Summary
Skin and soft tissue infections (SSTIs) are a group of heterogeneous conditions affecting the epidermis, dermis, subcutaneous tissue, or superficial fascia. Uncomplicated infections are most commonly caused by gram-positive pathogens (Streptococcus, Staphylococcus) that infiltrate the skin after minor injuries (e.g., scratches, insect bites). Complicated infections have a higher tendency to be polymicrobial. SSTIs primarily manifest with painful, warm, erythematous skin lesions and may also lead to purulent fluid collections and/or necrosis of the affected tissue. Systemic symptoms like fever are usually a sign of more severe infections. Risk factors for developing SSTIs (or more severe forms of SSTIs) include diabetes mellitus, immunodeficiency, and chronic edema. Diagnosis is mostly clinical, but some patients may require imaging or laboratory studies. Purulent infections, such as abscesses, are primarily treated with incision and drainage, while nonpurulent infections (e.g., erysipelas, cellulitis) require antibiotic therapy. Necrotizing soft tissue infections (NSTIs) have a high mortality rate; they are a surgical emergency and require immediate wound debridement.

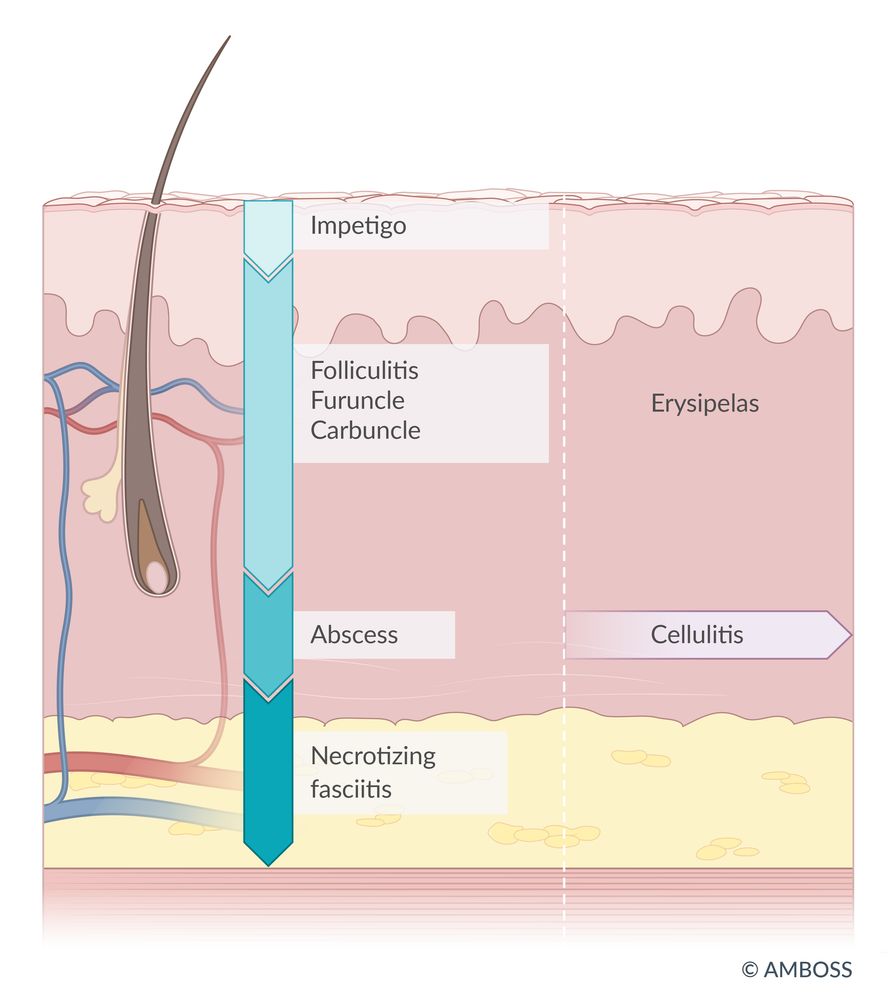
Schematic cross-section of common skin and soft tissue infections:
Impetigo contagiosa affects the upper epidermis.
Beneath this, in the dermis, are folliculitis, furuncles (boils), and carbuncles, as well as cutaneous abscesses.
Cellulitis spreads within the subcutis (subcutaneous tissue).
Erysipelas affects the dermis and subcutis but often manifests at a location distant from the portal of entry (e.g., an infection entering via a wound on the foot results in erysipelas on the lower leg).
In necrotizing fasciitis, the fascia is involved.
© AMBOSS
Overview
| Overview of skin and soft tissue infections | ||||
|---|---|---|---|---|
| Condition | Most common pathogens | Tissue involvement | Clinical features | |
| Impetigo |
|
|
|
|
| Staphylococcal scalded skin syndrome (generalized form of impetigo) |
|
|
|
|
| Nonpurulent SSTIs | Erysipelas |
|
|
|
| Cellulitis |
|
|
|
|
| Purulent SSTIs | Skin abscess |
|
|
|
| Folliculitis, furuncles, carbuncles |
|
|
|
|
| Necrotizing soft tissue infections |
|
|
|
|
Tissue involvement of SSTI (from superficial to deep): impetigo (superficial epidermis), erysipelas (superficial dermis and lymphatic vessels), cellulitis (deep dermis and subcutaneous tissue), necrotizing fasciitis (subcutaneous tissue including superficial and deep fascia)
Cardinal signs of inflammation
- Rubor = redness
- Calor = heat
- Tumor = swelling/edema
- Dolor = pain
- Functio laesa = loss of function
Risk factors for skin and soft tissue infections [1]
- Local factors
- Chronic lymphedema
- Local skin defects (e.g., tinea pedis)
- Circulatory disorders: arteriovenous insufficiency, chronic edema, stasis
- Peripheral neuropathy, paresis
- Systemic factors
- Diabetes mellitus
- Immunodeficiency (e.g., HIV infection, asplenia, chemotherapy)
- Chronic kidney disease (leading to, e.g., chronic edema, dialysis)
- Obesity, poor nutritional status
- Drug or alcohol use disorder
- Older and younger age
- Increased exposure to pathogens
- Nosocomial pathogens (e.g., prolonged hospitalization, surgery)
- Water exposure (e.g., sea water, hot tubs)
- IV drug use, long-term intravascular devices [2]
- Trauma (e.g., open wounds, exposed fractures)
Complications
- Local spread of infection
- Systemic involvement with fever and possible sepsis (see “Sepsis” for details on the management of severe infections)
- Spread of infection to distant sites (see “Staphylococcal infections”)

Multiple red papules of varying sizes are visible around the mouth and on the left cheek. The characteristic honey-colored crusts have, for the most part, been scratched off; remnants visible in the left corner of the mouth.
Source: © IMPP

Perioral, cervical and axillary reddening of the skin is visible, resulting in a scalded appearance on this child's face. In some areas, the superficial epidermal layer is detached (e.g., on the chin). On the right side of the neck, several flaccid blisters can be seen. The lips appear dry, with several rhagades in the corners of the mouth.
Source: Courtesy of Dr. Gary M. White, MD

Well-demarcated erythema is visible over the right side of the face, spreading to the helix and antihelix of the ear and mastoid process.
Source: © IMPP

A sharply demarcated erythematous rash with discrete narrowing extensions is visible on the lower leg of this patient.
Location and appearance of the lesion are typical of a bacterial infection with Group A Streptococcus affecting the upper dermis and lymphatic vessels.
Source: “Wundrose am Unterschenkel” by Failing79, Wikimedia Commons, licensed under CC BY-SA 4.0.
{kind=link}

Diffuse, poorly demarcated erythema and edema associated with small, crusted red patches are visible over the left leg.
These findings are consistent with cellulitis due to scabies infection.
© AMBOSS

There is marked erythema and swelling with pus and a large comedone.
Source: “File:Five day old Abscess.jpg” by Amrith Raj, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}

A solitary pustule with surrounding erythema is visible in the center of the image. In many cases of folliculitis, a single hair can be seen in the middle of the lesion.
Source: “Isolated folliculitis” by Jmarchn, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}

Two pustules with surrounding erythema can be seen emerging from the hair follicles.
Source: “Figure 5” by Regina E. Oladokun et al, Atlas of Paediatric HIV Infection, licensed under CC BY-ND 4.0.

Posterolateral aspect of the left thigh, gluteal region, and popliteal fossa
There is significant diffuse edema and erythema across the entire visible region, with well-defined areas of necrosis, desquamation, and hemorrhagic bullae.
These features are strongly suggestive of necrotizing fasciitis, a rapidly progressive infection of the skin, subcutaneous tissue, and superficial and deep fascia that requires urgent debridement.
Source: “Figure 1, in: Late diagnosed necrotizing fasciitis as a cause of multiorgan dysfunction syndrome: A case report” by Smuszkiewicz P, Trojanowska I, Tomczak H, BMC Cases Journal, licensed under CC BY 2.0.
Nonpurulent SSTIs
Definitions [3][4]
- Erysipelas: superficial skin infection involving the upper dermis
- Cellulitis: local infection of the deep dermis and subcutaneous tissue
Clinical features [3][4]
-
Local signs: erythema, edema, warmth, tenderness
- Specific to erysipelas: raised, sharply demarcated lesion
- Specific to cellulitis: poorly defined lesion with induration
- Cutaneous lymphatic edema (historically referred to as “peau d'orange”)
- Common locations: lower limbs, face
- Possible additional features
- Lymphangitis: red streaks radiating from the skin lesion and following the direction of the lymphatic vessels
- Lymphadenitis: swollen, tender, regional lymph nodes
- Bullae
- Purulent exudate
- Systemic symptoms (in moderate/severe infections): fever, chills, confusion, nausea, headache, muscle and joint pain
Bilateral cellulitis is exceedingly rare. Patients presenting with bilateral leg erythema should also be evaluated for alternative diagnoses, including stasis dermatitis and lymphedema. [5]
Pathophysiology [3][4]
- Entry is commonly via a minor skin injury ; erysipelas can consequently spread via superficial lymphatic vessels.
- May also be secondary to a systemic infection
In both erysipelas and cellulitis, the most common point of entry for the pathogen is a small skin lesion (e.g., interdigital tinea pedis).
Etiology [3][4]
- Beta-hemolytic streptococci: mostly group A Streptococcus (S. pyogenes)
- Less common pathogens for cellulitis
- S. aureus
- Pasteurella multocida (gram-negative, encapsulated coccobacillus): secondary to dog and cat bites
GAS is the most common cause of nonpurulent skin and soft tissue infections (i.e., erysipelas, cellulitis).
Diagnostics [3][6]
Diagnosis is usually clinical. In patients with systemic symptoms, laboratory studies, cultures, and imaging may be indicated to assess severity and tailor treatment.
-
Laboratory studies
- CBC: possible leukocytosis
- BMP: signs of underlying conditions that are risk factors for infections (e.g., diabetes mellitus, chronic kidney disease)
- Inflammatory markers; (e.g., CRP, procalcitonin): may be elevated
-
Imaging
-
Soft tissue ultrasound
- Indication: consider if there is suspicion for skin abscess and/or foreign body (see “Purulent SSTI” section)
- Findings: hypoechoic strands (signs of edema) between subcutaneous fat tissue [7]
- CT/MRI with or without IV contrast: consider if there is concern for complications (e.g., pyomyositis, osteomyelitis) [6]
-
Soft tissue ultrasound
-
Microbiology: Gram stain and cultures are not routinely recommended. [3]
- Consider skin biopsy, aspirate, and/or blood cultures in patients with the following: [3]
- Malignancy or patients receiving chemotherapy
- Neutropenia
- Severe immunodeficiency
- Immersion injuries
- Animal bites
- Consider skin biopsy, aspirate, and/or blood cultures in patients with the following: [3]
Treatment of nonpurulent SSTIs [1][3][8]
General principles
- Empiric antibiotic therapy active against streptococci and S. aureus is the mainstay of treatment for nonpurulent SSTIs.
- Treatment should also include the control of any predisposing factors (e.g., edema, fungal infections).
- The majority of patients with cellulitis or erysipelas are clinically stable and can be managed as outpatients.
- Patients with systemic symptoms often require hospitalization and parenteral antibiotic therapy.
- See “Sepsis” for further details on the management of severe infections.
Antibiotic therapy
- Systemic antibiotic therapy is usually required.
- Empiric regimens should usually cover Streptococcus spp. and S. aureus (see “Empiric antibiotic therapy for nonpurulent SSTIs” for detailed recommendations).
- Consider inpatient management with parenteral antibiotics for patients with any of the following:
- Systemic symptoms
- Suspicion for deeper infection
- Immunocompromise
- Failure of outpatient treatment. [3]
- Consider coverage for MRSA in the following cases:
- Penetrating trauma
- Evidence of MRSA infection or colonization elsewhere
- Injection drug use
- Purulent drainage
- SIRS
Antibiotics should be targeted against gram-positive pathogens and provide broad-spectrum coverage in severe cases. [4]
Supportive care
- Elevation of the affected limbs
- Rest and acute pain management as needed
Acute management checklist for nonpurulent SSTI
- Stabilize the patient as needed.
- Consider indications for laboratory studies and imaging.
- Start empiric antibiotic therapy according to recommendations for severity and risk factors (see “Empiric antibiotic therapy for nonpurulent SSTIs”).
- Provide supportive care (limb elevation, pain management).
- Identify and treat the underlying cause, if present (e.g., tinea pedis, poorly controlled diabetes).
- Consider indications for admission/inpatient management.
Subtypes and variants
Perianal streptococcal dermatitis [9][10][11]
- Definition: : an infection of the perianal skin with group A Streptococcus characterized by pain, pruritus, and rash
- Epidemiology: Most common in children between 6 months and 10 years of age
- Etiology: group A Streptococcus infection
-
Clinical features
- Signs of systemic infection are rare
- Pruritus, rectal pain, blood-streaked stools
- Sharply demarcated, erythematous perianal rash with pseudoexudate, crusting, and/or superficial anal fissures/cracks
- Diagnosis: Rapid strep and culture of the perianal region
-
Differential diagnosis
- See “Overview of diaper dermatitis.”
- See “Differential diagnoses of diaper dermatitis.”
-
Treatment [10][11] [12]
- Amoxicillin for 10 days; preferred in children [10][12]
- Alternatives: penicillin V and clindamycin; see “Empiric antibiotic therapy for nonpurulent SSTIs” for dosage information
If the rapid strep test of the perianal region is negative, consider treating for perianal staphylococcal infection, as the manifestation is identical. [9]
Other
- Orbital cellulitis; periorbital (preseptal) cellulitis
- Ludwig angina
Complications [3][4]
- Recurrent infections
- Abscess
- Infection of deeper tissues: cellulitis, necrotizing fasciitis, osteomyelitis
- Thrombophlebitis, lymphedema
- Systemic complications (e.g., sepsis, endocarditis, streptococcal toxic shock syndrome, poststreptococcal glomerulonephritis, acute rheumatic fever)
- In orbital cellulitis: blindness, cavernous sinus thrombosis, intracranial abscess










Well-demarcated erythema is visible over the right side of the face, spreading to the helix and antihelix of the ear and mastoid process.
Source: © IMPP
A sharply demarcated erythematous rash with discrete narrowing extensions is visible on the lower leg of this patient.
Location and appearance of the lesion are typical of a bacterial infection with Group A Streptococcus affecting the upper dermis and lymphatic vessels.
Source: “Wundrose am Unterschenkel” by Failing79, Wikimedia Commons, licensed under CC BY-SA 4.0.
Diffuse, poorly demarcated erythema and edema associated with small, crusted red patches are visible over the left leg.
These findings are consistent with cellulitis due to scabies infection.
© AMBOSS

A well-demarcated wound covered with granulation tissue is visible on the patient's palm. The adjacent erythema extends to the forearm in flat, erythematous streaks along the course of lymphatic vessels.
These features are characteristic of lymphangitis with the source of infection likely being the present wound.
Source: “File:CellulitisJmh649.JPG” by James Heilman, MD, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}
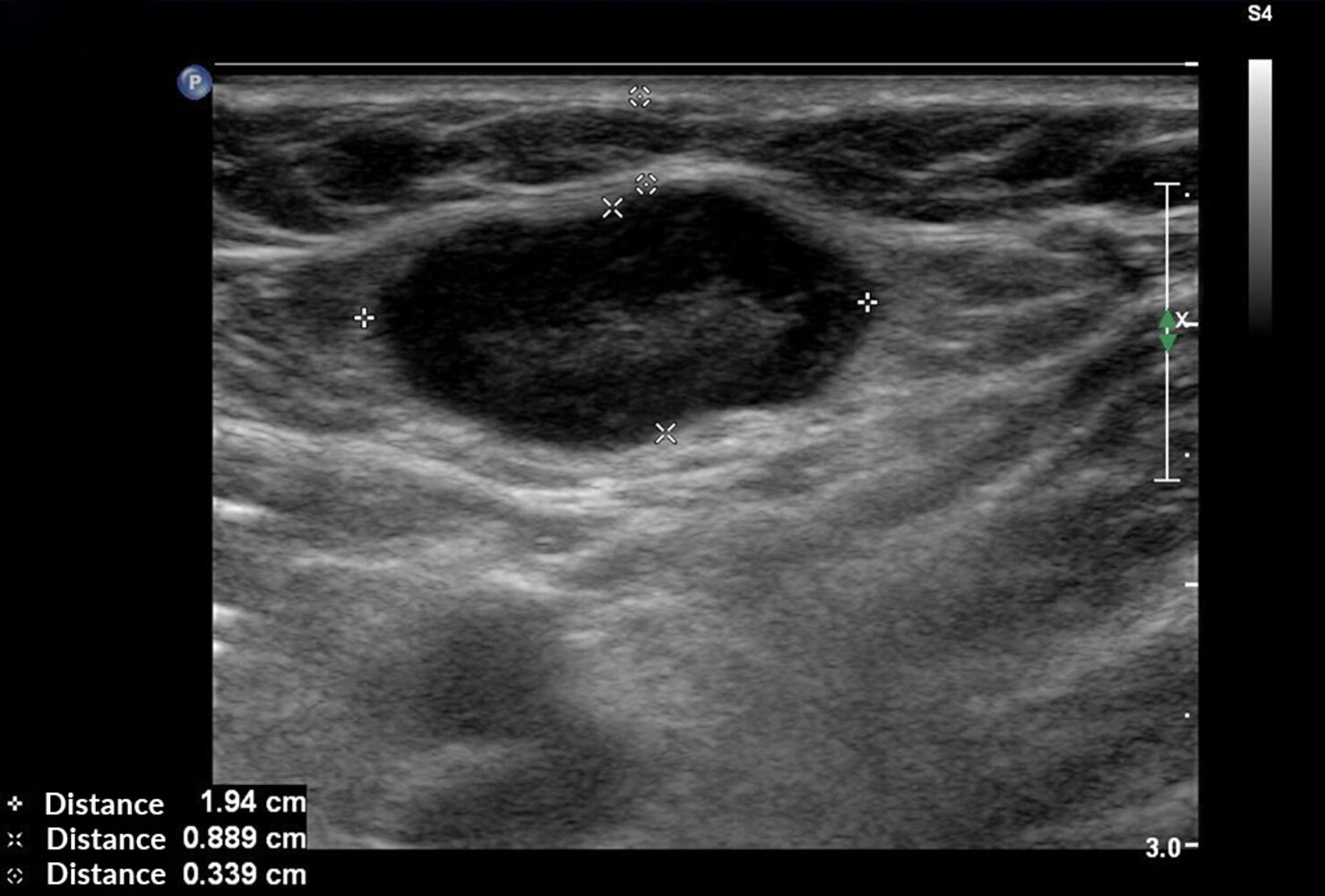
Ultrasound inguinal lymph node (longitudinal plane) of a patient with erysipelas
A superficial lymph node (green overlay) measuring 1.9 x 0.9 cm is more hypoechoic than normal. The node has maintained an oval shape and well-demarcated margins.
Image source of original image: sonographiebilder.de - Innere Medizin des Albertinen-Krankenhauses Hamburg. Original title: “Borreliose_Lk”. Created by: Dr. J. Guntau. Modifications to original image: text removed.

Extensive, sharply demarcated erythema with swelling, bullae, and necrosis is visible on the right anterior distal forearm and wrist.
Source: © IMPP

Extensive, sharply demarcated erythema can be seen on the left breast. Cracked skin at the lower edge of the areola is also visible.
Source: © IMPP

A well-demarcated area of erythema on the left posterior forearm with one large blister and several smaller blisters can be seen. Some mild edema is also visible around the affected areas.
These findings are consistent with erysipelas, a superficial skin infection.
© AMBOSS

Erythema with several blisters can be seen over the posterior aspect of the forearm, particularly localized around the elbow. There is marked edema surrounding the affected area.
These findings are consistent with erysipelas, a superficial skin infection.
© AMBOSS

The left upper and lower eyelids are red and severely swollen, resulting in the patient not being able to open the eye. Orbital cellulitis is an emergency requiring immediate treatment.
Image source of original image: www.paediatrie-in-bildern.de. Created by: Dr. Thomas Rautenstrauch.
Purulent SSTIs
Folliculitis, furuncles, and carbuncles [3]
-
Definitions
- Folliculitis: localized inflammation of the hair follicle (or sebaceous glands) that is limited to the epidermis
- Hot tub folliculitis: pseudomonal folliculitis that appears 8–48 hours after exposure to contaminated water; usually a self-limiting condition that does not require antibiotic treatment
- Furuncle: deep folliculitis beyond the dermis with abscess formation in the subcutaneous tissue
- Carbuncle: confluent folliculitis that forms an inflammatory mass; abscess and skin necrosis may be present
-
Clinical features
- Tender papules and/or pustules, often pruritic
- Located at the site of hair follicles
- Possible pus drainage from follicular orifices
- Potentially multiple lesions
- Variable locations (e.g., carbuncles most often develop on the back of the neck)
-
Differential diagnoses
- Ecthyma
- Acne vulgaris
- Eosinophilic folliculitis
Facial furuncles can result in severe complications (e.g., periorbital cellulitis, cavernous sinus thrombosis).








Skin abscess [3][4]
- Definition: an accumulation of white-yellow pus that contains proteins, leukocytes (especially neutrophils), bacteria, and cellular debris and is located in the dermis and subcutaneous tissue
-
Clinical features
- Cardinal signs of inflammation
- Painful, tender, and fluctuant red nodules
- Pain is usually relieved after rupture or drainage.
- May be surrounded by erythema and induration.
- Differential diagnosis: inflamed epidermoid cyst, carbuncle
-
Subtypes and variants
- Recurrent skin abscess: a new abscess at the site of a previous infection
- Complex skin abscess: a skin abscess that requires specialized treatment because of its location (e.g., perianal, perirectal), the pathogens involved (e.g., polymicrobial, resistant pathogens), or patient characteristics (e.g., immunodeficiency) [4]
-
Scrotal abscess: a subcutaneous collection of pus in the scrotal region, usually a result of inflamed hair follicles
- Differential diagnoses: neoplasia of the testis, infected hydrocele, genital warts
- May progress to fournier gangrene.
In both scrotal abscess and epididymitis, the classic signs of inflammation are prominent and help to confirm the diagnosis.




Etiology [3]
- S. aureus: most common pathogen for any form of purulent SSTI; MRSA is frequently identified. [13][14]
- Streptococcus spp. [15]
- P. aeruginosa (e.g., hot tub folliculitis)
- Polymicrobial (e.g., anaerobes or gram-negative bacteria, especially in complex abscesses)
- Noninfectious causes (e.g., ingrown hairs, friction, trauma, or occlusion)
- Fungi (rare): Candida albicans or Malassezia (particularly M. furfur)
Diagnostics [1][3]
Diagnosis is usually clinical. In patients with systemic symptoms, laboratory studies, cultures, and imaging may be indicated to assess severity and tailor treatment.
-
Laboratory studies
- CBC: possible leukocytosis
- BMP: signs of underlying conditions that are risk factors for infections (e.g., diabetes mellitus, chronic kidney disease)
- Inflammatory markers; (e.g., CRP, procalcitonin) may be elevated
-
Imaging [6]
-
Soft tissue ultrasound
- Indications include:
- Systemic signs of infection (i.e., moderate or severe disease)
- Confirmation of diagnosis prior to incision and drainage of an abscess
- Assessment of size, extent, and depth of the abscess [16][17]
- Suspected foreign object at the site of infection (e.g., needle tip, splinter)
- Suspected complex skin abscess
- Possible findings [7]
- Skin abscess: hypoechoic, heterogeneous fluid collection with posterior enhancement
- Surrounding edema (especially in accompanying cellulitis)
- Indications include:
- CT/MRI with or without IV contrast: usually only necessary for complex skin abscesses (e.g., perianal abscess) and the evaluation of complications (e.g., osteomyelitis)
-
Soft tissue ultrasound
-
Microbiology
- Gram stain and cultures are not routinely recommended, even if CA-MRSA is suspected. [1][3][13]
-
Indications for abscess and blood cultures include:
- Systemic symptoms, severe infections (see “Severity of SSTI”)
- Immunocompromised patients
- Recurrent skin abscess
- Carbuncles
-
Additional evaluation: Consider additional evaluation for underlying conditions in patients with recurrent abscess and/or complex skin abscess.
- Colonization with resistant pathogens (e.g., MRSA)
- Local causes (e.g., foreign body, pilonidal cyst, hidradenitis suppurativa)
- Systemic predisposing conditions (e.g., neutrophil disorders)

Treatment of purulent SSTIs
General principles
- Incision and drainage are the mainstay of treatment for purulent SSTIs and are usually sufficient for mild infections.
- Patients with systemic signs of infections require empiric antibiotic therapy.
- Outpatient management is appropriate for clinically stable patients.
- Consider inpatient management for patients with systemic symptoms.
- See “Sepsis” for more details on the management of severe infections.
Interventional therapy [3][4]
-
Incision and drainage (I&D)
- Bedside procedure
- Indications: small skin abscesses carbuncles, large furuncles , inflamed epidermoid cysts
- See “Abscess incision and drainage” for detailed procedural guidance.
-
Surgical drainage
- Usually performed in the OR
- Indications can include:
- Recurrent skin abscesses
- Multiple abscesses (may be associated with fistulas)
- Size > 5 cm
- High-risk anatomical location
- Suspected mycotic or mycobacterial abscess
- Comorbidities that increase the risk of complications (e.g., coagulopathy)


Antibiotic therapy [3][4]
- Topical antibiotics: Consider in MRSA folliculitis (e.g., mupirocin ). [1]
-
Systemic antibiotic therapy for purulent SSTIs: Usually not indicated after successful drainage in otherwise healthy individuals. [3][4][18][19]
- Indications: moderate/severe infections, recurrent or complex abscesses, according to risk factors and comorbidities (e.g., diabetes mellitus)
- Regimens often include coverage for MRSA (see “Empiric antibiotic therapy for purulent SSTIs” for detailed recommendations).
Mild purulent skin infections usually do not require systemic antibiotic treatment following drainage.
Supportive measures
- Warm compresses (in folliculitis, furuncles, and carbuncles)
- Rest and acute pain management as needed
- Keep the affected area clean and dry. [7]
- Consider MRSA decolonization for recurrent abscesses. [20]
Acute management checklist for moderate and severe purulent infections
- Stabilize the patient as needed.
- Complete labs and imaging (e.g., soft tissue ultrasound or CT) based on initial results, extension, and location.
- Consider surgery consult if concern for large abscess or severe infection.
- Incision and drainage if indicated; Consider sending fluid samples for Gram stains and cultures.
- Start empiric antibiotic therapy according to recommendations for severity and risk factors (see “Empiric antibiotic therapy for purulent SSTIs”).
- Provide symptomatic treatment (e.g., pain management, warm compresses).
- Consider indications for admission/inpatient management.
A solitary pustule with surrounding erythema is visible in the center of the image. In many cases of folliculitis, a single hair can be seen in the middle of the lesion.
Source: “Isolated folliculitis” by Jmarchn, Wikimedia Commons, licensed under CC BY-SA 3.0.

Multiple pustules with surrounding erythema can be seen emerging from the hair follicles.
Source: “Folliculitis2” by Da pacem Domine, Wikimedia Commons, licensed under CC0 1.0.
{kind=link}
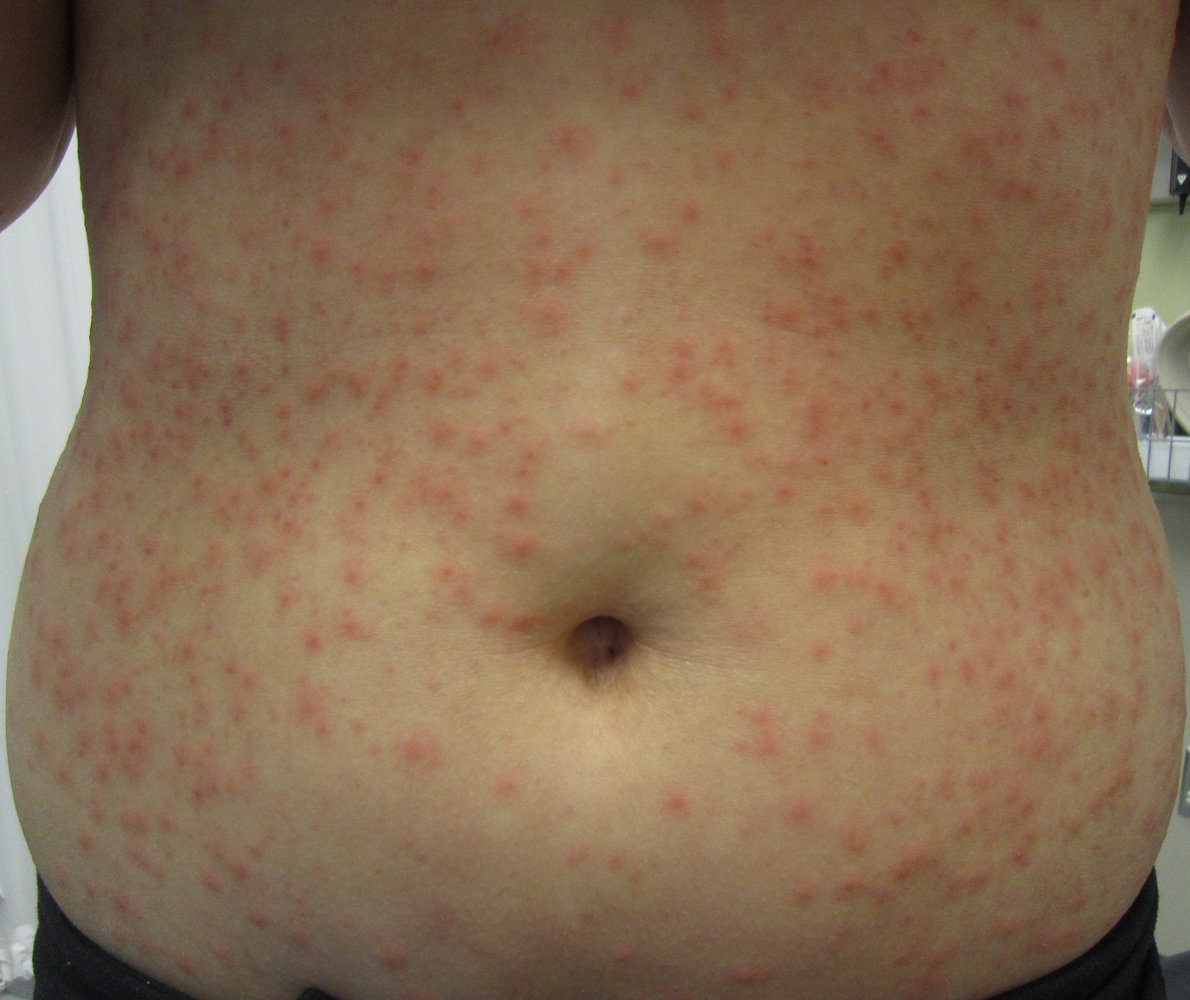
There is a diffuse distribution of erythematous papules across the abdomen.
This appearance is consistent with folliculitis caused by community-acquired skin infection with Pseudomonas aeruginosa.
Source: “Folliculitis” by James Heilman, MD, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}

Thigh of a male patient
A solitary purulent lesion surrounded by erythematous and edematous skin is visible.
This is the typical appearance of a furuncle, an acute deep bacterial infection of a single hair follicle.
Source: “Furoncle” by Mahdouch, Wikimedia Commons, licensed under CC BY 1.0.
{kind=link}

A large, inflammatory, subcutaneous mass can be seen over the right gluteal region. The mass is composed of tightly clustered suppurative furuncles (boils), resulting in a sieve-like appearance on the surface.
This is the characteristic appearance of a carbuncle.
Source: “Carbuncle_on_buttok” by Drvgaikwad, Wikimedia Commons, licensed under CC BY 3.0.
{kind=link}

Right scapular region
There is a large, erythematous nodule with multiple pustules and purulent sinuses visible on its surface.
Source: © IMPP

An erythematous, swollen nodule is visible on the upper arm.
The abscess formation appears bulging. During its further development, the painful mass will typically open up and drain off.
Source: “Figure 7, in: Atlas of Paediatric HIV Infection” by Regina E. Oladokun; Rannakoe J. Lehloenya; Carol Hlela; Agozie C. Ubesie; Sherifat O. Katibi; Ombeva O. Malande; Brian S. Eley, Openbooks, licensed under CC BY-ND 4.0.

An eruption of pruritic, erythematous, and perifollicular papules and pustules is visible. The lesions are well-defined and occur discretely.
These findings represent the clinical manifestation of eosinophilic folliculitis. Histology confirms the diagnosis.
Source: “Figure 63, In: Atlas of Paediatric HIV Infection” by Regina E. Oladokun, Rannakoe J. Lehloenya, Carol Hlela et.al., Openbooks, licensed under CC BY-ND 4.0.
There is marked erythema and swelling with pus and a large comedone.
Source: “File:Five day old Abscess.jpg” by Amrith Raj, Wikimedia Commons, licensed under CC BY-SA 3.0.

There is a prominent area of erythema and swelling on the left buttock and perianal region.
This is the typical appearance of an anal abscess.
Source: “Perianalabszess 01” by Dr. K.-H. Günther, Wikimedia Commons, licensed under CC BY 3.0.
{kind=link}

There is a large, circular, erythematous swelling with a central purulent lesion located in the lateral elbow flexure.
© AMBOSS

© Massachusetts Medical Society. All rights reserved. AMBOSS SE, exclusive licensee.
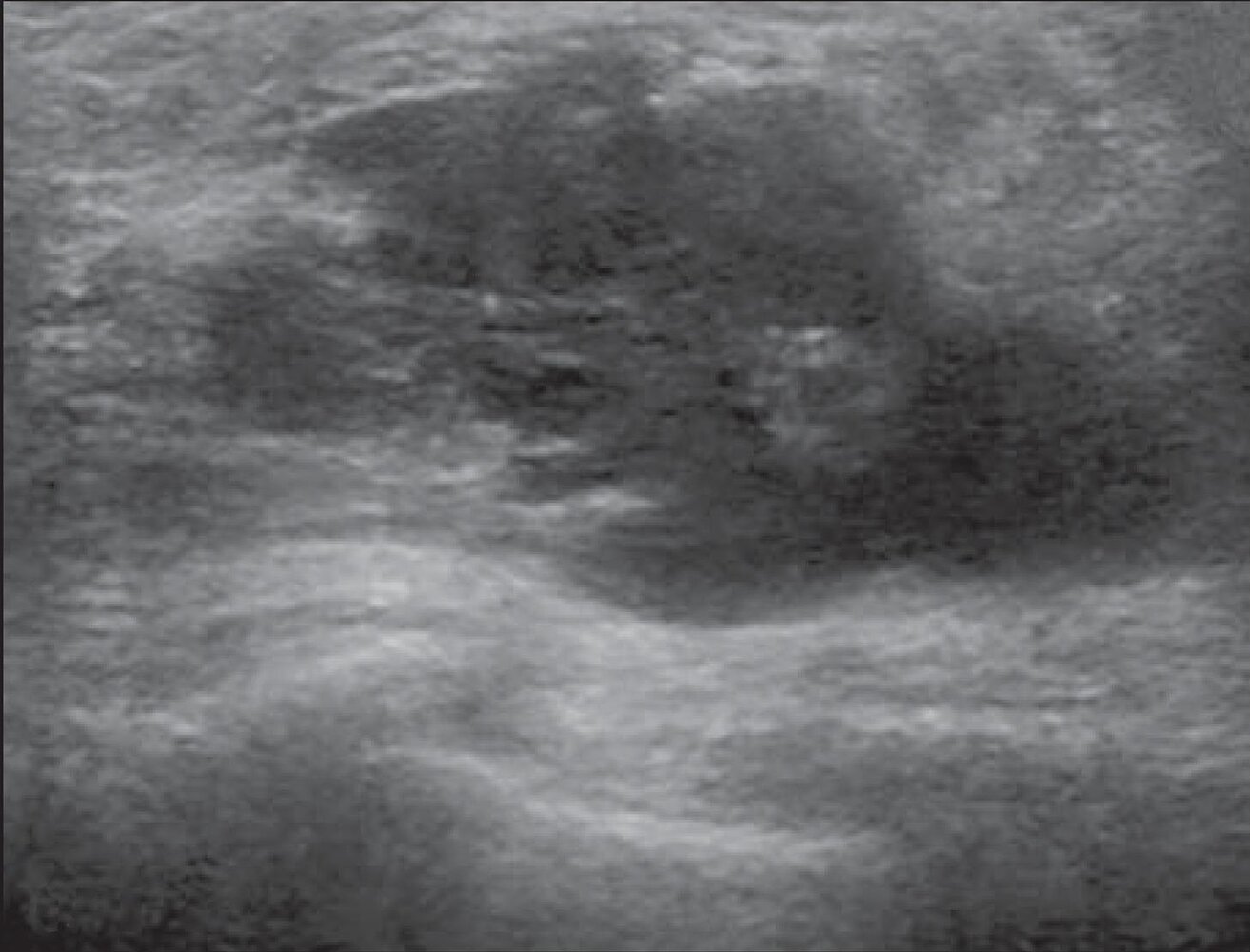
Ultrasound breast of a patient with fever, chills, and breast erythema
The long axis of the lobulated complex lesion (green overlay) is oriented parallel to the skin. The lesion is predominantly hypoechoic and demonstrates posterior acoustic enhancement (PAE; indicated by dashed lines).
Malignant lesions may demonstrate these features, although the patient history suggests that abscess is the most likely diagnosis. Common features of malignant lesions include spiculation, angular margins, taller-than-wide orientation, posterior acoustic shadowing, and microcalcifications. Abscesses are often ill-defined and may show central hypoechoic areas, debris, internal septations, posterior acoustic enhancement, eccentrically thickened walls, and increased mural Doppler flow without internal color Doppler flow.
Source: “Fig 4A, In: Ultrasound findings of the physiological changes and most common breast diseases during pregnancy and lactation” by de Holanda AAR, da Silveira Gonçalves AK, de Medeiros RD, de Oliveira AMG, de Oliveira Maranhão TM, SciELO, licensed under CC BY 4.0. Modifications: removal of the A. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
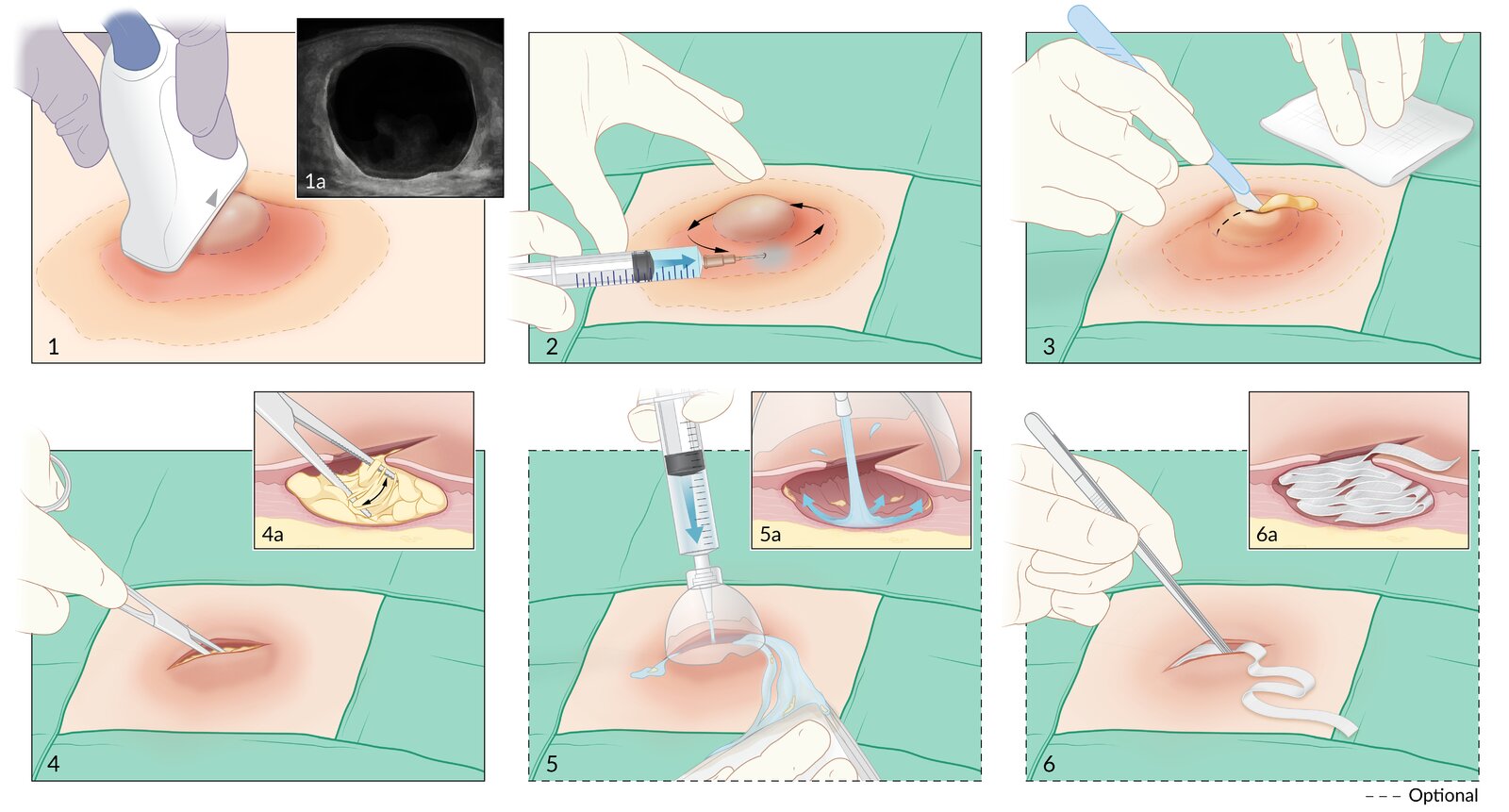
1. The abscess is identified using clinical examination or bedside ultrasound (1a).
2. The abscess is anesthetized by injecting local anesthetic.
3. A linear incision is made along the length of the abscess allowing the pus to drain.
4. A clamp is used to bluntly dissect the abscess cavity to break up loculations.
Optional steps
5. The abscess cavity is irrigated with sterile normal saline.
6. Forceps are used to loosely pack the abscess cavity with ribbon gauze, with a short tail left outside.
© AMBOSS. See related article for detailed procedural guidance.

Original title: “Guiding incision and drainage with ultrasound”. Created by: Medmastery.
Necrotizing soft tissue infections (NSTIs)
Definitions [3][4]
- Necrotizing soft tissue infection (NSTI): an aggressive, life-threatening infection involving necrosis of the tissue. Superficial and/or deep tissue may be affected (i.e., necrotizing cellulitis, necrotizing fasciitis, necrotizing myositis).
- Necrotizing fasciitis (most common NSTI): a rapidly progressive infection resulting in extensive necrosis of superficial and deep fascia and overlying subcutaneous fat that can develop into a life-threatening condition within hours
- Fournier gangrene: Necrotizing fasciitis of the external genitalia that can spread rapidly to the anterior abdominal wall and gluteal muscles.
- Clostridial myonecrosis: a rapidly spreading necrotizing infection caused by Clostridium perfringens or Clostridium septicum (see “Gas gangrene” for details)

Etiology [3][4]
- Aerobic and anaerobic, gram-positive and gram-negative bacteria are frequently isolated.
-
Both monomicrobial and polymicrobial causes are common. ; [4][21]
- Polymicrobial: wide variety; of aerobic and anaerobic pathogens, often of intra-abdominal or genitourinary origin (E. coli, Bacteroides spp.)
- Monomicrobial: commonly group A Streptococcus (S. pyogenes), Peptostreptococcus spp., S. aureus
- Fournier gangrene: usually mixed infection with facultative pathogens (E. coli, Klebsiella, Enterococcus) and anaerobic bacteria
The only way to definitively establish the causative pathogen is by obtaining a deep tissue culture (i.e., during surgical exploration). Clinical features alone are not reliable enough to distinguish between pathogens.
Clinical features [3][4]
- Systemic symptoms: fever, chills, altered mental status
- Cutaneous findings
- Diffuse erythema (often manifests initially as suspected cellulitis that is not responding to initial antibiotic therapy)
- Extreme tenderness and pain out of proportion to the area of erythema
- Significant induration of the subcutaneous tissue
- Crepitus: due to the production of methane and CO2 by bacteria
- Purple skin discoloration; (skin necrosis, ecchymosis)
- Bullae
- Loss of sensation in the affected area (paresthesias)
Necrotizing fasciitis first spreads along the fascia before spreading to the superficial cutaneous tissue. Local findings may, therefore, be unremarkable, with patients experiencing a disproportionate level of pain.
Red flags that suggest necrotizing deep tissue infection include the presence of crepitus, bullous lesions, skin necrosis, pain out of proportion to examination, and signs of systemic toxicity (especially altered mental status).


Diagnostics [3]
A definitive diagnosis is usually made during the visualization of the tissue during surgery.
Do not delay surgical consultation and definitive surgical intervention for imaging and laboratory studies.
-
Laboratory studies
- CBC: leukocytosis
- BMP: possibly hyperglycemia; renal function may be compromised
- Inflammatory markers (CRP, ESR; , procalcitonin): elevated
- CK: elevated
- Assess organ failure and severity.
-
Microbiology
- Blood cultures (2 sets)
- Gram stain and cultures from deep tissue [3]
-
Imaging: not routinely indicated and should not delay treatment [4][6]
-
CT/MRI with/without IV contrast ; [4]
- Gas in soft tissue
- Fascial thickening and edema
- Lack of contrast enhancement (confirms necrosis)
- Fluid collections on deep fascial planes
- Intermuscular septal edema
-
X-ray [4]
- May detect gas in soft tissue
- The absence of gas does not rule out NSTI.
- Ultrasound: can identify fluid accumulation and diffuse thickening of the deep tissue [4]
-
CT/MRI with/without IV contrast ; [4]
Superficial wound cultures may not accurately represent the pathogens found in deep tissue and should not be used to guide management.
Management [3][4]
- Admit all patients with suspected or confirmed NSTI to hospital for treatment.
-
If clinical features suggest NSTI, start immediate surgical and medical treatment.
- Surgical exploration with debridement (confirms the diagnosis and the mainstay of treatment)
- Broad-spectrum antibiotic therapy
-
Consult ICU for admission and aggressive supportive care for sepsis, if present. [3][4]
- Provide immediate hemodynamic support: e.g., fluid resuscitation, vasopressors
- Begin sepsis management.
- Consider respiratory support as needed, e.g., oxygen therapy, mechanical ventilation.
- Consider adjuvant therapy on an individual basis (e.g., hyperbaric oxygen, negative pressure wound therapy, intravenous immunoglobulin therapy).
Necrotizing soft tissue infections are a surgical emergency. Expedite and prioritize surgical exploration for diagnostic confirmation and debridement as much as possible!
Surgical exploration and debridement
- Procedure [4]
- Extensive exploration with surgical debridement (removal of necrotic tissue)
- Obtain deep tissue samples for Gram stain, cultures, and histopathology.
- Tissue with uncertain perfusion may be left for reassessment on a second intervention.
- Reexploration every 12–36 hours until there is no evidence of necrotic tissue
- Supportive findings
- Fascia appears swollen
- Dull gray fascia; areas of necrosis may be visible
- Possible brown exudate (no pus)
- Easy dissection of tissue planes with a blunt instrument or gloved finger
Antibiotic therapy [3][4]
- Start systemic, broad-spectrum antibiotic therapy immediately after blood cultures have been obtained.
- See “Empiric antibiotic therapy for NSTIs” for detailed recommendations.
- Consider polymicrobial infections (provide coverage against aerobes, anaerobes, MRSA).
- If there is evidence of toxic shock syndrome, include antitoxin active antibiotics (e.g., clindamycin, linezolid). [4]
Acute management checklist for necrotizing SSTI
- Stabilize the patient as needed (see “Sepsis” for more details on the management of severe infections).
- Consider the need for laboratory and imaging studies.
- Consult surgery, infectious diseases, and intensive care teams immediately.
- Urgent surgical exploration and debridement
- Send deep tissue samples for Gram stain and cultures.
- Aggressive and early empiric antibiotic therapy (see “Empiric antibiotic therapy for NSTIs”)
- Admit to intensive care unit.
- Reexploration every 12–36 hours
Complications
- Severe necrosis requiring amputation of the affected limb
- Sepsis
- Disseminated intravascular coagulation
- Organ dysfunction (e.g., acute kidney injury)
- Death: high mortality rate; even with adequate treatment (> 30%) [21]
Differential diagnoses
- Gas gangrene: caused by C. perfringens
- Severe SSTI without necrosis
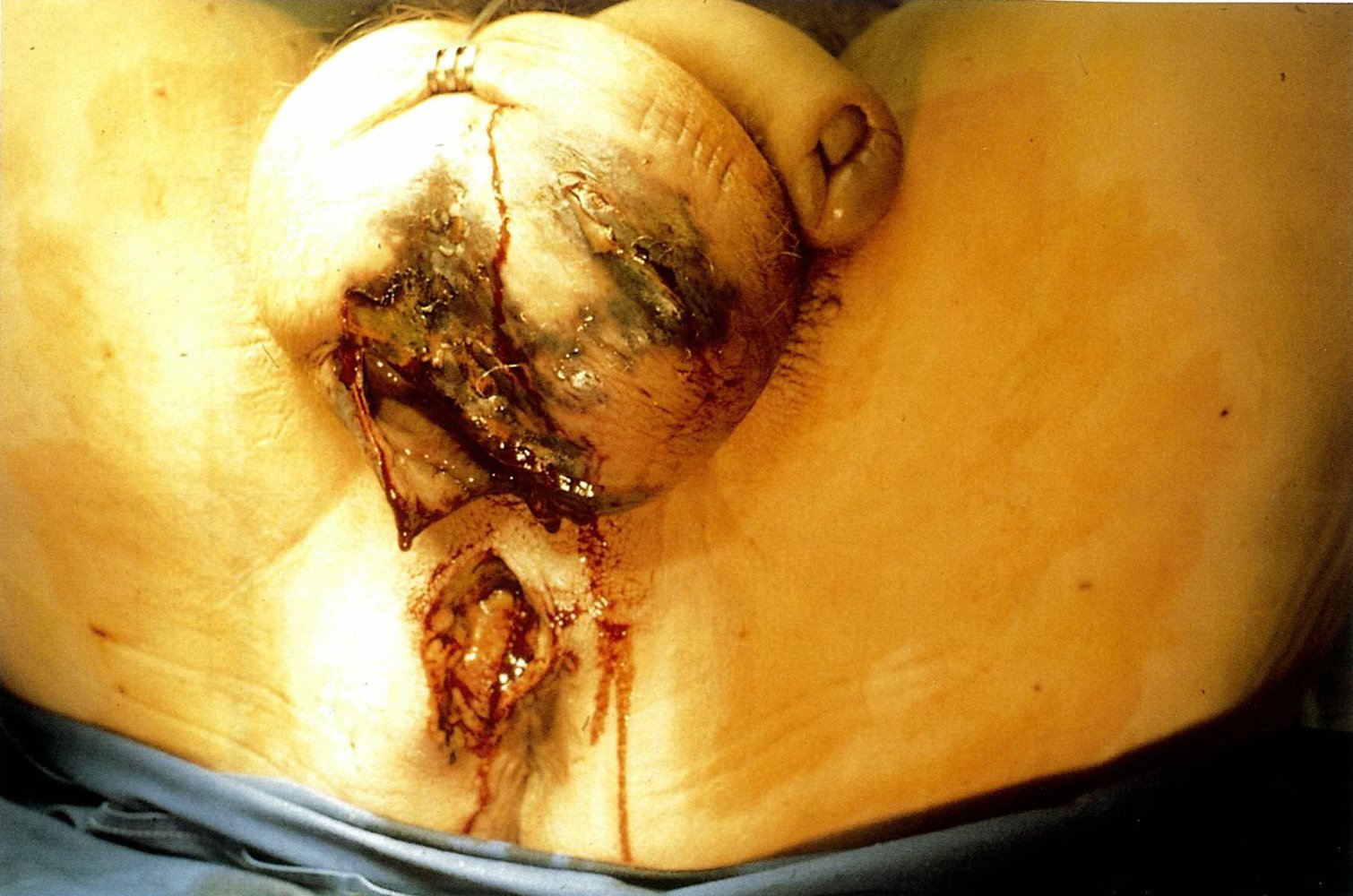
Necrotizing fasciitis of the perineal region
Source: © IMPP
Posterolateral aspect of the left thigh, gluteal region, and popliteal fossa
There is significant diffuse edema and erythema across the entire visible region, with well-defined areas of necrosis, desquamation, and hemorrhagic bullae.
These features are strongly suggestive of necrotizing fasciitis, a rapidly progressive infection of the skin, subcutaneous tissue, and superficial and deep fascia that requires urgent debridement.
Source: “Figure 1, in: Late diagnosed necrotizing fasciitis as a cause of multiorgan dysfunction syndrome: A case report” by Smuszkiewicz P, Trojanowska I, Tomczak H, BMC Cases Journal, licensed under CC BY 2.0.

Necrotic tissue with well-defined borders covers a large part of the child's skin surface. Slight erythema and affection of the deep fascia and subcutaneous tissue are also visible.
Although, in this case, the skin appears necrotic on the surface, this is not always the case and the skin surface may appear normal despite far-reaching necrosis underneath.
Source: “Figure 8a: Necrotizing fasciitis, in: Atlas of Paediatric HIV Infection” by Regina E. Oladokun; Rannakoe J. Lehloenya; Carol Hlela; Agozie C. Ubesie; Sherifat O. Katibi; Ombeva O. Malande; Brian S. Eley, Openbooks, licensed under CC BY-ND 4.0.
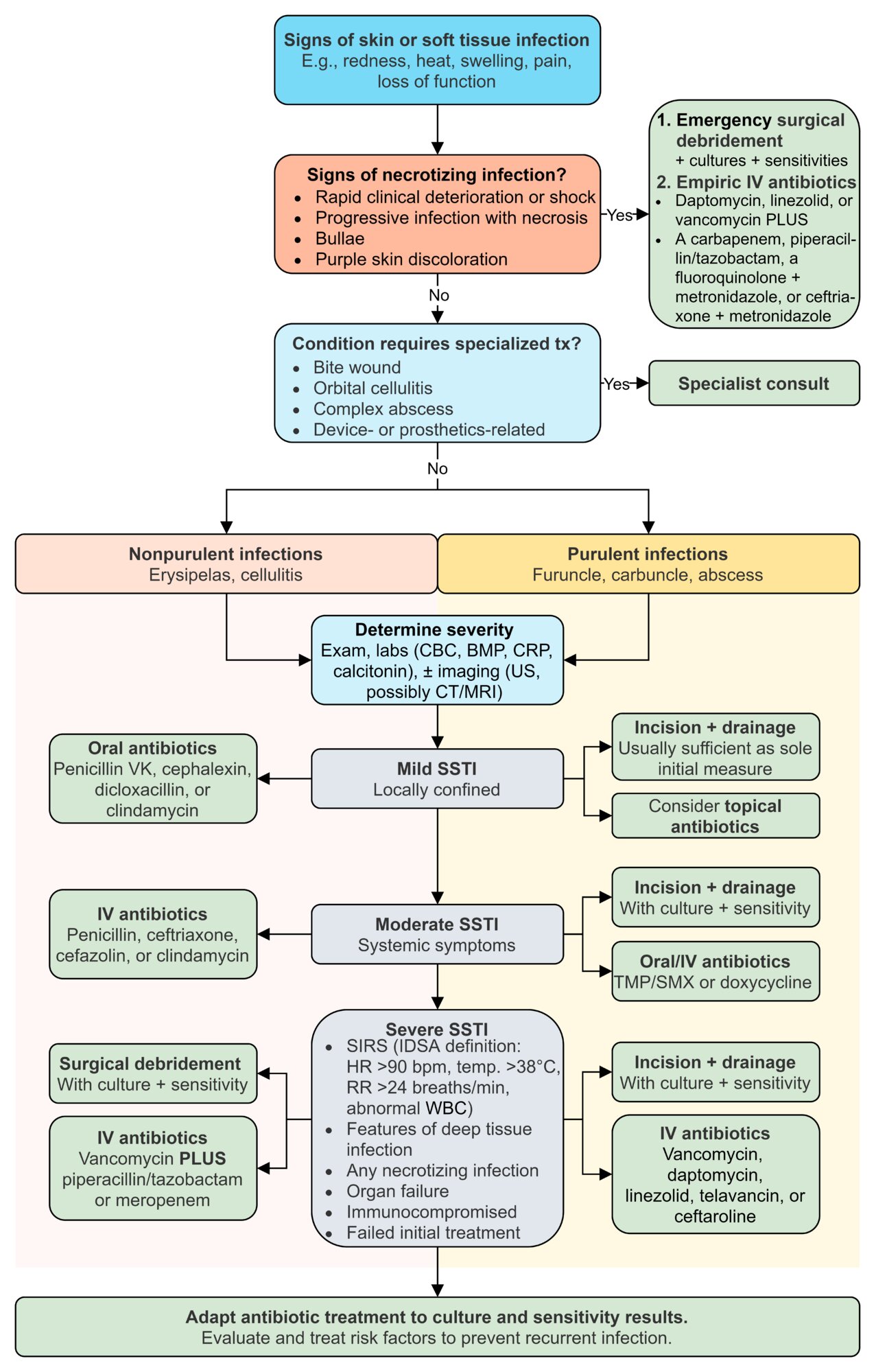
Management
Approach [3]
See the respective sections for details.
-
Patients with purulent or nonpurulent SSTI
- Determine SSTI severity.
- For purulent SSTI, perform incision and drainage.
- Start empiric antibiotic therapy for SSTI as indicated.
-
Patients with severe nonpurulent SSTI or NSTI
- Consult surgery for emergency surgical debridement with culture.
- Start empiric antibiotic therapy for SSTI.
- All patients: Adjust antibiotics based on culture and sensitivity results.

Severity of SSTI [3]
| SSTI severity grading [3] | ||
|---|---|---|
| Grade | Characteristics | |
| Mild SSTI |
|
|
| Moderate SSTI |
|
|
| Severe SSTI |
|
|
Necrotizing infections are always considered severe!
Empiric antibiotic therapy for SSTIs [3]
Adjust empiric antibiotics based on culture and sensitivity results.
- Choice of empiric antibiotic therapy should include the following factors:
- Severity (see “SSTI severity grading”)
- Presence of purulence
- Local resistance patterns
- Risk for complications
- Risk factors for skin and soft tissue infections
-
Variants that may require a more specialized treatment include:
- Bite wounds
- Recurrent or complex skin abscesses
- Orbital and periorbital cellulitis
- Device-associated infections (e.g., dialysis catheters, prosthetic joints)
- Patients at risk for endocarditis (e.g., patients with a prosthetic heart valve)
Individualize antibiotic regimen based on patient presentation and risk profile. Even patients with localized infections may require admission for IV antibiotic therapy.
© AMBOSS
Empiric antibiotic therapy for nonpurulent and purulent SSTIs
Perform incision and drainage or surgical drainage in patients with purulent SSTIs, and obtain cultures in patients with moderate and severe infections. [3]
Rule out necrotizing soft tissue infection in patients with severe nonpurulent SSTIs. Consider performing surgical exploration and obtaining samples for culture. [3]
Adults
| Empiric antibiotic therapy for nonpurulent and purulent SSTIs in adults (based on the 2014 IDSA guidelines) [1][3][4] | ||
|---|---|---|
| Nonpurulent SSTI | Purulent SSTI | |
| Mild infection |
|
|
| Moderate infection |
|
|
| Severe infection |
|
|
Children [11]
Antibiotic options in children are similar for nonpurulent and purulent SSTIs. Consult specialists for appropriate antibiotic therapy for neonates.
Mild to moderate infection
Duration of antibiotic therapy is usually 5–7 days; tailor duration based on response to treatment. [11]
-
Oral options
- Cephalexin [3][11]
- Trimethoprim/sulfamethoxazole (off-label) [3][11]
- Doxycycline [3][11]
- Clindamycin [3][11]
-
Intravenous options
- Cefazolin [3][11]
- Clindamycin [3][11]
- For nonpurulent infections only:
- Oxacillin (off-label) [3][11]
- Or nafcillin (off-label) [3][11]
In nonpurulent SSTI, trimethoprim/sulfamethoxazole, doxycycline, or clindamycin are recommended for patients with penicillin allergy. [11]
Severe infection
- Vancomycin (IV) [3][11]
- Linezolid (IV/PO) [3][11]
- Consult a specialist for other options (e.g., IV ceftaroline, IV daptomycin)
Empiric antibiotic therapy for NSTIs
NSTIs are always classified as severe infections. Consult surgery for immediate debridement and infectious diseases for antibiotic recommendations. [3][11]
Adults [1][3][4]
- Broad-spectrum intravenous combination therapy with one of the following (MRSA coverage):
- Daptomycin [1]
- Linezolid [1]
- Vancomycin [3]
- PLUS one of the following:
- A carbapenem (e.g., meropenem ) [3]
- Piperacillin/tazobactam [3]
- A fluoroquinolone (e.g., ciprofloxacin ) PLUS metronidazole [3]
- Ceftriaxone PLUS metronidazole [3]
- If linezolid is not part of the regimen, consider the addition of clindamycin to reduce the risk of TSS (antitoxin activity). [3][4]
Children [3][11]
- A β-lactam antibiotic, e.g., piperacillin/tazobactam (off-label) [3][11]
- PLUS clindamycin [3][11]
- Vancomycin may also be added.[3][11]
Dot phrase
Cellulitis (inpatient management, adult)
Assessment: This is a @AGE@-year-old @SEX@ presenting with [**erythema, warmth, swelling, tenderness] of the [**location] most consistent with cellulitis, likely caused by [**most likely pathogen (e.g., beta-hemolytic Streptococcus, S. aureus)]. Notable features include [**risk factors, systemic symptoms such as fever, chills, diabetes, immunosuppression].
Differential diagnoses: stasis dermatitis, lymphedema, necrotizing fasciitis [**excluded clinically or on imaging as appropriate], DVT.
Plan
Disposition: Inpatient admission for IV antibiotics and monitoring based on [**presence of systemic symptoms (e.g., fever, leukocytosis); immunosuppression or comorbidities (e.g., diabetes, chronic kidney disease); failed outpatient antibiotic therapy; suspicion of deep tissue infection or complication]
Monitoring and support
–Vital signs every 4–6 hours, including fever monitoring
–Monitor for clinical improvement or erythema progression.
Diagnostics (if not already performed)
–Blood tests: CBC, BMP, CRP, procalcitonin if sepsis is suspected
–Imaging: ultrasound (if abscess or DVT is suspected) or CT (if deeper infection or complications are suspected)
–Wound cultures or blood cultures if systemic symptoms are present
Empiric antibiotics targeting beta-hemolytic Streptococcus and MSSA
–Penicillin G 2–4 million units IV every 4–6 hours
–OR [Ceftriaxone 1–2 g IV once daily]
–OR [Cefazolin IV 1 g IV every 8 hours]
–OR [Clindamycin 600 mg IV every 8 hours]
MRSA coverage for [**penetrating trauma, IVDU, known MRSA colonization/infection, purulent drainage]
–Vancomycin 15 mg/kg IV every 12 hours
–OR [Daptomycin 4 mg/kg IV every 24 hours]
–OR [Linezolid 600 mg IV every 12 hours]
Consults: [**urgent general surgery consult for suspected necrotizing fasciitis]
Supportive care
–Elevate the affected limb.
–Pain management (e.g., acetaminophen or NSAIDs) PRN
–Management of [**tinea pedis or chronic lymphedema]
Reevaluation and discharge
–Monitor for 24–48 hours for treatment response.
–Discharge with oral antibiotics if there is improvement: cephalexin [OR clindamycin if MRSA risk].
–Provide education on monitoring symptoms
–Follow up with PCP in 2–5 days.
Cellulitis (outpatient management, adult)
Assessment: This is a @AGE@-year old @SEX@ presenting with [**erythema, warmth, swelling, and tenderness] of the [**location] most consistent with cellulitis, likely caused by [**most likely pathogen (e.g., beta-hemolytic Streptococcus or S. aureus)]. Infection is locally confined. No high-risk features [e.g., **risk factors or systemic symptoms such as fever, chills, diabetes, or immunosuppression] are present.
Differential diagnoses: stasis dermatitis, lymphedema, necrotizing fasciitis [**excluded clinically or on imaging as appropriate], DVT
Plan
Disposition: outpatient management
Empiric therapy targeting beta-hemolytic Streptococcus and MSSA
–Penicillin VK 250–500 mg PO every 6 hours for 10 days
–OR [Cephalexin 500 mg PO every 6 hours]
–OR [Dicloxacillin 500 mg PO every 6 hours]
–OR [Clindamycin 300–450 mg PO every 6 hours]
Supportive care
–Elevate the affected limb.
–Pain management (e.g., acetaminophen or NSAIDs) PRN
–Follow up [via tele or in person] in 2–5 days.
Differential diagnoses
Ecthyma gangrenosum
- Definition: an ulcerative lesion extending into the dermis that develops in the setting of bacteremia
- Pathogen: Pseudomonas aeruginosa (not pathognomonic but is the most common causative organism)
-
Pathophysiology
- Classically develops in patients with P. aeruginosa bacteremia who are immunocompromised
- Bacteria invade vasculature, causing septic vasculitis and cutaneous necrosis
-
Virulence factors destroy tissue:
- Exotoxin A: inhibits elongation factor 2, impairing protein synthesis
- Elastase: degrades elastin in blood vessel walls
- Phospholipase C: breaks down cell membranes
- Pyocyanin: produces damaging reactive oxygen species
-
Clinical features
- Rapid progression (within 12–18 hours) of painless red macules → induration, development of pustules, vesicles, and/or bullae → crusted ulcers
- Can involve skin or mucous membranes; anogenital and axillary areas most commonly involved
- Can be solitary or multiple
- Patients typically also systemically ill (e.g., septic shock)
- Diagnosis: primarily a clinical diagnosis
- Treatment: see treatment of skin and soft tissue infections



Erysipeloid
- Definition: cellulitis caused by Erysipelothrix rhusiopathiae
- Pathogen: Erysipelothrix rhusiopathiae, a gram-positive, capsulated bacilli that is found in a variety of animals including fish, shellfish, pigs, and birds
- Pathophysiology: infection usually acquired occupationally by contact with infected meat (enters through abrasions in the hand)
- Clinical features: warm, tender, well-demarcated, erythematous plaques (most commonly affects the hands)
- Treatment: penicillin
- Complications: sepsis, endocarditis
Other
-
Dermatological conditions [7][22]
- Acne vulgaris
- Atopic dermatitis
- Hidradenitis suppurativa
- Vascular malformations
-
Viral infections
- HSV infection (e.g., herpetic whitlow, eczema herpeticum)
- Shingles
-
Bacterial infections
- Lymphogranuloma venereum
- Cat scratch disease
- Verruga peruana
- Botryomycosis
- Fungal infections (e.g., sporotrichosis, kerion)
- Parasitic infections (e.g., scabies, myiasis, larva migrans)
The differential diagnoses listed here are not exhaustive.

Two purpuric erythematous patches are visible. The large lesion has a necrotic center with an erythematous halo. The smaller lesion at the bottom right may represent an earlier stage.
These lesions are suggestive of ecthyma gangrenosum, which is typically caused by an infection by pseudomonas aeruginosa.
Source: “Figure 1, in: Ecthyma Gangrenosum: Escherichia coli or Pseudomonas aeruginosa?” by M. Abbas, S. Emonet, T. Köhler et al., Frontiers in Microbiology - Infectious diseases, licensed under CC BY 4.0.

Gluteal region of a young child
Multiple crusted ulcerative lesions of varying sizes and depths are visible, some of which extend into the dermis.
Source: Courtesy of Dr. Gary M. White, MD

© Massachusetts Medical Society. All rights reserved. AMBOSS SE, exclusive licensee.

Multiple boil-like lesions with whitish edges and purple circumference are visible.
These lesions are suggestive of cutaneous tissue infested with fly larvae.
Source: “Figure 61b, In: Atlas of Paediatric HIV Infection” by Regina E. Oladokun, Rannakoe J. Lehloenya, Carol Hlela et.al., Openbooks, licensed under CC BY-ND 4.0.
External Resources
- 2020 (update) SIS Guidelines on the Management of Complicated SSTI
- 2018 WSES/SIS-E Consensus Conference: Recommendations for the Management of Skin and Soft-Tissue Infections
- 2017 ACR Appropriateness Criteria® for Suspected Osteomyelitis, Septic Arthritis, or Soft Tissue Infection (Excluding Spine and Diabetic Foot)
- 2014 IDSA Practice Guidelines for the Diagnosis and Management of Skin and Soft Tissue Infections
- 2011 IDSA Clinical Practice Guidelines for the Treatment of Methicillin-Resistant Staphylococcus Aureus Infections in Adults and Children
- 2009 IDSA Clinical Practice Guidelines for the Diagnosis and Management of Intravascular Catheter-Related Infection
References
- Ramakrishnan K, Salinas RC, Agudelo Higuita NI. "Skin and Soft Tissue Infections". Am Fam Physician. 92(6). :474-83. (2015)
- Mermel LA, Allon M, Bouza E, et al. "Clinical practice guidelines for the diagnosis and management of intravascular catheter-related infection: 2009 Update by the Infectious Diseases Society of America". Clin Infect Dis. 49(1). :1-45. (2009)
- Stevens DL, Bisno AL, Chambers HF, et al. "Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the Infectious Diseases Society of America". Clin Infect Dis. 59(2). :e10-52. (2014)
- Sartelli M, Guirao X, Hardcastle TC, et al. "2018 WSES/SIS-E consensus conference: recommendations for the management of skin and soft-tissue infections". World Journal of Emergency Surgery. 13(1). (2018)
- Committee on Infectious Disease, American Academy of Pediatrics. "Red Book: 2024-2027 Report of the Committee on Infectious Diseases, 33rd Edition". American Academy of Pediatrics. (2024). ISBN: 9781610027373
- Brook I, Frazier EH. "Clinical and microbiological features of necrotizing fasciitis.". J Clin Microbiol. 33(9). :2382-7. (1995)
- Expert Panel on Musculoskeletal Imaging:., Beaman FD, von Herrmann PF, et al. "ACR Appropriateness Criteria® Suspected Osteomyelitis, Septic Arthritis, or Soft Tissue Infection (Excluding Spine and Diabetic Foot)". J Am Coll Radiol. 14(5S). :S326-S337. (2017)
- Jameson JL, Fauci AS, Kasper DL, et al. "Harrison's Principles of Internal Medicine, Twentieth Edition (Vol.1 & Vol.2)". McGraw-Hill Education / Medical. (2018). ISBN: 9781259644030
- Walls R, Hockberger R, Gausche-Hill M. "Rosen's Emergency Medicine". Elsevier Health Sciences. (2018). ISBN: 9780323354790
- Raff AB, Kroshinsky D. "Cellulitis". JAMA. 316(3). :325. (2016)
- Chitalia VC, Kothari J, Wells EJ, et al. "Cost-benefit analysis and prediction of 24-hour proteinuria from the spot urine protein-creatinine ratio.". Clin Nephrol. 55(6). :436-47. (2001)
- Shin HT. "Diagnosis and Management of Diaper Dermatitis". Pediatr Clin North Am. 61(2). :367-382. (2014)
- Monika L. Dietrich, Russell W. Steele. "Group A Streptococcus". Pediatrics In Review. 39(8). :379-391. (2018)
- Brilliant LC. "Perianal streptococcal dermatitis". Am Fam Physician. 61(2). :391-3, 397. (2000)
- Miller LG, Quan C, Shay A, et al. "A Prospective Investigation of Outcomes after Hospital Discharge for Endemic, Community-Acquired Methicillin-Resistant and -Susceptible Staphylococcus aureus Skin Infection". Clinical Infectious Diseases. 44(4). :483-492. (2007)
- Klevens RM, Morrison MA, Nadle J, et al. "Invasive methicillin-resistant Staphylococcus aureus infections in the United States.". JAMA. 298(15). :1763-71. (2007)
- Summanen PH, Talan DA, Strong C, et al. "Bacteriology of Skin and Soft-Tissue Infections: Comparison of Infections in Intravenous Drug Users and Individuals with No History of Intravenous Drug Use". Clinical Infectious Diseases. 20(Supplement_2). :S279-S282. (1995)
- Talan DA, Moran GJ, Krishnadasan A, et al. "Subgroup Analysis of Antibiotic Treatment for Skin Abscesses". Ann Emerg Med. 71(1). :21-30. (2018)
- Daum RS, Miller LG, Immergluck L, et al. "A Placebo-Controlled Trial of Antibiotics for Smaller Skin Abscesses". N Engl J Med. 376(26). :2545-2555. (2017)
- Gottlieb M, DeMott JM, Hallock M, Peksa GD. "Systemic Antibiotics for the Treatment of Skin and Soft Tissue Abscesses: A Systematic Review and Meta-Analysis". Ann Emerg Med. 73(1). :8-16. (2019)
- Duane TM, Huston JM, Collom M, et al. "Surgical Infection Society 2020 Updated Guidelines on the Management of Complicated Skin and Soft Tissue Infections". Surg Infect (Larchmt). 22(4). :383-399. (2021)
- Liu C, Bayer A, Cosgrove SE et al. "Clinical Practice Guidelines by the Infectious Diseases Society of America for the Treatment of Methicillin-Resistant Staphylococcus Aureus Infections in Adults and Children". Clin Infect Dis. 52(3). :e18-55. (2011)
- Fitch MT, Manthey DE, McGinnis HD, Nicks BA, Pariyadath M. "Abscess Incision and Drainage". N Engl J Med. 357(19). :e20. (2007)