Summary
The scaphoid bone is the most commonly fractured carpal bone. Fractures are most often localized in the middle third of the scaphoid bone. Generally, scaphoid bone fractures result when an individual falls onto the outstretched hand with a hyperextended and radially deviated wrist. Pain when applying pressure to the anatomical snuffbox is highly suggestive of a scaphoid bone fracture. X-ray is the initial test of choice for diagnosis. CT and MRI may be indicated if x-ray findings are negative but clinical suspicion is high. All suspected scaphoid fractures should be immobilized in a thumb spica cast. Definitive treatment can be nonoperative (i.e., wrist immobilization) or surgical (e.g., for proximal pole fractures). Complications include nonunion and avascular necrosis.
Epidemiology
- Most common carpal bone fracture (50–80%) [1]
- Peak incidence: 15–19 years [2]
Epidemiological data refers to the US, unless otherwise specified.
Classification
- According to the localization of the fracture [3]
- Proximal third (proximal pole): ∼ 10%
- Middle third (waist): ∼ 70%
-
Distal third (distal pole): ∼ 20%
- Distal articular surface
- Distal tubercle
Clinical features
- History of falling onto the outstretched hand; with a hyperextended and radially deviated wrist [4]
- Pain when applying pressure to the anatomical snuffbox and scaphoid tubercle (a palpable bony prominence on the inferior lateral edge of the scaphoid bone)
- Minimal reduction in the range of motion (except in dislocated fractures)
- Decreased grip strength
- Painful pinching and grasping
- Pain can be induced through axial compression along the first metacarpal (scaphoid compression test). [4]


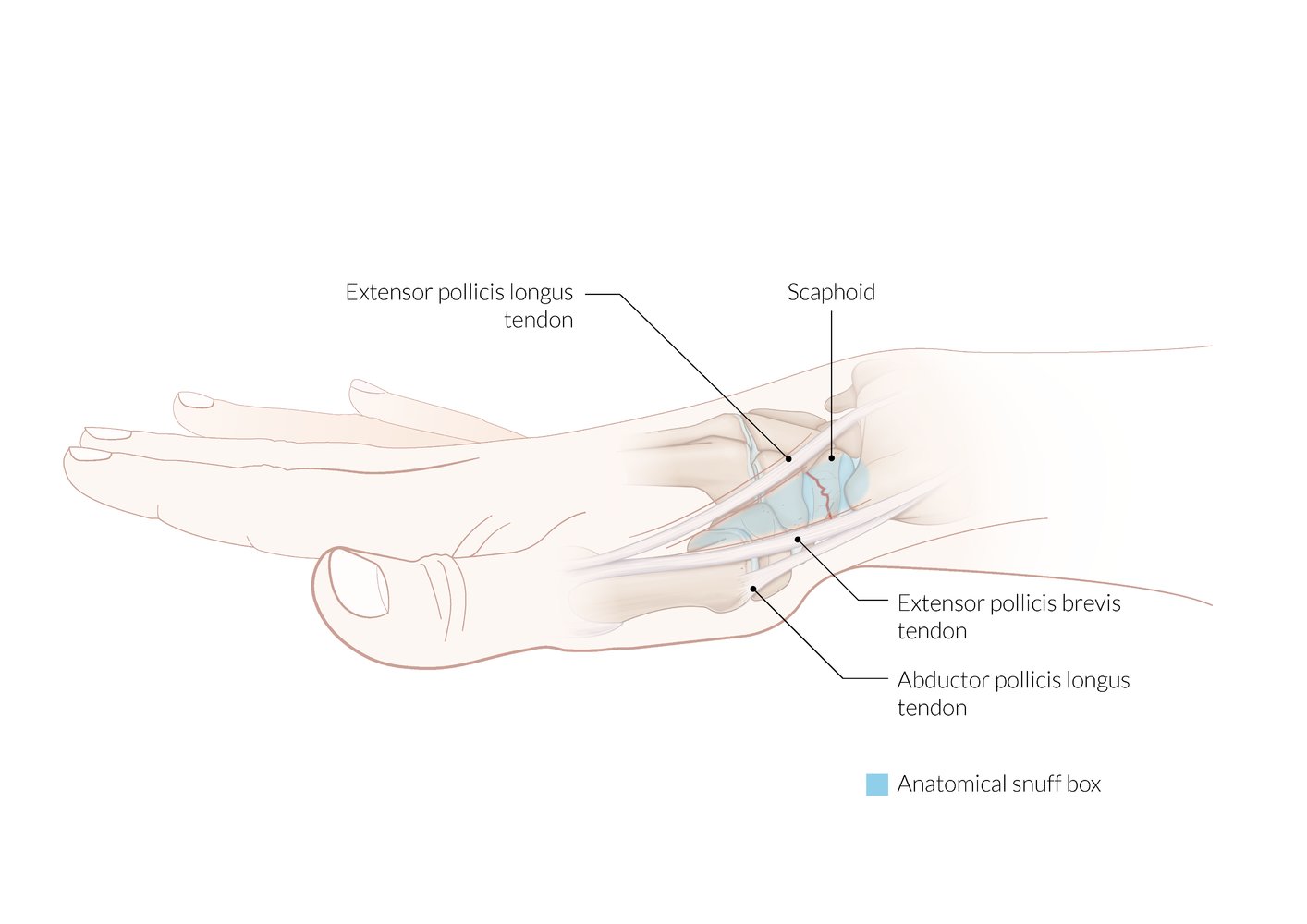
A triangular depression over the dorsal aspect of the base of the thumb that becomes prominent when the thumb is extended or abducted.
Boundaries: tendon of the extensor pollicis longus (on the ulnar side) and the tendons of the extensor pollicis brevis and the abductor pollicis longus (radial side)
The scaphoid bone lies in the floor of the anatomical snuff box. Tenderness on application of pressure to the anatomical snuffbox is a clinical sign of a scaphoid fracture.
© AMBOSS
© AMBOSS
Diagnosis
X-ray is the best initial test; advanced imaging is only indicated in selected cases. [5]
X-ray [5][6][7]
- Indication: suspected scaphoid fracture
- Views: posteroanterior, lateral, oblique, and scaphoid views
-
Findings
- Radiographic signs of fractures
- Displacement, bowing, or obliteration of the scaphoid fat pad
Consider advanced imaging if initial x-rays are negative for fractures, as 15–20% of scaphoid fractures are undetectable on the initial x-ray. [6]



Advanced imaging [5][6]
-
Indications
- Suspected occult fracture [8]
- Suspected associated tendon or ligament injury
- Preoperative planning for complicated injuries
-
Modalities [9]
- Standard modalities: MRI, CT
- Additional modalities include bone scintigraphy and ultrasound. [5][6][7]

X-ray hand (PA view)
A nondisplaced fracture (red line) is visible through the waist of the scaphoid bone of the wrist.
© AMBOSS

X-ray of the hand (dorsopalmar view): proximal scaphoid fracture (green line = bone and fracture line)
Source: © IMPP

Radiograph of the right hand: scaphoid fracture (arrow) following a fall on the outstretched hand.
(1 = scaphoid; 2 = lunate; 3 = triquetrum; 4 = pisiform; 5 = trapezium; 6 = trapezoid, 7 = capitate; 8 = hamate; I–V = metacarpals; R = radius; U = ulna)
Source: © IMPP
Differential diagnoses
Carpal ligament injuries
- Scapholunate dissociation
- Perilunate dislocation
- Lunate dislocation
Distal radius fractures
- Colles fracture
- Smith fracture
- Barton fracture
- Reverse Barton fracture
- Hutchinson fracture
- Die-punch fracture
Hand fractures
- Metacarpal fractures (e.g., boxer's fracture)
- Phalangeal fractures
The differential diagnoses listed here are not exhaustive.
Treatment
Approach [7]
-
All suspected scaphoid fractures
- Provide analgesia for acute fractures.
- Immobilize in a thumb spica cast or splint.
- Arrange orthopedic follow-up within one week.
- Confirmed fractures: nonoperative or surgical management (depending on stability)
- Suspected occult fractures: immobilization with x-ray reevaluation after 10–14 days or advanced imaging [5]
When pain occurs in the anatomical snuffbox after trauma, the injury should be treated as a suspected scaphoid fracture until proven otherwise.
Nonoperative management [6]
-
Indications: Consider for all stable fractures.
- Nondisplaced or minimally displaced fractures (< 1 mm)
- Distal pole fractures
- Fractures with normal intercarpal alignment
- Technique: immobilization in a short- or long-arm thumb spica cast for at least 6–8 weeks [6]
Surgical management [6]
-
Indications
- General indications for surgical fracture management, e.g., open fractures, neurovascular compromise
- Displaced fractures (> 1 mm)
- Proximal pole fractures [6]
- Carpal instability
- Radiographic signs of instability, e.g., bone loss
- Older fractures (> 4 weeks)
- Technique: percutaneous or open reduction and internal fixation
Complications
- Avascular necrosis (especially in proximal fractures that disrupt blood flow from branches of the radial artery) of the scaphoid bone in up to 50% of cases [10]
- Nonunion (especially in proximal fractures) in approx. 10% [11]
- Delayed union of fracture (more common in smokers)
- Instability among carpal joints
- Post-traumatic arthritis
Fractures in the distal third tend to heal better because of the retrograde blood supply reaching the bone from the distal pole.


We list the most important complications. The selection is not exhaustive.

Radiograph of the left hand: scaphoid fracture with pseudarthrosis (arrow). The patient fell onto the outstretched left hand.
(1 = scaphoid; 2 = lunate; 3 =triquetrum; 4 = pisiforme; 5 = trapezium/ trapezoid; 6 = Os capitatum; 7 = hamate; 8 = Hamulus of hamate; I - V = metacarpals; R = radius; U = ulna)
Source: © IMPP
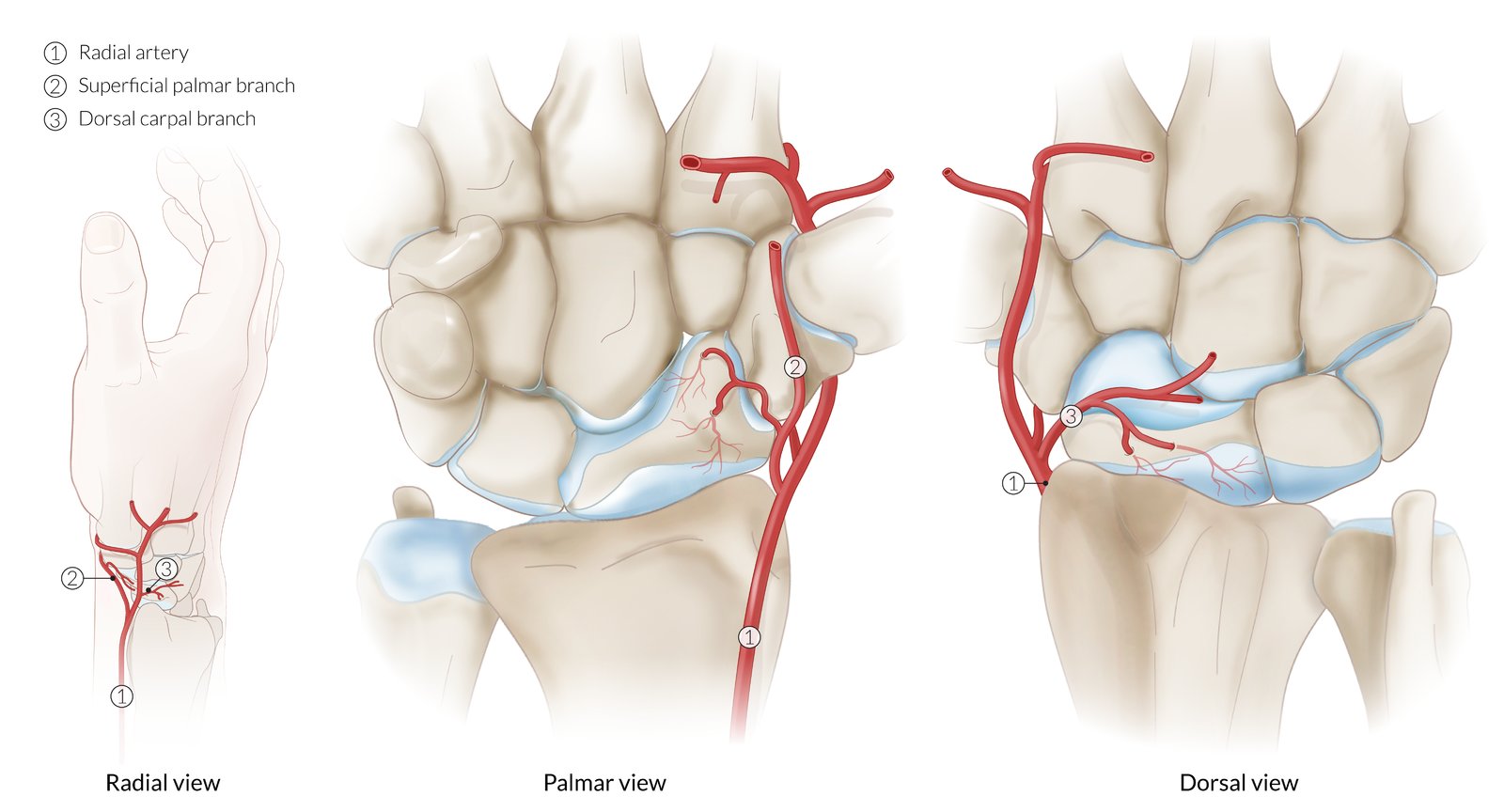
The scaphoid is supplied primarily by branches of the radial artery. As illustrated here, the superficial palmar branch penetrates the bone from the palmar side and the dorsal carpal branch from the dorsal side, both at the distal pole. There may, however, be significant variation, both in which radial branches are the principal contributors and in their branching patterns.
Because the arterial blood supply of the scaphoid flows from the distal pole to the proximal pole, more proximal scaphoid fractures are at higher risk of nonunion and avascular necrosis.
© AMBOSS
References
- Alshryda S, Shah A, Odak S, et al. "Acute fractures of the scaphoid bone: Systematic review and meta-analysis". The Surgeon. 10(4). :218-229. (2012)
- Garala K, Taub NA, Dias JJ. "The epidemiology of fractures of the scaphoid". The Bone & Joint Journal. 98-B(5). :654-659. (2016)
- Rhemrev SJ, Ootes D, Beeres FJ, Meylaerts SA, Schipper IB. "Current methods of diagnosis and treatment of scaphoid fractures". International Journal of Emergency Medicine. 4(1). (2011)
- Phillips TG, Reibach AM, Slomiany WP. "Diagnosis and management of scaphoid fractures". Am Fam Physician. 70(5). :879-84. (2004)
- Torabi M, Lenchik L, Beaman FD, et al. "ACR Appropriateness Criteria® Acute Hand and Wrist Trauma". J Am Coll Radiol. 16(5). :S7-S17. (2019)
- Li NY, Dennison DG, Shin AY, Pulos NA. "Update to Management of Acute Scaphoid Fractures". J Am Acad Orthop Surg. 31(15). :e550-e560. (2023)
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904
- Rua T, Malhotra B, Vijayanathan S, et al. "Clinical and cost implications of using immediate MRI in the management of patients with a suspected scaphoid fracture and negative radiographs results from the SMaRT trial". Bone Joint J. 101-B(8). :984-994. (2019)
- Mallee WH, Wang J, Poolman RW, et al. "Computed tomography versus magnetic resonance imaging versus bone scintigraphy for clinically suspected scaphoid fractures in patients with negative plain radiographs". Cochrane Database Syst Rev. 2015(6). (2015)
- Steinmann SP, Adams JE. "Scaphoid fractures and nonunions: diagnosis and treatment". Journal of Orthopaedic Science. 11(4). :424-431. (2006)
- Severo AL, Lemos MB, Lech OLC, et al. "Bone graft in the treatment of nonunion of the scaphoid with necrosis of the proximal pole: a literature review". Revista Brasileira de Ortopedia (English Edition). 52(6). :638-643. (2017)
- "UpToDate". http://www.uptodate.com. [2012-01-01]
- Bhatia M, Sharma A, Ravikumar R, Maurya VK. "Lunate dislocation causing median nerve entrapment.". Medical journal, Armed Forces India. 73(1). :88-90. (2017)
- Wingelaar M, Newbury P, Adams NS, Livingston AJ. "Lunate Dislocation and Basic Wrist Kinematics.". Eplasty. 16. :ic37. (2016)
- Wickramasinghe NR, Duckworth AD, Clement ND, et al. "Acute Median Neuropathy and Carpal Tunnel Release in Perilunate Injuries Can We Predict Who Gets a Median Neuropathy?". Journal of hand and microsurgery. 7(2). :237-40. (2015)
- Scalcione LR, Gimber LH, Ho AM, et al. "Spectrum of Carpal Dislocations and Fracture-Dislocations: Imaging and Management". American Journal of Roentgenology. 203(3). :541-550. (2014)
- Pinho AB, Sobania RL. "Perilunate carpal dislocation. Clinical evaluation of patients operated with reduction and percutaneous fixation without capsular-ligament repair". Revista Brasileira de Ortopedia (English Edition). 52(4). :402-409. (2017)
- Malović M, Pavić R, Milošević M. "Treatment of Trans-Scaphoid Perilunate Dislocations Using a Volar Approach With Scaphoid Osteosynthesis and Temporary Kirschner Wire Fixation". Mil Med. 176(9). :1077-1082. (2011)
- Cowell GW, Ng CY, Tiemessen CH, Phillips JE. "Transscaphoid perilunate dislocation - a tale of two carpals?". Case Reports. 2011(aug24 1). :bcr0720114513-bcr0720114513. (2011)
- Beeres FJP, Rhemrev SJ, den Hollander P, et al. "Early magnetic resonance imaging compared with bone scintigraphy in suspected scaphoid fractures". J Bone Joint Surg Br. 90-B(9). :1205-1209. (2008)
- Gupta V, Rijal L, Jawed A. "Managing scaphoid fractures. How we do it?". Journal of Clinical Orthopaedics and Trauma. 4(1). :3-10. (2013)
- Clementson M, Björkman A, Thomsen NOB. "Acute scaphoid fractures: guidelines for diagnosis and treatment". EFORT Open Reviews. 5(2). :96-103. (2020)