Summary
Soft tissue lesions of the shoulder involve the shoulder's ligaments, tendons, cartilage, and/or capsule. The rotator cuff is the most commonly affected structure. Rotator cuff disease includes a range of pathologies from tendinopathy to rotator cuff tears and is commonly associated with subacromial bursitis and biceps tendinopathy. Many patients present with subacromial impingement syndrome, caused by inflammation of subacromial structures (e.g., rotator cuff tendons, subacromial bursa, and long head of the biceps) and subsequent narrowing of the subacromial space. Other frequently encountered soft tissue lesions of the shoulder include adhesive capsulitis, calcific tendonitis, and labral tears. Soft tissue lesions may result from overuse (e.g., repetitive overhead arm movements in young athletes) or degenerative or inflammatory processes. Symptoms of soft tissue lesions of the shoulder include pain with movement (usually shoulder abduction), nocturnal pain, tenderness, and/or restricted range of motion (ROM). A clinical diagnosis can often be made after an orthopedic shoulder examination that utilizes provocation tests for specific shoulder injuries. Imaging tests, primarily MRI, are usually obtained to make a definitive diagnosis and/or plan for surgery, if necessary. Management is typically conservative: activity modification, NSAIDs, and physical therapy. Intraarticular corticosteroid injections and/or surgery may be required if symptoms do not resolve with conservative measures. Early surgical intervention is indicated for labral tears causing instability and acute or large rotator cuff tears, especially in active individuals.
See also “Biceps tendonitis,” “Subacromial bursitis,” “Acromioclavicular joint injury,” and “Shoulder dislocation.”
Overview
General principles
- The majority of shoulder pain is the result of rotator cuff disease, a spectrum of pathophysiology ranging from subacromial impingement to complete tears of rotator cuff tendons (most commonly the supraspinatus).
- Other sources of pain include the: [1][2][3]
- Biceps tendon
- Glenohumeral joint capsule
- Subacromial bursa
- Acromioclavicular (AC) joint
- Glenohumeral joint
Management approach [4][5]
- Perform a thorough orthopedic shoulder examination.
- Perform a neurovascular examination of the entire arm.
- Obtain standard x-rays in all patients. [5][6]
- Consider MRI or ultrasound imaging if the diagnosis remains unclear. [6][7]
- Begin conservative management, unless there is an indication for surgery.
- Consult orthopedics urgently for the following: [8]
- Suspected joint infection, e.g., warmth, red skin, systemic symptoms
- Unreduced dislocation
- Acute traumatic rotator cuff tear
- Mass on examination or imaging
Overview of soft tissue injuries and pain syndromes
| Overview of shoulder soft tissue lesions [4][5][9][10] | |||
|---|---|---|---|
| Affected structures | Positive provocation tests and examination findings | Imaging | |
| Subacromial impingement syndrome |
|
|
|
| Rotator cuff tendinopathy |
|
|
|
| Rotator cuff tear |
|
|
|
| Bicipital tendonitis |
|
|
|
| Calcific tendonitis |
|
|
|
| Adhesive capsulitis [15] |
|
|
|
| Labral tears |
|
|
|
| Osteoarthritis |
|
|
|
| Acromioclavicular joint injury |
|
|
|
| Shoulder dislocation |
|
|
|
Always compare the affected shoulder to the contralateral shoulder when performing an orthopedic shoulder examination.








")
")
© AMBOSS

© AMBOSS
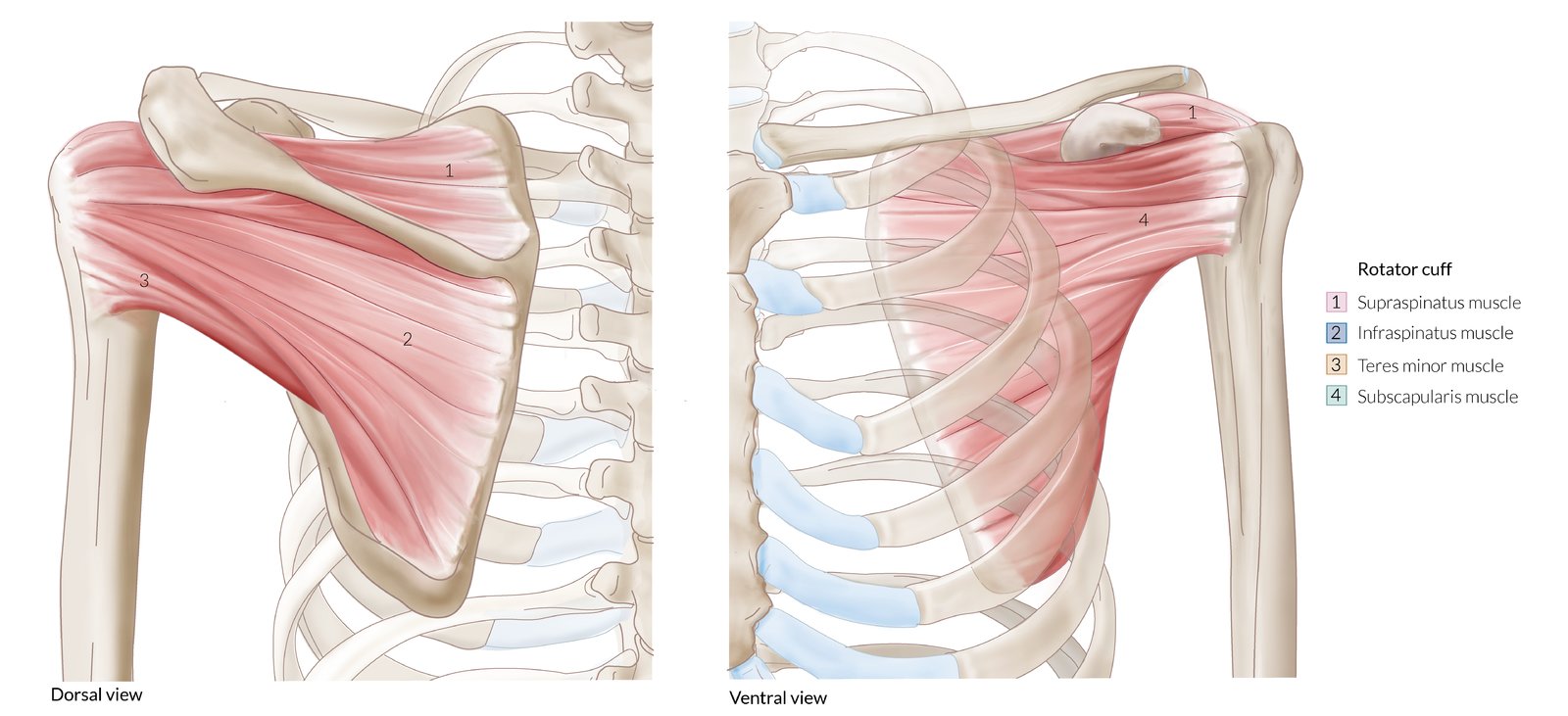
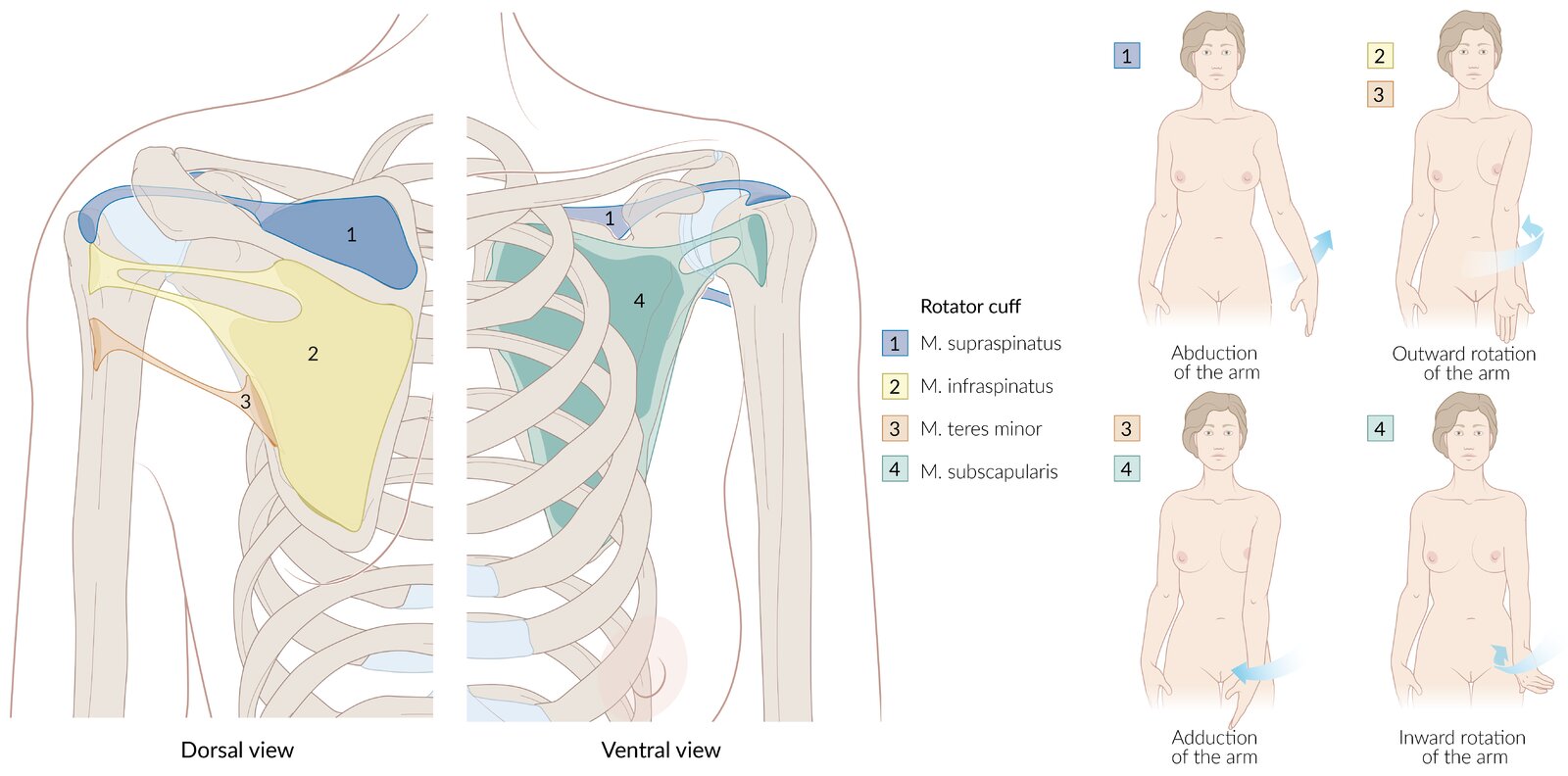
Anterior view
– Subscapularis muscle: internal rotation and adduction
– Supraspinatus muscle: initiates abduction
Posterior view
– Supraspinatus muscle: initiates abduction
– Infraspinatus muscle: external rotation
– Teres minor muscle: external rotation and adduction
© AMBOSS
© AMBOSS
© AMBOSS

© AMBOSS
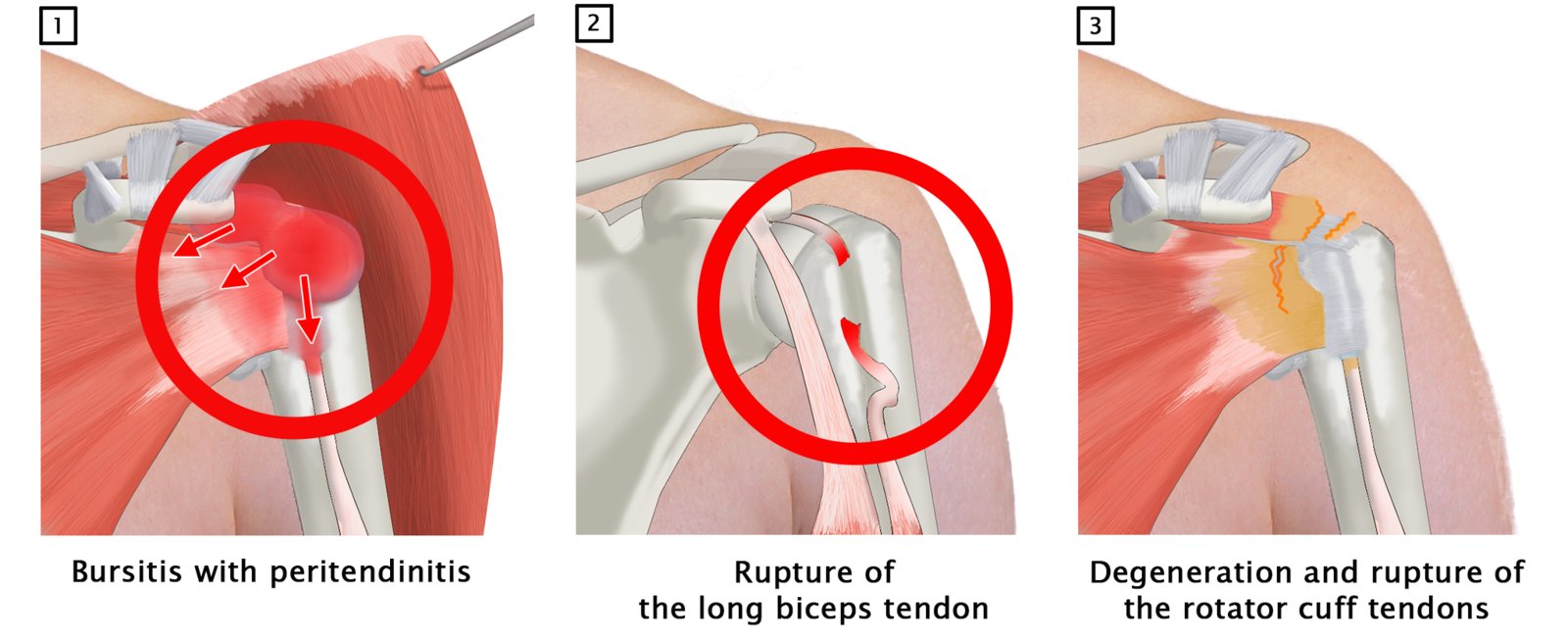
Image 1: bursitis with comprehensive inflammation. The bursae are severely swollen and show inflammatory changes. There may be degeneration of the rotator cuff tendon over the course of the inflammatory reaction. As a result, complications such as rupture of the long biceps tendon (2) or a tear of the affectced muscles can occur.
© AMBOSS
© AMBOSS
© AMBOSS

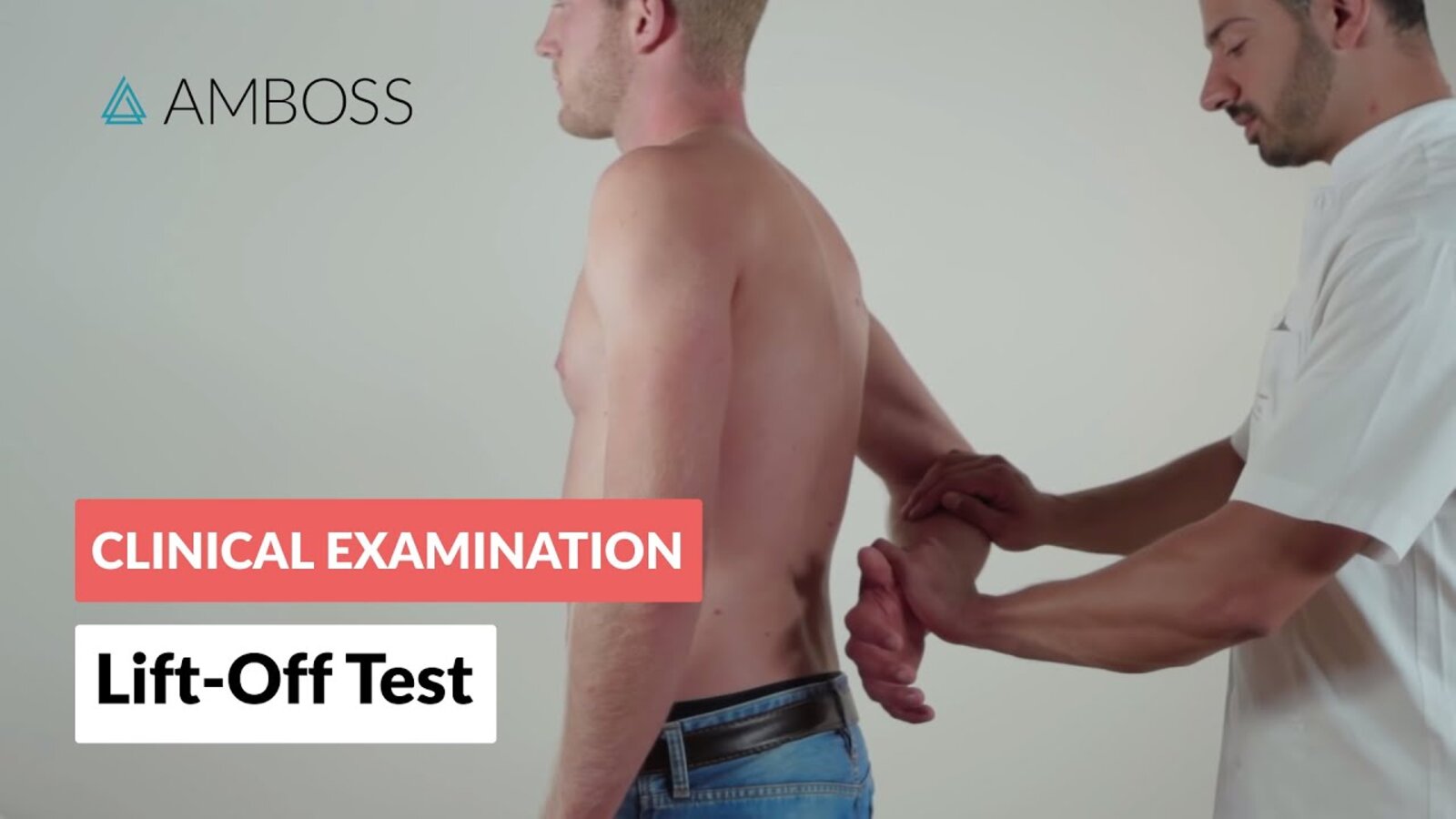
The examiner slightly abducts the patient's arm with the elbow at 90° flexion and the forearm supinated. The long head of the biceps tendon in the bicipital groove is palpated and the patient is asked to bend the elbow (green arrow) against resistance (red arrow). If the patient is unable to move against resistance or experiences pain in the bicipital groove, the test is considered positive. It may indicate a pathological condition of the long head of the biceps tendon.
© AMBOSS

Photograph of a patient who sustained a fall on her right shoulder (ventral view)
The lateral end of the right clavicle is displaced cranially and is visible as a step-like deformity of the shoulder outline.
Examination revealed a positive piano key sign (spring test), in which the displaced clavicle was reducible with the application of pressure and returned to this elevated position when the pressure was released.
These are the typical clinical features of type III acromioclavicular injury.
Source: © IMPP

Photograph of a patient who sustained a fall on her right shoulder (dorsal view)
The lateral end of the right clavicle is displaced cranially and is visible as a step-like deformity of the shoulder outline.
Examination revealed a positive piano key sign (spring test), in which the displaced clavicle was reducible with the application of pressure and returned to this elevated position when the pressure was released.
These are the typical clinical features of type III acromioclavicular injury.
Source: © IMPP
Etiology
- Overuse: especially with activities involving repetitive overhead arm movement, e.g., baseball, volleyball
- Degenerative processes (especially in older individuals)
- Trauma
- Inflammation
- Systemic diseases (See “Adhesive capsulitis.”)
- Postoperative changes, e.g., inflammation, fibrous tissue, implants
Clinical features
The following are nonspecific features. Provocative clinical examination and diagnostic tests are usually required to identify the underlying condition (see “Overview of shoulder soft tissue lesions).
-
Painful active and/or passive abduction [4][5]
- May be aggravated by internal and/or external rotation
- Localization of pain over the deltoid with shoulder abduction suggests rotator cuff disease.
- Anterior superior pain suggests acromioclavicular joint pathology.
- Patient apprehension before shoulder movement
- Tenderness, e.g., subacromial
- Limited ROM (active and/or passive)
- Weakness

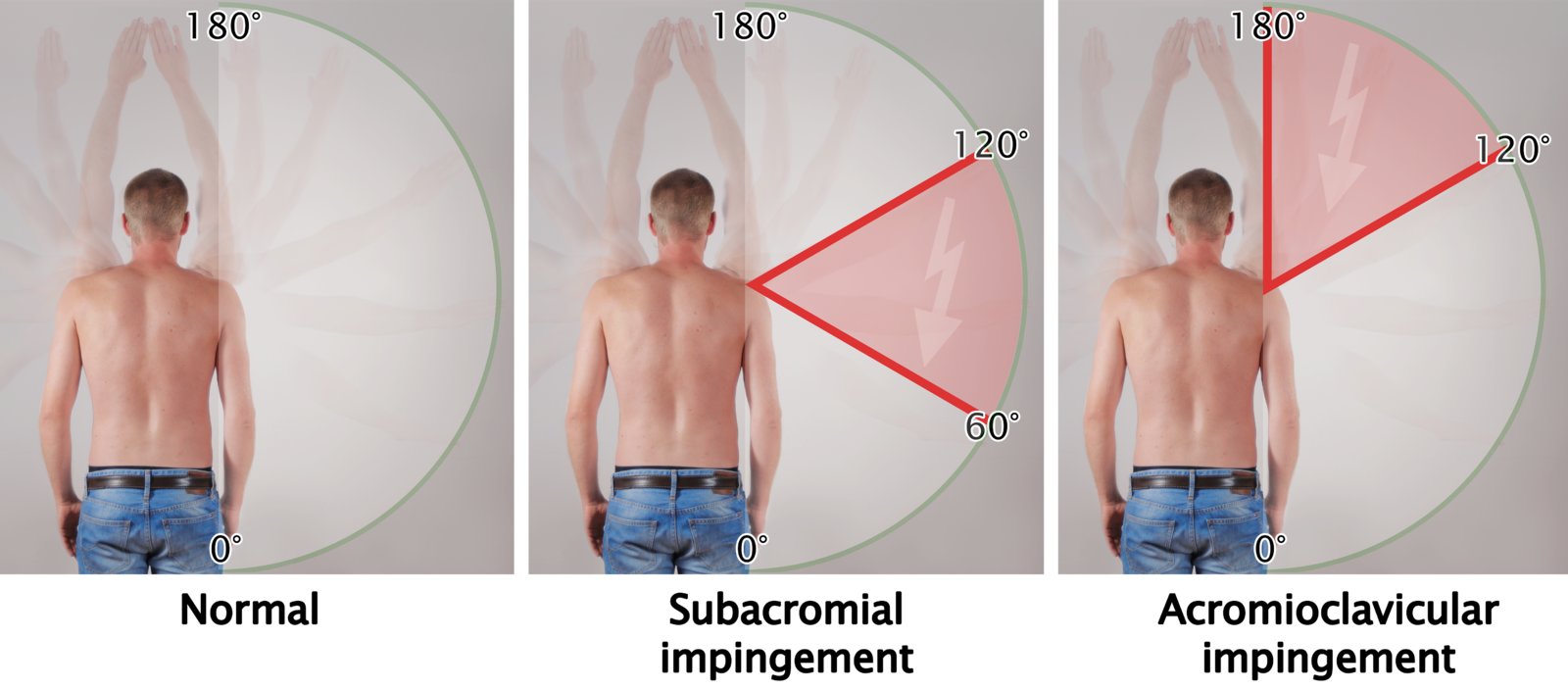
The normal range of motion is shown as a green semicircle. The angle range, in which impingement results in pain (painful arc), is indicated in red.
© AMBOSS
Diagnosis
The clinical examination can guide early management (see “Overview of shoulder soft tissue lesions”). Imaging is usually obtained to confirm the diagnosis and/or rule out alternative diagnoses. [6][7][9]
Clinical evaluation
-
Orthopedic shoulder examination should include the following:
- Shoulder mobility testing
- Shoulder impingement tests
- Shoulder instability tests
- Rotator cuff examination
- Proximal biceps tendon examination
-
Neurovascular examination
- Check upper extremity capillary refill time and pulses at the radial artery, ulnar artery, and brachial artery.
- Identify signs of median nerve palsy, radial nerve palsy, ulnar nerve palsy, or axillary nerve palsy.
X-ray [6][7]
- Initial imaging for all patients
- Required views: standard AP, AP glenoid , trans-scapular lateral , and axillary [11][17]
- Often normal
- Findings may include:
- Degenerative changes or narrowing of the subacromial space (e.g., due to structural abnormalities of the acromion)
- Calcification of the supraspinatus tendon in calcifying tendinitis
- Alternative causes of shoulder pain (e.g., pathological fracture)

 of the shoulder")
MRI [6]
- Gold standard imaging for evaluation of the shoulder
- Indications: diagnostic uncertainty or symptoms that persist following conservative treatment
- Supports surgical planning

Ultrasound [18]
- Provides real-time imaging during provocation maneuvers and is used to guide interventional treatment
- Accuracy comparable to MRI for rotator cuff tears, bursitis, and other shoulder soft tissue lesions [9][19]
-
Findings may include:
- Damage to the soft tissue structures (bursae, rotator cuff tendons)
- Bicep tendon rupture, subluxation, or dislocation (e.g., acromioclavicular or glenohumeral joints)

Both scapulae are shaded in green. The white dotted lines highlight the bony prominences.
Our great thanks to PD Dr. M. Jergas (Center for Diagnostic and Interventional Radiology, St. Elizabeth Hospital, Cologne) for kindly providing this image.

X-ray scapula (lateral view; tangential or “Y” view)
The patient is placed in the erect PA oblique position or supine AP oblique position. The medial and lateral margins of the scapula are aligned perpendicular to the x-ray detector, resulting in a tangential view of the body of the scapula.
The stem of the Y is formed by the scapular body, while the bifurcation of the Y is formed by the acromion process (1) and coracoid process (2). The humeral head normally projects over the glenoid at the bifurcation of the Y. The lateral extent of the clavicle (3) is visible, and a nearly straight line can be drawn through the inferior borders of the acromion (1) and clavicle (3).
This view is useful for detecting dislocations, fractures, and degenerative disease, especially in patients with restricted movement at the shoulder.
Dotted line: humerus; green overlay: scapula
Source: “Y CR shoulder” by RSatUSZ, Wikimedia Commons, licensed under CC BY-SA 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 4.0.
{kind=link}
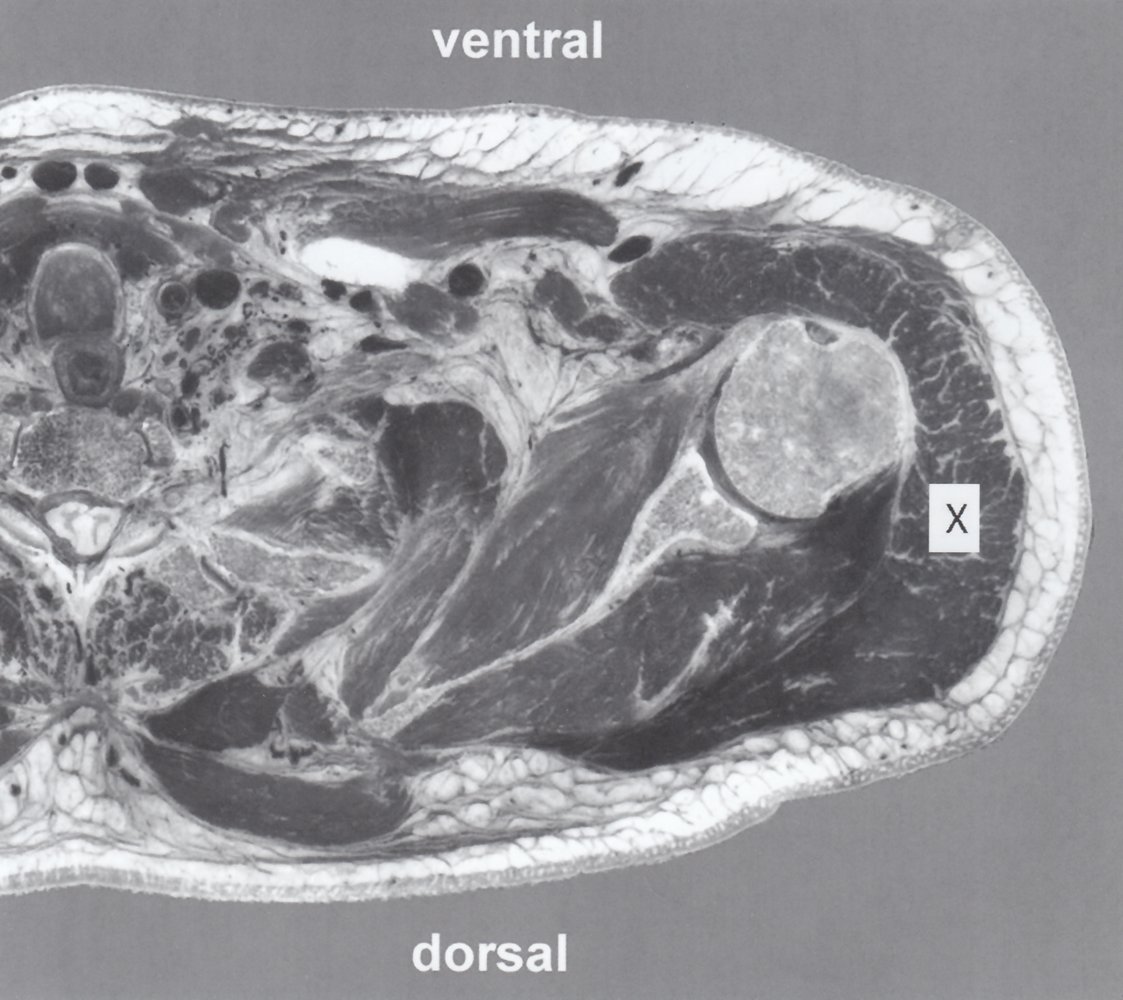
MRI left shoulder (T1-weighted; axial plane)
The head of the humerus (1) and glenoid of the scapula (2) are separated by the hypointense glenohumeral joint space. The deltoid muscle (X) overlies the humeral head. The subscapularis (3) and serratus anterior muscles (4) are ventral to the scapula, and the infraspinatus muscle (5) is dorsal to the scapula.
6: pectoralis muscle; 7: trachea; 8:esophagus; 9: spinal canal and cord
Source: © IMPP
Differential diagnoses
- Fracture and/or dislocation
- Osteoarthritis
- Brachial plexus neuritis
- Cervical radiculopathy
- Thoracic outlet syndrome
- Fibromyalgia
The differential diagnoses listed here are not exhaustive.
Treatment
The majority of patients with soft tissue injuries of the shoulder can be managed initially with conservative therapy. [5][20]
Conservative therapy of shoulder soft tissue lesions
- Utilize the POLICE principle for acute injuries or inflammation.
- Manage acute pain, e.g., NSAIDs.
- Modify activities, especially those involving overhead movements.
- Consult physical therapy.
- Consider subacromial glucocorticoid injections for refractory chronic pain.
Adequate pain control is necessary to optimize the results of physical therapy. [21]
Wait at least 4 months between glucocorticoid injections to avoid weakening the tendons. [5]
Surgical treatment
-
Indications [5]
- Acute injury with full-thickness rotator cuff tear and/or shoulder dislocation
- Acute labral injuries with recurrent shoulder dislocation [22][23]
- Chronic full-thickness rotator cuff tear(s) in individuals < 65 years of age
- Symptoms that persist after 3–6 months of conservative treatment [20]
-
Technique: depends on the specific condition
- Arthroscopic surgery, e.g., decompression of subacromial impingement
- Open arthrotomy, e.g., open rotator cuff repair
- Manipulation under anesthesia, e.g., for adhesive capsulitis
Subacromial impingement syndrome
Background
-
Definition
- A syndrome of pain during shoulder abduction, forward flexion, and/or extreme adduction associated with narrowing of the subacromial space
- Encompasses a spectrum of pathologies, including rotator cuff disease, subacromial bursitis, and biceps tendinopathy [2]
- Etiology: repetitive overhead activity or other overuse injuries
-
Pathophysiology [2]
- Extrinsic compression: Narrowed subacromial space causes bursitis and tendonitis.
- Intrinsic compression: Degenerative tendonitis causes glenohumeral changes that narrow the subacromial space.
- Stages
- Degeneration leads to the formation of edema and bleeding in the area of the rotator cuff tendons and subacromial bursa.
- Fibrosis of the bursa
- Tendon tear or rupture, intermittent bursitis, and pseudoparalysis of the arm
Clinical features
- Pain on movement that is worsened by overhead activities (e.g., combing hair or reaching up to a cupboard)
- Nocturnal exacerbation of pain, especially when lying on the affected shoulder
- Pain and restriction of active movement between 60 and 120°
- Symptoms typically develop over weeks to months. [24]
Diagnosis [2]
Can be diagnosed clinically
-
Positive provocative clinical examination
- Neer test
- Hawkins test
- Painful arc test
- X-rays: may show narrowing of acromiohumeral distance, osteoarthritis
- MRI: provides definitive evidence of tendinitis and/or impingement [24]
-
Subacromial lidocaine injection test [25][26]
- Indication: inability to differentiate between subacromial impingement syndrome and other causes of shoulder pain and/or restricted ROM, e.g., rotator cuff tear, frozen shoulder, glenohumeral joint arthritis [27]
- Technique: subacromial injection of 5 mL of lidocaine or bupivacaine [26]
- Interpretation: Pain relief following injection suggests subacromial impingement syndrome.
Treatment [2]
- All patients: Begin conservative therapy of shoulder soft tissue lesions.
- Surgical treatment: if there is no improvement after conservative treatment (e.g., arthroscopic decompression, acromioplasty)
Complications
- Adhesive capsulitis
- Otherwise dependent on underlying pathology
- See “Rotator cuff disease.”
- See “Subacromial bursitis.”
- See “Biceps tendinopathy.”

The normal range of motion is shown as a green semicircle. The angle range, in which impingement results in pain (painful arc), is indicated in red.
© AMBOSS
© AMBOSS
© AMBOSS
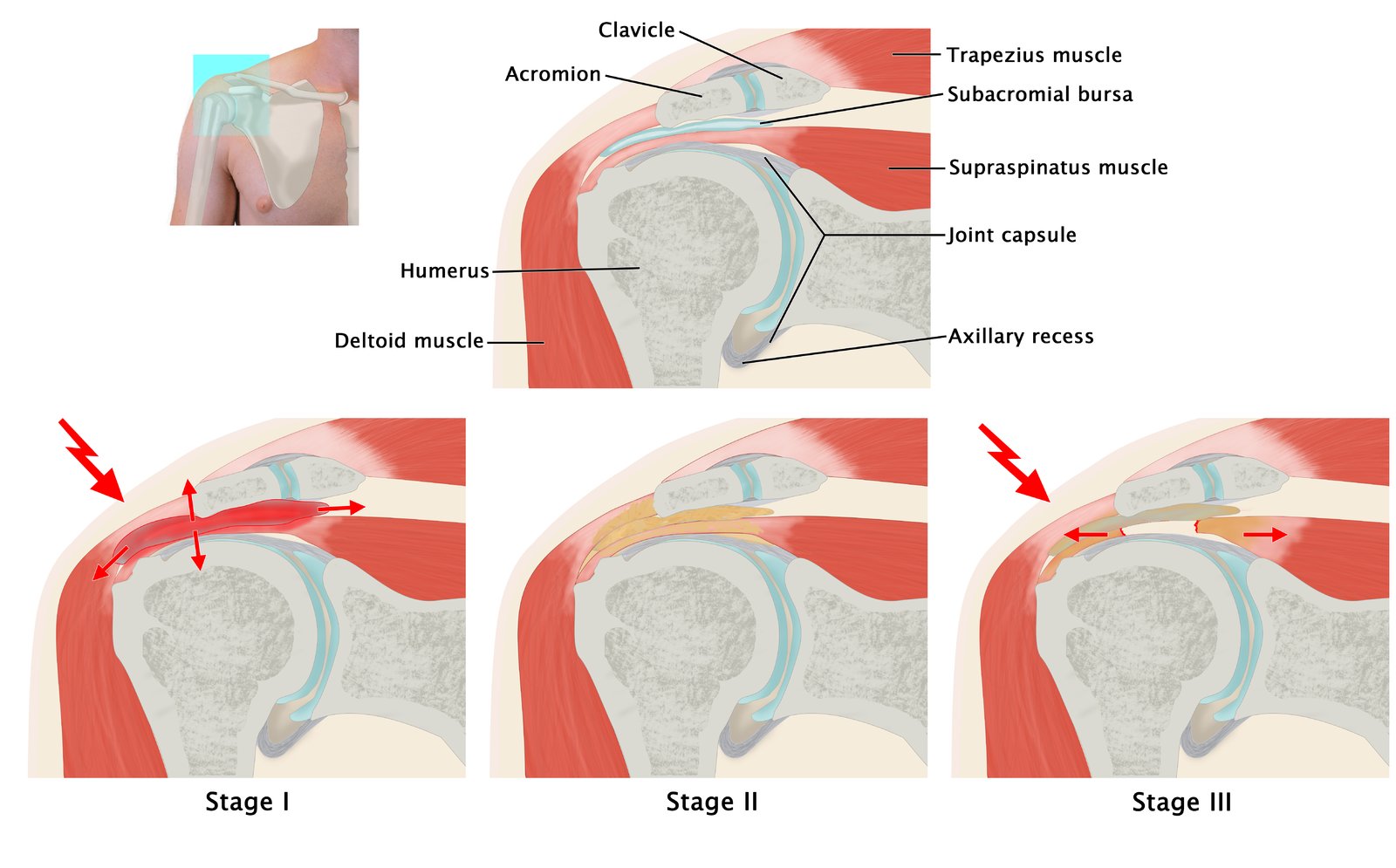
The upper images shows the sectional plane and anatomy of the frontal cross-section of the shoulder. The lower images show the stages of impingement.
Stage 1, which is very painful, is characterized by irritation of the rotator cuff and bursa. Stage 2 involves fibrosis of the structures, leading to restricted function. Stage 3 involves the painful rupture of the rotator cuff, intermittent bursitis, and pseudoparalysis of the arm.
© AMBOSS
Rotator cuff disease
General principles [28][29]
- Rotator cuff disease is a poorly defined collection of traumatic injuries and/or degenerative changes to rotator cuff tendons.
- It includes a spectrum of conditions ranging from tendonitis to rotator cuff tears.
- Comorbid adjacent lesions are common, e.g., subacromial bursitis, biceps tendinopathy.
- Clinical features vary depending on the underlying conditions and course.
- Subacromial impingement syndrome is a common (but not universal) manifestation of rotator cuff tendinopathy and calcific tendonitis of the shoulder.
- Loss of active rotator cuff function suggests a rotator cuff tear.
Rotator cuff tendinopathy [29][30]
-
Definition
- Inflammatory and/or degenerative changes of one or more rotator cuff tendons
- Encompasses the spectrum of rotator cuff disease between impingement and rotator cuff tear
- Etiology: acute injury and/or chronic degeneration from overuse
-
Clinical features
- Can present as subacromial impingement syndrome
- Subacromial tenderness on palpation
- Referred pain in the deltoid area with overhead activities
- Possible atrophy of the supraspinatus and infraspinatus muscles
-
Diagnosis [30]
- Often a clinical diagnosis based on provocation testing
- Painful arc test (early finding)
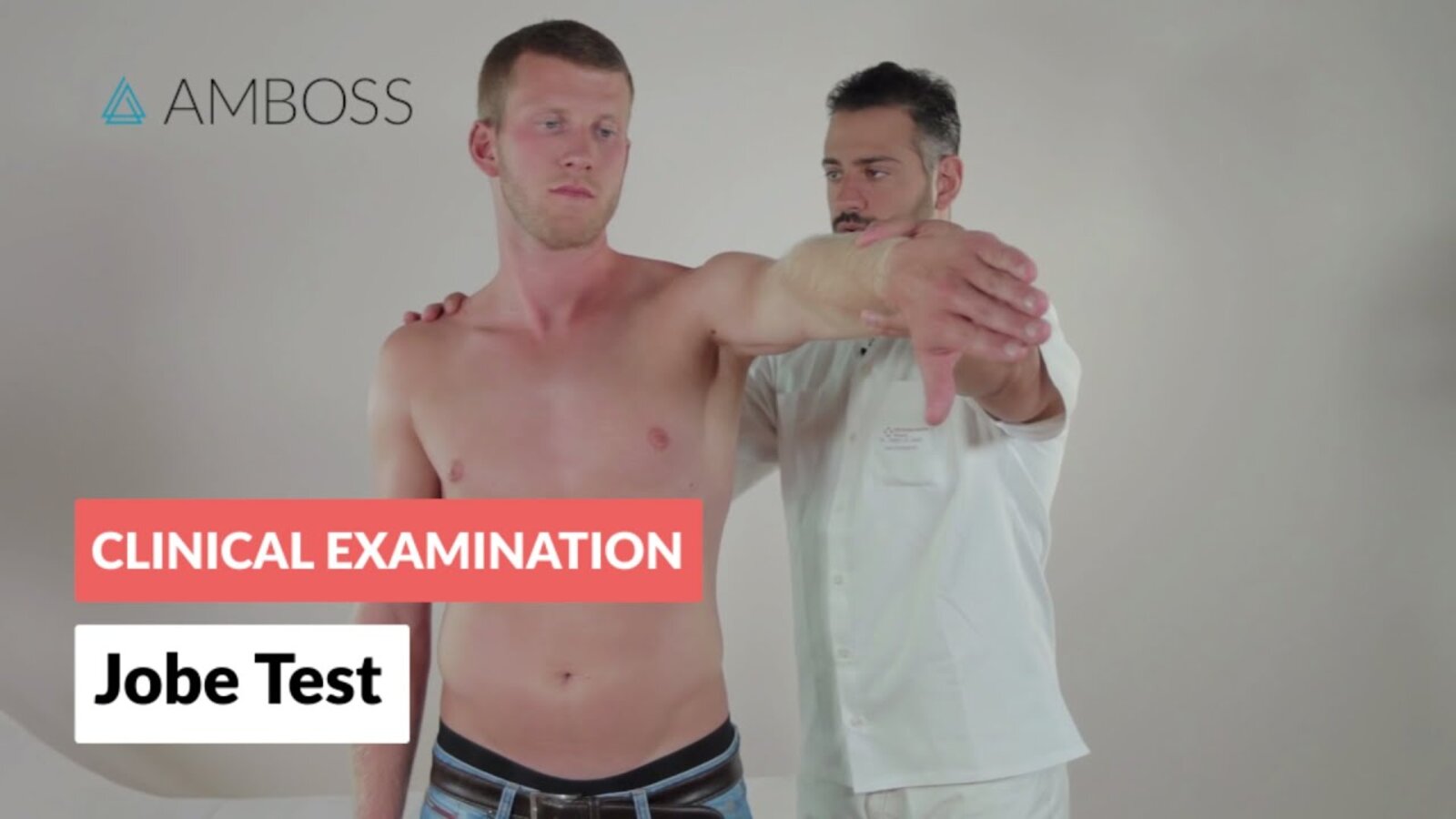
- Empty can test
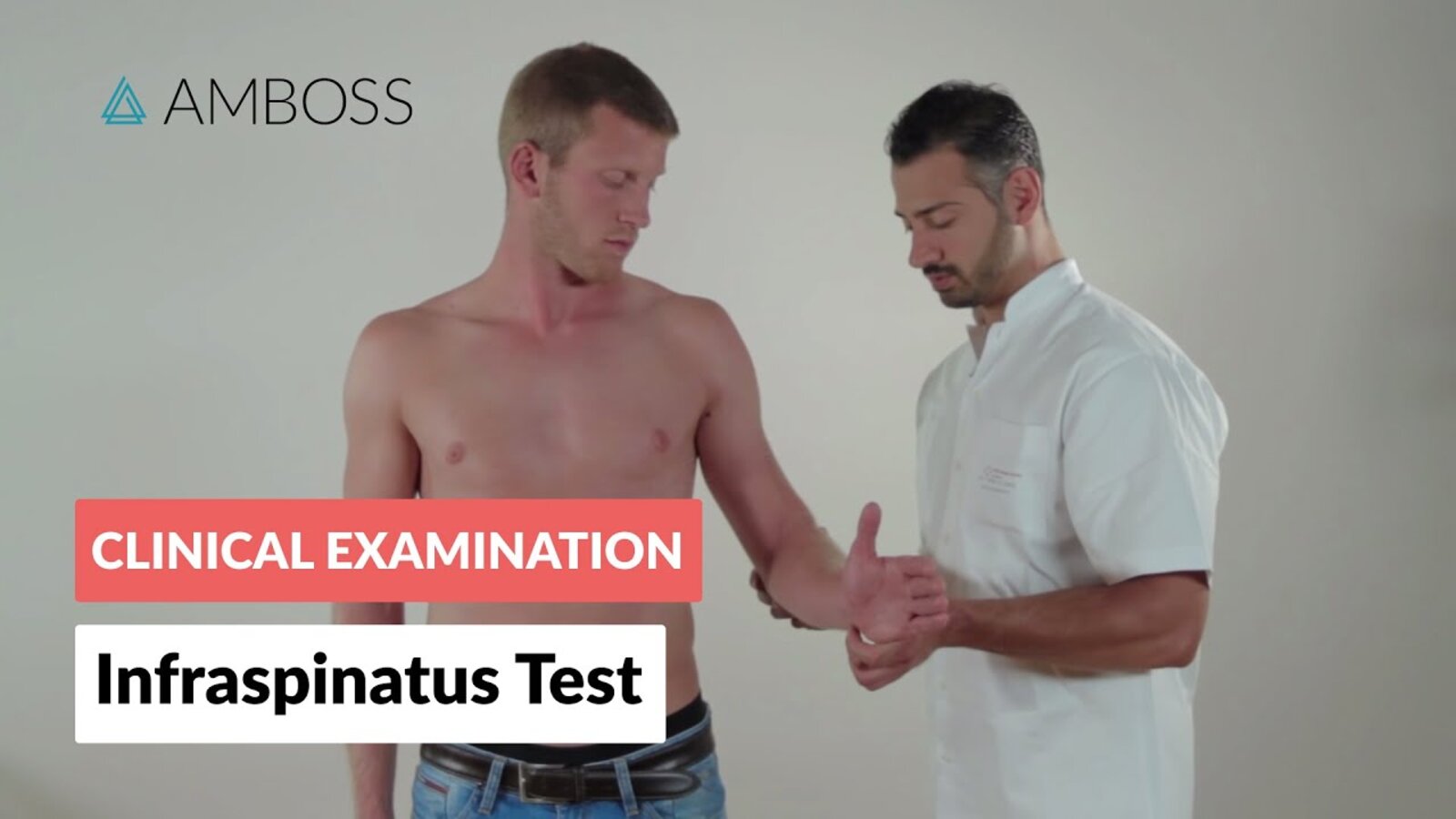
- Infraspinatus test
- Belly press test
- MRI or ultrasound findings provide a definitive diagnosis.
- Often a clinical diagnosis based on provocation testing
- Treatment: : Follow conservative therapy of shoulder soft tissue lesions.
-
Complications [28]
- Muscle atrophy or fatty degeneration
- Rotator cuff tear, rupture, and/or retraction
- Adhesive capsulitis


Rotator cuff tear
Rotator cuff tears are often preceded by rotator cuff tendonitis and most commonly involve the supraspinatus tendon. [31]
-
Etiology [28][29]
- Chronic degenerative tear (most common): usually seen in individuals > 40 years of age and/or performing repetitive overhead movements (e.g., infraspinatus tear in baseball pitchers) [11]
- Acute traumatic injury (∼ 10% of cases): usually seen following a fall or dislocation, often in young adults [11]
-
Clinical features [11]
- Acute rupture: sudden severe pain and loss of strength
- Degenerative rupture: chronic pain; loss of strength is less pronounced than with acute tear
- Restricted active ROM (especially if passive ROM is normal)
-
Diagnostics [6]
- Positive drop-arm test suggests supraspinatus tear.
- Provocation tests that may be abnormal (depending on the affected tendon)
- Empty can test
- Lift-off test
- Belly press test
- Infraspinatus test
- POCUS: may show full or partial-thickness tears [11]
- X-ray: superior displacement of the humeral head (high-riding humeral head)
- Ultrasound or MRI: definitive test to determine the location and extent of the rupture
-
Treatment
- All patients: Optimize conservative therapy of shoulder soft tissue lesions.
- Acute injury: Immobilize for comfort and consult orthopedic surgery early.
-
Surgical repair ; [5][32][33]
-
Typically considered for:
-
Younger patients (< 65 years old) with:
- Acute traumatic full-thickness tears
- Chronic full-thickness tears [33]
- Significantly reduced arm function
- High risk of tear progression
- Insufficient improvement after 3–6 months of conservative treatment [20]
-
Younger patients (< 65 years old) with:
- Typically inappropriate for:
- Sedentary and older patients (> 65 years) [5]
- Most partial-thickness tears
-
Typically considered for:
-
Complications
- Tear progression [5]
- Adhesive capsulitis
Early surgical repair of a rotator cuff tear is often preferred in young and/or physically active patients. [11][34]


")
Calcific tendonitis of the shoulder [13][14]
- Etiology: See “Calcific tendonitis” in “BCP crystal deposition diseases.”
-
Clinical features
- Primarily affects rotator cuff tendons causing features similar to rotator cuff tendinopathy.
- Can occasionally affect the long head of the biceps (see “Biceps tendonitis.”)
-
Diagnosis
- X-rays usually show calcium deposits.
- Ultrasound or MRI are diagnostic but not required if calcium deposits are seen on x-ray. [13]
-
Treatment
- Follow conservative therapy of shoulder soft tissue lesions. [13]
- Physical removal of calcium deposits may be considered if symptoms persist after 6 months of conservative management. [14][35]
- Percutaneous ultrasound-guided barbotage of crystals
- Arthroscopic surgery
- Extracorporeal shock wave therapy
")
")
© AMBOSS
Anterior view
– Subscapularis muscle: internal rotation and adduction
– Supraspinatus muscle: initiates abduction
Posterior view
– Supraspinatus muscle: initiates abduction
– Infraspinatus muscle: external rotation
– Teres minor muscle: external rotation and adduction
© AMBOSS
Image 1: bursitis with comprehensive inflammation. The bursae are severely swollen and show inflammatory changes. There may be degeneration of the rotator cuff tendon over the course of the inflammatory reaction. As a result, complications such as rupture of the long biceps tendon (2) or a tear of the affectced muscles can occur.
© AMBOSS
© AMBOSS
© AMBOSS
© AMBOSS
© AMBOSS
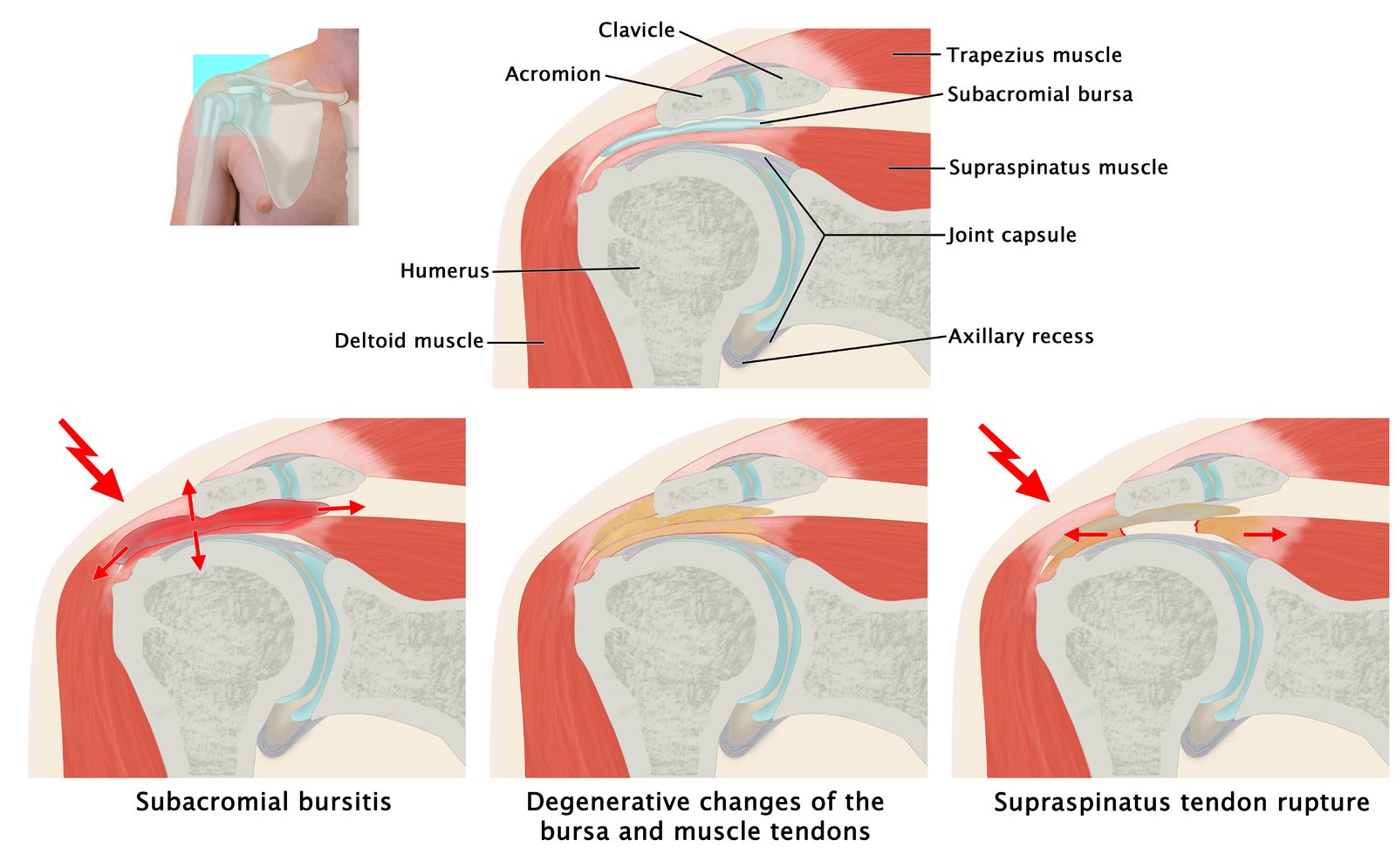
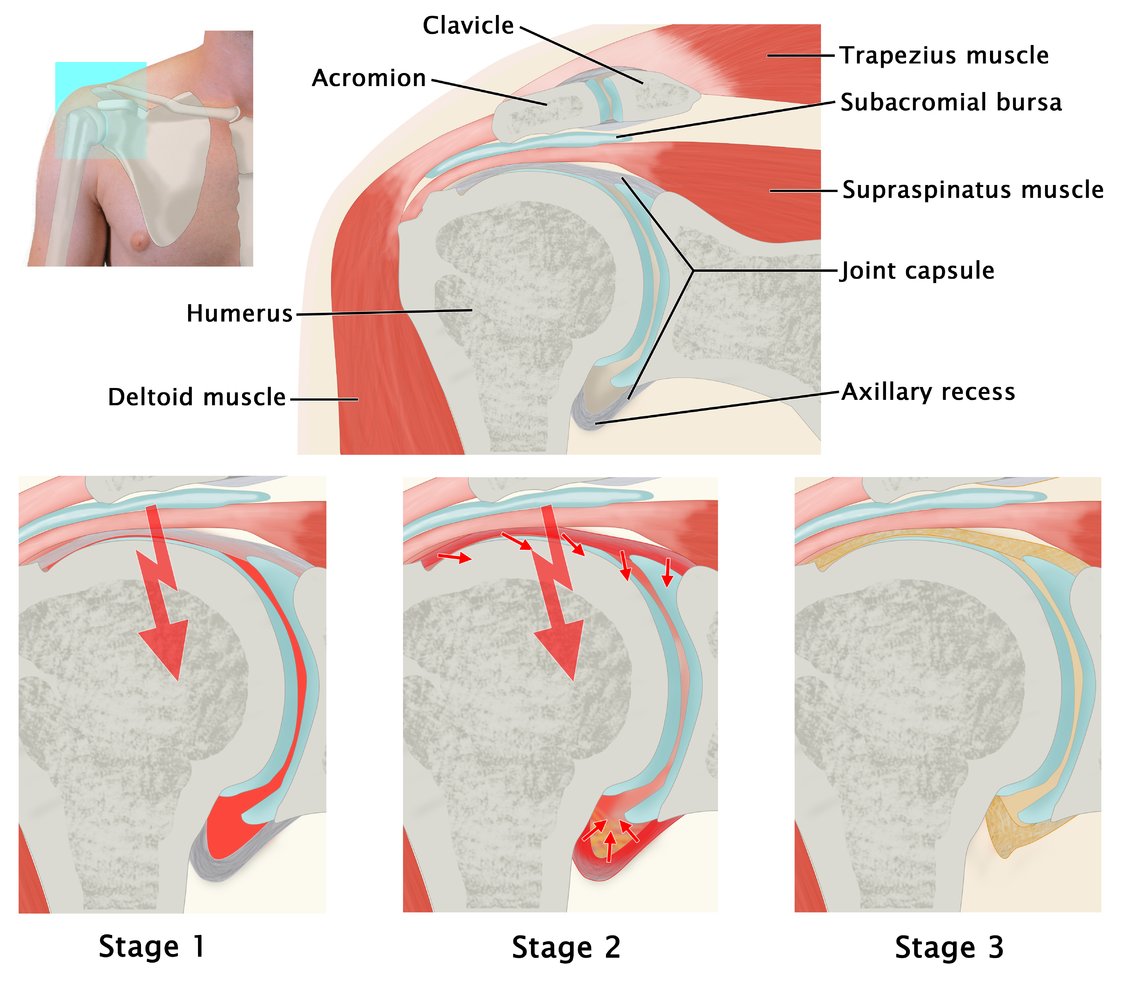
The top image shows a cross-section of the shoulder joint.
The bottom images show the progression of a degenerative rotator cuff tear. Repetitive overhead movement and/or anatomical variants of the acromion can result in inflammation of the subacromial bursa and rotator cuff tendons (left). This may progress to degeneration of the bursa and tendons (middle). As a result, the tendon fibers are less elastic and prone to tear, resulting in a rotator cuff tear (right). The supraspinatus tendon is most commonly affected.
© AMBOSS
© AMBOSS

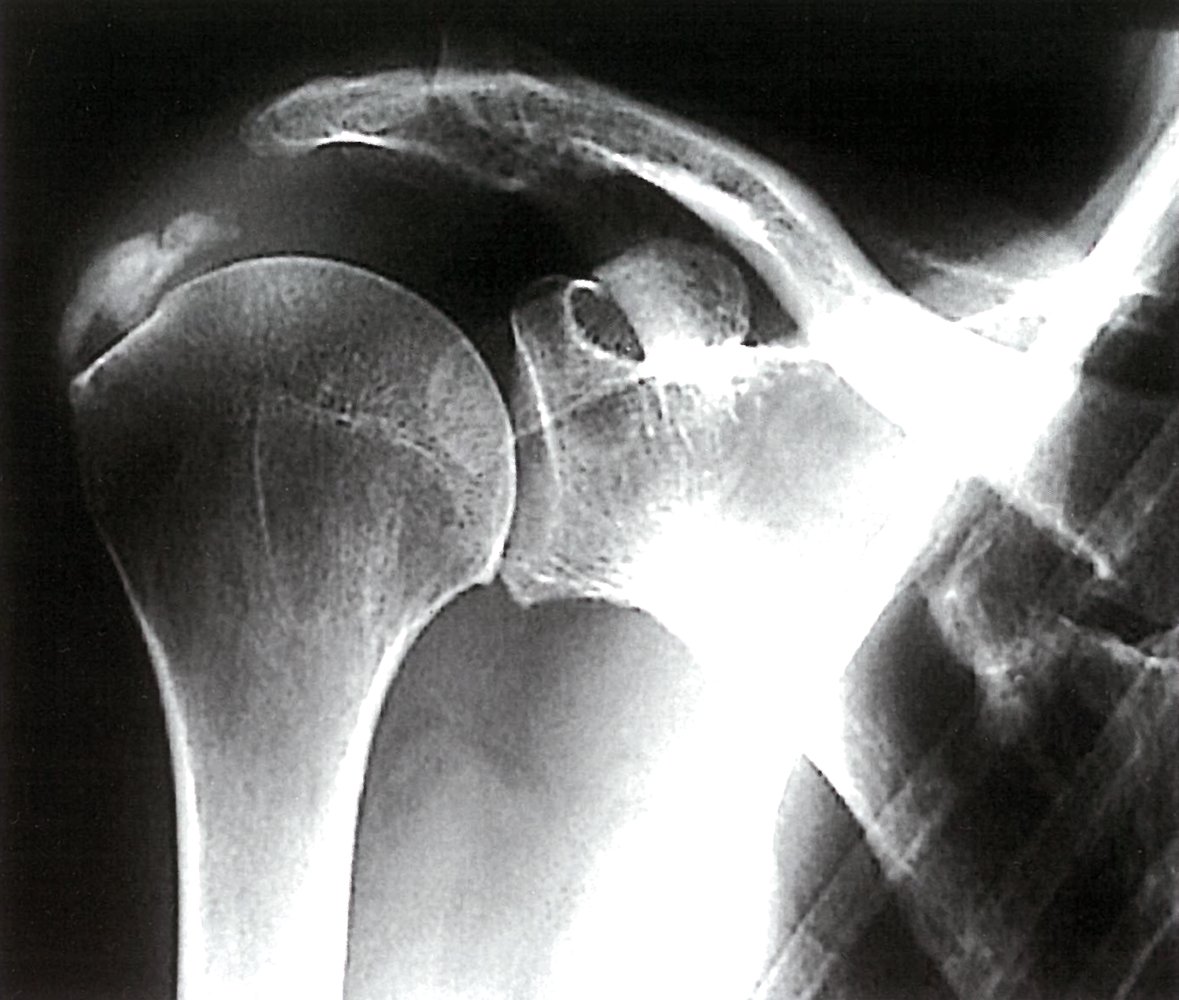
X-ray of the right shoulder (AP view)
The acromiohumeral interval (red overlay; white arrowheads), which is normally ∼10 mm wide, has been obliterated.
As some of the rotator cuff tendons lie within the acromiohumeral interval, its obliteration indicates either a tear or degeneration of the rotator cuff tendon(s). MRI is needed to confirm the diagnosis.
Int-Rot: internal rotation
Source: "Rot cuff tear x-ray", Micaela E., Wikimedia Commons licensed under Public Domain
{kind=link}
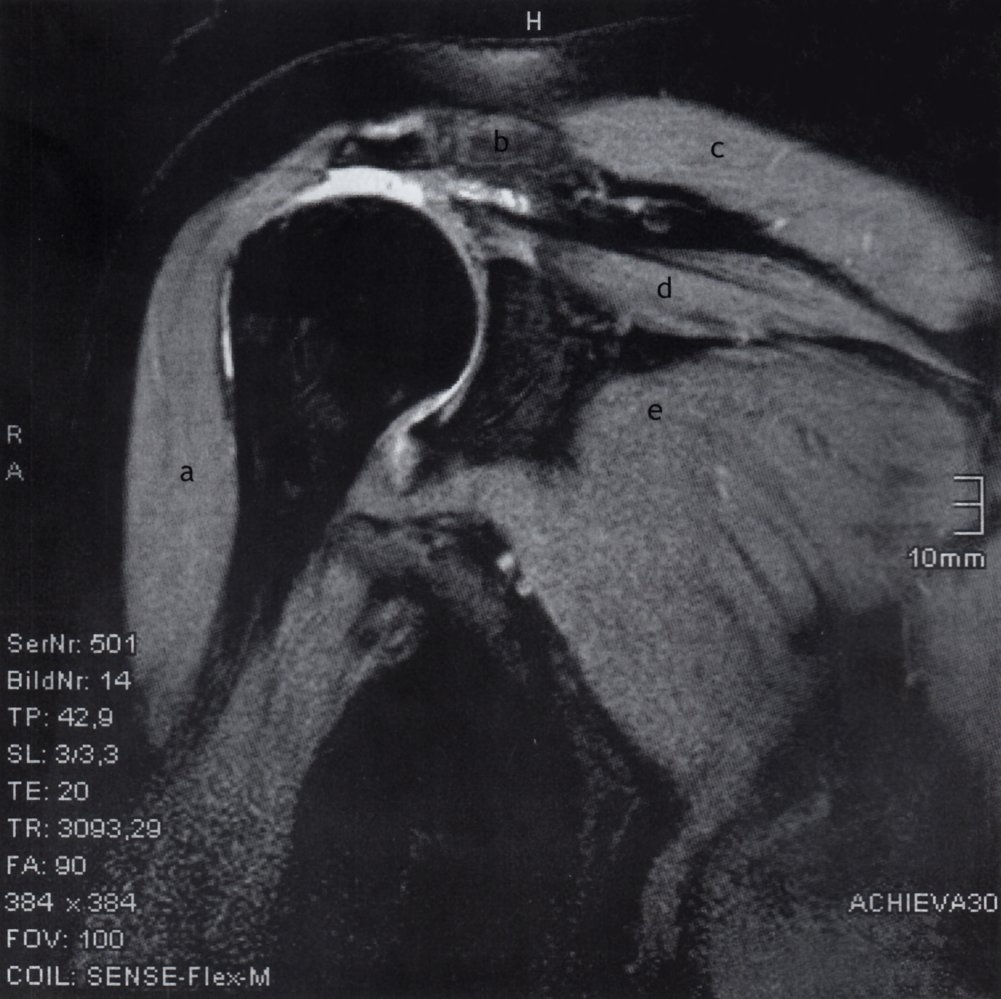
MRI right shoulder (fluid sensitive fat-suppressed sequence; coronal plane)
A tear of the hypointense supraspinatus tendon (white arrow) has resulted in tendon retraction proximally. Fluid (red arrow) inferior to the acromion (green overlay) in the subacromial-subdeltoid space appears hyperintense and communicates with joint effusion along the rest of the humeral head.
These are MRI features of a full-thickness tear of the supraspinatus tendon
a: deltoid muscle; b: clavicle; c: trapezius muscle; d: supraspinatus muscle; e: subscapularis muscle
Source: © IMPP
© AMBOSS

X-ray right shoulder (external rotation view)
A calcification (arrow) is seen adjacent to the greater tuberosity of the humerus in the region of the rotator cuff.
Red overlay: course of the supraspinatus muscle; green overlay: insertion site on the greater tuberosity
Source: © IMPP
X-ray right shoulder (external rotation view)
Calcific densities (green overlay) are seen in the subacromial space adjacent to the greater tuberosity of the humerus.
The appearance is consistent with basic calcium phosphate calcific-associated periarthritis (calcific tendinitis or calcific tendinopathy) in the region of the tendon of the supraspinatus muscle.
Source: © IMPP
Adhesive capsulitis (frozen shoulder)
- Definition: inflammation and fibrosis of the joint capsule leading to contracture of the shoulder joint
-
Epidemiology [36]
- ♀ > ♂
- Onset > 40 years of age
-
Etiology [15][16][37]
- Primary adhesive capsulitis (idiopathic): associated with diabetes mellitus, thyroid disorders, scleroderma, Dupuytren contracture, ASCVD
- Secondary adhesive capsulitis: associated with previous shoulder injury (e.g., shoulder dislocation, rotator cuff disease), prolonged immobilization, arthroscopic surgery
-
Stages
- Freezing or painful stage: minimal synovitis with pain, causing a limitation of ROM
- Frozen or transitional stage: Pain decreases, but synovitis continues (with axillary adhesions and contraction of the capsule).
- Thawing stage: Inflammation decreases and movement slowly improves.
-
Clinical features [11][36][38]
-
Shoulder pain
- Most commonly involves the nondominant side
- May be poorly localized; sometimes pain is referred to the deltoid and bicep
- More severe at night
- Stiffness that interferes with activities of daily living
-
Severe restriction of active and passive ROM of the glenohumeral joint in all planes, especially:
- External rotation
- Passive abduction (restricted to < 90°)
-
Shoulder pain
-
Diagnosis
- Can be diagnosed clinically
- X-rays are usually obtained to rule out underlying pathology.
- MRI provides a definitive diagnosis but is typically not required.
-
Treatment [36][37]
- Physical therapy: early mobilization and exercise
- NSAIDs
- Oral corticosteroid (burst and taper) for severe pain
- Intraarticular corticosteroid injection
- Surgical treatment if symptoms persist after 9 months of conservative management [11]
- Prognosis: self-limiting (improvement typically takes > 1 year)
- Complications: atrophy of the deltoid and spinatus muscles

")
Frontal cross-section of the shoulder and the three stages of frozen shoulder
Stage 1 (freezing stage): minimal synovitis with pain and limitation of motion
Stage 2 (frozen stage): proliferative synovitis with contraction of the capsule and adhesion of the axillary recess
Stage 3 (thawing stage): contracted capsule following the end of inflammation
© AMBOSS
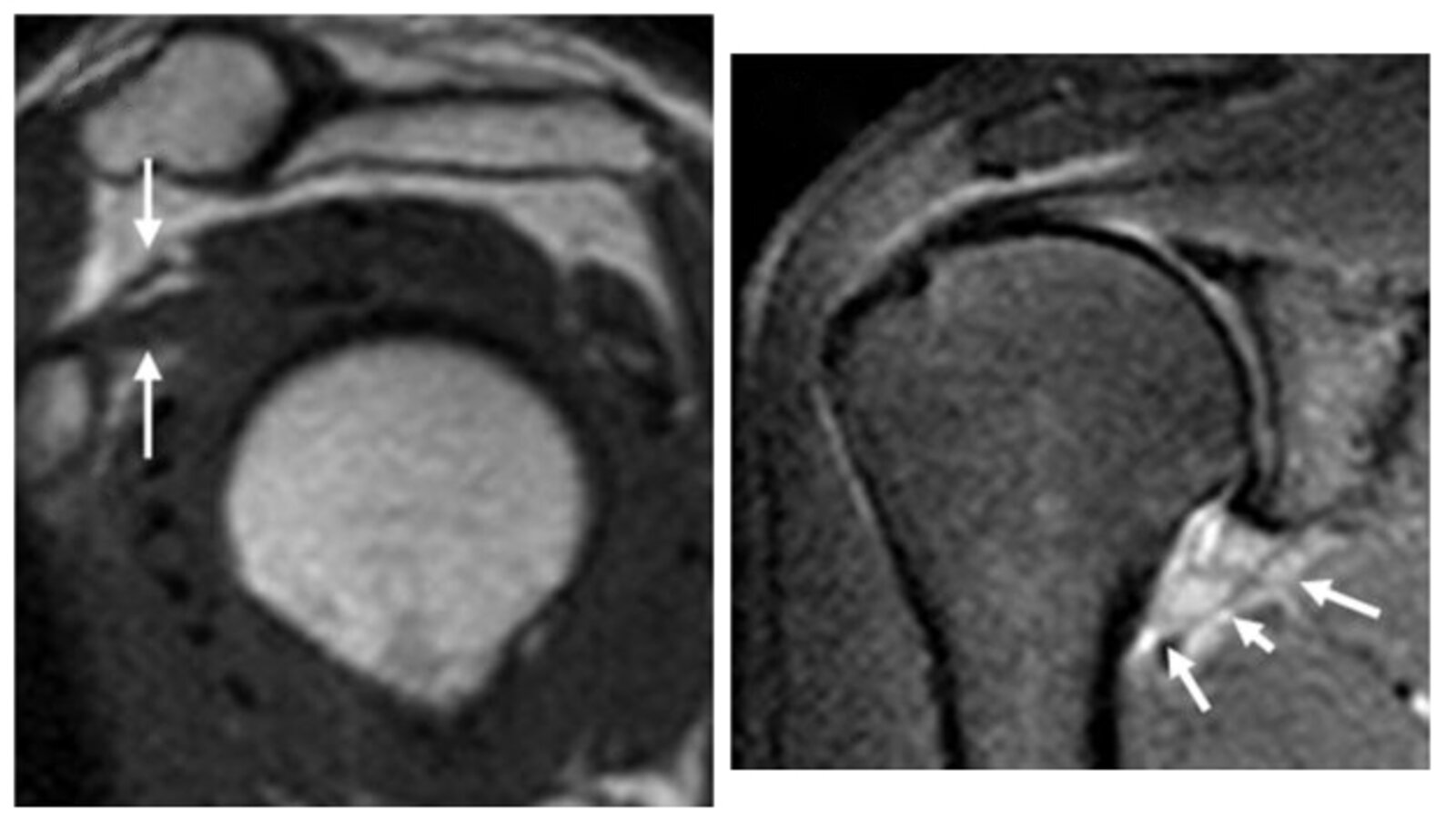
MRI shoulder (left: T1-weighted, sagittal oblique plane; right: fat-suppressed, proton density-weighted spin-echo, coronal oblique plane)
Thickening of the coracohumeral ligament (left, arrows) is seen. There is also thickening of the inferior glenohumeral ligament (right, arrows).
MR allows for visualization of several characteristic findings of adhesive capsulitis, including thickening of the coracohumeral ligament, glenohumeral ligament (axillary pouch), rotator interval capsule, and loss of the subcoracoid fat triangle.
Source: “Figure 1, from: MRI Findings for Frozen Shoulder Evaluation: Is the Thickness of the Coracohumeral Ligament a Valuable Diagnostic Tool?” by Jin-qing Li, Kang-lai, Tang,Jian Wang, Qi-yu Li, Hao-tong Xu, Hui-feng Yang, PLOS ONE, licensed under CC BY 3.0. Modifications: Cropped and merged.
Glenoid labrum injuries
The glenoid labrum can be damaged by an acute injury or overuse of the shoulder and arm.
Superior labrum from anterior to posterior lesion (SLAP lesion) [39]
- Definition: a tear of the superior glenoid labrum and the long head of the biceps tendon [39]
-
Etiology
- Overuse injury, e.g., microtrauma from repeated throwing motion (most common)
- Fall on an extended arm
-
Clinical features
- Shoulder pain
- Shoulder instability
- May be asymptomatic
-
Diagnostics
- Clinical evaluation
- Clinical tests for detecting SLAP lesions are of limited value.
- Positive Speed test, O'Brien test, and Yergason test may indicate an injury to the long head of the biceps.
- MRI and/or MRI arthrogram findings provide a definitive diagnosis.
- Clinical evaluation
-
Treatment
- Follow conservative therapy of shoulder soft tissue lesions.
- Arthroscopic surgical repair is indicated if symptoms persist after conservative treatment.
Bankart lesion [22][23]
- Definition: a tear of the anteroinferior portion of the glenoid labrum
- Etiology: acute anterior dislocation of the shoulder
-
Clinical features
- Shoulder pain
- Shoulder instability
- Recurrent dislocations
-
Diagnostics
- Clinical evaluation
- Positive anterior apprehension test
- Positive anterior drawer test of the shoulder
- MRI findings provide a definitive diagnosis.
- Clinical evaluation
-
Management [22][40]
- Follow treatment of acute shoulder dislocation for an acute dislocation.
- Most patients are treated conservatively with sling immobilization and physical therapy.
- Early surgical repair may be preferred for young active individuals to prevent recurrent dislocations.


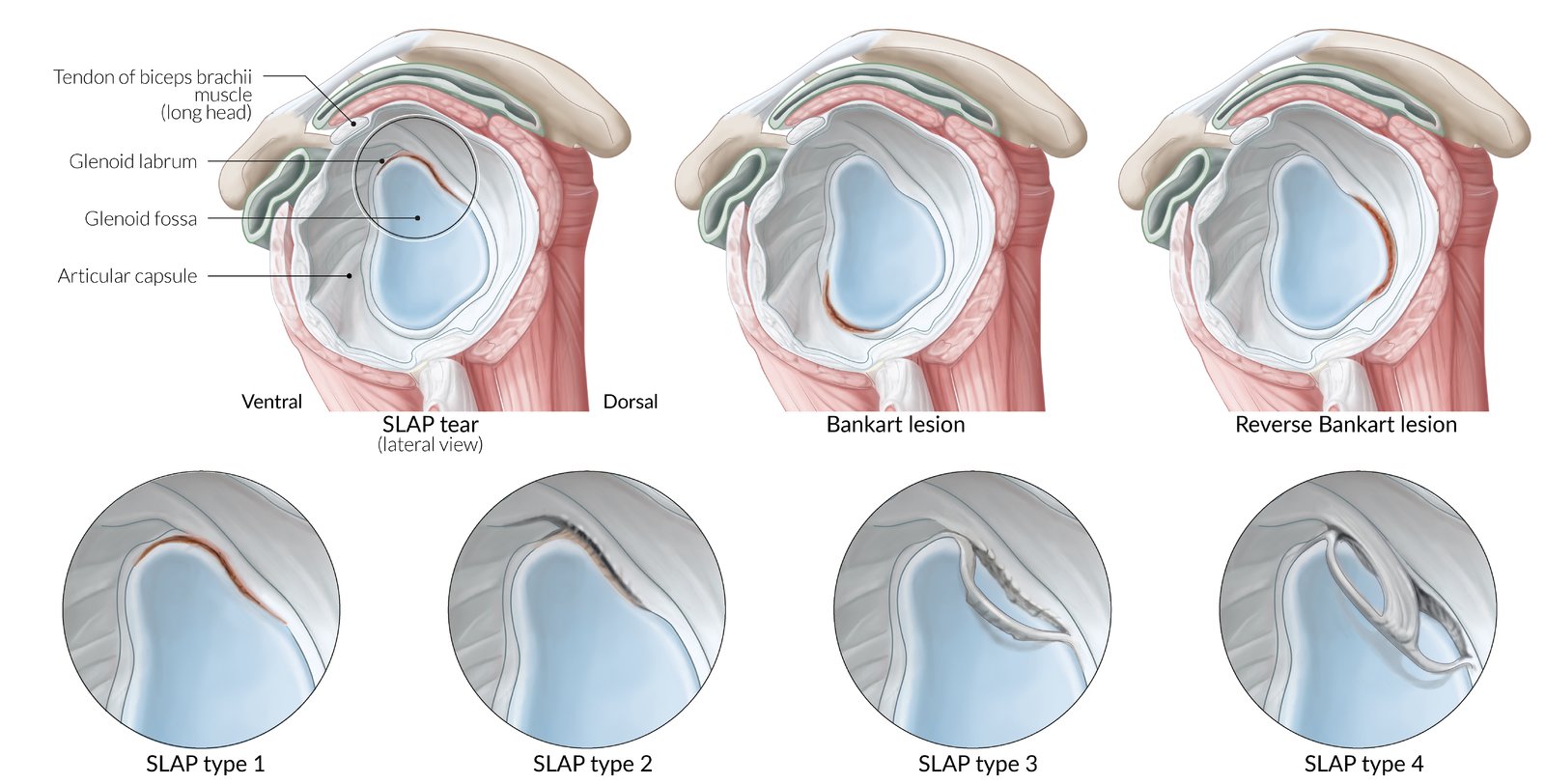
Lateral view of the shoulder joint. The upper three illustrations present different locations of a labral tear (from left to right):
Superior tear = SLAP lesion (“superior labral tear from anterior to posterior”; Anterior tear = Bankart lesion; Posterior tear = Reversed-Bankart lesion
The circle in the first example of the upper row marks the site of the detailed illustrations in the second row. It is the classification of SLAP lesions according to Synder:
I. Micro tears and degenerative findings; II. Detachment of the superior labrum and biceps tendon; III: Bucket-handle tear of the superior tendon; IV: Bucket-handle tear of the labrum that extends to the biceps tendon root
© AMBOSS
Click on the overlay icon below the taskbar on the left to toggle the overlay on and off.
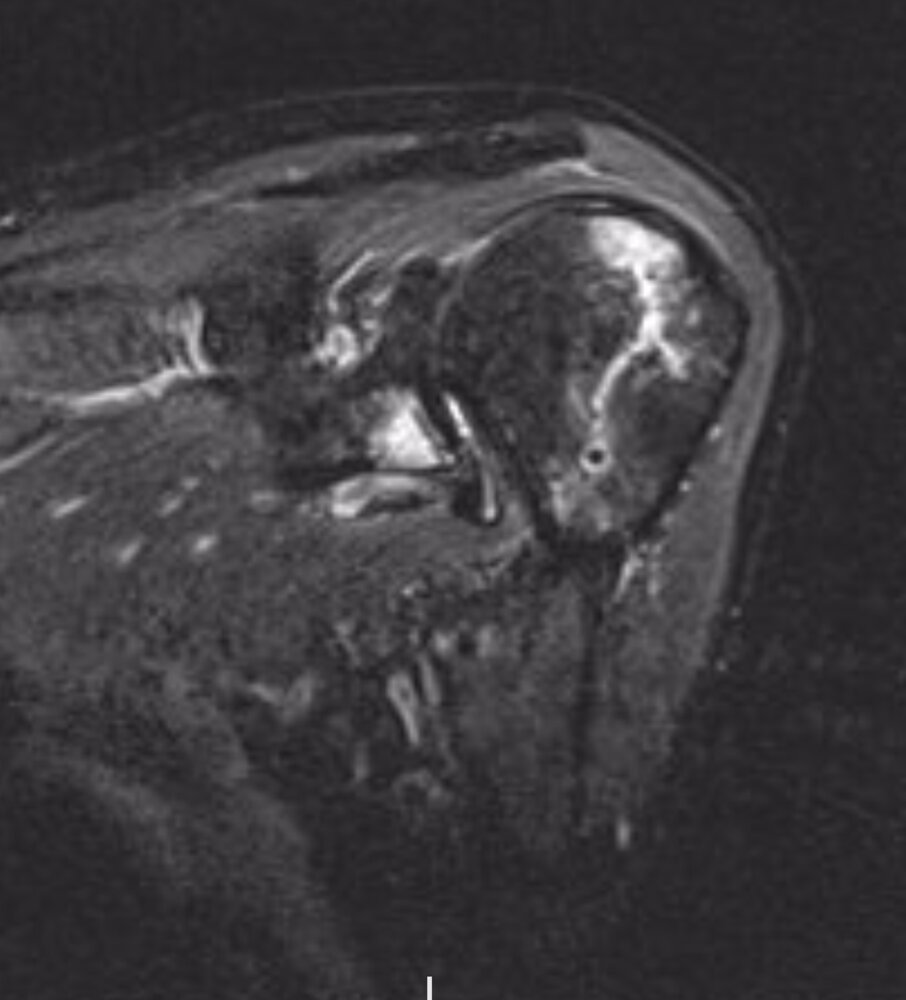
MRI left shoulder (STIR and T1, coronal plane; PD FS, axial and sagittal plane)
On the fat-saturated sequences (STIR and both PD images), there is hyperintensity in the posterolateral humeral head and anteroinferior glenoid rim with corresponding hypointensity on the T1 image. These findings indicate contusion. In addition, a depression in the cortex of the affected region of the humeral head (Hill-Sachs depression fracture) is seen. There is also a fracture through the affected anteroinferior glenoid (osseous or bony Bankart Lesion).
This pattern of injury occurs during anterior dislocation as the humeral head externally rotates and descends inferiorly, impacting the anteroinferior glenoid rim with its posterolateral surface.
Image source of original image: Radiologie Frechen-Erftstadt. Original title: “Anterior shoulder dislocation”. Created by: Markus Le Blanc.
References
- Burbank KM, Stevenson JH, Czarnecki GR, Dorfman J. "Chronic shoulder pain: part I. Evaluation and diagnosis". Am Fam Physician. 77(4). :453-60. (2008)
- Armstrong A. "Evaluation and Management of Adult Shoulder Pain". Med Clin North Am. 98(4). :755-775. (2014)
- Nazarian LN, Jacobson JA, Benson CB, et al. "Imaging Algorithms for Evaluating Suspected Rotator Cuff Disease: Society of Radiologists in Ultrasound Consensus Conference Statement". Radiology. 267(2). :589-595. (2013)
- McNally EG, Rees JL. "Imaging in shoulder disorders". Skeletal Radiol. 36(11). :1013-1016. (2007)
- Small KM, Adler RS, Shah SH, et al. "ACR Appropriateness Criteria® Shoulder Pain-Atraumatic". J Am Coll Radiol. 15(11). :S388-S402. (2018)
- Sherman SC. "Simon's Emergency Orthopedics, 8th edition". McGraw Hill Professional. (2018). ISBN: 9781259860836
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904
- Hinsley H, Nicholls A, Daines M, et al. "Classification of rotator cuff tendinopathy using high definition ultrasound". Muscles, ligaments and tendons journal. 4(3). :391-7. (2014)
- Fischer CA, Weber MA, Neubecker C, et al. "Ultrasound vs. MRI in the assessment of rotator cuff structure prior to shoulder arthroplasty". J Orthop. 12(1). :23-30. (2015)
- Burbank KM, Stevenson JH, Czarnecki GR, Dorfman J. "Chronic shoulder pain: part II. Treatment". Am Fam Physician. 77(4). :493-7. (2008)
- "Gay and Bisexual Men's Health For Your Health: Recommendations for A Healthier You". https://web.archive.org/web/20230421190704/https://www.cdc.gov/msmhealth/for-your-health.htm. [2022-09-16]
- Belk JW, Wharton BR, Houck DA, et al. "Shoulder Stabilization Versus Immobilization for First-Time Anterior Shoulder Dislocation: A Systematic Review and Meta-analysis of Level 1 Randomized Controlled Trials". Am J Sports Med. 51(6). :1634-1643. (2022)
- Loh B, Lim JBT, Tan AHC. "Is clinical evaluation alone sufficient for the diagnosis of a Bankart lesion without the use of magnetic resonance imaging?". Ann Transl Med. 4(21). :419-419. (2016)
- Harrison AK, Flatow EL. "Subacromial Impingement Syndrome". Am Acad Orthop Surg. 19(11). :701-708. (2011)
- Umer M, Qadir I, Azam M. "Subacromial impingement syndrome". Orthop Rev (Pavia). 4(2). :18. (2012)
- McFarland E, Bernard J, Dein E, Johnson A. "Diagnostic injections about the shoulder". J Am Acad Orthop Surg. 25(12). :799-807. (2017)
- Tallia AF, Cardone DA. "Diagnostic and therapeutic injection of the shoulder region". Am Fam Physician. 67(6). :1271-8. (2003)
- MacDonald PB, Clark P, Sutherland K. "An analysis of the diagnostic accuracy of the Hawkins and Neer subacromial impingement signs". Journal of Shoulder and Elbow Surgery. 9(4). :299-301. (2000)
- Ramirez J. "Adhesive Capsulitis: Diagnosis and Management". Am Fam Physician. 99(5). :297-300. (2019)
- Siegel LB, Cohen NJ, Gall EP. "Adhesive capsulitis: a sticky issue". Am Fam Physician. 59(7). :1843-52. (1999)
- Redler LH, Dennis ER. "Treatment of Adhesive Capsulitis of the Shoulder". J Am Acad Orthop Surg. 27(12). :e544-e554. (2019)
- Le HV, Lee SJ, Nazarian A, Rodriguez EK. "Adhesive capsulitis of the shoulder: review of pathophysiology and current clinical treatments". Shoulder Elbow. 9(2). :75-84. (2016)
- Date A, Rahman L. "Frozen shoulder: overview of clinical presentation and review of the current evidence base for management strategies". Future Science OA. 6(10). (2020)
- Weber S, Chahal J. "Management of Rotator Cuff Injuries". J Am Acad Orthop Surg. 28(5). :e193-e201. (2020)
- Hsu J, Keener JD. "Natural History of Rotator Cuff Disease and Implications on Management". Operative Techniques in Orthopaedics. 25(1). :2-9. (2015)
- Dang A, Davies M. "Rotator Cuff Disease: Treatment Options and Considerations". Sports Med Arthrosc. 26(3). :129-133. (2018)
- Perry SM, Getz CL, Soslowsky LJ. "After rotator cuff tears, the remaining (intact) tendons are mechanically altered". J Shoulder Elbow Surg. 18(1). :52-57. (2009)
- Karjalainen TV, Jain NB, Heikkinen J, et al. "Surgery for rotator cuff tears". Cochrane Database Syst Rev. (2019)
- Reinholz AK, Till SE, Arguello AM, et al. "Advances in the Treatment of Rotator Cuff Tears". Clin Sports Med. 42(1). :69-79. (2023)
- Lazarides AL, Alentorn-Geli E, Choi JHJ, et al. "Rotator cuff tears in young patients: a different disease than rotator cuff tears in elderly patients". J Shoulder Elbow Surg. 24(11). :1834-1843. (2015)
- Kim MS, Kim IW, Lee S, Shin SJ. "Diagnosis and treatment of calcific tendinitis of the shoulder". Clin Shoulder Elbow. 23(4). :210-216. (2020)
- Merolla G, Singh S, Paladini P, Porcellini G. "Calcific tendinitis of the rotator cuff: state of the art in diagnosis and treatment". J OrthopTraumatol. 17(1). :7-14. (2015)
- Chianca V, Albano D, Messina C, et al. "Rotator cuff calcific tendinopathy: from diagnosis to treatment". Acta Biomedica. 89(1-S). :186-196. (2018)
- Murphy RJ, Carr AJ. "Shoulder pain.". BMJ Clin Evid. 2010. (2010)
- Zhao J, Luo M, Liang G, et al. "Risk Factors for Supraspinatus Tears: A Meta-analysis of Observational Studies". Orthop J Sports Med. 9(10). :232596712110428. (2021)
- Kulkarni R, Gibson J, Brownson P, et al. "Subacromial shoulder pain". Shoulder Elbow. 7(2). :135-143. (2015)
- Wolfson AB. "Harwood-Nuss' Clinical Practice of Emergency Medicine". LWW. (2014). ISBN: 9781451188813
- Seo JB, Yoo JS, Ryu JW. "Sonoelastography findings of biceps tendinitis and tendinosis". J Ultrasound. 17(4). :271-277. (2014)
- Brockmeyer M, Tompkins M, Kohn DM, Lorbach O. "SLAP lesions: a treatment algorithm". Knee Surgery, Sports Traumatology, Arthroscopy. 24(2). :447-455. (2016)
- Boffano M, Mortera S, Piana R. "Management of the first episode of traumatic shoulder dislocation". EFORT Open Rev. 2(2). :35-40. (2017)