Summary
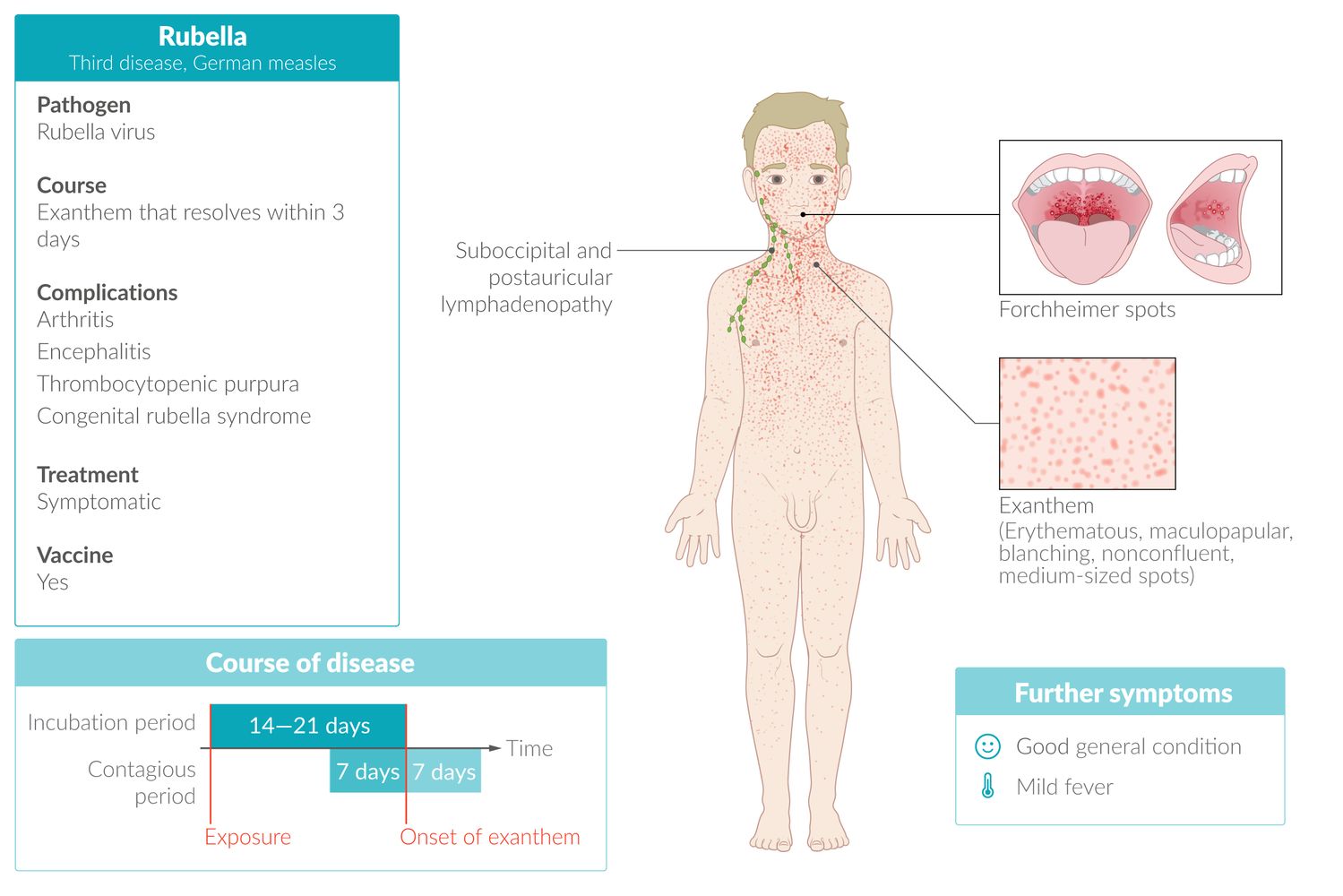
Rubella (German measles) is an infectious disease caused by the rubella virus and transmitted via airborne droplets or transplacentally (see “Congenital rubella syndrome”). Since the introduction of the measles, mumps, and rubella (MMR) vaccine, rubella is relatively rare. The clinical course is mild, characterized by an erythematous maculopapular rash that typically starts on the face and progresses distally. The rash may be preceded by nonspecific flu-like symptoms and postauricular and/or suboccipital lymphadenopathy. The combination of RT-PCR and serology for rubella-specific IgM antibodies is preferred to confirm active disease. Treatment is supportive and isolation is recommended. Immunization with the MMR vaccine or MMRV vaccine is recommended for all children and adults without evidence of immunity.
This article pertains to rubella acquired postnatally; congenital rubella syndrome is addressed separately.
Epidemiology
- A rare disease in the US following the implementation of the MMR vaccine
- Risk factors: See “Risk factors for measles, mumps, and/or rubella.”
Epidemiological data refers to the US, unless otherwise specified.
Etiology
-
Pathogen
- Rubella virus, an RNA virus of the family Matonaviridae
- Prior to 2019, the rubella virus was classified as the sole member of the Rubivirus genus in the Togaviridae family. [1]
- Humans are the only hosts.
-
Route of transmission
- Respiratory droplets or transplacental
- Infectivity: 7 days prior to and 7 days following the appearance of an exanthem
- Low infectivity and virulence
- Incubation period: 2–3 weeks after infection
Clinical features
Patients with rubella infection are asymptomatic in ∼ 50% of cases. Young children have a far milder course than older children and adults; the latter group often presents with prodromal symptoms, other systemic complaints (e.g., arthritis), and a longer duration of infection.
Prodromal phase
- Duration: 1–5 days
-
Findings
- Post-auricular and suboccipital lymphadenopathy and occasionally splenomegaly
- Mild and nonspecific symptoms such as low-grade fever; , mild sore throat, cough, conjunctivitis, headache, and aching joints
- Forchheimer sign: enanthem of the soft palate
Exanthem phase
- Duration: lasts 2–3 days
-
Findings
-
Fine, nonconfluent, pink maculopapular rash
- Begins on the face and extends to the trunk and extremities, sparing palms and soles
- Rash may be itchy in adults
- Polyarthritis
-
Fine, nonconfluent, pink maculopapular rash



© AMBOSS

A nonconfluent, pink, maculopapular rash is visible across this infant's trunk and extremities.
Source: "ID#: 4513", CDC, Centers for Disease Control and Prevention (CDC) licensed under Public Domain

© AMBOSS
Management
Clinical features of rubella are typically nonspecific; ; consider acute infection in an unvaccinated patient with a febrile rash.
Infection control [2][3][4]
- Isolate patient and institute standard precautions and droplet precautions.
- Ensure that only health care professionals with evidence of rubella immunity provide direct care to the patient.
- Notify the local health department immediately of a suspected case.
Rubella is a nationally notifiable disease in the US; immediately report all suspected and confirmed cases to the local health department.
Diagnostics for rubella [2][3][4]
Obtain and interpret diagnostic studies in all patients in coordination with the health department.
Studies
- All patients: serology for rubella-specific IgM and IgG antibodies
- Patients presenting ≤ 7 days (ideally ≤ 3 days) after rash onset: [4]
- RT-PCR of a nasopharyngeal or throat swab
- If presenting close to day 7 after rash onset, also consider RT-PCR of a urine sample. [4]
Interpretation of results
-
Confirmatory results include any of the following:
- Positive RT-PCR or viral culture [4]
- Positive IgM antibodies [4]
- A 4-fold increase in IgG antibodies seen on two serum samples taken ∼ 2 weeks apart, starting from the onset of symptoms [4]
-
Results that cannot rule out acute infection include:
- A single negative IgM test within the first 5 days of rash onset (in this case, repeat IgM test) [5]
- A single negative IgG test
RT-PCR with serology for rubella-specific IgM antibodies is preferred to confirm acute rubella infection. RT-PCR should be collected as soon as possible and within 7 days of rash onset. [2][3]
Further management [6]
-
Supportive therapy, e.g.:
- Fever: supportive care for pediatric fever
- Severe pruritus: antihistamines
- Severe polyarthritis: rest and NSAIDs
- For treatment of congenital rubella syndrome and seronegative women following exposure to rubella virus, see “Congenital rubella syndrome.”
- Instruct patients and exposed contacts on isolation precautions; see “Exposure control for rubella.”


© AMBOSS
Differential diagnoses
- Differential diagnoses of pediatric rashes

The differential diagnoses listed here are not exhaustive.
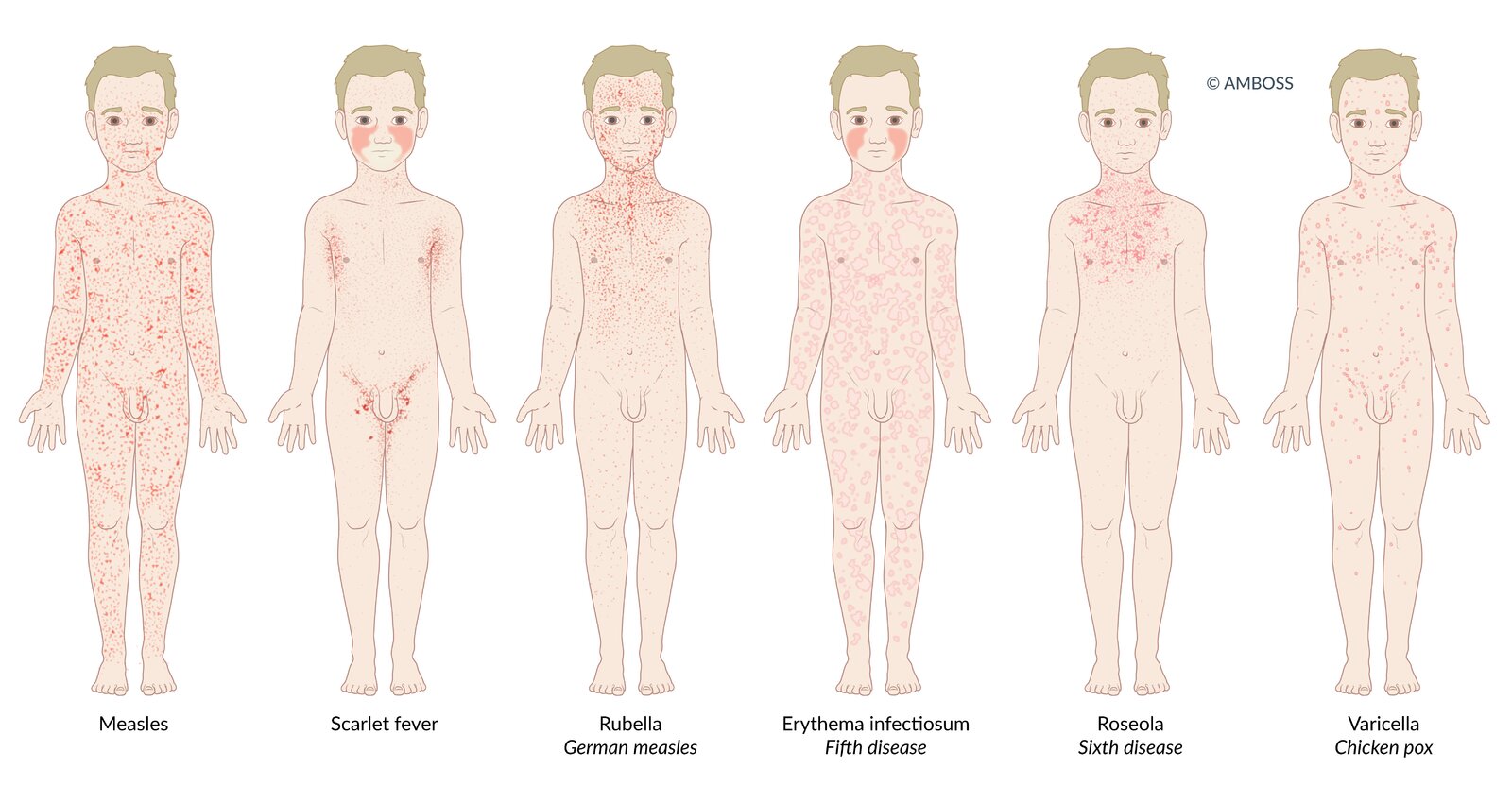
Many infectious diseases in children present with a rash (exanthem). The distribution and morphological characteristics of the exanthem allow the diseases to be differentiated from one another.
Measles: Patients present with a dark red, erythematous, maculopapular, partially confluent exanthem, which spreads from behind the ears to the rest of the body.
Scarlet fever: Patients present with a fine, light red rash with sandpaper-like texture. The exanthem begins on the neck or trunk and disseminates to the whole body. Cheeks may be flushed with perioral pallor. In flexural areas (e.g., axilla and groin), the rash may be more pronounced and linear petechiae (Pastia lines) may be present.
Rubella (German measles): Patients typically present with a nonconfluent, pink, maculopapular exanthem, which begins on the face and spreads to the trunk and extremities.
Erythema infectiosum (fifth disease): A confluent, maculopapular rash appears only in ¼ of patients. It may take on a lace-like, reticular appearance over time. Additionally, patients present with diffuse redness of the face with perioral sparing (slapped-cheek rash).
Roseola infantum (sixth disease): 3-7 days of high fever are followed by a sudden decrease in temperature and development of a patchy, blanching rose-pink maculopapular rash. The rash originates on the trunk, and may spread to the face and extremities.
Varicella (chickenpox): The exanthem affects the whole body, typically spreading to the scalp as well. Various stages of the rash occur simultaneously, which leads to the characteristic clinical finding known as “starry sky.”
© AMBOSS
Complications
- Chronic arthritis (especially women)
- Thrombocytopenic purpura
- Rubella during pregnancy (TORCH infection): congenital rubella syndrome
- Rare: rubella encephalitis, bronchitis, otitis, myocarditis, pericarditis
We list the most important complications. The selection is not exhaustive.
Prognosis
- The disease usually has a benign course and the exanthem disappears rapidly.
- Joint pain may persist for several weeks; arthralgia may persist up to a month in adults.
Prevention
Vaccination [7][8][9]
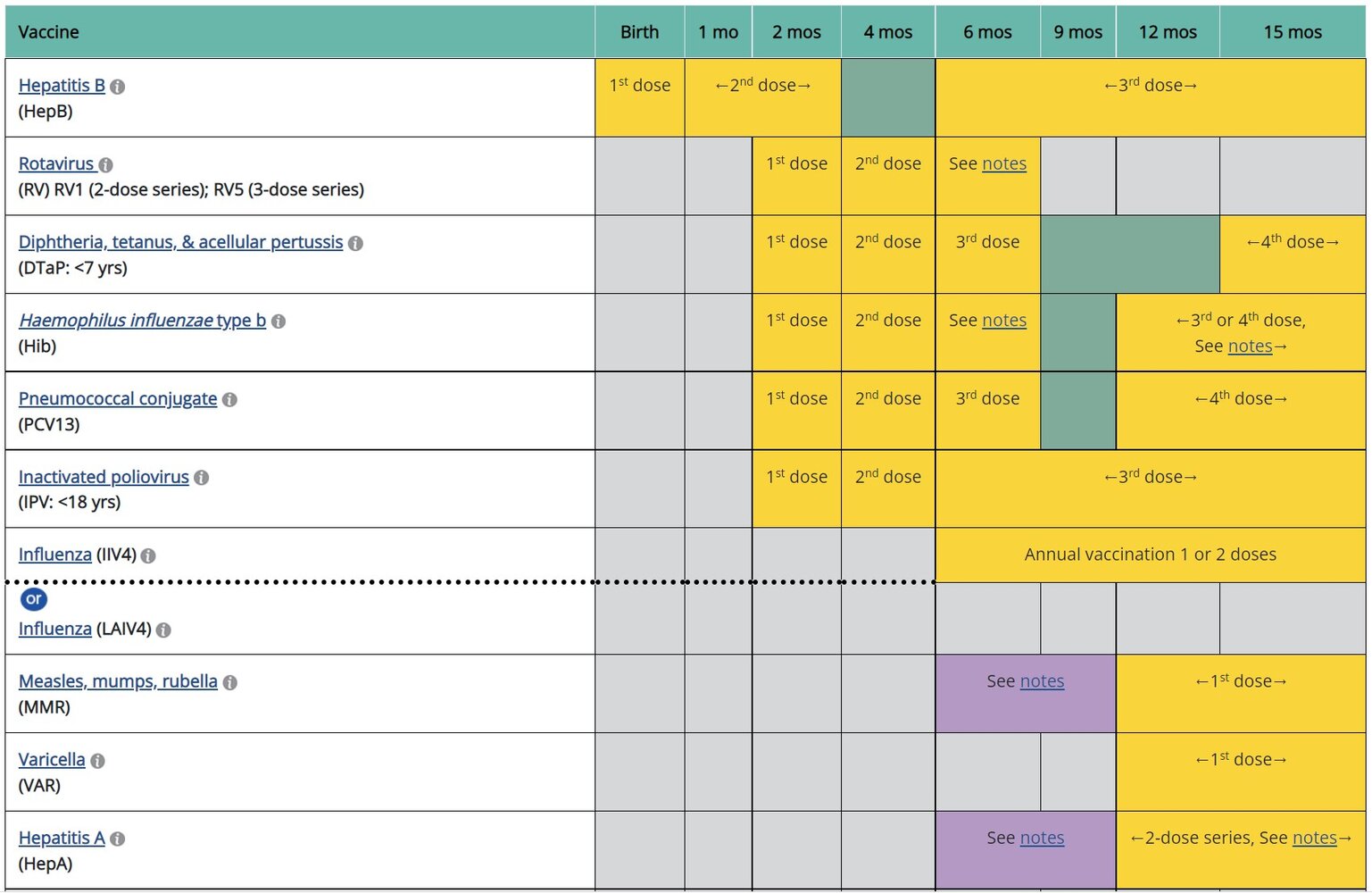
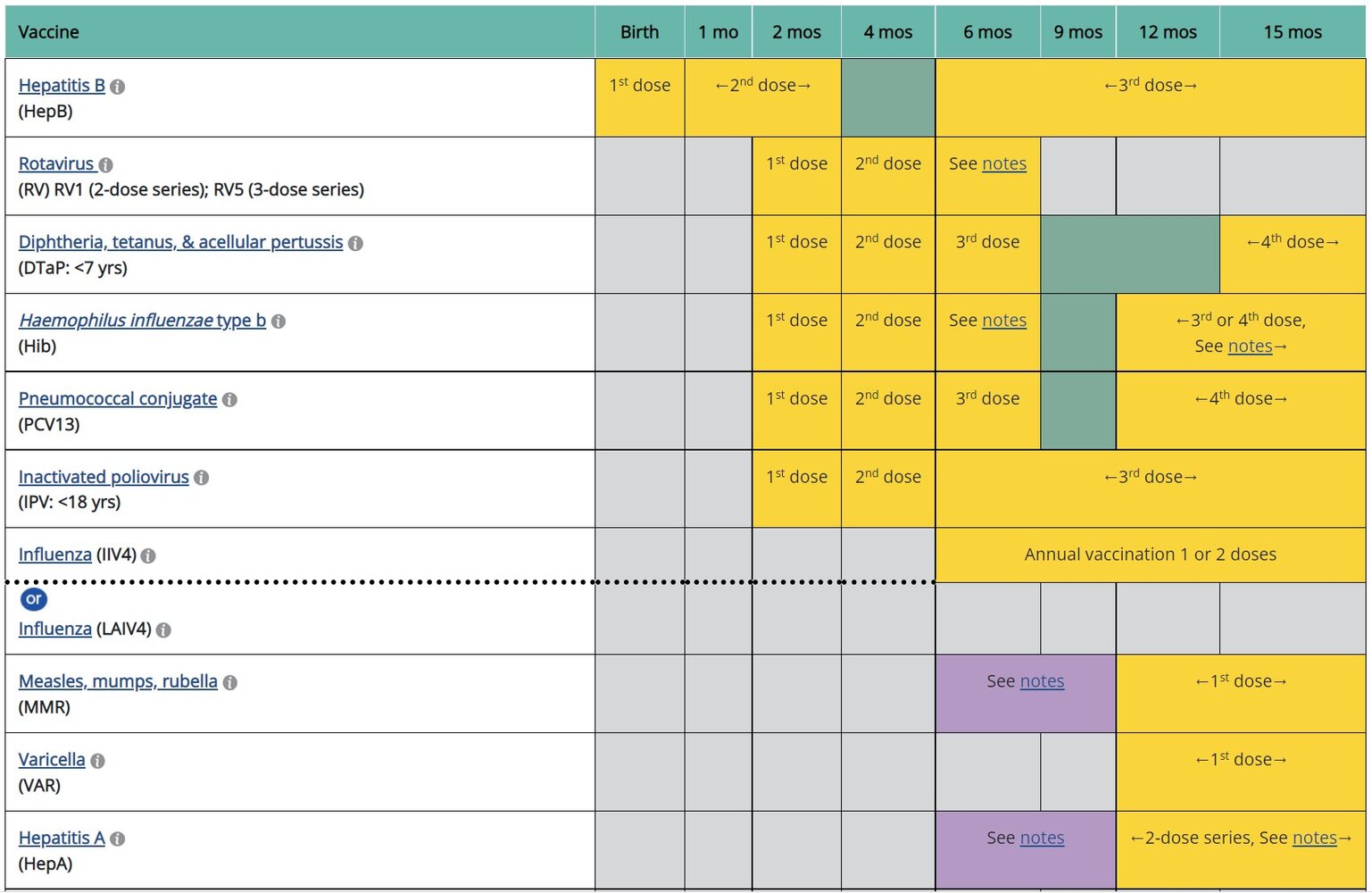
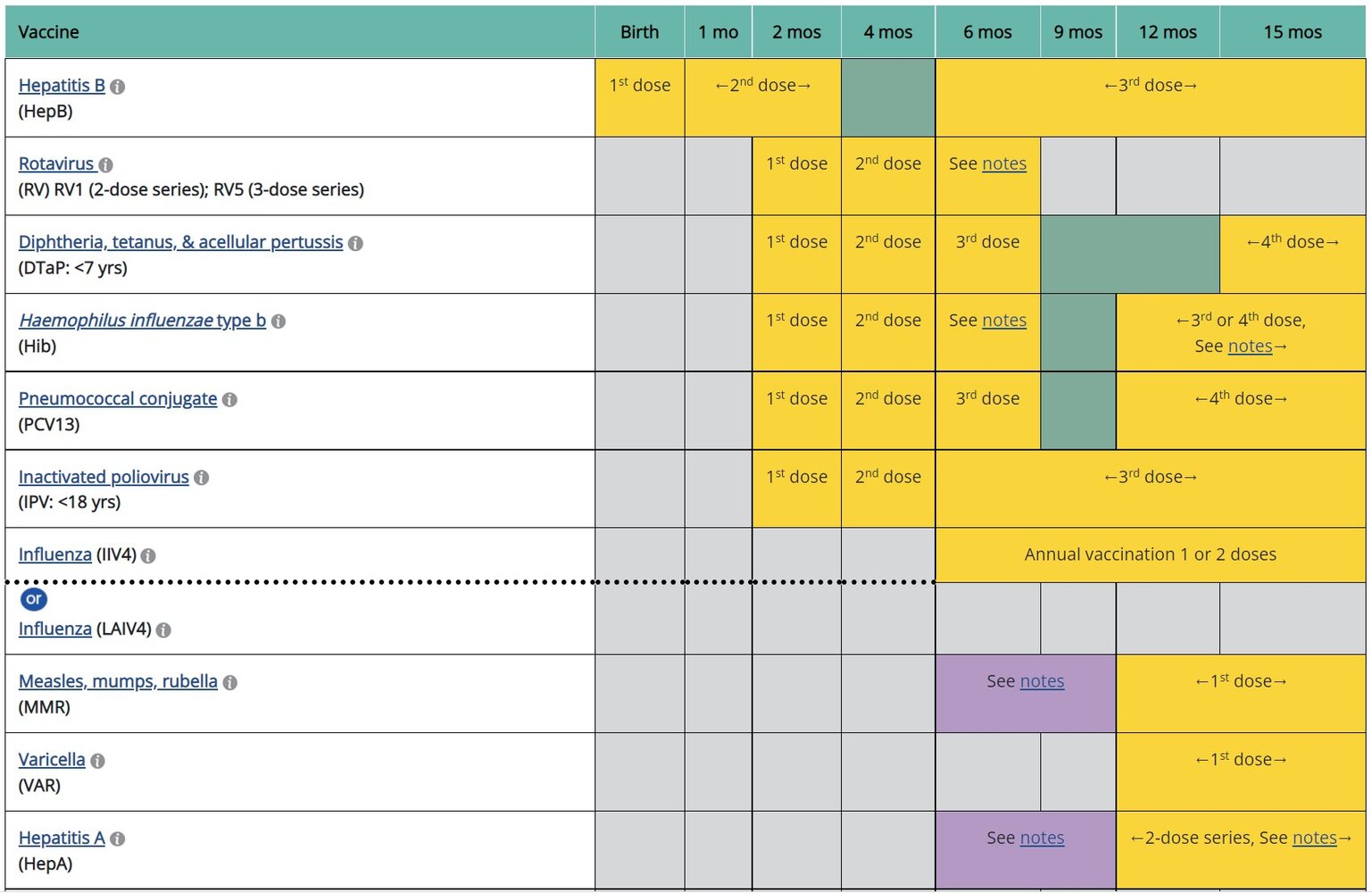
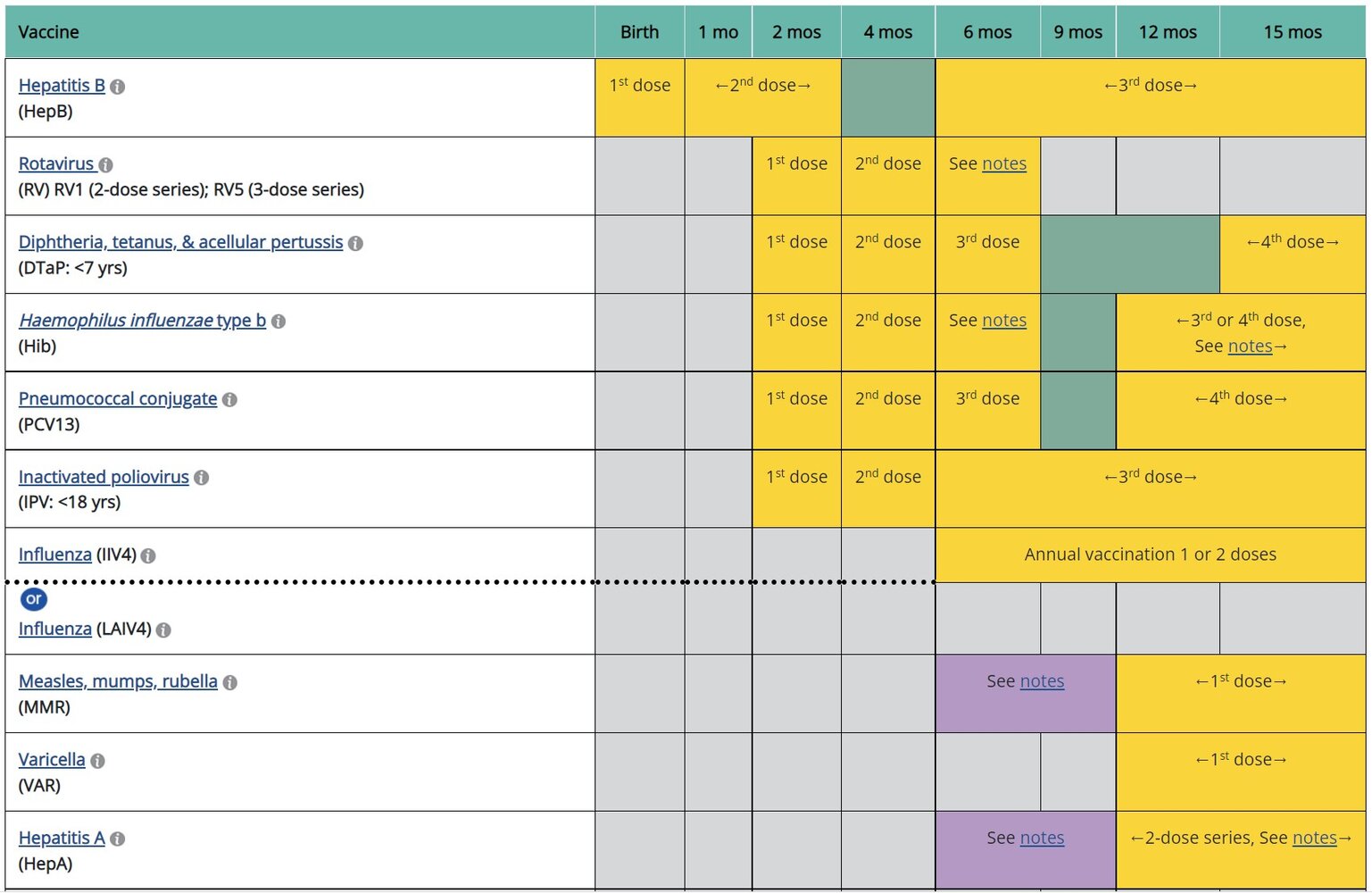
Administer a live attenuated rubella vaccine; (i.e., MMR vaccine, MMRV vaccine) according to the ACIP immunization schedule. See the following:
- Immunizations for measles, mumps, and rubella
- ACIP immunization schedule
- Contraindications to live vaccines (e.g., pregnancy, immunocompromise)

Evidence of immunity to rubella [5][10]
- See “Indications to test for immunity to rubella” and “Evidence of immunity to measles, mumps, and/or rubella.”
- If laboratory evidence of immunity to rubella is required, perform serologic testing. [5][10]
- IgG measurement by enzyme immunoassay is preferred.
- A rubella IgG titer > 10 IU/mL indicates immunity to rubella. [5]
Women of reproductive age without evidence of immunity to rubella should be vaccinated prior to pregnancy to prevent congenital rubella syndrome. [11]
Exposure control for rubella [12]
-
Suspected and confirmed rubella
- Hospitalized patients: Initiate standard precautions and droplet precautions.
- Isolate for 7 days from rash onset to prevent further transmission. [12]
- Exposed contacts without evidence of immunity to rubella
- Women of reproductive age: Obtain pregancy test.
- Pregnant individuals: Promptly obtain serology for rubella-specific IgM and IgG antibodies; follow up with health department.
- Individuals without contraindications to live vaccines: Offer MMR vaccine to protect from future exposures. [3][13]
- Isolation
- Health care workers: Exclude from work from day 7 after first exposure until day 23 after last exposure. [12]
- Others: Refer to health department guidance.
Further notes: Materials developed and hosted by the CDC and available free of charge on the CDC website. Reference to specific commercial products, manufacturers, companies, or trademarks does not constitute its endorsement or recommendation by the U.S. Government, Department of Health and Human Services, or Centers for Disease Control and Prevention.
Further notes: Materials developed and hosted by the CDC and available free of charge on the CDC website. Reference to specific commercial products, manufacturers, companies, or trademarks does not constitute its endorsement or recommendation by the U.S. Government, Department of Health and Human Services, or Centers for Disease Control and Prevention.
Further notes: Materials developed and hosted by the CDC and available free of charge on the CDC website. Reference to specific commercial products, manufacturers, companies, or trademarks does not constitute its endorsement or recommendation by the U.S. Government, Department of Health and Human Services, or Centers for Disease Control and Prevention.
Further notes: Materials developed and hosted by the CDC and available free of charge on the CDC website. Reference to specific commercial products, manufacturers, companies, or trademarks does not constitute its endorsement or recommendation by the U.S. Government, Department of Health and Human Services, or Centers for Disease Control and Prevention.
External Resources
References
- Walker PJ, Siddell SG, Lefkowitz EJ, et al. "Changes to virus taxonomy and the International Code of Virus Classification and Nomenclature ratified by the International Committee on Taxonomy of Viruses (2019)". Arch Virol. 164(9). :2417-2429. (2019)
- "Adult Immunization Schedule by Age Recommendations for Ages 19 Years or Older, United States, 2023". https://web.archive.org/web/20230324184103/https://www.cdc.gov/vaccines/schedules/hcp/imz/adult.html. [2023-02-10]
- "CDC Adult Immunization Schedule by Medical Condition and Other Indication". https://web.archive.org/web/20220616182014/http://www.cdc.gov:80/vaccines/schedules/hcp/imz/adult-conditions.html
- "Child and Adolescent Immunization Schedule. Recommendations for Ages 18 Years or Younger, United States, 2023". https://web.archive.org/web/20230324163634/https://www.cdc.gov/vaccines/schedules/hcp/imz/child-adolescent.html. [2023-02-10]
- "Serology Testing for Rubella and Congenital Rubella Syndrome (CRS)". https://web.archive.org/web/20230503193331/https://www.cdc.gov/rubella/lab/serology.html. [2023-04-12]
- Isaac BM, Zucker JR, Giancotti FR, et al. "Rubella Surveillance and Diagnostic Testing among a Low-Prevalence Population, New York City, 2012–2013". Clin Vaccine Immunol. 24(9). (2017)
- "Chapter 15: Congenital Rubella Syndrome". https://web.archive.org/web/20230505185254/https://www.cdc.gov/vaccines/pubs/surv-manual/chpt15-crs.html. [2020-04-28]
- "Manual for the Surveillance of Vaccine-Preventable Diseases". https://web.archive.org/web/20240511050346/https://www.cdc.gov/vaccines/pubs/surv-manual/chpt14-rubella.html. [2020-03-06]
- Committee on Infectious Disease, American Academy of Pediatrics. "Red Book: 2024-2027 Report of the Committee on Infectious Diseases, 33rd Edition". American Academy of Pediatrics. (2024). ISBN: 9781610027373
- "Prevention of Measles, Rubella, Congenital Rubella Syndrome, and Mumps, 2013: Summary Recommendations of the Advisory Committee on Immunization Practices (ACIP)". https://web.archive.org/web/20241226075912/https://www.cdc.gov/mmwr/preview/mmwrhtml/rr6204a1.htm. [2013-06-14]
- "CDC Pink Book: Rubella". https://web.archive.org/web/20240419182714/https://www.cdc.gov/vaccines/pubs/pinkbook/rubella.html. [2021-08-01]
- "Recommendations for Measles, Mumps, Rubella, and Varicella Testing for Clinicians". https://web.archive.org/web/20240419195612/https://www.cdc.gov/chickenpox/downloads/MMRV-Testing-for-Clinicians.pdf. [2020-12-31]
- "CDC Yellow Book: Rubella". https://web.archive.org/web/20240419183021/https://wwwnc.cdc.gov/travel/yellowbook/2024/infections-diseases/rubella. [2023-04-04]