Quick guide
Diagnostic approach
- ABCDE survey
- Targeted clinical evaluation
- Seizure history and/or witness account
- Evaluate for underlying causes of seizure.
- Vital signs
- POC glucose
- Continuous ECG monitoring
- Pulse oximetry
- CBC
- CMP (including calcium and magnesium)
- VBG
Consider toxicology screen, blood cultures, pregnancy test, and/or anticonvulsant drug levels if applicable.
Red flag features
- Seizure lasting ≥ 5 minutes
- Persistent postictal altered mental status
- Focal neurological deficit
- Signs of increased ICP
- Hyperthermia
- Hemodynamic instability
- Respiratory depression
Life-threatening causes
- Status epilepticus
- Hypoglycemia
- Severe electrolyte imbalance (e.g., hyponatremia, hypocalcemia)
- CNS infection (e.g., meningitis, encephalitis)
- Intracranial hemorrhage
- Eclampsia
- Hypertensive encephalopathy
- Drug poisoning
- Alcohol withdrawal
Management checklist
- Call for help and remove hazards.
- Place patient in recovery position.
- Start basic airway maneuvers.
- Oxygen therapy and pulse oximetry
- IV access
- Seizure < 5 minutes: Monitor and prepare benzodiazepines.
- Seizure ≥ 5 minutes: IV lorazepam OR IV diazepam
- No IV access: IM midazolam
- Concurrently manage rapidly reversible causes of seizures.
- Monitor for respiratory depression and hypotension.
- Consult neurology if the patient has refractory seizures.

© AMBOSS
Summary
A seizure is a transient manifestation of abnormal excessive or synchronous electrical brain activity that causes convulsions, loss of consciousness, and/or lapses of consciousness. The underlying cause of seizures is a state of neuronal hyperexcitability, which may be temporary (e.g., due to electrolyte imbalances) or long-lasting (e.g., due to inherited or acquired neural abnormalities). Provoked seizures occur as a result of various seizure triggers and underlying conditions (e.g., stroke, traumatic brain injury, alcohol withdrawal), while unprovoked seizures occur in the absence of an identifiable cause. Seizures can also be classified by onset and degree of CNS involvement (e.g., focal seizures, generalized seizures). Epilepsy is a chronic neurological disorder with diagnostic criteria that are based on seizure type, frequency, risk factors, and underlying conditions (e.g., epilepsy syndromes).
Acute complications of seizures include physical trauma and CNS tissue damage due to hyperthermia, cardiorespiratory deficits, or excitatory toxicity. Status epilepticus is a potentially life-threatening condition characterized by continuous seizure activity for more than 5 minutes that requires immediate management and stabilization. Acute seizures and status epilepticus in adults and children are most often initially treated with parenteral benzodiazepines, and then with the addition of other parenteral antiepileptic drugs (e.g., fosphenytoin) if there is no resolution. Rapidly reversible causes of seizures (e.g., hypoglycemia) should also be managed concurrently. The underlying cause is investigated based on a combination of clinical evaluation (e.g., seizure classification, identifying seizure triggers), laboratory studies, and neuroimaging. Electroencephalography (EEG) can provide additional evidence to support the diagnosis, although a normal EEG between seizures does not rule out epilepsy. Important antiepileptic drugs for the long-term treatment of epilepsy include lamotrigine (first-line treatment in focal seizures), valproate (first-line treatment in generalized seizures), and ethosuximide (first-line treatment in absence seizures). Appropriate medical treatment allows the majority of patients to remain seizure‑free in the long term and prevents long-term complications such as psychiatric conditions (e.g., anxiety, depression, psychosis), sleep disorders, and sudden unexpected death in epilepsy (SUDEP); however, patients must be monitored for adverse effects of medications (e.g., bone disease). Epilepsy in certain groups (e.g., pregnant individuals, children) also may require specific considerations for management.
For information on individual epilepsy syndromes, see “Generalized epilepsy in childhood.”
Definitions
Seizures [1]
- Seizure: an excessive and/or hypersynchronous activity of cortical neurons that results in transient neurological symptoms
-
Acute symptomatic seizure (provoked seizure): a seizure that occurs at the time or soon after the onset of an acute systemic or CNS condition. Examples include: [2]
- Within 1 week of stroke, traumatic brain injury (TBI), anoxic encephalopathy, or intracranial surgery
- Subdural hematoma
- Acute CNS infection
- Exacerbation of multiple sclerosis or other autoimmune diseases
- Metabolic disturbances
- Drug/alcohol intoxication or withdrawal
- Reflex seizure: a seizure constantly evoked by a particular stimulus (trigger) that lowers seizure threshold (e.g., flashing lights; see “Seizure triggers”)
- Unprovoked seizure: a seizure that occurs in the absence of an identifiable cause or beyond the specified interval after an acute CNS condition [1]
-
Descriptors: the following terms are used to describe events, clinical features, and EEG signs related to seizures [3]
- Ictal: occurring during a seizure
- Interictal: occurring between the seizures
- Postictal: occurring signs after a seizure
Epilepsy [1]
-
Epilepsy: a chronic neurologic disorder characterized by a predisposition to seizures as defined by one of the following: [1][4]
- Two or more unprovoked or reflex seizures separated by more than 24 hours
- One unprovoked or reflex seizure in an individual with a high risk of subsequent seizures (e.g., after traumatic brain injury, stroke, CNS infections)
- Diagnosis of an epilepsy syndrome: a group of epileptic disorders characterized by a set of features typically occurring together.
- Common features include triggers, age of onset, EEG patterns, radiological findings, and associated conditions (e.g., depression and other mood disorders, psychosis, and anxiety disorders)
- For more information about individual epilepsy syndromes, see “Generalized epilepsy in childhood.”
-
Reflex epilepsy: Epilepsy in which seizures are consistently provoked by a certain trigger (e.g., lights, music, hormonal changes during menstrual cycle). Subtypes can be determined based on the trigger and include:
- Photosensitive epilepsy
- Musicogenic epilepsy
- Catamenial epilepsy
- Drug-resistant epilepsy: epilepsy in which at least two antiepileptic drugs (administered as sequential monotherapies or as combination therapy) have failed to prevent seizures [5][6]
-
Resolved epilepsy
- An age‐dependent epilepsy syndrome that has not recurred in individuals who are now past the applicable age.
- No recurring seizures for 10 years in individuals who have not taken antiepileptic drugs for at least the last 5 years.
A single seizure or multiple provoked or triggered seizures (e.g., febrile seizures) without an underlying predisposition to seizures do not suffice for the diagnosis of epilepsy.
Epidemiology
- Incidence of unprovoked seizures: 61 per 100,000 population [7]
- Incidence of epilepsy: 79.1 per 100,000 population [8]
- Prevalence of epilepsy: 8.5 per 1,000 population [8]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
Seizure triggers [9]
Seizure triggers are stimuli that can precipitate seizures both in people with and without epilepsy. [10]
- Excessive physical exertion
- Alcohol consumption
- Fever (febrile seizures)
- Sleep deprivation
- Flashing lights (e.g., strobe lights, video games)
- Music [11]
- Hormonal changes (e.g., at different phases of the menstrual cycle, after menopause)
- Medication-related issues in patients with known epilepsy: e.g., poor adherence, recent changes in drug doses or formulation, new medication interactions
Causes of acute symptomatic seizures [2]
- TBI
- Stroke
- Anoxic encephalopathy
- Intracranial surgery
- Acute CNS infections (e.g., meningitis, encephalitis)
- Electrolyte imbalance (e.g., hypoglycemia, hypocalcemia)
- Acute metabolic disturbances (e.g., uremia)
- Alcohol withdrawal
- Recreational drug use
- Prescription drug toxicity
- Exacerbations of autoimmune disorders (e.g., SLE)
Common causes of epilepsy [12]
-
Genetic
- Genetic mutations affecting ion channels or transmitter receptors (e.g., mutations in KCNQ2 or SCN1A genes)
- Chromosomal abnormalities (e.g., Angelman syndrome, Prader-Willi syndrome, Rett syndrome)
- Genetic metabolic disorders (e.g., PKU, congenital disorders of glycosylation, lysosomal storage diseases, peroxisomal biogenesis disorders)
- Mitochondrial diseases (e.g., MELAS)
-
Structural: chronic cerebral lesion or abnormality
- Perinatal injury, e.g., hypoxic-ischemic injury
- Brain tumors and metastases [13]
- Traumatic brain injury (TBI)
- Hippocampal sclerosis
- Tuberous sclerosis
- Congenital cerebral or arteriovenous malformations
- Microcephaly, megalocephaly, cortical dysgenesis
- Cranial radiation therapy
-
Metabolic
- Inborn errors of metabolism (e.g., organic acidemias, phenylketonuria)
- Porphyrias
- Immune: autoimmune encephalitides (e.g., anti-NMDA receptor encephalitis), Rasmussen encephalitis
- Infectious: : chronic CNS infection (e.g., toxoplasmosis, malaria, neurocysticercosis) or complication of acute CNS infection (e.g., viral or bacterial meningitis or encephalitis)
Causes of epilepsy according to the age group [14]
| Etiology of epilepsy in different age groups | |
|---|---|
| Age group at manifestation | Causes |
| Neonates and infants (< 6 months) |
|
| Older infants (> 6 months) and children (< 10 years) |
|
| Adolescents (10–18 years) |
|
| Adults (18–60 years) |
|
| Older adults (> 60 years) |
|
Classification
Classification of seizures according to the ILAE 2017 classification [15]
Seizures are classified according to localization of abnormal neuronal activity and then further subcategorized based on symptoms and sometimes level of awareness.
| Basic classification of seizures | |||
|---|---|---|---|
| Focal | Generalized | Unknown | |
| Location of abnormal neuronal activity |
|
|
|
| Awareness |
|
|
|
| Symptoms |
|
|
|
| Other |
|
|
|
| * Note: An expanded version of the ILAE 2017 classification also considers further subtypes of motor and nonmotor categories. | |||
Classification of epilepsy [12]
-
General considerations
- The International League Against Epilepsy (ILAE) recommends a multilevel approach to classifying epilepsy.
- Etiology and comorbidities should be considered at each level of classification.
-
Levels of classification
- For level 1, first determine the seizure type (see “Classification of seizures” above).
- For level 2, then determine the epilepsy type, which can be:
-
Focal
- The lobe from which seizures originate should be determined.
- Epilepsy with focal-to-bilateral tonic-clonic seizures is classified as focal.
- Generalized: diagnosed in patients with generalized-onset seizures as evidenced by generalized ictal activity (e.g., 3 Hz spike-wave activity in absence seizures) and/or typical interictal discharges on EEG.
- Combined generalized and focal: diagnosed in patients who have both focal-onset and generalized-onset seizures (seen, e.g., in Dravet syndrome and Lennox-Gastaut syndrome)
- Unknown: diagnosed if there is not enough clinical information to classify seizures as focal, generalized, or combined
-
Focal
- For level 3, consider epilepsy syndromes (see “Focal seizures and syndromes” and “Generalized epilepsy in childhood” for discussion of specific syndromes)
Clinical features
Focal seizures (formerly partial seizures) [10][15][17]
- Originate in one brain hemisphere [18]
- Usually caused by focal structural abnormalities
- Symptoms depend on the anatomical location of the lesion or disturbance within the brain.
- For more information about the etiology and symptoms of seizures originating from the cortex of particular brain lobes, see “Focal seizures and syndromes.”
| Clinical features of focal seizures | |||
|---|---|---|---|
| Type | Awareness | Ictal | Postictal |
| Focal |
|
|
|
| Focal to bilateral tonic-clonic |
|
|
|
If focal to bilateral tonic-clonic type progresses rapidly to the bilateral generalized phase, initial focal symptoms may go unnoticed, leading to a potential misdiagnosis of generalized-onset seizures and inappropriate therapy.
Generalized-onset seizures [10][20][21]
- Involve one/both hemispheres
- Start with loss of consciousness.
- Patients do not recall the seizure.
| Clinical features of generalized seizures | ||
|---|---|---|
| Type | Ictal | Postictal |
| Generalized motor seizure | ||
| Tonic-clonic seizure (grand mal) |
|
|
| Clonic seizure |
|
|
| Tonic seizure |
|
|
| Myoclonic seizure |
|
|
| Myoclonic-atonic seizure |
|
|
| Myoclonic-tonic seizure |
|
|
| Atonic seizure (also known as “drop seizure” or “drop attack”) |
|
|
| Generalized nonmotor seizure (absence seizure) | ||
| Typical |
|
|
| Atypical |
|
|
It is important to distinguish between focal/bilateral tonic-clonic seizures and generalized tonic-clonic seizures, as they manifest similarly but are managed differently.
Diagnosis
The following addresses evaluation following the resolution of an acute seizure. See “Management of acute seizures and status epilepticus” for actively seizing patients.
Approach
-
First seizure
- Confirmation of seizure: Determine if the patient had a true seizure (see also “Differential diagnosis of a seizure”).
- If possible, identify the underlying cause at the initial presentation.
- Clinically evaluate the type of seizure (e.g., focal seizure vs. generalized tonic-clonic seizure) and identify potential seizure triggers.
- Obtain laboratory tests to identify metabolic abnormalities.
- Consider neuroimaging to evaluate for structural causes.
- Obtain an EEG. [22]
-
Previously diagnosed epilepsy
- Assess for common causes of breakthrough seizures and increased seizure frequency, e.g.: [23]
- Poor adherence and other medication-related issues
- Intercurrent infection or systemic illness
- Alcohol consumption and/or recreational drug use
- Check antiepileptic drug levels.
- Consider further investigations based on clinical suspicion, e.g., septic workup, selective neuroimaging. [23]
- Consider EEG for patients with treatment-refractory seizures, those who have had a change in seizure type, or if there is insufficient information for seizure classification.
- Assess for common causes of breakthrough seizures and increased seizure frequency, e.g.: [23]
In patients with an epilepsy diagnosis who present with an acute seizure, evaluate for medication-related issues, e.g., adherence, changes in drug doses or formulations, medication interactions.
Obtain neuroimaging in patients with an epilepsy diagnosis if there is a change in seizure pattern or other concerning features are present (e.g., recent head injury, new neurological deficit, persistent headache). [23]
Confirmation of seizure
-
History
-
History of present illness: description of the event by the patient (aware seizure) and/or witnesses (seizure with impaired awareness)
- Potential triggers (e.g., sleep deprivation, excessive alcohol intake)
- Prodromal symptoms (e.g., aura)
- Ictal symptoms
- Postictal symptoms
-
Past medical history
- History of epilepsy (including current antiepileptic drugs and adherence)
- History of other potential underlying conditions (e.g., head trauma, stroke, tumor, CNS infection)
-
History of present illness: description of the event by the patient (aware seizure) and/or witnesses (seizure with impaired awareness)
- Physical examination: attention should be paid to visual inspection (e.g., for bruises from falls, tongue bites, phakomatosis-specific skin manifestations) and evaluation for cardiovascular disorders
-
EEG
- Performed in individuals who present with first seizure, with insufficient information for seizure classification, and/or treatment-refractory seizures
-
Characteristic EEG findings help to establish the diagnosis of epilepsy; the absence of such findings cannot, however, rule out epilepsy.
- During the seizure (ictal)
- Epileptiform discharges (e.g., spikes, sharp waves, spike waves) are usually detected.
- Certain types of conditions characterized by seizures have characteristic discharge patterns (e.g., hypsarrhythmia in West syndrome, 3 Hz spike-and-wave in typical absence seizures, burst suppression in anoxic encephalopathy or barbiturate administration)
- If no epileptiform discharges are detected during a seizure, alternative diagnoses (e.g., psychogenic nonepileptic seizures) should be considered.
- After a seizure or between seizures (postictal or interictal)
- Often normal findings (even after provocation via sleep deprivation, hyperventilation, or visual stimuli)
- May show epileptiform activity (bursts of abnormal discharges featuring spikes and/or sharp waves, hypsarrhythmia in West syndrome)
- Video-EEG telemetry in hospitalized patients
- Continuous EEG in ambulatory patients
- During the seizure (ictal)
Nonconvulsive status epilepticus is diagnosed based on the clinical presentation (e.g., changes in behavior and/or mental status from baseline) and the demonstration of seizure activity on EEG.

Evaluation for underlying conditions
- ECG: Rule out cardiogenic causes (e.g., cardiac arrhythmias resulting in cerebral hypoxia) in all patients with loss of consciousness during a seizure.
-
MRI: Modality of choice for investigating potential underlying structural abnormalities. [24]
- All patients with first-time focal seizures
- Exception: children with history and examination suggestive of benign seizure or characteristic epilepsy syndrome
- CT: : May be used if MRI is not available, but is less sensitive for identifying soft-tissue lesions [24]
- Angiography: if vascular cause (e.g., cerebral arteriovenous malformation) is suspected
-
Laboratory screening: to identify metabolic disorders and infectious diseases, if suspected
- Blood
- CBC
- Glucose
- Electrolytes
- Prolactin
- Toxicology screening
- ESR
- Rapid plasma reagin
- Creatine kinase
- Renal and liver function tests
- Antiepileptic drug levels (e.g., phenytoin, carbamazepine, phenobarbital) [25]
- Urinalysis
- Bacterial cultures
- Cerebrospinal fluid analysis
- Endocrine studies
- Thyroid function tests
- Adrenal function tests
- Pituitary function tests
- Blood

")
")
In adults, an isolated unprovoked focal or focal to bilateral tonic-clonic seizure typically indicates a structural or metabolic origin and should receive further evaluation.
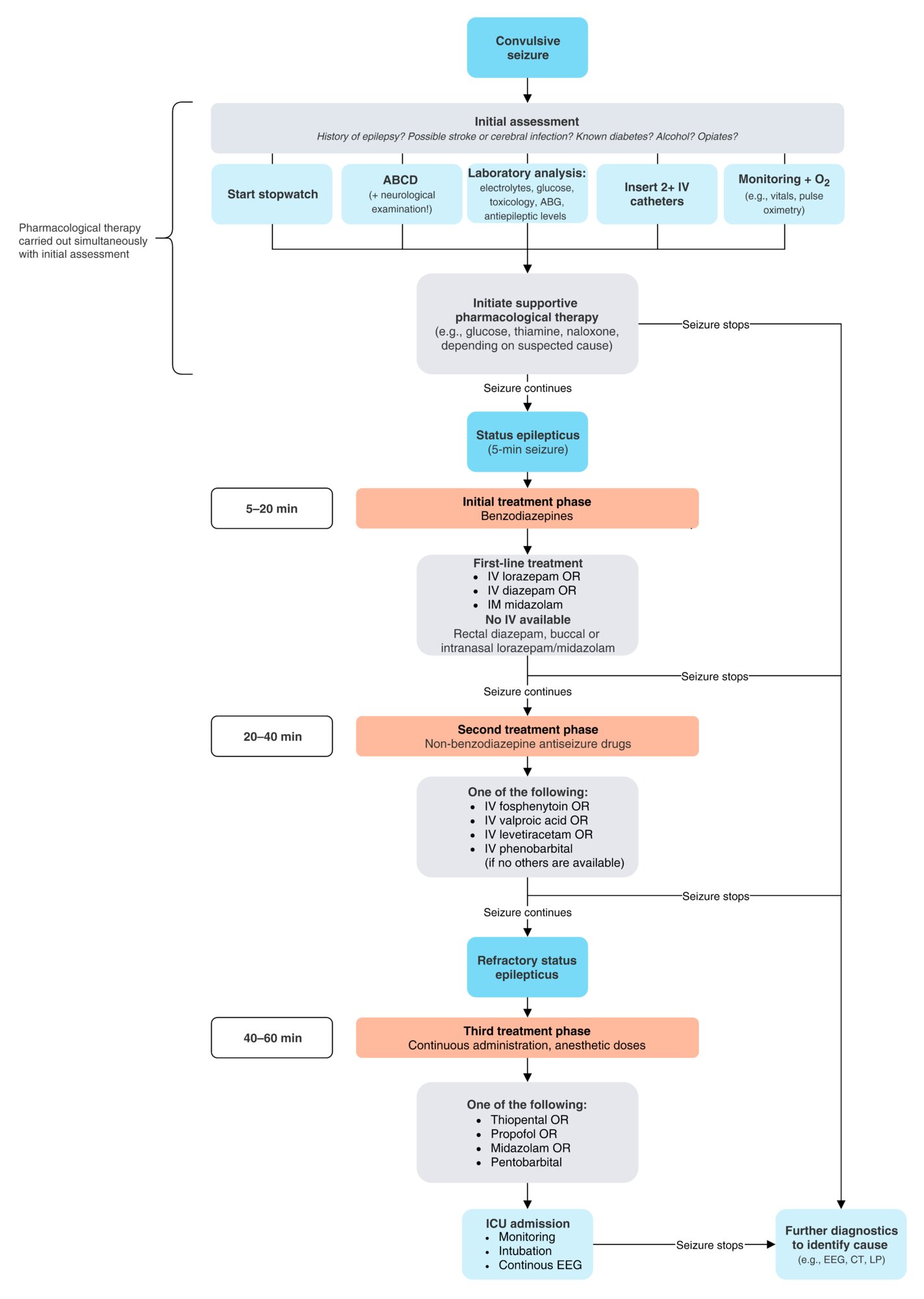
EEG (10-20 system; longitudinal bipolar montage) of a patient with temporal lobe epilepsy
Tracings of the left cerebral hemisphere show anterior temporal spikes and sharp waves (examples in red boxes).
These findings indicate a possible epileptogenic source in the left anterior temporal lobe.
Source: “Figure 2, in: Childhood temporal lobe epilepsy: correlation between electroencephalography and magnetic resonance spectroscopy: a case–control study” by Seham FA Azab, Laila M Sherief, Safaa H Saleh et al., Italian Journal of Pediatrics, licensed under CC BY 4.0. Modifications: replaced arrows. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
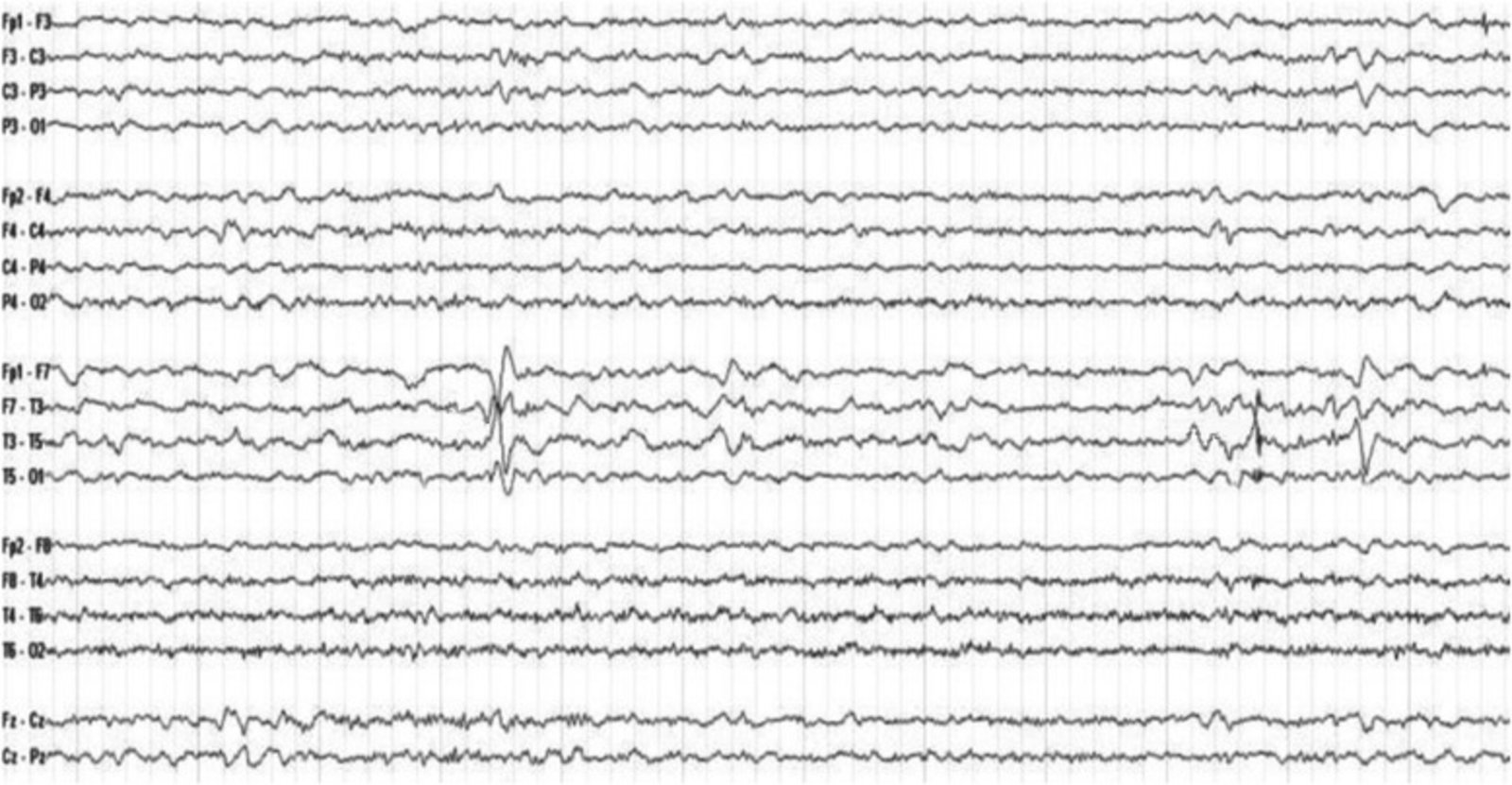
Head CT (axial view; upper row without contrast; lower row with contrast)
Calcifications can be seen even without contrast (marked areas). Additionally, the images with contrast reveal conglomerates of vessels (two examples are traced here).
Source: © IMPP
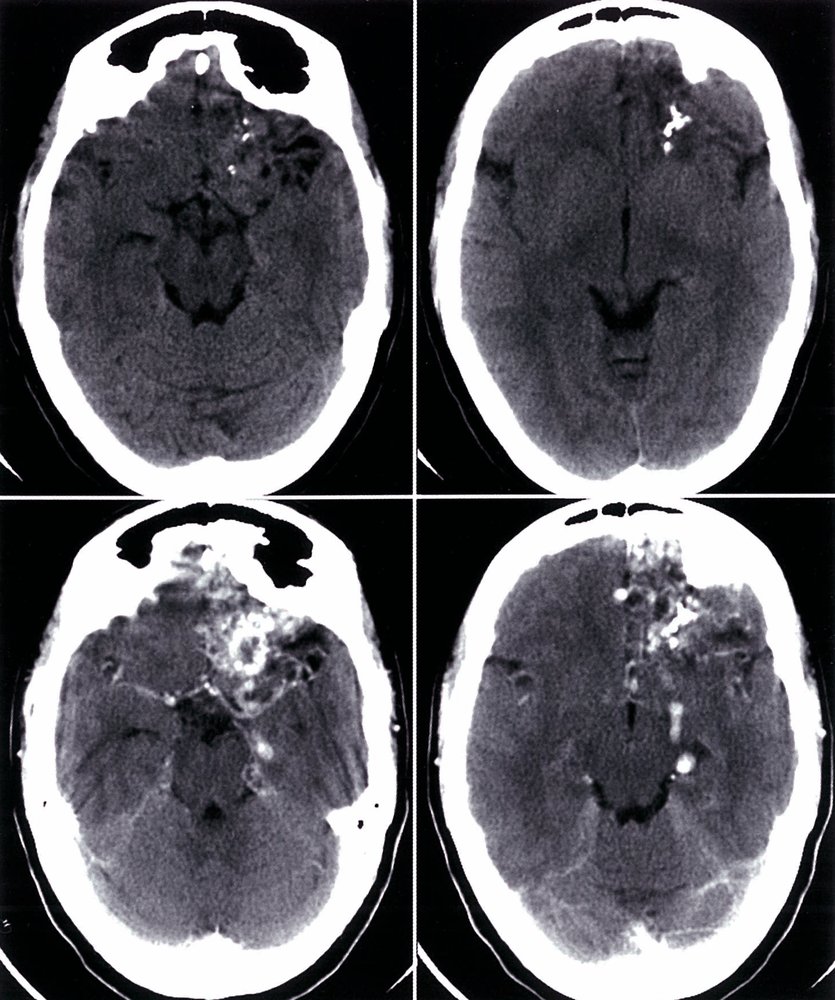
Cerebral angiography
Top left: arterial phase, coronal section
Top right: arterial phase, sagittal section
Bottom left: venous phase, coronal section
Bottom right: venous phase, sagittal section
A large vascular malformation (red overlay) is visible in the area of the temporal lobe. Since the malformation is clearly visible during both arterial and venous phases, it can be identified as arteriovenous.
Source: © IMPP
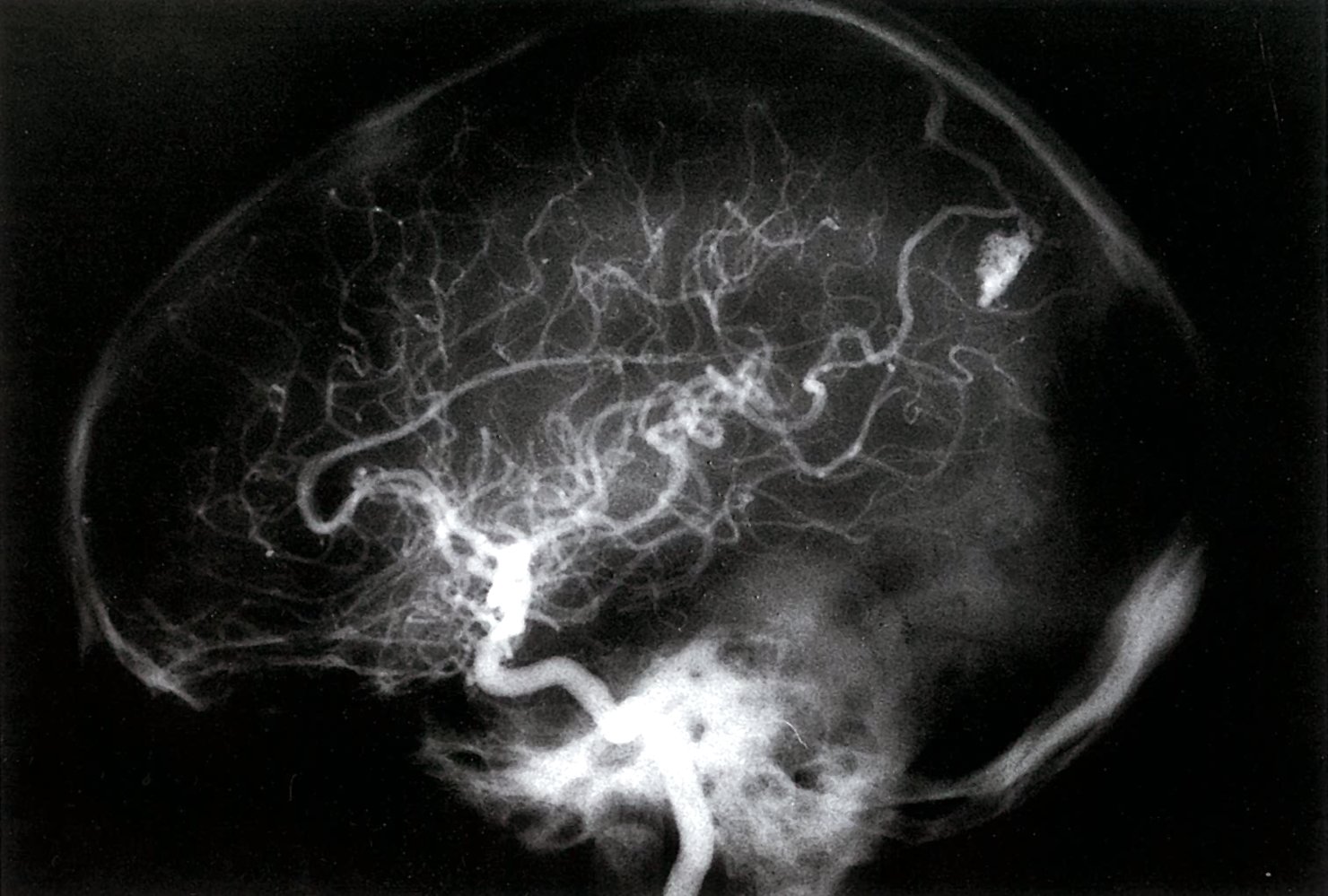
Angiography of the internal carotid artery and its branches. The parietal-occipital region shows a conglomerate of very small vessels (arteriovenous angioma, green overlay). Both the afferent artery (A) and the efferent vein (V), which drains the blood into the dural venous sinus, can be seen.
Source: © IMPP
Differential diagnoses
| Differential diagnosis of epilepsy | ||||
|---|---|---|---|---|
| Condition | Risk factors and triggers | Clinical features | Duration | Diagnostics |
| Focal-onset seizure |
|
|
|
|
| Generalized-onset motor seizure |
|
|
|
|
| Febrile seizure |
|
|
|
|
| Psychogenic nonepileptic seizure (PNES) |
|
|
|
|
| Panic attack |
|
|
|
|
| Syncope |
|
|
|
|
| Stroke/TIA |
|
|
|
|
| Migraine aura |
|
|
|
|
| Breath-holding spell |
|
|
|
|
| Self-stimulatory behavior |
|
|
|
|
| Masturbation in children [30] |
|
|
|
|
The differential diagnoses listed here are not exhaustive.
Acute management
Acute management steps are determined by the time from seizure onset and include patient stabilization, identification and treatment of reversible acute causes of seizures, and pharmacotherapy to terminate the seizure. Treatment recommendations are consistent with the 2016 American Epilepsy Society (AES) guidelines on the treatment of convulsive status epilepticus in adults and children. [31]
Approach [31][32][33]
- Start initial stabilization steps for acute seizures as needed.
- Identify and treat rapidly reversible causes of seizures.
- Implement phased-based acute seizure management.
- If < 5 minutes from seizure onset: monitor and prepare for benzodiazepine administration.
-
If the seizure lasts ≥ 5 minutes (i.e., status epilepticus): ; [34]
- Urgently administer a parenteral benzodiazepine.
- If no response; to benzodiazepines: Start a parenteral antiepileptic drug.
Status epilepticus is a life‑threatening condition. If not interrupted, it can lead to cerebral edema, hyperthermia, rhabdomyolysis, and cardiovascular failure. If the time from seizure onset is unknown, begin management for status epilepticus.
Acute seizures are often self-limited and may not require immediate pharmacological intervention.
Initial stabilization for acute seizures
- Call for help and remove or control hazards (e.g., remove sharp objects in the patient's vicinity).
- Perform an ABCDE assessment; if needed, perform cardiopulmonary resuscitation.
- Initiate basic airway maneuvers, start oxygen therapy, and place the patient in the recovery position.
- Check POC glucose and vital signs.
- Initiate continuous ECG monitoring if available and start pulse oximetry.
-
Obtain IV access and blood samples for investigations.
- Routine: CBC, CMP (including calcium and magnesium), venous blood gases
- Consider also: toxicology screen, blood cultures, pregnancy test, antiepileptic drug levels
- Perform a neurological assessment and collect relevant history.
A severe but self-limited metabolic acidosis due to marked and transient hyperlactatemia commonly occurs immediately after a seizure and usually does not require specific intervention. [35][36]
When indicated in an actively seizing patient, a nasopharyngeal airway is preferred over an oropharyngeal airway to avoid damaging intraoral structures in the setting of muscle spasms.
Phase-based acute seizure management
The following addresses acute seizure management in adults and children. For other patient groups see “Neonatal seizures”, “Eclampsia”, or “Febrile seizures.” If initial contact is ≥ 5 minutes from seizure onset or the time from seizure onset is unknown, implement interventions for early seizure and early status epilepticus simultaneously. [31]
Overview
| Overview of pharmacotherapy for acute seizures [31][34][37] | ||
|---|---|---|
| Pharmacotherapy | ||
| Seizure phase (time from seizure onset) | Preferred agents | Alternatives |
| Early seizure (0–5 minutes) |
|
|
|
Early status epilepticus (5–20 minutes): first-line therapy Administer push dose. Repeat every 5–10 minutes if no response. |
|
|
| Persistent status epilepticus (20–40 minutes): second-line therapy Administer loading dose. |
|
|
| Refractory status epilepticus (40–60 minutes) Expert guidance is required. |
|
|
Concurrently manage rapidly reversible causes of seizures (e.g., hypoglycemia, hyponatremia, hypocalcemia) without delay.
Early seizure (0–5 minutes)
- Perform initial stabilization for acute seizures.
- Monitor vital signs, oxygen saturation, and ECG.
- Identify and treat rapidly reversible causes of seizures.
- Preemptively prepare for benzodiazepine administration
Early status epilepticus (5–20 minutes)
Initiate first-line pharmacotherapy with a benzodiazepine (IV route is preferred).
- If IV access is available, administer:
- IV lorazepam [31][38]
- OR IV diazepam [31][34]
- If IV access is unavailable, administer one of the following:
- Preferred: IM midazolam [37]
- Alternatives
- Intranasal midazolam [34][37]
- OR buccal midazolam [34][37]
- OR rectal diazepam
- If there is no response to the initial dose, repeat IV benzodiazepine after 5 minutes (after 10 minutes for other routes).
- Monitor for benzodiazepine-induced hypotension and respiratory suppression.
- Consider ICU consult if there is no response to the first dose of benzodiazepine.
Persistent status epilepticus (20–40 minutes)
If first-line pharmacotherapy is unsuccessful, initiate second-line pharmacotherapy.
- Preferred: loading dose of any ONE of the following
- IV fosphenytoin [31][34][37]
- IV valproic acid [31][34][37]
- IV levetiracetam [37]
- Alternative: IV phenobarbital [31][37]
- If second-line pharmacotherapy successfully stops the seizure, consult neurology regarding the need for maintenance therapy.
- Monitor for medication adverse effects, including:
- Hypotension
- Arrhythmias
- Respiratory depression
- Postictal agitation and/or psychosis
- Prepare for possible intubation and ICU transfer if there is no response to second-line pharmacotherapy.
Refractory status epilepticus (40–60 minutes)
If first and second-line pharmacotherapy are unsuccessful:
- Consult a specialist: e.g., neurology, anesthesia, and/or critical care.
- Consider:
- Repeat dosing of second-line pharmacotherapy
- Induction of general anesthesia (coma), e.g., with IV propofol, thiopental, midazolam, or pentobarbital.
- Consider intubation and ICU admission.
- Start continuous EEG monitoring.
A recurrent seizure following full neurological recovery from a preceding seizure should be managed as a discrete episode: repeat first-line pharmacotherapy with benzodiazepines while carefully monitoring for respiratory depression.
Focal motor status epilepticus is often drug-resistant but rarely life-threatening. Phase-based management is similar to that of generalized motor seizures but general anesthesia is NOT typically required. [34]
© AMBOSS
Management of rapidly reversible causes of seizures
| Management of rapidly reversible causes of seizures | ||
|---|---|---|
| Cause | Recommended initial interventions | |
| Hypoglycemia |
|
|
| Electrolyte imbalance [41] | Hyponatremia |
|
| Hypocalcemia [45] |
|
|
| Hypomagnesemia [46] |
|
|
| Hyperthermia |
|
|
| Eclampsia [47] |
|
|
| Hypertensive encephalopathy |
|
|
| Alcohol withdrawal [48] |
|
|
| Poisoning [49] |
|
|
After seizure resolution
- Continue close monitoring until the GCS returns to baseline.
- If a normal level of consciousness is not regained within 20–30 minutes: Consider EEG to rule out ongoing nonconvulsive status epilepticus.
- Complete the history, physical examination, and neurological assessment and consider further investigations.
- See “Diagnosis of seizure disorders.”
- For children, see also “Diagnosis of febrile seizures.”
Disposition
- Hospital admission and inpatient workup is recommended for patients with any of the following: [23][32][49]
- Required > 1 dose of benzodiazepines to terminate the seizure
- Failure to return to baseline clinical status after the seizure
- Recurrent seizures
- New-onset acute symptomatic seizures for which the immediate cause has not been definitively corrected
- Acute illness (including isolated fever) or trauma
- New neurological abnormalities preceding or following the seizure
- Persistent headache
- Concerns regarding adherence or inability to ensure follow-up
- In patients who have returned to their baseline clinical status and do not require hospitalization:
- Consult neurology to advise if any adjustments to long-term treatment of epilepsy are needed.
- Consider discharge home; ensure outpatient follow-up with neurology.
- Provide education on avoiding seizure triggers, driving restrictions, and abstaining from activities that might pose a risk if seizures recur.
Driving requirements for individuals with epilepsy vary between jurisdictions but generally include a physician's evaluation and a seizure-free period of time (most commonly 6 months).
Long-term management
Long-term management following an isolated seizure [31][32][33]
- Consult neurology.
- Remove cause or provoking factors (e.g., cessation of recreational drug use, treatment of underlying disorders).
- Assess for risk of recurrence; patients with a CNS insult or lesion , abnormality on brain imaging or EEG, or nocturnal seizure are at higher risk of recurrence.
- Low risk of recurrence: shared decision-making with the patient; expectant management is usually appropriate. [32][33]
- High risk of recurrence: Treat as epilepsy.
Long-term medical therapy following a first unprovoked seizure is not required unless the patient meets the criteria for epilepsy or is at high risk of recurrence.
After the confirmation of PNES diagnosis with video-EEG, anticonvulsants should be withdrawn under medical supervision.
Patients with PNES may benefit from cognitive behavioral therapy. [53]
Long-term management of epilepsy [31][32][33]
- Start, continue, or optimize long-term antiepileptic drugs.
- Monotherapy is preferred unless the seizures are not adequately controlled.
- Drug-resistant epilepsy may be managed with nonpharmacological methods (e.g., surgery, neurostimulation, ketogenic diet).
Pharmacotherapy (antiepileptic drugs or AEDs) [54]
- AEDs reduce the risk of future seizures by raising the seizure threshold, which is pathologically lowered in individuals with epilepsy.
- Criteria for the choice of antiepileptic drugs:
- Seizure type
- Patient age
- Comorbidities
| Pharmacotherapy for epilepsy | |||
|---|---|---|---|
| Seizure type | First line | Second line | |
| Focal |
|
|
|
| Generalized | Tonic-clonic |
|
|
| Typical absence |
|
|
|
| Atypical absence |
|
|
|
| Myoclonic | |||
| Atonic | |||
Treatment regimen
-
Monotherapy should be maintained if possible.
- If initial monotherapy is ineffective, increase the dosage of the single agent or switch to an alternative agent before initiating combination therapy.
- Approx. ⅔ of epilepsy patients become seizure-free with monotherapy. [55]
-
Combination therapy should only be given if monotherapy fails.
- In this case, drugs from different classes and/or with different pharmacologic modes of action should be tried.
- Combining two or three of the standard antiepileptic drugs is usually safe.
- Failure of combination therapy : Consider nonpharmacological therapy. [56]
Termination of treatment
- Evaluated on a case‑by‑case basis
- May be considered if the patient meets all of the following:
- < 2 seizures/year
- An inconspicuous provocation EEG
- Normal psychological findings
- No hereditary predisposition
- Generally possible after 2–5 seizure‑free years with normal EEG results
- Medications should be tapered with caution.
Adverse effects of AEDs [57][58]
See “Overview of AEDs” for agent-specific adverse effects.
- Neurocognitive changes (e.g., sedation, headache, dizziness, tremor, memory impairment)
- Skin disorders (e.g., rash, SJS, DRESS)
- Psychiatric symptoms (e.g., depression, psychosis)
- Laboratory abnormalities (e.g., hyponatremia, neutropenia, thrombocytopenia)
- Gastrointestinal symptoms (e.g., nausea, vomiting, constipation)
- Weight gain or loss
In patients with liver disease, hepatically metabolized anticonvulsants (e.g., valproic acid, phenytoin, felbamate, lamotrigine) should be avoided or dose adjusted. [57][59]
Nonpharmacological therapy
- Indications: pharmacoresistant epilepsy
-
Surgery
-
Resection (surgical removal of pathological lesions)
- Patients with temporal lobe epilepsy (e.g., due to hippocampal sclerosis): resection of the anteromedial temporal lobe or of the amygdala and the hippocampus
- Patients with severe intractable seizures due to structural cerebral abnormalities confined to one hemisphere: resection of an entire hemisphere (hemispherectomy)
-
Disconnection (surgical section of neuronal circuits)
-
Callosotomy: section of the corpus callosum [60]
- Initially: partial disconnection only (usually the anterior ⅔)
- If seizures persist: complete disconnection
- Hemispherotomy: disconnection of the cortex of one hemisphere from the ipsilateral subcortical structures and cortex of the other hemisphere without removal of the affected hemisphere [61]
-
Callosotomy: section of the corpus callosum [60]
-
Resection (surgical removal of pathological lesions)
- Stimulation techniques: vagus nerve stimulation, deep brain stimulation
- Dietary measures: ketogenic diet [62]
Successful epilepsy therapy depends on determining whether the patient has focal or generalized seizures and prescribing medication accordingly.
Complications
Acute
- Hyperthermia, cardiorespiratory deficits, and excitatory toxicity, which can cause irreversible tissue damage, especially to the CNS (e.g., cortical laminar necrosis) and, in turn, increase the risk of further seizures
- Postictal lactic acidosis: postictal transient anion gap metabolic acidosis with increased lactic acid and reduced serum bicarbonate (usually resolves spontaneously within 60–90 minutes after seizure activity stops)
-
Physical trauma, such as:
- Tongue biting
- Posterior dislocation of the glenohumeral joint due to falling
- Polytrauma from a car accident
- Status epilepticus

Long term
- Psychiatric [63]
- Anxiety
- Depression and risk of suicide
- Cognitive impairment
- Psychosis (interictal psychosis, postictal psychosis, or secondary to antiepileptic drugs)
- Psychosocial distress (e.g., at the workplace)
- Sleep disturbances and insomnia [64]
- Bone disease (osteomalacia, osteoporosis) associated with antiepileptic drugs
Sudden unexpected death in epilepsy (SUDEP) [65]
- The sudden death of a person with diagnosed epilepsy that cannot be attributed to trauma or drowning and occurs with or without evidence of preceding seizure in the absence of any underlying medical conditions that could explain the event
- Usually occurs while the patient is asleep
- Is more common in patients with intractable epilepsy, frequent seizures (especially tonic-clonic seizures), and early age of onset
We list the most important complications. The selection is not exhaustive.
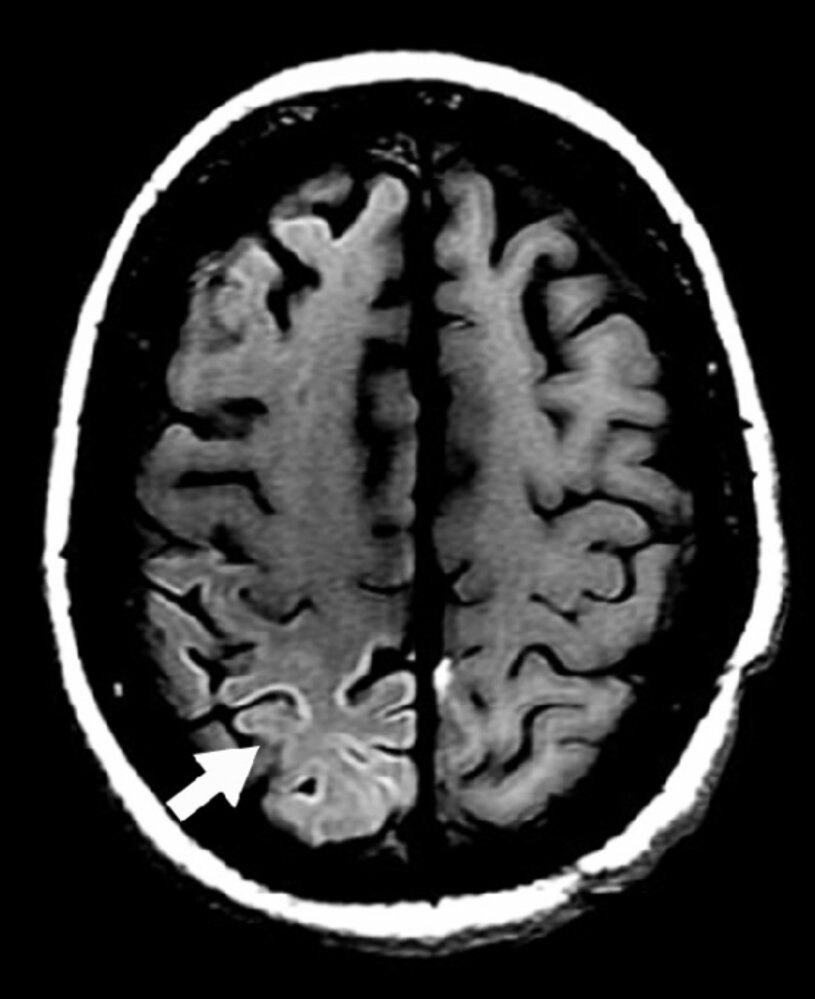
MRI head (T1 weighted; axial plane) of a patient after status epilepticus
The cortex of the right parietal lobe shows hyperintense signal (arrow). The white matter appears normal.
Cortical neurons have higher metabolic activity than white matter neurons, making them more vulnerable to damage if oxygen or nutrient supply is reduced, such as during status epilepticus.
Source: “Fig 24 b, In: Thalamic Lesions: A Radiological Review” by Renard D, Castelnovo G, Campello C et al., Hindawi, licensed under CC BY 3.0. Modifications: image cropped.
Prognosis
-
Risk of seizure recurrence
- After the first unprovoked seizure [66][67]
- With no underlying brain insult (stroke, trauma, or CNS infection): ∼ 40–50% within 2 years
- 80% of recurrences occur within 2 years of the initial seizure.
- Occurring after at least 1 week after a brain insult: ∼ 65% over the next 10 years
- With no underlying brain insult (stroke, trauma, or CNS infection): ∼ 40–50% within 2 years
- After the second unprovoked seizure: 60% within 1 year
- After an acute symptomatic seizure: ∼ 19% over the next 10 years
- After the first unprovoked seizure [66][67]
-
Treatment outcomes [68]
- 60–70% of all treated patients become seizure-free at 10 years after first seizure
- 60–90% of children and 35–57% of adults remain seizure-free after discontinuing medical therapy following a 2-year seizure-free period on antiepileptic drugs.
- Legal regulations: State laws vary with regard to the requirements for individuals with epilepsy to operate vehicles and heavy machinery. [69]
-
Mortality [70]
- Risk of all-cause mortality is 1.6–3 times higher in individuals with epilepsy than in the general population.
- The worldwide incidence of SUDEP is 1.2–6.3 per 1,000 individuals with epilepsy.
Status epilepticus
Definition [31][71]
- Status epilepticus is a seizure that lasts ≥ 5 minutes or a series of seizures in rapid succession without full neurological recovery in the interictal period, which increases the risk of long-term consequences such as neuronal injury and functional deficits.
- The time threshold after which a seizure is considered status epilepticus differs according to the type of seizure:
- Tonic-clonic seizures: ≥ 5 minutes
- Focal seizures with impaired consciousness: ≥ 10 minutes
- Absence seizures: 10–15 minutes
Etiology [72]
- Withdrawal from antiepileptic drugs
- Electrolyte imbalance (e.g., hyponatremia, hypocalcemia)
- Metabolic disturbances (e.g., hypoglycemia, uremia, porphyria)
- Structural brain lesions and/or injury (e.g., tumors, trauma, stroke)
- Anoxic brain injury
- Alcohol withdrawal
- Recreational drug use
- Drug toxicity (e.g., from tricyclic antidepressants, isoniazid)
- CNS infections (e.g., cerebral malaria, neurocysticercosis, viral encephalitis, prion diseases)
- Late-stage neurodegenerative diseases (e.g., Alzheimer disease)
Classification [71]
- With prominent motor features
- Convulsive (tonic-clonic)
- Myoclonic (with or without coma)
- Focal motor
- Tonic
- Hyperkinetic
- Without prominent motor features: nonconvulsive status epilepticus (NCSE)
- With coma
- Without coma
- Absence
- Focal (e.g., aphasia, impaired consciousness, ongoing autonomic or sensory symptoms)
Management
- See “Management of acute seizures and status epilepticus.”
- Maintain a high level of suspicion for NCSE: Consider continuous EEG and urgent neurology consult. [37]
Consider NCSE in patients with persistently altered mental status following a seizure or with otherwise unexplained altered mental status, bizarre behavior, autonomic dysfunction, or sensory symptoms.
Prognosis
- Mortality is bimodal, with the highest risk in neonates (25–39%) and patients > 80 years of age (> 50%). [73][74]
- Overall infant and child mortality: 3.6% [75]
- Overall adult mortality: 15.9% [75]
© AMBOSS
Epilepsy and contraception
General principles [76][77]
- Ongoing education on relevant pregnancy planning techniques is essential
- Contraception selection should be a shared decision (ideally with neurologist) [76]
The CDC has developed a free app to help select a contraceptive method best suited to individual needs [78][79]
Preferred contraceptive options [76][77]
-
Routine contraception:
- Levonorgestrel-containing IUD (USMEC category 1)
- DMPA (USMEC category 1) [76][80]
- Emergency contraception: Any method of emergency contraception may be used. (USMEC category 1–2).
Enzyme-inducing AEDs do not alter the efficacy of levonorgestrel-containing IUD or DMPA. [76]
Special considerations in patients on AEDs [76][77]
Hepatic enzyme-inducing AEDs
- When feasible, avoid progestin implants (USMEC category 2), combination hormonal contraceptives (USMEC category 3), and progestin-only pills (USMEC category 3).
- Alternatively, recommend simultaneous use of barrier methods.
Hepatic enzyme-inducing AEDs can make hormonal contraceptives less effective and increase the risk of unplanned pregnancies. [76][77]
Nonenzyme-inducing AEDs
- Combination hormonal contraceptives (USMEC category 1) and progestin-only pills may be used.
-
Combined hormonal contraceptives can lower lamotrigine levels significantly (risk of breakthrough seizures).
- Avoid concomitant use when feasible.
- Alternatively, consider increased lamotrigine dosage and monitor lamotrigine levels.
Combination OCPs may decrease serum concentrations of lamotrigine, thereby increasing the risk of breakthrough seizures. [76][77]
Epilepsy in pregnancy
Folic acid supplementation is recommended in all individuals capable of pregnancy. [81]
Information on other seizure disorders that can occur in pregnancy (e.g., eclampsia, acute symptomatic seizure) is detailed separately.
Epidemiology [82][83][84]
- Approximately 1.5 million female individuals of reproductive age in the US have epilepsy.
- Approximately 24,000 female individuals with epilepsy become pregnant per year.
- In the majority of cases, pregnancy does not affect seizure frequency.
Etiology
Factors associated with an increased risk of epileptic seizures during pregnancy include:
- Reduced plasma concentration of AEDs due to physiologic changes in pregnancy (e.g., steroid-hormone induced hepatic enzyme induction, increased renal clearance)
- Psychosocial stress
- Sleep deprivation
- Hormonal changes (e.g., increased estrogen:progesterone ratio)
Management [77][82][84][85]
General principles
- For all female individuals with epilepsy who are currently pregnant or expecting to be pregnant:
- Initiate folic acid supplementation. [77][81][82][86][87]
- Counsel patients on the teratogenic potential of AEDs and the associated risks of adverse pregnancy outcomes. [76]
- Consult neurology and maternal-fetal medicine for obstetrical and drug management recommendations.
- If possible, obtain AED drug levels prior to pregnancy to determine a baseline level for continued monitoring. [82]
- Strict management of therapeutic AED levels during pregnancy is the gold standard of care for pregnant individuals with epilepsy. [77]
-
Vitamin K supplementation to prevent vitamin K deficiency bleeding of the newborn (VKDB) [85][86]
- All neonates should receive the standard dose of parenteral vitamin K supplementation at birth. [86][88]
- There is insufficient evidence to support the use of prenatal vitamin K supplementation to prevent VKDB in neonates of patients on enzyme-inducing AEDs.
- Epilepsy alone is not an indication for cesarean delivery. [77]
Intrapartum exposure to teratogenic AEDs is associated with a 2–3 fold increase in the likelihood of major congenital malformations. [76]
AED management [77][82][84][85][87]
Adjust AED regimen as needed in consultation with a neurologist to maximize seizure control and minimize teratogenic risk. [84][87][89]
- Reduce AED-associated risk of major congenital malformations (MCMs).
- AEDs with low teratogenic risk: lamotrigine and levetiracetam
- AEDs with high teratogenic risk: valproate (highest risk), phenobarbital, topiramate, and phenytoin
- Monotherapy is associated with a lower risk of MCMs compared to polytherapy. [77][90]
In patients planning pregnancy
-
Adjust AED therapy as needed early enough to: [82]
- Measure AED levels before conception (if possible) and determine the lowest effective dose
- Evaluate the efficacy of any new therapies
- Consult the treating neurologist before discontinuing AEDs. [91]
During pregnancy
- Measure AED levels regularly (e.g., monthly), especially for AEDs with increased clearance during pregnancy. [77][82]
- Adjust target levels as needed, in consultation with neurology.
During the postpartum period
- Encourage breastfeeding; counsel patients regarding the following: [82]
- Overall, the benefits of breastfeeding outweigh the risks. [84][86]
- Monitor infants for adverse effects of AEDs (e.g., sedation, poor sucking, rash). [90]
- Adjust AED dosage in consultation with neurology; specialists may taper dosage to prepregnancy levels within 2–3 weeks after delivery. [90]
Valproate is the AED associated with the highest risk of major congenital malformations and should be avoided, if possible, in patients with epilepsy who may become pregnant. [57][77][82][87]
Complications [77][87]
- Fetal complications
- Increased risk of low birth weight and small size for gestational age due to maternal seizures
- Teratogenic effects of AEDs (e.g., congenital malformations, abnormal neurocognitive development)
- Maternal complications: increased risk of the following
- Preterm delivery
- Need for cesarean section
- Preeclampsia
- Severe postpartum hemorrhage
- Death during delivery
Seizures in neonates (birth to 4 weeks of age)
Risk factors [92][93][94]
- Birth and/or pregnancy complications
- Family history
- See also “Etiology of epilepsy in different age groups.”
Clinical features [92][93]
Clinical features are often subtle or absent.
- Automatism
- Focal seizures (tonic or clonic)
- Myoclonic seizures
- Behavioral arrest
- Autonomic
- See also “Brief resolved unexplained event.”
Diagnosis [92][93][94]
- Clinical evaluation: E.g., determine the patient's age at seizure onset (i.e., in days or weeks) and perform a full history and physical examination.
- POC glucose, electrolytes
- Neonatal sepsis workup (See “Neonatal infection.”)
- Continuous video-EEG for at least 24 hours [95]
- Neuroimaging: cranial ultrasound and/or brain MRI
- Consider further investigations on a case-by-case basis: e.g., testing for inborn errors of metabolism, evaluating for nonaccidental trauma
Management [92][93][94]
- Stabilize the patient while focusing on supporting ABCs (see also “CPR in infants” and “Neonatal resuscitation”).
- Treat the underlying cause: e.g., correction of hypoglycemia and electrolyte abnormalities, empiric antibiotics for neonatal infection.
- Administer an antiepileptic agent to terminate clinical and subclinical neonatal seizures. [92][93][94][96]
- First-line: phenobarbital
- Second-line: Fosphenytoin (preferred) or phenytoin
- Alternative and third-line agents may include midazolam, lidocaine, or levetiracetam; expert consultation is advised.
- Consult neonatology and pediatric neurology.
EEG screening and diagnostic confirmation are essential, as most seizures in neonates are subclinical and many other clinical entities can mimic true seizures.
Related One-Minute Telegram
- One-Minute Telegram 61-2022-1/3: Restock your aspirin and laceration repair kits - it’s almost Halloween!
Interested in the newest medical research, distilled down to just one minute? Sign up for the One-Minute Telegram in “Tips and links” below.
External Resources
- One-Minute Telegram
- Free CDC Application to Assist Contraception Selection According to the USMEC category
- 2020 ACOG Committee Opinion on Gynecologic Management of Adolescents and Young Women With Seizure Disorders
- 2019 International League Against Epilepsy Task Force on Women and Pregnancy:Management of Epilepsy in Pregnancy (Executive Summary)
- 2016 AES Guideline on the Treatment of Convulsive Status Epilepticus in Children and Adults
- Youtube video "Understanding generalized seizures"
- Youtube video "Understanding partial epilepsy"
References
- Fisher RS, Acevedo C, Arzimanoglou A, et al. "ILAE official report: a practical clinical definition of epilepsy". Epilepsia. 55(4). :475-482. (2014)
- Beghi E, Carpio A, Forsgren L, et al. "Recommendation for a definition of acute symptomatic seizure". Epilepsia. 51(4). :671-675. (2010)
- Fisher RS, Scharfman HE, deCurtis M. "How Can We Identify Ictal and Interictal Abnormal Activity?". Springer Netherlands. :3-23. (2014). ISBN: 9789401789134
- Fisher RS, Boas W van E, Blume W, et al. "Epileptic Seizures and Epilepsy: Definitions Proposed by the International League Against Epilepsy (ILAE) and the International Bureau for Epilepsy (IBE)". Epilepsia. 46(4). :470-472. (2005)
- Kalilani L, Sun X, Pelgrims B, Noack-Rink M, Villanueva V. "The epidemiology of drug-resistant epilepsy: A systematic review and meta-analysis". Epilepsia. 59(12). :2179-2193. (2018)
- Kwan P, Arzimanoglou A, Berg AT, et al. "Definition of drug resistant epilepsy: Consensus proposal by the ad hoc Task Force of the ILAE Commission on Therapeutic Strategies". Epilepsia. 51(6). :1069-1077. (2009)
- Hauser WA, Beghi E. "First seizure definitions and worldwide incidence and mortality". Epilepsia. 49. :8-12. (2008)
- Helmers SL, Thurman DJ, Durgin TL, Pai AK, Faught E. "Descriptive epidemiology of epilepsy in the U.S. population: A different approach". Epilepsia. 56(6). :942-948. (2015)
- Anna Szűcs, Beáta Rosdy, Anna Kelemen, András Horváth, Péter Halász. "Reflex seizure triggering: Learning about seizure producing systems". Seizure. 69. :25-30. (2019)
- Blume WT, Lüders HO, Mizrahi E, et al. "Glossary of descriptive terminology for ictal semiology: report of the ILAE task force on classification and terminology". Epilepsia. 42(9). :1212-1218. (2001)
- Ellis L. "The potential mechanism of musicogenic epilepsy and future research avenues". Bioscience Horizons: The International Journal of Student Research. 10. (2017)
- "The Organization of the Epilepsies: Report of the ILAE Commission on Classification and Terminology"
- Maschio M. "Brain Tumor-Related Epilepsy". Current Neuropharmacology. 10(2). :124-133. (2012)
- Ropper A, Klein J, Samuels M. "Adams and Victor's Principles of Neurology 10th Edition". McGraw-Hill Education / Medical. (2014). ISBN: 9780071794794
- Scheffer IE, Berkovic S, Capovilla G, et al. "ILAE classification of the epilepsies: Position paper of the ILAE Commission for Classification and Terminology". Epilepsia. 58(4). :512-521. (2017)
- Fisher RS, Cross JH, D’Souza C, et al. "Instruction manual for the ILAE 2017 operational classification of seizure types". Epilepsia. 58(4). :531-542. (2017)
- Daroff RB, et al. "Bradley's Neurology in Clinical Practice". Elsevier. ISBN: 9780323287838
- "Epilepsy Diagnosis - Focal Onset Seizure". https://www.epilepsydiagnosis.org/seizure/focal-seizure-overview.html
- Berg AT, Berkovic SF, Brodie MJ et al. "Revised terminology and concepts for organization of seizures and epilepsies: Report of the ILAE Commission on Classification and Terminology, 2005–2009". Epilepsia. 51(4). :676-685. (2010)
- Kasper DL, Fauci AS, Hauser SL, et al. "Harrison's Principles of Internal Medicine". McGraw-Hill Education. (2015). ISBN: 9780071802161
- "Seizure Disorders". http://www.merckmanuals.com/professional/neurologic-disorders/seizure-disorders/seizure-disorders. [2016-06-01]
- Jagoda A, Gupta K. "The Emergency Department Evaluation of the Adult Patient Who Presents with a First-Time Seizure". Emerg Med Clin North Am. 29(1). :41-49. (2011)
- Galizia EC, Faulkner HJ. "Seizures and epilepsy in the acute medical setting: presentation and management". Clin Med (Northfield Il). 18(5). :409-413. (2018)
- Bernasconi A, Cendes F, Theodore WH, et al. "Recommendations for the use of structural magnetic resonance imaging in the care of patients with epilepsy: A consensus report from the International League Against Epilepsy Neuroimaging Task Force". Epilepsia. (2019)
- Walters RJL, Hutchings AD, Smith DF, Smith PEM. "Inappropriate requests for serum anti-epileptic drug levels in hospital practice". QJM.. 97(6). :337-341. (2004)
- Woollacott IOC, Scott C, Fish DR, Smith SM, Walker MC. "When do psychogenic nonepileptic seizures occur on a video/EEG telemetry unit?". Epilepsy & Behavior. 17(2). :228-235. (2010)
- Szabó L, Siegler Z, Zubek L, et al. "A detailed semiologic analysis of childhood psychogenic nonepileptic seizures". Epilepsia. 53(3). :565-570. (2012)
- Seneviratne U, Minato E, Paul E. "How reliable is ictal duration to differentiate psychogenic nonepileptic seizures from epileptic seizures?". Epilepsy Behav. 66. :127-131. (2017)
- Gedzelman E, LaRoche S. "Long-term video EEG monitoring for diagnosis of psychogenic nonepileptic seizures". Neuropsychiatric Disease and Treatment. :1979. (2014)
- Nechay A, Ross LM, Stephenson JB, O'Regan M. "Gratification disorder ("infantile masturbation"): a review.". Arch Dis Child. 89(3). :225-6. (2004)
- Tellez-Zenteno JF, Patten SB, Jetté N, Williams J, Wiebe S. "Psychiatric Comorbidity in Epilepsy: A Population-Based Analysis". Epilepsia. :070728063136006-???. (2007)
- Schmitt B. "Sleep and Epilepsy Syndromes". Neuropediatrics. 46(03). :171-180. (2015)
- Nashef L, So EL, Ryvlin P, Tomson T. "Unifying the definitions of sudden unexpected death in epilepsy". Epilepsia. 53(2). :227-233. (2011)
- Berg AT. "Risk of recurrence after a first unprovoked seizure". Epilepsia. 49(Suppl 1). :13-18. (2008)
- Hesdorffer DC, Benn EK, Cascino GD, Hauser WA. "Is a first acute symptomatic seizure epilepsy? Mortality and risk for recurrent seizure.". Epilepsia. 50(5). :1102-8. (2009)
- Beghi E, Giussani G, Sander JW. "The natural history and prognosis of epilepsy.". Epileptic Disord. 17(3). :243-53. (2015)
- "State Driving Laws Database". https://www.epilepsy.com/driving-laws
- Thurman DJ, Logroscino G, Beghi E, et al. "The burden of premature mortality of epilepsy in high-income countries: A systematic review from the Mortality Task Force of the International League Against Epilepsy.". Epilepsia. 58(1). :17-26. (2017)
- Trinka E, Cock H, Hesdorffer D, et al. "A definition and classification of status epilepticus - Report of the ILAE Task Force on Classification of Status Epilepticus". Epilepsia. 56(10). :1515-1523. (2015)
- Glauser T, Shinnar S, Gloss D, et al. "Evidence-Based Guideline: Treatment of Convulsive Status Epilepticus in Children and Adults: Report of the Guideline Committee of the American Epilepsy Society". Epilepsy Currents. 16(1). :48-61. (2016)
- Trinka E, Höfler J, Zerbs A. "Causes of status epilepticus". Epilepsia. 53. :127-138. (2012)
- Brophy GM, Bell R, et al. "Guidelines for the Evaluation and Management of Status Epilepticus". Neurocrit Care. 17(1). :3-23. (2012)
- Pisani F, Cerminara C, Fusco C, Sisti L. "Neonatal status epilepticus vs recurrent neonatal seizures: Clinical findings and outcome". Neurology. 69(23). :2177-2185. (2007)
- Boggs JG. "Mortality Associated with Status Epilepticus". Epilepsy Currents. 4(1). :25-27. (2004)
- Neligan A, Noyce AJ, Gosavi TD, et al. "Change in Mortality of Generalized Convulsive Status Epilepticus in High-Income Countries Over Time: A Systematic Review and Meta-analysis.". JAMA neurology. (2019)
- Huff JS, Melnick ER, Tomaszewski CA, et al. "Clinical Policy: Critical Issues in the Evaluation and Management of Adult Patients Presenting to the Emergency Department With Seizures". Ann Emerg Med. 63(4). :437-447.e15. (2014)
- Krumholz A, Wiebe S, Gronseth GS, et al. "Evidence-based guideline: Management of an unprovoked first seizure in adults: Report of the Guideline Development Subcommittee of the American Academy of Neurology and the American Epilepsy Society". Neurology. 84(16). :1705-1713. (2015)
- Crawshaw AA, Cock HR. "Medical management of status epilepticus: Emergency room to intensive care unit". Seizure. 75. :145-152. (2020)
- Bibbins-Domingo et al. "Folic Acid Supplementation for the Prevention of Neural Tube Defects". JAMA. 317(2). :183-189. (2017)
- Tomson T, Battino D, Bromley R, et al. "Executive Summary: Management of epilepsy in pregnancy: A report from the International League Against Epilepsy Task Force on Women and Pregnancy". Epilepsia. 60(12). :2343-2345. (2019)
- Sazgar M. "Treatment of Women With Epilepsy". CONTINUUM: Lifelong Learning in Neurology. 25(2). :408-430. (2019)
- Voinescu PE, Meador KJ. "Epilepsy Complicating Pregnancy". Curr Obstet Gynecol Rep. (2022)
- Li Y, Meador KJ. "Epilepsy and Pregnancy". Continuum (Minneap Minn). 28(1). :34-54. (2022)
- Patel SI, Pennell PB. "Management of epilepsy during pregnancy: an update". Therapeutic Advances in Neurological Disorders. 9(2). :118-129. (2015)
- Harden CL, Pennell PB, Koppel BS, et al. "Practice Parameter update: Management issues for women with epilepsy--Focus on pregnancy (an evidence-based review): Vitamin K, folic acid, blood levels, and breastfeeding: Report of the Quality Standards Subcommittee and Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology and American Epilepsy Society". Neurology. 73(2). :142-149. (2009)
- Spiegel R, Merius H. "Principles of Epilepsy Management for Women in Their Reproductive Years". Front Neurol. 11. (2020)
- ACOG. "Gynecologic Management of Adolescents and Young Women With Seizure Disorders. ACOG Committee Opinion, Number 806". Obstetrics & Gynecology. 135(5). :e213-e220. (2020)
- Hand I, Noble L, Abrams SA. "Vitamin K and the Newborn Infant". Pediatrics. 149(3). (2022)
- Harden CL, Hopp J, Ting TY, et al. "Practice Parameter update: Management issues for women with epilepsy--Focus on pregnancy (an evidence-based review): Obstetrical complications and change in seizure frequency: Report of the Quality Standards Subcommittee and Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology and American Epilepsy Society". Neurology. 73(2). :126-132. (2009)
- Bui E. "Women’s Issues in Epilepsy". Continuum (Minneap Minn). 28(2). :399-427. (2022)
- Hessler A, Dolbec K. "Seizures". Obstet Gynecol. 137(1). :207-207. (2021)
- Kanner AM, Bicchi MM. "Antiseizure Medications for Adults With Epilepsy". JAMA. 327(13). :1269. (2022)
- Soul JS. "Acute symptomatic seizures in term neonates: Etiologies and treatments". Semin Fetal Neonatal Med.. 23(3). :183-190. (2018)
- Glass HC. "Neonatal Seizures". Clin Perinatol. 41(1). :177-190. (2014)
- Co JPT, Elia M, Engel J, et al. "Proposal of an Algorithm for Diagnosis and Treatment of Neonatal Seizures in Developing Countries". Epilepsia. 48(6). :1158-1164. (2007)
- Renée A. Shellhaas, Taeun Chang, Tammy Tsuchida, et al. "The American Clinical Neurophysiology Society's Guideline on Continuous Electroencephalography Monitoring in Neonates". Journal of Clinical Neurophysiology. 28(6). :611-617. (2011)
- Kaminiów K, Kozak S, Paprocka J. "Neonatal Seizures Revisited". Children. 8(2). :155. (2021)
- Goldstein LH, Chalder T, Chigwedere C, et al. "Cognitive-behavioral therapy for psychogenic nonepileptic seizures: A pilot RCT". Neurology. 74(24). :1986-1994. (2010)
- Kanner AM, Ashman E, Gloss D, et al. "Practice guideline update summary: Efficacy and tolerability of the new antiepileptic drugs I: Treatment of new-onset epilepsy". Neurology. 91(2). :74-81. (2018)
- Glauser T, Ben-Menachem E, Bourgeois B, et al. "Updated ILAE evidence review of antiepileptic drug efficacy and effectiveness as initial monotherapy for epileptic seizures and syndromes". Epilepsia. 54(3). :551-563. (2013)
- St. Louis E. "Truly “Rational” Polytherapy: Maximizing Efficacy and Minimizing Drug Interactions, Drug Load, and Adverse Effects". Current Neuropharmacology. 7(2). :96-105. (2009)
- Vossler DG, Weingarten M, Gidal BE. "Summary of Antiepileptic Drugs Available in the United States of America". Epilepsy Curr. 18(4_suppl). :1-26. (2018)
- Vidaurre J, Gedela S, Yarosz S. "Antiepileptic Drugs and Liver Disease". Pediatr Neurol. 77. :23-36. (2017)
- Asadi-Pooya AA, Sharan A, Nei M, Sperling MR. "Corpus callosotomy.". Epilepsy Behav. 13(2). :271-8. (2008)
- De Ribaupierre S, Delalande O. "Hemispherotomy and other disconnective techniques.". Neurosurg Focus. 25(3). :E14. (2008)
- Bough KJ, Rho JM. "Anticonvulsant mechanisms of the ketogenic diet.". Epilepsia. 48(1). :43-58. (2007)
- Lipka K, Bülow H-H. "Lactic acidosis following convulsions". Acta Anaesthesiol Scand. 47(5). :616-618. (2003)
- Orringer CE, Eustace JC, Wunsch CD, Gardner LB. "Natural History of Lactic Acidosis after Grand-Mal Seizures". N Engl J Med. 297(15). :796-799. (1977)
- Manno EM. "Status Epilepticus". Neurohospitalist. 1(1). :23-31. (2011)
- Dhir S, Tarasenko M, Napoli E, Giulivi C. "Neurological, Psychiatric, and Biochemical Aspects of Thiamine Deficiency in Children and Adults.". Front psychiatry. 10. :207. (2019)
- Smith TJ, Johnson CR, Koshy R, et al. "Thiamine deficiency disorders: a clinical perspective". Ann N Y Acad Sci. 1498(1). :9-28. (2020)
- Castilla-Guerra L, Fernández-Moreno M del C, López-Chozas JM, Fernández-Bolaños R. "Electrolytes Disturbances and Seizures". Epilepsia. 47(12). :1990-1998. (2006)
- Fleisher GR, Ludwig S. "Textbook of Pediatric Emergency Medicine ". Lippincott Williams & Wilkins. (2010). ISBN: 9781605471594
- Verbalis JG, Goldsmith SR, Greenberg A, et al. "Diagnosis, evaluation, and treatment of hyponatremia: expert panel recommendations". Am J Med. 126(10). :S1-S42. (2013)
- Watson S, Thompson A. "Pediatric Intensive Care". Oxford University Press. (2017). ISBN: 9780190638436
- "Hypocalcemia: Diagnosis and Treatment". https://www.ncbi.nlm.nih.gov/books/NBK279022/. [2016-01-03]
- Chen BB, Prasad C, Kobrzynski M, Campbell C, Filler G. "Seizures Related to Hypomagnesemia". Child Neurology Open. 3. :2329048X1667483. (2016)
- Leeman L, Dresang LT, Fontaine P. "Hypertensive Disorders of Pregnancy". Am Fam Physician. 93(2). :121-7. (2016)
- Alvanzo et al. "The ASAM Clinical Practice Guideline on Alcohol Withdrawal Management". Journal of Addiction Medicine. 14(3S). :1-72. (2020)
- Walls R, Hockberger R, Gausche-Hill M. "Rosen's Emergency Medicine". Elsevier Health Sciences. (2018). ISBN: 9780323354790
- "Ten Things Physicians and Patients Should Question". https://www.choosingwisely.org/societies/american-college-of-medical-toxicology-and-the-american-academy-of-clinical-toxicology/. [2015-03-06]
- Daly FFS. "A risk assessment based approach to the management of acute poisoning". Emerg Med J. 23(5). :396-399. (2006)
- Nelson LS, Howland M, Lewin NA, et al. "Goldfrank's Toxicologic Emergencies, 11th edition". McGraw-Hill Education. (2019). ISBN: 9781259859618
- "CDC USMEC USSPR Contraception App". https://web.archive.org/web/20230128132619/https://www.cdc.gov/reproductivehealth/contraception/contraception-app.html. [2022-05-19]
- Clark EA, Curtis KM. "Contraception Recommendations: Updates for the Busy Clinician". Am Fam Physician. 106(3). :227-228. (2022)
- ACOG. "ACOG Practice Bulletin No. 206: Use of Hormonal Contraception in Women With Coexisting Medical Conditions". Obstet Gynecol. 133(2). :e128-e150. (2019)