Summary
Volvulus is defined as the twisting of a loop of bowel on its mesentery and is one of the most common causes of intestinal obstruction. The sigmoid colon, and less frequently, the cecum, are the common sites of volvulus in adults. Patients typically show features of bowel obstruction (abdominal pain, distension, bilious vomiting) or of bowel ischemia and gangrene (tachycardia, hypotension, hematochezia, peritonitis) in severe cases. The whirl sign and a grossly dilated loop of bowel on an abdominal CT scan establish the diagnosis of volvulus in adults. Sigmoid volvulus without peritonitis is initially managed with endoscopic detorsion, followed by a semi-elective surgery (sigmoid colectomy). Sigmoid volvulus with peritonitis, and all cases of cecal volvulus, require emergency surgery. Endoscopic detorsion should not be attempted in a patient with cecal volvulus because of the high risk of perforation.
See “Midgut volvulus and intestinal malrotation” for volvulus in a neonate or infant.
Epidemiology
-
Incidence
- Volvulus: 3rd most common cause (∼ 10–15%) of intestinal obstruction in the United States
-
Age [1][2]
- Sigmoid volvulus: ∼ 70 years
- Cecal volvulus: 40–60 years
-
Sex [1][2]
- Sigmoid volvulus: ♂ > ♀
- Cecal volvulus: ♀ >♂
SigmOid volvulus is more common in Older individuals while Midgut volvulus and Malrotation are more common in Minors.
Epidemiological data refers to the US, unless otherwise specified.
Etiology
Risk factors
-
Long mesentery [3]
- Acquired (sigmoid volvulus): chronic constipation , high-fiber diet resulting in bulky stools → chronic overloading of the sigmoid colon → lengthening of the sigmoid colon and its mesentery → increased risk of torsion
- Congenital (cecal volvulus): abnormally mobile cecum → predisposition of the cecum to rotate on its axis (axial torsion) or fold upwards (cecal bascule)
- Megacolon (Hirschsprung disease, Chagas disease)
- Intestinal bands/adhesions
- Decreased pelvic space: pregnancy or pelvic mass
- Previous history of volvulus
Pathophysiology
-
Torsion of bowel on its axis [4]
- Closed-loop mechanical bowel obstruction → accumulation of gas and feces within the loop → increased intraluminal pressure → impaired capillary perfusion of bowel → bowel strangulation, ischemia, and gangrene
- Torsion of the mesenteric vascular pedicle → occlusion/thrombosis of mesenteric vessels → bowel strangulation, ischemia, and gangrene
- Location: may affect all parts of the bowel [5]
- Sigmoid volvulus (most common, 80%)
- Cecal volvulus (15%)
- Transverse colon volvulus (3%)
- Splenic flexure volvulus (2%)

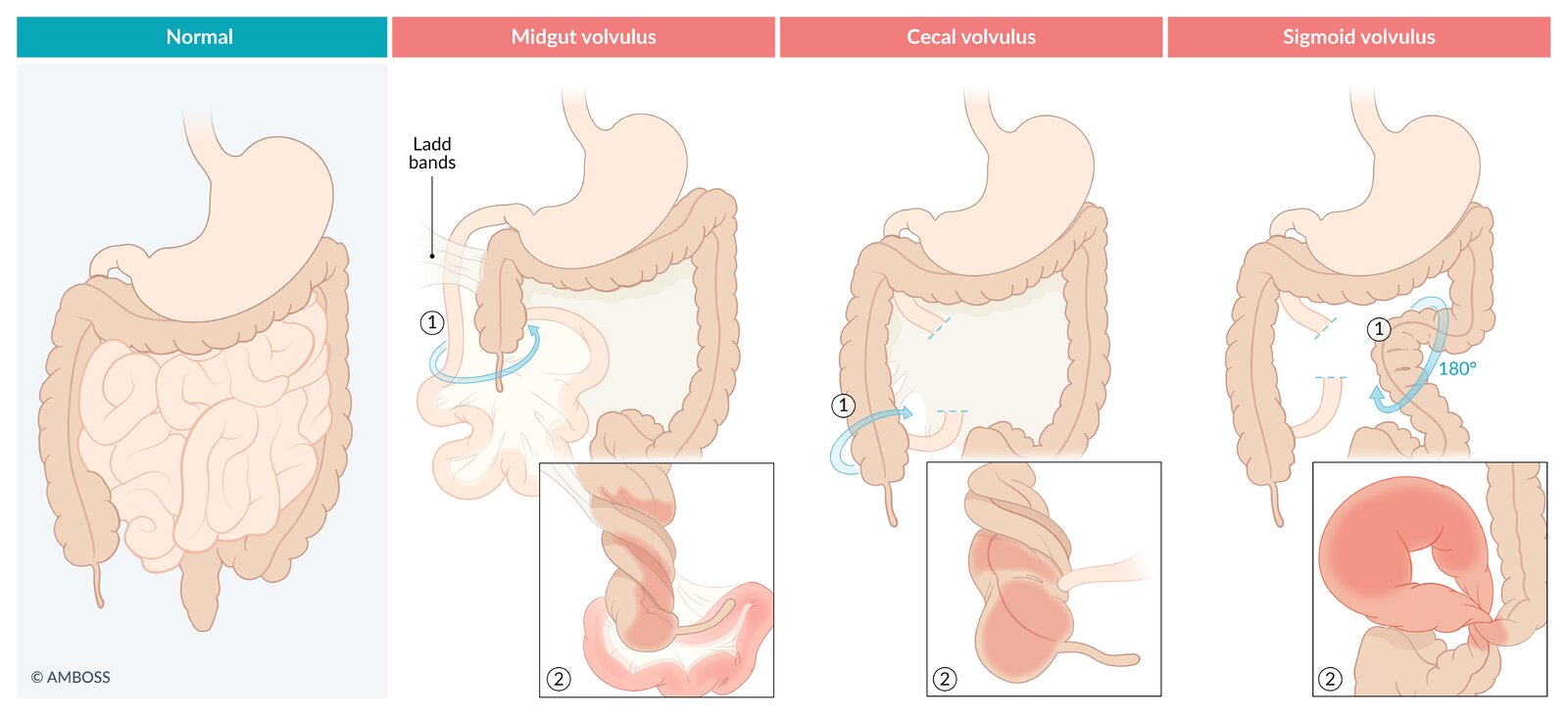
The types of volvulus are classified by anatomical location as illustrated here.
- Midgut volvulus: A malrotated midgut causing mechanical bowel obstruction, mostly in neonates and infants. Fibrous peritoneal bands (Ladd bands) attaching the cecum to the retroperitoneum are a common pathological finding in midgut volvulus.
- Cecal volvulus: The cecum rotates on its mesenteric axis resulting in mechanical bowel obstruction and vascular compromise.
- Sigmoid volvulus: The sigmoid colon rotates on its mesenteric axis resulting in mechanical bowel obstruction and vascular compromise.
© AMBOSS
Clinical features
Sigmoid volvulus
- Previous episodes of abdominal pain, which decreased after explosive passage of stool/gas
- Slowly (most common) or rapidly progressive symptoms of bowel obstruction
- If bowel ischemia occurs → tachycardia, hypotension, peritonitis (rebound tenderness), hematochezia or blood on DRE may be present
- If bowel perforation occurs → obliteration of liver dullness on percussion
Cecal volvulus
-
Types [6]
- Axial torsion of the cecum (90% of cases): the cecum rotates on its mesenteric axis → bowel obstruction with vascular compromise
- Cecal bascule (10%): the cecum folds upwards onto the ascending colon → bowel obstruction often without vascular compromise
-
Clinical features
- Acute presentation: features of small bowel obstruction
- Insidious onset: recurrent episodes of right lower abdominal pain
Diagnosis
- Work-up follows the same protocol as that for bowel obstruction.
-
Abdominal x-ray (erect and supine)
-
Sigmoid volvulus: coffee bean sign (bent inner tube sign/inverted U sign, kidney bean sign): dilated loop of bowel (sigmoid colon) with absent haustrae that arises in the left lower abdomen and extends towards the right upper abdomen
- Proximal colonic and small bowel dilation, with air-fluid levels
- Absence of air in the rectum
-
Cecal volvulus: dilated loop of bowel (cecum) with maintained haustrae that arises in the right lower abdomen and extends towards the left upper abdomen
- Upward displacement of the appendix
- Dilated small bowel loops with multiple air-fluid levels
- The colon distal to the obstruction does not dilate
- Cecal bascule: dilated cecum in the center of the abdominal cavity; an air-distended appendix may also be seen
- Bowel perforation: air under diaphragm [7]
-
Sigmoid volvulus: coffee bean sign (bent inner tube sign/inverted U sign, kidney bean sign): dilated loop of bowel (sigmoid colon) with absent haustrae that arises in the left lower abdomen and extends towards the right upper abdomen
-
CT scan
- Whirl sign: pathognomonic for volvulus [8]
- Specific features of sigmoid/cecal volvulus are similar to those seen in x-rays
- Demonstrates bowel ischemia , or perforation , if present
-
Barium enema: : bird beak sign (tapering of the dye column at the site of the twist)
- In cecal bascule, the end of the barium column is rounded, rather than tapered (inverted teardrop sign).
- Cecal volvulus: normal-sized colon with bird's beak sign at the cecum; dye does not enter the small bowel
- Sigmoid volvulus: normal-sized rectum with bird's beak sign at the sigmoid; dye does not enter the sigmoid colon



References:[7][8][9][10][11][12][13][14][15]
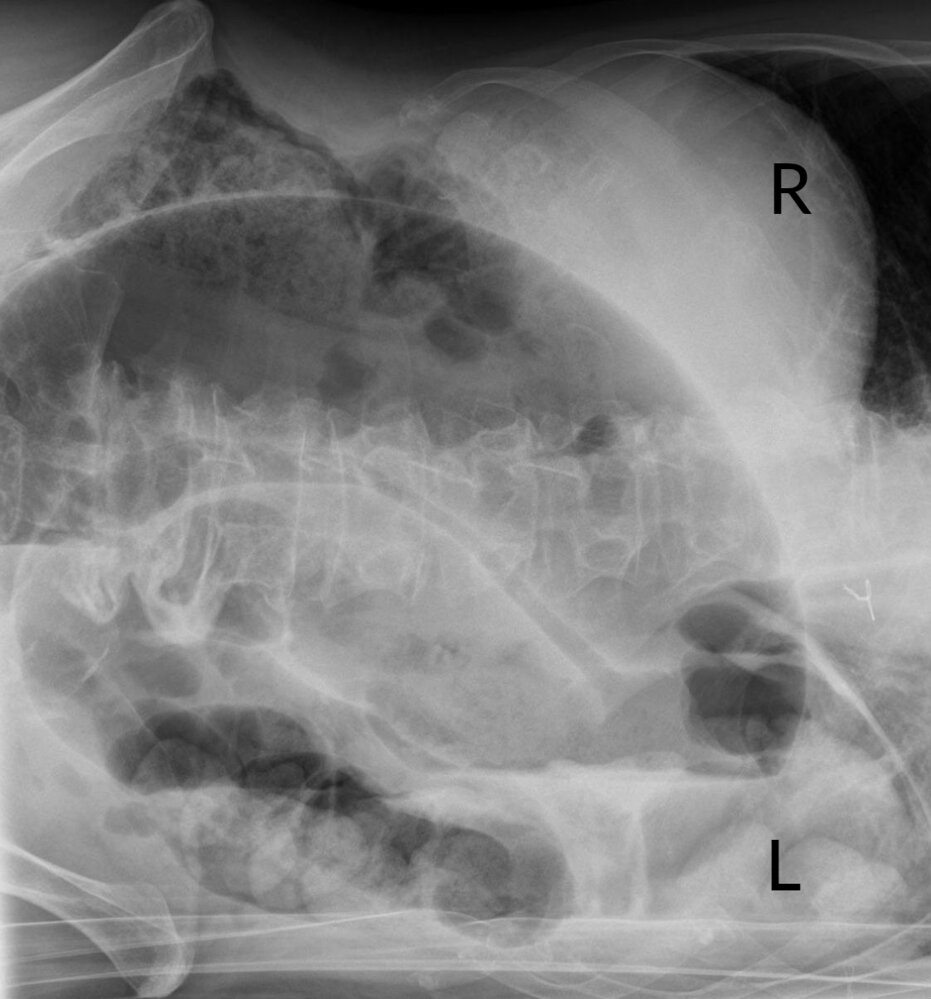
X-ray abdomen (left lateral decubitus view)
Gaseous distention of a closed loop of sigmoid colon (red overlay) has caused apposition of the medial walls (green lines). The resultant cleft-like configuration, in conjunction with the lateral walls of the loop, produces an appearance reminiscent of a coffee bean (illustration).
The coffee bean sign (also called “kidney-bean sign” or “bent-inner-tube sign”) is a classic conventional radiographic finding of sigmoid volvulus.
Dashed line: air-fluid level
Source: “Sigmavolvulus - Coffee-bean-sign - LSL” by Hellerhoff, Wikimedia Commons, licensed under CC BY-SA 3.0. Modifications: - letters added. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}

Fluoroscopy (single contrast barium enema; AP view; supine position)
As a result of axial torsion of the cecum, the barium column tapers (green overlay) until it eventually terminates at a point of complete obstruction (arrowhead). This appearance has been termed the “bird beak” sign. A featureless loop of gas-filled bowel in the left upper quadrant (white arrows) may represent the dilated cecum proximal to the point of obstruction.
Source: “Figure 2, in: Laparoscopic assisted right hemicolectomy for caecal volvulus” by Michael D Kelly, John Bunni, Anne M Pullyblank, World Journal of Emergency Surgery, licensed under CC BY 2.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

X-ray abdomen (AP view) of a child
Markedly dilated bowel (green overlay) extends obliquely from the right upper pelvis into the left upper abdomen. The configuration, including the double wall thickness (red overlay) of the two apposed bowel loops, resembles a bean (hence the terms “coffee bean sign” and “kidney bean sign;” also called “bent inner tube sign”).
Source: “Sigmoidvolvulus” by Mont4nha, Wikimedia Commons, licensed under CC0 1.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
{kind=link}
Differential diagnoses
Differential diagnoses of sigmoid volvulus
- Acute megacolon
- Toxic megacolon
- Other causes of mechanical bowel obstruction (e.g., colon cancer, strictures, cecal volvulus)
Differential diagnoses of cecal volvulus
- Sigmoid volvulus
- Small bowel obstruction (e.g., adhesions, tumors, intussusception)
The differential diagnoses listed here are not exhaustive.
Treatment
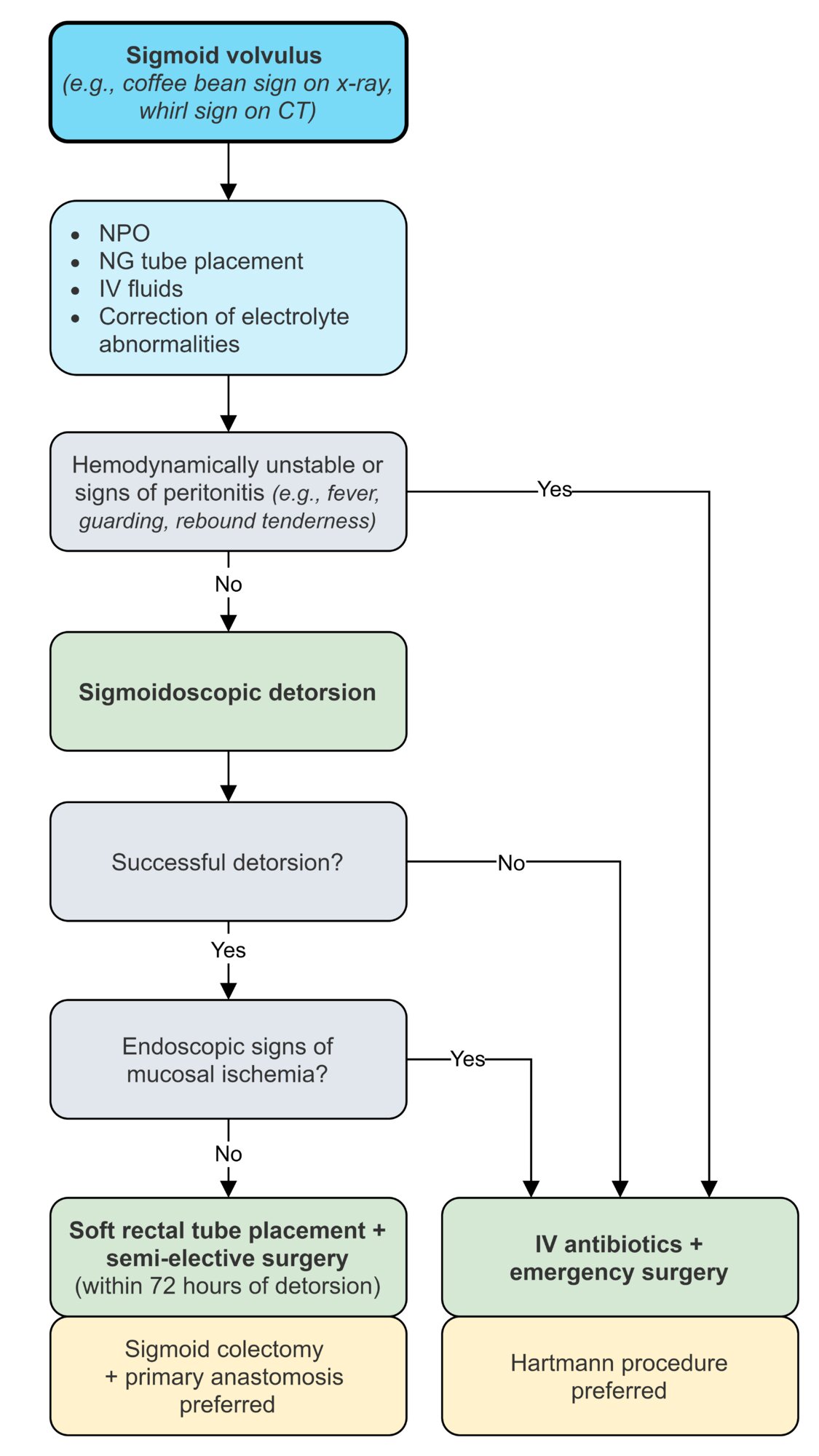
Treatment of sigmoid volvulus [16][17]

- Initial resuscitation: IV fluids; acid-base and electrolyte imbalance correction; NPO; placement of a nasogastric tube
-
Evaluation
-
No signs of peritonitis : rigid/flexible endoscopic decompression, detorsion, and reduction of the volvulus → inspection of the mucosa for signs of ischemia [18]
- No signs of mucosal ischemia → placement of a soft rectal tube (for bowel decompression) → semi-elective surgery within 72 hours of detorsion
- Signs of mucosal ischemia → emergency surgery (see below)
- Signs of peritonitis/unsuccessful endoscopic detorsion → broad-spectrum IV antibiotics and emergency surgery [18]
-
No signs of peritonitis : rigid/flexible endoscopic decompression, detorsion, and reduction of the volvulus → inspection of the mucosa for signs of ischemia [18]
-
Surgery
- Sigmoid colectomy and primary anastomosis : indicated in hemodynamically stable patients with viable bowel [17]
- Hartmann procedure: indicated in hemodynamically unstable patients or those with ischemic/gangrenous bowel
Treatment of cecal volvulus [19]
- Initial resuscitation (See “Treatment” of sigmoid volvulus above.)
-
Surgery
- Hemodynamically stable patients: ileocecal resection or right colectomy with ileocolic anastomosis
-
Hemodynamically unstable patients
- Cecostomy [3][20]
- Detorsion with cecopexy [21]

© AMBOSS

Intraoperative photograph
Massively distended and twisted cecum with no apparent ischemic changes.
Source: “Figure 2, in: Cecal volvulus following mini gastric bypass: A case report and review of literature” by H. M. Alghamdi, S. AlShammary, H. Lardhi et al., Elsevier - International Journal of Surgery Case Reports, licensed under CC BY 4.0.
References
- Chalya PL, Mabula JB. "Sigmoid volvulus and ileo-sigmoid knotting: a five-year experience at a tertiary care hospital in Tanzania". World J Emerg Surg. 10. :10. (2015)
- Halabi WJ, Jafari MD, Kang CY, et al. "Colonic volvulus in the United States: trends, outcomes, and predictors of mortality". Ann Surg. 259(2). :293-301. (2014)
- Corman ML. "Colon and Rectal Surgery". Lippincott Williams & Wilkins. (2004). ISBN: 9780781740432
- Lou Z, Yu ED, Zhang W, et al. "Appropriate treatment of acute sigmoid volvulus in the emergency setting". World J Gastroenterol. 19(30). :4979-4983. (2013)
- Steele SR, Hull TL, Read TE, et al. "The ASCRS Textbook of Colon and Rectal Surgery". Springer. (2016). ISBN: 9783319259680
- Atamanalp SS, Ozogul B, Kisaoglu A. "Cecal volvulus: a rare cause of intestinal obstruction". Eurasian J Med. 44(2). :115-116. (2012)
- Kim SH, Shin SS, Jeong YY, et al. "Gastrointestinal tract perforation: MDCT findings according to the perforation sites". Korean J Radiol. 10(1). :63-70. (2009)
- Khurana B. "Signs in Imaging: The whirl sign". Radiology. 226(1). :69-70. (2003)
- Applegate KE, Anderson JM, Klatte EC. "Intestinal malrotation in children: a problem-solving approach to the upper gastrointestinal series". Radiographics. 26(5). :1485-1500. (2006)
- Yigit M, Turkdogan KA. "Coffee bean sign, whirl sign and bird's beak sign in the diagnosis of sigmoid volvulus". Pan Afr Med J. 19. :56. (2014)
- Jaffe T, Thompson WM. "Large-Bowel Obstruction in the Adult: Classic Radiographic and CT Findings, Etiology, and Mimics". Radiology. 275(3). :651-663. (2015)
- Gennari FJ, Weise WJ. "Acid-Base Disturbances in Gastrointestinal Disease". Clin J Am Soc Nephrol. 3(6). :1861-1868. (2008)
- Van den heijkant TC, Aerts BA, Teijink JA, Buurman WA, Luyer MD. "Challenges in diagnosing mesenteric ischemia". World J Gastroenterol. 19(9). :1338-1341. (2013)
- Tackett JJ, Muise ED, Cowles RA. "Malrotation: Current strategies navigating the radiologic diagnosis of a surgical emergency". World J Radiol. 6(9). :730-736. (2014)
- Rokade ML, Yamgar S, Tawri D. "Ultrasound “Whirlpool Sign” for Midgut Volvulus". J Med Ultrasound. 19(1). :24–26. (2011)
- Gingold D, Murrell Z. "Management of colonic volvulus". Clin Colon Rectal Surg. 25(4). :236-244. (2012)
- Katsikogiannis N, Machairiotis N, Zarogoulidis P, et al. "Management of sigmoid volvulus avoiding sigmoid resection". Case Rep Gastroenterol. 6(2). :293-299. (2012)
- "Sigmoid Volvulus: An Update". http://www.ptolemy.ca/members/archives/2009/Sigmoid/. [2017-03-28]
- Yeo CJ, Matthews JB, McFadden DW, Pemberton JH, Peters JH. "Shackelford's Surgery of the Alimentary Tract". Elsevier Saunders. (2012). ISBN: 9781437722062
- "Laparoscopic Treatment of Volvulus of the Colon, In: Laparoscopic Surgery, Saunders Co, 1994". http://www.lapsurgery.com/volvulus.htm. [2010-09-11]
- Ortega PM, Rotellar F, Arredondo J, et al. "Minimal invasive management of acute cecal volvulus: colonoscopy followed by laparoscopic cecopexy". Rev Esp Enferm Dig. 106(7). :497-499. (2014)