Summary
Short stature (dwarfism) in children is defined as a height that is at least two standard deviations (SDs) below the mean for children of the same age and sex. In adults, the condition is commonly defined as a height of 5 ft 1 in (155 cm) or less in men and 4 ft 10 in (147 cm) or less in women. Nonpathological variant short stature can be classified into three types: familial short stature (inherited short stature), constitutional delay of growth and puberty (an inherited pattern of short stature during childhood that is followed by a growth spurt during puberty, typically resulting in normal adult height), and idiopathic short stature (short stature in the absence of any metabolic, endocrine, or other diagnosis). These types of short stature are most often normal variants of growth and rarely affect a child's development beyond longitudinal growth. The pathological causes of short stature are diverse and include psychosocial circumstances as well as a variety of genetic, endocrine, and metabolic disorders, which may affect a child's development in other ways than longitudinal growth. Further diagnostic testing is indicated if a child's growth is less than what might be expected given the average height of the parents. An x-ray of the left hand and wrist are made to determine bone age (skeletal age), based on which the adult size of the child can be predicted. Laboratory testing can help rule out any underlying condition. Treatment is rarely indicated in nonpathological short stature (e.g., if short stature does not represent a disability to the patient), while pathological short stature is treated according to the underlying condition and usually involves growth hormone supplementation.
Definitions
-
Short stature (dwarfism)
- Children: height of > 2 SDs below the mean for children of the same age, sex, and similar genetic background
- Adults: height of ≤ 4 ft 10 in (147 cm) for women and ≤ 5 ft 1 in (155 cm) for men [1]
-
Proportionate short stature
- Limbs proportionate to trunk
- Seen in most cases of familial short stature
-
Disproportionate short stature
- Limbs disproportionately short compared to trunk
- Seen mostly in cases of skeletal dysplasia
- Growth failure: growth rate below the rate considered appropriate for sex and age.
")
")
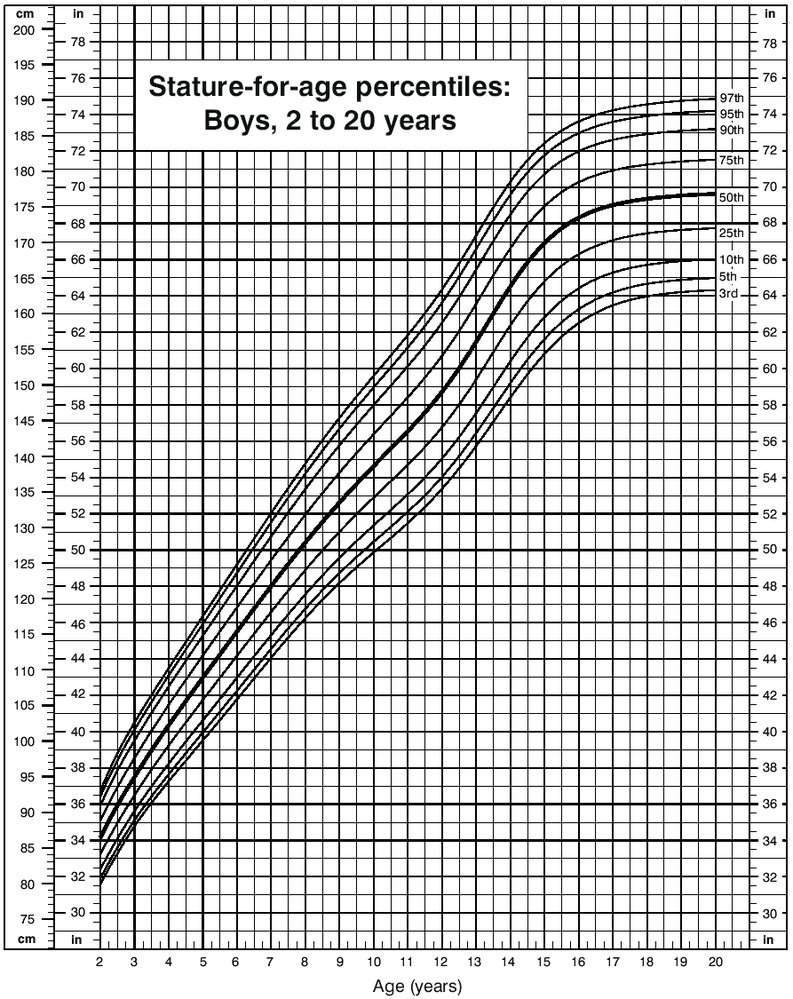
Source: "Figure 11, in: 2000 CDC Growth Charts for the United States: Methods and Development", Kuczmarski RJ, Ogden CL, Guo SS, et al., Centers for Disease Control and Prevention licensed under Public Domain
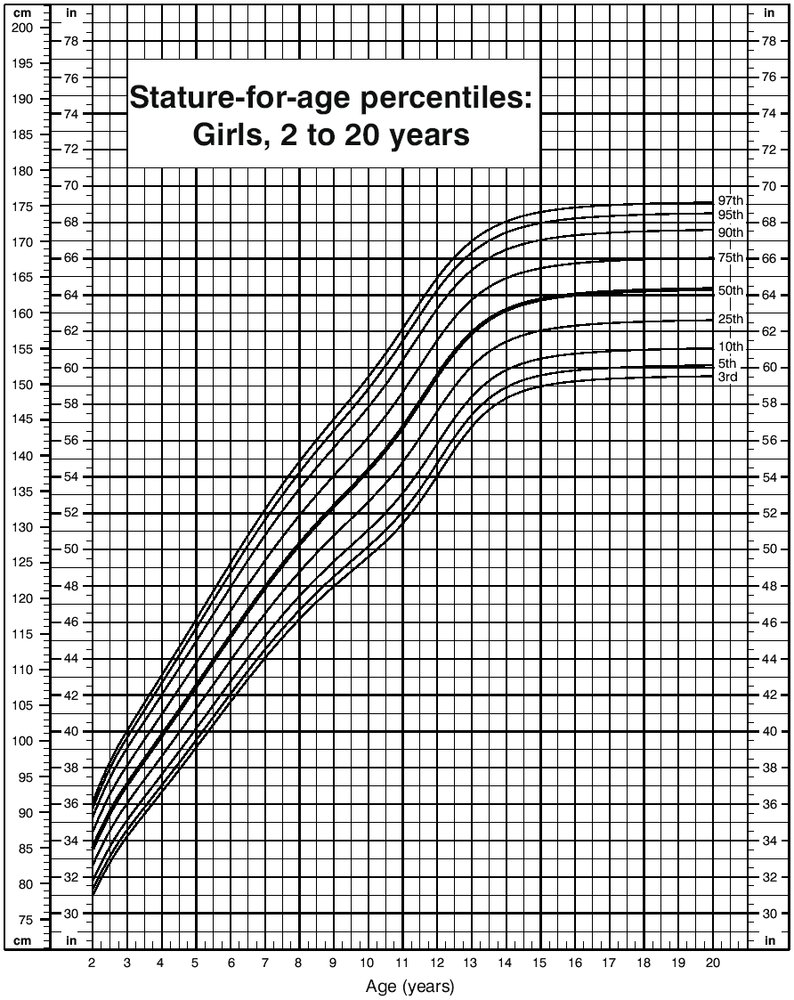
Source: "Figure 12, in: 2000 CDC Growth Charts for the United States: Methods and Development", Kuczmarski RJ, Ogden CL, Guo SS, et al., Centers for Disease Control and Prevention licensed under Public Domain
Causes of short stature
Short stature can have a variety of genetic, systemic, and psychosocial causes.
-
Genetic causes include:
- Constitutional growth delay
- Laron syndrome
- Turner syndrome
-
Systemic causes include:
- Congenital hypothyroidism
- GH deficiencies
- Glucocorticoid excess
-
Psychosocial causes include:
- Maternal substance use (e.g., alcohol)
- Psychosocial short stature
- Psychiatric conditions (e.g., anorexia nervosa)
Genetic causes of short stature
| Genetic causes of short stature | |||
|---|---|---|---|
| Condition | Underlying cause | Characteristics | |
| Nonpathological variant short stature | |||
| Familial short stature |
|
|
|
| Constitutional growth delay |
|
|
|
| Idiopathic short stature |
|
|
|
| Pathological short stature | |||
| Laron syndrome |
|
|
|
| Skeletal dysplasias |
|
|
|
| Turner syndrome |
|
|
|
| Down syndrome |
|
|
|
| Williams syndrome |
|
|
|
| Cystic fibrosis |
|
|
|
| Pseudohypoparathyroidism (Albright hereditary osteodystrophy) |
|
|
|
| McCune-Albright syndrome |
|
|
|
Systemic causes of short stature
| Systemic causes of short stature | ||
|---|---|---|
| Condition | Underlying cause | Characteristics |
| Endocrine disorders | ||
| Congenital hypothyroidism |
|
|
| GH deficiencies |
|
|
| Congenital adrenal hyperplasia |
|
|
| Glucocorticoid excess |
|
|
| Type 1 diabetes mellitus |
|
|
| Rheumatological diseases | ||
| Juvenile idiopathic arthritis |
|
|
| Renal disorders | ||
| Chronic kidney disease (CKD) |
|
|
| Fanconi syndrome |
|
|
| Metabolic disorders | ||
| Rickets |
|
|
| Gastrointestinal disorders | ||
|
Celiac disease/ Inflammatory bowel disease |
|
|
| Chronic oxygen deficiency | ||
| Congenital heart defects |
|
|
| Anemias |
|
|
| Immunological diseases | ||
| HIV infection |
|
|
| Severe combined immunodeficiency |
|
|
| Other causes of short stature | ||
| Neoplasms |
|
|
Behavioral and psychosocial circumstances of short stature
| Psychosocial causes of short stature | ||
|---|---|---|
| Condition | Underlying cause | Characteristics |
| Maternal substance use |
|
|
| Psychosocial short stature |
|
|
| Anorexia nervosa |
|
|
Diagnosis
Patient history
- Physical examination findings
- Growth rate
- Family history of short stature
-
Midparental height (estimated adult height of a child calculated on the basis of parental height), calculated via the following formula:
- ♀ = [mother's height in cm + (father's height in cm - 13)]/2
- ♂ = [father's height in cm + (mother's height in cm + 13)]/2
Laboratory tests
- CBC, differential blood count, ESR
- Thyroid function tests (see “Hypothyroidism”)
- Renal function tests and urinalysis (in case of CKD and associated renal osteodystrophy)
- Screening for GH deficiency (see “Hypopituitarism”)
- Hormone profile (LH, FSH, estrogen/testosterone) for puberty status assessment
- Karyotyping
Imaging tests
- X-ray: : used to determine an individual's bone age and height by comparing their x-ray images of the nondominant hand and wrist to those displayed in the standard bone development atlas
- Cranial MRI: in suspicion of hypothalamic or pituitary tumors
Treatment
Management depends on the underlying cause:
- Reassurance that low height is a normal variant (e.g., familial short stature) that does not require treatment
- Discontinuation of growth-inhibiting medication (e.g., glucocorticoids)
- Sex hormone substitution in children with delayed puberty and growth
- GH supplementation (e.g., somatropin) in cases of GH deficiency, idiopathic short stature, and Turner syndrome
- In case of primary severe IGF-1 deficiency: mecasermin (recombinant insulin-like growth factor)
- Treatment of underlying conditions (see “Causes of short stature” above)
References
- "Dwarfism". https://www.mayoclinic.org/diseases-conditions/dwarfism/symptoms-causes/syc-20371969. [2018-08-17]