Summary
Septic (infectious) arthritis is an infection of the joint space, which can occur in a native joint or a prosthetic joint. Patients with underlying joint diseases (e.g., rheumatoid arthritis) are at an increased risk of septic arthritis. Routes of infection include hematogenous spread (most common), direct inoculation (e.g., iatrogenic, penetrating trauma), and contiguous spread. Patients with native joint infections usually present with an acutely swollen, painful joint, limited range of motion, and fever, whereas patients with prosthetic joint infections (PJIs) usually have a milder, chronic course, which often makes diagnosis more challenging. All patients with suspected septic arthritis should undergo prompt arthrocentesis for synovial fluid analysis. Early administration of empiric antibiotic therapy and therapeutic arthrocentesis is indicated for native joint infections to prevent cartilage destruction. PJIs typically require surgical debridement, including removal of the prosthesis in some cases; empiric antibiotics are not recommended unless the patient is critically ill. Targeted antibiotics should be initiated in all patients once culture and sensitivity results are available.


© AMBOSS
Etiology
Routes of spread
-
Hematogenous spread (most common)
- From a distant site (e.g., abscesses, wound infection, septicemia)
- Disseminated infection (e.g., gonorrhea)
-
Direct contamination
- Iatrogenic (e.g., joint injection, arthrocentesis , arthroscopy ) [1]
- Trauma (e.g., open wounds around the joint , penetrating trauma)
- Contiguous spread (e.g., septic bursitis, osteomyelitis)
Risk factors for septic arthritis
- Prosthetic implant
- Interventions (e.g., intra-articular injections)
- Underlying joint disease, especially rheumatoid arthritis
- Immunosuppressed state
- Diabetes mellitus
- Age > 80 years
- Chronic skin infections
- IV drug use
- Endocarditis (polyarticular septic arthritis)
Causative organisms
For etiology in children, see “Septic arthritis in children.”
-
Staphylococcus aureus
- Most common in adults
- Frequently found in patients with arthritis following invasive joint procedures [2]
- Streptococci
- Neisseria gonorrheae
- Gram-negative rods esp. E. coli and P. aeruginosa
- S. epidermidis
- H. influenzae
- M. tuberculosis and atypical mycobacteria
Clinical features
- Acute onset
- Classical triad of fever, joint pain, and restricted range of motion
-
Arthritis
- Usually monoarticular
- Most commonly affected joints: knees (followed by hip, wrists, shoulders, and ankles)
- Joints are swollen, red, warm, and painful.


The right knee and area around the knee is markedly swollen and slightly erythematous.
Source: “Kneeffusion” by James Heilman, MD, Wikimedia Commons, licensed under CC BY-SA 3.0. Modifications: arrow removed.
{kind=link}
Subtypes and variants
Prosthetic joint infection (PJI) [3][4]
-
Etiology
- Early onset (< 3 months of placement): most commonly S. aureus
- Delayed onset (3–12 months of placement); : coagulase-negative staphylococci, particularly S. epidermidis
- Late onset (> 12 months of placement): most commonly S. aureus
-
Clinical features
- Usually prolonged, low-grade course
- Minimal swelling, with or without a sinus that drains pus
- Can present acutely (see “Clinical features” above)
- Management: See “Diagnostics” and “Treatment” sections.
In order to avoid infection, strict aseptic precautions should be ensured in any procedure that involves penetration of the joint space.
Bacterial coxitis [5]
- Description: septic arthritis of the hip (rare)
- Etiology: S. aureus and group A streptococcus account for the majority of cases
-
Clinical findings
- Joint pain (may be referred to the groin or knee)
- Patient's hip is often flexed and externally rotated (this decreases intraarticular pressure and alleviates pain)
- See “Clinical features” above
- Management: See “Diagnostics” and “Treatment” sections.
Bacterial coxitis is an orthopedic emergency that requires urgent management to avoid joint destruction.
Gonococcal arthritis
- Gonococcal arthritis may often present in sexually active young adults.
- See “Purulent gonococcal arthritis” and “Arthritis-dermatitis syndrome.”
- See “Targeted antimicrobial therapy for septic arthritis.”
In a young, sexually active adult presenting with classic symptoms of septic arthritis, gonococcal infection must be ruled out.
Diagnosis
Approach
Any red, painful joint with a reduced range of motion should be considered infectious until proven otherwise. The absence of fever does not rule out a diagnosis of septic arthritis. [6]
-
All patients [6][7][8]
- Arthrocentesis with synovial fluid analysis and culture (gold standard)
- Blood cultures in patients with fever or acute onset of symptoms
- X-rays of the affected joint
-
Suspected PJI [7]
- Diagnostic criteria for PJIs can be used alongside clinical features to establish a diagnosis. [9]
- Prompt specialist consultation is recommended (e.g., orthopedic surgery, infectious diseases).
- Advanced imaging (e.g., MRI, nuclear medicine studies) may be necessary.
- Intraoperative samples (e.g., of infected periprosthetic tissue) for culture are usually required.
-
Suspected gonococcal arthritis [10]
- Additional cultures and PCR testing of swabs from mucosal sites are recommended.
- See also “Disseminated gonococcal infection.”
Maintain a high index of suspicion for septic arthritis in patients with underlying joint diseases (e.g., osteoarthritis, rheumatoid arthritis) who present with joint pain, as the signs and symptoms of an acute flare and an infection often overlap. [6]
Arthrocentesis [11]
- Indication: : all patients with suspected septic arthritis [7]
- Procedure: See “Arthrocentesis steps.”
-
Additional considerations
- Consider specialist input prior to arthrocentesis in patients receiving anticoagulants.
- Consider inoculating synovial fluid into blood culture bottles to improve the sensitivity of cultures. [6]
Do not delay joint aspiration in suspected septic arthritis as early detection and treatment are imperative to prevent cartilage destruction. [12]
Synovial fluid analysis in septic arthritis
See “Interpretation of synovial fluid analysis” for comparative findings of differential diagnoses.
- Appearance: : often yellow-green and turbid (nonspecific) [6]
-
Cell count
- ↑ WBC count (e.g., > 50,000/mm3) [6][10]
- Neutrophil (PMN) dominance of > 90%
- Glucose levels: lower than blood glucose levels
-
Gram stain [6][10][13]
- To guide empiric antibiotic therapy for native joint infection
- A negative Gram stain does not rule out septic arthritis.
- Culture and sensitivity testing: to guide targeted antibiotic therapy [6]
Synovial fluid WBC count may be much lower in PJI than septic arthritis in a native joint. > 1,100/mm3 (≥ 64%) should raise suspicion for PJI. [10]
Neutrophil predominant leukocytosis on SFA may also be present in crystal arthropathy (e.g., acute gout flare). Interpret SFA in close conjunction with clinical features and risk factors.

Laboratory studies [6][8][10]
Routine studies
-
Blood cultures (for aerobic and anaerobic organisms)
- Obtain in patients with fever or acute onset of symptoms. [7]
- Positive in 25–50% of cases of septic arthritis and 25–70% of cases of gonococcal arthritis [10]
- CBC, CRP, ESR: Leukocytosis and elevated inflammatory markers may be seen (nonspecific).
- BMP and liver chemistries: to guide antibiotic selection [8]
Additional studies
-
Serum procalcitonin [6]
- Consider if diagnostic arthrocentesis is not feasible or in patients with comorbid inflammatory arthritis.
- Levels > 0.2–0.3 ng/mL provide supportive evidence of a bacterial infection of bones or joints.
- Coagulation panel: Perform prior to arthrocentesis in patients on anticoagulation.
- Culture and PCR testing for N. gonorrhoeae : For suspected gonococcal arthritis [10]
Uric acid levels have no diagnostic value in the evaluation of swollen joints. [8]
Inflammatory markers may be normal in septic arthritis. [10]
Imaging of the affected joint [6][10][14]
- Imaging findings of septic arthritis are nonspecific and should be interpreted in conjunction with the clinical picture.
- May be useful to evaluate for other causes of acute joint pain (e.g., fractures, osteomyelitis, chondrocalcinosis).
- Ultrasound and fluoroscopy is also useful to guide arthrocentesis in difficult joints, e.g., hip, sacroiliac joint. [14]
X-ray
- Indication: preferred initial imaging modality (prosthetic and native joints) [6][14]
-
Supportive findings
- May be unremarkable in early septic arthritis
- Soft tissue swelling, gas within periarticular soft tissue, and synovial effusion may be seen [11]
- Radiodense foreign bodies can be detected
- Osteolysis may be seen in concurrent osteomyelitis (2–3 weeks after onset). [14][15]
- Loosening of the prosthesis and periosteal reactions may be seen in PJIs.
Ultrasound
- Indication: Consider in patients with suspected foreign body (e.g., history of penetrating trauma) and negative x-rays. [14]
-
Supportive findings [14][15][16]
- Joint effusion with or without synovial thickening
- Inflammatory changes in periarticular soft tissue
- Effusions and small collections
- Can detect radiolucent foreign bodies, if present.
CT or MRI
-
Indications: Consider CT or MRI in the following situations [6][14]
- Chronic infection and/or suspected osteomyelitis
- History of penetrating trauma or suspected foreign body (as an alternative to ultrasound)
-
Supportive findings [10][14]
- Similar to ultrasound findings
- Bone marrow edema
- Can detect intra- or periarticular foreign bodies


Nuclear medicine studies (e.g., scintigraphy, PET-CT) [7][17]
- Indication: Consider in the workup of PJIs (not routinely recommended).
- Findings: focal increase in radiotracer uptake in the affected joint

Nuclear medicine studies can not distinguish between septic arthritis and inflammatory arthritis and are hence not recommended in the diagnostic workup of septic arthritis in a native joint. [14]
Diagnostic criteria for prosthetic joint infections
There are several diagnostic criteria for PJI that can be used alongside clinical features to establish a diagnosis. Clinical judgment plays an important role in determining the likelihood of PJI even in patients who do not fulfill the diagnostic criteria. [7][9]
Infectious Diseases Society of America (IDSA) diagnostic criteria for PJI (for all joints) [7]
| 2013 IDSA diagnostic criteria for PJI [7] | |
|---|---|
| Definitive PJI |
|
| High likelihood of PJI |
|
Musculoskeletal Infection Society (MSIS) for hip and/or knee PJI [9]
| MSIS diagnostic criteria for prosthetic hip and/or knee infections [9] | |
|---|---|
| Major criteria |
|
| Minor criteria |
|
| |
A diagnosis of PJI can be made even if the IDSA and/or MSIS criteria are not fulfilled. Clinical judgment based on clinical features and diagnostic findings plays an important role in determining the diagnosis. [7]
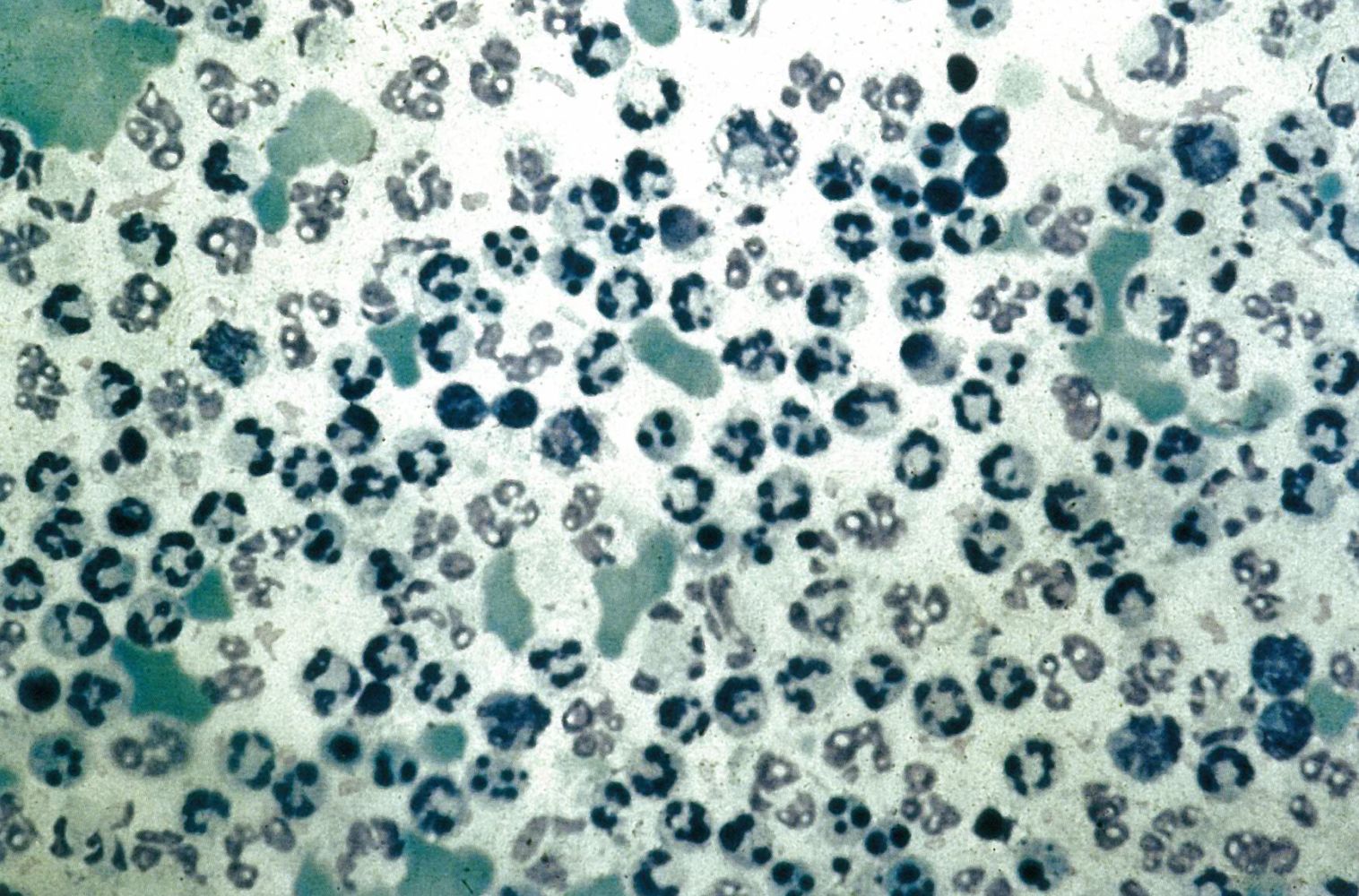
Sample of synovial fluid under light microscopy
There is a high concentration of neutrophils.
This finding suggests septic arthritis.
Source: © IMPP
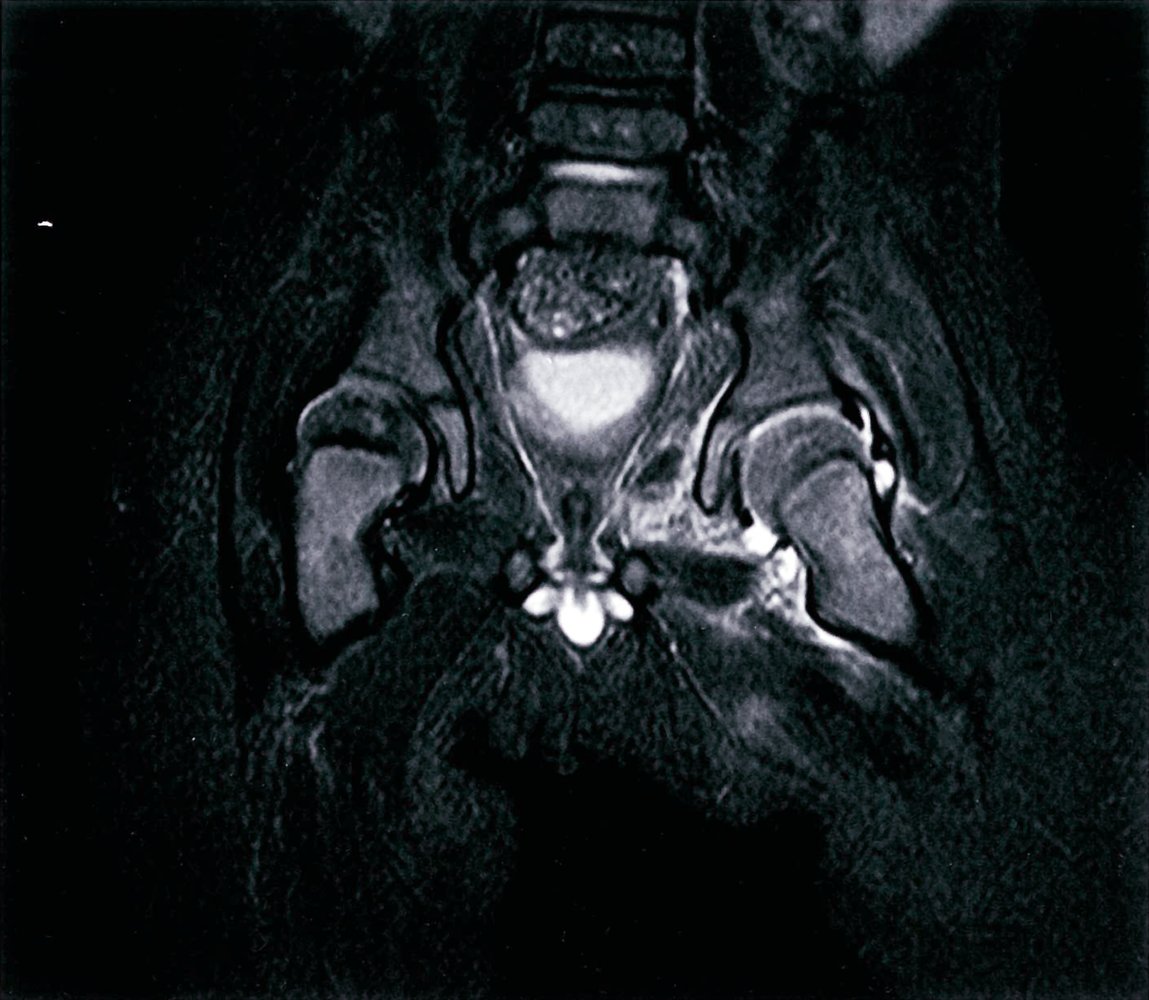
MRI pelvis (T2 fat saturated or STIR sequence, coronal plane) of an 11-month-old boy with a mildly elevated temperature and painful left hip.
There is a left-sided hip joint effusion (red overlay). The soft tissues surrounding the joint demonstrate increased signal intensity (green overlay), indicating an inflammation surrounding the septic joint.
The main differentials for these imaging findings are septic arthritis and transient synovitis. It is often very difficult to differentiate these two conditions on imaging alone during the early stages. Bone marrow edema in the femur or acetabulum, or extensive soft tissue edema around the joint is more suggestive of septic arthritis but is not always demonstrated early, and aspiration of joint fluid may be required to aid diagnosis. This is an example of septic arthritis.
Source: © IMPP

MRI Hips (axial view; T1 weighted; with contrast) of an 11-year-old boy with a painful left hip and a fever.
The synovium of the left hip is thickened and there is a joint effusion. As this is a T1-weighted image, fluid appears hypointense and therefore the effusion demonstrates hypointense signal (blue overlay). The synovium of the hip demonstrates hyperintense signal due to enhancement (green overlay). A large area of soft tissue around the left hip enhances, demonstrated as hyperintense signal around the hip joint (red overlay). This is due to inflammation of these soft tissues.
The main differentials for these imaging findings are septic arthritis and transient synovitis. It is often very difficult to differentiate these two conditions on imaging alone during the early stages. Bone marrow edema in the femur or acetabulum, or extensive soft tissue edema around the joint is more suggestive of septic arthritis but is not always demonstrated early, and aspiration of joint fluid may be required to aid diagnosis. This is an example of septic arthritis.
Outlines: Sartorius m., Rectus femoris m., Tensor fasciae latae m.
Source: © IMPP
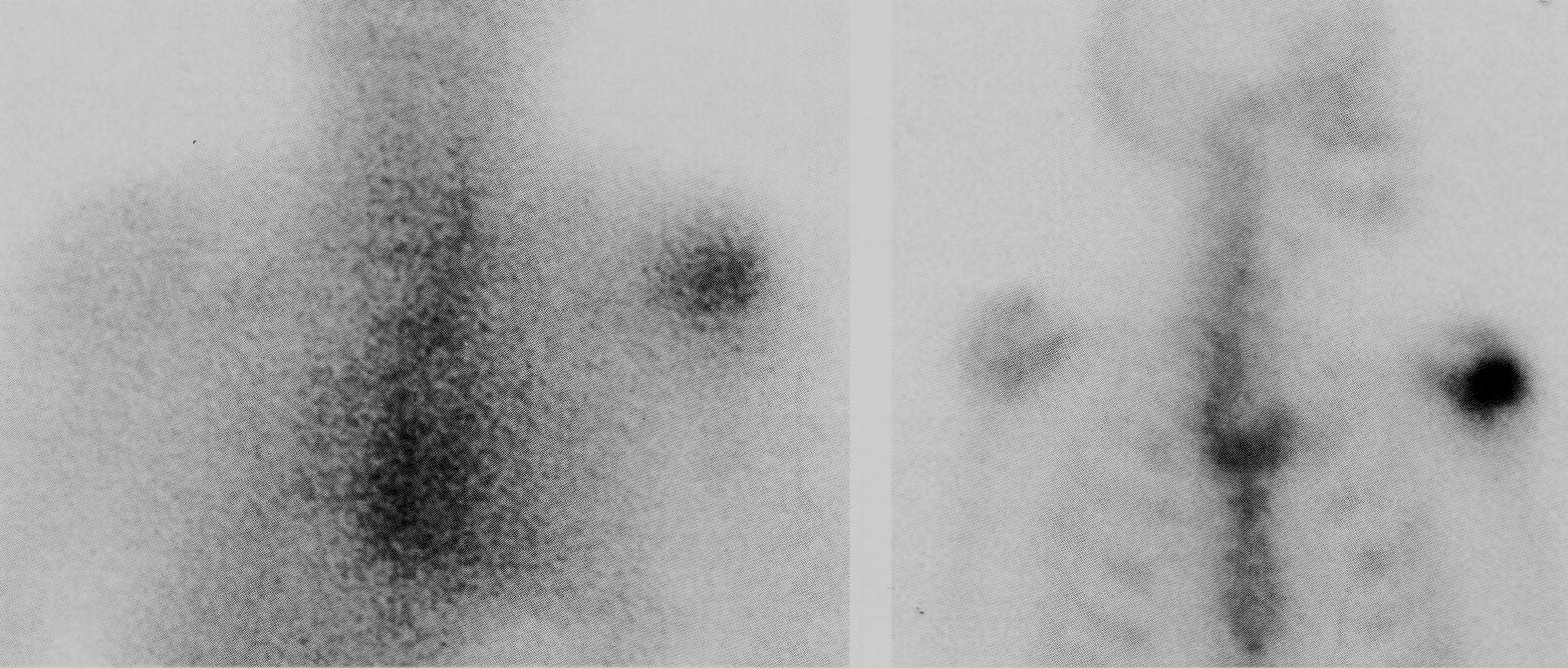
Scintigraphy: increased radionuclide activity in the left shoulder joint
Diagnosis: septic arthritis of the shoulder
Source: © IMPP
Differential diagnoses
Based on clinical features and imaging
See also “Differential diagnoses of inflammatory arthritis.”
Viral arthritis
- Etiology: parvovirus B19, hepatitis B virus, hepatitis C virus, rubella virus, HIV
-
Pathophysiology
- Direct invasion of the virus (e.g., rubella, enteroviruses)
- Immune complex formation (e.g., hepatitis B, hepatitis C, parvovirus)
-
Clinical features
- Symmetric involvement of multiple small joints
- Sudden onset
- Possibly accompanied by rash and fever
- Usually no destruction of the joint
-
Diagnostics
- History and clinical findings are the mainstays of establishing a diagnosis
- Serology: antibodies against the suspected virus
-
Synovial joint analysis
- Very variable (can be normal or inflammatory)
- Not routinely used since viral isolation is usually not successful
- For other diagnostic tests, see “Diagnostics” above.
-
Therapy
- Supportive treatment only (usually self-limited)
- See “Hepatitis B”, “Hepatitis C“, “Rubella“, “Parvovirus B19-associated arthritis”, and “HIV-associated arthritis.”
Fungal arthritis [18]
- Etiology: Histoplasma species, Sporothrix schenckii, Blastomyces species, Coccidioides species
-
Clinical features
- Very variable with acute and chronic courses
- Often with symptoms of disseminated infection (e.g., pulmonary symptoms)
-
Diagnostics
- Synovial fluid analysis may show normal, inflammatory, or septic findings
- Synovial fluid culture
- Possibly serologic studies: positive antibodies against the pathogen (e.g., in coccidioidal arthritis)
- See also: “Overview of fungal infections” in the “General mycology”
Miscellaneous
- Avascular osteonecrosis
- Bursitis
Based on synovial fluid analysis [10]
Synovial fluid analysis comprises a group of tests that examine synovial fluid to help differentiate between subtypes of arthritis.
| Interpretation of synovial fluid analysis [10] | ||||||
|---|---|---|---|---|---|---|
| Type of arthritis | Appearance | WBC count (PMN) | Gram stain | Crystals | Glucose levels (compared to blood glucose levels) | |
| No arthritis |
|
|
|
|
|
|
| Noninflammatory arthritis E.g., osteoarthritis |
|
|
|
|
|
|
| Inflammatory arthritis E.g., rheumatoid arthritis, SLE, gout, pseudogout |
|
|
|
|
|
|
| Septic arthritis [10] E.g., caused by bacterial infections |
|
|
|
|
|
|
| Lyme arthritis [23] |
|
|
|
|
|
|
| Hemarthrosis [26] E.g., caused by trauma |
|
|
|
|
|
|
The differential diagnoses listed here are not exhaustive.
Treatment
Approach
-
Native joint infection
- Serial therapeutic arthrocentesis
- Empiric antibiotic therapy guided by Gram stain and clinical features
- Targeted antibiotic therapy once antibiotic sensitivities are known
-
Prosthetic joint infection (PJI)
- Orthopedic consultation for surgical intervention (debridement with/without exchange arthroplasty)
- Infectious disease consultation for targeted antibiotic therapy once antibiotic sensitivities are known
- All patients require a prolonged course of pathogen-specific systemic antibiotics. [7]
Evacuation of purulent material from the joint and systemic antibiotic therapy are the mainstays of treatment in septic arthritis.
Joint drainage
Native joints [8]
- Therapeutic arthrocentesis (drained to dryness) is indicated in all patients.
- Repeat arthrocentesis as often as needed; SFA should be performed at each aspiration.
- Signs of improvement include a reduction in synovial fluid volume, cell count, and percentage of PMNs with each aspiration. [8][16]
-
Consider surgical drainage if symptoms persist despite serial arthrocentesis ; ; examples of surgery include: [8][10]
- Serial lavage via arthroscopy or tidal irrigation systems [16]
- Arthrotomy and open debridement [8][16]

If effusion persists beyond 7 days of arthrocentesis, arthroscopic or open drainage is indicated. [16]
Prosthetic joints [7]
Surgery to remove pus and infected tissue from the affected joint is typically required; examples include:
- Debridement of infected periarticular tissue with retention of prosthesis
- Exchange arthroplasty (e.g., one-stage exchange arthroplasty, two-stage exchange arthroplasty)
- Arthrodesis
Consult orthopedic surgery early in patients with suspected prosthetic joint infection.
Empiric antibiotic therapy
- Indication: septic arthritis of a native joint (after diagnostic arthrocentesis has been performed) [10]
-
Antibiotic coverage
- Should be guided by Gram stain results on SFA
- In patients with negative Gram stain but a high likelihood of septic arthritis, select empiric antibiotics based on clinical features and patient history.
-
Special patient groups: Consult infectious diseases for appropriate antibiotic selection in the following groups of patients. [8]
- Patients with risk factors for atypical infection
- Patients with risk factors for methicillin-resistant Staphylococcus aureus (MRSA)
- Patients at high risk for Gram-negative infections
Empiric antibiotic therapy is not routinely recommended for PJIs.
Adult patients
| Empiric antibiotic therapy for adults with septic arthritis of native joints [10][27] | ||
|---|---|---|
| Causative pathogen | Suggested regimens | |
| Gram-positive cocci |
|
|
| Gram-negative cocci |
|
|
| Gram-negative bacilli |
|
|
| Gram stain negative | Concern for gonococcal arthritis [28] |
|
| No concern for gonococcal arthritis |
|
|
Intraarticular injection of antibiotics is not recommended. [27]
Targeted antibiotic therapy
Switch from empiric antibiotic therapy to culture-specific antibiotics once antibiotic sensitivities are known in patients with native joint infections. Initiation of targeted antibiotic therapy directly (i.e., without preceding empiric therapy) is sufficient for PJI. Specialist consultation is advised especially in patients with PJIs.
Agents
| Targeted antimicrobial therapy for adults with septic arthritis (native joint infection and PJI) [7][8] | ||
|---|---|---|
| Microorganism | Example regimens | |
| Staphylococcus aureus | MSSA |
|
| MRSA |
|
|
| Enterococci | Penicillin-susceptible |
|
| Penicillin-resistant |
|
|
| Pseudomonas aeruginosa |
|
|
| Enterobacter spp. |
|
|
| Enterobacteriaceae |
|
|
| Beta-hemolytic streptococci |
|
|
| Propionibacterium acnes |
|
|
| N. gonorrhoeae [27] |
|
|
Duration of therapy [8]
The total duration of antibiotic therapy is variable and should be adjusted according to signs of clinical and laboratory evidence of improvement.
-
Native joint infections [27]
- Nongonococcal arthritis: 4–6 weeks
- Gonococcal arthritis: typically 7 days
- PJI: weeks to months
Supportive therapy
-
Acute phase
- Analgesics and immobilization for pain relief
- VTE prophylaxis as needed
- Perioperative management if surgery is indicated
- Optimal joint positioning to prevent deformation and contractures [16]
-
Following the acute phase
- Early mobilization [16][30]
- Physiotherapy
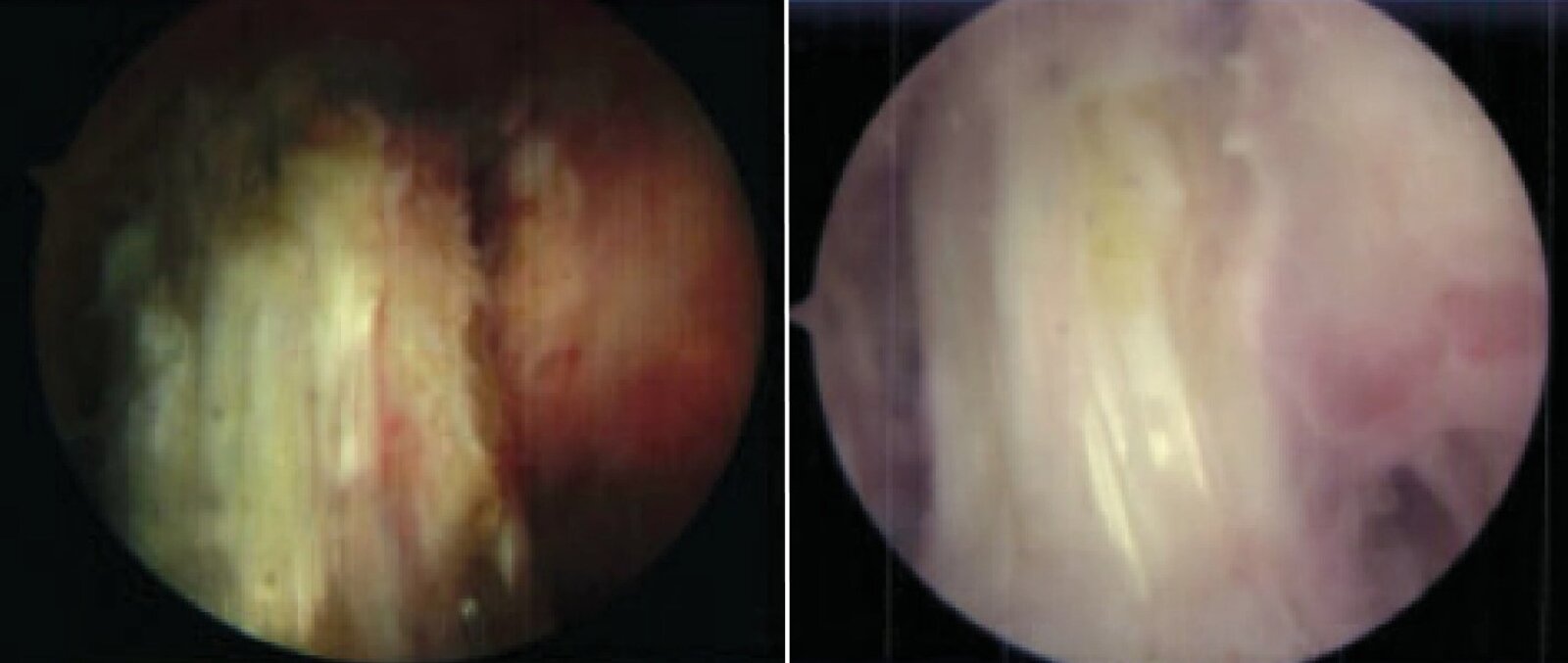
Knee arthroscopy of a 26-year-old patient with Staphylococcus lugdunensis septic arthritis after arthroscopic anterior cruciate ligament reconstruction. Three successive arthroscopies were carried out for irrigation and debridement.
Initial arthroscopy (left): hyperemia of the synovial membrane (indicating synovitis) and opacity of the synovial fluid with purulent material
Third arthroscopy (10 days later; right): reduced hyperemia, and a clear view with no purulent material
Source: “Fig. 2 and 3, in: Staphylococcus lugdunensis Septic Arthritis following Arthroscopic Anterior Cruciate Ligament Reconstruction” by Kamaci S, Bedeir YH, Utz CJ, Colosimo AJ, Hindawi, licensed under CC BY 4.0. Modifications: images combined and cropped.
Acute management checklist
Native joint infections
- Initiate empiric antibiotic therapy for septic arthritis.
- Serial therapeutic arthrocentesis
- Repeat synovial fluid analysis at each arthrocentesis to monitor response to therapy.
- Tailor antibiotics as needed once the antibiotic sensitivities are known.
Prosthetic joint infections
- Consult orthopedics for surgical intervention (e.g., debridement, exchange arthroplasty, or arthrodesis).
- Initiate pathogen-specific antibiotics once the antibiotic sensitivities are known (preferably in consultation with infectious diseases specialists)
Empiric antibiotic therapy for septic arthritis is not routinely recommended for PJIs unless the patient is critically ill.
Complications
- Joint destruction [31]
- Osteomyelitis
- Sepsis
We list the most important complications. The selection is not exhaustive.
Septic arthritis in children
Etiology [32][33]
The etiology of septic arthritis in children varies by age.
-
Infants < 6 months of age [32]
- Group B streptococci (S. agalactiae)
- Enterobacteriaceae
- Older infants and preschool children (6 months to 4 years of age)
- Kingella kingae (most common) [32][33]
- S. aureus
- Children ≥ 4 years of age
- S. aureus (most common) [32]
- Group A beta-hemolytic streptococci (S. pyogenes)
- N. gonorrhoeae (in sexually active adolescents)
Septic arthritis due to Streptococcus pneumoniae and H. influenzae type b is uncommon in highly immunized populations. [33]
Clinical features [33]
Clinical features of septic arthritis are similar in children and adults with the following additional considerations in children.
- The most common presentation is monoarthritis of the hip or knee. [33][34]
- Children may refuse to move or bear weight on the affected limb (pseudoparalysis).
- Clinical features may indicate the causative organism. [33]
- S. aureus: acute onset with rapidly progressing joint pain over 1–2 days
- K. kingae: indolent course; systemic symptoms may be absent and localizing features hard to elicit.
Diagnostics [32][33]
Approach
- In patients with sepsis or rapidly progressive infection, initiate empiric antibiotics immediately.
- Obtain routine laboratory studies and imaging.
- In patients with hip arthritis, consider prediction rules (e.g., Kocher criteria for septic arthritis) to distinguish between transient synovitis and septic arthritis.
- Refer to a specialist for arthrocentesis.
- Consider additional studies (e.g., Lyme serology) as indicated.
In patients with sepsis or rapidly progressive infection, initiate empiric antibiotics immediately, before performing synovial fluid collection and other diagnostics. [33]

Routine studies
-
Laboratory studies
- CBC: may show leukocytosis
- CRP: typically elevated
- Blood cultures [33]
-
Imaging [33][35]
- Modalities: x-ray, ultrasound, or MRI (without and with IV contrast) of the affected joint [33][35]
- Findings: See “Imaging findings of septic arthritis.”
- Follow-up: Additional imaging is required if x-rays and/or ultrasound are normal but clinical suspicion for septic arthritis persists.
-
Arthrocentesis
- Refer to a specialist for synovial fluid collection.
- Perform synovial fluid analysis in septic arthritis.
Additional studies
- Molecular testing of joint fluid for K. kingae: Consider if Gram stain or aerobic bacterial culture are negative, especially in children aged 6 months to 4 years.
- Lyme serology for features suggesting Lyme arthritis
- Culture for atypical pathogens in children with:
- Immunocompromised state
- Penetrating injuries
- Insufficient response to empiric antibiotic therapy
Differential diagnoses [23][33][35]
See also “Common causes of hip pain in children.”
- Transient synovitis
- Fractures including nonaccidental trauma
- Juvenile idiopathic arthritis
- Lyme arthritis
- Reactive arthritis
- Legg-Calvé-Perthes disease
- Slipped capital femoral epiphysis
- Acute rheumatic fever
Treatment [33]
If adjacent osteomyelitis is detected, manage accordingly; see “Osteomyelitis in children.”
Approach
- Initial treatment includes both of the following:
- Joint drainage (via arthrocentesis, arthroscopy, or arthrotomy)
- Empiric antibiotic therapy
- Switch to definitive antibiotic therapy based on culture and sensitivity results.
- Monitor for response to therapy based on clinical improvement and downtrending CRP levels.
- Poor response
- Perform MRI if not already obtained.
- Consult orthopedics for possible repeat joint drainage.
- Good response: Transition to oral antibiotics.
- Poor response
- Determine total duration of therapy in consultation with infectious diseases. [32][33]
- Typically 10–14 days
- Longer courses (up to 4 weeks) may be required if response to therapy is slow.
- Routine monitoring is not typically required after antibiotic therapy is completed.
Empiric antibiotic therapy for children with septic arthritis [33]
- Consult infectious diseases for antibiotic selection for:
- Neonates
- Suspected atypical pathogens
- Severe infection
- In adolescents, consider ceftriaxone to cover for N. gonorrhoeae. [33]
- Tailor empiric antibiotic therapy to local and/or hospital antibiograms.
| Empiric parenteral antibiotic therapy for children with septic arthritis [33] | ||
|---|---|---|
| Area prevalence of MRSA | Patient age | Recommended regimen |
| Low (≤ 10%) | 6 months to 4 years |
|
| Other ages |
|
|
| Moderate or high (> 10%) | All ages |
|
Antibiotic therapy should routinely cover S. aureus; in children aged ≥ 6 months and < 4 years, additional coverage for K. kingae is recommended. [33]
Complications [33]
- Similar to complications of septic arthritis in adults
- Growth arrest of the bone can also occur in children.
- Long-term sequelae are more common if there is adjacent osteomyelitis.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
External Resources
- 2023 PIDS/IDSA Clinical Practice Guideline on Diagnosis and Management of Acute Bacterial Arthritis in Pediatrics
- 2012 IDSA Clinical Practice Guideline on the Diagnosis and Management of Prosthetic Joint Infections
- 2011 IDSA Clinical Practice Guideline for the Treatment of MRSA Infections in Adults and Children
References
- Goldman L, Schafer AI. "Goldman-Cecil Medicine, 25th Edition". Elsevier. (2016). ISBN: 9781455750177
- Chun KC, Kim KM, Chun CH. "Infection following total knee arthroplasty.". Knee surgery & related research. 25(3). :93-9. (2013)
- Costales C, Butler-Wu SM. "A Real Pain: Diagnostic Quandaries and Septic Arthritis". J Clin Microbiol. 56(2). (2017)
- Osmon DR, Berbari EF, Berendt AR, et al. "Diagnosis and Management of Prosthetic Joint Infection: Clinical Practice Guidelines by the Infectious Diseases Society of America". Clin Infect Dis. 56(1). :e1-e25. (2012)
- Coakley G, Mathews C, Field M, et al. "BSR & BHPR, BOA, RCGP and BSAC guidelines for management of the hot swollen joint in adults". Rheumatology. 45(8). :1039-1041. (2006)
- Parvizi J, Zmistowski B, Berbari EF, et al. "New Definition for Periprosthetic Joint Infection: From the Workgroup of the Musculoskeletal Infection Society". Clin Orthop Relat Res. 469(11). :2992-2994. (2011)
- Horowitz DL, Katzap E, Horowitz S, Barilla-LaBarca ML. "Approach to Septic Arthritis". Am Fam Physician. 84(6). :653-660. (2011)
- Hansford B, Stacy G. "Musculoskeletal Aspiration Procedures". Semin Intervent Radiol. 29(04). :270-285. (2012)
- Chisolm-Straker M, Jardine L, Bennouna C, et al. "Transgender and Gender Nonconforming in Emergency Departments: A Qualitative Report of Patient Experiences.". Transgender health. 2(1). :8-16. (2017)
- Carpenter CR, Schuur JD, Everett WW, Pines JM. "Evidence-based Diagnostics: Adult Septic Arthritis". Acad Emerg Med. 18(8). :781-796. (2011)
- Expert Panel on Musculoskeletal Imaging:., Beaman FD, von Herrmann PF, et al. "ACR Appropriateness Criteria® Suspected Osteomyelitis, Septic Arthritis, or Soft Tissue Infection (Excluding Spine and Diabetic Foot)". J Am Coll Radiol. 14(5S). :S326-S337. (2017)
- Chau CLF, Griffith JF. "Musculoskeletal infections: ultrasound appearances". Clin Radiol. 60(2). :149-159. (2005)
- Shirtliff ME, Mader JT. "Acute Septic Arthritis". Clin Microbiol Rev. 15(4). :527-544. (2002)
- Seltzer A, Xiao R, Fernandez M, Hasija R. "Role of nuclear medicine imaging in evaluation of orthopedic infections, current concepts". J Clin Orthop Trauma. 10(4). :721-732. (2019)
- Gilbert, DN; Chambers, HF. "Sanford Guide to Antimicrobial Therapy 2020". Antimicrobial Therapy, Inc. (2020). ISBN: 9781944272135
- Workowski KA, Bachmann LH, Chan PA, et al. "CDC Sexually Transmitted Infections Treatment Guidelines 2021". MMWR Recomm Rep. 70(4). :1-187. (2021)
- Liu C, Bayer A, Cosgrove SE et al. "Clinical Practice Guidelines by the Infectious Diseases Society of America for the Treatment of Methicillin-Resistant Staphylococcus Aureus Infections in Adults and Children". Clin Infect Dis. 52(3). :e18-55. (2011)
- Kirchhoff C, Braunstein V, et al. "Septic arthritis as a severe complication of elective arthroscopy: Clinical management strategies". Patient Saf Surg. 3(1). :6. (2009)
- Mabille C, El Samad Y, Joseph C, et al. "Medical versus surgical treatment in native hip and knee septic arthritis". Med Mal Infect. (2020)
- Bennett JE, Dolin R, Blaser MJ. "Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases". Elsevier Saunders. (2015). ISBN: 9781455748013
- Rosenthal AK. "Crystals, inflammation, and osteoarthritis". Curr Opin Rheumatol. 23(2). :170-173. (2011)
- Richette P, Bardin T. "Gout". Lancet. 375(9711). :318-328. (2009)
- Rosenthal AK, Ryan LM. "Calcium Pyrophosphate Deposition Disease". N Engl J Med. 374(26). :2575-2584. (2016)
- Yu KH, Luo SF, Liou LB, et al. "Concomitant septic and gouty arthritis--an analysis of 30 cases.". Rheumatology (Oxford). 42(9). :1062-6. (2003)
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904
- Lantos PM, Rumbaugh J, Bockenstedt LK, et al. "Clinical Practice Guidelines by the Infectious Diseases Society of America (IDSA), American Academy of Neurology (AAN), and American College of Rheumatology (ACR): 2020 Guidelines for the Prevention, Diagnosis and Treatment of Lyme Disease". Clinical Infectious Diseases. 72(1). :e1-e48. (2020)
- Earwood JS, Walker TR, Sue GJC. "Septic Arthritis: Diagnosis and Treatment". Am Fam Physician. 104(6). :589-597. (2021)
- Long B, Koyfman A, Gottlieb M. "Evaluation and Management of Septic Arthritis and its Mimics in the Emergency Department". West J Emerg Med. 20(2). :331-341. (2019)
- Tande AJ, Patel R. "Prosthetic joint infection". Clin Microbiol Rev. 27(2). :302-345. (2014)
- Betts RF, Chapman SW, Penn RL. "Reese and Betts' A Practical Approach to Infectious Diseases". Lippincott Williams & Wilkins. (2002). ISBN: 9780781732819
- Berry DJ, Lieberman J, Keeney J. "Surgery of the Hip". Elsevier Saunders. 2(1). (2013). ISBN: 9780443069918
- Hachem A, Copley LAB. "What’s New in Pediatric Septic Arthritis? A Review of Pertinent Clinical Questions". J Pediatr Orthop. 43(9). :578-583. (2023)
- Woods CR, Bradley JS, Chatterjee A, et al. "Clinical Practice Guideline by the Pediatric Infectious Diseases Society (PIDS) and the Infectious Diseases Society of America (IDSA): 2023 Guideline on Diagnosis and Management of Acute Bacterial Arthritis in Pediatrics". J Pediatric Infect Dis Soc.. 13(1). :1-59. (2023)
- Committee on Infectious Disease, American Academy of Pediatrics. "Red Book: 2024-2027 Report of the Committee on Infectious Diseases, 33rd Edition". American Academy of Pediatrics. (2024). ISBN: 9781610027373
- Shet NS, Iyer RS, Chan SS, et al. "ACR Appropriateness Criteria® Osteomyelitis or Septic Arthritis-Child (Excluding Axial Skeleton)". J Am Coll Radiol. 19(5). :S121-S136. (2022)