Summary
Subdural hematoma (SDH) refers to bleeding into the intracranial subdural space that is typically caused by a rupture of the bridging veins. Trauma, including minor falls, cerebral atrophy, and conditions that increase the risk of bleeding (e.g., coagulopathy, hypertension) are common etiologies of SDH. According to the onset of symptoms, SDH can be classified into acute SDH, subacute SDH, and chronic SDH. Acutely symptomatic SDH typically manifests with altered mental status, focal neurological signs, and signs of increased ICP, and it can progress to brain herniation and death if not treated. Chronic SDH manifests gradually with cognitive deficits, impaired memory, personality changes, and focal neurological signs. Subacute SDH can manifest with features of acute and/or chronic SDH. In patients with acutely symptomatic SDH, neuroprotective measures to prevent secondary brain injury take precedence over diagnostics. Diagnosis is confirmed with a noncontrast head CT, which would show a crescent-shaped (concave) lesion that may cross cranial sutures typically located in the supratentorial region. Surgery is recommended in SDH that is symptomatic, ≥ 10 mm in size, or causing ≥ 5 mm shift in the midline. Conservative management can be considered for small asymptomatic SDHs in patients with no signs of increased ICP.
Definitions
Subdural hematoma refers to a hemorrhage into the intracranial subdural space, which lies between the dura mater and the arachnoid mater. [1]
Classification
Depending on the length of time between the onset of symptoms and the inciting event, SDH can be classified into the following: [2][3]
- Acute SDH: symptom onset within 3 days of the inciting event
- Subacute SDH: symptom onset 4–20 days after the inciting event
- Chronic SDH: symptom onset ≥ 21 days after the inciting event
Epidemiology
-
Incidence
- Nontraumatic acute SDH: unknown [4]
- Traumatic acute SDH: seen in approx. 30% of patients with severe traumatic brain injury (TBI) [5][6]
- Chronic SDH: 2–13 individuals per 100,000 population [4]
- Sex: ♂ > ♀ (3:1) [2][7]
-
Age
- SDH is common in infants and toddlers. [2][8]
- Acute SDH: more common in younger adults (30–50 years of age) [3]
- Chronic SDH: more common in the elderly, especially individuals older than 70 years of age [3]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
SDH is caused by a rupture of the bridging veins, which can occur secondary to any of the following factors.
Acute SDH [3]
- Most common cause: blunt head trauma (high-energy impact due to motor vehicle accidents) [9]
- Nonaccidental trauma, e.g., shaken baby syndrome
- Acceleration-deceleration injury [10]
Chronic SDH [3][8]
Traumatic chronic SDH
- In adults: mild trauma secondary to falls (e.g., due to old age, alcohol use disorder, epilepsy, hyponatremia)
-
In infants [11]
- Nonaccidental trauma, e.g., shaken baby syndrome
- Birth trauma
Nontraumatic chronic SDH
-
In adults: cerebral atrophy ; [12]
- Advanced age
- Alcohol use disorder [13]
-
Neurodegenerative disease, such as:
- Alzheimer disease
- Dementia (including HIV dementia, vascular dementia)
- Chronic diabetes mellitus [14][15]
- Previous traumatic brain injury
- Cerebral irradiation [16]
- In infants and young children: meningitis [11]
-
In both
- Increased risk of hemorrhage due to:
- Antithrombotic therapy or coagulopathy [4]
- Intracranial aneurysm
- Intracranial arteriovenous malformation
- Intracranial tumors
- Hypertension
- Arteriosclerosis
- Hemodialysis [17]
- Iatrogenic (e.g., after neurosurgical procedures)
- Spontaneous intracranial hypotension (rare) [18]
- Increased risk of hemorrhage due to:
SDH may occur after trivial trauma in patients with multiple risk factors.
Individuals at extremes of age (i.e., infants and the elderly) are at an increased risk of developing nontraumatic chronic SDH.
Pathophysiology
- Rupture of bridging veins → low-pressure venous bleeding into the subdural space → SDH

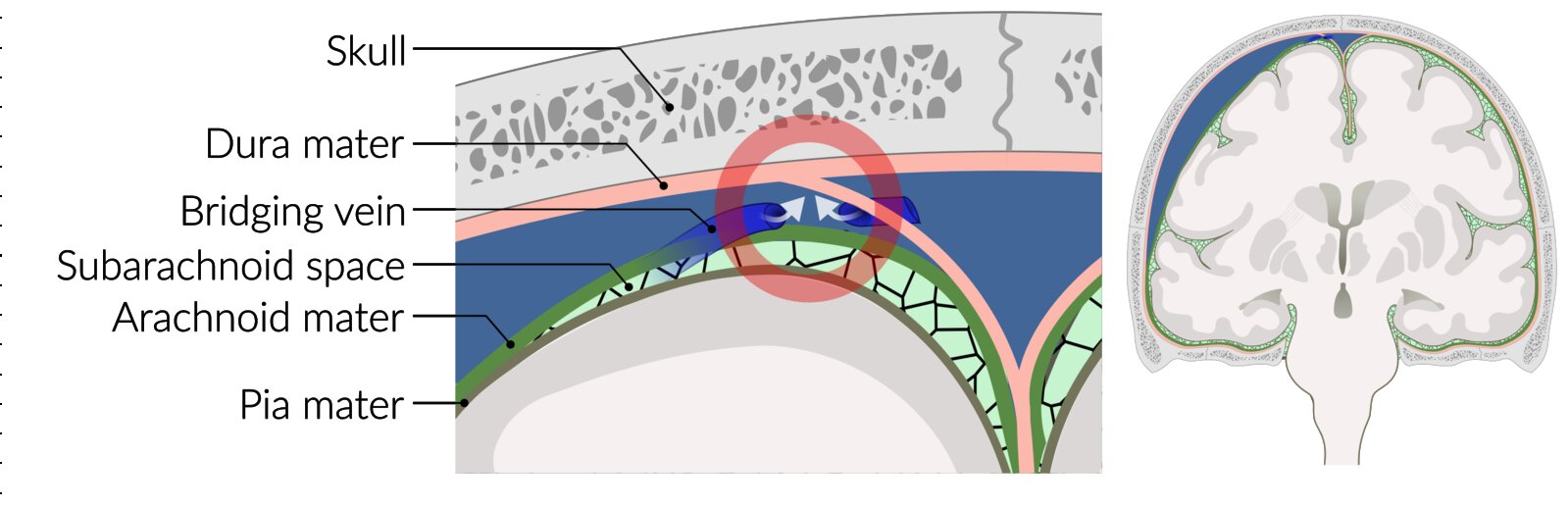
Rupture of a bridging vein results in hemorrhage into the subdural space between the dura and arachnoid mater. Bleeding into the subdural space results in a crescent-shaped hematoma (right) that can cross suture lines but not the midline.
© AMBOSS
Clinical features
Clinical features depend on the size and location of the hematoma and the length of time since the inciting event. In infants and young children unable to articulate symptoms, the presentation can be nonspecific (see abusive head trauma).
Acute SDH [2][3][9]
-
Symptom onset
- Typically immediately after (or within 3 days of) the inciting event [19]
- A lucid interval between head injury and onset of neurological symptoms is present in 12–40% of patients. [9]
-
Progression
- Rapid
- Can progress to cerebral herniation and death
-
Clinical features
- Impaired consciousness and confusion, rapidly deteriorating to coma [2]
-
Focal neurological signs, such as:
- Contralateral hemiparesis and UMN signs
- Ipsilateral hemiparesis due to Kernohan syndrome (false localizing sign; uncommon)
-
Cranial nerve palsies, manifesting as:
- Diplopia
- Blurred vision
- Unequal pupils
- Anosmia
- Slurred and/or disorganized speech
- Pupillary abnormalities (e.g., anisocoria, unilateral or bilateral fixed dilated pupils)
-
Manifestations of ↑ ICP, such as:
- Headache
- Vomiting
- Cushing triad
- Signs of cerebral herniation syndromes
- Abnormal posturing (e.g., decorticate posturing, decerebrate posturing)
- Seizures
- See ''Clinical features of traumatic brain injury'' for more information.
Traumatic acute SDH and acute EDH have similar clinical manifestations and are indistinguishable without neuroimaging.
Subacute SDH [20]
-
Symptom onset
- 4–20 days after the inciting event
- Can be acute or insidious
- Progression: A rebleed can cause rapid neurological decline.
- Clinical features: a combination of features of acute SDH and chronic SDH
Chronic SDH [3][21]
-
Symptom onset
- Insidious
- ≥ 3 weeks after the inciting event
- Progression: typically gradual
-
Clinical features
-
Altered mental state that can progress to coma, characterized by:
- Confusion
- Delirium
- Excessive drowsiness
- Recurrent headaches
-
Cognitive deficits
- Impaired memory
- Dementia [22]
-
Focal neurological signs
- Contralateral hemiparesis (most common) that can progress to hemiplegia
- Incontinence
- Ataxia and recurrent falls
- Changes in personality [23]
- Seizures (rare)
-
Altered mental state that can progress to coma, characterized by:
Diagnosis
Important considerations [5][6]
- Immediate initiation of neuroprotective measures takes precedence over diagnostics in patients with acutely symptomatic SDH.
- Traumatic acute SDH: Follow trauma protocols, i.e., primary survey in TBI.
- Diagnostics should not delay the transfer of a patient to a neurocritical care unit if needed.
Laboratory studies
- Traumatic SDH: See ''Diagnostics'' in “TBI” for routine laboratory studies that should be obtained in all patients with TBI.
- Nontraumatic SDH: Workup for the underlying cause (See “Etiology”)
Neuroimaging [24][25]
In trauma patients, findings of other injuries often accompany SDH, e.g., skull fractures, cerebral edema, and other types of TBI
CT head without IV contrast
- Indication: first-line imaging modality for suspected acute SDH
-
Characteristic findings [24]
- Crescent-shaped, concave, sharply demarcated extraaxial lesion
- Can cross cranial suture lines
- Does not cross the midline
- A large unilateral SDH can cause midline shift to the contralateral side; midline shift may be absent or less significant in bilateral SDH. [26]
-
Radiodensity of the lesion depends on the length of time since the inciting event.
- Acute SDH: hyperdense
- Subacute SDH: isodense [27]
- Chronic SDH: hypodense
- Acute-on-chronic SDH: hyperdense areas (recent hemorrhage) admixed with isodense or hypodense areas (older hematoma) [4][28]
- Common locations
- Supratentorial location (most common)
- Posterior cranial fossa
- Interhemispheric [24][29]
- Radiographic signs of other concurrent TBIs can be present, e.g., EDH with SDH.










MRI head [24][25]
-
Indications
- Neurological features unexplained by CT findings [2]
- Suspected subacute SDH or chronic SDH [24][25]
- Evaluation for nontraumatic etiologies (e.g., AVM, dural metastases) [29][30]
-
Characteristic findings [24][29]
- Similar to those on CT scan
- Intensity of the lesion on T2-weighting depends on the length of time since the inciting event.
- Acute SDH: hypointense [29]
- Subacute SDH: hyperintense [28][29]
- Chronic SDH: hyperintense core with a hypointense rim [29]





")
Angiography [2][24]
- Indication: to determine the etiology of a nontraumatic SDH (e.g., ruptured aneurysm, vascular meningeal tumor, AVM)
-
Modalities
- CTA
- MR angiography
- DSA
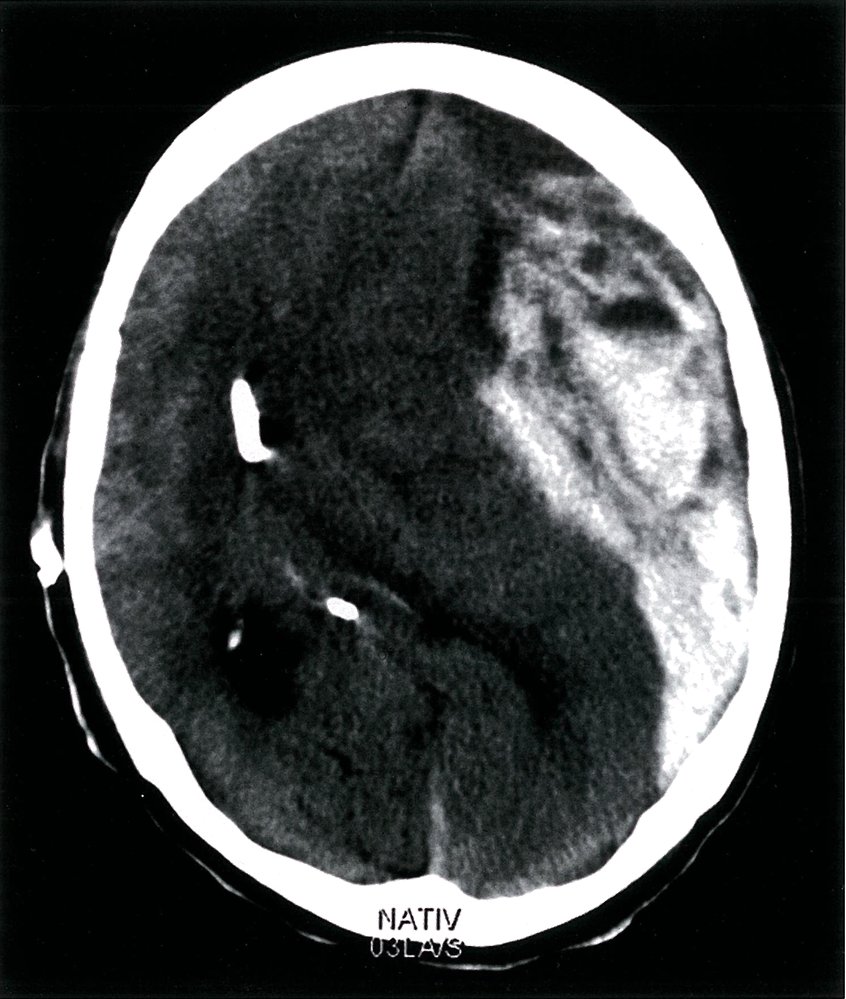
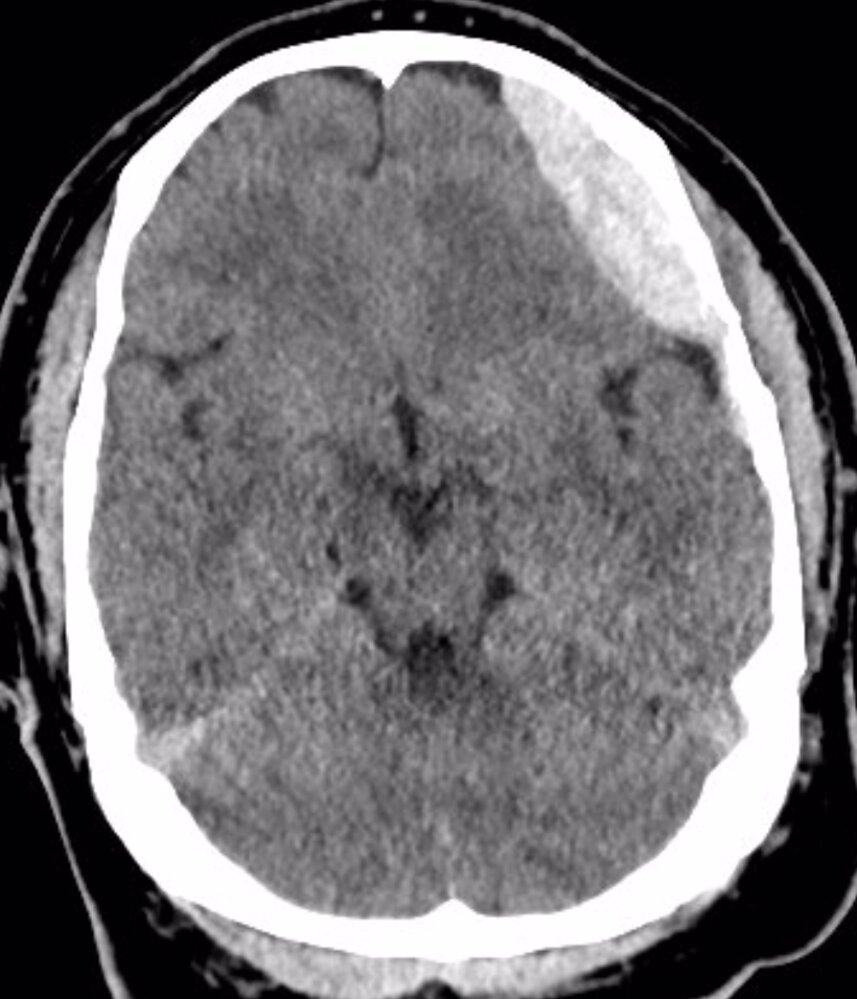
CT head (without IV contrast; axial section; brain window) of a patient with a history of trauma
A large acute subdural hematoma is visible as a hyperdense crescent-shaped lesion along the lateral aspect of the left hemisphere (red overlay). It is accompanied by an extracranial soft tissue hematoma (hatched red overlay). There is extensive hypodense left cerebral edema (gray overlay), with sulcal effacement and shift of midline structures (green line) to the right. The anterior horns of the lateral ventricles (hatched green overlay) are compressed and the posterior horn of the right lateral ventricle (red circle) is dilated.
Source: © IMPP
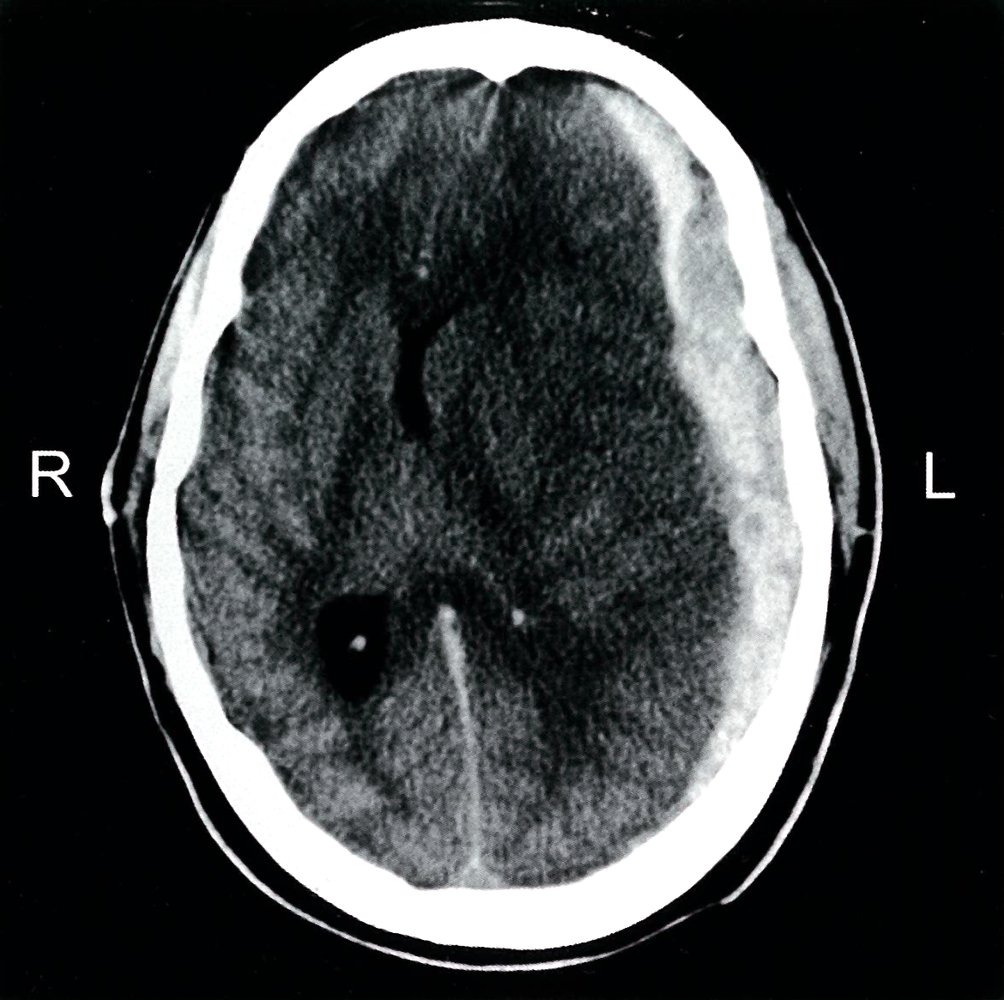
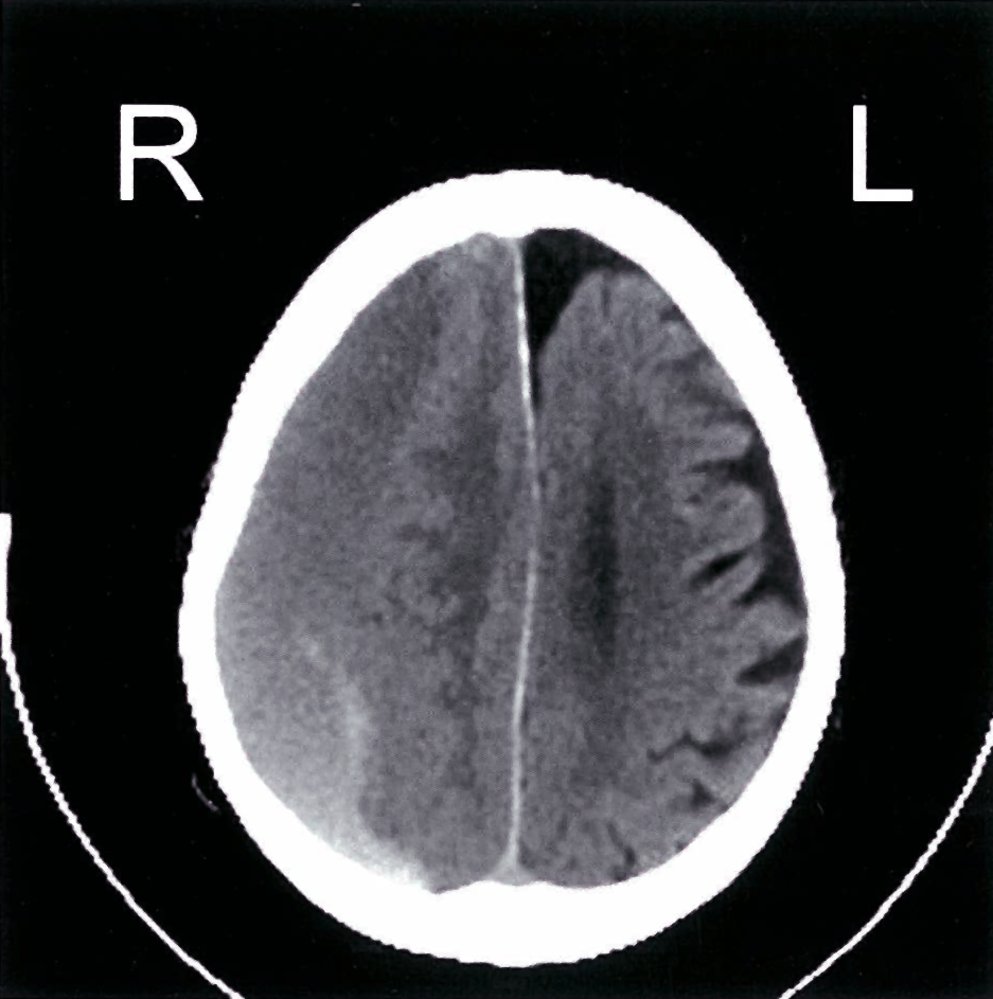
CT head (without IV contrast; axial section; brain window)
There is a crescent-shaped, hyperdense lesion (green overlay) over the left cerebral hemisphere that crosses cranial sutures. There is a midline shift to the right (dotted line and arrows).
These findings are characteristic of an acute subdural hematoma.
Source: © IMPP

Click on the overlay icon below the taskbar on the left to toggle the overlay on and off.
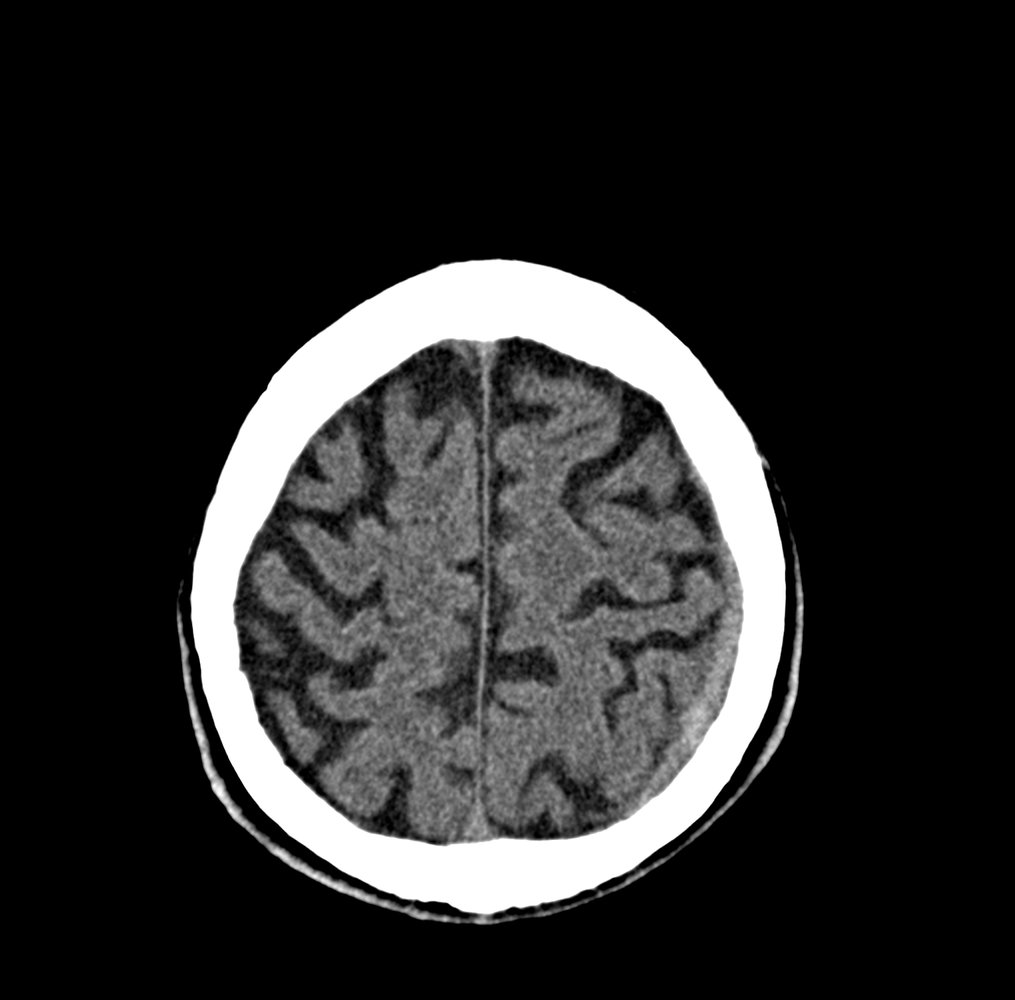
CT head (without contrast; axial plane)
The hyperdense, crescent-shaped, extra-axial collection (green overlay) visible along the left frontal convexity is compatible with an acute subdural hematoma.
Additional findings of dilated ventricles and sulci indicate generalized cerebral atrophy. The periventricular hyperlucencies are consistent with cerebral small vessel disease.
Original title: “Subdurales Hämatom”. Created by: Dr. med. Kerstin Bohse. Organization providing image: Clinic Pfeiffersche Stiftungen. Further notes: Our great thanks to Dr. med. Kerstin Bohse (Clinic Pfeiffersche Stiftungen) for kindly providing this case.
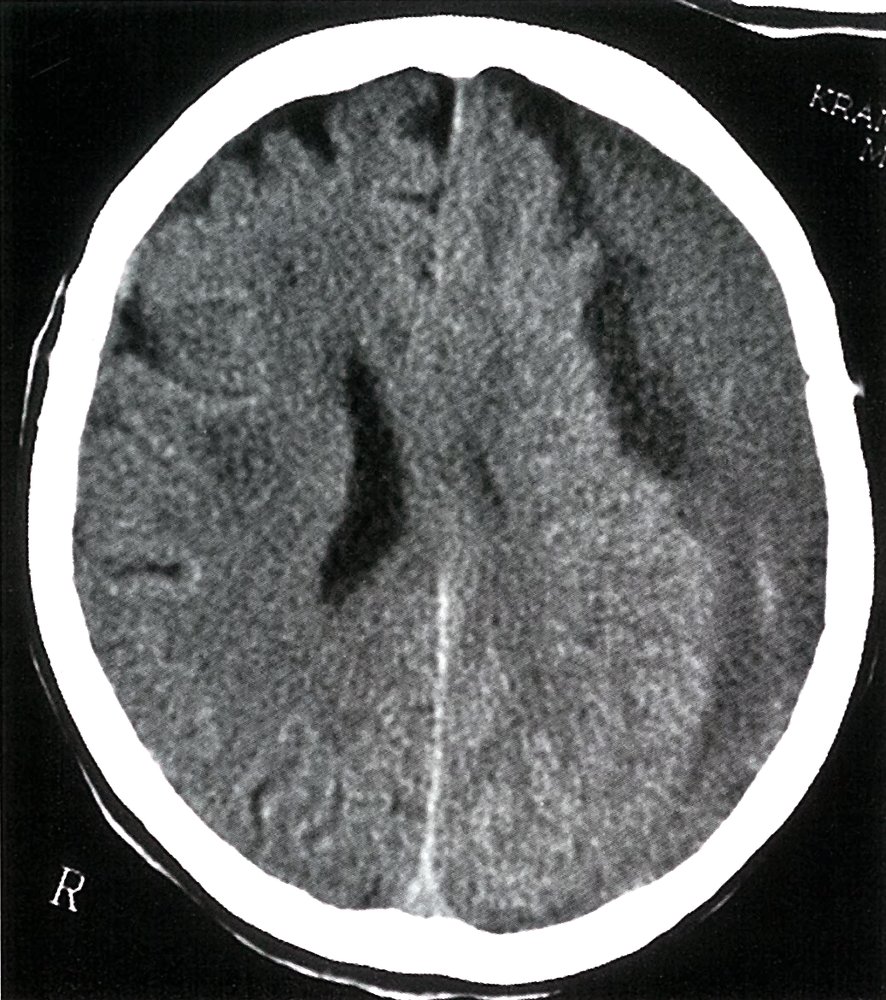
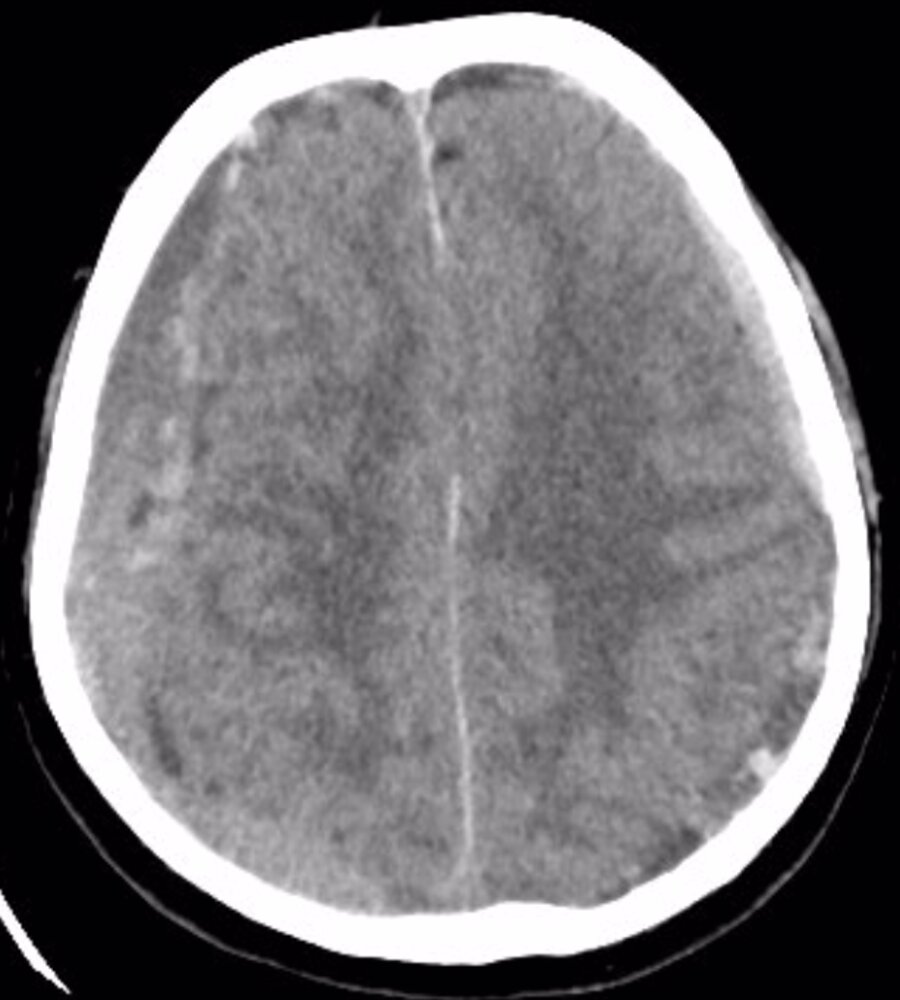
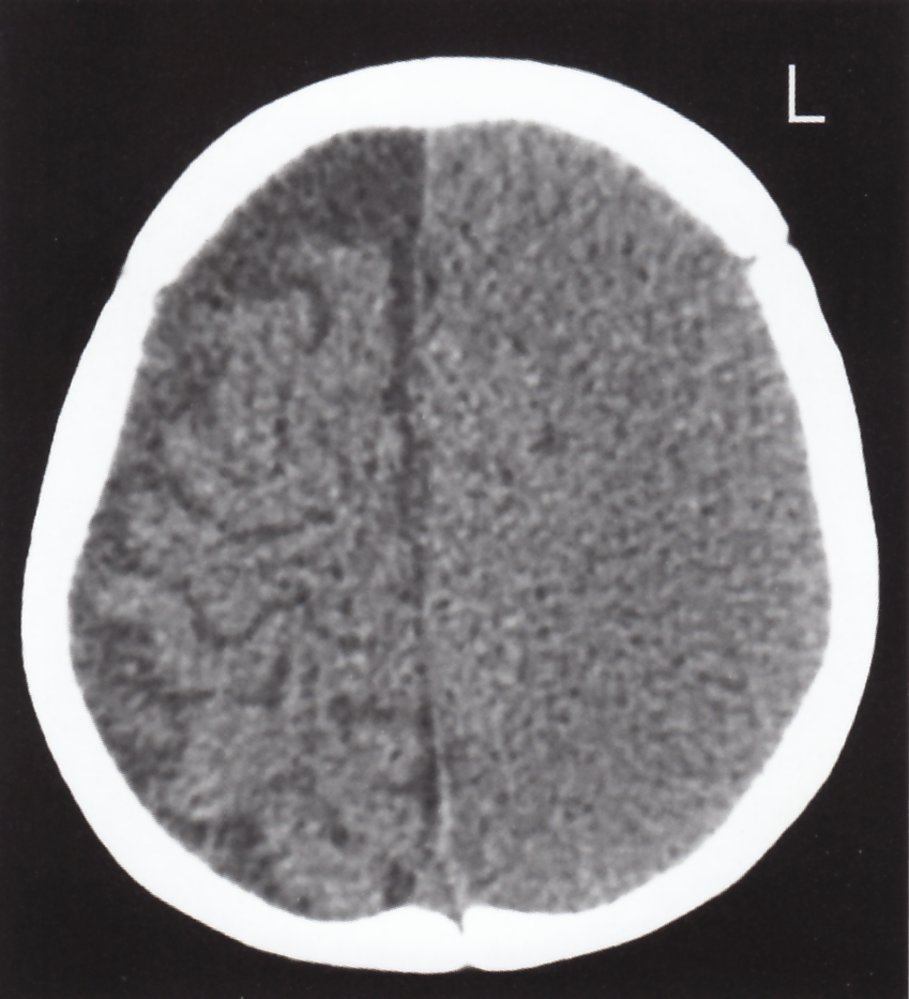
CT head (without IV contrast; axial section; brain window)
There is a large, crescent-shaped, hypodense lesion (green overlay) over the lateral aspect of the left hemisphere that crosses cranial sutures. Mass effect of the lesion is visible as compression of the left lateral ventricle.
These findings are characteristic of a large chronic subdural hematoma.
Source: © IMPP
CT head (without IV contrast; axial section; brain window)
A crescent-shaped, heterogeneous lesion that crosses cranial sutures is visible on the anterolateral aspect of the right hemisphere. The anterior aspect of the lesion is hypodense (green overlay), indicating a chronic hematoma (serum extrusion and degradation of the clot decreases its radiodensity). The posterior aspect of the lesion is isodense to hyperdense (red overlay), indicating a more recent hematoma (recent blood clots contain concentrated hemoglobin, which appears hyperdense). In addition, the parenchyma adjacent to the lesion is compressed and edematous as visualized by the loss of sulci and gyri. There is a shift in the midline to the left (green line and arrow).
These features are characteristic of a large acute-on-chronic subdural hematoma.
Source: © IMPP

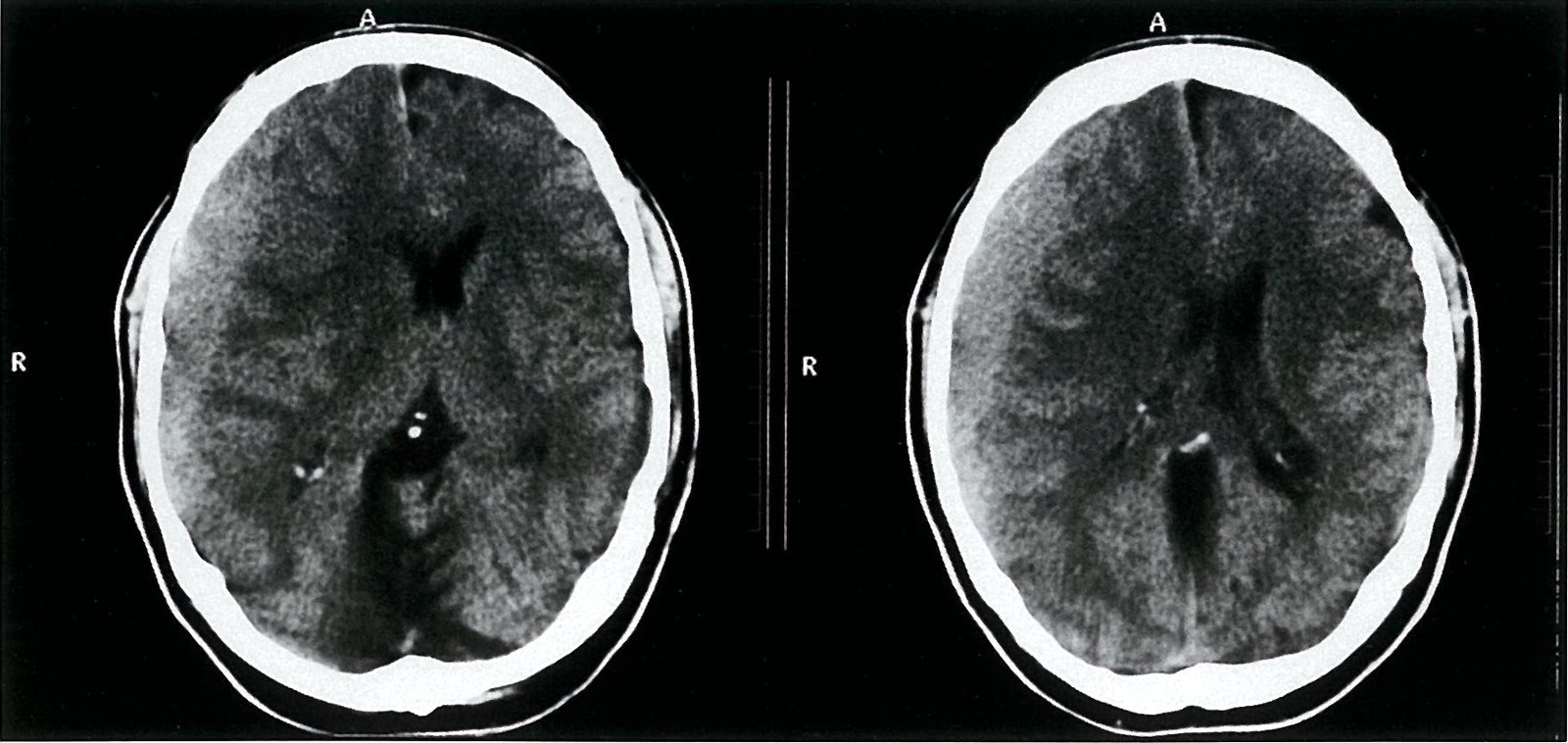
CT head (without IV contrast; axial section; brain window)
A crescent-shaped, heterogeneous lesion that crosses cranial sutures is visible on the anterolateral aspect of the right hemisphere. The anterior aspect of the lesion is hypodense (green overlay) indicating a chronic hematoma (serum extrusion and degradation of the clot decreases its radiodensity). The posterior aspect of the lesion is isodense to hyperdense (red overlay), indicating a recent hemorrhage into the existing hematoma (recent blood clots contain concentrated hemoglobin, which is hyperdense). Mass effect is visualized as a shift in the midline (white line) to the left (dashed white line), compression of the left lateral ventricle, and compression of the adjacent cerebral parenchyma, which appears edematous (hyperdense with loss of the sulci and gyri).
These features are characteristic of an acute-on-chronic subdural hematoma.
Our great thanks to PD Dr. M. Jergas (Center for Diagnostic and Interventional Radiology, St. Elizabeth Hospital, Cologne) for kindly providing this image.
Click on the overlay icon below the taskbar on the left to toggle the overlay on and off.
CT head (brain window: axial and coronal planes; bone window: axial plane)
A biconvex epidural hematoma (green overlay) with mass effect is seen in the left frontal region, adjacent to which is a small frontotemporal subdural hematoma (red overlay). A calvarial fracture (arrowheads) involves the left temporal and parietal bones.
Created by: Nándor Faluhelyi. Organization providing image: University of Pécs, Medical School. Further notes: Our great thanks to Nándor Faluhelyi (University of Pécs, Medical School) for kindly providing this case.
CT head (without contrast; axial and coronal planes) of a patient with history of head trauma, factor V Leiden mutation, and anticoagulation therapy
Bilateral collections, right larger than left, each have a crescentic shape typical of subdural hematoma. Mass effect has resulted in right ventricular effacement and shift of midline structures to the left (series 303, 42/66; series 304, 34/70). The collections are heterogeneous due to a mixture of old (hypodense) and recent (hyperdense) hemorrhage.
Our great thanks to Nandor Faluhelyi M.D., Ph.D. (University of Pécs, Medical School) for kindly providing this image.
CT head (without contrast; axial plane; brain window)
A hyperdense, crescent-shaped extra-axial collection (green overlay) on the right side is accompanied by a contralateral shift of the midline structures.
The appearance is characteristic of an acute subdural hematoma.
White dashed line and arrow: midline; arrowhead: right lateral ventricle
Source: © IMPP
CT head (without IV contrast; axial section; brain window)
An acute subdural hematoma is visible as a hyperdense, crescent-shaped lesion on the posterolateral aspect of the left cerebral hemisphere (green overlay).
Our great thanks to PD Dr. M. Jergas (Center for Diagnostic and Interventional Radiology, St. Elizabeth Hospital, Cologne) for kindly providing this image.
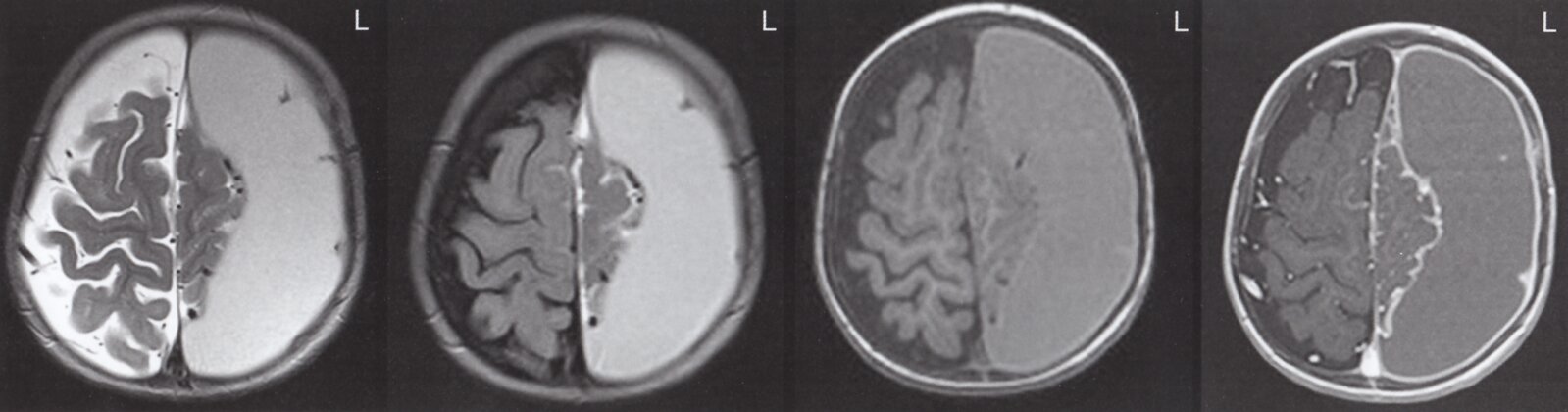
MRI head (axial plane; left to right: T2-weighted without contrast, T2 FLAIR without contrast, T1-weighted without contrast, T1-weighted with contrast) of infant one week after traumatic brain injury
An extracerebral crescent-shaped fluid collection (yellow overlay) is hyperintense on the T2-weighted sequence without contrast and produces mass effect on the left cerebral hemisphere with mild midline shift to the right side (indicated by dashed line and arrowheads). It is not restricted by cranial sutures and does not cross the midline, consistent with a subdural collection. The collection is hyperintense to CSF on the T2 FLAIR sequence and hyperintense to gray matter on the T1-weighted sequence without contrast, suggesting a subacute subdural hematoma. Meningeal enhancement is seen on the T1-weighted sequence with contrast (blue overlay).
Source: © IMPP
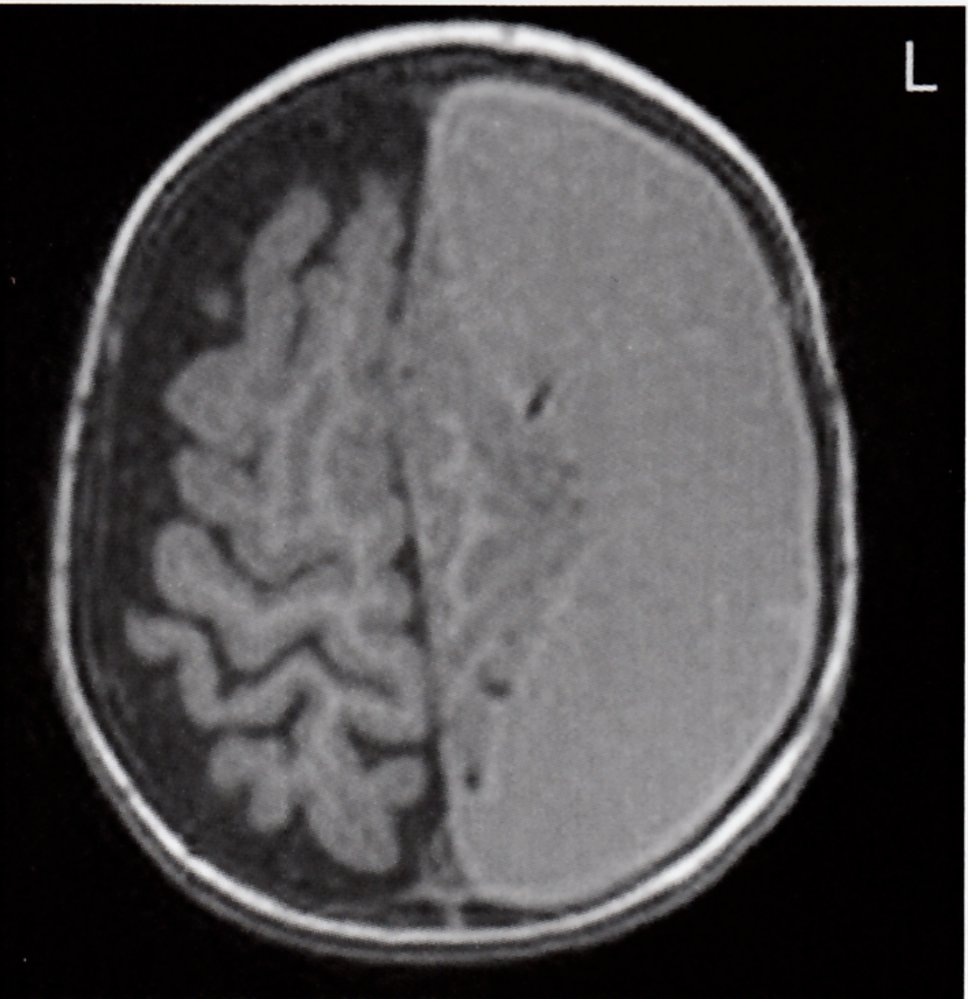
MRI head of an 11-month-old infant (T1-weighted; axial section)
Left hemicranium: A crescent-shaped lesion (green overlay) is visible over the left hemisphere. The lesion crosses cranial sutures but does not cross the midline, which are pathognomonic features of a subdural hematoma (SDH). The lesion appears isodense to hypointense in relation to the brain parenchyma, indicating that it is likely an early subacute SDH. There is a shift in the midline to the right (white line and arrows).
Right hemicranium: A subdural collection (white overlay and arrowheads) isointense in relation to CSF is visible in the right frontal region, suggesting a subdural hygroma.
Source: © IMPP
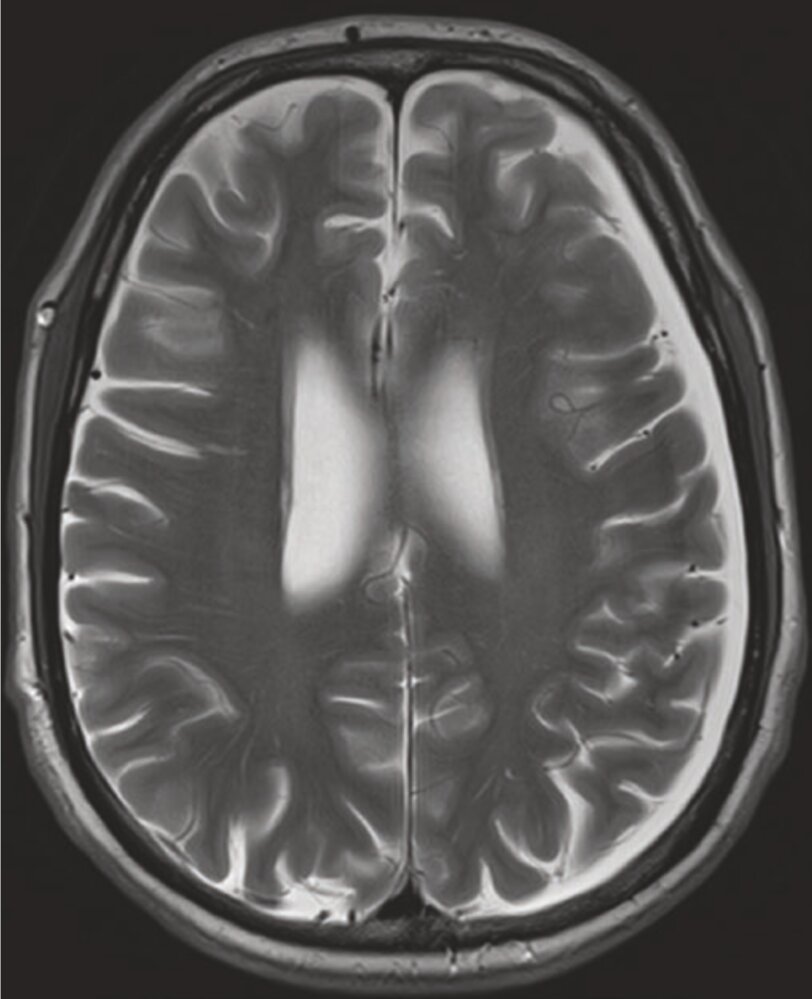
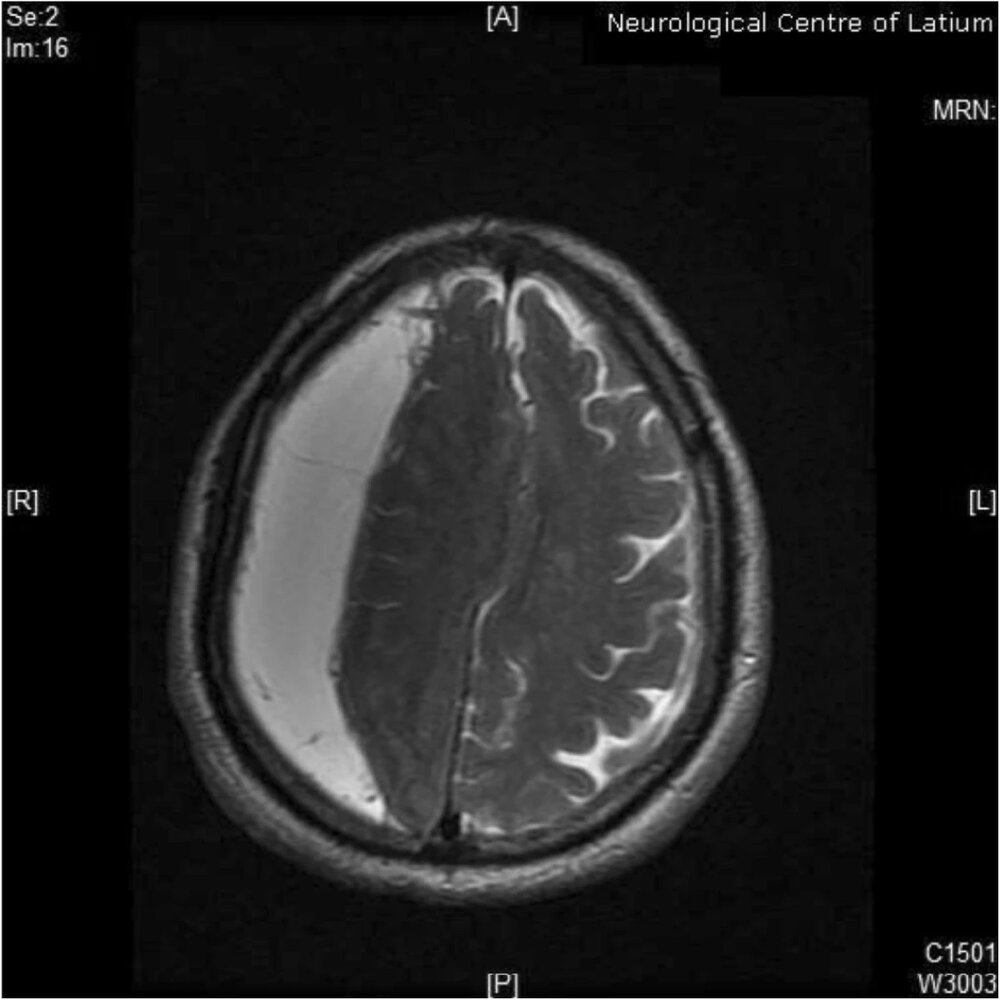
MRI head (T2-weighted; axial plane)
A hyperintense, crescent-shaped, space-occupying collection (green overlay) along the left hemisphere is isointense to CSF. On a FLAIR sequence (not shown), the collection was hyperintense to CSF.
A stable chronic subdural hematoma typically appears isointense to CSF on T1 and T2 sequences and hyperintense to CSF on a FLAIR sequence. If there is rebleeding or infection, the collection may appear hyperintense to CSF on T1 and hypointense to CSF on T2.
LV: lateral ventricle
Source: “Fig. 7.8, in: Diseases of the Brain, Head and Neck, Spine 2020–2023: Diagnostic Imaging” by Parizel PM, Philips CD, Springer, licensed under CC BY 4.0. Modifications: Image was cropped, letter "a" was removed.. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
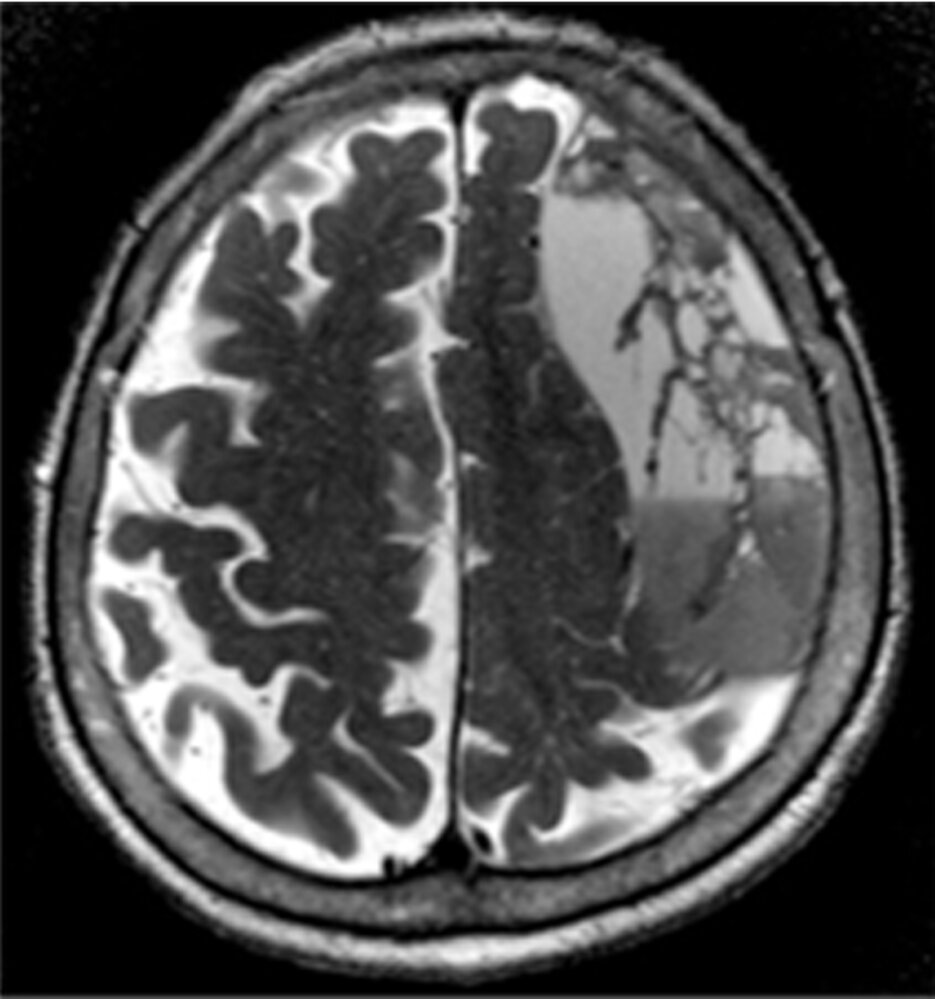
MRI head (T2 weighted; axial plane) of an 86-year-old patient with word-finding difficulties and generalized weakness after two falls (at 2 months at 1 month before presentation).
A large space-occupying lesion with heterogeneous signal intensity can be seen in the left high frontal region, shifting the midline to the contralateral side (red lines and arrow).
In the context of the patient's two falls, these findings are consistent with a chronic subdural hematoma (hypointense parts of the lesion; green overlay) with additional subacute hemorrhage (hyperintense parts of the lesion; red overlay).
Source: “Fig. 1 D, in: Use of Subdural Evacuating Port System Following Open Craniotomy with Excision of Native Dura and Membranes for Management of Chronic Subdural Hematoma” by Cage T, Bach A, Mcdermott M, Cureus, licensed under CC BY 3.0. Modifications: Image was cropped, letter "D" was removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
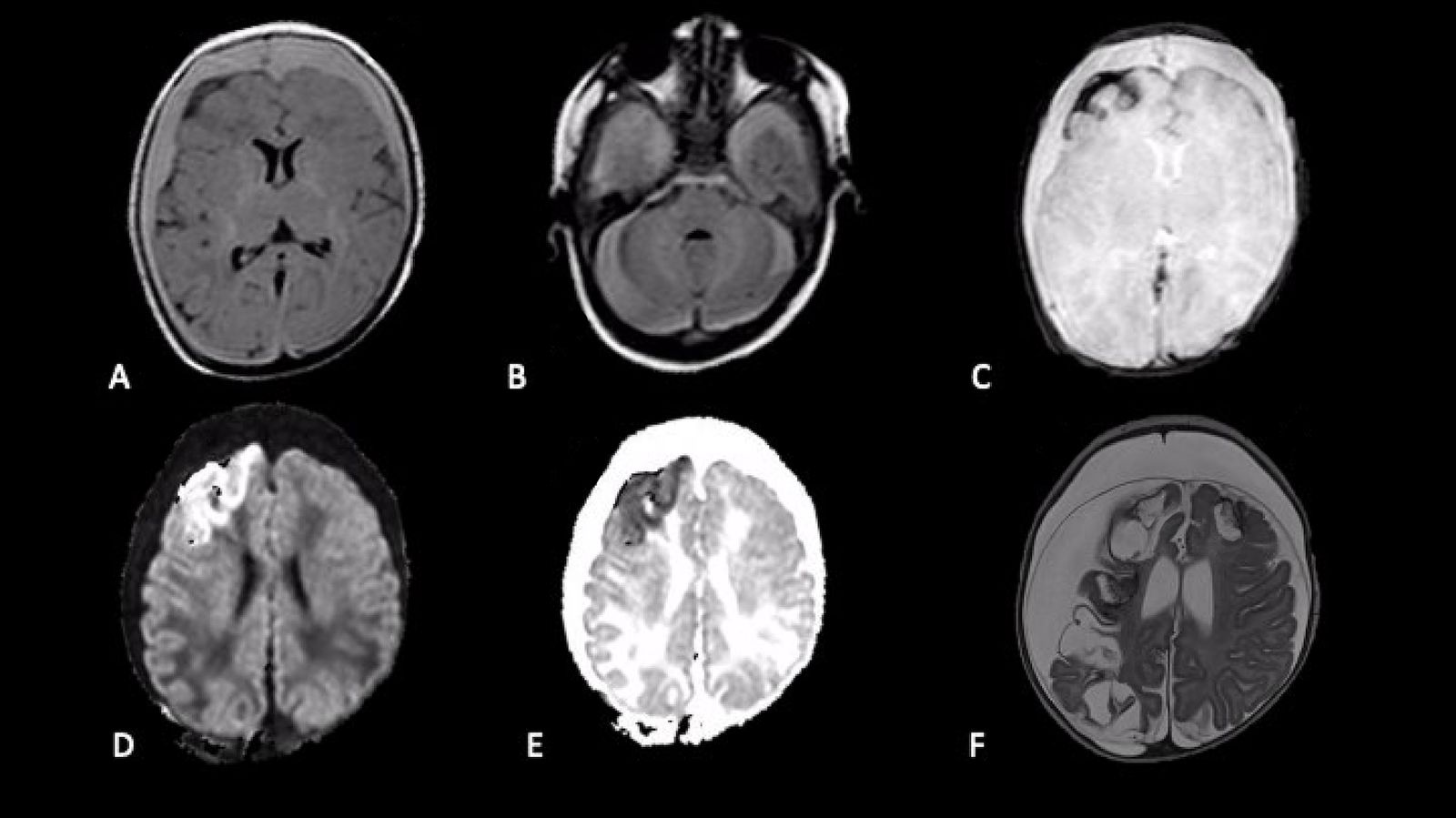
MRI head (axial plane) of a newborn who presented with with generalized seizures, fever, and vomiting
A and B: FLAIR
Crescentic supratentorial (A) and infratentorial (B) subdural hematomas (arrows) are slightly hyperintense to parenchyma.
C: Susceptibility-weighted imaging (SWI)
Hypointense subarachnoid hemorrhage (arrow) extends into right frontal lobe sulci.
D: Diffusion-weighted imaging (DWI) and E: apparent diffusion coefficient (ACD) map
Right frontal lobe cortical-subcortical hemorrhage appears hyperintense on DWI and hypointense on the ACD map (arrows).
F: T2-weighted (one-month follow-up) Bilateral cresentic subdural hygromas (arrows) and areas of encephalomalacia (examples indicated by arrowheads) are isointense to CSF. Mass effect from the hygromas causes compression of brain parenchyma and a thin membrane (blue overlay) is visible.
Source: “Figure 2, in: Shaken Baby Syndrome: Magnetic Resonance Imaging Features in Abusive Head Trauma” by Cartocci, Gaia, Vittorio Fineschi, Martina Padovano, Matteo Scopetti, Maria C. Rossi-Espagnet, and Costanza Giannì, Brain Sciences, licensed under CC BY 4.0. Modifications: - removed white rim - arrows and asterixes removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Differential diagnoses
- Other intracranial hemorrhages: See “Differential diagnosis of intracranial hemorrhage.”
- In addition, chronic SDH should be differentiated from:
-
Subdural hygroma [31]
- Collection of CSF in the subdural space
- Thought to be caused by a tear in the arachnoid membrane following head injury
- Difficult to distinguish from a chronic SDH on CT scan
- Surgical evacuation is recommended in symptomatic subdural hygroma.
- Other causes of dementia (e.g., neurodegenerative diseases, ischemic stroke)
-
Subdural hygroma [31]
")
EDH is typically caused by arterial bleeding into the epidural space; SDH is typically caused by venous bleeding into the subdural space.
On neuroimaging, an EDH is biconvex (lentiform), does not cross cranial sutures, but can cross the midline; an SDH is concave, can cross cranial sutures but does not cross the midline.
The differential diagnoses listed here are not exhaustive.
CT head of an 11-month-old infant (without IV contrast; axial section; brain window)
Right hemicranium: A hypodense collection (white overlay and arrowheads) is visible in the right frontal region, suggesting a subdural hygroma.
Left hemicranium: A crescent-shaped lesion (green overlay) is visible overlying the left cerebral hemisphere. The lesion crosses cranial sutures but does not cross the midline, which are pathognomonic features of a subdural hematoma (SDH). The lesion is isodense in relation to the brain parenchyma, indicating a subacute SDH (better visualized on an MRI; see image 2/2 of this series). There is a shift in the midline to the right (white line and arrows).
Source: © IMPP
MRI head of an 11-month-old infant (T1-weighted; axial section)
Left hemicranium: A crescent-shaped lesion (green overlay) is visible over the left hemisphere. The lesion crosses cranial sutures but does not cross the midline, which are pathognomonic features of a subdural hematoma (SDH). The lesion appears isodense to hypointense in relation to the brain parenchyma, indicating that it is likely an early subacute SDH. There is a shift in the midline to the right (white line and arrows).
Right hemicranium: A subdural collection (white overlay and arrowheads) isointense in relation to CSF is visible in the right frontal region, suggesting a subdural hygroma.
Source: © IMPP
Treatment
Approach
Specific treatment of SDH depends on the size of the hematoma, neurological status of the patient at presentation, and etiology (traumatic or nontraumatic). For patients with acute traumatic SDH, see also “Management approach for TBI”.
-
Symptomatic SDH (acute, subacute, or chronic)
- Immediate neurosurgery consult and/or transfer to a neurocritical care unit if expertise is not available on site
- Medical management
- Neuroprotective measures
- Empiric ICP management if there are signs of ↑ ICP
- See also “Initial management of TBI.”
- Surgical management: Hematoma evacuation (see “Neurosurgical interventions”)
- Emergency temporizing measure: If there is rapid neurological decline (e.g., cerebral herniation syndrome) and surgery is delayed, consider immediate burr hole craniotomy, e.g., prior to interfacility transfer. [32][33]
- Asymptomatic SDH (acute, subacute, or chronic): urgent neurosurgery consult to determine surgical vs. conservative management and disposition.
-
All patients
-
Supportive care, monitoring, and prevention of complications in brain injuries
- Frequent neurological examinations
- Prevention of secondary bleeding or hematoma expansion, e.g., discontinuing antithrombotics, anticoagulant reversal, possible platelet transfusion
- Prevention of other complications as needed, e.g., VTE, seizures, CNS infections
- Treatment of reversible underlying causes for spontaneous SDH (e.g., management of coagulopathy, hypertension, diabetes mellitus)
- For patients with traumatic SDH see also “Management of trauma patients,” and “TBI.”
-
Supportive care, monitoring, and prevention of complications in brain injuries
Neurosurgical interventions [4][9][26]
-
Indications [1][26]
- Hematoma size ≥ 10 mm
- Midline shift ≥ 5 mm
- Signs of cerebral herniation syndromes (e.g., extensor posturing, anisocoria)
- Rapid neurological deterioration (e.g., ≥ 2-point decrease in GCS score from the time of injury or symptom onset to ER transfer) [9]
- Unilateral or bilateral fixed dilated pupils
- ICP > 20 mm Hg [9]
- Failure of conservative management [26]
- Additional indications in chronic SDH include: [4]
- Change in baseline neurological status
- Evidence of mass effect
- Increasing size of hematoma
-
Timing
- Acute SDH: preferably within ≤ 4 hours of the inciting event [9][19]
- Subacute SDH or chronic SDH: as soon as possible [34]
-
Options
- Signs of cerebral herniation syndromes: emergency craniotomy or decompressive craniectomy; consider emergency temporizing burr hole craniotomy if definitive neurosurgical management is delayed (e.g., requires interfacility transfer) [19][35]
-
Acute SDH [9][19][26]
- Craniotomy with evacuation of hematoma
- Decompressive craniectomy
-
Subacute SDH and chronic SDH [26][34][36]
- Definitive surgery: Craniotomy and clot evacuation (with/without drain placement) [21][37]
- Elderly or high surgical risk: Consider minimally invasive or bedside interventions, e.g., twist drill craniostomy. [38]
An SDH ≥ 10 mm in size or causing ≥ 5 mm midline shift should be surgically removed, even if the patient is asymptomatic. [1]
Conservative management
-
Indications (all of the following): [1][26][39]
- Asymptomatic
- Hematoma < 10 mm in size
- Midline shift < 5 mm
- Normal pupillary reflex and no signs of ↑ ICP, regardless of the GCS score
-
Acute SDH [1][26]
- Admit to neurocritical care unit.
- Neuroprotective measures
- ICP monitoring
- Serial neurological examinations [19]
- Serial neuroimaging
- Neuroimaging should be repeated within the first 36 hours or earlier if there is neurological deterioration. [1]
- Subsequent neuroimaging may be repeated as needed. [40]
- Urgent surgery in patients with neurological deterioration and/or evidence of hematoma expansion on neuroimaging [19]
-
Subacute SDH or chronic SDH
- Disposition depends on the size and location of the hematoma and neurological examination findings. [4]
- Corticosteroids may have a role in aiding spontaneous regression of the hematoma. [34][41]
- Surgery may be required for patients who become symptomatic. [34]
All conservatively managed patients should also receive supportive care, monitoring, secondary prevention measures for complications, and treatment of reversible underlying conditions.
Acute management checklist for acute traumatic SDH
General TBI management approach
See also “Acute management checklist for moderate or severe TBI.”
- Follow ABCDE approach to evaluate, prioritize, and manage other injuries (e.g., C-spine precautions, fluid resuscitation).
- Perform rapid focused neurological examination (e.g., GCS, pupillary exam, screening for lateralizing signs).
- Intubate for airway protection if necessary (e.g., low GCS): See “Intubation of patients with high ICP.”
- Stabilize and obtain immediate neuroimaging.
- Urgent neurosurgery consult: for operative intervention and to determine disposition
- Neurosurgery available on-site: Transfer to operating room, or admit directly to neurocritical care unit.
- Neurosurgery not available on-site
- Urgent interfacility transfer to a neurocritical care unit.
- If signs of cerebral herniation syndrome, consider skull trephination prior to transfer.
- Neurosurgery not indicated: conservative management only
Concurrent medical management
- Initiate neuroprotective measures (See “Acute management checklist for neuroprotective measures.”)
- ICP management if signs of ↑ ICP
- Prevention of secondary bleeding and hematoma expansion: See “Prevention of complications in brain injuries.”
- Administer tranexamic acid if GCS is 9–13 and < 3 hours have elapsed since TBI.
- Hold antithrombotic agents.
- Anticoagulant reversal as needed.
- Consider platelet transfusion if platelet count < 100,000/mm3 [42]
- Serial neurological examination (e.g., GCS, pupillary examination)
- Continuous monitoring of vitals, pulse oximetry, and capnography
Prognosis
- Acute SDH has a higher likelihood of an underlying parenchymal injury and is therefore associated with a worse prognosis than acute EDH. [29][43]
- The prognosis of chronic SDH is better than that of acute SDH, however chronic SDH is associated with higher mortality with increasing age. [44]
Pre- XC clinician content for treatment section; has some postponed content that may be useful in the #future.
Initial management
- Acute traumatic SDH: see Management approach for TBI and Moderate and severe TBI treatment
- Acute atraumatic SDH and chronic SDH
- Protect the airway (see Airway management)
- Treat any associated coagulopathy
- Reverse anticoagulation (see Anticoagulant Reversal) [45]
- Stop any further doses of anticoagulants and anti-platelet agents
-
Platelet transfusion is recommended if platelets are < 100 and surgery is planned [46][47]
- If on antiplatelet therapy: the decision to transfuse platelets should be individually based on factors such as severity, size and location of bleed, and point of care tests [47]
- Start general neuroprotective measures and ICP management
Ongoing management
- All patients require a neurosurgical consult
- In patients with a small SDH (hematoma is < 10 mm, midline shift < 5 mm) and no change to neurological status conservative management may be appropriate
- In all other patients, neurosurgical evacuation is required
Surgical management [9][26]
- Indicated for both acute and chronic patients if:
- Hematoma is > 10 mm
- Midline shift > 5 mm
- There are signs of herniation e.g., extensor posturing
- Additional indications in acute SDH include:
- Rapidly deteriorating neurological examination (> 2 point decrease in GCS) with GCS < 8
- Fixed and dilated pupils (either unilateral or bilateral)
- ICP > 20 mmHg
- Additional indications in chronic SDH include:
- GCS is affected
- Neurological deficits are present
Surgical management in acute SDH
- Should occur within ≤ 4 hours of injury [19]
- The aim is to evacuate the hematoma and relieve raised intracranial pressure
- Surgical options include: [19][26][48]
- Decompressive craniectomy
- Cranioplastic craniotomy
-
Trephination
- In acute SDH with impending herniation, can be used as a temporizing measure [19][35]
- Needs to be followed by either decompressive craniectomy or cranioplastic craniotomy [19][35]
Surgical management in subacute and chronic SDH
- Surgical technique depends on whether patients are high anesthetic risk and whether neomembranes have formed or not [26][49][50][51]
- No neomembranes or patient at high anesthetic risk: twist drill craniostomy +/- subdural evacuating port system (SEPS) [26]
- Neomembranes
- Burr hole evacuation/Trephination [26]
- Craniotomy evacuation (large or mini, with or without assisted endoscopy)
Conservative management
- Some patients with both acute and chronic subdural hematomas may be suitable for conservative management
- In both cases there is no clear guidance on when anticoagulation and antiplatelet agents should be restarted; consult with neurosurgical service on when to restart [1]
Conservative management of acute SDH
- Can be considered for patients with small acute subdural hematomas if: [1]
- There is no pupillary abnormality
- No intracranial hypertension in patients with GCS < 9
- The hematoma is < 10 mm with midline shift < 5 mm
- Patients should be monitored in the ICU
- ICP should be monitored if GCS < 9 [1]
- CT head should be repeated within the first 36 hours (sooner if there is neurological deterioration) [1]
- Surgery should occur within < 2 hours of deterioration [19]
Conservative management of chronic and subacute SDH
- Indicated if the patient is: [26]
- Asymptomatic
- No clinical signs of herniation
- Hematoma is < 10 mm with midline shift < 5 mm
- Patients should have close monitoring of their neurological status
- Patients require serial CT scans [40]
Related One-Minute Telegram
- One-Minute Telegram 77-2023-1/3: The drill still fits the bill for chronic SDH
Interested in the newest medical research, distilled down to just one minute? Sign up for the One-Minute Telegram in “Tips and links” below.
External Resources
References
- Gerard C, Busl KM. "Treatment of Acute Subdural Hematoma". Curr Treat Options Neurol. 16(1). (2013)
- Katz DI, MD DI, Zafonte RD, et al. "Brain Injury Medicine". Demos Medical Publishing. (2006). ISBN: 9781934559505
- Bullock MR, Chesnut R, Ghajar J, et al. "Guidelines for the Surgical Management of Traumatic Brain Injury Author Group". Neurosurgery. 58(3). :S2-vi-S2-vi. (2006)
- Mckee AC, Daneshvar DH. "The neuropathology of traumatic brain injury.". Handbook of clinical neurology. 127. :45-66. (2015)
- Jayawant S, Parr J. "Outcome following subdural haemorrhages in infancy". Arch Dis Child. 92(4). :343-347. (2007)
- Kemp AM. "Investigating subdural haemorrhage in infants". Arch Dis Child. 86(2). :98-102. (2002)
- Yang AI, Balser DS, Mikheev A, et al. "Cerebral atrophy is associated with development of chronic subdural haematoma.". Brain injury. 26(13-14). :1731-6. (2012)
- Watson RR, Zibadi S. "Addictive Substances and Neurological Disease". Academic Press. (2017). ISBN: 9780128053737
- Wang I-K, Chen H-J, Cheng Y-K, et al. "Subdural hematoma in diabetic patients". European Journal of Neurology. 22(1). :99-105. (2014)
- Moran C, Beare R, Wang W, Callisaya M, Srikanth V. "Type 2 diabetes mellitus, brain atrophy, and cognitive decline". Neurology. 92(8). :e823-e830. (2019)
- Aminoff MJ, Josephson SA. "Aminoff's Neurology and General Medicine". Academic Press. (2014). ISBN: 9780124077102
- Ferri FF. "Ferri's Clinical Advisor 2017". Elsevier Health Sciences. (2016). ISBN: 9780323448383
- Power A, Hamady M, Singh S, et al. "High but stable incidence of subdural haematoma in haemodialysis--a single-centre study". Nephrol Dial Transplant. 25(7). :2272-2275. (2010)
- Zhang J, Jin D, Pan K-H. "Epidural blood patch for spontaneous intracranial hypotension with chronic subdural haematoma: A case report and literature review". J Int Med Res. 44(4). :976-981. (2016)
- Fomchenko EI, Gilmore EJ, Matouk CC, Gerrard JL, Sheth KN. "Management of Subdural Hematomas: Part I. Medical Management of Subdural Hematomas". Curr Treat Options Neurol. 20(8). (2018)
- Karibe H, Hayashi T, Hirano T, et al. "Surgical management of traumatic acute subdural hematoma in adults: a review.". Neurol Med Chir (Tokyo). 54(11). :887-94. (2014)
- Tripathy SR, Swarnakar PK, Mishra S, et al. "A review of sub acute subdural hematoma (SASDH) with our institutional experience and its management by double barrel technique (DbT): A novel technique.". Surgical neurology international. 7(Suppl 28). :S767-S774. (2016)
- Adhiyaman V. "Chronic subdural haematoma in the elderly". Postgrad Med J. 78(916). :71-75. (2002)
- Sahyouni R, Goshtasbi K, Mahmoodi A, Tran DK, Chen JW. "Chronic Subdural Hematoma: A Perspective on Subdural Membranes and Dementia.". World neurosurgery. 108. :954-958. (2017)
- Alvarez-Pinzon AM, Valerio JE, Barkley KA, Swedberg HN, Wolf AL. "A case report and technical tip of chronic subdural hematoma treated by the placement of a subdural peritoneal shunt". Trauma Case Reports. 7. :7-10. (2017)
- American College of Surgeons and the Committee on Trauma. "ATLS Advanced Trauma Life Support". American College of Surgeons. (2018). ISBN: 9780996826235
- Walls R, Hockberger R, Gausche-Hill M. "Rosen's Emergency Medicine". Elsevier Health Sciences. (2018). ISBN: 9780323354790
- Mutch CA, Talbott JF, Gean A. "Imaging Evaluation of Acute Traumatic Brain Injury.". Neurosurg Clin N Am. 27(4). :409-39. (2016)
- Shetty VS, Reis MN, et al. "ACR Appropriateness Criteria Head Trauma". Journal of the American College of Radiology. (2015)
- Fomchenko EI, Gilmore EJ, Matouk CC, Gerrard JL, Sheth KN. "Management of Subdural Hematomas: Part II. Surgical Management of Subdural Hematomas". Curr Treat Options Neurol. 20(8). (2018)
- Wind JJ, Leiphart JW. "Bilateral Subacute Subdural Hematomas". N Engl J Med. 360(17). :e23. (2009)
- Lee S-H, Choi J-I, Lim D-J, et al. "The Potential of Diffusion-Weighted Magnetic Resonance Imaging for Predicting the Outcomes of Chronic Subdural Hematomas". Journal of Korean Neurosurgical Society. 61(1). :97-104. (2018)
- Castillo M. "Neuroradiology". Lippincott Williams & Wilkins. (2002). ISBN: 9780781736640
- Chye CL, Lin KH, Ou CH, et al. "Acute spontaneous subdural hematoma caused by skull metastasis of hepatocellular carcinoma: case report.". BMC Surg. 15. :60. (2015)
- Barro B, Kobner S, Ansari A. "Decompression of Subdural Hematomas Using an Intraosseous Needle in the Emergency Department: A Case Series". Clinical Practice and Cases in Emergency Medicine. 4(3). :312-315. (2020)
- Nelson JA. "Local skull trephination before transfer is associated with favorable outcomes in cerebral herniation from epidural hematoma". Acad Emerg Med. 18(1). :78-85. (2011)
- Shapey J, Glancz LJ, Brennan PM. "Chronic Subdural Haematoma in the Elderly: Is It Time for a New Paradigm in Management?". Current Geriatrics Reports. 5(2). :71-77. (2016)
- Liu X, Qiu Y, Zhang J, et al. "Emergent Single Burr Hole Evacuation for Traumatic Acute Subdural Hematoma with Cerebral Herniation: A Retrospective Cohort Comparison Analysis". World Neurosurg. 120. :e1024-e1030. (2018)
- Sinclair AJ, Morley JE, Vellas B. "Pathy's Principles and Practice of Geriatric Medicine". John Wiley & Sons. (2012). ISBN: 9781119954149
- Sahyouni R, Mahboubi H, Tran P, Roufail JS, Chen JW. "Membranectomy in Chronic Subdural Hematoma: Meta-Analysis.". World neurosurgery. 104. :418-429. (2017)
- Jablawi F, Kweider H, Nikoubashman O, Clusmann H, Schubert GA. "Twist Drill Procedure for Chronic Subdural Hematoma Evacuation: An Analysis of Predictors for Treatment Success.". World neurosurgery. 100. :480-486. (2017)
- Parlato C, Guarracino A, Moraci A. "Spontaneous resolution of chronic subdural hematoma.". Surg Neurol. 53(4). :312-5; discussion 315-7. (2000)
- Dougherty DD, Rauch SL, Rosenbaum JF. "Essentials of Neuroimaging for Clinical Practice". American Psychiatric Pub. (2008). ISBN: 9781585626922
- Henaux PL, Le Reste PJ, Laviolle B, Morandi X. "Steroids in chronic subdural hematomas (SUCRE trial): study protocol for a randomized controlled trial.". Trials. 18(1). :252. (2017)
- Metcalf RA, Nahirniak S, Guyatt G, et al. "Platelet Transfusion". JAMA. (2025)
- Frontera JA, Lewin III JJ, Rabinstein AA, et al. "Guideline for Reversal of Antithrombotics in Intracranial Hemorrhage". Neurocrit Care. 24(1). :6-46. (2015)
- Kaufman RM, Djulbegovic B, Gernsheimer T. "Platelet Transfusion: A Clinical Practice Guideline From the AABB". Ann Intern Med. 162(3). :205-213. (2015)
- Stolla M, Zhang F, Meyer MR, Zhang J, Dong J. "Current state of transfusion in traumatic brain injury and associated coagulopathy". Transfusion (Paris). 59(S2). :1522-1528. (2019)
- Kirollos R, Helmy A, Thomson S, Hutchinson P. "Oxford Textbook of Neurological Surgery". Oxford University Press. (2019). ISBN: 9780191063640
- Klatt EC. "Robbins and Cotran Atlas of Pathology E-Book". Elsevier Health Sciences. (2011). ISBN: 9781455726837
- Small JE, Noujaim DL, Ginat DT, Kelly HR, Schaefer PW. "Neuroradiology". Elsevier Health Sciences. (2018). ISBN: 9780323447256
- Park H-R, Lee K-S, Shim J-J, et al. "Multiple Densities of the Chronic Subdural Hematoma in CT Scans". J Korean Neurosurg Soc. 54(1). :38. (2013)
- F. Servadei. "Prognostic factors in severely head injured adult patients with acute subdural haematoma's". Acta Neurochir (Wien). 139(4). :279-285. (1997)
- Rauhala M, Helén P, Seppä K, et al. "Long-term excess mortality after chronic subdural hematoma". Acta Neurochir (Wien). 162. :1467–1478. (2020)
- Hotta K, Sorimachi T, Honda Y, Matsumae M. "Chronic Subdural Hematoma in Women". World Neurosurg. 105. :47-52. (2017)
- Jr. RPG. "Traumatic Brain Injury". CRC Press. (2007). ISBN: 9780849381393
- Ferri FF. "Ferri's Clinical Advisor 2015 E-Book". Elsevier Health Sciences. (2014). ISBN: 9780323084307
- Dunn LT. "RAISED INTRACRANIAL PRESSURE". J Neurol Neurosurg Psychiatry. 73(suppl 1). :i23-i27. (2002)
- ENA. "Sheehy’s Manual of Emergency Care - E-Book". Elsevier Health Sciences. (2012). ISBN: 9780323171106
- Kahan S, Raves JJ. "In a Page: Surgery". Lippincott Williams & Wilkins. (2004). ISBN: 9781405103657
- Larner AJ, Coles AJ, Scolding NJ, Barker RA. "A-Z of Neurological Practice". Springer Science & Business Media. (2011). ISBN: 9781848829947
- Murphy JG, Lloyd MA. "Mayo Clinic Cardiology Concise Textbook and Mayo Clinic Cardiology Board Review Questions & Answers". CRC Press. (2007). ISBN: 9781420067484
- Zasler N, Katz D, MD D, Zafonte R, DO R. "Brain Injury Medicine". Demos Medical Publishing. (2007). ISBN: 9781888799934
- Grelat M, Madkouri R, Bousquet O. "Acute isodense subdural hematoma on computed tomography scan – diagnostic and therapeutic trap: a case report". J Med Case Reports. 10(1). (2016)
- Ogunlade J, Wiginton JG, Ghanchi H, et al. "Efficacy of platelet transfusion in the management of acute subdural hematoma". Clin Neurol Neurosurg. 174. :163-166. (2018)
- Sarov M, Guichard J-P, Chibarro S, et al. "Sinking Skin Flap Syndrome and Paradoxical Herniation After Hemicraniectomy for Malignant Hemispheric Infarction". Stroke. 41(3). :560-562. (2010)
- Ashayeri K, Jackson EM, Huang J, Brem H, Gordon CR. "Syndrome of the Trephined". Neurosurgery. 79(4). :525-534. (2016)
- Kwon YS, Yang KH, Lee YH. "Craniotomy or Decompressive Craniectomy for Acute Subdural Hematomas: Surgical Selection and Clinical Outcome". Korean J Neurotrauma. 12(1). :22. (2016)
- Kim H, Suh S-J, Kang H-J, et al. "Predictable Values of Decompressive Craniectomy in Patients with Acute Subdural Hematoma: Comparison between Decompressive Craniectomy after Craniotomy Group and Craniotomy Only Group". Korean J Neurotrauma. 14(1). :14. (2018)
- Flint AC, Chan SL, Rao VA, et al. "Treatment of chronic subdural hematomas with subdural evacuating port system placement in the intensive care unit: evolution of practice and comparison with bur hole evacuation in the operating room". J Neurosurg. 127(6). :1443-1448. (2017)
- Baek H-G, Park S-H. "Craniotomy and Membranectomy for Treatment of Organized Chronic Subdural Hematoma". Korean J Neurotrauma. 14(2). :134. (2018)
- Vella MA, Crandall ML, Patel MB. "Acute Management of Traumatic Brain Injury". Surg Clin North Am. 97(5). :1015-1030. (2017)
- Krishnamoorthy V, Chaikittisilpa N, Kiatchai T, Vavilala M. "Hypertension After Severe Traumatic Brain Injury". J Neurosurg Anesthesiol. 29(4). :382-387. (2017)
- Lubin MF, Smith RB, Dodson TF, Spell NO, Walker HK. "Medical Management of the Surgical Patient". Cambridge University Press. (2006). ISBN: 9781139457675
- Yadav Y, Parihar V, Namdev H, Bajaj J. "Chronic subdural hematoma". Asian J Neurosurg. 11(4). :330. (2016)
- Lewis A, Sen R, Hill TC, et al. "Antibiotic prophylaxis for subdural and subgaleal drains.". J Neurosurg. 126(3). :908-912. (2017)
- Louisdon Pierre; Noah P. Kondamudi.. "Subdural Hematoma". StatPearls. (2019)
- Pin-on P, Saringkarinkul A, Punjasawadwong Y, Kacha S, Wilairat D. "Serum electrolyte imbalance and prognostic factors of postoperative death in adult traumatic brain injury patients". Medicine. 97(45). :e13081. (2018)
- Saag MS et al. "The Sanford Guide to Antimicrobial Therapy 2016". Antimicrobial Therapy, Inc. (2016). ISBN: 9781930808935
- Rybak MJ, Lomaestro BM, Rotschafer JC, et al. "Vancomycin Therapeutic Guidelines: A Summary of Consensus Recommendations from the Infectious Diseases Society of America, the American Society of Health‐System Pharmacists, and the Society of Infectious Diseases Pharmacists". Clin Infect Dis. 49(3). :325-327. (2009)
- Toi H, Kinoshita K, Hirai S, et al. "Present epidemiology of chronic subdural hematoma in Japan: analysis of 63,358 cases recorded in a national administrative database". J Neurosurg. 128(1). :222-228. (2018)
- Holly LT, Kelly DF, Counelis GJ, et al. "Cervical spine trauma associated with moderate and severe head injury: incidence, risk factors, and injury characteristics". J Neurosurg. 96(3). :285-291. (2002)