Summary
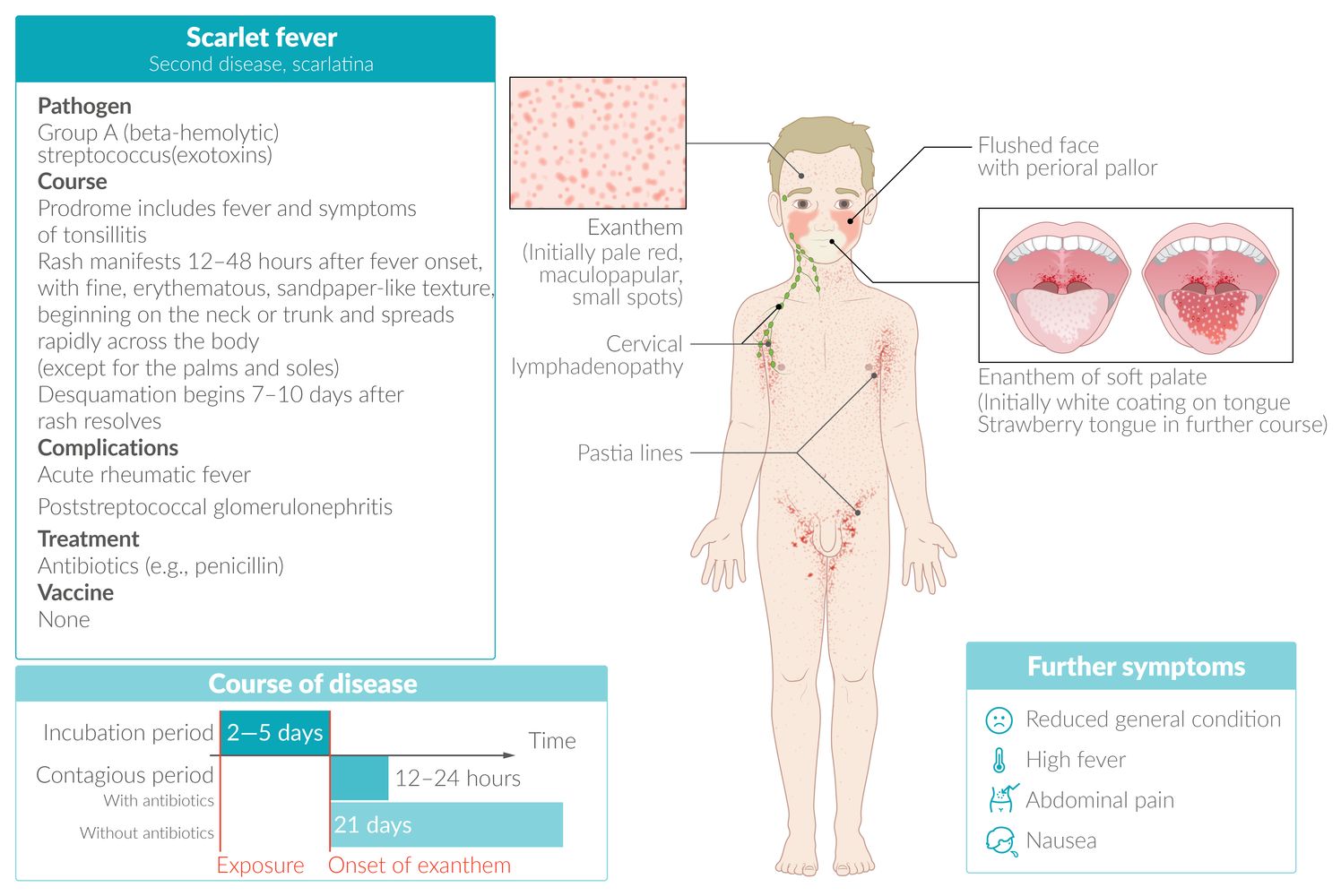
Scarlet fever is an acute syndrome caused by Streptococcus pyogenes, a highly contagious toxin-producing group A Streptococcus (GAS). The syndrome most commonly occurs in children and in less than 10% of patients with streptococcal tonsillopharyngitis. Scarlet fever classically manifests with fever, pharyngeal erythema, flushed cheeks with perioral pallor, strawberry tongue, and an erythematous rash with sandpaper-like texture. Desquamation of the face, trunk, hands, fingers, and toes begins approx. one week after the rash resolves. Antibiotic treatment with penicillin is recommended as scarlet fever may progress to severe disease and lead to complications (e.g., rheumatic fever and poststreptococcal glomerulonephritis). Recurrent infection with other toxins may occur as S. pyogenes produces several types of erythrogenic toxins.

© AMBOSS
Epidemiology
- Peak incidence: 5–15 years (although it may affect individuals of any age) [1]
- Generally occurs in association with streptococcal cases of tonsillopharyngitis
Epidemiological data refers to the US, unless otherwise specified.
Etiology
-
Pathogenic
- Group A Streptococcus (i.e., S. pyogenes) produces erythrogenic exotoxin A, B, and/or C.
- Previous infection does not rule out additional episodes of the disease as there are several different types of scarlet fever toxin.
- Route of transmission: aerosol
- Incubation period: 2–5 days [2]
References:[3]
Clinical features
Prodrome [2]
- Fever
-
Symptoms of tonsillopharyngitis, e.g.:
- Sore throat and difficulty swallowing
- Pharyngeal erythema, possibly with tonsillar exudates
- Enlarged cervical lymph nodes
- Abdominal pain, nausea, and/or vomiting [4]
Rarely, scarlet fever develops after a streptococcal skin and soft tissue infection rather than tonsillopharyngitis. [2]

Exanthem phase [5]
- Rash manifests 12–48 hours after fever onset. [6]
- Fine, erythematous, sandpaper‑like texture
- Blanches with pressure, but nonblanching petechiae may also be present
- Often pruritic
- Begins on neck or trunk and spreads rapidly across the body (except for the palms and soles)
- Characteristic features include:
- Flushed cheeks with perioral pallor
- Strawberry tongue: bright red tongue color with papillary hyperplasia, which may initially be covered with a white coating
-
Pastia lines
- A characteristic sign of scarlet fever
- Linear, petechial appearance
- Most pronounced in the groin, underarm, and elbow creases (i.e., flexural areas)
- Lasts ∼ 7 days [1]
Findings such as coryza, rhinorrhea, cough, hoarseness, anterior stomatitis, conjunctivitis, and ulcerative lesions are atypical for scarlet fever and warrant further investigation.






Desquamation phase [5]
- Desquamation; begins 7–10 days after rash resolves. [7]
- Most affected areas include the face, skin folds, hands, and feet.
- Lasts up to 4–6 weeks [5]


There is tonsillar erythema and edema bilaterally and a petechial enanthem of the soft palate.
Source: "ID#: 3183", CDC/Heinz F. Eichenwald, MD, Centers for Disease Control and Prevention licensed under Public Domain

Upper body of a child showing an elevated, maculopapular, fine exanthem, which is spread evenly over the patient's torso. Combined with characteristic findings such as tonsillopharyngitis, flushed cheeks with perioral pallor, and a strawberry tongue, this finding indicates scarlet fever. The disease is caused by exotoxins produced by group A β‑hemolytic streptococci.
Source: Courtesy of Dr. Gary M. White, MD

Chest and neck of an 8-year-old presenting with fever, confirmed streptococcal tonsillopharyngitis, and strawberry tongue.
An evenly distributed, maculopapular exanthem (papule examples indicated by arrowheads; the rash texture is often described as sandpaper-like) is visible on the trunk.
These findings are consistent with scarlet fever rash.
Source: “Scarlet fever rash” by Whispyhistory, Wikimedia Commons, licensed under CC BY-SA 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 4.0.
{kind=link}

The typical scarlet-colored, fine, maculopapular exanthem of scarlet fever is seen on the right arm. Flushed cheeks and perioral pallor are also evident.
Source: “Scarlet Fever” by Badobadop, Wikimedia Commons, licensed under CC BY-SA 3.0. Modifications: Pixelated eyes.
{kind=link}

Typical red, flushed cheeks with perioral pallor in a child with scarlet fever.
Source: “Scarlet fever” by Alicia Williams (Estreya), Wikimedia Commons, licensed under CC BY-SA 2.5. Modifications: Pixelated eyes.
{kind=link}

Bright red tongue with papillary hyperplasia
Strawberry tongue may be seen in various conditions, e.g., scarlet fever, toxic shock syndrome, Kawasaki disease, and MIS-C.
Source: “Scarlatina tongue” by SyntGrisha, Wikimedia Commons, licensed under CC BY-SA 4.0.
{kind=link}

Enlarged, reddened papillae resembling a strawberry protrude through a white coating of keratinized epithelium.
A white strawberry tongue is commonly seen in patients with scarlet fever, toxic shock syndrome, Kawasaki disease, and MIS-C.
Source: “Skarlatina” by Afag Azizova, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}

Palms showing lamellar desquamation of the skin ("skin glove"). Desquamation typically begins 7–10 days after rash resolves, and lasts up to 4–6 weeks. The face and trunk typically show pityriasiform scales.
Source: "Scharlach", YasminFeth, Wikimedia Commons licensed under Public Domain
{kind=link}
Diagnosis
Scarlet fever can rarely occur after nonpharyngeal infection; for management in those cases, see “Impetigo” and/or “Nonpurulent skin and soft tissue infections.”
Confirmatory tests [1][2]
Scarlet fever has characteristic clinical features, but the diagnosis must be confirmed with one of the following laboratory studies. For acute pharyngitis without the other clinical features of scarlet fever, see “Diagnosis of acute pharyngitis.”
- Throat culture for GAS (gold standard)
-
Rapid antigen detection testing (rapid strep test)
- Positive test: Treat as scarlet fever.
- Negative test
- Adults: No further testing is routinely required.
- Children > 3 years of age: Obtain a throat culture for GAS.
- Children ≤ 3 years of age: Consider obtaining a throat culture for GAS. [1][2][8]
- NAAT from a throat swab [2]
- Delayed presentation with nonsuppurative complications of GAS infection: antistreptolysin O (ASO) and anti-DNase B (ADB) titers [8][9]
Blood tests are not routinely recommended as common findings (e.g., leukocytosis, raised inflammatory markers) are nonspecific. [10]
Differential diagnoses
- Other infectious rashes in childhood
- Drug hypersensitivity reaction
- Chickenpox (varicella)
- Kawasaki disease
- Viral tonsillitis (infectious mononucleosis, herpangina)


The differential diagnoses listed here are not exhaustive.
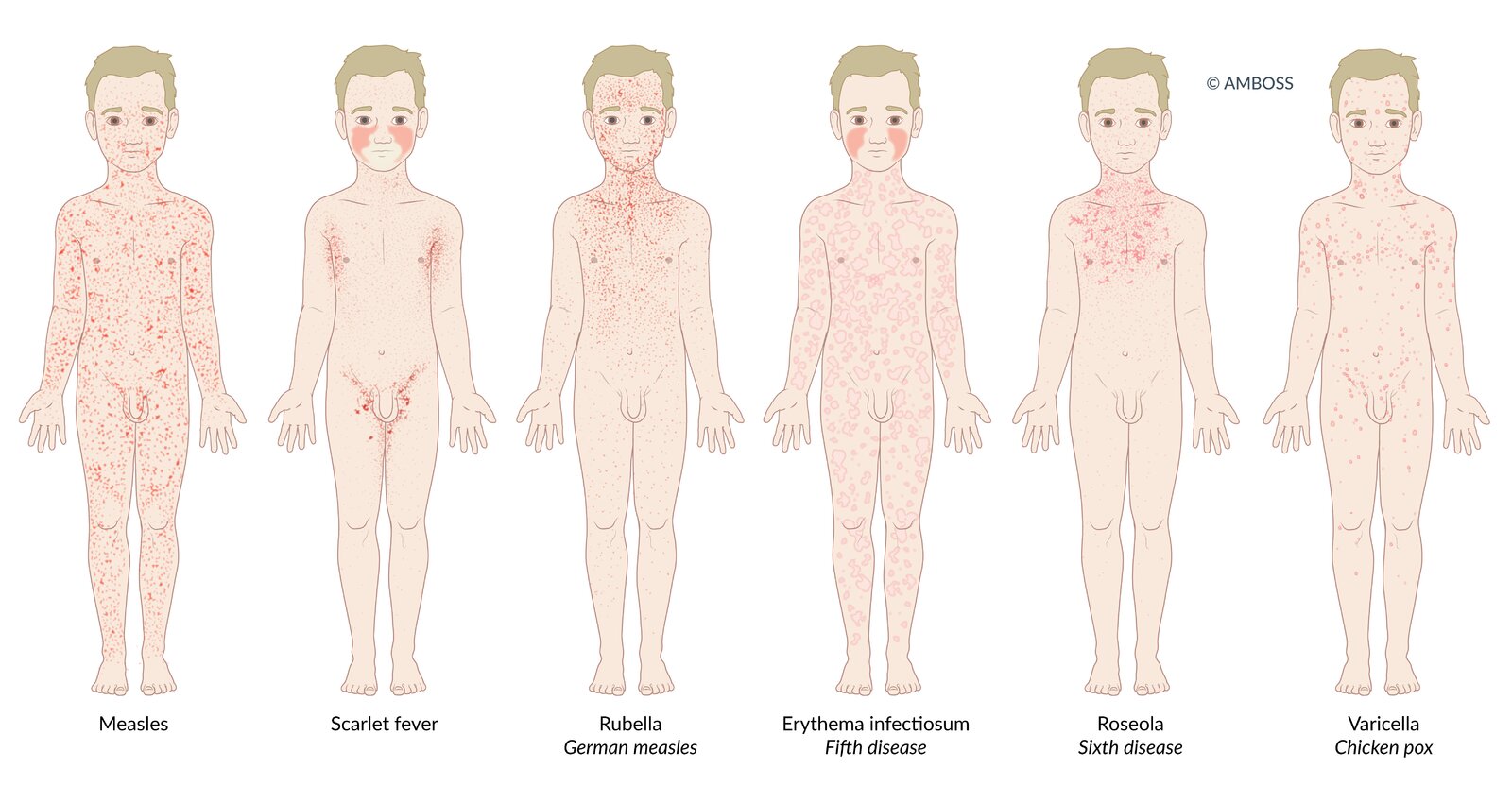
Many infectious diseases in children present with a rash (exanthem). The distribution and morphological characteristics of the exanthem allow the diseases to be differentiated from one another.
Measles: Patients present with a dark red, erythematous, maculopapular, partially confluent exanthem, which spreads from behind the ears to the rest of the body.
Scarlet fever: Patients present with a fine, light red rash with sandpaper-like texture. The exanthem begins on the neck or trunk and disseminates to the whole body. Cheeks may be flushed with perioral pallor. In flexural areas (e.g., axilla and groin), the rash may be more pronounced and linear petechiae (Pastia lines) may be present.
Rubella (German measles): Patients typically present with a nonconfluent, pink, maculopapular exanthem, which begins on the face and spreads to the trunk and extremities.
Erythema infectiosum (fifth disease): A confluent, maculopapular rash appears only in ¼ of patients. It may take on a lace-like, reticular appearance over time. Additionally, patients present with diffuse redness of the face with perioral sparing (slapped-cheek rash).
Roseola infantum (sixth disease): 3-7 days of high fever are followed by a sudden decrease in temperature and development of a patchy, blanching rose-pink maculopapular rash. The rash originates on the trunk, and may spread to the face and extremities.
Varicella (chickenpox): The exanthem affects the whole body, typically spreading to the scalp as well. Various stages of the rash occur simultaneously, which leads to the characteristic clinical finding known as “starry sky.”
© AMBOSS

© AMBOSS
Treatment
Scarlet fever can rarely occur after nonpharyngeal infection; for management in those cases, see “Impetigo” and/or “Nonpurulent skin and soft tissue infections.”
- Initiate one of the recommended antibiotic regimens for acute GAS pharyngitis, e.g.: [1][2]
- Oral penicillin V or amoxicillin
- Nonsevere penicillin reaction: oral cephalosporins (e.g., cephalexin)
- Severe penicillin reaction: oral macrolides (e.g., azithromycin) or clindamycin
- Recommend supportive care for sore throats.
- Isolation recommendations [1][2]
- Hospitalized patients: Maintain droplet precautions for 24 hours after initiating antibiotic therapy.
-
Advise outpatients to isolate until they:
- Are afebrile
- Have been taking antibiotic therapy for at least 12–24 hours
Antibiotic therapy reduces symptom duration, infectiousness, and risk of developing complications of scarlet fever. [1]


© AMBOSS
Complications
- Scarlet fever is considered a nonsuppurative (i.e., non-pus-forming) complication of streptococcal tonsillopharyngitis.
- Other complications of GAS tonsillopharyngitis may occur during or after scarlet fever, especially in patients who did not receive antibiotic therapy. E.g.:
- Nonsuppurative complications of GAS infection (e.g., poststreptococcal glomerulonephritis, acute rheumatic fever)
- Suppurative complications of acute tonsillopharyngitis (e.g., retropharyngeal abscess, peritonsillar abscess)
We list the most important complications. The selection is not exhaustive.
External Resources
References
- "CDC: Clinical Guidance for Scarlet Fever". https://web.archive.org/web/20241218162834/https://www.cdc.gov/group-a-strep/hcp/clinical-guidance/scarlet-fever.html
- Committee on Infectious Disease, American Academy of Pediatrics. "Red Book: 2024-2027 Report of the Committee on Infectious Diseases, 33rd Edition". American Academy of Pediatrics. (2024). ISBN: 9781610027373
- Forbish Skipwith D, Kelly Freeman M. "Scarlet fever". US Pharm. 33(3). :48-58. (2008)
- Herdman MT, Cordery R, Karo B, et al. "Clinical management and impact of scarlet fever in the modern era: findings from a cross-sectional study of cases in London, 2018–2019". BMJ Open. 11(12). :e057772. (2021)
- Allmon A, Deane K, Martin KL. "Common Skin Rashes in Children". Am Fam Physician. 92(3). :211-6. (2015)
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904
- Basetti S, Hodgson J, Rawson TM, Majeed A. "Scarlet fever: a guide for general practitioners". L J Prim Care. 9(5). :77-79. (2017)
- Shulman et al. "Clinical Practice Guideline for the Diagnosis and Management of Group A Streptococcal Pharyngitis: 2012 Update by the Infectious Diseases Society of America". Clinical Infectious Diseases. 55(10). :e86–e102. (2012)
- Gerber MA, Baltimore RS, Eaton CB, et al. "Prevention of Rheumatic Fever and Diagnosis and Treatment of Acute Streptococcal Pharyngitis". Circulation. 119(11). :1541-1551. (2009)
- Schachner LA, Hansen RC. "Pediatric Dermatology E-Book". Elsevier Health Sciences. (2011). ISBN: 9780723436652