Summary
In shoulder dislocation, the head of the humerus dislocates completely or partially (subluxation) in one of three directions: anterior (most common), posterior, or inferior. Shoulder dislocation is usually the result of trauma, and, because the head of the humerus is substantially larger than the glenoid fossa, it is the most common type of joint dislocation. Typical symptoms include pain and restricted range of motion. Examination reveals a palpable dent in the shoulder caused by the empty glenoid fossa, while the head of the humerus may be palpable anterior or inferior to the glenoid fossa. X-rays of the shoulder in at least two views are necessary to rule out fractures and confirm the diagnosis. With adequate analgesia and muscle relaxation, the head of the humerus can be carefully repositioned into the glenoid fossa through various maneuvers. Reduction is followed by immobilization and subsequent rehabilitation. Patients with concomitant soft tissue lesions or recurrent shoulder dislocation may require surgery to stabilize the shoulder joint. Possible complications of shoulder dislocation include neurovascular damage (most commonly axillary nerve injury), continued instability, restricted range of motion, and rotator cuff injury.
For details on closed reduction techniques for anterior shoulder dislocations, see “Shoulder reduction.”
Epidemiology
- Most common joint dislocation
- Sex: ♂ > ♀ [1]
- Peak incidence: 20–29 years of age [1]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
- Anatomy: The head of the humerus is larger than the shallow glenoid fossa, which accounts for the high incidence of shoulder dislocation.
- Trauma (e.g., falling on an outstretched arm): commonly associated with contact sports [1]
-
Predisposing factors for recurrent shoulder dislocation
- Rotator cuff tear
- Damage to the glenohumeral ligament
- Bankart lesion and Hill-Sachs lesion
- Loose joint capsule
- For posterior dislocation: uncoordinated muscle contraction (e.g., seizure, electrical shock)
Classification
- Anterior shoulder dislocation: displacement of the humeral head anterior (and often also inferior) to the glenohumeral fossa (> 95% of cases) [2][3]
- Posterior shoulder dislocation: displacement of the humeral head posterior to the glenohumeral fossa (< 4% of cases) [4]
- Inferior shoulder dislocation: displacement of the humeral head inferior to the glenohumeral fossa (< 1% of cases) [5]
 after a fall from a ladder")
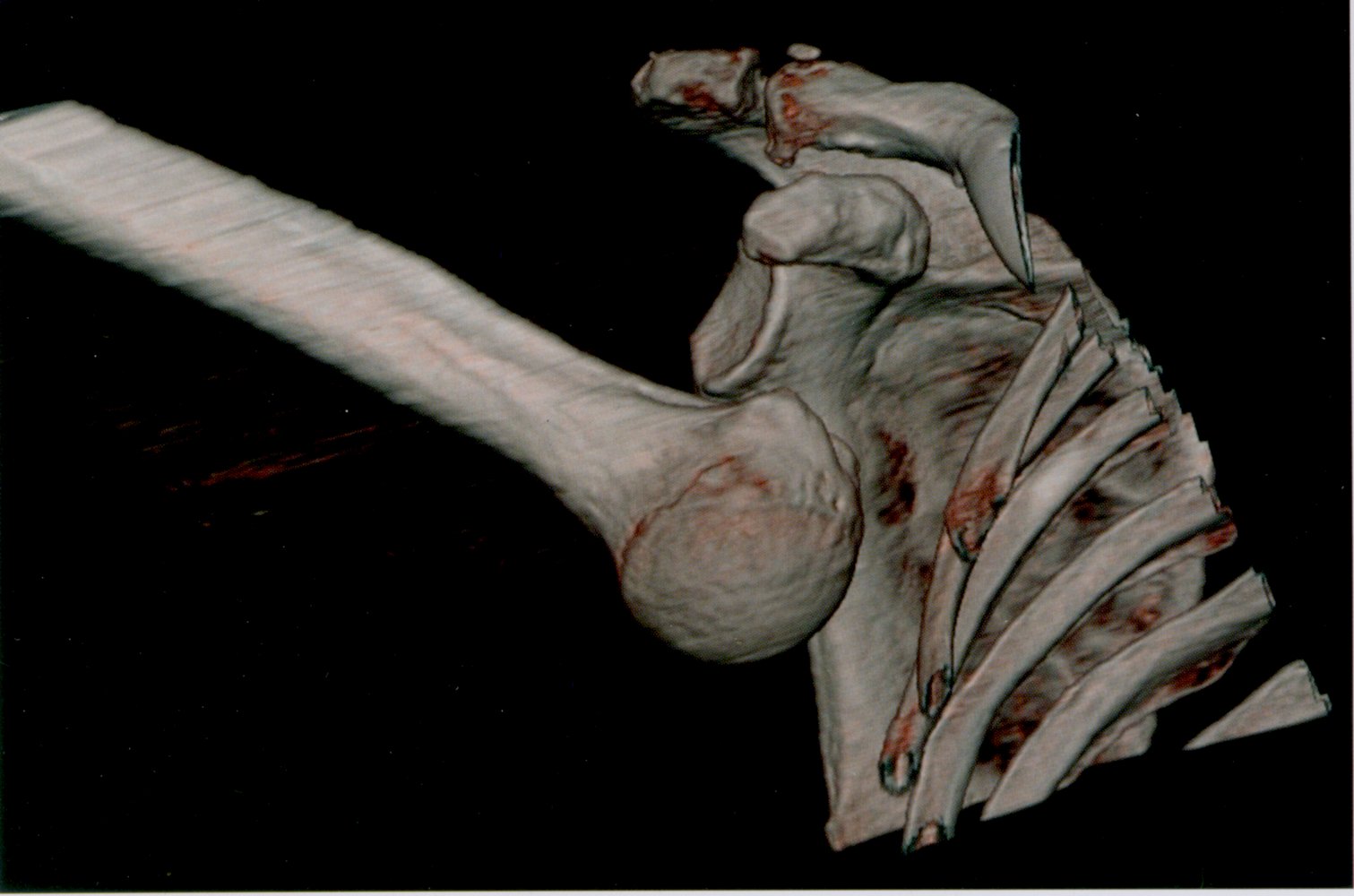
3-D CT reconstruction of the right shoulder joint
The humeral head is displaced ventrally and caudally. The arm is abducted by 120° and cannot be adducted.
Source: © IMPP
Clinical features
-
General symptoms
- Severe shoulder pain
- Resistance to shoulder and arm movement
- Empty glenoid fossa: A palpable or visible dent may be present where the humeral head is expected.
-
Anterior shoulder dislocation [2][3]
- Arm typically held in abduction and slight external rotation (limited adduction)
- Humeral head palpable below the coracoid process
- Loss of shoulder contour: prominent acromion and flattening of the deltoid muscle
-
Posterior shoulder dislocation [4]
- Arm held in adduction and internal rotation (limited external rotation)
- Prominent coracoid process with anterior soft tissue flattening
- Humeral head not palpable [6]
-
Inferior shoulder dislocation [5]
- Arm held in fixed abduction at ∼ 125° (limited adduction)
- Humeral head may be palpable in axilla
- Elbow typically held in flexion with a pronated forearm
- Axillary nerve injury may be present.
Posterior shoulder dislocation is frequently overlooked during clinical examination. [7]




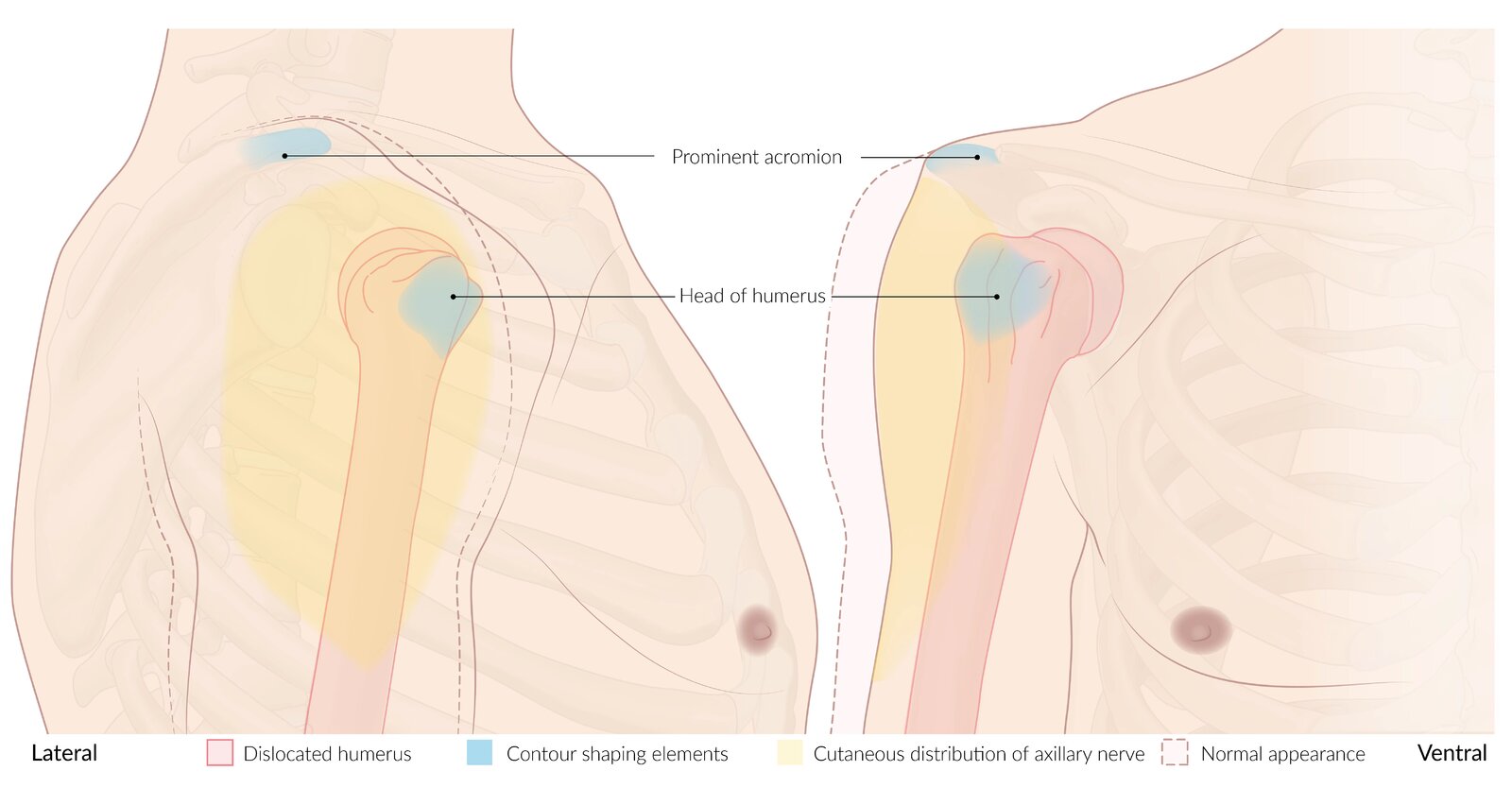
Lateral and ventral view of the right shoulder
The dashed line shows the normal position and the solid red line shows the pathological position that occurs with anterior dislocation. Axillary nerve palsy is a known complication of both shoulder dislocation and reduction. Axillary nerve function should be evaluated before and after attempting reduction, by testing sensation over the lateral surface of the shoulder (yellow overlay).
© AMBOSS
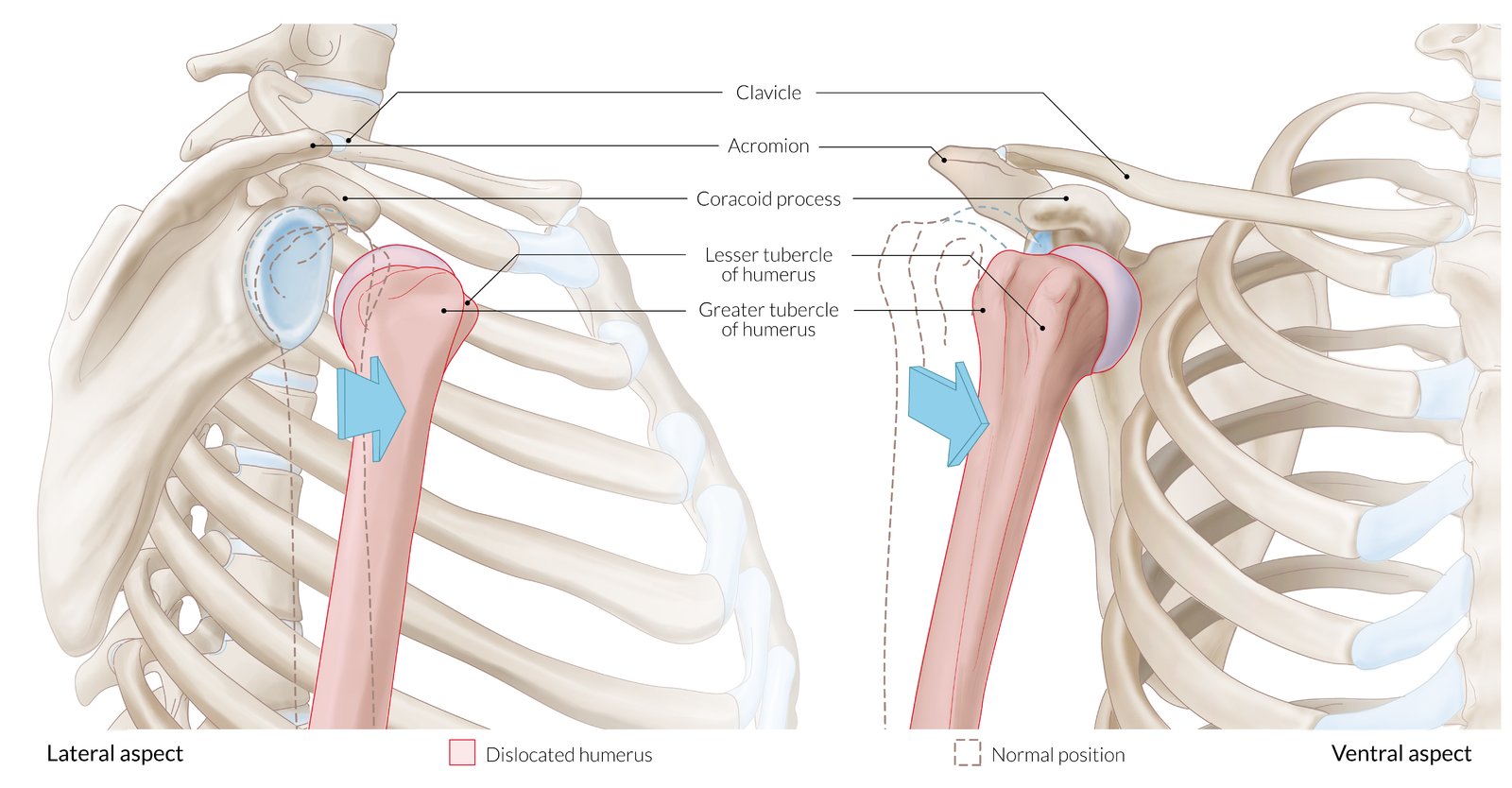
Lateral and ventral view of the right shoulder
The dashed line shows the normal position and the solid red line shows the pathological position that occurs with anterior dislocation.
© AMBOSS
© AMBOSS

The arm is held in ∼120° abduction with the elbow flexed and the forearm pronated.
This is the typical presentation of inferior shoulder dislocation. Patients are unable to adduct the arm, and the humeral head may be palpable in the axilla.
Source: © IMPP
Diagnosis
Clinical evaluation [3][6]
Signs of neurovascular injury or fracture-dislocation on clinical examination should prompt urgent orthopedic consultation.
- Assess for signs of a fracture (e.g., concomitant humerus fracture).
-
Conduct a neurovascular examination to identify: [6]
- Axillary nerve palsy
- Brachial plexus injury
- Radial nerve palsy
- Median nerve palsy
- Ulnar nerve palsy
- Recurrent uncomplicated anterior shoulder dislocation can be diagnosed clinically. [8]
The risk of concomitant fracture is increased in patients with age > 40 years, first-time dislocation, or a severe injury mechanism (e.g., MVC, fall > 1 flight of stairs, or interpersonal violence). [9]
Axillary nerve injury is common with inferior shoulder dislocation. Document signs of axillary nerve palsy prior to manipulation and reduce without delay (see “Treatment”). [5]
Shoulder x‑ray
- Goal: confirm dislocation and exclude fracture
-
Views [10][11]
- Anteroposterior view (AP view) with the shoulder in internal and external rotation
- Lateral scapular view (Y view): a radiographic angle where the body of the scapula forms the letter "Y" with the coracoid process and the acromion [11]
- Axillary view: a radiographic angle visualizing the glenohumeral joint axially from the inferior aspect with the arm in abduction [11]
-
Findings
- Displacement of the humeral head from the glenoid fossa [11]
- Anterior shoulder dislocation: humeral head may be overlapping with and/or inferior to the glenoid on the AP view; anterior displacement visible on the Y view and axillary view
- Posterior shoulder dislocation: displacement may not be visible on AP view; posterior displacement visible on the Y view and axillary view
- Inferior shoulder dislocation: humeral head inferior to the glenoid on the AP view and humerus abducted; inferior displacement visible on Y view [6]
- Radiographic fracture signs may be present if there is a concomitant fracture.
- Light bulb sign: diagnostic of posterior shoulder dislocation on the AP view [8]
- Hill-Sachs lesion and/or Bankart lesion may be visible.
- Displacement of the humeral head from the glenoid fossa [11]
Obtain a Y view and/or axillary view in addition to the AP view to reduce the risk of missing or misclassifying shoulder dislocations (especially posterior shoulder dislocation). [10][11]
 of the shoulder")

")


MRI [10]
- Goal: deeper evaluation of soft tissue injuries related to dislocation event
-
Indications
- Hill-Sachs lesion or Bankart lesion identified on x-ray
- Normal x-ray despite history consistent with dislocation event
- Modalities: MRI shoulder without IV contrast or MR arthrography






X-ray scapula (lateral view; tangential or “Y” view)
The patient is placed in the erect PA oblique position or supine AP oblique position. The medial and lateral margins of the scapula are aligned perpendicular to the x-ray detector, resulting in a tangential view of the body of the scapula.
The stem of the Y is formed by the scapular body, while the bifurcation of the Y is formed by the acromion process (1) and coracoid process (2). The humeral head normally projects over the glenoid at the bifurcation of the Y. The lateral extent of the clavicle (3) is visible, and a nearly straight line can be drawn through the inferior borders of the acromion (1) and clavicle (3).
This view is useful for detecting dislocations, fractures, and degenerative disease, especially in patients with restricted movement at the shoulder.
Dotted line: humerus; green overlay: scapula
Source: “Y CR shoulder” by RSatUSZ, Wikimedia Commons, licensed under CC BY-SA 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 4.0.
{kind=link}
X-ray left shoulder (AP view (left); lateral (scapular) Y-view (right))
There is an anterior and slightly inferior displacement of the humeral head from the glenoid fossa.
Green overlay: scapula
Red overlay: proximal humerus
Source: “Dislocated shoulder X-ray 10” by Hellerhof, Wikimedia Commons, licensed under CC BY 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
{kind=link}

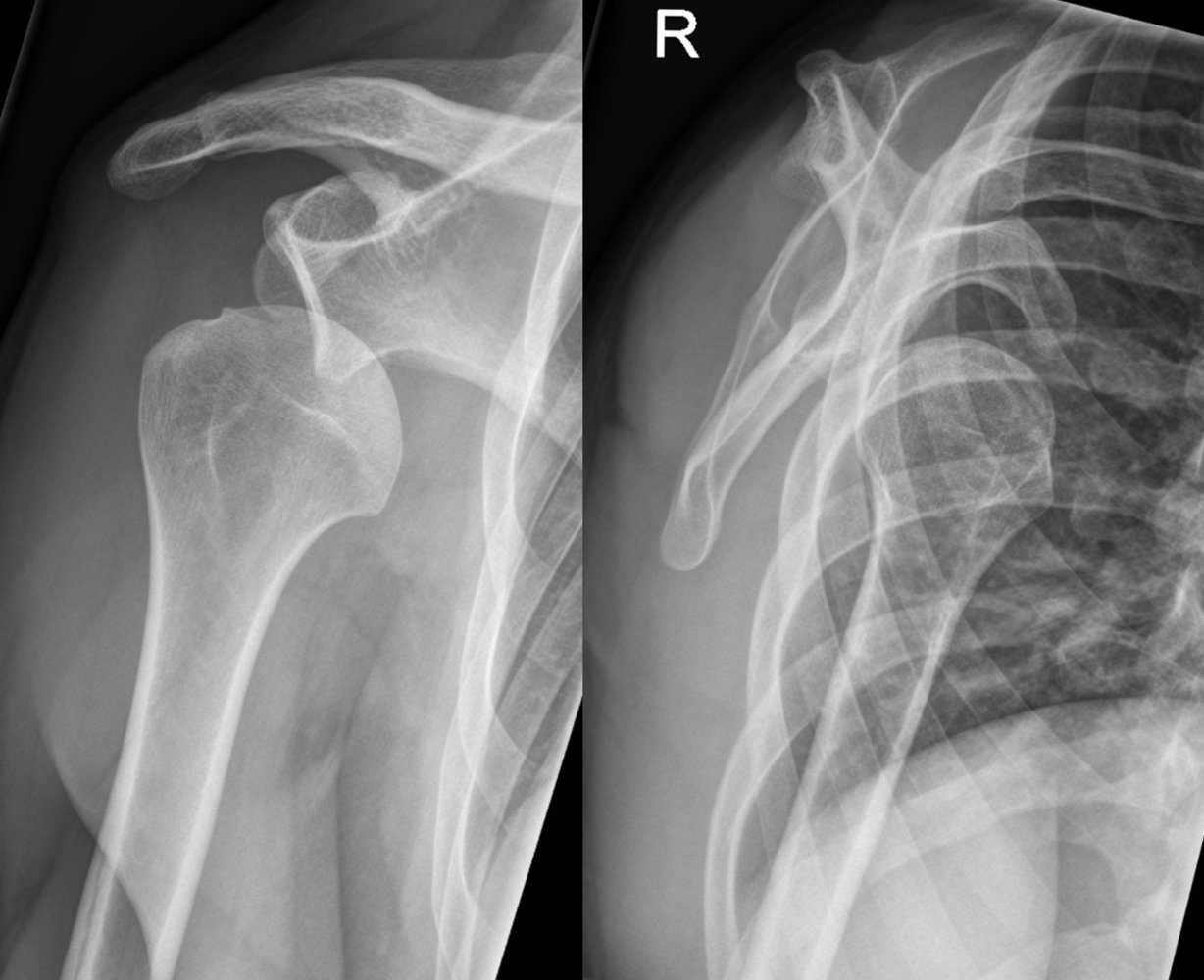
X-ray shoulder (AP view; left: dislocation; right: post reduction)
Internal rotation of the humerus during posterior dislocation produces a contour resembling a lightbulb on the AP radiograph (overlay). In addition, poor congruency of the humeral head with the glenoid is seen in this patient. After reduction, the greater tubercle (tuberosity) is visible laterally and the humeral head is well-aligned with the glenoid fossa.
Source: “Lightbulb sign - posterior shoulder dislocation - Roe vor und nach Reposition 001” by Hellerhoff, Wikimedia Commons, licensed under CC BY 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
{kind=link}
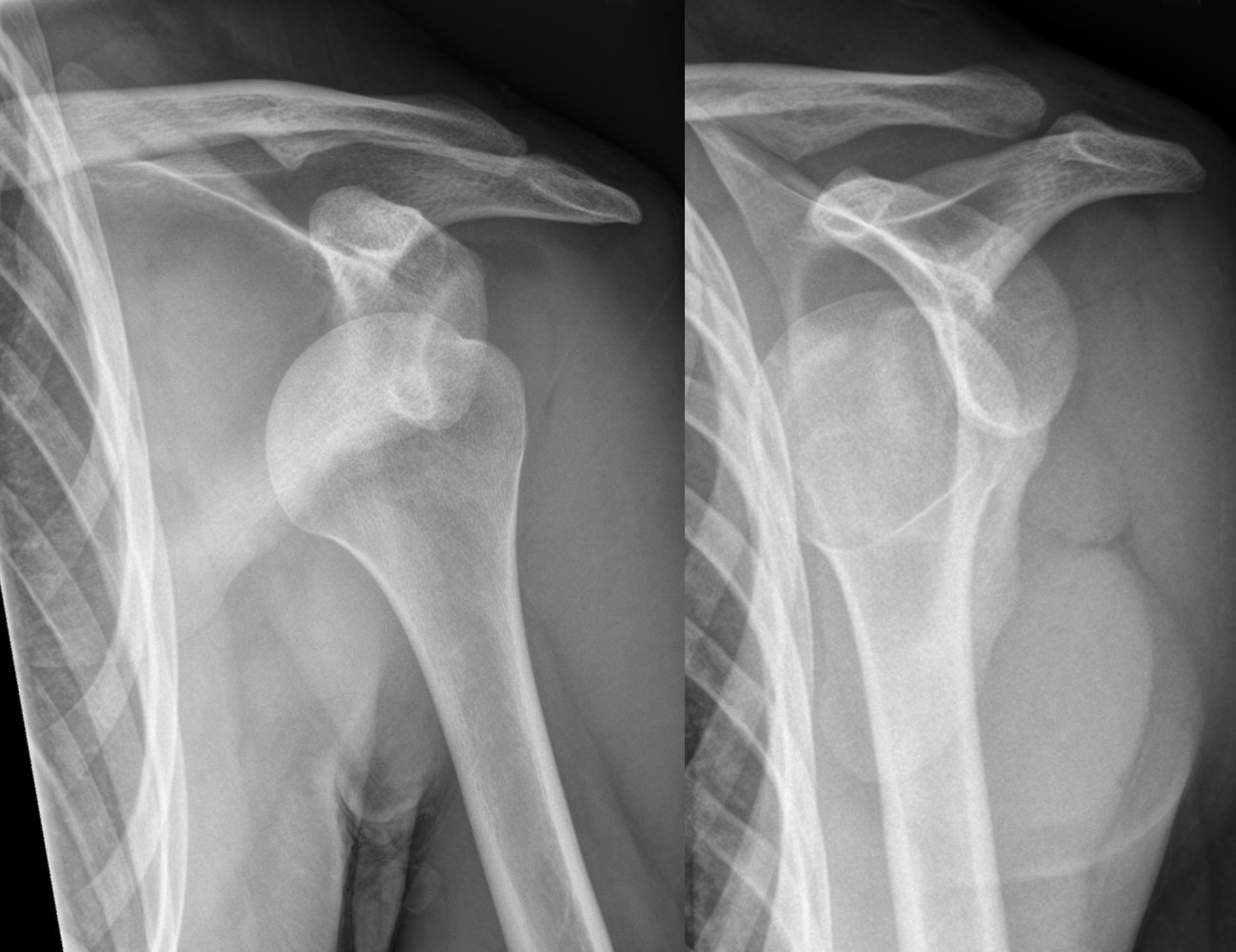
X-ray right shoulder (AP view (left); lateral (scapular) Y-view (right))
There is anterior and inferior displacement of the humeral head from the glenoid fossa. Hill-Sachs lesion can be seen in AP view.
Source: “File:Dislocated shoulder X-ray 11.png” by Hellerhoff, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}
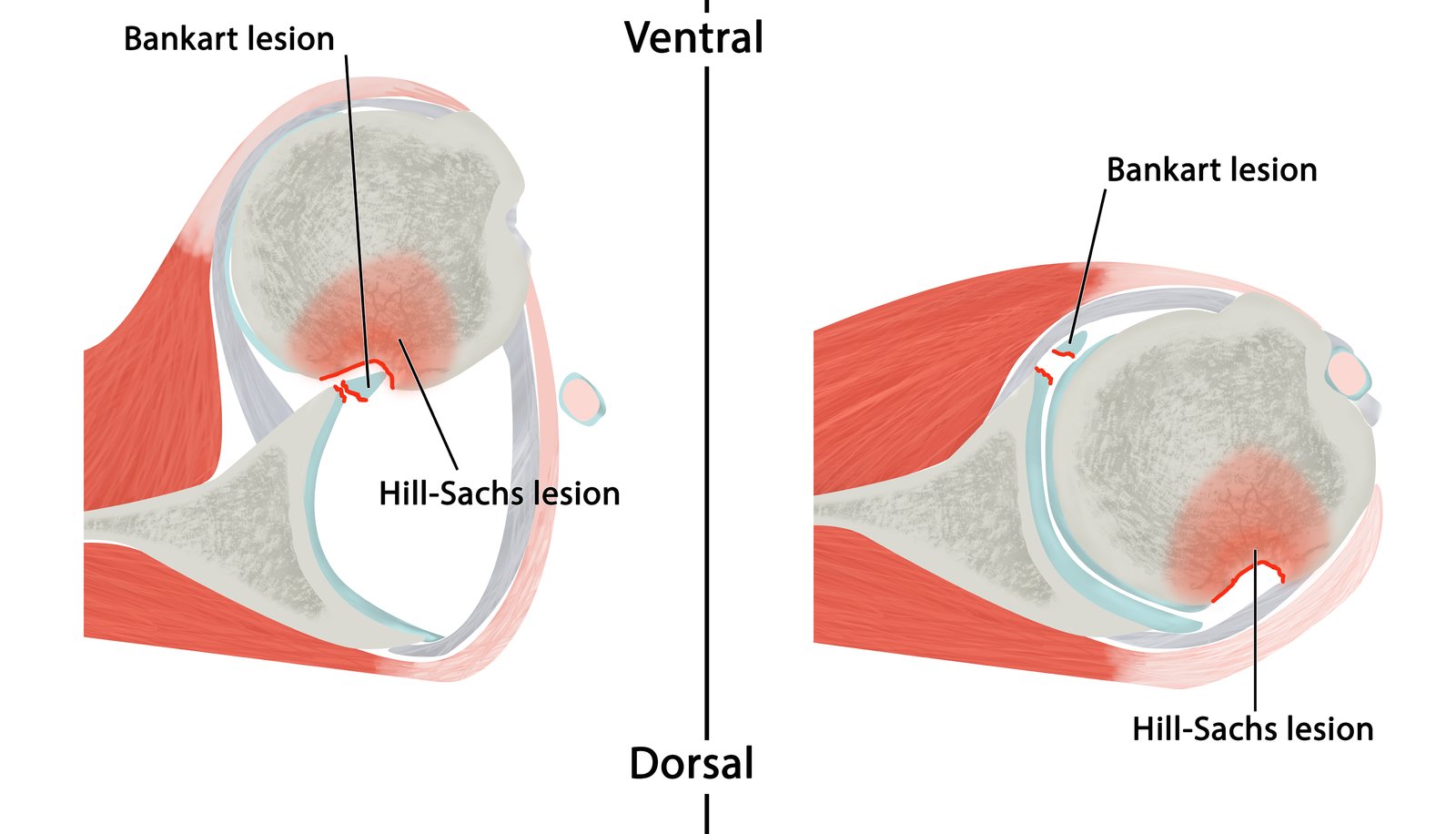
In an anterior shoulder dislocation, the glenoid rim may indent on the dorsolateral surface of the humeral head, which is called a Hill-Sachs lesion. In Bankart lesions, the anterior inferior lip of the glenoid labrum is also damaged. Fractures can be seen after reposition, e.g., on MRI.
© AMBOSS
Click on the overlay icon below the taskbar on the left to toggle the overlay on and off.
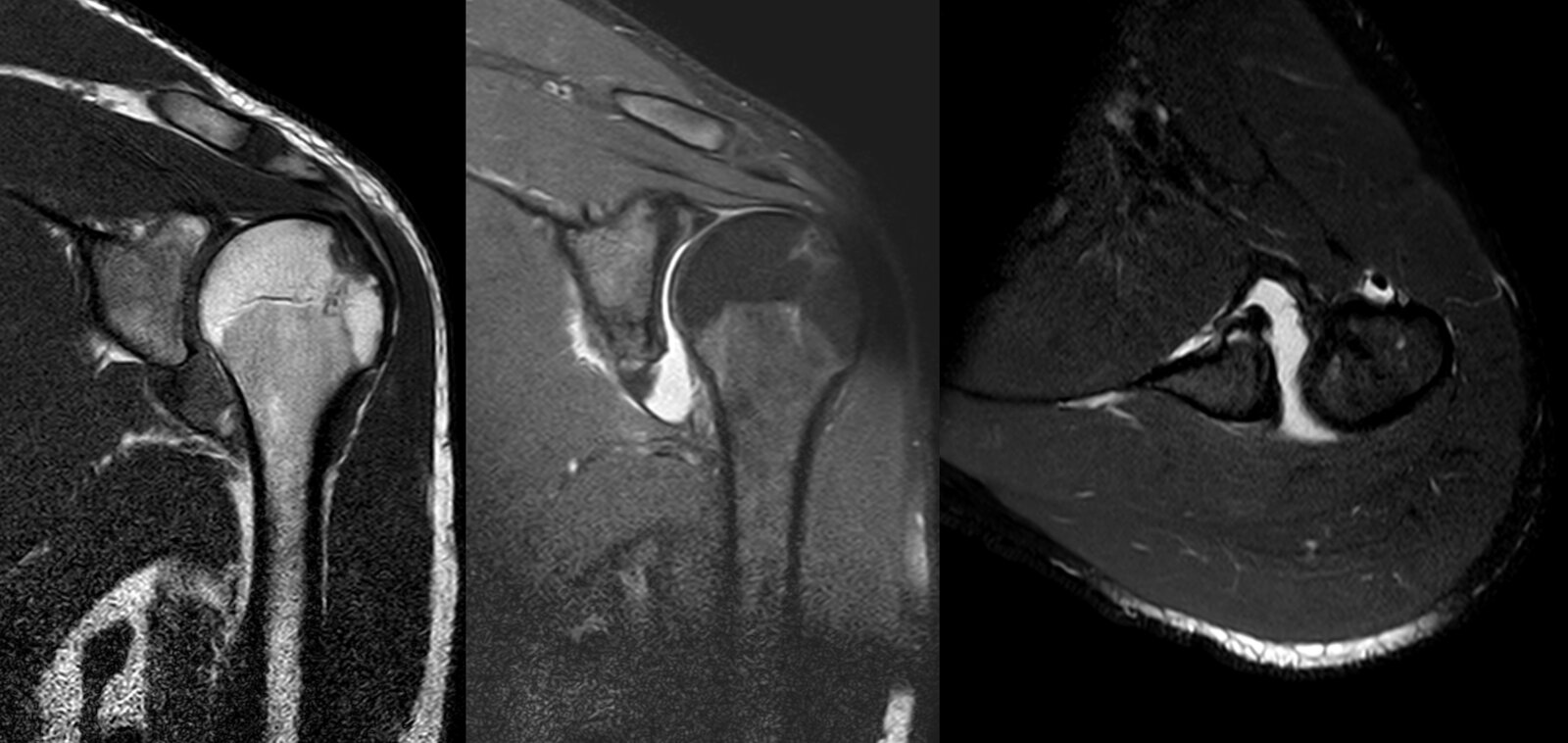
MRI left shoulder (STIR and T1, coronal plane; PD FS, axial and sagittal plane)
On the fat-saturated sequences (STIR and both PD images), there is hyperintensity in the posterolateral humeral head and anteroinferior glenoid rim with corresponding hypointensity on the T1 image. These findings indicate contusion. In addition, a depression in the cortex of the affected region of the humeral head (Hill-Sachs depression fracture) is seen. There is also a fracture through the affected anteroinferior glenoid (osseous or bony Bankart Lesion).
This pattern of injury occurs during anterior dislocation as the humeral head externally rotates and descends inferiorly, impacting the anteroinferior glenoid rim with its posterolateral surface.
Image source of original image: Radiologie Frechen-Erftstadt. Original title: “Anterior shoulder dislocation”. Created by: Markus Le Blanc.
MRI shoulder (A: T1-weighted, coronal plane; B: proton density-weighted fat-suppressed, coronal plane; C: T2-weighted fat-suppressed, axial plane)
Coronal images show a labral Bankart lesion (green overlay) and humeral Hill-Sachs lesion (red arrows). Only the Bankart lesion is seen on the axial image. Joint effusion (E) is visible on all images.
Source: “Post Dislocated shoulder MRI 01” by Hellerhoff, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
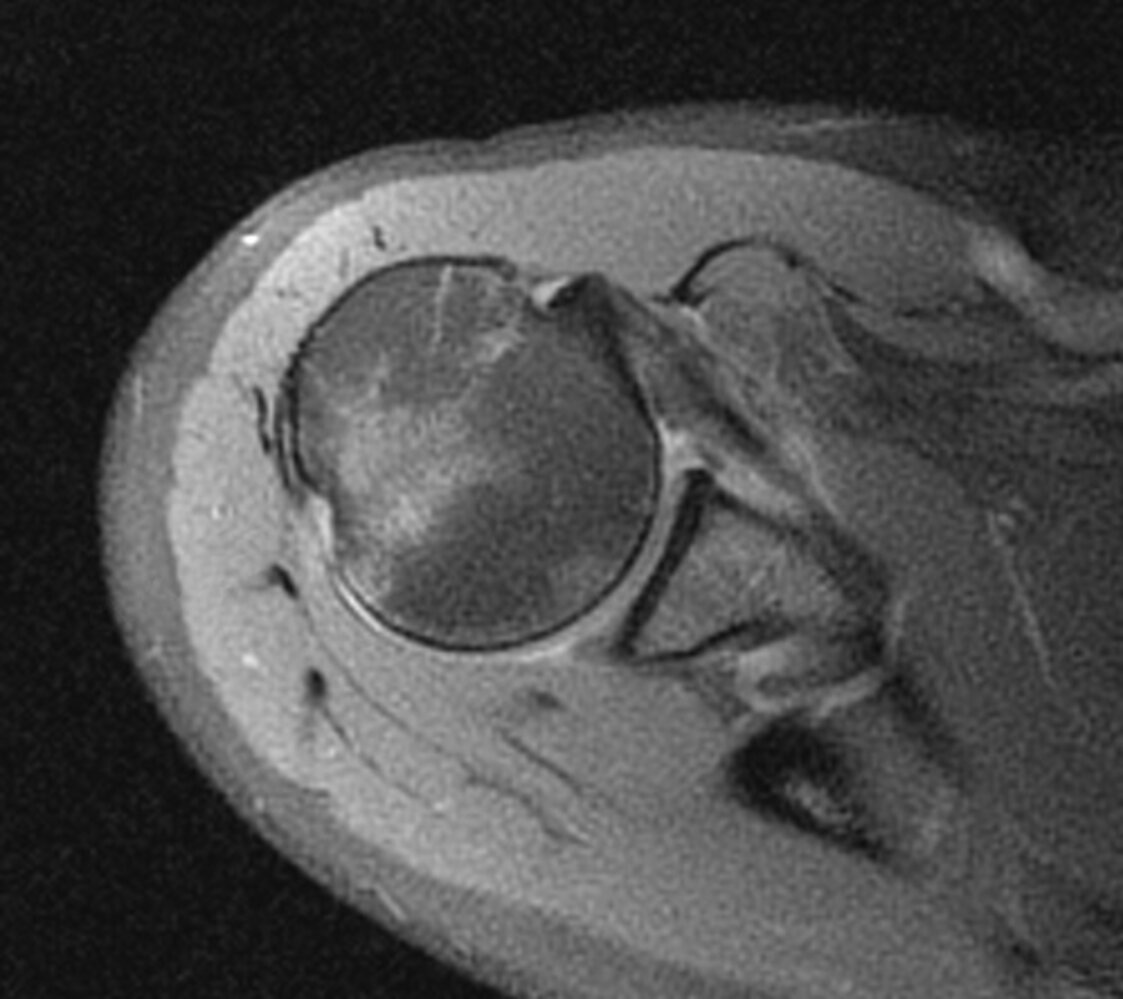
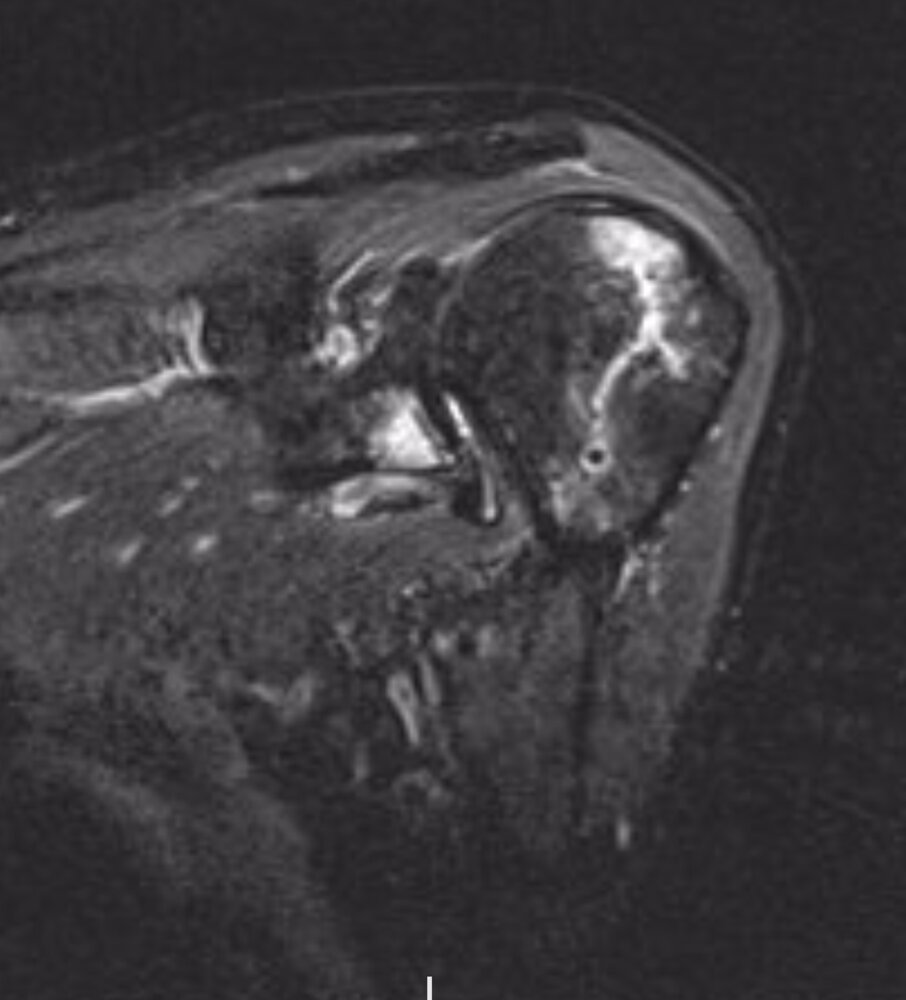
MRI shoulder (fluid sensitive sequence; axial plane)
A posterolateral depression fracture of the humeral head (Hill-Sachs lesion, black arrow) is associated with marrow edema (green overlay). Edema is also present along the subscapularis tendon (red overlay).
G: glenoid; H: humerus; ST: subscapularis tendon
Source: “Hill sachs Delle” by Braegel, Wikimedia Commons, licensed under CC BY-SA 3.0. Modifications: - removed arrow. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
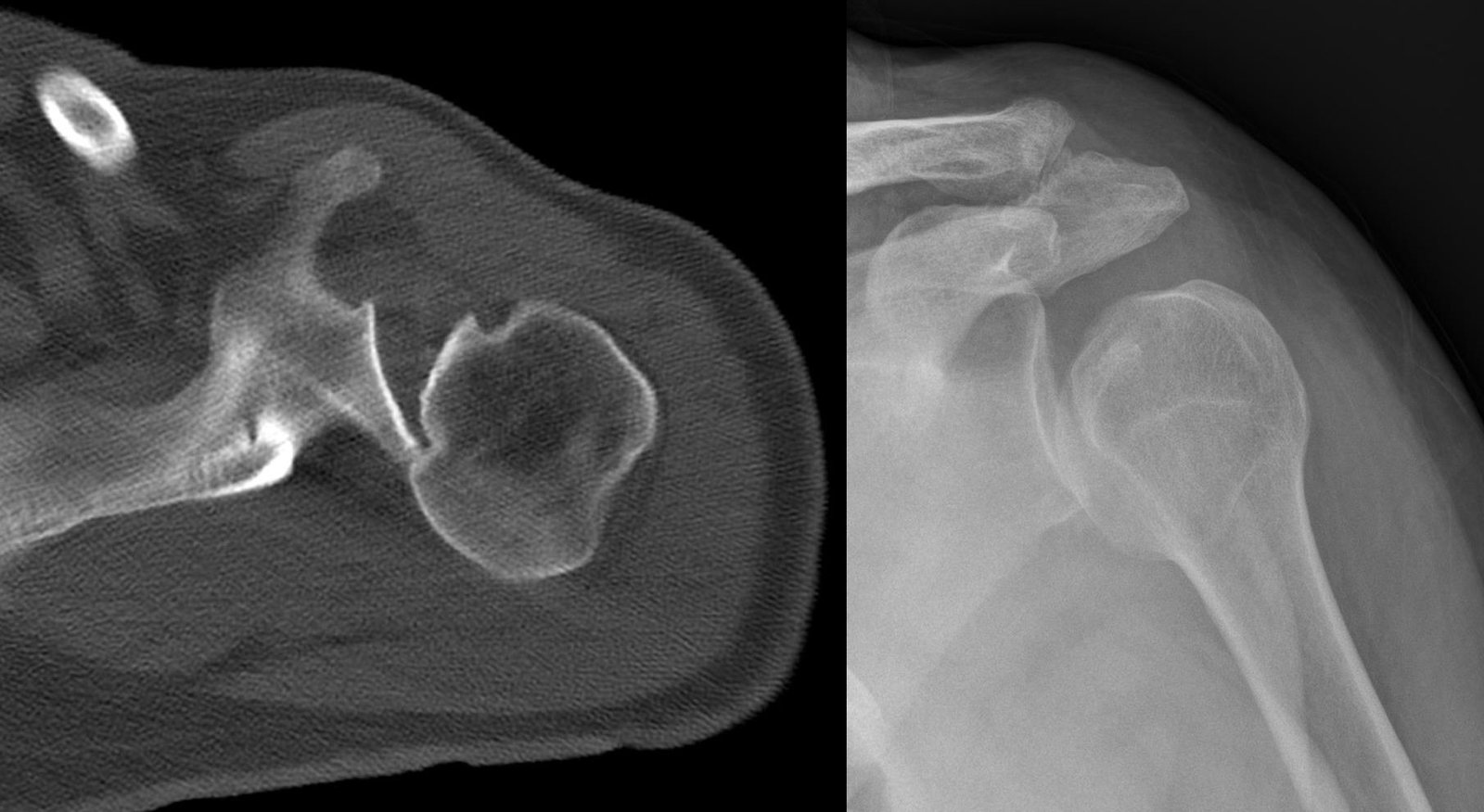
Source: “Inverse Hill-Sachs-Laesion - posterior shoulder dislocation - CT axial und Roe 001” by Hellerhof, Wikimedia Commons, licensed under CC BY 3.0.
{kind=link}

CT shoulder (coronal plane)
An intraarticular displaced fracture (bony Bankart lesion; red overlay) involves the anterior glenoid labral complex.
This injury is a common complication of anterior dislocation of the humerus (H).
S: scapula; R: rib
Source: “File:CT. Bony Bankart lesion at the antero-inferior glenoid. Clearly dislocated at the cranial part. Humeral head is still centered..jpg” by RSatUSZ, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
Treatment
The primary aim of treatment is to reposition the humeral head into the glenoid cavity and restore full range of motion.
Initial management [6]
- Patients with polytrauma: Follow the ABCDE approach.
- Patients with posterior shoulder dislocation: Treat acute seizures or manage electrical injuries, if present.
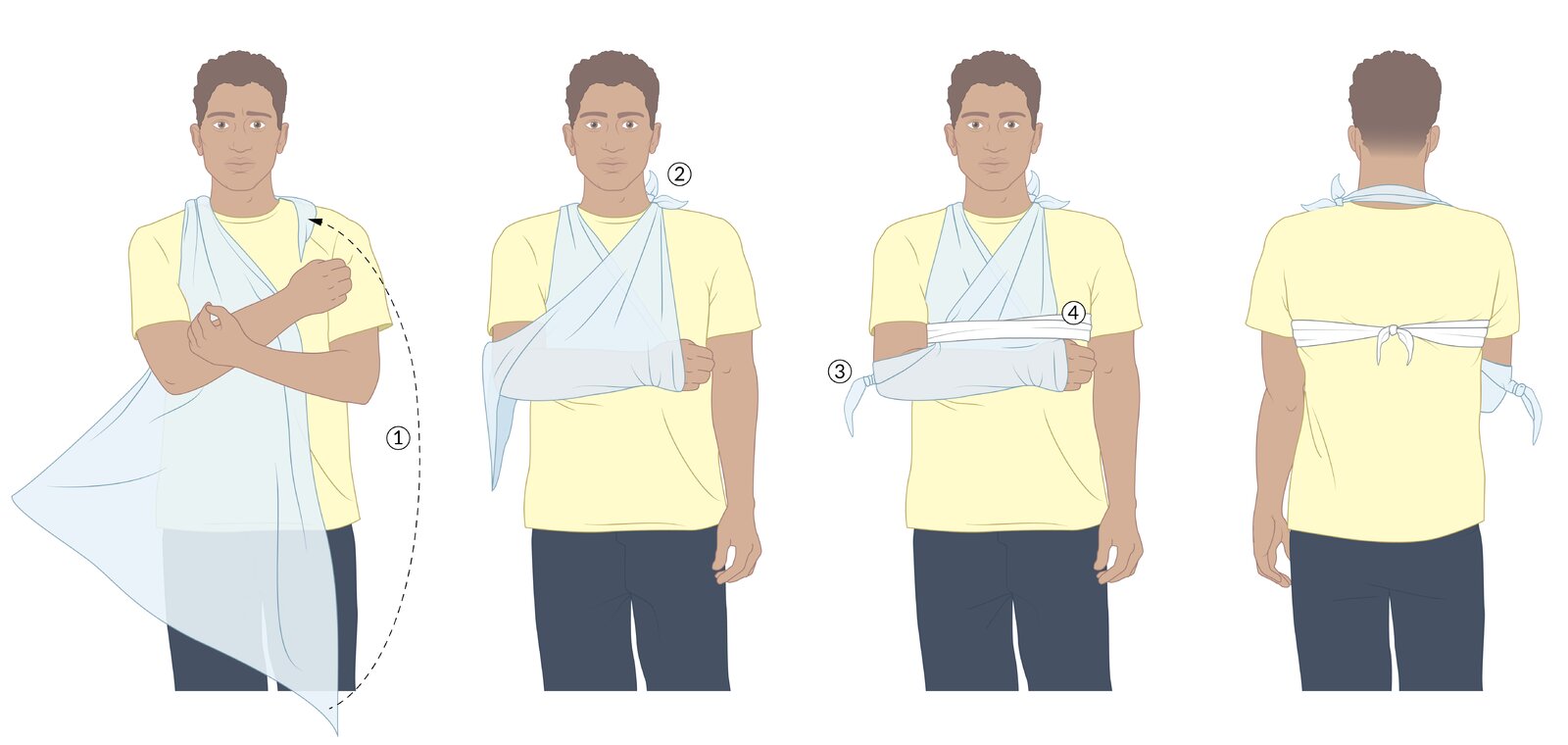
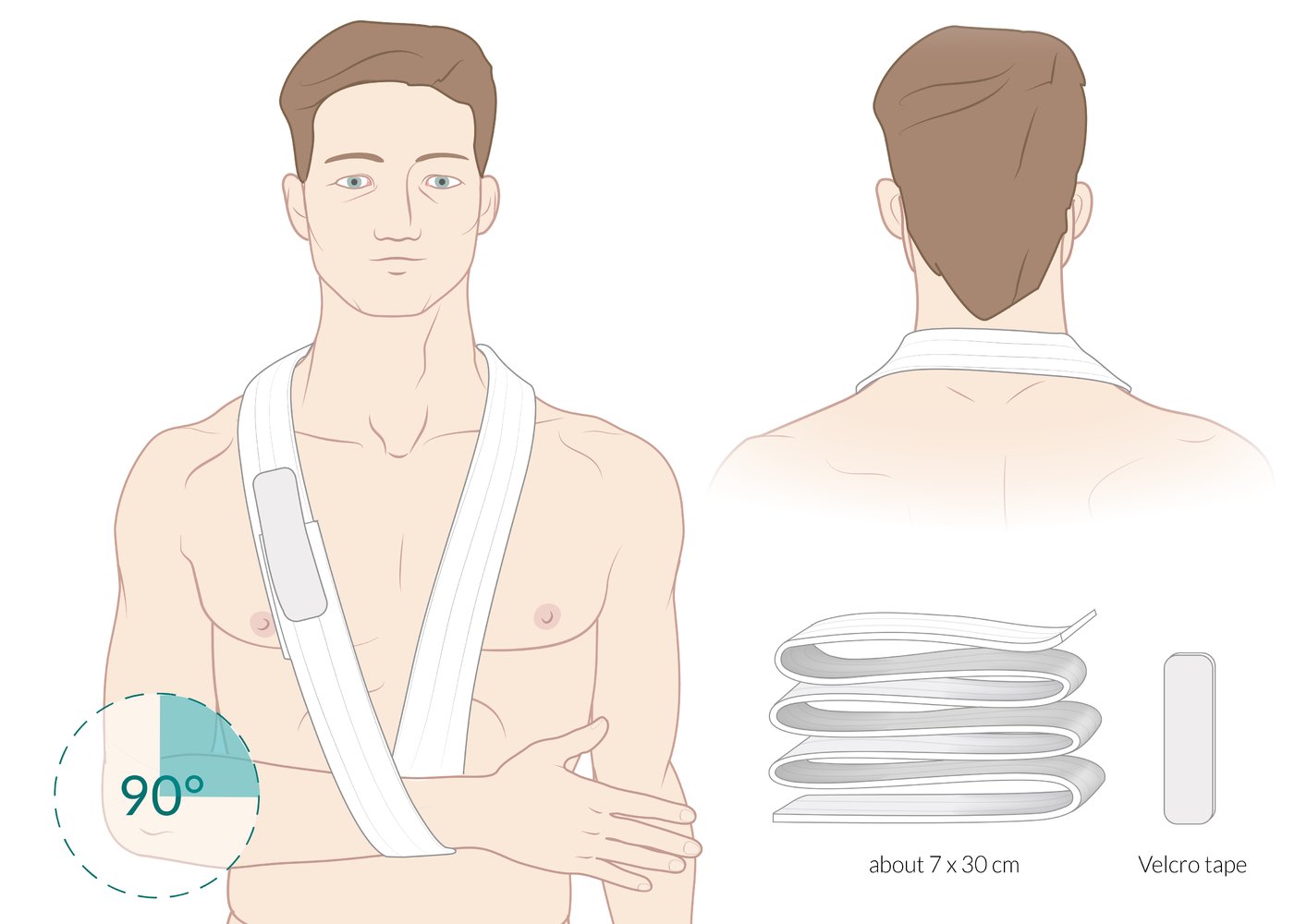
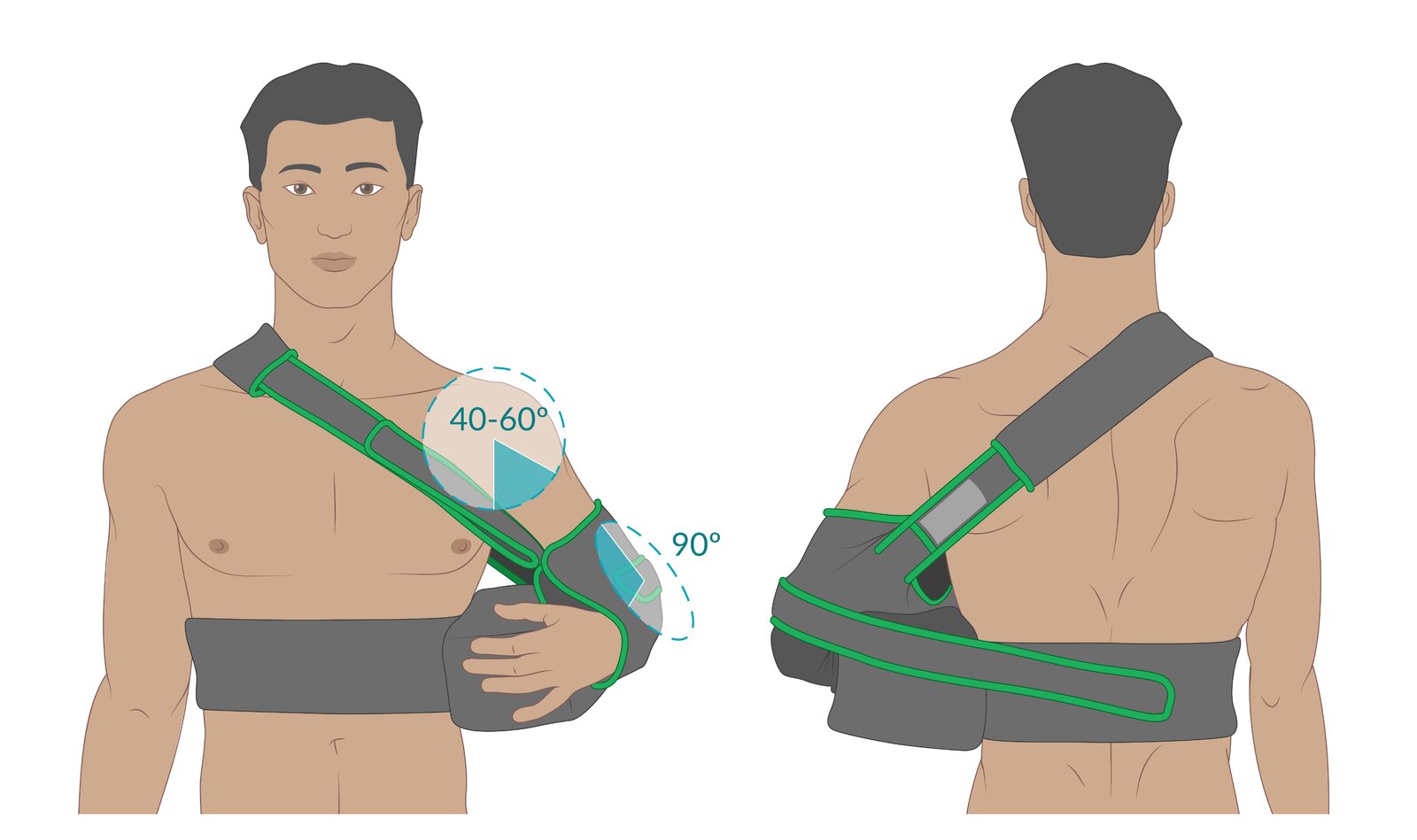
- All patients: Manage acute pain and consider a broad arm sling to immobilize in a position of comfort while waiting for imaging.
- If indicated, initiate steps for immediate closed reduction, e.g., preparation for procedural sedation.
- Consult orthopedics if reduction by a specialist or surgery is required.

Closed reduction [6]
Indications
- Consider urgent closed reduction for all uncomplicated shoulder dislocations. [12]
- See “Indications for shoulder reduction” for reasons to consult orthopedics before attempting reduction.
Techniques
-
Anterior shoulder dislocation
- Multiple recommended techniques exist with similar success and complication rates. [12][13][14][15]
- See “Shoulder reduction” for details on, e.g., scapular manipulation, Milch technique, and traction-countertraction.
- Procedural sedation is often required.
- Posterior shoulder dislocation: typically reduced under general anesthesia [4]
-
Inferior shoulder dislocation [5]
- Consider traction-countertraction OR gentle rotation of the humeral head to convert it to an anterior dislocation, followed by an anterior dislocation reduction technique.
- Consult orthopedics if the humeral head is entrapped, e.g., by the glenohumeral ligament or joint capsule.
Post-reduction care [3]
- Repeat neurovascular examination and imaging to evaluate reduction success and identify complications (e.g., Hill-Sachs lesion).
- Apply an arm sling or shoulder immobilizer. [3][16][6][17][18]
- Provide analgesia, e.g., acetaminophen, NSAIDs, and/or ice packs.
- Ensure short-term follow-up (e.g., in 5–8 days) for orthopedics assessment and subsequent rehabilitation.
- Counsel patients on the risk of early recurrence and advise avoidance of contact sports until fully healed. [16]
Conduct a thorough neurovascular examination before and after shoulder reduction to identify axillary nerve injury and other neurovascular injuries as early as possible. [6]


Surgical management
Surgical management may be indicated for complicated shoulder dislocation or for prevention and treatment of recurrent shoulder dislocations.
Complicated shoulder dislocation [3]
-
Examples
- Fracture-dislocation (e.g., concomitant proximal humerus fracture, clavicle fracture, or scapula fracture)
- Open dislocation
- Unsuccessful closed reduction
- Neurovascular injury
- Associated rotator cuff tear (more common in patients > 40 years of age)
-
Management
- Urgent operative intervention (e.g., ORIF) may be required, e.g., for displaced fracture-dislocations and other associated injuries.
- Most otherwise uncomplicated irreducible shoulder dislocations are treated with closed reduction under general anesthesia. [3]
Recurrent shoulder dislocation [3][16]
-
Risk factors
- Demographic factors: age < 30 years, active lifestyle, male sex [16]
- Glenohumeral instability, e.g., caused by Bankart lesions, Hill-Sachs lesions, glenoid labrum injury, glenoid rim fracture (bony Bankart lesion)
- Management: Elective operative intervention is often recommended (e.g., arthroscopic surgery, open surgery).
Young, active patients with first-time uncomplicated shoulder dislocations are likely to benefit from surgery and should be referred to orthopedics after successful closed reduction. [3]
© AMBOSS
© AMBOSS
© AMBOSS
Complications
-
Neurovascular injury: can be a complication of both dislocation and reduction
- Axillary nerve injury
- Brachial plexus injury
- Injury of the axillary artery and/or axillary vein
-
Hill-Sachs lesion ; [19]
- A depression fracture on the posterolateral surface of the humeral head caused by impact with the glenoid rim
- Highly prevalent in patients with an anterior shoulder dislocation
- Increases the risk of glenohumeral instability and recurrent shoulder dislocation
- Bankart lesion
- Avulsion fracture of the major and/or minor tubercles
- Shoulder joint instability
- Rotator cuff injury
- Shoulder stiffness due to prolonged immobilization
- Osteoarthritis of the shoulder joint
A sensory deficit over the lateral surface of the shoulder and limited abduction due to deltoid muscle weakness suggest axillary nerve injury. [8]
We list the most important complications. The selection is not exhaustive.
X-ray right shoulder (AP view (left); lateral (scapular) Y-view (right))
There is anterior and inferior displacement of the humeral head from the glenoid fossa. Hill-Sachs lesion can be seen in AP view.
Source: “File:Dislocated shoulder X-ray 11.png” by Hellerhoff, Wikimedia Commons, licensed under CC BY-SA 3.0.
Prognosis
- High rate of recurrence
- After rotator cuff repair, the rate of recurrence is significantly lower.
External Resources
References
- Zachilli MA, Owens BD. "Epidemiology of shoulder dislocations presenting to emergency departments in the United States". J Bone Joint Surg Am. 92(3). :542-549. (2010)
- Cutts S, Prempeh M, Drew S. "Anterior shoulder dislocation.". Ann R Coll Surg Engl. 91(1). :2-7. (2009)
- Khiami F, Gérometta A, Loriaut P. "Management of recent first-time anterior shoulder dislocations". Orthop Traumatol Surg Res. 101(1). :S51-S57. (2015)
- C. Michael Robinson, Joseph Aderinto. "Posterior Shoulder Dislocations and Fracture-Dislocations". J Bone Joint Surg Am. 87(3). :639-650. (2005)
- Nambiar M, Owen D, Moore P, Carr A, Thomas M. "Traumatic inferior shoulder dislocation: a review of management and outcome". Eur J Trauma Emerg Surg. 44(1). :45-51. (2018)
- Verweij LP, Baden DN, van der Zande JM, van den Bekerom MP. "Assessment and management of shoulder dislocation". BMJ. :m4485. (2020)
- Haritinian EG, Stoica IC, Popescu R, Gheorghievici GL, Nové-Josserand L. "Treatment and outcomes of chronic locked posterior shoulder dislocations: a retrospective case series.". BMC Musculoskelet Disord. 24(1). :82. (2023)
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904
- Émond M, Le Sage N, Lavoie A, Rochette L. "Clinical Factors Predicting Fractures Associated with an Anterior Shoulder Dislocation". Acad Emerg Med. 11(8). :853-858. (2004)
- Amini B, Beckmann NM, Beaman FD, et al. "ACR Appropriateness Criteria ® Shoulder Pain–Traumatic". J Am Coll Radiol. 15(5). :S171-S188. (2018)
- Sanders TG, Jersey SL. "Conventional Radiography of the Shoulder". Semin Roentgenol. 40(3). :207-222. (2005)
- Reichman EF. "Reichman's Emergency Medicine Procedures, 3rd Edition". McGraw Hill Professional. (2018). ISBN: 9781259861932
- Alkaduhimi H, van der Linde JA, Willigenburg NW, van Deurzen DFP, van den Bekerom MPJ. "A systematic comparison of the closed shoulder reduction techniques". Arch Orthop Trauma Surg. 137(5). :589-599. (2017)
- Gonai S, Yoneoka D, Miyoshi T, da Silva Lopes K. "A Systematic Review With Pairwise and Network Meta-analysis of Closed Reduction Methods for Anterior Shoulder Dislocation". Ann Emerg Med. 81(4). :453-465. (2023)
- Roberts JR. "Roberts and Hedges' Clinical Procedures in Emergency Medicine and Acute Care". Elsevier. (2018). ISBN: 9780323354783
- Hasebroock AW, Brinkman J, Foster L, Bowens JP. "Management of primary anterior shoulder dislocations: a narrative review". Sports Med - Open. 5(1). (2019)
- Braun C, McRobert CJ. "Conservative management following closed reduction of traumatic anterior dislocation of the shoulder". Cochrane Database Syst Rev. 2019(5). (2019)
- Hurley ET, Fried JW, Alaia MJ, et al. "Immobilisation in external rotation after first-time traumatic anterior shoulder instability reduces recurrent instability: a meta-analysis". J ISAKOS. 6(1). :22-27. (2021)
- Provencher MT, Frank RM, LeClere LE, et al. "The Hill-Sachs Lesion: Diagnosis, Classification, and Management". J Am Acad Orthop Surg. 20(4). :242-252. (2012)