Quick guide
Diagnostic approach
- ABCDE survey
- Identify sensory level.
- Segmental motor testing for key myotomes (C5–T1, L2–S1)
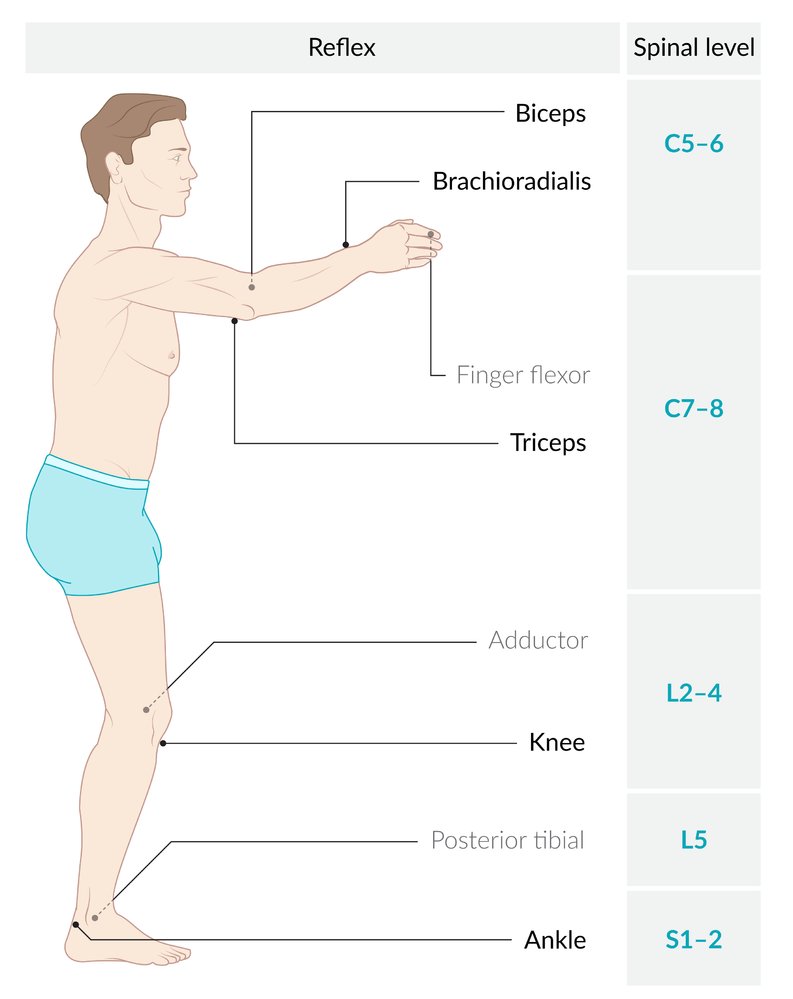
- Grade deep tendon reflexes.
- Digital rectal exam
- Imaging for SCI (e.g., noncontrast CT spine)
- Additional diagnostics for trauma as needed


Red flag features
- Complete SCI above C4
- Unstable vertebral injury
- Paraplegia or tetraplegia
- Areflexia
- Bilateral diaphragm paralysis
- Neurogenic shock
- Loss of bladder control
- Loss of bowel control (e.g., paralytic ileus)
- Priapism
Absence of sacral sparing in the acute phase typically indicates a high degree of autonomic dysfunction
Management checklist
- Consult a spine surgeon urgently.
- Apply spinal motion restrictions.
- Monitor for impending respiratory failure.
- Initiate blood pressure management for SCI.
- Insert a urinary catheter early.
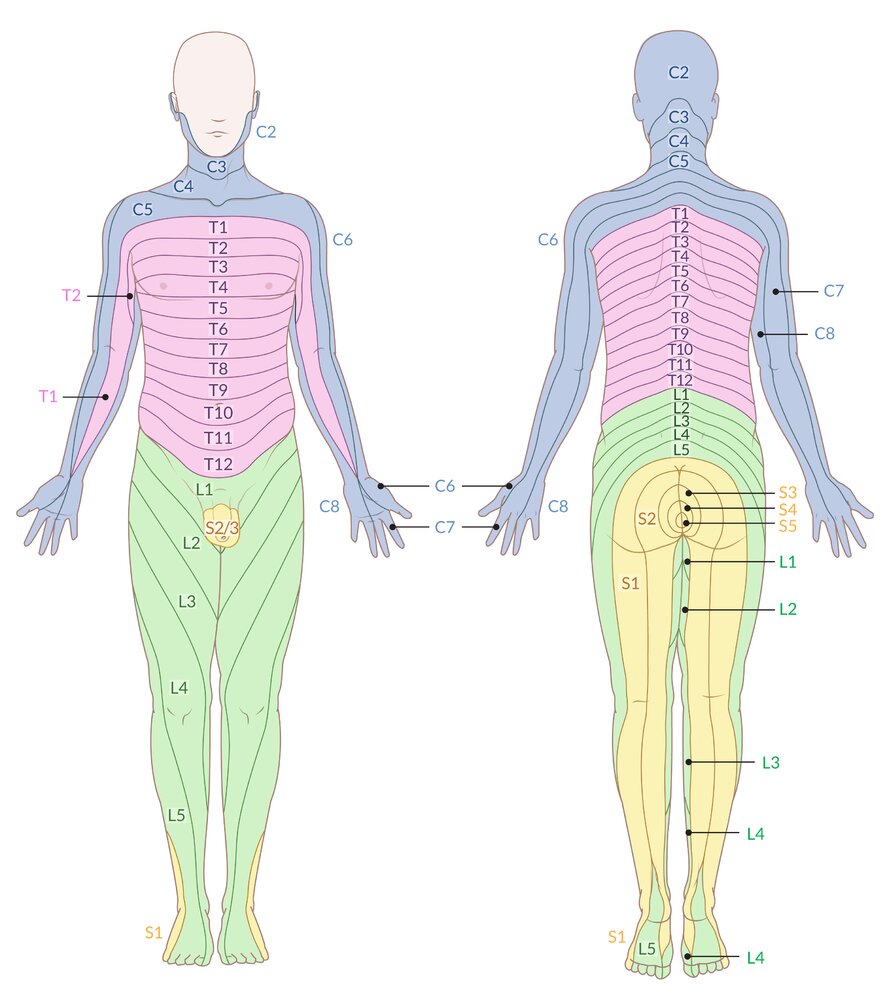
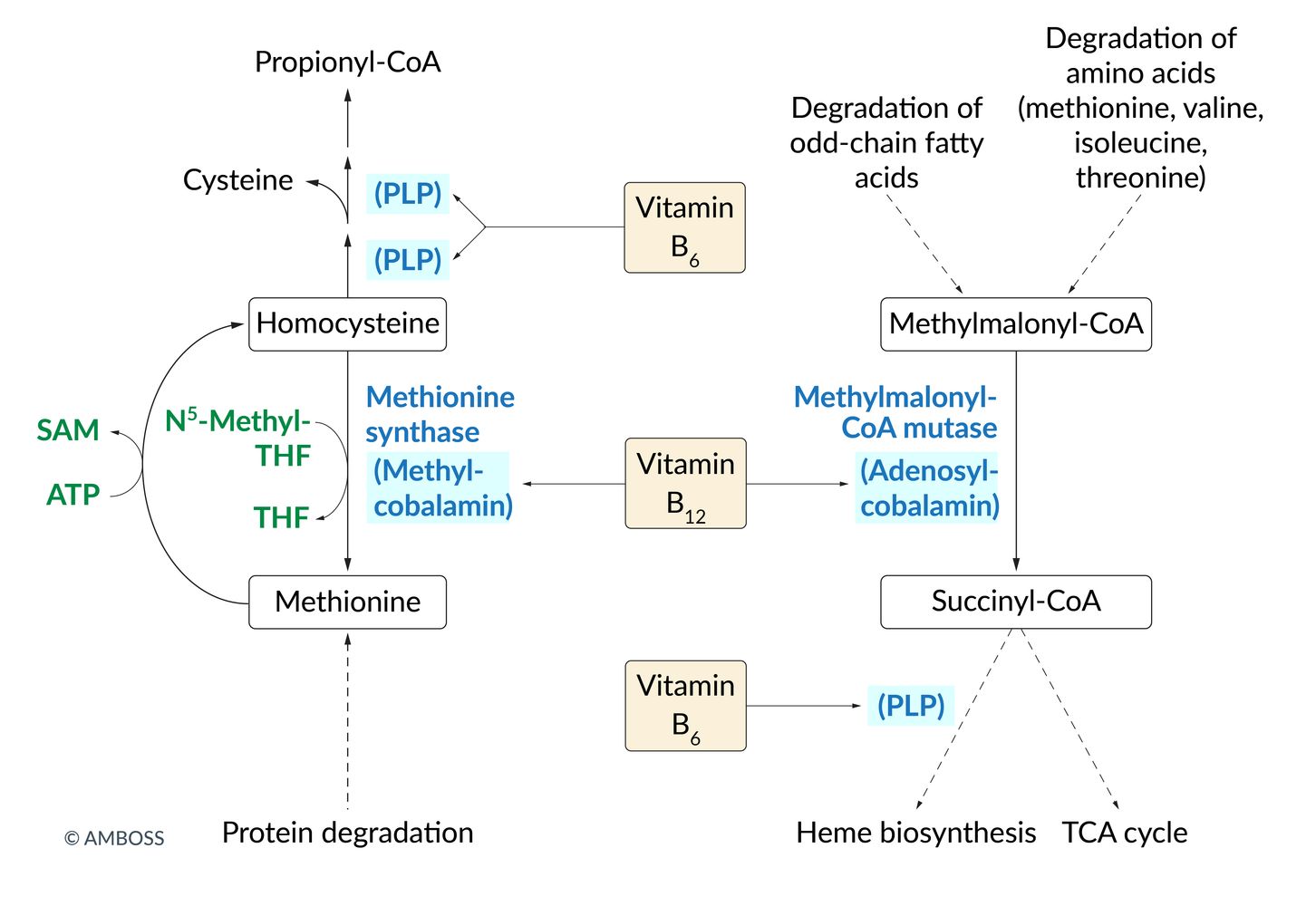
Schematic representation of the body's dermatomes (i.e., areas of skin that are innervated by a single sensory spinal root)
Note: Nearly all dermatome maps refer to publications by Head and Campbell (1900), Foerster (1933), or Keegan and Garrett (1948), which differ significantly in some areas. After careful review of the current literature, this illustration has been based on Keegan and Garrett's work, as it is most likely to be based on valid methodology and correlates with established clinical findings.
© AMBOSS
© AMBOSS
Summary
Spinal cord injuries (SCIs) result from trauma (e.g., motor vehicle crashes and falls) or nontraumatic causes (i.e., ischemic, compressive, or inflammatory). SCIs initially manifest with an acute phase of spinal shock, characterized by flaccid areflexic paralysis, anesthesia, and autonomic dysfunction that occurs below the level of the injury. Spinal shock typically resolves within 48 hours, leading to a chronic phase of incomplete or complete SCI, depending on whether the spinal cord has been partially or completely transected. Symptoms of complete SCI typically occur 6–8 weeks after resolution of spinal shock and include bilateral absence of sensory and motor function, muscle hypertonia with spastic paralysis, and hyperreflexia below the level of the lesion. Diagnosis requires serial neurological examinations and imaging (e.g., CT and MRI spine). Acute management includes spinal stabilization, respiratory and hemodynamic support, urinary catheterization, and analgesia; operative management typically involves surgical decompression and stabilization. SCIs can lead to several complications in the acute and chronic phases, including autonomic dysreflexia, which can cause life-threatening episodes of cardiovascular instability.
This article focuses on the complete transection of the spinal cord. For more information on incomplete SCIs, see “Incomplete spinal cord syndromes.”
Overview
-
Complete spinal cord injury
- SCI caused by a lesion affecting all spinal tracts at a given spinal level (e.g., complete transection)
- Results in total bilateral loss of communication between the nerve fibers above and below the level of the lesion
- Characterized by a complete absence of motor, sensory, bowel, and bladder function below the level of injury
-
Incomplete spinal cord injury
- SCI caused by a lesion affecting select parts of the ascending or descending spinal tracts at a given spinal level
- Characterized by dissociated sensory loss with preservation of some sensorimotor functions below the level of injury
- For more information, see ''Incomplete spinal cord syndromes.''
- Spinal shock: acute transient loss or depression of all sensorimotor functions and reflexes below the level of an SCI
Do not confuse spinal shock with neurogenic shock.
SCI can occur with or without vertebral fractures or dislocations. Even when these coincide, the neurological level of injury does not always correspond to the skeletal level. [1]
Etiology
Traumatic [2]
- Motor vehicle crashes
- Falls (e.g., especially in older adults)
- Severe sports injuries (e.g., diving, skiing)
- Stab wounds and gunshot wounds
- Iatrogenic injuries (e.g., following spinal surgery, due to antiplatelet agents) [3]
Nontraumatic [4]
- Ischemic (e.g., atherosclerosis, aortic dissection, due to clamping during surgery, emboli)
- Inflammatory (e.g., multiple sclerosis, transverse myelitis)
- Compressive (e.g., spinal tumors, spinal abscesses, hematomas)
Pathophysiology
- Spinal cord injuries usually occur in conjunction with vertebral column injuries.
- Mechanisms of injury
- Primary (immediate effect) → direct trauma (e.g., due to compression or contusion) → irreversible damage to neural tissue
- Secondary (take effect in minutes to hours) → hypoxia, increased oxidative stress, inflammation, lipid peroxidation, cell apoptosis → injury to adjacent tissue
Clinical features
The features of SCI depend on the level and severity of injury and the amount of affected spinal tissue. Most individuals with traumatic SCI have associated brain and systemic injuries (e.g., hemothorax, extremity fractures).
Acute phase (spinal shock)
- Progression: immediately after an SCI, typically resolves within 48 hours [5]
-
Clinical features [6]
-
Flaccid, areflexic paralysis
- Paraplegia or tetraplegia (if the cervical cord is involved)
- Areflexia: absence of the proprioceptive and polysynaptic reflexes (e.g., abdominal reflex)
- Bilateral diaphragm paralysis: impaired breathing
- Anesthesia: below the level of the lesion
-
Autonomic dysfunction
- Neurogenic shock: hypotension and bradycardia
- Loss of bladder control: urine retention, bladder distention, and dribbling incontinence
- Loss of bowel control: paralytic ileus, fecal incontinence
- Absent bulbocavernosus reflex: fecal incontinence
- Priapism
-
Flaccid, areflexic paralysis
Absence of sacral sparing in the acute phase typically indicates a high degree of autonomic dysfunction.
Neurological deficits due to SCI should be evaluated after the resolution of spinal shock.
A complete SCI above C4 can be life-threatening because of the risk of diaphragmatic paralysis.
Chronic phase
As spinal shock resolves, reflexes and spinal cord function gradually return.
- In mild injuries that spare some of the spinal nerve pathways, the return of any neurological function after resolution of spinal shock indicates an incomplete SCI. For more information on this type of SCI, see ''Incomplete spinal cord syndromes.''
- In the case of complete spinal cord transection, the persistence of total neurological impairment after resolution of spinal shock indicates a complete SCI with a poor prognosis.
Complete spinal cord injury
- Progression: Symptoms typically occur 6–8 weeks after spinal shock has resolved.
-
Clinical features
- Below the level of lesion
- Bilateral absence of sensory and motor function (including sacral segments S4–S5)
- Muscle hypertonia with spastic paralysis
- Hyperreflexia
- Inexhaustible clonus (e.g., ankle clonus)
- Bilateral diaphragm paralysis: impaired breathing, coughing, and sneezing
- Absent anal reflex
- Pathological reflexes (e.g., positive Babinski reflex)
- Autonomic dysfunction
- Spastic bladder: detrusor sphincter dyssynergia
- Neurogenic bowel: constipation/bowel impaction, fecal incontinence, diarrhea
- Erectile dysfunction
- Below the level of lesion
Features of complete SCI classically occur 6–8 weeks after resolution of spinal shock and include spastic paralysis, hyperreflexia, and the presence of pathological reflexes (e.g., plantar reflex) below the level of injury.
Classification
Neuroanatomic classification
- Complete SCI
-
Incomplete SCI
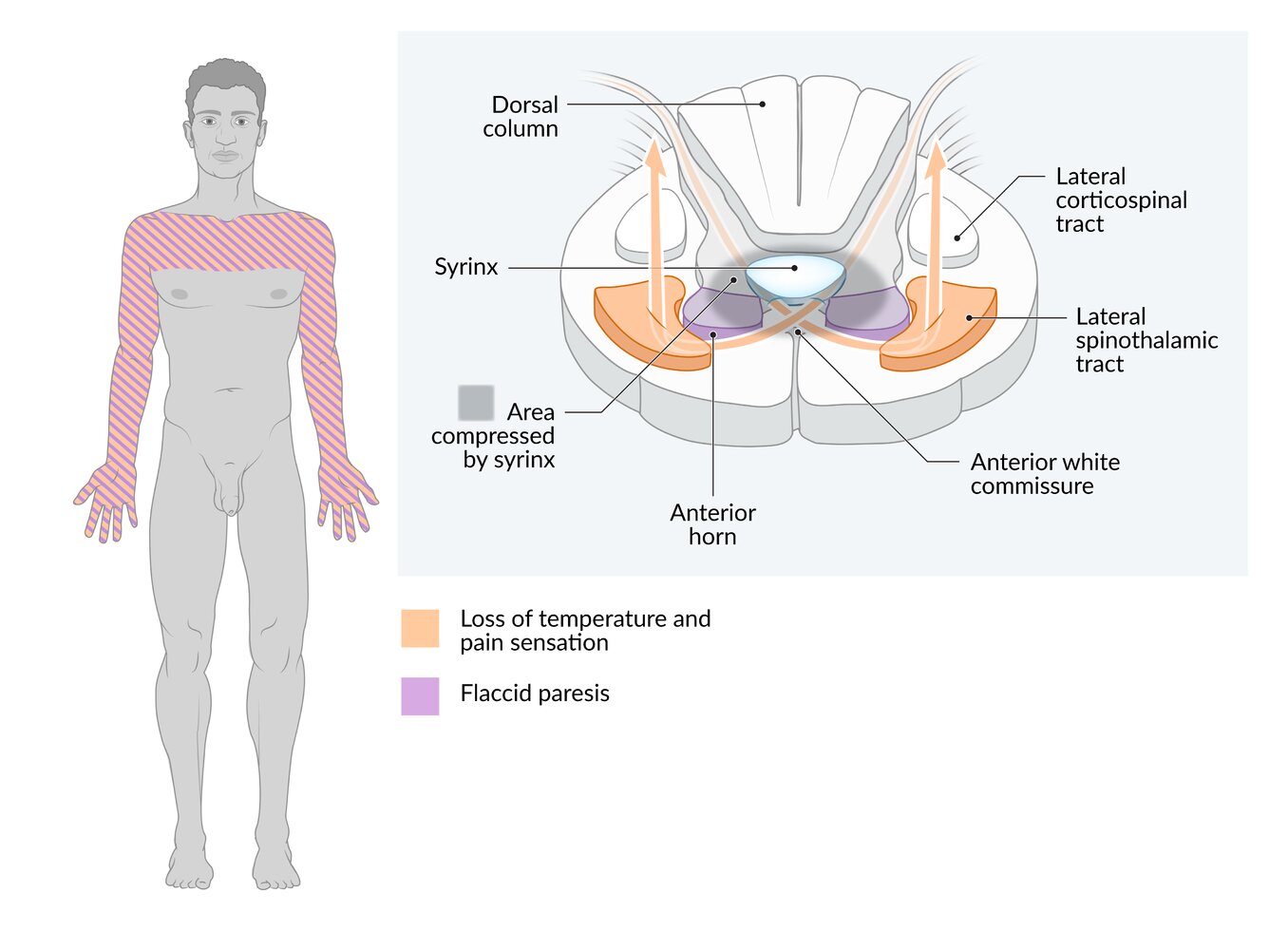
- Central cord syndrome
- Anterior cord syndrome
- Posterior cord syndrome
- Brown-Séquard syndrome
- Conus medullaris syndrome
- Cauda equina syndrome
American Spinal Injury Association (ASIA) impairment scale [1]
A system used to classify SCI severity once spinal shock is resolved
- Complete: Grade A; no sacral sparing
-
Sensory incomplete: Grade B
- Sensory but not motor sacral sparing
- AND no motor function > 3 levels below the level of SCI
-
Motor incomplete
- Sensory OR motor sacral sparing present
- Sparing of motor function > 3 levels below the level of SCI
-
Proportion of muscle groups below the level of injury that can actively move against gravity
- < 50%: Grade C
- ≥ 50%: Grade D
- Normal: Grade E; normal function in a patient with prior deficits
Do not use the ASIA scale to evaluate SCI severity while the patient still has spinal shock. [1]
Diagnosis
Approach [1][5][7]
- Perform a detailed neurological examination to determine the neurological level of injury. [1]
- Identify the sensory level.
- Perform segmental motor testing for key paired myotomes (i.e., C5–T1 and L2–S1).
- Grade deep tendon reflexes.
- Check tone and sensation on digital rectal examination.
- Document SCI severity, e.g., using the ASIA scale.
- Obtain imaging for SCI to evaluate suspected injuries and facilitate preoperative planning.
- Obtain other diagnostics for trauma as needed, e.g., TBI diagnostics.
Imaging for SCI [5][7][8]
- X-rays: not recommended for screening or evaluation of SCI because of low sensitivity
-
CT spine without IV contrast: test of choice to assess for vertebral fractures and dislocations
- Usually obtained as the initial study
- Less sensitive than MRI for soft tissue injuries
-
MRI spine: test of choice to evaluate for SCI [9]
- Indications: concern for SCI based on clinical or CT findings
- More sensitive than CT for spinal cord, nerve root, disc, and ligamentous lesions
- CTA or MRA: indicated if there is suspicion for vascular injury (e.g., due to penetrating trauma or BCVI)
In patients with blunt trauma, use the NEXUS criteria, Canadian C-spine rule, and/or indications for imaging the thoracic and/or lumbar spine to determine if imaging is indicated. [5][8][10]





Schematic representation of the body's dermatomes (i.e., areas of skin that are innervated by a single sensory spinal root)
Note: Nearly all dermatome maps refer to publications by Head and Campbell (1900), Foerster (1933), or Keegan and Garrett (1948), which differ significantly in some areas. After careful review of the current literature, this illustration has been based on Keegan and Garrett's work, as it is most likely to be based on valid methodology and correlates with established clinical findings.
© AMBOSS
© AMBOSS

MRI cervical spine (T2-weighted; sagittal view) in a patient with a previous C4 vertebral body fracture
There is subtle increased signal within the spinal cord extending from the level of the 3rd to 5th cervical vertebral bodies; this segment of the cord also appears swollen. This represents myelopathy. High signal is shown within the soft tissues surrounding the spinous processes of the 2nd to 6th cervical vertebrae. The patient underwent surgery for a C4 cervical spine fracture prior to this MRI, and this soft tissue high signal is likely related to this. Some of the signal may also be due to the initial traumatic event that resulted in the C4 fracture.
Myelopathy is a broad term meaning disease of the spinal cord. It can be due to various causes, one of the most common being compression of the cord due to trauma, as seen here.
Source: © IMPP

MRI cervical spine (T2-weighted; sagittal plane) of a 58-year-old patient on long-term warfarin therapy presenting with acute tetraplegia
A region of heterogeneous signal lies along the posterior aspect of the spinal canal (indicated by arrows), between the dura and vertebral canal, representing a hematoma. The hematoma displaces the spinal cord anteriorly and compresses it, most prominently between the levels of C3 and C7. At the level of C7, there is an oval area of hyperintense signal within the spinal cord (arrowhead), representing myelopathic change (injury to the spinal cord).
Source: “Fig. 1, in: Anti-coagulation Drug Warfarin Contributes to Severe Adverse Outcomes in Prolonged Unsupervised Use: A Double-edged Sword” by Ordookhanian C, Kaloostian SW, Kaloostian PE, Cureus, licensed under CC BY 3.0. Modifications: Arrows have been removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

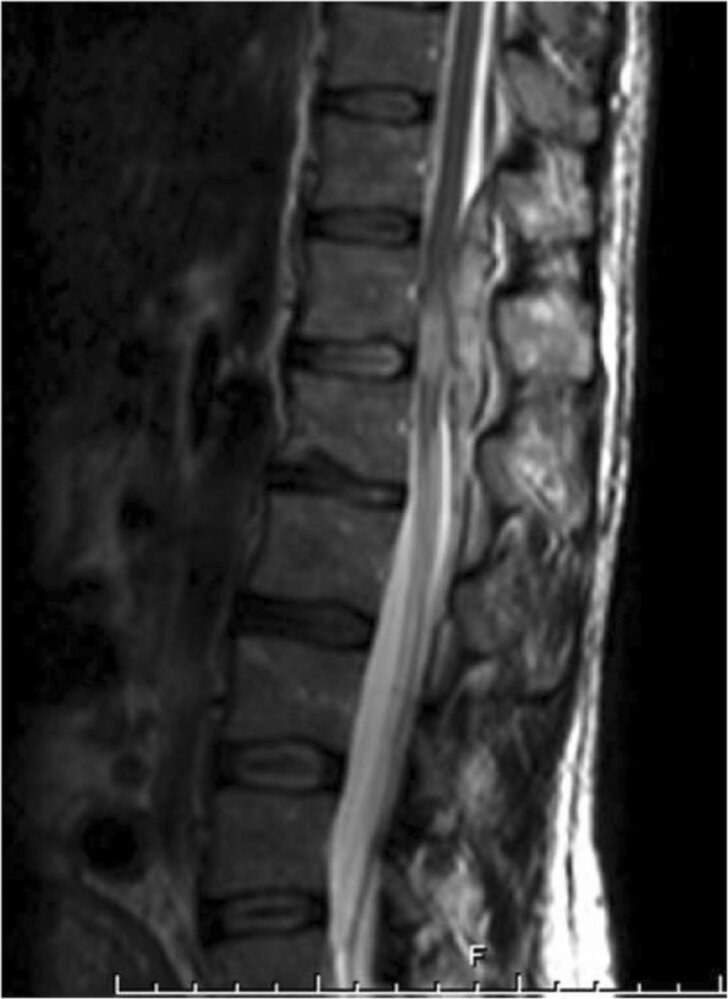
MRI lumbar spine (T2-weighted; sagittal plane) after L4 laminectomy
After decompressive surgery with laminectomy of L4, there is an extensive, heterogeneous hyperintense mass (overlay) in the operative access path at the level of L4 and in the posterior epidural space with maximum extension at the level of L2–L5. Here, the cauda equina is displaced anteriorly and markedly compressed.
The findings are consistent with a postoperative lumbar epidural hematoma.
Source: “Figure 2A, in: Unplanned revision spinal surgery within a week: a retrospective analysis of surgical causes” by T.-T. Tsai, S.-H. Lee, C.-C. Niu et al., BMC - Musculoskeletal Disorders, licensed under CC BY 4.0. Modifications: Original image was made up of 2 images. Arrows and "the A" removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
MRI spine (T2-weighted; sagittal plane)
A hyperintense collection (green overlay) in the posterior spinal epidural space at level T11–L1 causes a narrowing of the spinal canal and compression of the spinal cord. There is an increased T2 signal (red overlay) within the cord, likely reflecting cord edema.
These findings are consistent with spinal epidural hematoma.
Source: “Figure 1, in: Case report: difficulty in diagnosis of delayed spinal epidural hematoma in puerperal women after combined spinal epidural anaesthesia” by A. Svelato, A. Rutili, C. Bertelloni et al., BMC - Anesthesiology, licensed under CC BY 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
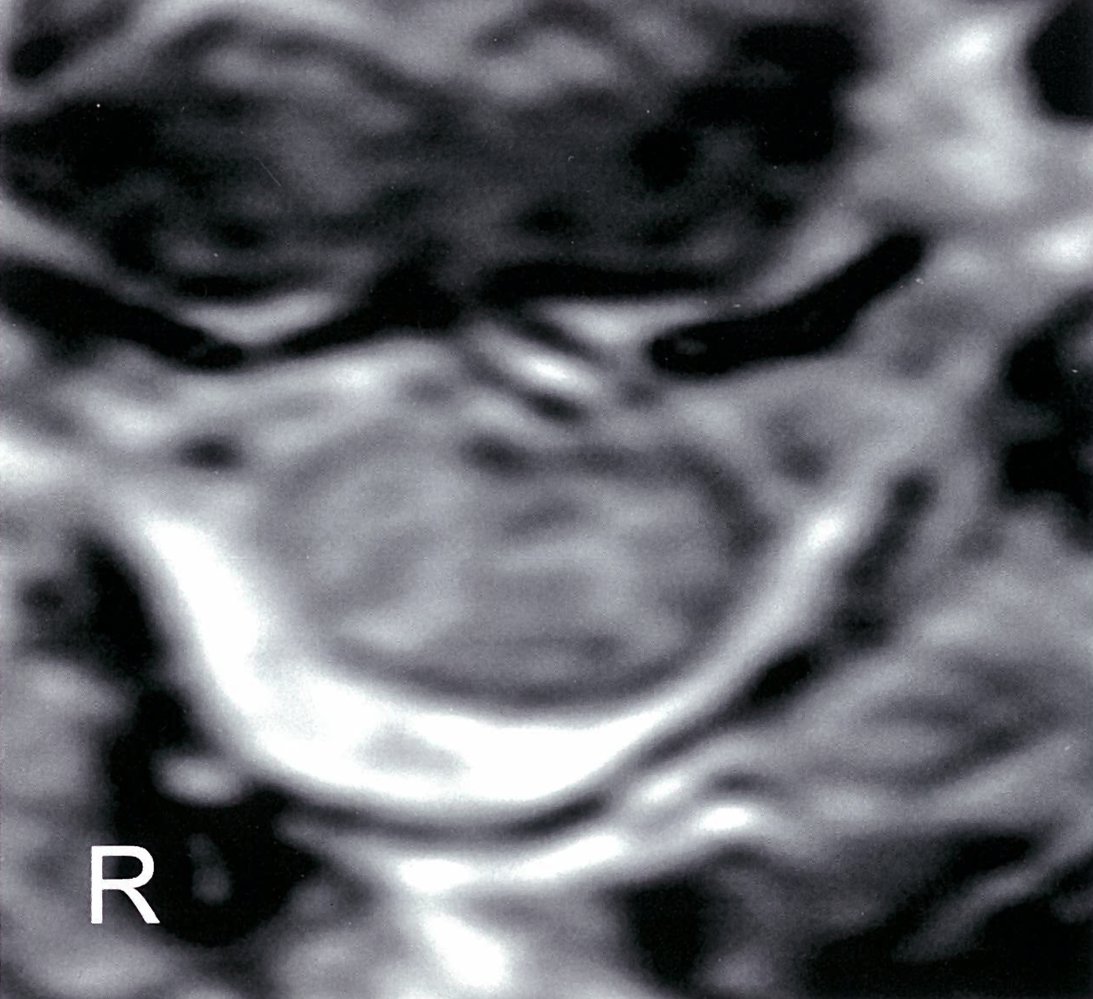
MRI cervical spine (T2-weighted; axial view) of a patient with a vertebral body fracture
Multiple regions of hyperintense signal are visible within the grey and white matter of the spinal cord, indicating myelopathy. In this patient, the myelopathy was caused by direct trauma.
Source: © IMPP
Differential diagnoses
See “Weakness and paralysis.”
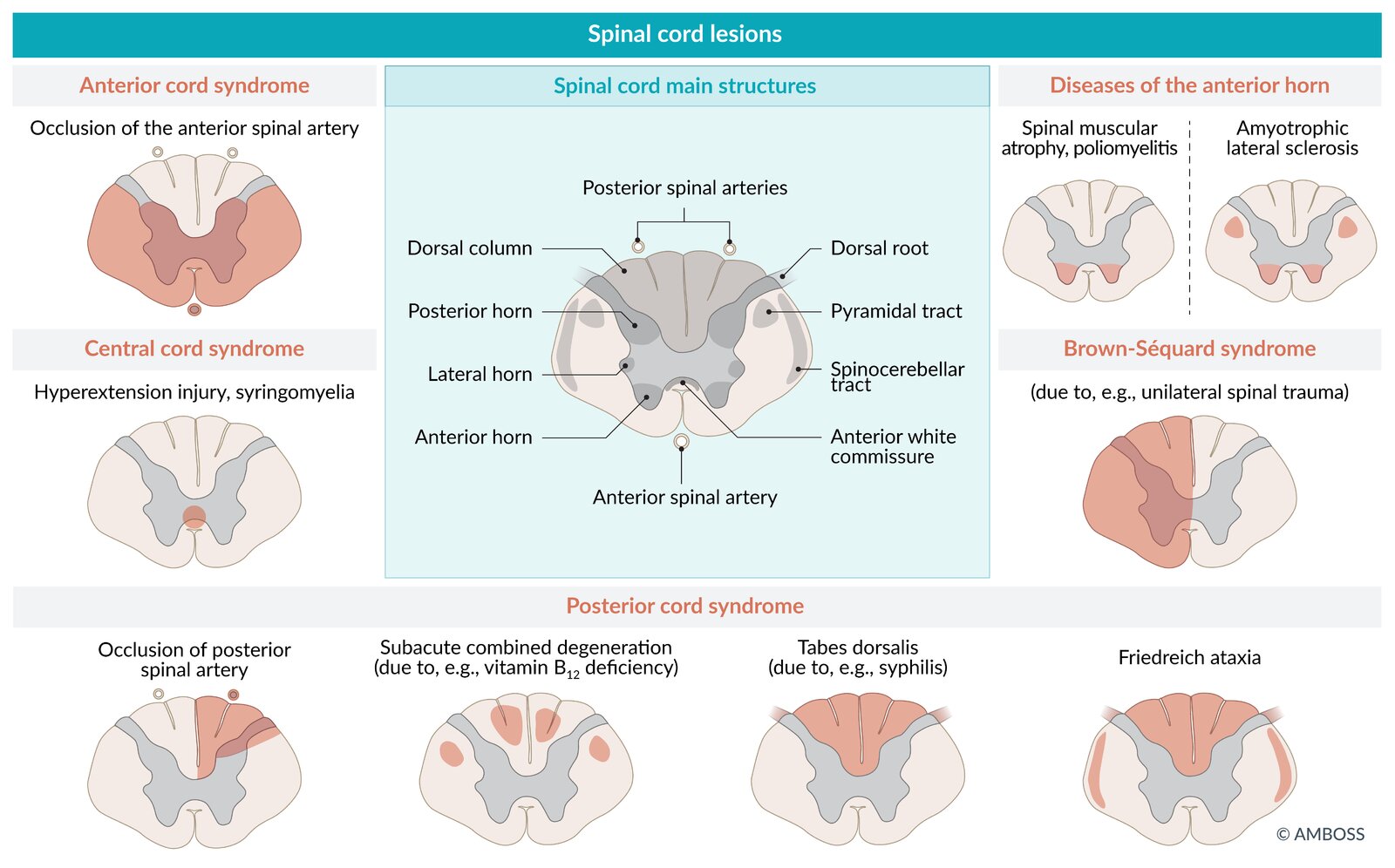
Overview of spinal cord lesions
| Spinal cord lesions | |||
|---|---|---|---|
| Pathophysiology | Affected spinal tracts | Clinical features | |
| Syringomyelia |
|
|
|
| Spinal muscular atrophy |
|
|
|
| Amyotrophic lateral sclerosis |
|
|
|
| Multiple sclerosis |
|
|
|
| Poliomyelitis |
|
|
|
| Tabes dorsalis |
|
|
|
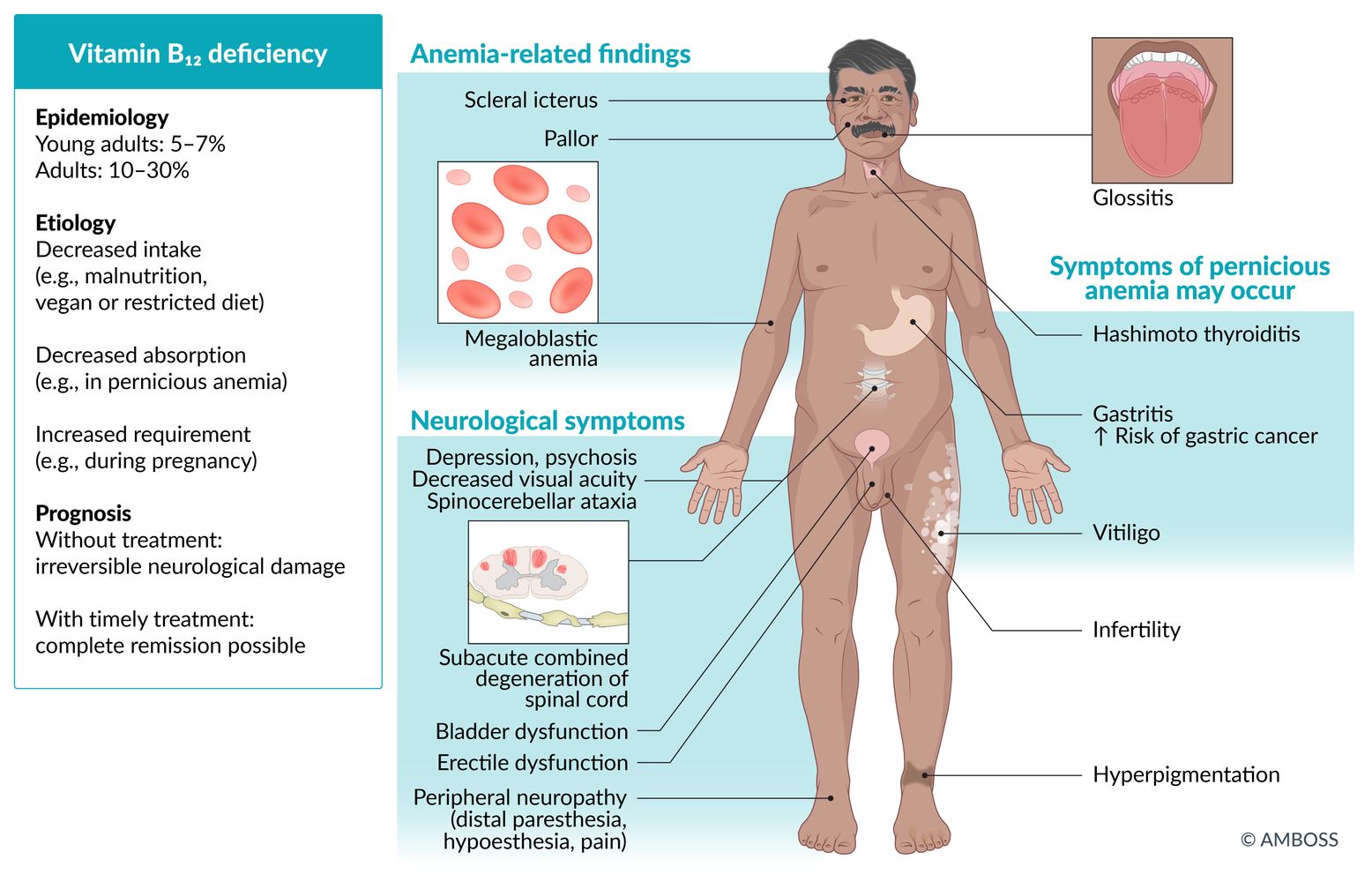
| Vitamin B12 deficiency |
|
|
|






The differential diagnoses listed here are not exhaustive.
© AMBOSS
© AMBOSS

MRI of the cervical spine (T2 weighted; sagittal view)
The majority of the spinal column appears hyperintense (green overlay), it normally appears hypointense on T2-weighted images.
This is the typical radiographical appearance of a syrinx in syringomyelia.
Source: “Figure 1. in: Shunting of recurrent post-traumatic syringomyelia into the fourth ventricle: a case report” by Chih-Lung Lin, Journal of Medical Case Reports, licensed under CC BY 2.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
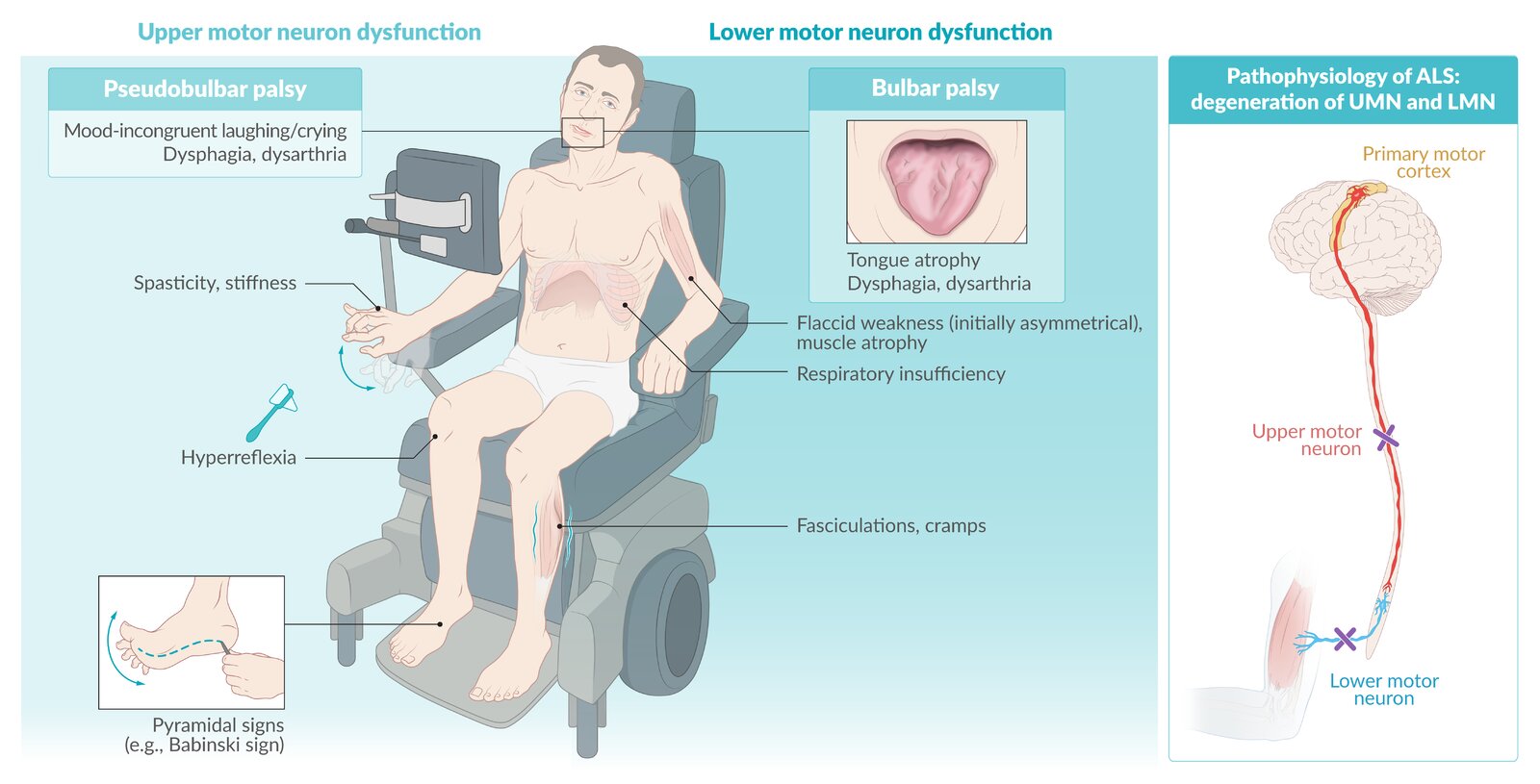
Amyotrophic lateral sclerosis is a neurodegenerative disease that affects the entire motor neuron system (degeneration of the upper motor neuron in the precentral gyrus and lower motor neuron in the brainstem or anterior horn of the spinal cord). The disease most commonly manifests between 50 and 70 years of age, often beginning with unilateral weakness in the hands or feet, which then progresses to the contralateral side (asymmetric limb weakness). However, initial manifestations are highly variable and individuals may have atypical or nonspecific symptoms such as subtle vocal changes. As the disease progresses, most individuals eventually develop one or both of the life-threatening symptoms: respiratory impairment and dysphagia.
© AMBOSS
© AMBOSS
© AMBOSS
Treatment
The following reviews the management of a confirmed SCI. For vertebral column trauma, see “Initial management of vertebral injuries.”
Initial management [5][11][12][13]
Urgently consult a critical care or trauma specialist and spine surgeon (e.g., neurosurgery or orthopedics) as the management of acute SCI is complex.
-
Begin resuscitation as needed using the ABCDE approach.
- Respiratory support for SCI
- BP management for SCI
- If an unstable spinal injury is suspected, apply spinal motion restrictions until definitive treatment can be performed.
- Insert a urinary catheter early. [5][7]
- Provide acute pain management. [5]
- Admit to a neurocritical care unit or ICU.
- Expedite surgical management of SCI, if indicated.
- Consider only with expert consultation: 24-hour infusion of high-dose methylprednisolone within 8 hours of injury (controversial). [5][9][14]
Patients with SCI may experience recurrent transient life-threatening cardiovascular and respiratory instability during the first 7–10 days after injury. [15]

Respiratory support for SCI [7][15][16]
- All patients: Monitor for impending respiratory failure.
-
Initial management of respiratory failure
-
Airway management
- For patients with spinal immobilization, ensure manual in-line cervical stabilization.
- For hypotensive patients, see “Intubation of hemodynamically unstable patients.”
- For patients with concomitant TBI and ↑ ICP, see “Intubation of patients with high ICP.”
- Mechanical ventilation: See “Ventilation strategy for neuromuscular weakness.”
-
Airway management
-
Ongoing management
- Closely monitor mechanical ventilation.
- Consider early tracheostomy and diaphragmatic pacing in patients with a high SCI. [5]
Manage respiratory failure early, especially in patients with cervical and upper thoracic SCIs as they have a high risk of acute and delayed respiratory complications. [7][15][16]
Blood pressure management for SCI [17]
- Avoid hypotension (sBP < 90 mm Hg): Promptly treat hemorrhagic shock and/or neurogenic shock. [5][17]
- Monitor hemodynamic parameters.
- Consider maintaining a MAP of 75–90 mm Hg for 3–7 days after injury. [5][12][17]
- Begin immediate treatment for acute BP elevations: See “Autonomic dysreflexia.” [18]
Exclude hemorrhagic shock and/or obstructive shock in patients who have persistent hypotension after traumatic SCI. [19]
Surgical management of SCI [5][11]
- Procedure: surgical spinal cord decompression and spine stabilization
- Timing: ideally performed within 24 hours of injury (if the patient is hemodynamically stable) [11]
-
Indications [20]
- Spinal cord compression with progressive neurological deficit following blunt trauma
- Spinal cord compression by bone fragments or foreign bodies due to penetrating trauma
- Anterior cord syndrome
- Unstable spinal injury
Early closed reduction may be considered for cervical fracture-dislocations. [21]
Supportive care [5]
Neurological symptom management
- Serial neurological examinations: to assess for neurological deterioration or improvement. [7]
-
Neurogenic bladder: to prevent permanent bladder injury [5]
- Early: Use an indwelling urine catheter to guide fluid therapy and measure urine output.
- Late (after hemodynamic stabilization): Switch to intermittent catheterization.
-
Neurogenic bowel: Ensure regular bowel movements with complete emptying of the rectal vault. [5]
- Scheduled laxatives, stool softeners, and/or enemas
- Digital rectal stimulation
- Colostomy or ileostomy in severe cases
Other supportive care in the ICU
- VTE prophylaxis: Initiate within 72 hours (in consultation with neurosurgery). [5][9]
- Physical therapy: Initiate as soon as the patient is hemodynamically stable. [22]
- Prevention of decubitus ulcers
- Specialized nutrition support
- Pain management in critically ill patients
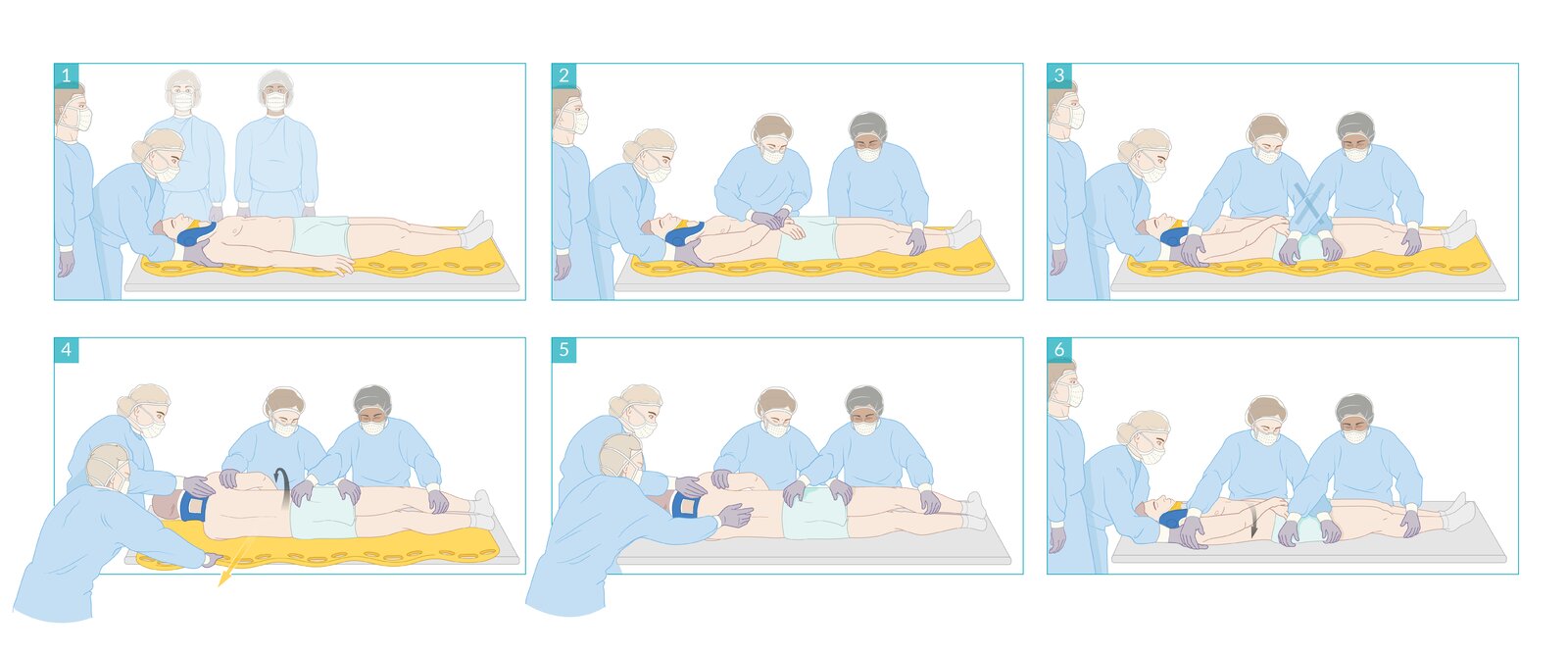
A maneuver used to reposition patients between the supine and lateral decubitus positions while maintaining spinal immobilization. Helpful for posterior body examination, preventing aspiration during emesis, and for transfers (e.g., off stretchers). Requires synchronized movement of multiple trained health providers.
(1) One provider maintains manual in-line cervical stabilization of the patient's head and neck.
(2) Other providers position the patient's limbs securely by crossing their arms over the torso and approximating the legs.
(3) Two providers support the patient's weight evenly by crossing their arms over the patient's pelvis as shown.
(4) In synchrony, all three providers roll the patient into the decubitus position while maintaining full spinal alignment.
(5) The position is maintained by all three providers until the examination and/or intervention is complete.
(6) In synchrony, all three providers roll the patient back into the supine position while maintaining full spinal alignment.
© AMBOSS
Spinal cord injury without radiographic abnormality (SCIWORA)
- Definition: SCI without signs of vertebral fracture or dislocation on x-ray or CT
-
Epidemiology
- More common in children than adults
- Most common in male individuals (∼ 70% of cases) [24]
- Location: 90% of cases occur in the cervical spine. [24]
- Pathophysiology: ligamentous and capsular laxity (common in children) → hyperextension or hyperflexion injury with spontaneous reduction → damage to the spinal cord without damage to the spinal column
-
Clinical features
- Clinical features of SCI (complete SCIs, incomplete SCIs)
- Can manifest immediately or develop over several days
-
Diagnosis: See “Diagnosis of spinal cord injuries.”
- X-rays and CT of the spine do not show evidence of acute spinal column injuries.
- MRI of the spine is typically indicated, but findings are normal in up to 40% of cases. [8]
-
Management
- Usually managed conservatively with external cervical immobilization
- Surgical stabilization may be indicated for persistent ligamentous instability.
- See also “Treatment of spinal cord injury.”
-
Prognosis
- Most patients with incomplete SCI achieve significant neurological recovery.
- Improvement after complete SCI is rare.
Complications
Acute phase [25]
- Neurogenic shock
- Hemodynamic shock
- Sinus bradycardia
Chronic phase [25]
- Autonomic dysreflexia
- Neurogenic bladder
- Bowel dysfunction
- Spasticity
- Coronary artery disease
- Deep vein thrombosis
- Orthostatic hypotension
- Pneumonia
- Major depressive disorder (MDD)
- Central neuropathic pain
We list the most important complications. The selection is not exhaustive.
Autonomic dysreflexia
Autonomic dysreflexia is a medical emergency. Remain vigilant for acute blood pressure elevations in patients with SCI above T6. [18]
Definition
- A cardiovascular complication of SCI characterized by an imbalanced autonomic reflex response
- Causes sudden onset excessively high blood pressure, headache, and diaphoresis
Etiology
- Autonomic dysreflexia develops in individuals with SCIs above the level of T6 in response to stimuli affecting the body below the level of injury. [26]
-
Precipitating stimuli
-
Visceral
- Bladder (e.g., distended bladder, UTI)
- Intestinal (e.g., constipation, bowel obstruction)
- Genital (e.g., childbirth, sexual intercourse)
- Cutaneous; (e.g., pressure ulcer, skin infection, traumatic injury)
- Other: e.g., vasopressors, pain, scrotal compression, contact with hard or sharp objects [18][27]
-
Visceral
Individuals with SCIs at T6 or above are at the highest risk for autonomic dysreflexia.
Individuals with autonomic dysreflexia are predisposed to episodes of life-threatening autonomic dysfunction.
Pathophysiology [26]
- Development of predisposition: damage to descending spinal cord fibers → loss of modulating signaling from the brain → uninhibited spinal cord reflexes → excessive sympathetic reflex response to stimuli below the level of the lesion → life-threatening overactivation of the sympathetic and parasympathetic autonomic nervous systems
- Development of a hypertensive emergency
- Precipitating stimulus below the level of the spinal cord lesion → uninhibited sympathetic activation → diffuse vasoconstriction and tachycardia → hypertension
- Compensatory parasympathetic activation (by carotid sinus baroreceptor) → vasodilation in the area above the level of the lesion → bradycardia, heart block, and hypertensive emergency
Clinical features [5][18][27][28]
-
Sudden elevation of blood pressure above baseline
- Adults: > 20 mm Hg elevation
- Children: > 15 mm Hg elevation
- Rhythm abnormalities, e.g., bradycardia, tachycardia, SV block, arrhythmias
- Headache
- Nasal congestion
- Piloerection, flushing, and diaphoresis above the level of injury
- Vasoconstriction below the level of injury
- Other: anxiety, blurred vision, nausea
Low baseline blood pressure is common in patients with SCI and can mask acute blood pressure elevations. [18]
Management [18][27]
- Acute treatment typically involves:
- Management of reversible triggers
- BP-lowering medication as needed
- Trigger avoidance is the cornerstone of prevention.
- Consult a specialist for a comprehensive prevention plan.
Trigger management
See “Etiology” for potential triggers.
-
Urinary retention
- Acute: Insert a urinary catheter or address indwelling catheter obstruction.
- Treat urinary retention long-term (e.g., with intermittent bladder catheterization).
- Prevent catheter-associated UTIs.
-
Constipation
- Acute fecal impaction: Perform manual disimpaction.
- Optimize treatment of constipation (e.g., scheduled stool softeners).
-
Skin, extremities, and external organs
- Include log-roll and pelvic examination in clinical evaluation.
- Protect the skin: prevention of decubitus ulcers, treatment of decubitus ulcers.
Identify and address urinary retention and fecal impaction, as they are the most common triggers of autonomic dysreflexia. [18]
Blood pressure management
- Position the patient upright, lower the legs, and loosen clothing and constrictive devices. .
- Monitor BP at 2–5-minute intervals until autonomic dysreflexia resolves.
- If systolic blood pressure remains ≥ 150 mm Hg: Start a short-acting antihypertensive.
- Nitroglycerin ointment (off-label) : preferred [18][27]
- Nifedipine immediate release (off-label) [18][27]
- Hydralazine (off-label) [18][27]
- Clonidine immediate release (off-label) [18][27]
- Captopril immediate release (off-label) [18][27]
- Monitor for hypotension and recurrent autonomic dysreflexia for at least 2 hours.
- Consider home blood pressure monitoring.
To avoid worsening hypertension, use lidocaine jelly and consider short-acting antihypertensives before any rectal or urethral manipulation in patients with systolic blood pressure ≥ 150 mm Hg. [18]
Disposition
- Persistent or recurrent blood pressure elevations: Admit to the hospital.
- Autonomic dysreflexia resolved: Discharge with return precautions and a home blood pressure monitoring device
Complications [5][28]
- Myocardial ischemia
- Cardiac arrest
- Intracerebral hemorrhage
- Seizures
Myocardial ischemia may be asymptomatic. Consider an ECG and troponin levels in patients with severe or difficult to control autonomic dysreflexia. [27]
External Resources
- 2024 AO Spine/Praxis Clinical practice guidelines for the management of acute spinal cord injury
- 2021 American Spinal Injury Association: Evaluation and Management of Autonomic Dysreflexia and Other Autonomic Dysfunctions
- 2020 World Federation of Neurosurgical Societies Recommendations for rehabilitation of spinal cord injury
References
- Rupp R, Biering-Sørensen F, Burns SP, et al. "International Standards for Neurological Classification of Spinal Cord Injury". Top Spinal Cord Inj Rehabil. 27(2). :1-22. (2021)
- Krassioukov A, Linsenmeyer TA, Beck LA, et al. "Evaluation and Management of Autonomic Dysreflexia and Other Autonomic Dysfunctions: Preventing the Highs and Lows". Top Spinal Cord Inj Rehabil. 27(2). :225-290. (2021)
- Bycroft J. "Autonomic dysreflexia: a medical emergency". Postgrad Med J. 81(954). :232-235. (2005)
- Krassioukov A, Stillman M, Beck LA. "A Primary Care Provider’s Guide to Autonomic Dysfunction Following Spinal Cord Injury". Top Spinal Cord Inj Rehabil. 26(2). :123-127. (2020)
- Wan D, Krassioukov AV. "Life-threatening outcomes associated with autonomic dysreflexia: a clinical review.". J Spinal Cord Med. 37(1). :2-10. (2014)
- "American College of Surgeons, American Congress of Rehabilitation Medicine, Best practices guidelines: Spine injury". https://www.facs.org/media/k45gikqv/spine_injury_guidelines.pdf. [2022-03-01]
- McAllister AS, Nagaraj U, Radhakrishnan R. "Emergent Imaging of Pediatric Cervical Spine Trauma". RadioGraphics. 39(4). :1126-1142. (2019)
- Atesok K, Tanaka N, O’Brien A, et al. "Posttraumatic Spinal Cord Injury without Radiographic Abnormality". Adv Orthop. 2018. :1-10. (2018)
- "ACS TQIP Best Practices in Imaging Guidelines 2018". https://www.facs.org/media/oxdjw5zj/imaging_guidelines.pdf. [2018-10-01]
- Tetreault LA, Kwon BK, Evaniew N, et al. "A Clinical Practice Guideline on the Timing of Surgical Decompression and Hemodynamic Management of Acute Spinal Cord Injury and the Prevention, Diagnosis, and Management of Intraoperative Spinal Cord Injury 2024". Global Spine J. 14(3_suppl). :10S-24S. (2024)
- Walters BC, Hadley MN, Hurlbert RJ, et al. "Guidelines for the Management of Acute Cervical Spine and Spinal Cord Injuries". Neurosurgery. 60(CN_suppl_1). :82-91. (2013)
- Sánchez JAS, Sharif S, Costa F, et al. "Early Management of Spinal Cord Injury: WFNS Spine Committee Recommendations". Neurospine. 17(4). :759-784. (2020)
- Consortium for Spinal Cord Medicine.. "Early acute management in adults with spinal cord injury: A clinical practice guideline for health-care professionals.". J Spinal Cord Med. 31(4). :403-79. (2008)
- Hurlbert RJ, Hadley MN, Walters BC, et al. "Pharmacological Therapy for Acute Spinal Cord Injury". Neurosurgery. 72(supplement 2). :93-105. (2013)
- Fehlings MG, Tetreault LA, Wilson JR, et al. "A Clinical Practice Guideline for the Management of Acute Spinal Cord Injury: Introduction, Rationale, and Scope.". Global Spine J.. 7(3 Suppl). :84S-94S. (2017)
- Ryken TC, Hurlbert RJ, Hadley MN, et al. "The Acute Cardiopulmonary Management of Patients With Cervical Spinal Cord Injuries". Neurosurgery. 72(supplement 2). :84-92. (2013)
- Berlly M, Shem K. "Respiratory Management During the First Five Days After Spinal Cord Injury". J Spinal Cord Med. 30(4). :309-318. (2007)
- Kwon BK, Tetreault LA, Martin AR, et al. "A Clinical Practice Guideline for the Management of Patients With Acute Spinal Cord Injury: Recommendations on Hemodynamic Management". Global Spine J. 14(3_suppl). :187S-211S. (2024)
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904
- Rath N, Balain B. "Spinal cord injury—The role of surgical treatment for neurological improvement". J Clin Orthop Trauma. 8(2). :99-102. (2017)
- Gelb DE, Hadley MN, Aarabi B, et al. "Initial Closed Reduction of Cervical Spinal Fracture-Dislocation Injuries". Neurosurgery. 72(supplement 2). :73-83. (2013)
- Fehlings MG, Tetreault LA, Aarabi B, et al. "A Clinical Practice Guideline for the Management of Patients With Acute Spinal Cord Injury: Recommendations on the Type and Timing of Rehabilitation". Global Spine J. 7(3_suppl). :231S-238S. (2017)
- J Spinal Cord Med. "Spinal Cord Injury (SCI) 2016 Facts and Figures at a Glance.". J Spinal Cord Med. 39(4). :493-4. (2016)
- Alcanyis-Alberola M, Giner-Pascual M, Salinas-Huertas S, Gutiérrez-Delgado M. "Iatrogenic spinal cord injury: an observational study". Spinal Cord. 49(12). :1188-1192. (2011)
- Müller-Jensen L, Ploner CJ, Kroneberg D, Schmidt WU. "Clinical Presentation and Causes of Non-traumatic Spinal Cord Injury: An Observational Study in Emergency Patients". Frontiers in Neurology. 12. (2021)
- Ditunno JF, Little JW, Tessler A, Burns AS. "Spinal shock revisited: a four-phase model". Spinal Cord. 42(7). :383-395. (2004)
- Beckmann NM, West OC, Nunez D, et al. "ACR Appropriateness Criteria® Suspected Spine Trauma". J Am Coll Radiol. 16(5). :S264-S285. (2019)
- Wang TY, Park C, Zhang H, et al. "Management of Acute Traumatic Spinal Cord Injury: A Review of the Literature". Frontiers in Surgery. 8. (2021)
- Vaidyanathan S, Soni BM, Sett P, et al. "Pathophysiology of autonomic dysreflexia: long-term treatment with terazosin in adult and paediatric spinal cord injury patients manifesting recurrent dysreflexic episodes.". Spinal cord. 36(11). :761-70. (1998)
- Eltorai I, Kim R, Vulpe M, Kasravi H, Ho W. "Fatal cerebral hemorrhage due to autonomic dysreflexia in a tetraplegic patient: case report and review". Paraplegia. 30(5). :355-360. (1992)