Summary
Sexually transmitted infections (STIs) are a group of infections that are primarily transmitted via sexual intercourse and intimate physical contact. Some of the most common STIs include HPV infection, chlamydia infection, and gonorrhea. Urethral or vaginal discharge, painful or painless genital lesions, and pelvic pain are the most common presenting symptoms in symptomatic patients. Patients with an active STI have an increased risk of coinfection with additional STIs. In addition to treating the patient, simultaneous treatment of the partner is often necessary to prevent recurrent infections. Regular STI screening in adults is recommended since affected individuals are frequently asymptomatic.
This article provides an overview of the diagnosis and management of undifferentiated STIs and details on screening for STIs in asymptomatic individuals. See the respective articles for details on specific diseases.
Overview
Overview of STIs
See respective articles for details and dosages.
| Overview of sexually transmitted infections [1] | ||
|---|---|---|
| Pathogens | Associated disease | Management |
| Viral pathogens | ||
| Human papillomavirus |
|
|
| Herpes simplex virus type 2 (HSV-2) |
|
|
| HIV |
|
|
| Hepatitis B virus (HBV) |
|
|
| Monkeypox virus [3] |
|
|
| Bacterial pathogens | ||
| Chlamydia trachomatis D–K |
|
|
| Chlamydia trachomatis L1–L3 |
|
|
| Klebsiella granulomatis |
|
|
| Haemophilus ducreyi |
|
|
| Mycoplasma genitalium |
|
|
| Neisseria gonorrhoeae |
|
|
| Treponema pallidum |
|
|
| Parasitic pathogens | ||
| Trichomonas vaginalis |
|
|
| Phthirus pubis |
|
|
| Sarcoptes scabiei |
|
|
")

")


Overview of genital lesions caused by STIs [1]
The most common causes of genital ulcers in the United States are genital herpes and syphilis. [1]
| Overview of sexually transmitted genital lesions | ||
|---|---|---|
| Solitary | Multiple | |
| Painful |
|
|
| Painless |
|
|
Consider a noninfectious etiology (e.g., trauma, psoriasis, fixed drug eruptions, Wegener granulomatosis, Behcet syndrome) if a pathogen is not detected on diagnostics. [1][5]








")

")



Photograph of the perianal region of a child with HIV (image rotated: gluteal cleft runs from upper right to lower left of image)
Multiple flesh-colored papules with a folded irregular surface have formed a plaque in the perianal region.
Immunodeficiency (e.g., due to HIV infection) increases both the risk of HPV infection becoming symptomatic (in this case with anogenital warts) and the severity of symptoms
Source: “Figure 31, In: Atlas of Paediatric HIV Infection” by Regina E. Oladokun, Rannakoe J. Lehloenya, Carol Hlela et.al., Openbooks, licensed under CC BY-ND 4.0.

Labia majora of an immunocompetent patient with an infiltrative and eroded tumor (arrow)
Multiple flat and hyperpigmented patches are disseminated over the patient's upper labia majora.
These patches suggest Bowenoid papulosis, caused by human papillomavirus (HPV) infection.
Source: “Fig 7A, In: Update on human papilloma virus - part I: epidemiology, pathogenesis, and clinical spectrum” by Magela Magalhães G, Vieira EC, Campos Garcia L, de Lourdes Ribeiro De Carvalho-Leite M, Martins Guedes AC, Grossi Araújo M, ABD, licensed under CC BY 4.0. Modifications: image cropped.
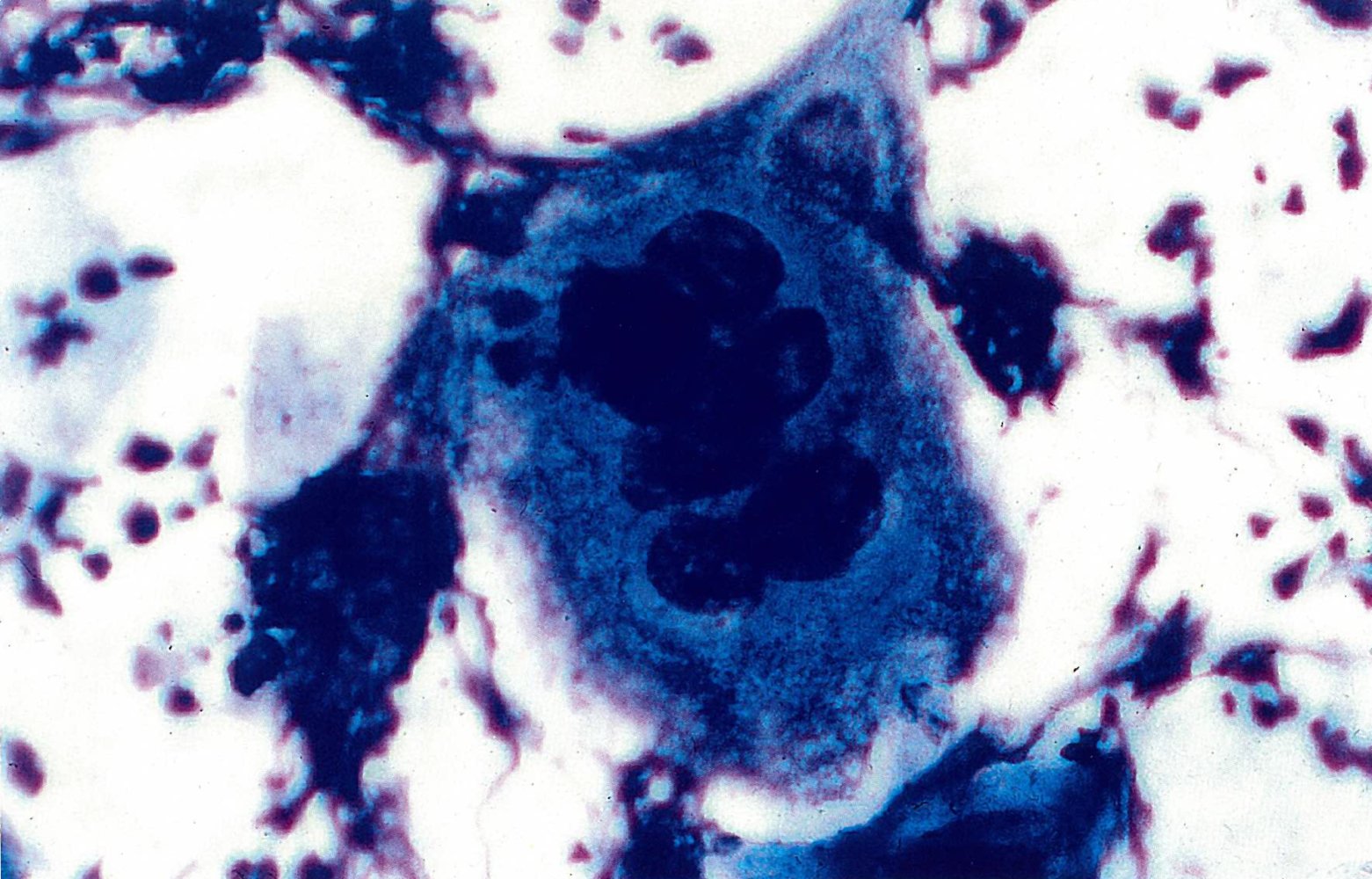
Exudate smear (Giemsa stain)
Coccobacilli are visible as inclusion bodies within macrophages (Donovan bodies). In some cases, the characteristic safety pin shape can be seen (examples indicated by arrowheads).
Source: “SOA-Donovanosis” by GerardM, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
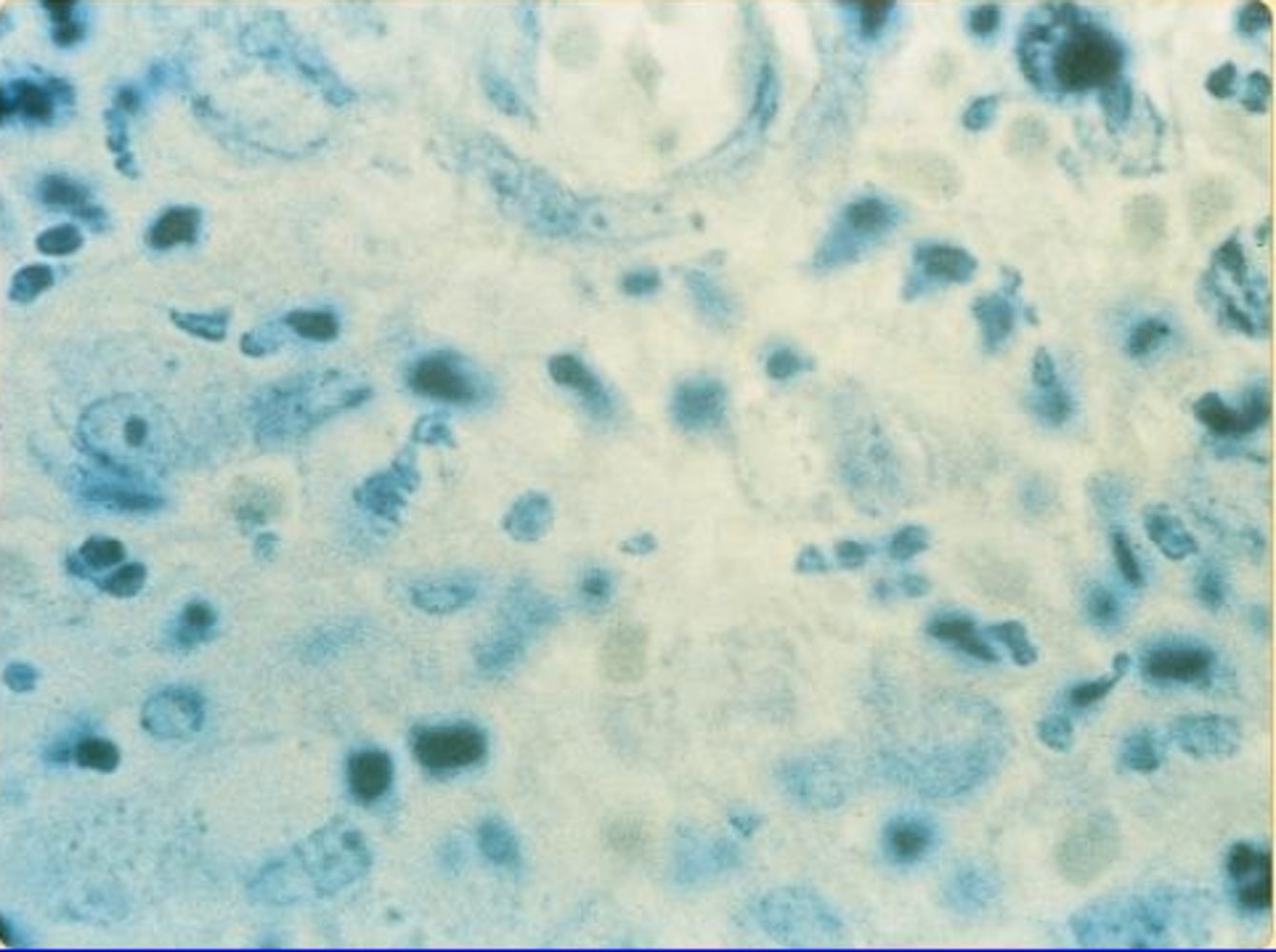
Photomicrograph of a smear from the base of a herpetic (HSV-1) gingivostomatitis lesion (Pappenheim stain; very high magnification)
A multinucleated giant cell (Tzanck cell) can be seen, indicating a positive Tzanck test.
Source: © IMPP
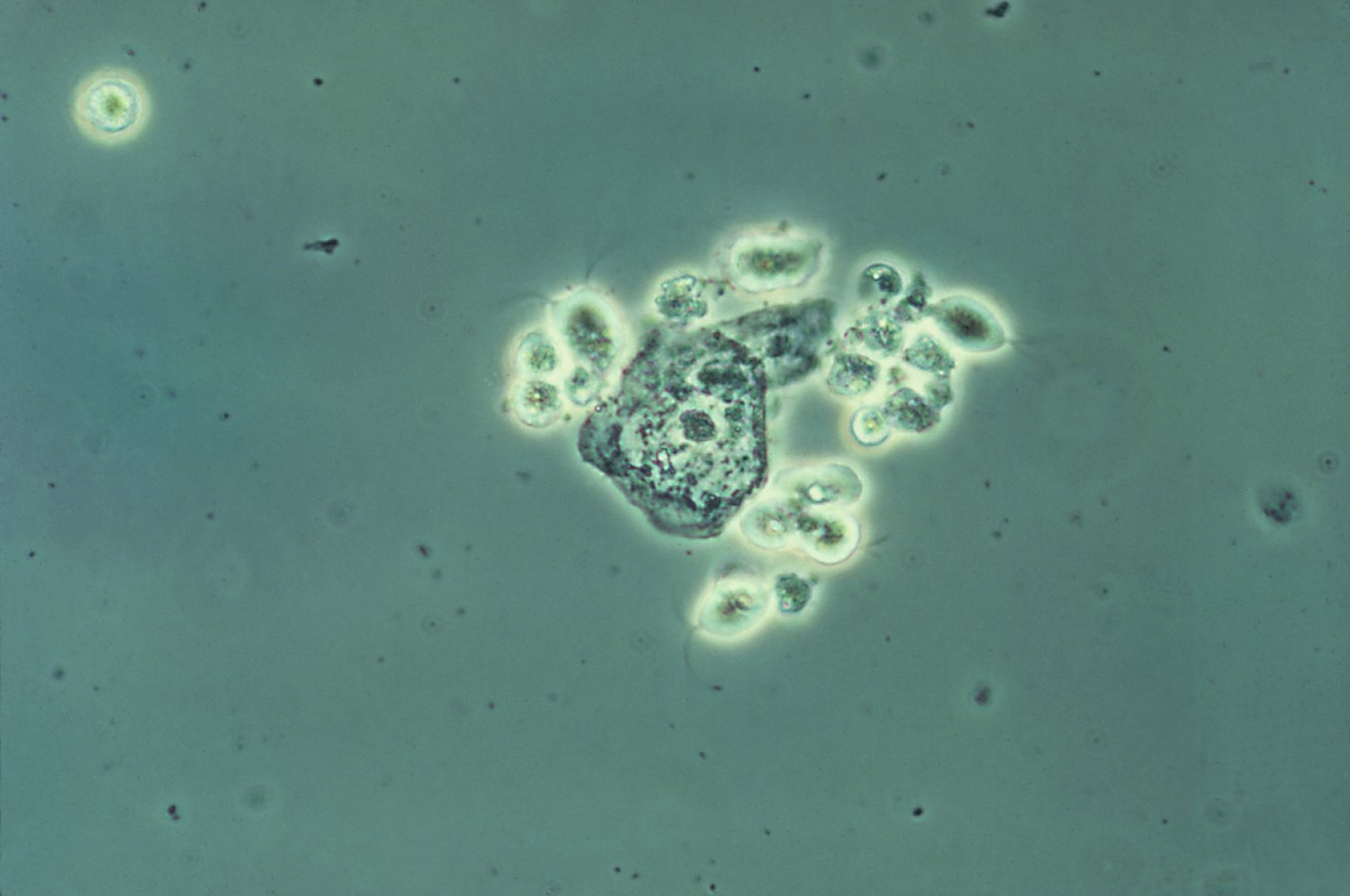
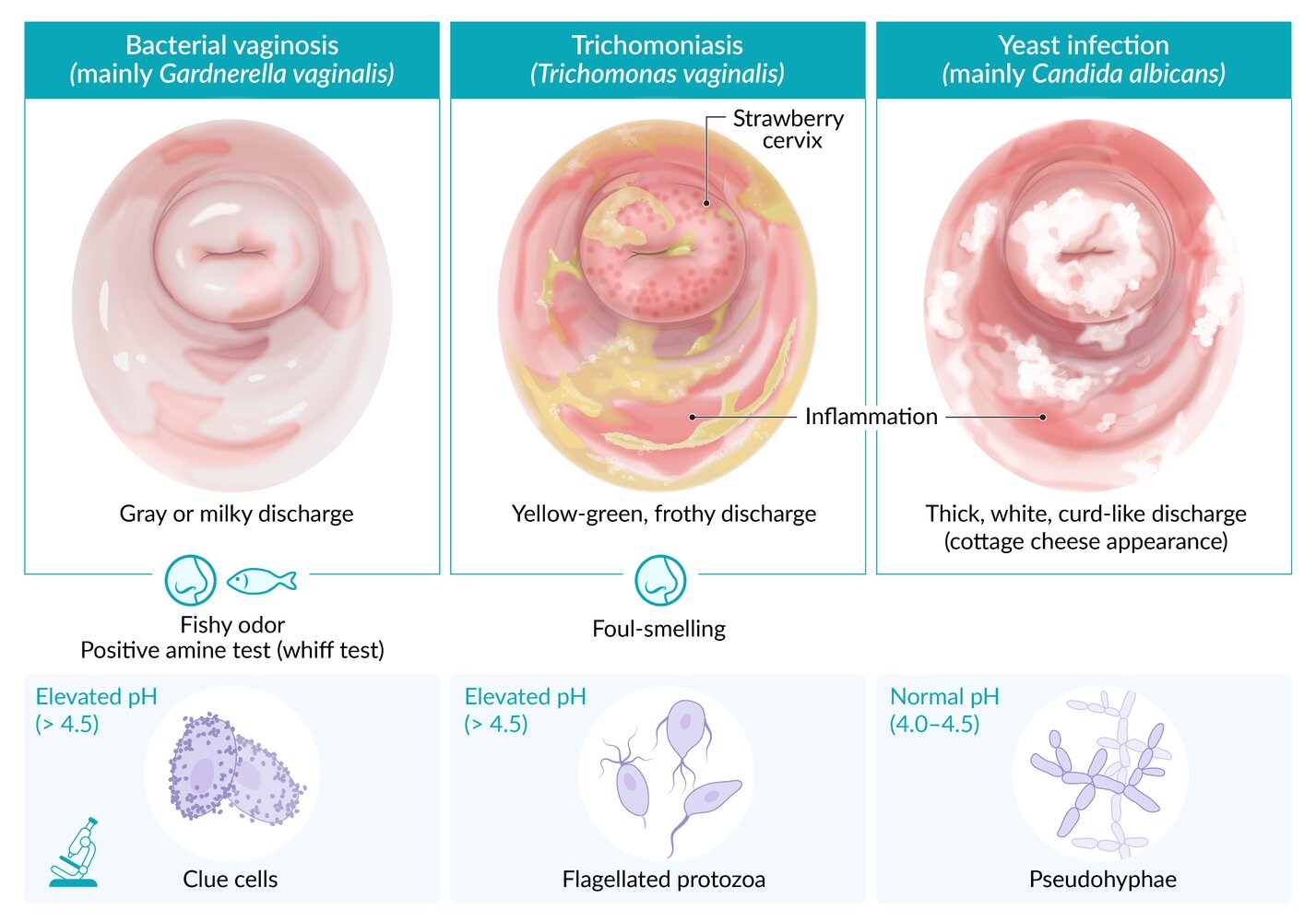
Phase contrast photomicrograph of vaginal discharge (high magnification)
These parasites with flagella (blue overlay) are Trichomonas vaginalis, the causative pathogen of trichomonal vaginitis.
In the center, two squamous epithelial cells can be seen.
Source: "ID#: 5238", CDC, Centers for Disease Control and Prevention (CDC) licensed under Public Domain

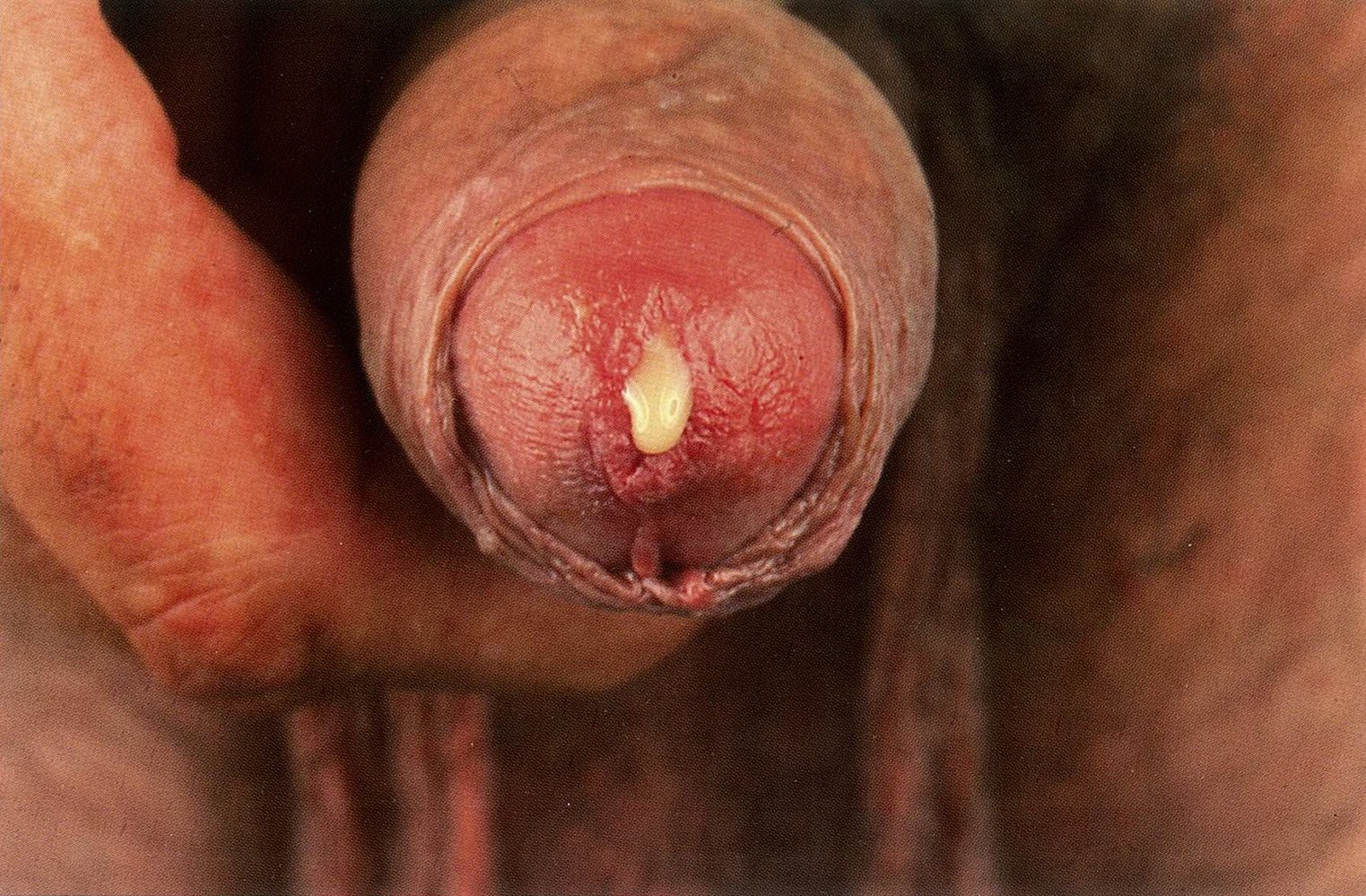
There is an ulcer with an erythematous margin on the corona of the glans penis. This is a characteristic chancroid lesion, which is caused by Haemophilus ducreyi infection.
Source: "ID#: 3728", CDC/ Joe Miller, Centers for Disease Control and Prevention (CDC) licensed under Public Domain

The entire genital area appears erythematous with an inflamed vaginal vestibule and urinary meatus. Solitary erythematous papules are visible inside the labia minora. Furthermore, there are white purulent lesions in the vaginal introitus.
These findings are consistent with genital herpes, most likely caused by infection with herpes simplex virus type 2.
Source: "#16968", CDC/ Dr. Wiesner, Public Health Image Library licensed under Public Domain

Penile shaft and glans
Two ulcerated blisters with erythematous margins are visible proximal to the corona of the glans.
Source: "#15822", CDC/ Susan Lindsley, CDC licensed under Public Domain

Disseminated mpox rash
There are numerous well-defined papules and vesiculopustules, some of which are umbilicated.
Note that different stages of the rash can be present simultaneously.
Source: "Figure 1, in: Imported Monkeypox from International Traveler, Maryland, USA, 2021", ostello V, Sowash M, Gaur A, Cardis M, Pasieka H, Wortmann G, et al., Centers for Disease Control and Prevention licensed under Public Domain

Mpox rash on different patients
Umbilicated vesiculopustules are visible on the right dorsal penis (A) and the left tip of the tongue and right chin (C). An ulcer is seen on the anus (B). All lesions have erythematous margins. The lesion on the right chin (C) also shows central crusting.
Source: “Fig 2, In: Monkeypox: From A Neglected Tropical Disease to a Public Health Threat” by Antunes F, Cordeiro R, Virgolino A, MDPI, licensed under CC BY 4.0. Modifications: image cropped & insertion of Lato letters A, B, C.

A superficial ulcer with indurated borders is visible on the glans penis.
This finding is consistent with primary syphilis.
Source: "Primary stage syphilis sore (chancre) on glans (head) of the penis.", Unknown, Centers for Disease Control and Prevention (CDC), National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention licensed under Public Domain

Perianal region of a female patient with Klebsiella granulomatis infection
Multiple confluent, partially ulcerated papules are visible.
Diagnosis was confirmed via visualization of darkly staining Donovan bodies in biopsy crush preparations.
Source: "ID#: 15433", CDC/ Joe Miller, Centers for Disease Control and Prevention licensed under Public Domain

A small, shallow ulcer is visible on the shaft of the penis (arrow).
This lesion is suggestive of early LGV caused by Chlamydia trachomatis infection.
Source: "#18035", CDC/ Dr. Pirozzi, CDC licensed under Public Domain

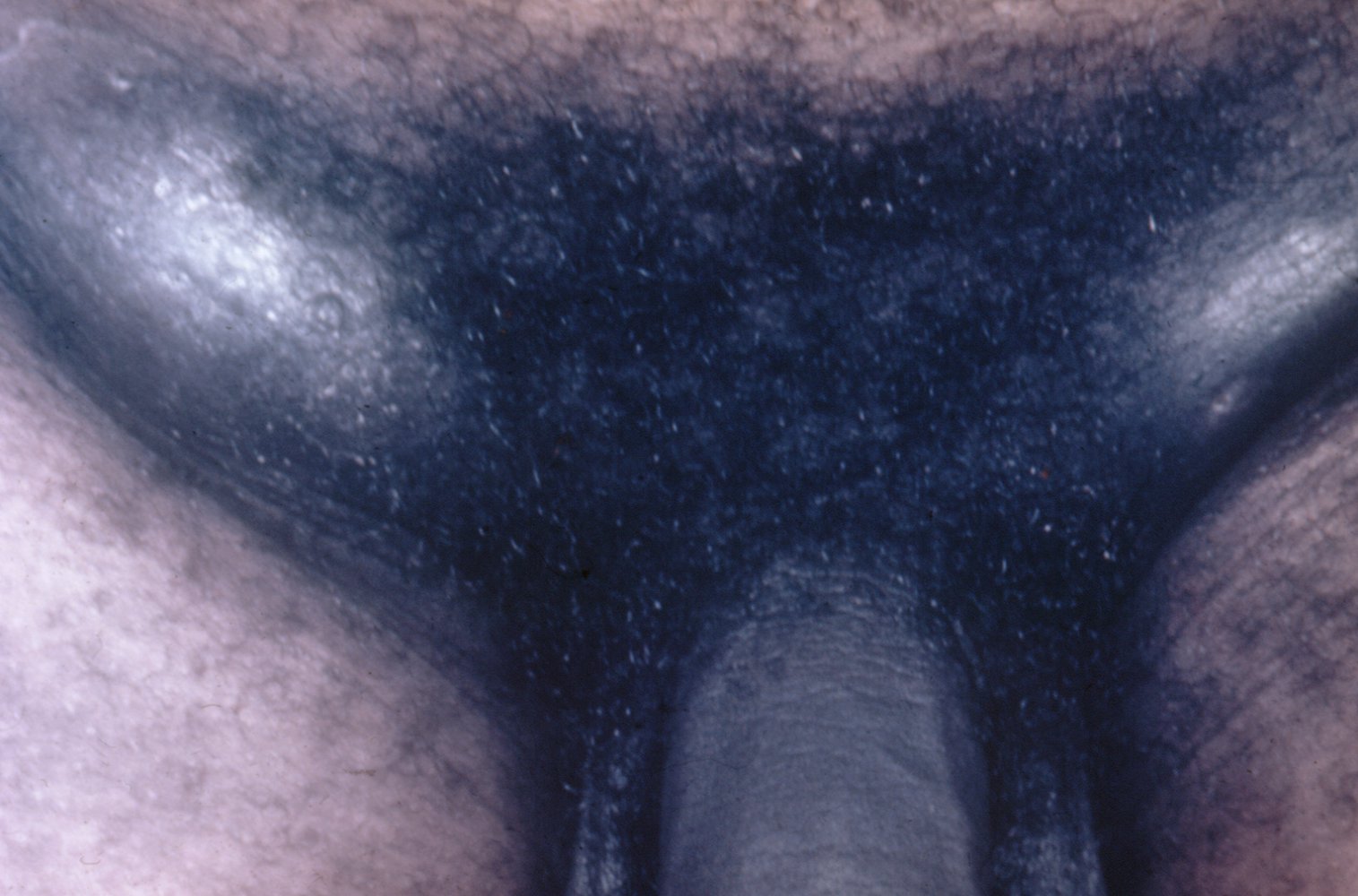
Bilateral enlargement of the inguinal lymph nodes above and below the inguinal ligament is visible (groove sign).
The groove sign is characteristic of lymphogranuloma venereum, which is caused by acute Chlamydia trachomatis infection.
Source: “Case 10, in: Images of Memorable Cases: 50 Years at the Bedside” by Hendrik A. van Dijk, Herbert L. Fred, MD, openstax cnx, licensed under CC BY 2.0.

Multiple exophytic, cauliflower-like, confluent, erythematous lesions are visible in the perianal region.
Source: © IMPP

Broad-based papular erosions are visible around this patient's anus.
Clustering around the anus and the typical appearance are suggestive of condylomata lata, a sign of secondary syphilis.
Source: © IMPP

Several discrete, broad-based, papular erosions are visible on the glans penis.
These findings suggest condylomata lata, a cutaneous feature seen in secondary syphilis.
Source: © IMPP
There is massive bilateral swelling of inguinal lymph nodes. The skin above the lymph nodes is livid. The causative agent is Haemophilus ducreyi.
Source: "ID#: 5811", Susan Lindsley, Centers for Disease Control and Prevention (CDC) licensed under Public Domain
Risk factors
- Sexually active individuals < 25 years of age
- Inconsistent condom use
- Current STI or an STI in the past year
- Multiple sexual partners
- New sexual partner
- Partner with an STI or at high risk for an STI
- Men who have sex with men
- History of incarceration
- Exchanging sex for drugs or money
- IV drug use
- Individuals who request STI testing
Management
- The following sections detail the initial approach to evaluate suspected STIs; hepatitis B virus infection and HIV infection are detailed separately in their respective articles.
- Evaluate for child sexual abuse in children with STIs occurring beyond the neonatal period and before adolescence.
- An approach to undifferentiated symptoms that are unlikely to be caused by STIs is not covered here.
- See “Screening for STIs” for details on evaluating asymptomatic individuals for STIs.
Clinical evaluation
- Obtain a thorough sexual history to determine STI risk factors.
- Evaluate for signs of STI (e.g., lesions, discharge, lymphadenopathy, or tenderness):
- Perform a physical examination.
- Additionally, in women:
- Perform an abdominal and pelvic examination, ideally including a speculum examination (even in patients with neovaginas).
- Assess for diagnostic criteria for PID; if present, initiate empiric antibiotic therapy for PID.
- Patients with rectal symptoms or increased risk of anal cancer: Perform a rectal examination and anoscopy.
- Consult urology, gynecology, and/or infectious disease specialists for complicated STIs.
Ask about nonconsensual sexual encounters and assess for signs of human trafficking. When appropriate, refer patients to health care professionals with training in further examination and management as needed (see “Management of recent sexual assault”).
Some patient groups (survivors of previous sexual assault, transgender individuals) may find workup for STIs more distressing than others. Use a trauma-informed approach, consider allowing a friend or partner to be present, and reassure them that the exam may be stopped at any time. [9]
Diagnostics
- Collect appropriate swabs or first-void urine samples for microscopy and/or nucleic acid amplification testing (NAAT).
- Test for the most likely causative organism based on patient history and examination findings.
- See the table below for initial diagnostic tests.
- See the respective articles for further details.
- Routinely offer HIV testing and syphilis testing to all individuals with a suspected STI. [8]
- Perform a pregnancy test in women.
Provider-collected or self-collected swabs should be obtained from all sites of exposure (e.g., rectum, oropharynx, vagina, urethra) as needed. [1]
| Symptom-based STI diagnostics [1][8] | |
|---|---|
| Recommended diagnostics | |
| Men with urethral discharge, dysuria, or scrotal pain |
|
| Women with abnormal vaginal discharge |
|
| Women with pelvic pain and/or dyspareunia |
|
| Patients with genital and anorectal ulcers |
|
| Patients with anogenital warts [1] |
|
|
Patients with genital itching (suspected ectoparasitic infestation) [8] |
|

In patients with anogenital warts, testing for HPV infection is not recommended, as results are not specific and do not alter management. [1]
Syphilis serology interpretation is complex. Follow syphilis testing algorithms to reduce the risk of false-positive and false-negative results. [1]
All cases of syphilis, gonorrhea, chlamydia, chancroid, hepatitis, mpox, and HIV must be reported to the state health department for surveillance. Reporting of other STIs varies by state. [1]
© AMBOSS
Treatment
Approach [1][8]
-
Offer treatment to all patients with suspected STIs on the day of presentation.
- Same-day results available: Provide tailored treatment (see “Pathogen-specific management”).
- Same-day results not available: Offer empiric treatment; tailor treatment when results are available.
- Trace and treat partners if possible: See “Management of sexual partners.”
- Counsel patients on how to reduce the risk of STIs: See “Prevention of STIs.”
- Offer postexposure prophylaxis for STIs to eligible patients.
- If STI testing is negative, evaluate for less common causative pathogens and non-STI etiologies.
Empiric management of STIs
| Symptom-based management for STIs [1][8] | |
|---|---|
| Clinical presentation | Empiric management |
| Urethral discharge |
|
| Vaginal discharge | |
| Cervicitis (on speculum examination) | |
| Pelvic pain |
|
| Anorectal pain and/or discharge |
|
| Anogenital ulcers |
|
| Anogenital warts |
|



Genital herpes and syphilis are the most common causes of anogenital ulcers in the United States. [1][8]
Chancroid and granuloma inguinale (donovanosis) are rare in the United States. If there is diagnostic uncertainty or genital ulcers persist, immediately refer patients to centers with experience diagnosing and treating chancroid, granuloma inguinale, and LGV. [1][8]
Pathogen-specific management
Tailored antimicrobial therapy and additional management steps may be required depending on the pathogen identified, e.g.:
- See “Management of gonorrhea.”
- See “Management of genitourinary chlamydia.”
- See “Treatment of syphilis.”
- See “Treatment of HSV infection.”
- See “Treatment of hepatitis B.”
- See “Treatment of HIV.”
Follow-up [1]
- Patients with chlamydia, gonorrhea, and/or trichomoniasis:
- Most patients: Screen for repeat infection after 3 months of treatment.
- Obtain test of cure for patients with:
- Ongoing symptoms
- Nonadherence to treatment
- Pharyngeal gonorrhea
- Chlamydia infection during pregnancy
- Patients with syphilis: See “Posttreatment assessment for syphilis.”
Source: © IMPP

Purulent discharge can be seen on this patient's vulva on external genital examination.
Source: “SOA-gonorroe-female” by SOA-AIDS Amsterdam, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}

Colposcopy view of the ectocervix
The ectocervix is erythematous and there is purulent discharge from the external os.
Source: “SOA-Chlamydia-trachomatis-female” by GerardM, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}
Management of sexual partners
Bacterial STI
Contact tracing [1]
- Encourage patients with STIs to notify their sexual partners and have them seek clinical evaluation and appropriate treatment (except if there is a risk for intimate partner violence).
- Trace all sexual partners within the past 60 days (even if asymptomatic) OR the most recent sexual partner if last sexual contact was > 60 days ago.
- If timely evaluation and treatment of sexual partners seems unlikely: Offer expedited partner therapy. [1][11]
Sexual partners must be treated simultaneously to avoid reinfections. [1]
Expedited partner therapy (EPT) [1]
EPT is the treatment of sexual partners of patients with STIs without a preceding clinical examination or diagnostic test. Prescriptions are given to the index patient to pass on to their sexual partners (i.e., patient-delivered partner therapy).
-
EPT is recommended for all sexual partners of patients with gonorrhea and/or chlamydia if the partner is unlikely to seek medical evaluation.
- EPT for gonorrhea only (i.e., chlamydia has been ruled out in the index patient): cefixime [1]
- EPT for chlamydia only (i.e., gonorrhea has been ruled out in the index patient): doxycycline
- EPT for gonorrhea and chlamydia: cefixime PLUS doxycycline [1]
- Provide written information on medications for EPT and educational materials on STI symptoms, complications, and prevention strategies.
Offer HIV testing to partners of all patients diagnosed with STIs. Offer HIV PrEP to individuals at very high risk of contracting HIV. [1]
Routinely offer EPT (if permitted by local law) to patients diagnosed with chlamydia and/or gonorrhea if it seems unlikely that their partner will seek timely medical care. See “Tips and Links” for the CDC page detailing which states permit EPT. [1]
Prevention of onward transmission of a bacterial STI [1]
Advice patients to avoid unprotected (condomless) sex until the following criteria are met:
- Completion of 7-day treatment regimen OR 7 days have passed since a single-dose treatment.
- All symptoms have resolved.
- Any current sexual partners have also met the above criteria.
Viral STIs [12][13]
-
Contact tracing
- Contact all sexual partners and other individuals who may have been at risk.
- Determine the appropriate period for contact tracing based on the pathogen-specific window period and the date of the patient's last documented negative test, if available. [12]
- Offer recent contacts post-exposure prophylaxis for STIs.
- Advise isolation precautions as needed. [14]
- Treat identified infections; see respective articles for details.
- Avoid unprotected sex in infected patients and during the window period for exposed patients.
- Educate patients on the prevention of STIs.
Prevention
Reduction in the risk of infection [1][7]
Behavioral counseling
See “Counseling on sexual health and contraception” for details.
- Consistent condom use (internal or external ) during vaginal sex or anal sex
- Dental dam use during oral sex
- Mutual monogamy
- Reducing the number of sex partners
- STI testing of new sexual partners
- Abstinence
- Prevention of spread via fomites (e.g., contaminated sex toys)
Obtain a sexual history, assess for risk factors for STIs, and offer behavioral counseling to prevent or minimize the risk for STIs for all sexually active adolescents and adults at increased risk for STIs. [7][15]
")
Preexposure prophylaxis for STIs
- All patients: Vaccination against HPV, HBV, and HAV (see “ACIP immunization schedule” for details)
- Individuals at high risk for mpox infection: mpox immunization
- Individuals at very high risk of HIV infection: HIV PrEP
Routinely offer HIV PrEP to individuals at very high risk of HIV infection. [15]
Postexposure prophylaxis for STIs (PEP) [1][16]
Offer PEP to individuals who have been recently exposed to an STI.
- HIV PEP: for sexual contacts within the past 72 hours. [12][15][17]
- Hepatitis B PEP: Follow guidance for HBV PEP following nonoccupational exposure for contacts within the past 14 days. [13]
- Mpox PEP: Offer to all sexual contacts within 4 days of exposure; consider for patients within 4–14 days to reduce infection severity. [3]
-
Antibiotic prophylaxis
- Offer to all individuals who have experienced sexual assault (see “STI prophylaxis” in “Management of recent sexual violence”). [1]
- Offer a single dose of doxycycline (off-label) within 72 hours of unprotected sex for MSM and transgender women with ≥ 1 bacterial STI in the past 12 months [18]
- Offer emergency contraception for patients at risk of pregnancy.
Prevention of onward transmission [1]
- Recommend adherence to screening guidelines for STIs.
- Remove barriers to STI testing, for example, by offering self-testing.
- Where possible, provide EPT.
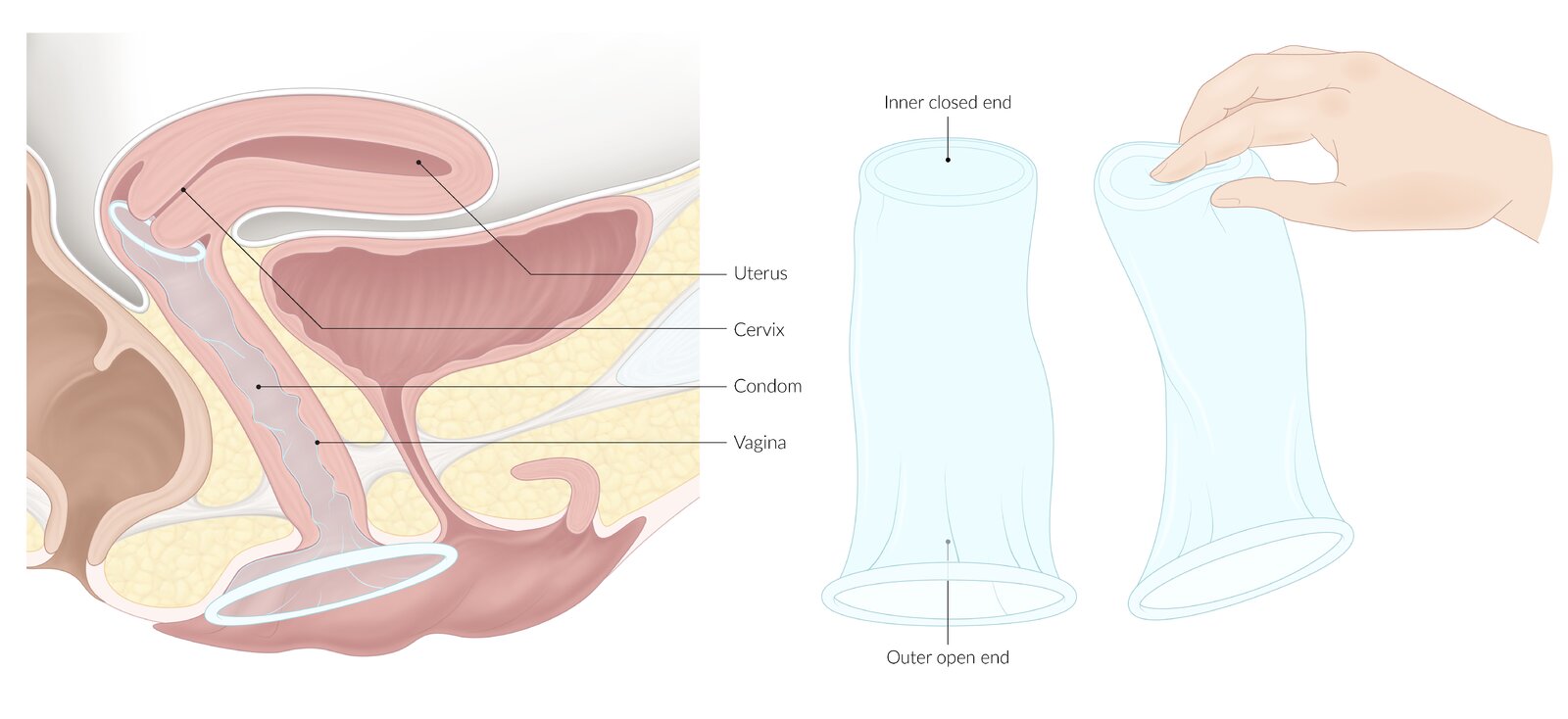
The smaller closed inner ring is placed within the vagina, the larger open-ended outer ring rests outside the vagina on the perineum.
© AMBOSS
Screening for STIs
The following information is an overview of STI screening; for more detailed information, see the respective disease articles.
General principles [1]
- STI screening recommendations should be tailored to the individual, considering the presence of risk factors.
- Any individual should receive STI screening if they request it, regardless of risk factors.
- For patients with a positive screening test, offer testing and treatment for partners (see “STI management of sexual partners”).
- Screening is an opportunity to educate individuals on STI prevention.
First-line screening tests [1]
- HIV screening: fourth-generation HIV test (combination HIV antigen/antibody immunoassay)
- Hepatitis B screening: triple panel including HBsAg, anti-HBc antibody, and anti-HBs antibody
- Hepatitis C screening: anti–HCV antibody
- Chlamydia screening and gonorrhea screening: NAAT (using samples from all sites of exposure)
- Syphilis screening: syphilis testing algorithms
- Trichomonas screening: NAAT and/or wet mount
The combination of self-swabs and a first-void urine sample allows for screening of most STIs and avoids the need for an intimate examination, which may deter individuals from seeking care. [19][20]
Routine serological screening for herpes simplex virus 2 in asymptomatic individuals is not recommended. [1][21]
Screening recommendations [1]
| STI screening by population [1] | |
|---|---|
| Population | Recommended screening |
| Women |
|
| Men who have sex with women |
|
| Men who have sex with men |
|
| Transgender and nonbinary individuals |
|
| Individuals with HIV |
|
| Pregnant individuals |
|
| Adolescents |
|
Related One-Minute Telegram
- One-Minute Telegram 101-2024-1/3: New CDC guidelines: doxy PEP for bacterial STI prevention
- One-Minute Telegram 90-2024-3/3: PEP challenges amid rising STIs
- One-Minute Telegram 70-2023-2/3: USPSTF reaffirms: Do not screen asymptomatic patients for HSV!
Interested in the newest medical research, distilled down to just one minute? Sign up for the One-Minute Telegram in “Tips and links” below.
External Resources
- 2024 CDC Clinical Guidelines on the Use of Doxycycline Postexposure Prophylaxis for Bacterial Sexually Transmitted Infection Prevention
- 2021 CDC Sexually Transmitted Infections Treatment Guidelines
- 2021 CDC Quick Guide for STI Treatment
- 2021 WHO Guidelines for the Management of Symptomatic STIs
- 2020 AFP Article on Differential Diagnosis and Management of Genital Ulcers
- USPSTF Overview of STI Screening and Behavioral Counselling
- CDC Page on Legal Status of Expedited Partner Therapy in the United States
- Sign up for the One-Minute Telegram
References
- Workowski KA, Bachmann LH, Chan PA, et al. "CDC Sexually Transmitted Infections Treatment Guidelines 2021". MMWR Recomm Rep. 70(4). :1-187. (2021)
- "Guidelines for the management of symptomatic sexually transmitted infections". https://www.who.int/publications/i/item/9789240024168. [2021-07-15]
- Bates CK, Carroll N, Potter J. "The Challenging Pelvic Examination". Journal of General Internal Medicine. 26(6). :651-657. (2011)
- Peng WS, Tan C. "Bowenoid papulosis in a linear distribution". Postepy Dermatol Alergol. 2. :146-148. (2016)
- "Monkeypox". https://web.archive.org/web/20220816192021/https://www.cdc.gov/poxvirus/monkeypox/about.html. [2022-07-22]
- Rao AK, Schrodt CA, Minhaj FS, et al. "Interim Clinical Treatment Considerations for Severe Manifestations of Mpox — United States, February 2023". MMWR Morb Mortal Wkly Rep. 72(9). :232-243. (2023)
- Roett MA. "Genital Ulcers: Differential Diagnosis and Management". Am Fam Physician. 101(6). :355-361. (2020)
- Krist AH, Davidson KW, et al. "Behavioral Counseling Interventions to Prevent Sexually Transmitted Infections". JAMA. 324(7). :674. (2020)
- Hsu KK, Rakhmanina NY. "Adolescents and Young Adults: The Pediatrician’s Role in HIV Testing and Pre- and Postexposure HIV Prophylaxis". Pediatrics. 149(1). (2021)
- Mayer KH, Traeger M, Marcus JL. "Doxycycline Postexposure Prophylaxis and Sexually Transmitted Infections". JAMA. (2023)
- "Updated guidelines for antiretroviral postexposure prophylaxis after sexual, injection drug use, or other nonoccupational exposure to HIV—United States, 2016". https://web.archive.org/web/20230511171545/https://stacks.cdc.gov/view/cdc/38856. [2016-04-18]
- Centers for Disease Control and Prevention (CDC). "Recommendations for partner services programs for HIV infection, syphilis, gonorrhea, and chlamydial infection.". MMWR Recomm Rep. 57(RR-9). :1-83; quiz CE1-4. (2008)
- Schillie S, Vellozzi C, Reingold A, et al. "Prevention of Hepatitis B Virus Infection in the United States: Recommendations of the Advisory Committee on Immunization Practices". MMWR Recomm Rep. 67(1). :1-31. (2018)
- Bachmann LH, Barbee LA, Chan P, et al. "CDC Clinical Guidelines on the Use of Doxycycline Postexposure Prophylaxis for Bacterial Sexually Transmitted Infection Prevention, United States, 2024". MMWR Recomm Rep. 73(2). :1-8. (2024)
- Guarner J, del Rio C, Malani PN. "Monkeypox in 2022—What Clinicians Need to Know". JAMA. 328(2). :139. (2022)
- "Legal Status of Expedited Partner Therapy (EPT)". https://web.archive.org/web/20220411171724/https://www.cdc.gov/std/ept/legal/default.htm
- "Mpox: Isolation and Infection Control At Home". https://web.archive.org/web/20240318015232/https://www.cdc.gov/poxvirus/mpox/clinicians/infection-control-home.html
- Serlin M, Shafer MA, Tebb K, et al. "What Sexually Transmitted Disease Screening Method Does the Adolescent Prefer?". Archives of Pediatrics & Adolescent Medicine. 156(6). :588. (2002)
- Chongsuwat T, Cody PJ. "At-Home Self-Collection of Urine or Vaginal Samples for Gonorrhea and Chlamydia Screening Among Young People Who Were Assigned Female at Birth". AJPM Focus. 2(4). :100138. (2023)
- Mangione CM, Barry MJ, et al. "Serologic Screening for Genital Herpes Infection". JAMA. 329(6). :502. (2023)
- Owens DK, Davidson KW, et al. "Screening for HIV Infection". JAMA. 321(23). :2326. (2019)