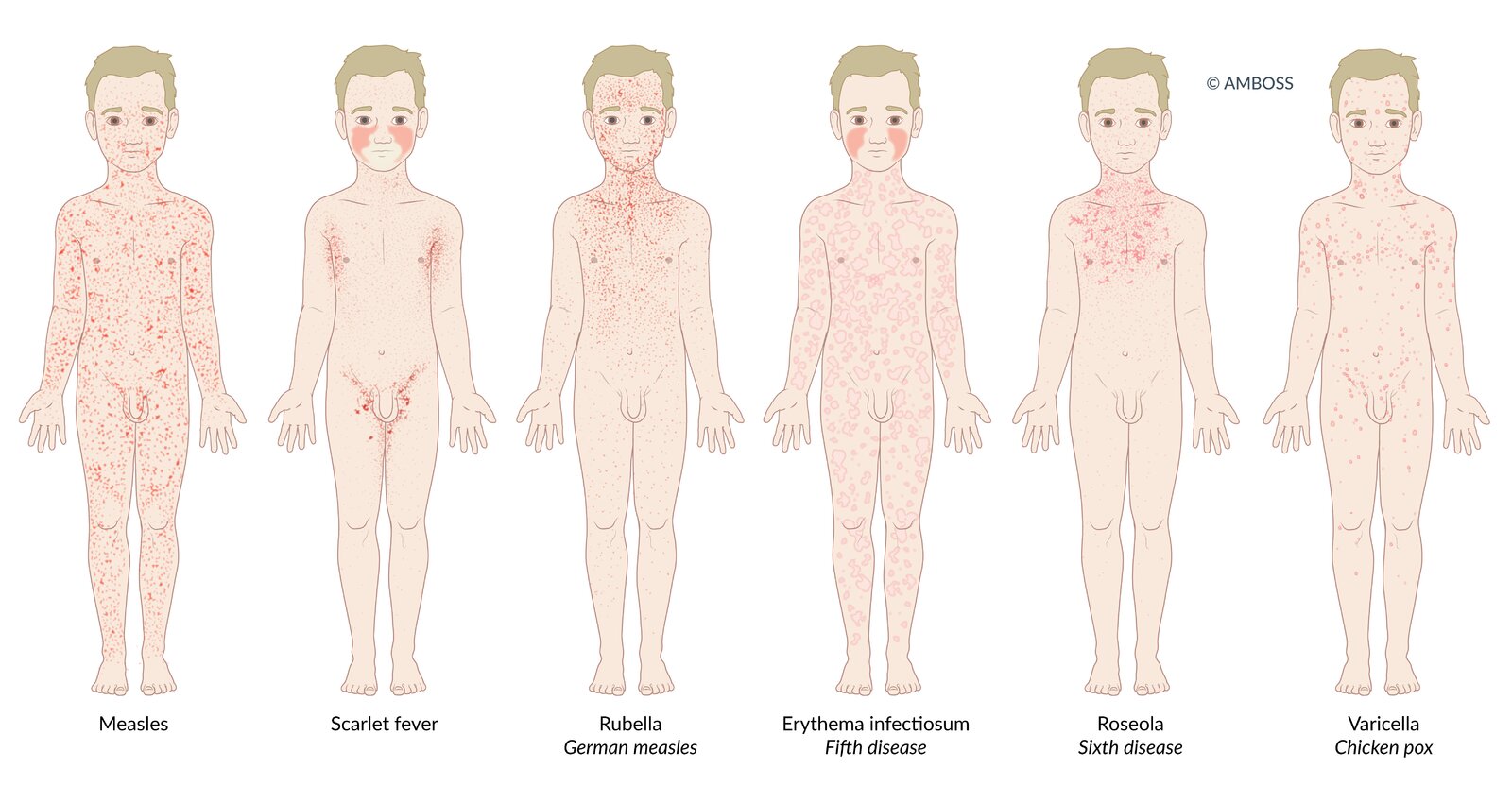
Many infectious diseases in children present with a rash (exanthem). The distribution and morphological characteristics of the exanthem allow the diseases to be differentiated from one another.
Measles: Patients present with a dark red, erythematous, maculopapular, partially confluent exanthem, which spreads from behind the ears to the rest of the body.
Scarlet fever: Patients present with a fine, light red rash with sandpaper-like texture. The exanthem begins on the neck or trunk and disseminates to the whole body. Cheeks may be flushed with perioral pallor. In flexural areas (e.g., axilla and groin), the rash may be more pronounced and linear petechiae (Pastia lines) may be present.
Rubella (German measles): Patients typically present with a nonconfluent, pink, maculopapular exanthem, which begins on the face and spreads to the trunk and extremities.
Erythema infectiosum (fifth disease): A confluent, maculopapular rash appears only in ¼ of patients. It may take on a lace-like, reticular appearance over time. Additionally, patients present with diffuse redness of the face with perioral sparing (slapped-cheek rash).
Roseola infantum (sixth disease): 3-7 days of high fever are followed by a sudden decrease in temperature and development of a patchy, blanching rose-pink maculopapular rash. The rash originates on the trunk, and may spread to the face and extremities.
Varicella (chickenpox): The exanthem affects the whole body, typically spreading to the scalp as well. Various stages of the rash occur simultaneously, which leads to the characteristic clinical finding known as “starry sky.”
© AMBOSS

© AMBOSS
Treatment
Roseola infantum is typically a self-limited illness that can be managed with symptomatic treatment as needed. [1][5]
- Consider supportive care for pediatric fever (e.g., acetaminophen)
- Manage associated complications of roseola infantum (e.g., treatment of febrile seizures).
- Immunocompromised patients: Consult infectious diseases for consideration of antiviral therapy. [1]
- No infection control measures are required for the exanthem of roseola infantum. [1]


© AMBOSS
Complications
- Febrile seizures (in up to 15% of cases), usually without sequelae [8]
- Hepatitis
- Meningoencephalitis (very rare)
We list the most important complications. The selection is not exhaustive.
Prognosis
- Very good prognosis; self-limiting disease
- The virus persists lifelong in its host, and reactivation of latent virus or reinfection may occur later in life (especially if individuals become immunocompromised)
References
- Committee on Infectious Disease, American Academy of Pediatrics. "Red Book: 2024-2027 Report of the Committee on Infectious Diseases, 33rd Edition". American Academy of Pediatrics. (2024). ISBN: 9781610027373
- Marcdante K, Kliegman RM. "Nelson Essentials of Pediatrics E-Book". Elsevier Health Sciences. (2018). ISBN: 9780323528061
- Kessler HH. "Molecular Diagnostics of Infectious Diseases". Walter de Gruyter GmbH & Co KG. (2014). ISBN: 9783110373479
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904
- Allmon A, Deane K, Martin KL. "Common Skin Rashes in Children". Am Fam Physician. 92(3). :211-6. (2015)
- Stone RC, Micali GA, Schwartz RA. "Roseola infantum and its causal human herpesviruses". Int J Dermatol. 53(4). :397-403. (2014)
- Tesini BL, Epstein LG, Caserta MT. "Clinical impact of primary infection with roseoloviruses". Curr Opin Virol. 9. :91-96. (2014)
- Leung AKC, Lam JMC, Barankin B, Leong KF, Hon KL. "Roseola Infantum: An Updated Review". Curr Pediatr Rev. 20(2). :119-128. (2024)