Summary
Supraventricular tachycardias (SVTs) are a group of tachyarrhythmias arising from abnormalities in pacemaker activity and/or conduction involving myocytes of the atria and/or AV node. Types of SVT include atrioventricular nodal reentrant tachycardia (AVNRT; approx. two-thirds of cases), atrioventricular reciprocating tachycardia (AVRT), focal atrial tachycardia (FAT), multifocal atrial tachycardia (MAT), and junctional tachycardia. AVNRT and AVRT are caused by abnormal conduction circuits that form an unending loop of conduction referred to as reentry. These reentry circuits can occur between parallel pathways within the AV node (as in AVNRT) or between the AV node and an accessory pathway of atrioventricular conduction (as in AVRT). Atrial tachycardias (FAT and MAT) and junctional tachycardias are usually the result of abnormal or ectopic pacemaker activity and do not involve reentry. The most common congenital accessory pathway (bundle of Kent) is seen in Wolff-Parkinson-White (WPW) syndrome and can cause ventricular preexcitation, in which supraventricular impulses bypass the AV node and are abnormally conducted to the ventricles, leading to a characteristic preexcitation pattern on ECG and a specific subset of preexcited tachyarrhythmias. SVTs have similar clinical features (typically paroxysms of tachycardia with dizziness, dyspnea, chest pain, or syncope) that may be self-limiting or progress to hemodynamic instability and sudden cardiac death. Common diagnostic steps include obtaining the patient's history and a 12-lead ECG to identify the type of SVT. The paroxysmal nature of SVTs means that continuous recording with a Holter monitor is often needed to confirm the diagnosis; in some cases, invasive electrophysiological studies (EP studies) may also be indicated. Management of SVT should be tailored to the patient. Most hemodynamically unstable patients are treated with emergency cardioversion, while patients with acute SVT episodes that are hemodynamically stable may benefit from vagal maneuvers and/or antiarrhythmic medication (typically intravenous), depending on the underlying rhythm. Long-term management may involve antiarrhythmic medication or curative catheter ablation.
The following are discussed in detail separately: “Management of tachycardia,” “Atrial fibrillation with rapid ventricular response” and “Atrial flutter.“
Definitions
Tachycardias
- Paroxysmal tachycardia: an arrhythmia with an abrupt onset and termination that can last from seconds to days (e.g., AVNRT) [1]
-
Supraventricular tachycardia (SVT)
- A tachycardia originating in the following: [2][3]
- Sinus node
- AV node
- Atrial myocardium
- Bundle of His above the bifurcation
- Includes:
- Reentrant tachycardias: e.g., AVNRT, AVRT
- Atrial tachycardias: focal AT, multifocal AT, Afib, Atrial flutter
- Inappropriate sinus tachycardia
- Junctional tachycardia
-
Paroxysmal SVT (PSVT)
- Any SVT with a narrow QRS complex and an abrupt onset
- Most commonly caused by AV nodal reentry
- A tachycardia originating in the following: [2][3]
Conduction abnormalities
Reentry
- A mechanism that causes an impulse in the heart (which would normally die out) to return via conduction circuit to reexcite the tissue, leading to an extra beat (or, if it continues, an ongoing tachyarrhythmia) [4][5]
- Examples of reentrant tachycardias include AVNRT and AVRT.

")
Aberrant conduction [6][7]
- Abnormal conduction of a myocardial impulse due to, e.g., a bundle branch block, conduction delay, or (according to some definitions) an accessory pathway
- Results in a wide QRS complex, as the depolarization of the ventricle happens more slowly (from myocyte to myocyte) rather than through rapidly conducting Purkinje fibers
- SVT with aberrant conduction can have a very similar appearance to ventricular tachycardia (see “Differentiating between VT and SVT” in “Management of tachycardia”).
Preexcitation
- Ventricular preexcitation: the premature activation of the ventricles by an accessory pathway
- Accessory pathway: an abnormal electrical connection outside of the AV node that allows for the propagation of impulses between the myocardium of the atrium and the ventricle; usually congenital, e.g., the bundle of Kent (see “Wolff-Parkinson-White syndrome”), but also rarely acquired [2]
- Preexcitation syndrome: the combination of ventricular preexcitation and associated tachyarrhythmias (e.g., AVRT, atrial flutter, atrial fibrillation, focal atrial tachycardia); WPW syndrome is the most common example
- Preexcitation pattern: the typical ECG appearance of ventricular preexcitation due to abnormal conduction and depolarization of the ventricles
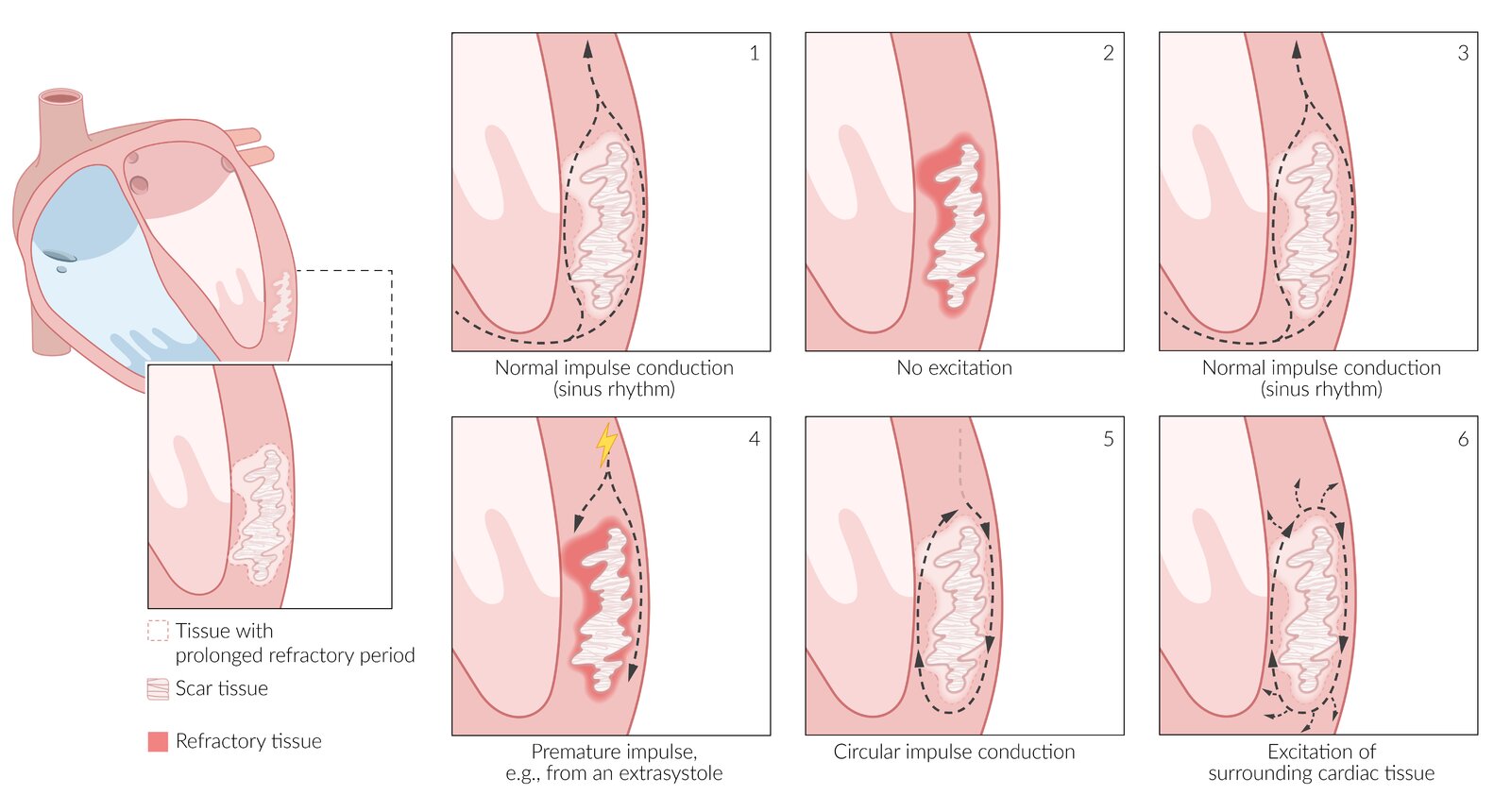
This illustration depicts the formation of a reentry circuit in ventricular tissue. However, similar principles apply to the formation of reentry circuits in other cardiac tissues.
Left: reentry requires the presence of a nonexcitable anatomical obstruction (here: ventricular scar tissue) and of 2 areas of tissue with mismatched conduction properties (here: healthy ventricular myocardium and a damaged area around the scar with a prolonged refractory period).
Right: development of a reentry tachyarrhythmia
1. Normal impulse conduction of sinus rhythm
2. Pause between impulses, healthy myocardium excitable again but damaged tissue remains refractory (red)
3. Normal impulse conduction of sinus rhythm
4. A premature impulse occurs in the pause shortly after the previous impulse, e.g., from a ventricular extrasystole. The wave of excitation is blocked on one side of the scar tissue by an area of refractory tissue but can pass on the other side.
5. By the time the wave of excitation has passed the scar tissue, the previously refractory tissue is now excitable again, leading to circular impulse conduction.
6. Circular impulse conduction continues and excites the surrounding myocardium, leading to a reentry tachycardia.
© AMBOSS
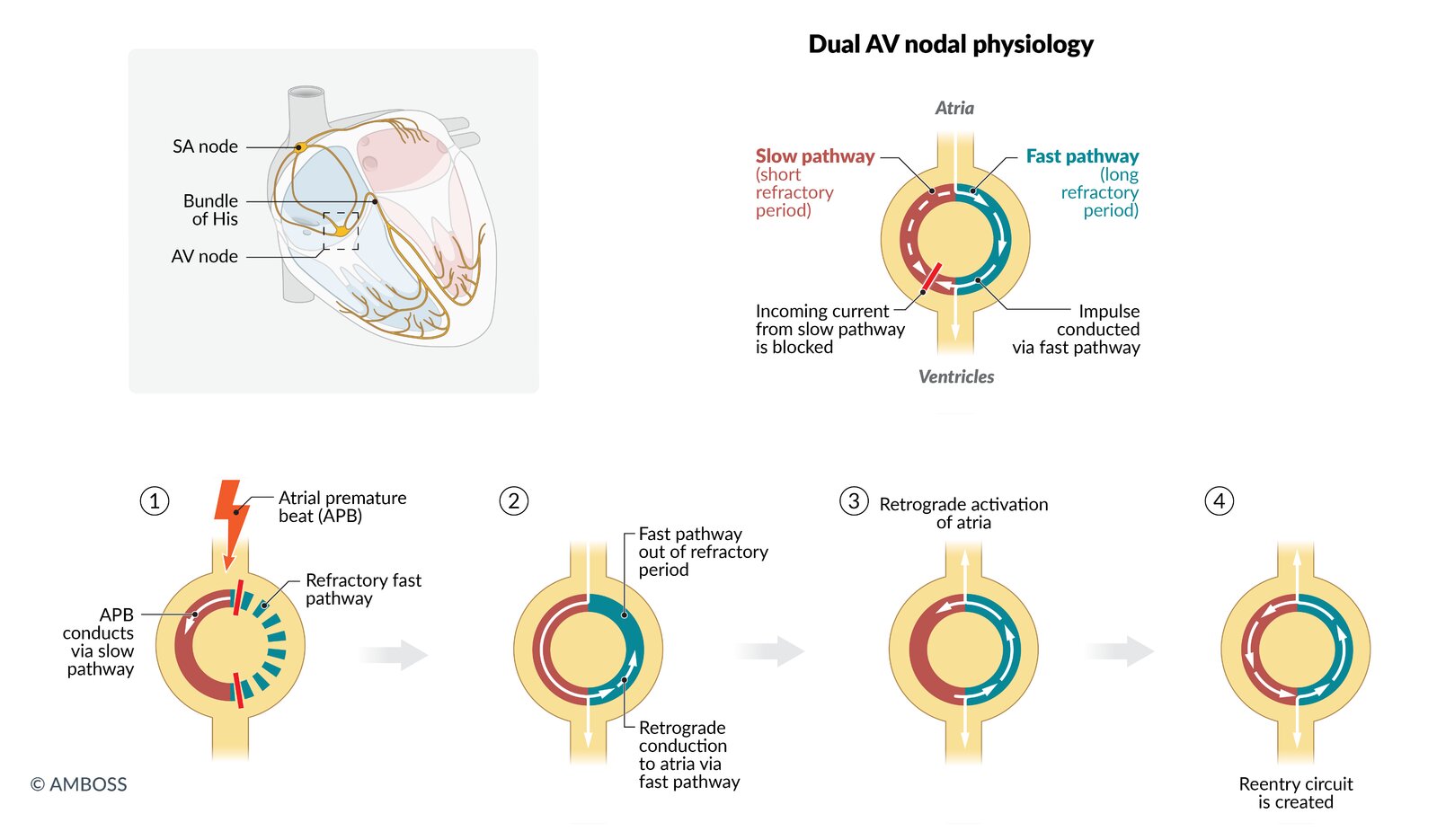
AVNRT is a tachyarrhythmia caused by a dysfunctional AV node with two electrical pathways, one fast with a long refractory period and one slow with a short refractory period (dual AV nodal physiology). During normal sinus rhythm, the conduction occurs via the fast pathway, and the incoming current from the slow pathway is extinguished (top right image).
Typical AVNRT is triggered by an atrial premature beat (APB).
(1) An APB arrives at the AV node during the fast pathway's refractory period. The impulse is, therefore, conducted through the slow pathway, which is out of its refractory period.
(2) When the impulse reaches the distal junction of the two pathways, the fast pathway has recovered its excitability and the impulse can travel up retrograde.
(3) The impulse reaches the atria, leading to an almost simultaneous depolarization of the atria and ventricles. The current reenters the slow pathway.
(4) A reentry circuit is created with anterograde conduction across the slow-conducting pathway and retrograde conduction in the fast pathway resulting in sustained tachycardia.
© AMBOSS
Overview
Treat unstable SVTs (except for MAT and junctional tachycardia) with electrical cardioversion.
If there is doubt about the supraventricular origin of a wide complex tachycardia, treat it as ventricular tachycardia.
| Overview of SVTs [2][8] | ||||
|---|---|---|---|---|
| Type of SVT | Description | Distinguishing ECG features | Acute management of stable patients | Long-term management options |
| AVNRT |
|
|
|
|
| Orthodromic AVRT |
|
|
|
|
| Antidromic AVRT |
|
|
|
|
| Focal AT |
|
|
|
|
| Multifocal AT |
|
|
|
|
| Afib with RVR |
|
|
|
|
| Atrial flutter |
|
|
||
| WPW syndrome [9] |
|
|
|
|
| Junctional tachycardia |
|
|
|
|

© AMBOSS
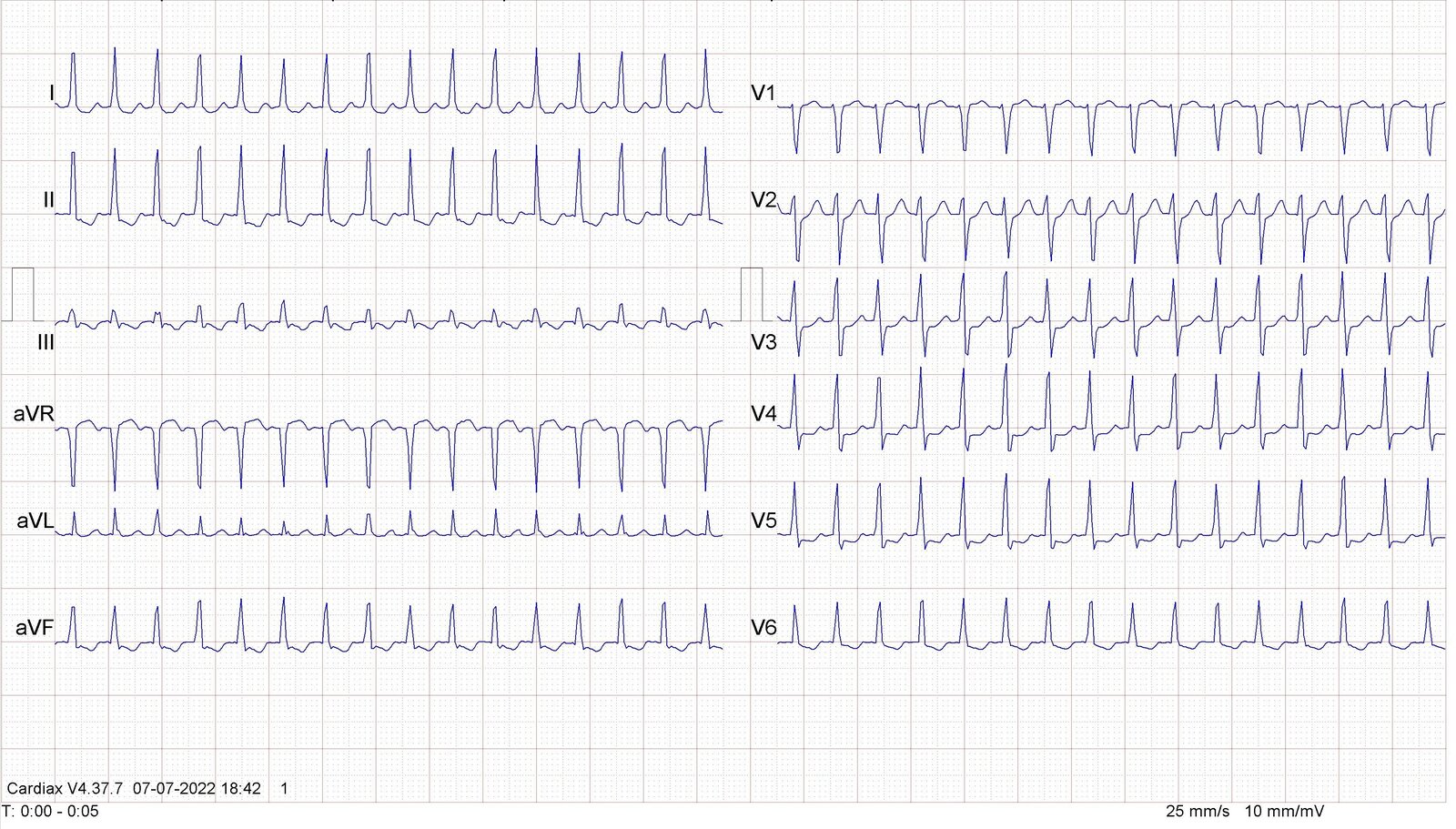
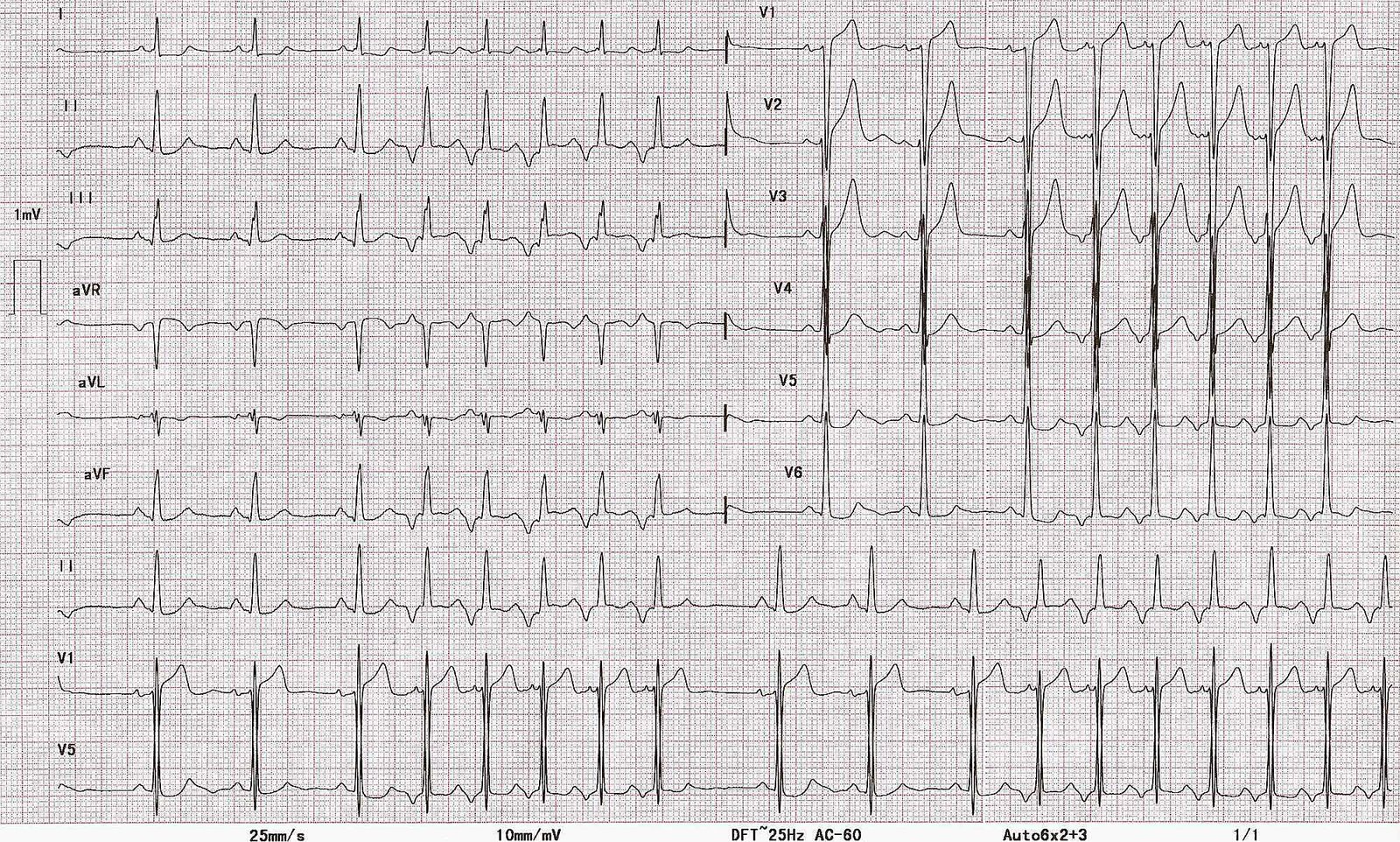
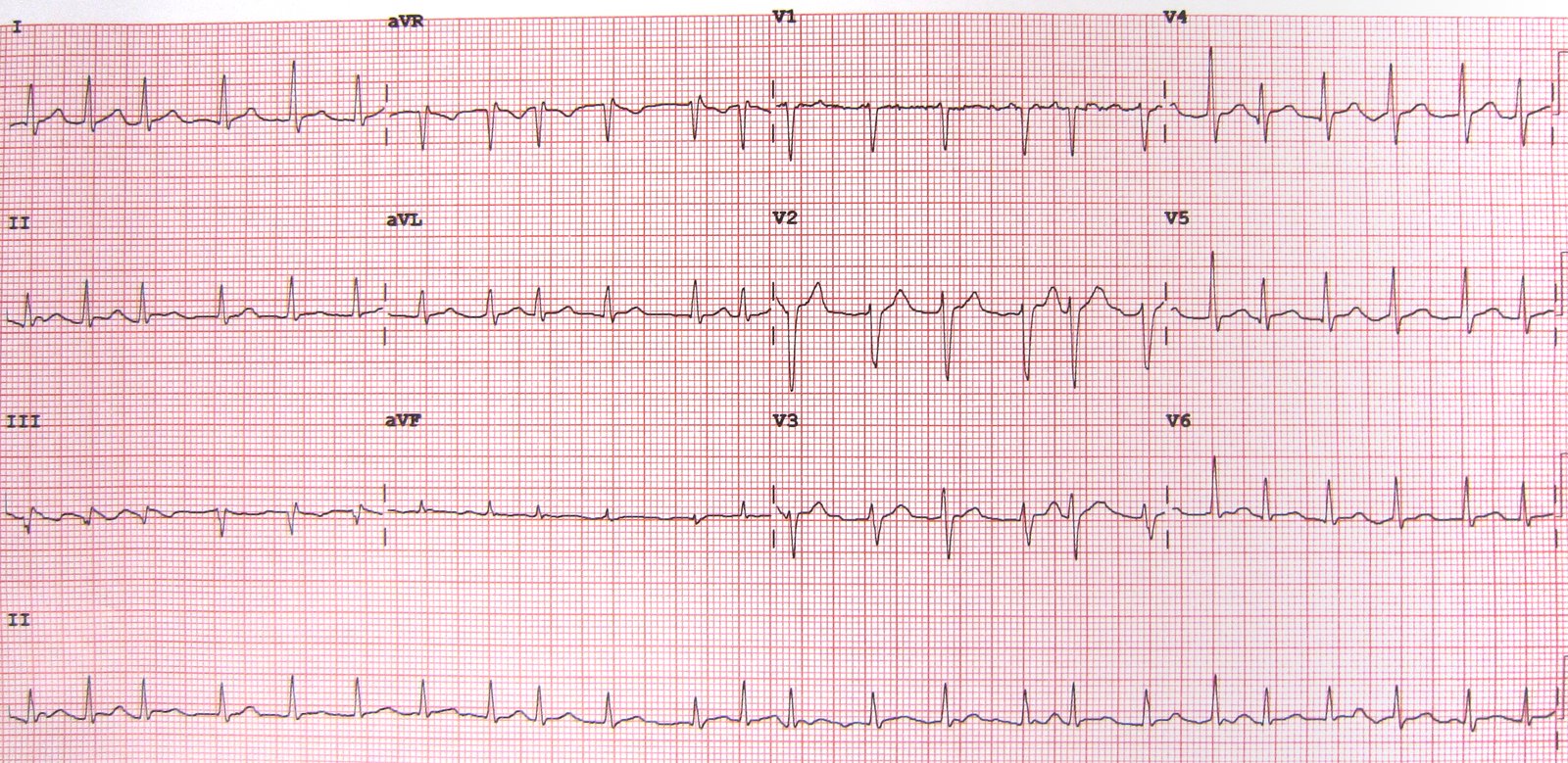
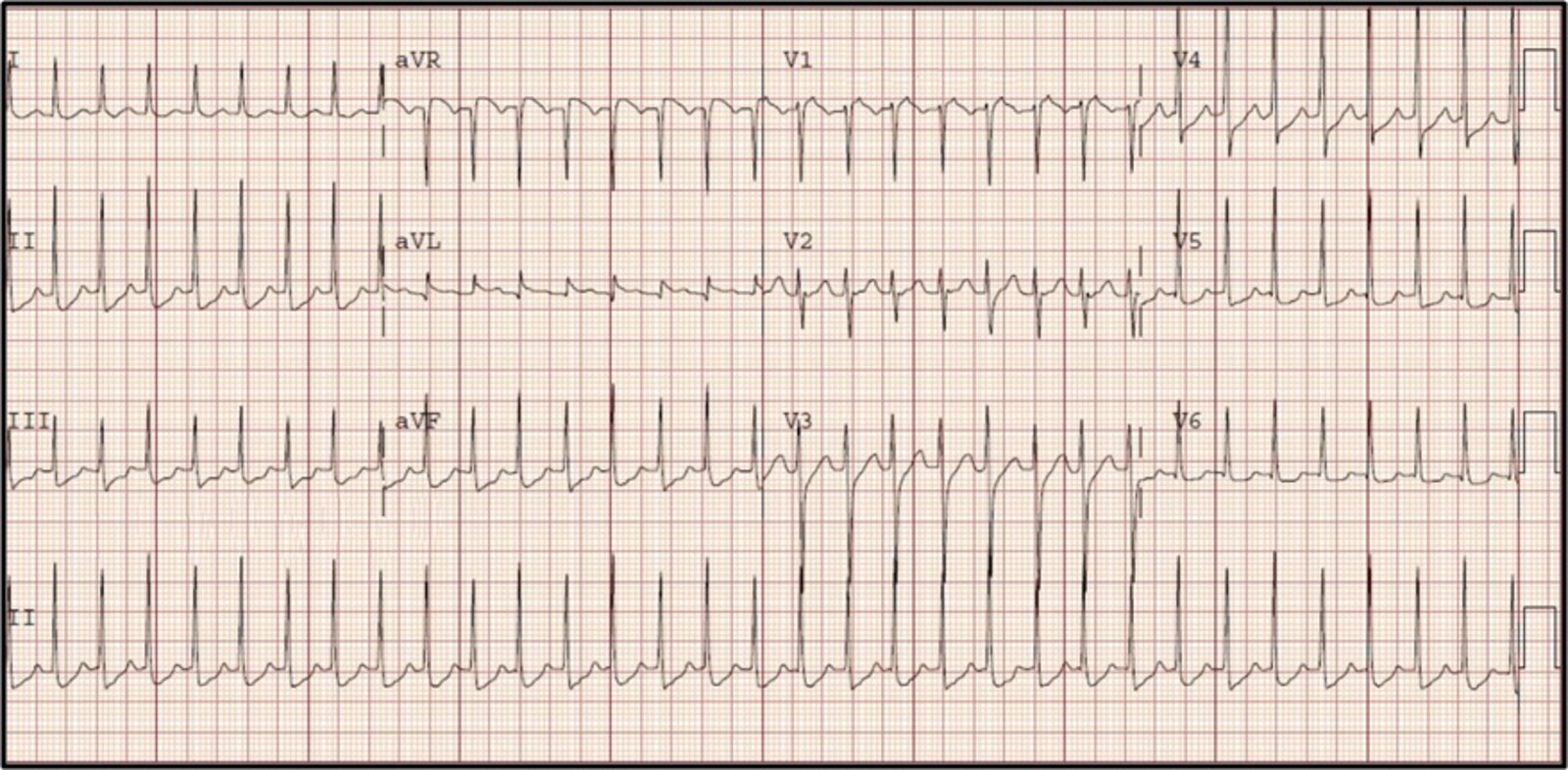
12-lead ECG (paper speed: 25 mm/s)
– Regular rhythm; heart rate ∼190/min.
– Normal cardiac axis (R > S in leads I and aVF)
– Narrow QRS complexes (< 100 ms)
– No visible P waves (they are buried in the QRS complexes)
– Widespread ST segment depression, most prominent in V3–V5 (likely rate-related; indicated by red overlay)
– QRS alternans: QRS amplitude is normal throughout but oscillates (indicated by green line)
A regular, narrow-complex tachycardia without visible P-waves is characteristic of AVNRT. Rate-related ST depression and QRS alternans are also commonly observed.
Our great thanks to Thomas Vahldieck, MD, for kindly providing this case.
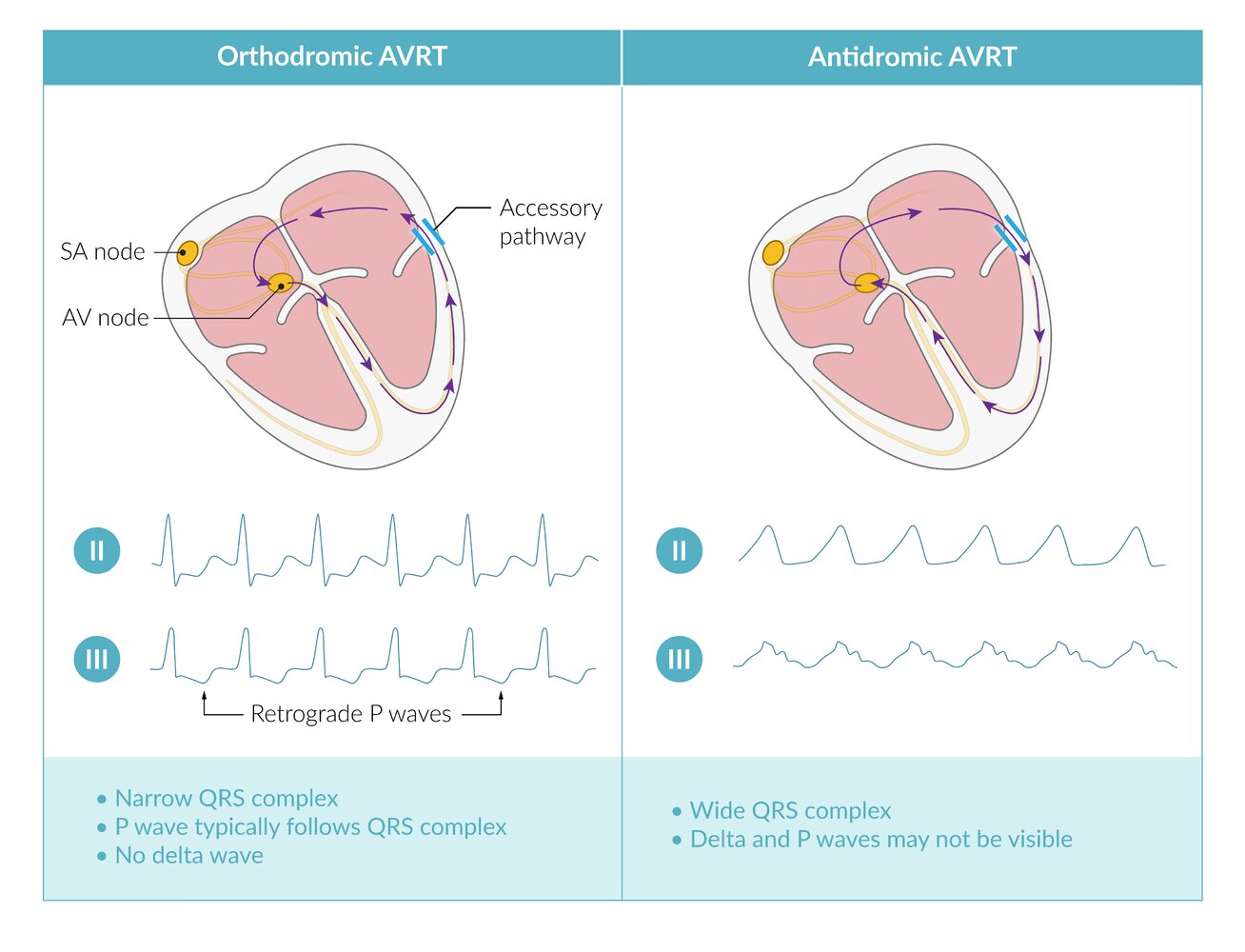
Atrioventricular reciprocating tachycardia (AVRT) can occur when an accessory pathway allows the formation of a reentrant circuit. AVRT is classified as orthodromic (90–95%; conduction through AV node is atrium → ventricle) or antidromic (rare; conduction through AV node is ventricle → atrium), which can be differentiated by their ECG features. Note that the ECG of antidromic AVRT is very difficult to distinguish from that of ventricular tachycardia (VT).
© AMBOSS
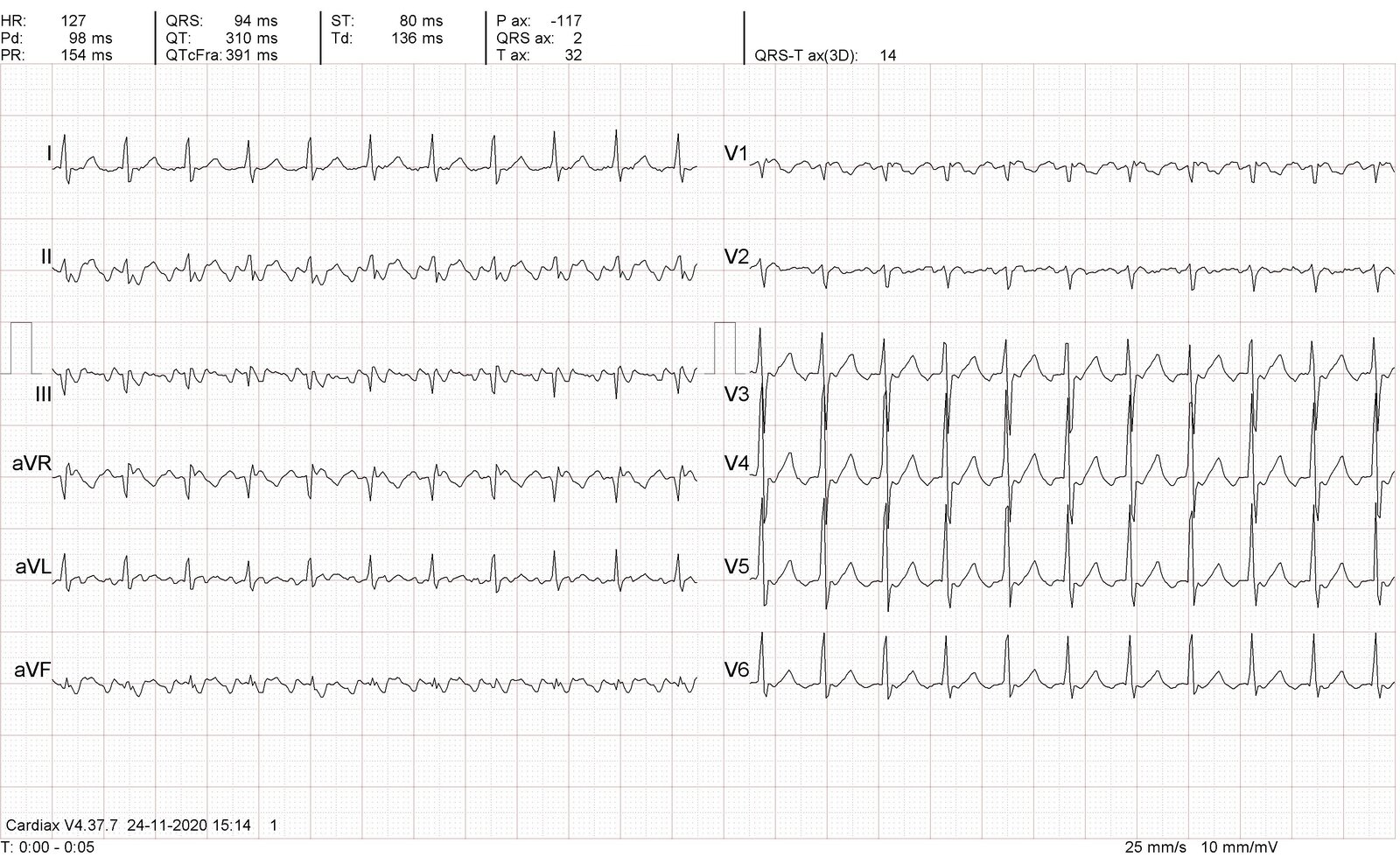
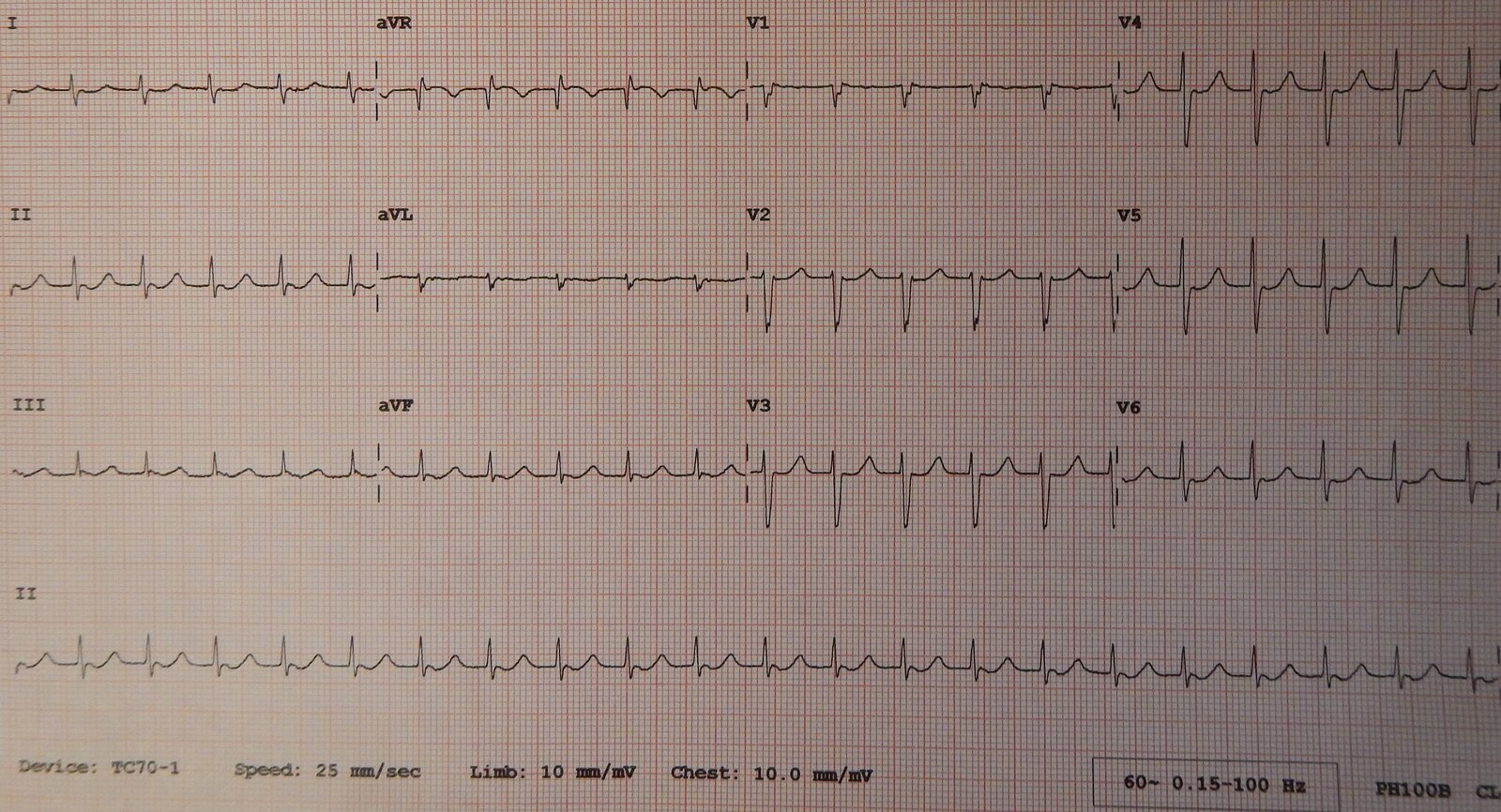
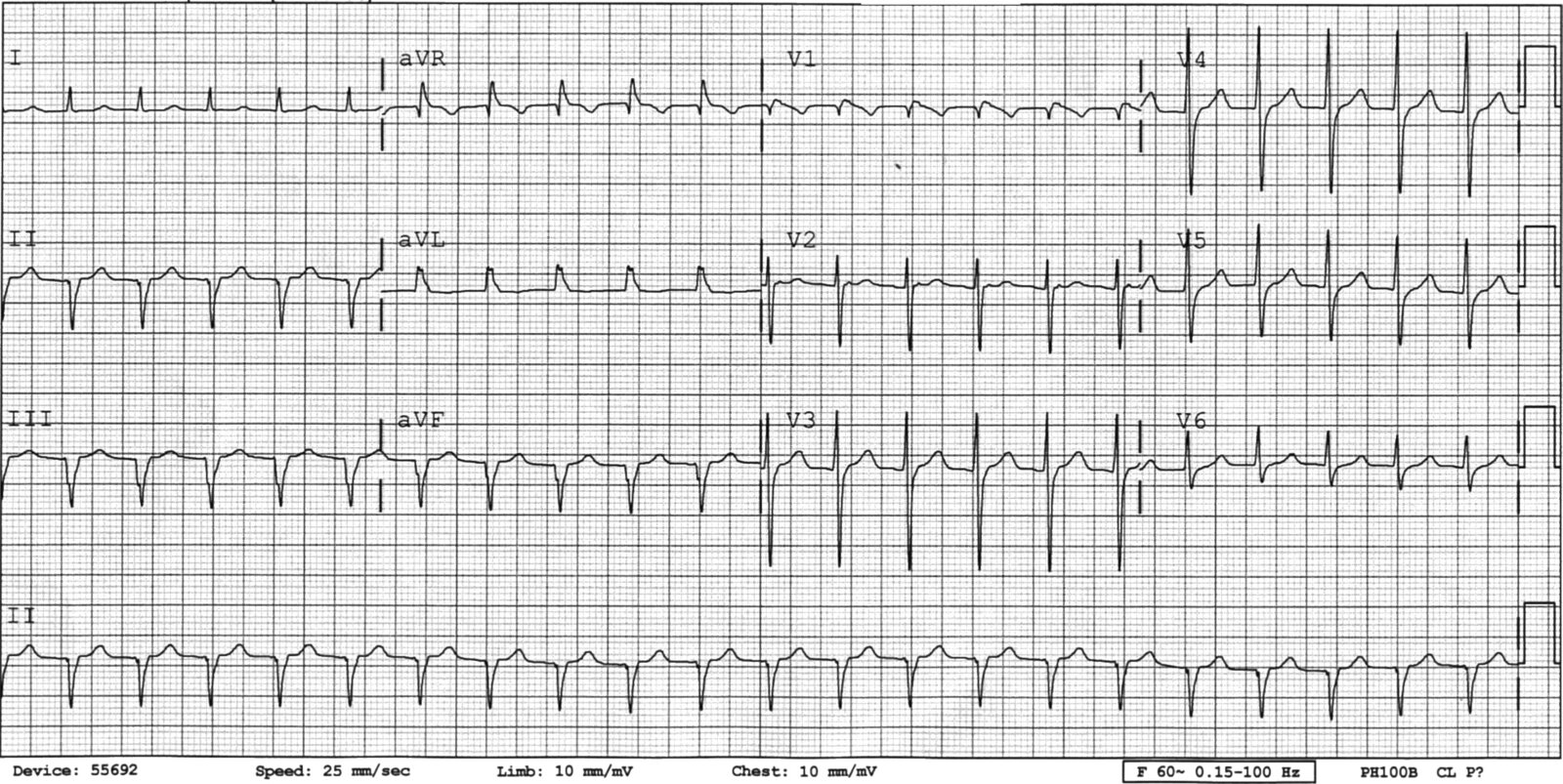
12-lead ECG (paper speed: 25 mm/s)
- Two periods of sinus rhythm (varying between 79–85/min; black interval lines) alternating with two periods of tachycardia (∼ 137/min; dashed black interval lines)
- P-wave morphology and axis during tachycardia (red overlay) are different from those during sinus rhythm (blue overlay). During the periods of tachycardia, the P waves remain constant, indicating a single ectopic focus.
- 1:1 AV conduction
- QRS morphology remains normal throughout.
- Normal QRS axis (R > S in I and aVF)
- An isoelectric baseline is present.
These features are suggestive of focal atrial tachycardia.
Source: “Fig. 2, Twelve-lead ECG at presentation, in: Incessant Focal Atrial Tachycardia Leading to Tachycardiomyopathy” by Bhasin D, Arora G, Gupta A, Isser HS, Bansal S, Cureus, licensed under CC BY 4.0. Modifications: arrows removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
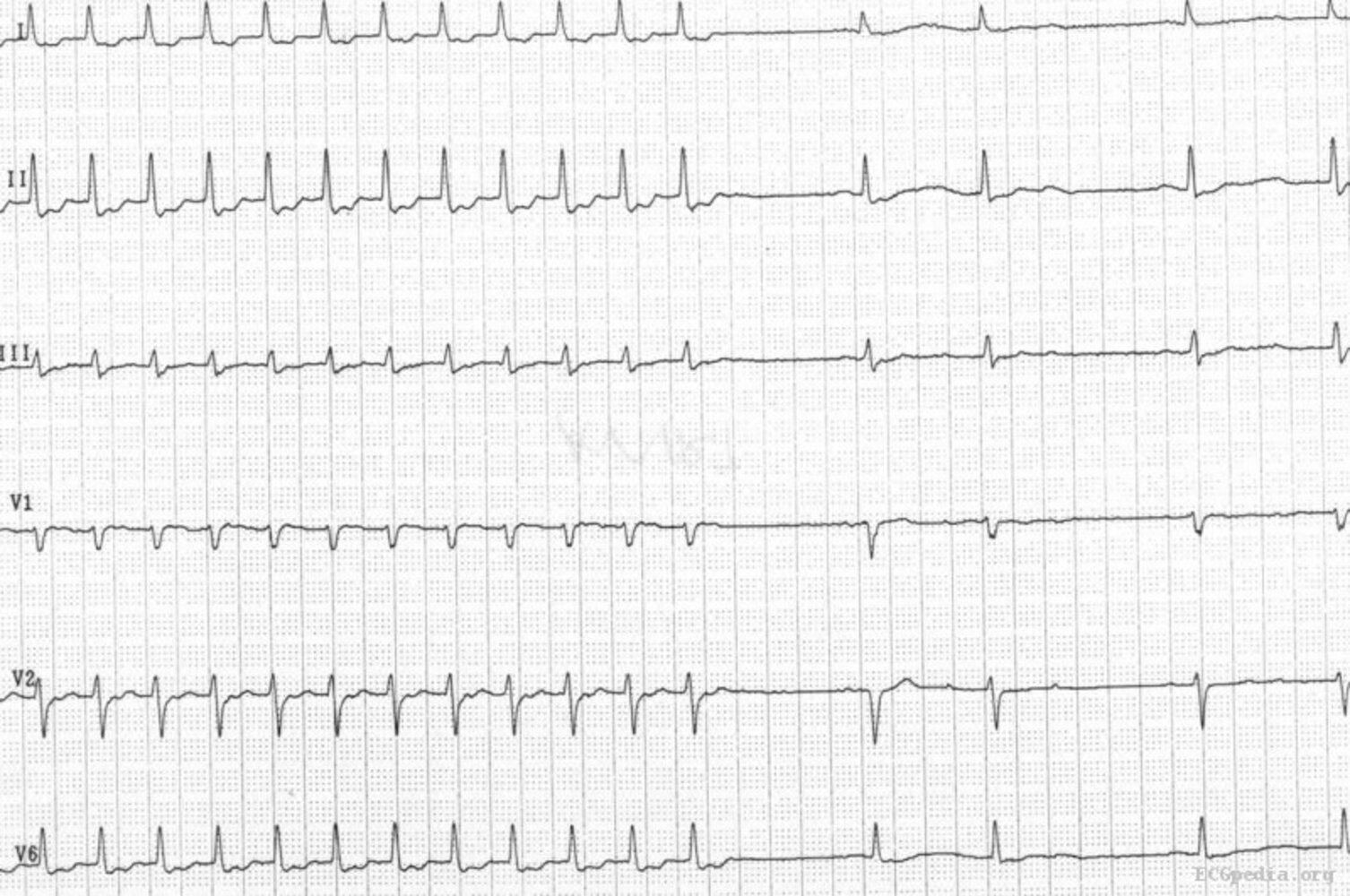
12-lead ECG (paper speed: 25 mm/s)
– Heart rate ∼ 160/min
– Irregularly irregular rhythm with wide variation in RR intervals (overlay) and variable PP, PR, and QT intervals
– ≥ P wave morphologies in the same lead (marked in rhythm strip II: normal, inverted, biphasic)
– Isoelectric baseline between P waves
– Narrow QRS complexes with similar morphology throughout
An irregularly irregular tachycardia with an isoelectric baseline and ≥ 3 distinct P wave morphologies in a single lead is consistent with multifocal atrial tachycardia.
Source: “Multifocal atrial tachycardia - MAT” by Jer5150, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
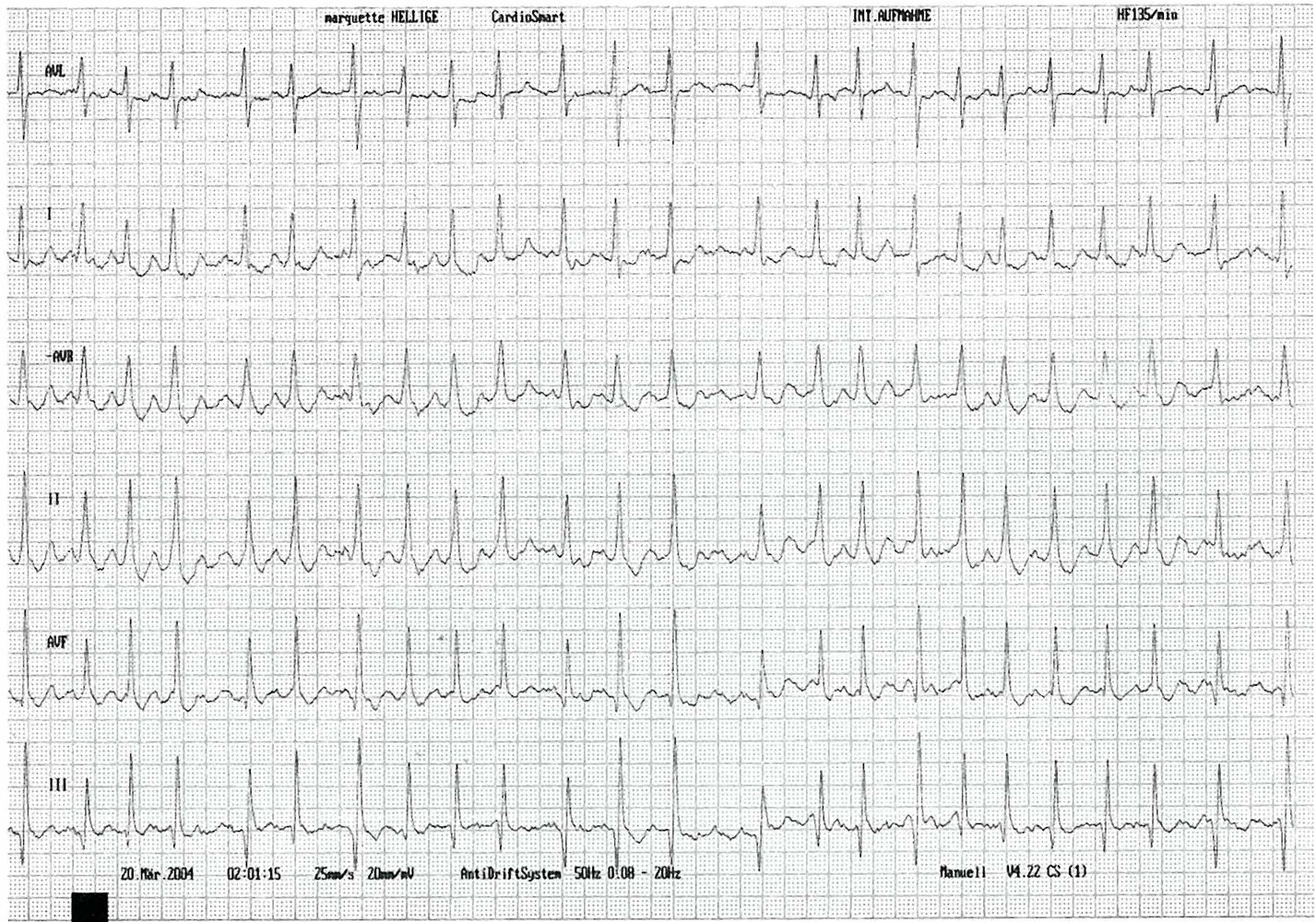
6-lead ECG (paper speed 25 mm/s)
– Heart rate: ~135/min
– Irregularly irregular RR intervals (examples indicated by black overlay)
– Normal axis
– Absent P waves
– Coarse fibrillatory waves (f waves; examples indicated by red overlay) can be seen between the QRS complexes. These are characterized by low amplitude, high frequency, and irregular morphology, and should not be confused with P waves or flutter waves.
The absence of P waves with irregularly irregular RR intervals and an elevated heart rate indicates atrial fibrillation with rapid ventricular response.
Source: © IMPP
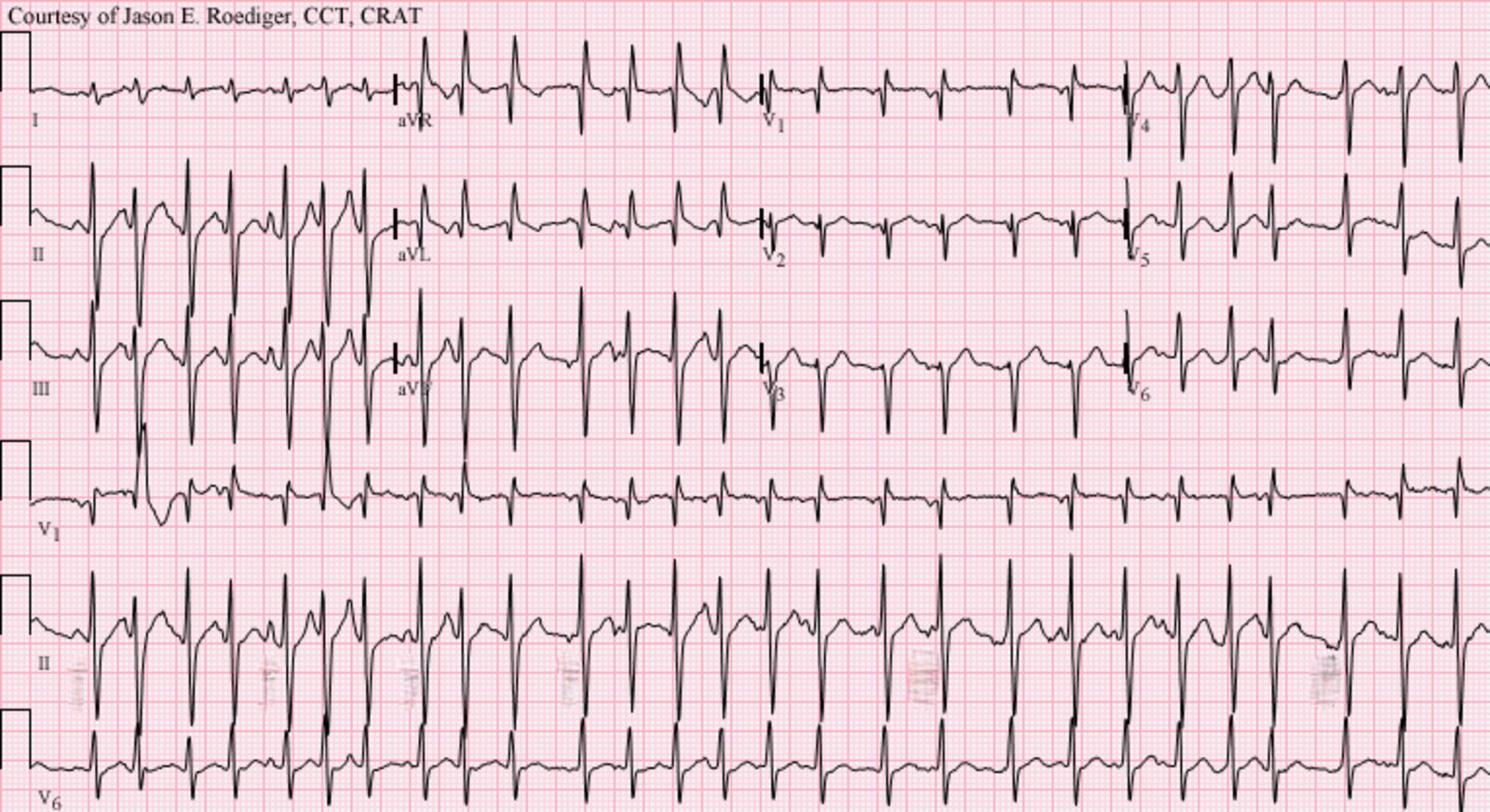
12-lead ECG (paper speed: 25 mm/s)
– Irregularly irregular rhythm
– Average ventricular rate is ∼ 144/min (24 QRS complexes can be seen on the 10-second rhythm strip)
– No discernable P waves
– Narrow QRS complexes
– Normal cardiac axis
These findings are characteristic of atrial fibrillation with rapid ventricular response.
Source: “RapidAFib150” by James Heilman, MD, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
12-lead ECG (paper speed: 25 mm/s)
- Regular rhythm
- Atrial rate of ∼ 250/min and ventricular rate of ∼ 125/min
- Normal axis (R > S in I and aVF)
- Sawtooth P wave morphology (flutter/F waves) best seen in II, III, aVF
These findings indicate atrial flutter with 2:1 AV block.
Our great thanks to Thomas Vahldieck, MD, for kindly providing this case.
12-lead ECG (paper speed: 25 mm/s)
- Regular rhythm
- Atrial rate of ∼ 250/min and ventricular rate of ∼ 83/min
- Normal axis (R > S in I and in II)
- Sawtooth P wave morphology (flutter/F waves) best seen in II, III, aVF
These findings are indicative of atrial flutter with 3:1 AV block.
Our great thanks to Thomas Vahldieck, MD, for kindly providing this case.
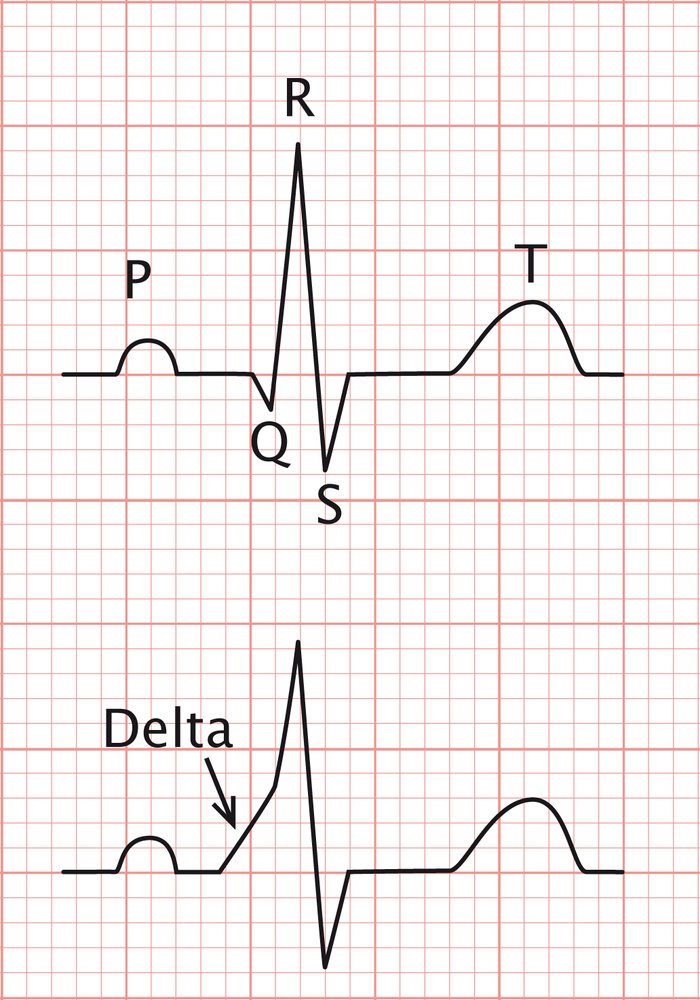
ECG Schematic (paper speed: 25 mm/s)
Top: normal ECG findings
Bottom: Slurred upstroke (i.e., delta wave) of the QRS complex is visible.
The delta wave is a sign of Wolff-Parkinson-White syndrome.
© AMBOSS
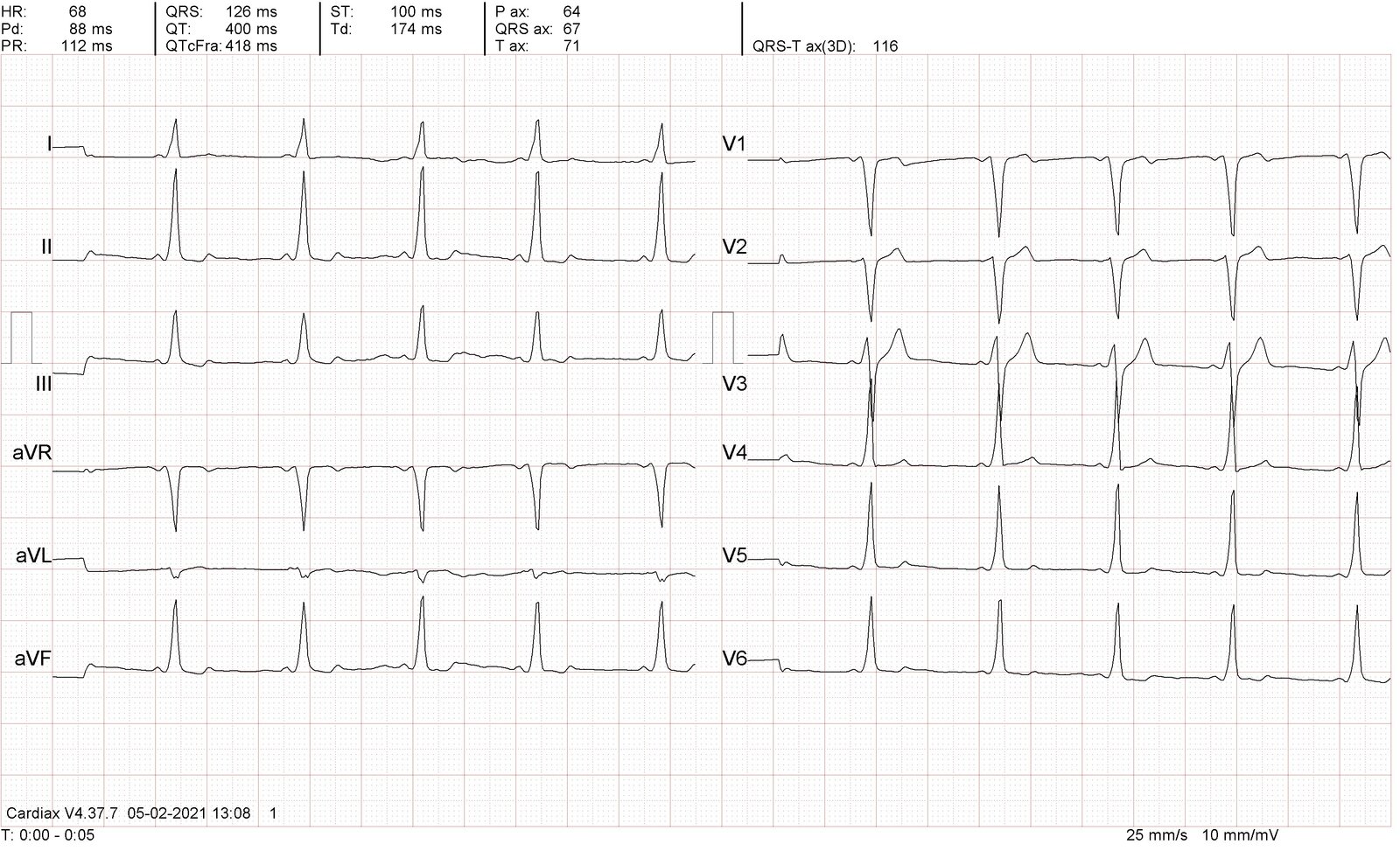
12-lead ECG (paper speed: 25 mm/s)
– Regular sinus rhythm
– Rate 68/min
– Normal axis (R > S in leads I and aVF)
– Short PR interval (112 ms)
– Wide QRS complexes (126 ms) with delta waves (the slurred initial portion of the QRS complex; zoom box)
A short PR interval and widened QRS complexes with delta waves are the characteristic ECG findings of Wolff-Parkinson-White (WPW) syndrome. If seen in asymptomatic patients with no evidence of arrhythmia, this constellation of findings is referred to as the "WPW pattern”.
Our great thanks to Thomas Vahldieck, MD, for kindly providing this case.
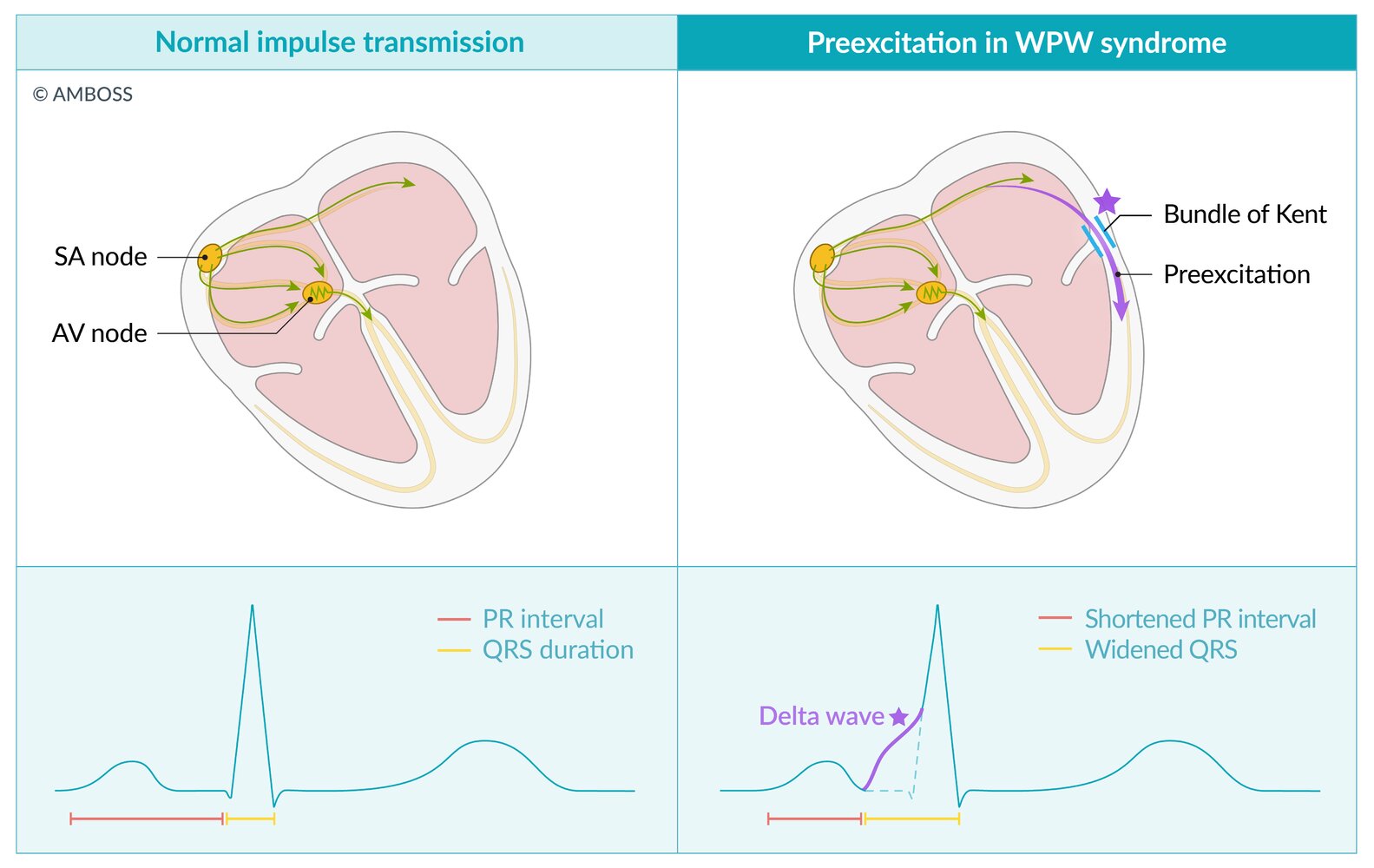
Conduction pathways and characteristic ECG findings in normal impulse transmission and in WPW syndrome. Note that the condition is referred to as WPW syndrome only if the characteristic ECG findings are present and the patient is also symptomatic or there is evidence of arrhythmia; if the characteristic ECG findings are present without these additional features, the condition is referred to as “WPW pattern.”
Left (normal impulse transmission and normal ECG findings): PR interval 120–200 ms; QRS duration < 100 ms
Right (WPW impulse transmission and characteristic ECG findings): short PR interval < 120 ms; slurred upstroke (delta wave) at the start of the QRS complex with widened QRS ≥ 120 ms
© AMBOSS
12-lead ECG (paper speed: 25 mm/s)
- Regular rhythm
- Heart rate: ∼ 130/min
- P waves immediately follow the QRS complexes (examples indicated with green arrowheads) and are inverted in I, II, aVF, and V4–V6 (retrograde P waves; examples indicated with red arrowheads).
- Cardiac axis borderline normal/right axis deviation (isoelectric in I, R > S in aVF)
- Narrow QRS complexes (∼80 ms)
- Persistent S wave
A regular, narrow complex tachycardia with retrograde P waves is suggestive of junctional tachycardia.
Source: “Junctional Tachycardia” by James Heilman, MD, Wikimedia Commons, licensed under CC BY-SA 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 4.0.
{kind=link}
Epidemiology
- Prevalence of SVT: ∼ 2.3 per 1000
- Incidence of PSVT: 36 per 100,000 per year
- Sex: ♀ > ♂ (2:1)
-
Risk factors
- Underlying structural heart disease
- Family history of SVT or sudden cardiac death
- Use of certain medications or illicit drugs [10]
Epidemiological data refers to the US, unless otherwise specified.
Clinical features
- Palpitations
- Fatigue
- Chest pain or discomfort
- Dyspnea
- Dizziness or presyncope
- Syncope (uncommon; occurs more frequently in older adults)
- Diaphoresis
- Additional features seen more commonly in AVNRT [2][11]
- Feeling of neck pounding/shirt flapping (thought to be due to cannon A waves)
- Urinary urgency and polyuria
- Symptom onset and resolution are typically abrupt, in contrast to sinus tachycardia (in which onset and resolution are more gradual).
- Sudden cardiac death (rare) [12]
Signs of unstable tachycardia due to SVT include acute pulmonary edema, hypotension, severe chest pain, and altered mental status.
Diagnosis
Approach
- Confirm the rhythm with a 12-lead ECG in all patients with new or recurrent SVT.
- Investigate the underlying cause using TTE and laboratory studies in patients with new or evolving diagnoses.
- Consider ambulatory ECG for with an uncertain diagnosis of paroxysmal SVT.
- Consider EP study for uncertain diagnoses that may also require catheter ablation.
- Consider cardiac stress testing for patients with ASCVD risk factors, suspected WPW, or provoked arrythmias.
Once the diagnosis is confirmed by ECG, do not delay acute management of SVT for additional investigations.
Initial diagnostics [11]
-
ECG: A 12-lead ECG should be performed in every patient with suspected SVT.
- Typical features during an episode include:
- Regular rhythm; may be irregular in MAT or atrial fibrillation
- Rate > 100/minute (typically exceeds > 150/minute) [2]
- Narrow QRS complex (< 120 ms); a wide complex may be seen with aberrant conduction
- If findings are inconclusive, consider recording the heart's electrical activity for 24–48 hours (e.g., Holter monitor, event recorder)
- Typical features during an episode include:
-
Laboratory studies: to identify underlying conditions
- CBC: can show signs of anemia or infection
- TSH: to assess for hyperthyroidism and hypothyroidism
- BMP: Electrolyte abnormalities (e.g., potassium disorders, calcium imbalances, hypomagnesemia) can cause arrhythmias.
-
TTE [13]
- Initial imaging modality of choice
- Potential findings include:
- Underlying structural or ischemic heart disease
- Heart failure in prolonged tachycardia
- Atrial thrombus (rare)
Additional diagnostics [11]
Consider the following tests depending on patient risk factors.
-
Prolonged electrocardiography [14]
- Indications: patients with infrequent symptoms
- Options
- 24-hour ambulatory ECG: if symptoms are frequent and likely to be captured in a 24-hour period
- Event recorder: if patients have infrequent and mild symptoms
- Implantable loop recorder: for patients with infrequent and severe symptoms that impede their ability to activate the recorder
- Data is downloaded from the device, allowing for an analysis of rhythm and an evaluation of whether symptoms correlate with arrhythmias.
-
EP study: with or without catheter ablation (Gold standard for diagnosing SVT; can be used for treatment)
- Indications include: uncertain diagnosis, planned ablation, risk stratification
- Disadvantages: invasive procedure, involves radiation
- Exercise tolerance testing: indicated in preexcitation (e.g., risk stratification in WPW syndrome) and suspected catecholamine-dependent arrhythmias
- Cardiac stress testing: indicated in patients with ASCVD risk factors
© AMBOSS
Differential diagnoses
Although differentiating between types of SVT can be challenging and may require EP studies to confirm the diagnosis, some ECG features may help to differentiate diagnoses.
- Sinus tachycardia: most common differential; often secondary to physiologic stress [15]
- Other narrow complex tachycardias (NCTs): See also “Differential diagnosis of SVT.”
- Other wide complex tachycardias (WCTs): See also “SVT with aberrancy vs. Vtach.”
Patients with SVT symptoms are frequently misdiagnosed with anxiety or panic disorders. Rule out paroxysmal tachycardia before making a psychiatric diagnosis to avoid anchoring bias.
The differential diagnoses listed here are not exhaustive.
© AMBOSS
Management
Acute management of SVT [2][8]
The underlying type of SVT is often unclear at presentation. A definitive diagnosis is not required to begin acute management of tachycardia following ACLS algorithms.
- Initiate continuous cardiac monitoring and ECG recording for all patients.
- Keep a defibrillator at the bedside in case rhythm and/or hemodynamics change (e.g., new Vfib).
Pulseless patients
- Start CPR.
- Defibrillate any WCT (i.e., possible Vtach); otherwise, treat as PEA.
Patients with unstable tachycardia with pulse
- Perform synchronized electrical cardioversion for most SVTs.
- Cardioversion will likely be ineffective for multifocal AT and junctional tachycardia.
Stable patients
Empiric management depends on QRS width and rhythm.
- SVT of unclear origin: See “Management of undifferentiated SVT.”
-
Regular NCT (e.g., AVNRT, orthodromic AVRT, focal AT)
- Typically includes vagal maneuvers and adenosine
- See “Management of stable regular NCT.”
-
Irregular NCT (e.g., multifocal AT, Afib)
- Can include rate control, rhythm control, or management of the underlying cause.
- See “Management of stable irregular NCT.”
-
WCT (e.g., SVT with aberrancy, antidromic AVRT, Afib with WPW)
- Usually treated with cardioversion
- AV nodal blockers are best avoided.
- See “Management of stable WCT”.
Avoid using AV nodal blockers to treat wide complex tachycardias, as they may precipitate Vfib. [16][17]
Vagal maneuvers
- Definition: a set of actions performed to decrease the heart rate through physical stimulation of the vagus nerve
- Physiology: slows the conduction through the AV node (negative homotopy) and may terminate the arrhythmia
-
Clinical application
- An important first step in acute management of most SVTs
- Avoid in ventricular preexcitation (due to an accessory pathway) with any of the following underlying tachyarrhythmias: atrial flutter, atrial fibrillation, focal atrial tachycardia, and MAT.
Valsalva maneuver
- Definition: forceful exhalation against a closed airway
-
Technique: four phases
- Phase 1 (start strain) and phase 2 (continued strain): ↑ intrathoracic pressure → ↓ venous return/ventricular preload → ↓ cardiac output
- Phase 3 (release of strain) & phase 4 (recovery phase): ↓ intrathoracic pressure → ↓ afterload → ↑ stroke volume → ↑ cardiac output
-
Applications
- Treatment of supraventricular tachycardia (e.g., AVNRT)
-
Evaluate conditions of the heart
- Augments heart sounds on physical exam (e.g., earlier click in mitral valve prolapse and louder murmur in hypertrophic obstructive cardiomyopathy)
- Decreases heart sounds intensity (most valve stenosis or regurgitation murmurs)
- Test for hernia or varicocele (increased intraabdominal pressure → bulging)
- Diagnosis of urinary stress incontinence (urine leakage during the maneuver)
- Measure to normalize middle-ear pressure (e.g., in diving)
- Contraindications: include recent myocardial infarction, aortic stenosis, and glaucoma. [18]
Modified Valsalva maneuver [18]
- Patient sits in a semirecumbent position
- Blows into a 10 mL syringe for 15 seconds (moving the plunger up achieves a strain of ∼ 40 mm Hg) [19]
- Afterwards the patient is laid supine and the legs are passively elevated to 45° for 15 seconds.
- Return to the semirecumbent position for 45 seconds before reassessing rhythm
Carotid sinus massage [20]
- Listen first to ensure there are no carotid bruits (if present, select another vagal maneuver). [21]
- Apply steady pressure at the level of the carotid bifurcation on one side for 10–15 seconds.
- If there is no response, the process can be repeated using the contralateral carotid sinus.
- Carotid sinus massage stimulates the baroreceptors → stimulates CN IX (specifically the branch of the glossopharyngeal nerve to the carotid sinus) → nerve impulse transmission to the medulla (nucleus tractus solitarius) → efferent signals from the medulla to the myocardium via the vagus nerve (parasympathetic supply) → ↓ AVN conduction, ↓ heart rate, ↓ contractility, and vasodilation (↓ blood pressure; may cause presyncope or syncope) → termination of arrhythmia
Diving reflex
- Traditionally involves immersing the head in cold water, which is uncomfortable for most patients
- Can be limited to applying a bag of ice water to the face (particularly the forehead and nasal area) for ∼ 10 seconds [22]
Do not simultaneously apply bilateral carotid artery pressure because this can impede cerebral blood flow.
Pharmacotherapy
- See “Management of undifferentiated SVT” for a general algorithm.
- Definitive pharmacotherapy depends on the underlying rhythm.
- See “Treatment of AVNRT.”
- See “Treatment of AVRT.”
- See “Treatment of WPW.”
- See “Treatment of focal AT.”
- See “Treatment of MAT.”
- See “Management of Afib with RVR.”
- See “Treatment of junctional tachycardia.”
Catheter ablation
-
Description
- Radiofrequency or cryothermal energy is applied via a cardiac catheter to eliminate aberrant pathways or impulses from arrhythmogenic foci.
- Usually performed in conjunction with an EP study
-
Indications [2]
- Curative therapy in AVNRT, AVRT with concealed pathway, or drug-refractory AT
- Symptomatic patients who want to avoid long-term drug therapy (especially younger patients)
- Asymptomatic patients with special lifestyle considerations (e.g., pilots)
Further management and disposition [23]
- Successful cardioversion: Consider discharge after a period of monitoring if clinically stable and no other acute medical issues.
-
Unsuccessful cardioversion
- Urgent cardiology consult for specialist treatment, e.g., a second dose of cardioversion, antiarrhythmic infusion
- Admit to critical care unit for further management.
-
Other indications for hospital admission
- Possible ischemic event
- Any VT or unstable rhythm (even if terminated)
- Any LOC
- Possible preexcitation syndrome
Atrioventricular nodal reentrant tachycardia
Definition
- A tachyarrhythmia caused by a dysfunctional AV node that contains two electrical pathways, which form a reentry circuit
Pathophysiology
- The AV node contains two electrical pathways, one fast and one slow → the electrical impulse circles around the AV node within both pathways → a continuous circuit conducts impulses to the ventricles → tachycardia
- Approx. 90% of cases are due to anterograde conduction across the slow-conducting pathway and retrograde conduction in the fast pathway (although the reverse is possible).
ECG findings in AVNRT [24][25]
ECG may be normal between episodes of tachycardia. Findings may be indistinguishable from those of orthodromic AVRT and include:
- Heart rate typically 150–220/minute
- Typically narrow QRS complexes (a wide QRS complex may be seen if there is aberrant conduction)
- Regular rhythm
- P wave is typically not visible (it falls in or is "buried" in the QRS complex)
")
")
")
")
Treatment of AVNRT
Acute management
- Unstable tachycardia with a pulse: electrical cardioversion
-
Stable with narrow QRS complex: See “Management of stable regular NCT.”
- First step: vagal maneuvers
-
If SVT persists: intravenous medical therapy
- First-line: adenosine (if no contraindications to adenosine present)
- Other options: calcium channel blockers (e.g., verapamil, diltiazem) or beta blockers (e.g., metoprolol)
-
Stable with wide QRS complex (suspected aberrant conduction): See “Management of stable WCT.”
- Established diagnosis of AVNRT: AV nodal blocking agents are generally safe. [26]
- Uncertain diagnosis of AVNRT: Avoid AV nodal blocking agents.
Long-term management
- Infrequent and mild episodes: may be managed with self-guided vagal maneuvers.
- First line: percutaneous catheter ablation of the slow pathway [2][27]
-
Second line: pharmacological therapy [2]
- Daily medication options
- Beta blockers, e.g., propranolol [2]
- Verapamil [2]
- Diltiazem [2]
-
Pill-in-the-pocket regimens (off-label) [28]
- Propranolol PLUS diltiazem [28]
- OR flecainide [2][28]
- Daily medication options
AVNRT is a tachyarrhythmia caused by a dysfunctional AV node with two electrical pathways, one fast with a long refractory period and one slow with a short refractory period (dual AV nodal physiology). During normal sinus rhythm, the conduction occurs via the fast pathway, and the incoming current from the slow pathway is extinguished (top right image).
Typical AVNRT is triggered by an atrial premature beat (APB).
(1) An APB arrives at the AV node during the fast pathway's refractory period. The impulse is, therefore, conducted through the slow pathway, which is out of its refractory period.
(2) When the impulse reaches the distal junction of the two pathways, the fast pathway has recovered its excitability and the impulse can travel up retrograde.
(3) The impulse reaches the atria, leading to an almost simultaneous depolarization of the atria and ventricles. The current reenters the slow pathway.
(4) A reentry circuit is created with anterograde conduction across the slow-conducting pathway and retrograde conduction in the fast pathway resulting in sustained tachycardia.
© AMBOSS
12-lead ECG (paper speed: 25 mm/s)
– Regular rhythm; heart rate ∼190/min.
– Normal cardiac axis (R > S in leads I and aVF)
– Narrow QRS complexes (< 100 ms)
– No visible P waves (they are buried in the QRS complexes)
– Widespread ST segment depression, most prominent in V3–V5 (likely rate-related; indicated by red overlay)
– QRS alternans: QRS amplitude is normal throughout but oscillates (indicated by green line)
A regular, narrow-complex tachycardia without visible P-waves is characteristic of AVNRT. Rate-related ST depression and QRS alternans are also commonly observed.
Our great thanks to Thomas Vahldieck, MD, for kindly providing this case.
6-lead ECG (paper speed 25 mm/s) showing AVNRT being terminated with adenosine
Left of dashed line: AVNRT before onset of adenosine effect (typical slow-fast subtype)
– Heart rate approx. 160/min
– Regular rhythm (regular RR intervals)
– Narrow QRS complexes
– P waves are visible after the QRS complexes (examples indicated by arrows and “P”)
– Short RP interval of ∼ 40 ms
Right of dashed line: transient irregular rhythm following termination of AVNRT by adenosine
Source: “De-Avnrt ecg (CardioNetworks ECGpedia)” by CardioNetworks, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
.jpg){kind=link}
12-lead ECG (paper speed: 25 mm/s)
– Regular rhythm; heart rate approx. 188/min
– Normal cardiac axis
– Narrow QRS complexes (< 100 ms)
– P waves are largely buried, occasional retrograde P waves (examples indicated by red lines and arrows) can be seen after the QRS complexes. e.g., in III, aVF
– ST depression in V5, V6
– QRS alternans: QRS amplitude is normal throughout but oscillates (best seen in rhythm strip at bottom of image; indicated by green line)
Source: “Figure 1, in: Atrioventricular Nodal Reentrant Tachycardia Triggered by Marijuana Use: A Case Report and Review of the Literature” by P. T. Kariyanna, A. Jayarangaiah, O. Yurevich et al., American Journal of Medical Case Reports, licensed under CC BY 4.0. Modifications: Arrows removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
12-lead ECG (paper speed: 25 mm/s)
– Regular rhythm; heart rate approx. 130/min.
– Left axis deviation (QRS complexes are positive in I, negative in aVF and II)
– Narrow QRS complexes (< 100 ms)
– No visible P waves (they are buried in the QRS complexes)
This ECG shows the characteristic features of AVNRT: a regular, narrow-complex tachycardia without visible P-waves. The rate however is typically higher (∼ 150–220/min).
Source: “EKG-AVNRT-030315” by Laniakea-rubikon, Wikimedia Commons, licensed under CC BY-SA 4.0.
{kind=link}
Atrioventricular reciprocating tachycardia
Definition
- A tachyarrhythmia caused by an accessory pathway that creates a reentrant circuit with the AV node
- Wolff-Parkinson-White syndrome is a common cause of AVRT but they are not synonymous. [11]
Pathophysiology [11][29]
-
Orthodromic AVRT (most common; 90–95%) [30]
- Antegrade conduction (atrium → ventricle) through AV node (narrow QRS complex); retrograde conduction (ventricle → atrium) through accessory pathway
- Can occur with a concealed or manifest pathway
- On rare occasions, occurs almost incessantly as a result of a concealed, posteroseptal pathway (permanent junctional reciprocating tachycardia; PJRT) [2][31]
-
Antidromic AVRT (rare; 5–10%) [32]
- Antegrade conduction (atrium → ventricle) through accessory pathway; retrograde conduction (ventricle → atrium) through AV node
- Wide QRS complex, as ventricular depolarization happens slowly from myocyte to myocyte rather than through the rapid His-Purkinje system
- Only occurs with a manifest pathway
AVRT is caused by an accessory pathway, whereas in AVNRT there are two functional pathways within the AV node.

ECG findings
| ECG findings in AVRT [11][33][34] | |
|---|---|
| Orthodromic AVRT |
|
| Antidromic AVRT |
|
Treatment of AVRT
Acute episodes
- Unstable tachycardia with a pulse: electrical cardioversion
-
Stable orthodromic AVRT: See “Management of stable regular NCT.”
- First step: vagal maneuvers
-
If SVT persists: intravenous medical therapy
- First-line: adenosine (if there are no contraindications to adenosine)
- Other options: calcium channel blockers (e.g., verapamil, diltiazem) or beta blockers (e.g., metoprolol)
-
Stable antidromic AVRT (wide QRS complex): See “Management of stable WCT.”
- Established diagnosis of AVRT: AV nodal blocking agents are safe.
- Uncertain diagnosis of AVRT: Avoid AV nodal blocking agents.
Long-term management [2]
- First-line: catheter ablation
-
Pharmacotherapy for AVRT: for patients who are not candidates for ablation or who prefer medication
- Treatment depends on whether a preexcitation pattern is seen on ECG (options include sotalol, flecainide; , and propafenone). [2]
-
Preexcitation pattern is visible.
- Known heart disease: sotalol OR dofetilide
- No known heart disease: flecainide OR propafenone
-
Preexcitation pattern is not visible.
- CCBs: verapamil OR diltiazem
- Beta blockers: propranolol OR metoprolol
- Alternative: : Consider amiodarone if no other treatments are effective or if all are contraindicated.
Atrioventricular reciprocating tachycardia (AVRT) can occur when an accessory pathway allows the formation of a reentrant circuit. AVRT is classified as orthodromic (90–95%; conduction through AV node is atrium → ventricle) or antidromic (rare; conduction through AV node is ventricle → atrium), which can be differentiated by their ECG features. Note that the ECG of antidromic AVRT is very difficult to distinguish from that of ventricular tachycardia (VT).
© AMBOSS
Wolff-Parkinson-White syndrome
Definitions
- Wolff-Parkinson-White syndrome: (WPW): a congenital condition characterized by intermittent tachycardias and signs of ventricular preexcitation on ECG, both of which arise from an accessory pathway known as the bundle of Kent
- Wolff-Parkinson-White pattern: characteristic signs of ventricular preexcitation on ECG with no evidence of arrhythmia and no reported symptoms [35]
Pathophysiology
- A congenital accessory pathway, the bundle of Kent, connects the atria and ventricles, bypassing the AV node and leading to ventricular preexcitation.
- May be associated with structural abnormalities of the heart, in particular Ebstein anomaly [36]
- ∼ 10% of patients have multiple accessory pathways (more common with coexisting structural heart disease). [35][37]
-
May be asymptomatic (WPW pattern) or associated with arrhythmias (WPW syndrome), including: [36]
- AVRT (most common; 80%)
- Atrial fibrillation (15–35%; incidence increases with age)
- Atrial flutter (5%)
- Others (rare): MAT, focal atrial tachycardia, ventricular fibrillation
 syndrome and pattern")
Epidemiology
- The prevalence of WPW pattern is 0.1–0.2% in the general population and 0.55% in first-degree relatives. [38]
- A proportion of these cases is due to familial WPW syndrome, a rare autosomal-dominant genetic disorder that causes conduction abnormalities and hypertrophic cardiomyopathy. [39]
- ♂ > ♀ [40]
- Symptoms typically develop at 20–40 years of age. [36]
ECG findings in WPW
-
While in sinus rhythm, a preexcitation pattern may be present. [9]
- Short PR interval
- ECG delta wave: a slurred upstroke at the start of the QRS complex, secondary to preexcitation
- Widened QRS
-
Can show any of the arrhythmias associated with WPW [36]
- See “ECG findings in AVRT.”
- See “WPW with atrial fibrillation.”


 syndrome with atrial fibrillation (1/2)")
 syndrome after conversion from atrial fibrillation (2/2)")
Treatment of WPW [8]
Acute episodes
- Unstable tachycardia with a pulse: electrical cardioversion
-
Stable: Assess underlying rhythm.
- Regular NCT (i.e., orthodromic AVRT): vagal maneuvers, adenosine; see “Management of stable regular NCT”
-
WCT: irregular (e.g., underlying Afib or multifocal AT) OR regular (underlying Aflut or focal AT) [8]
- Avoid AV nodal blocking agents and vagal maneuvers (may precipitate Vtach or Vfib)
- Rhythm control measures (i.e., cardioversion or IV procainamide) are the safest treatment option.
- See “Management of stable WCT” and ”Management of preexcited Afib.”
Avoid AV nodal blocking agents and vagal maneuvers for the following preexcited tachycardias: Afib, Aflut, focal AT, and MAT.
Long-term management of WPW [2][40]
Management of WPW pattern and WPW syndrome depends on underlying risk factors and patient preference.
Risk stratification in WPW syndrome [41]
Risk stratification is determined by a cardiologist based on clinical, ECG, and electrophysiological parameters.
-
Concerning clinical features
- Syncope
- Associated atrial fibrillation, atrial flutter, or atrial tachycardia
- Aborted sudden cardiac death
- Dynamic ECG testing: e.g., ambulatory Holter monitoring or exercise stress testing to assess for evidence of intermittency or loss of preexcitation [42]
-
EP studies
- Indicated in patients with:
- Concerning clinical features
- No evidence of intermittency or loss of preexcitation signs
- High-risk occupations (e.g., pilots, athletes)
- Allows the length of the refractory period to be determined [41]
- Indicated in patients with:
High-risk patients
Catheter ablation of the accessory pathway should be offered to all patients. [2]
Low-risk patients [2]
- Asymptomatic: usually no treatment required
- Symptomatic
- First-line: catheter ablation
- Second-line (e.g., ablation contraindicated or declined): long-term antiarrhythmics in consultation with a cardiologist
- No structural heart disease: Consider flecainide OR propafenone. [2]
-
Structural heart disease
- Consider dofetilide OR sotalol
- Use AV nodal blockers with caution.
Conduction pathways and characteristic ECG findings in normal impulse transmission and in WPW syndrome. Note that the condition is referred to as WPW syndrome only if the characteristic ECG findings are present and the patient is also symptomatic or there is evidence of arrhythmia; if the characteristic ECG findings are present without these additional features, the condition is referred to as “WPW pattern.”
Left (normal impulse transmission and normal ECG findings): PR interval 120–200 ms; QRS duration < 100 ms
Right (WPW impulse transmission and characteristic ECG findings): short PR interval < 120 ms; slurred upstroke (delta wave) at the start of the QRS complex with widened QRS ≥ 120 ms
© AMBOSS
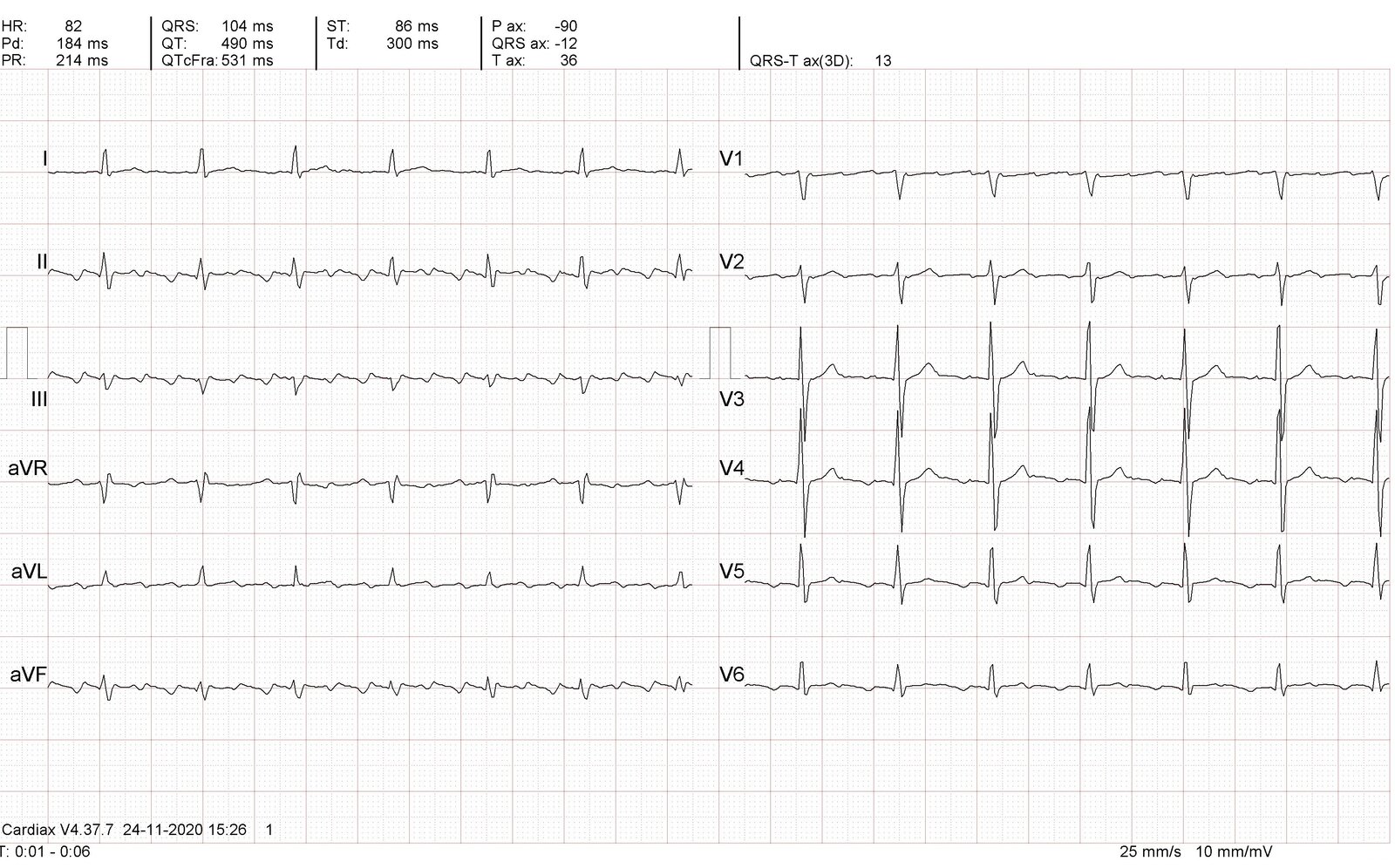
12-lead ECG (paper speed: 25 mm/s)
– Regular sinus rhythm
– Rate 68/min
– Normal axis (R > S in leads I and aVF)
– Short PR interval (112 ms)
– Wide QRS complexes (126 ms) with delta waves (the slurred initial portion of the QRS complex; zoom box)
A short PR interval and widened QRS complexes with delta waves are the characteristic ECG findings of Wolff-Parkinson-White (WPW) syndrome. If seen in asymptomatic patients with no evidence of arrhythmia, this constellation of findings is referred to as the "WPW pattern”.
Our great thanks to Thomas Vahldieck, MD, for kindly providing this case.
ECG Schematic (paper speed: 25 mm/s)
Top: normal ECG findings
Bottom: Slurred upstroke (i.e., delta wave) of the QRS complex is visible.
The delta wave is a sign of Wolff-Parkinson-White syndrome.
© AMBOSS
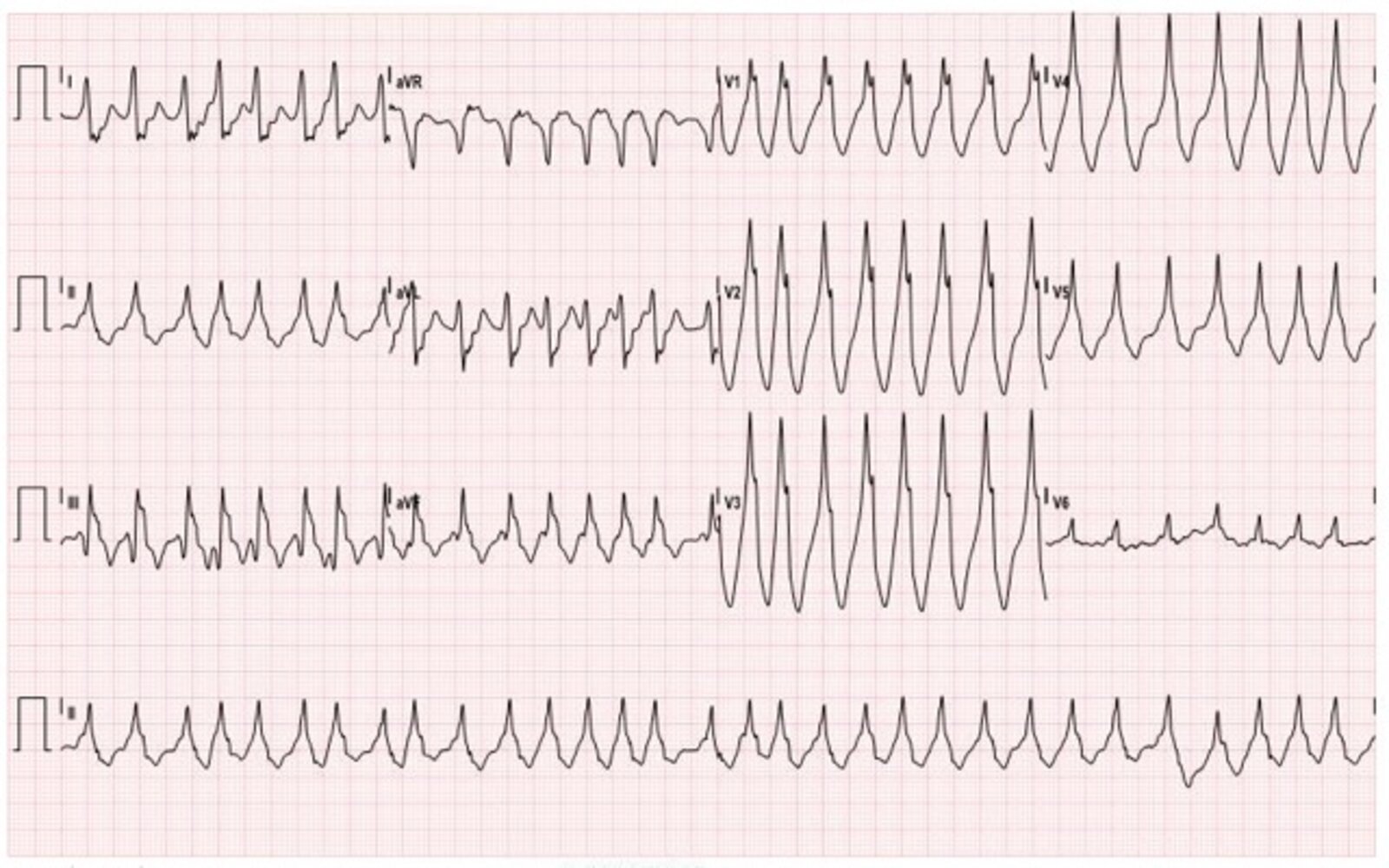
12-lead ECG (paper speed: 25 mm/s) of a patient presenting with palpitations
– Irregularly irregular rhythm
– Rate ∼185/min
– Normal axis (R > S in leads I and aVF)
– No P waves visible
– Wide, polymorphic QRS complexes
Atrial fibrillation is a common complication of WPW syndrome, resulting in an irregular, wide-complex tachycardia with polymorphic QRS complexes. The patient was treated with IV procainamide and converted to sinus rhythm, revealing the characteristic ECG features of WPW syndrome (see repeat ECG 2/2).
Source: “Fig. 1, in: Wolff-Parkinson-White Syndrome: Electrocardiogram” by Miner B, Patane J, Chandwani C, JETem, licensed under CC BY 4.0.
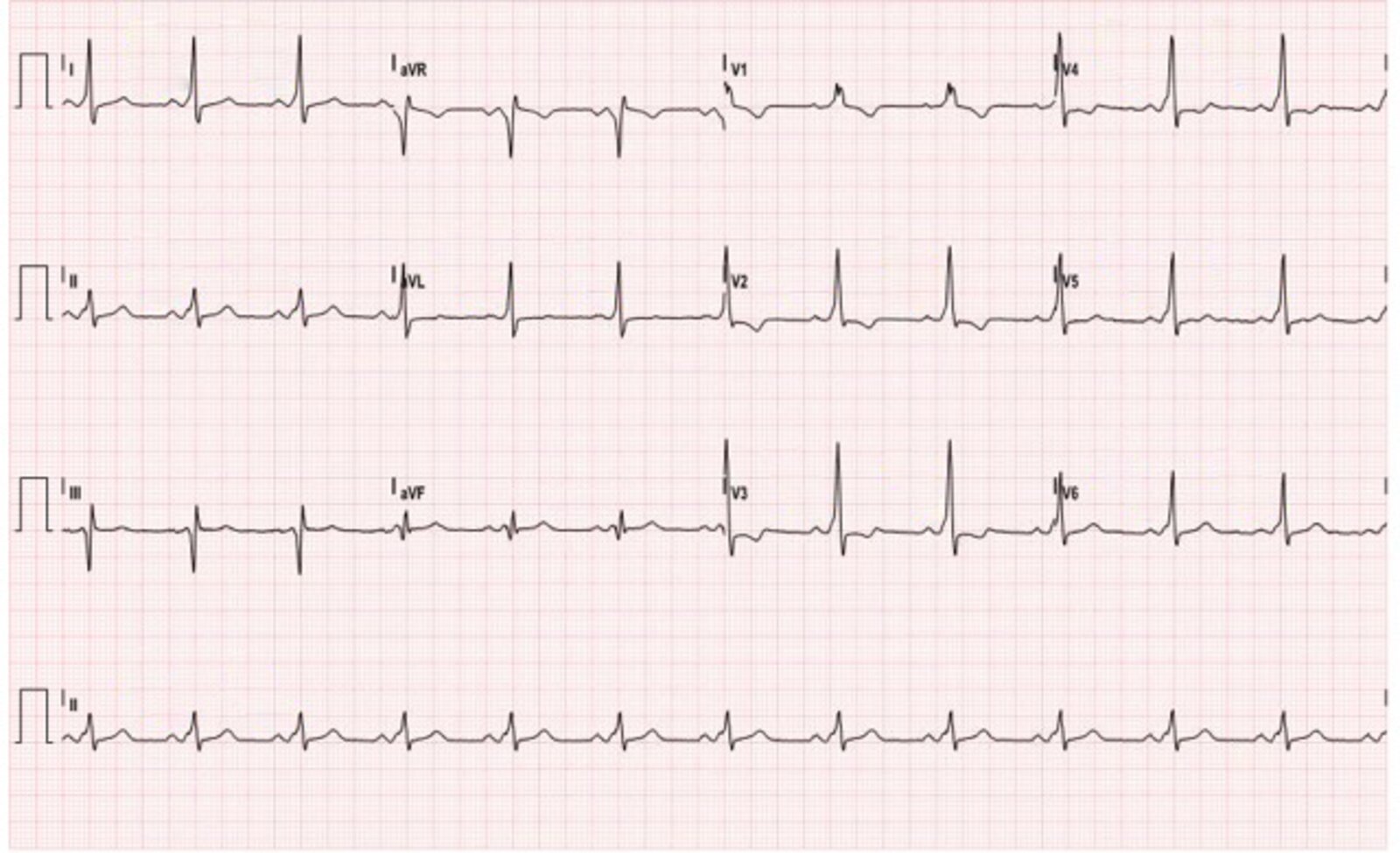
Repeat 12-lead ECG (paper speed: 25 mm/s) of a patient who initially presented with an irregular wide-complex tachycardia (see 1/2) after treatment with IV procainamide.
– Regular sinus rhythm
– Rate ∼75/min
– Normal axis (R > S in leads I and aVF)
– PR interval ∼120 ms (low end of normal range)
– Wide QRS complexes (∼160ms) with delta waves (the slurred initial upstroke of the QRS complex; examples indicated by arrows)
Procainamide terminated the atrial fibrillation seen in this patient's initial ECG (1/2) and revealed the characteristic ECG findings of Wolff-Parkinson-White (WPW) syndrome seen here: widened QRS complexes with delta waves and a short PR interval.
Source: “Fig. 4, in: Wolff-Parkinson-White Syndrome: Electrocardiogram” by Miner B, Patane J, Chandwani C, JETem, licensed under CC BY 4.0. Modifications: arrows removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Focal atrial tachycardia
Definition
- Focal atrial tachycardia (FAT; focal AT): a supraventricular tachycardia that arises from a localized atrial focus outside of the SA node [2]
- Atrial tachycardia (AT): an umbrella term for focal atrial tachycardia and multifocal atrial tachycardia (MAT) that is often used synonymously with focal atrial tachycardia
Etiology [15]
- Idiopathic: most common
- Chronic conditions: hypertension, heart disease, cardiomyopathy
- Acute conditions: myocardial infarction, infection, alcohol poisoning
-
Drug toxicity
- Digoxin (most common)
- Theophylline
- Cocaine
Pathophysiology [43][44]
-
Possible mechanisms [45]
- Triggered activity: a result of early afterdepolarizations (EAD) or delayed afterdepolarization (DAD)
- Microreentry: slow conduction at discrete regions of fibrotic cardiac tissue
- Enhanced automaticity: acceleration of a normal automatic pacemaker [46]
-
Key features
- Originates outside of the SA node
- Abrupt onset
- Can be sustained or nonsustained
- Worsened by adrenergic activity
ECG findings in focal AT [2][46]
- Heart rate 100–250/minute [46]
- Regular rhythm
- Can have 1:1 or 2:1 AV conduction
-
P wave
- Typically visible in 2:1 AT
- May be hidden by the QRS complex or T wave in 1:1 AT
- The morphology depends on the site of origin but remains constant.
- An isoelectric baseline is present between P waves.
-
QRS complex: morphology does not vary
- Narrow complex: most common
- Wide QRS complex may be present in SVT with aberrant conduction.
An isoelectric baseline between P waves can help distinguish focal AT from atrial flutter. [8]

Treatment of focal AT [2]
Acute episodes
Episodes of focal atrial tachycardia are most commonly self-limiting and asymptomatic, in which case they do not require treatment.
- Unstable tachycardia with a pulse: electrical cardioversion
-
Stable
-
Narrow QRS complex
- First step: vagal maneuvers
-
If SVT persists: intravenous medical therapy
- First-line if there are no contraindications to adenosine and diagnosis of focal AT is not established: adenosine
- First-line if diagnosis of focal AT is established: calcium channel blockers (e.g., verapamil, diltiazem) or beta blockers (e.g., metoprolol)
- See “Management of undifferentiated SVT” for details.
-
Wide QRS complex (suspected aberrant conduction)
- Preexcited focal AT ruled out: AV nodal blocking agents are generally safe.
- Preexcited focal AT possible: Avoid AV nodal blocking agents.
- See “Stable, wide-complex tachycardia” for details.
-
Narrow QRS complex
- All patients: Identify and treat acute reversible underlying conditions (see “Etiology”).
Avoid AV nodal blockers in patients with preexcited focal atrial tachycardia (e.g., due to WPW) because they can trigger ventricular arrhythmias.
Long-term management
- Catheter ablation: for symptomatic patients who are candidates (e.g., refractory AT, younger age, focal atrial tachycardia-induced cardiomyopathy) or those who prefer it as an alternative to pharmacotherapy [47][48]
-
Pharmacotherapy
- Beta blockers: e.g., metoprolol
- CCBs: verapamil OR diltiazem
- A cardiology consultation is required if the following medications are being considered:
- Class Ic antiarrhythmic drugs : flecainide OR propafenone
- Class III antiarrhythmic drugs : amiodarone OR sotalol
- Pacemaker implantation: Consider for patients with refractory symptoms after unsuccessful invasive and medical therapy.
- Surgery (e.g., left atrial isolation): less common since the advancement of catheter ablation [49]
-
Other
- Management of underlying conditions (see “Etiology”)
- Anticoagulation: not indicated in the absence of coexisting arrhythmia.
12-lead ECG (paper speed: 25 mm/s)
- Two periods of sinus rhythm (varying between 79–85/min; black interval lines) alternating with two periods of tachycardia (∼ 137/min; dashed black interval lines)
- P-wave morphology and axis during tachycardia (red overlay) are different from those during sinus rhythm (blue overlay). During the periods of tachycardia, the P waves remain constant, indicating a single ectopic focus.
- 1:1 AV conduction
- QRS morphology remains normal throughout.
- Normal QRS axis (R > S in I and aVF)
- An isoelectric baseline is present.
These features are suggestive of focal atrial tachycardia.
Source: “Fig. 2, Twelve-lead ECG at presentation, in: Incessant Focal Atrial Tachycardia Leading to Tachycardiomyopathy” by Bhasin D, Arora G, Gupta A, Isser HS, Bansal S, Cureus, licensed under CC BY 4.0. Modifications: arrows removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Multifocal atrial tachycardia
Definition
- An irregular SVT featuring ≥ 3 morphologies of P waves [2]
Etiology [50][51]
- Severe underlying conditions (e.g., heart failure and pulmonary diseases, such as COPD or pneumonia)
- Drugs (e.g., theophylline, isoproterenol) [52]
- Electrolyte abnormalities (e.g., hypokalemia, hypomagnesemia)
- Other: hypoxia, hypercapnia, acidosis, dysautonomia
Pathophysiology [53]
- Multifocal origin of pacemaker activity
- Mechanism remains unclear [50]
- Often associated with right atrial enlargement
ECG findings in MAT [50]
- Heart rate 100–200/minute
- Irregularly irregular rhythm
-
P waves
- Three or more varying morphologies
- Separated by an isoelectric baseline
- Variable PR interval
-
QRS complex: morphology does not vary
- Narrow QRS complex: most common
- Wide QRS complex may be present in aberrant conduction
- May progress to atrial fibrillation
Do not confuse MAT with atrial fibrillation. In Afib, there are no distinct or organized P waves, whereas in MAT there are distinct P waves with varying morphologies.
Unlike in atrial flutter, in MAT there are distinct isoelectric intervals between P waves.

Treatment of multifocal atrial tachycardia [2][11][54]
Treatment of MAT is challenging and specialists should be involved early. Patients often have severe underlying conditions and rhythm control and electrical cardioversion are not effective. For clinically-oriented management algorithms for patients with tachycardia, see “Management of tachycardia”.
-
First-line treatment: management of underlying causes [55]
- Manage exacerbations of chronic diseases (see “Etiology” above).
- Correct reversible conditions, e.g., hypoxemia, acidosis, electrolyte abnormalities.
- See “Potassium replacement” and “Magnesium replacement.”
- Discontinue potential offending medications.
- IV magnesium may be helpful even in patients with normal magnesium levels. [17]
-
Rate control
- Beta blockers: e.g., metoprolol
- Calcium channel blockers : verapamil
- AV node radiofrequency ablation: Consider in refractory MAT.
Avoid AV nodal blockers in patients with preexcited MAT (e.g., due to WPW) because of the risk of ventricular arrhythmias.
Avoid electrical cardioversion and antiarrhythmic drugs (e.g., procainamide, lidocaine, phenytoin), as they are not effective in treating MAT. [2][54]
12-lead ECG (paper speed: 25 mm/s)
– Heart rate ∼ 160/min
– Irregularly irregular rhythm with wide variation in RR intervals (overlay) and variable PP, PR, and QT intervals
– ≥ P wave morphologies in the same lead (marked in rhythm strip II: normal, inverted, biphasic)
– Isoelectric baseline between P waves
– Narrow QRS complexes with similar morphology throughout
An irregularly irregular tachycardia with an isoelectric baseline and ≥ 3 distinct P wave morphologies in a single lead is consistent with multifocal atrial tachycardia.
Source: “Multifocal atrial tachycardia - MAT” by Jer5150, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
Junctional tachycardia
Definition
- A tachyarrhythmia caused by abnormal automaticity of myocytes in the AV node and bundle of His
- There are two possible presentations.
- Paroxysmal junctional tachycardia (PJT): sudden onset, rapid tachycardia (heart rate > 100/minute)
- Accelerated AV junctional rhythm (nonparoxysmal junctional tachycardia): gradual onset (and termination) rhythm, which can cause a mild tachycardia (heart rate ∼ 60–100/minute)
Etiology [2]
-
Paroxysmal junctional tachycardia
- Most commonly seen in infants with congenital heart disease
- Following myocardial infarction
- Transiently during slow pathway ablation in AVNRT
-
Accelerated AV junctional rhythm [11]
- Digoxin toxicity
- Catecholamine use [56]
- COPD
- Hypokalemia
Pathophysiology [2][11]
- Caused by an ectopic focus of abnormal automaticity in the AV node or the proximal bundle of His
ECG findings in junctional tachycardia [2][57]
While the rate varies between paroxysmal junctional tachycardia and accelerated AV junctional rhythm, the ECG appearance is otherwise similar.
-
Heart rate
- PJT: > 100/minute
- Accelerated AV junctional rhythm: typically ∼ 60–100/minute
- Narrow QRS complex
- Regular (occasionally may be irregular)
-
P wave is inverted in lead II and can be:
- Hidden within the QRS complex
- Immediately before the QRS complex
- Immediately after the QRS complex
- Short PR interval

Treatment of junctional tachycardia [2]
These recommendations are for confirmed junctional tachycardia. For clinically-oriented management algorithms for patients with tachycardia, see “Management of tachycardia.”
-
Acute episodes: intravenous pharmacotherapy
- Beta blockers (e.g., metoprolol )
- Nondihydropyridine CCBs (e.g., verapamil )
-
Long-term management [2]
- Accelerated AV junctional rhythm: Identify and treat the underlying cause (e.g., digoxin toxicity).
-
Paroxysmal junctional tachycardia: medical therapy (e.g., nondihydropyridine CCBs, beta blockers)
- If there is no structural heart disease, consider flecainide OR propafenone. [2]
- Nondihydropyridine CCBs: verapamil OR diltiazem [2]
- Beta blockers: propranolol OR metoprolol [2]
- Catheter ablation: Consider in selected patients with PJT.
12-lead ECG (paper speed: 25 mm/s)
- Regular rhythm
- Heart rate: ∼ 130/min
- P waves immediately follow the QRS complexes (examples indicated with green arrowheads) and are inverted in I, II, aVF, and V4–V6 (retrograde P waves; examples indicated with red arrowheads).
- Cardiac axis borderline normal/right axis deviation (isoelectric in I, R > S in aVF)
- Narrow QRS complexes (∼80 ms)
- Persistent S wave
A regular, narrow complex tachycardia with retrograde P waves is suggestive of junctional tachycardia.
Source: “Junctional Tachycardia” by James Heilman, MD, Wikimedia Commons, licensed under CC BY-SA 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 4.0.
External Resources
References
- Page RL, Joglar JA, Caldwell MA, et al. "2015 ACC/AHA/HRS Guideline for the Management of Adult Patients With Supraventricular Tachycardia". Circulation. 133(14). :e506–e574. (2016)
- Brugada J, Katritsis DG, Arbelo E, et al. "2019 ESC Guidelines for the management of patients with supraventricular tachycardiaThe Task Force for the management of patients with supraventricular tachycardia of the European Society of Cardiology (ESC)". Eur Heart J. 41(5). :655-720. (2019)
- Lundqvist CB, Potpara TS, Malmborg H. "Supraventricular Arrhythmias in Patients with Adult Congenital Heart Disease". Arrhythm Electrophysiol Rev.. 6(2). :42. (2017)
- Papadopoulos CH, Oikonomidis D, Lazaris E, Nihoyannopoulos P. "Echocardiography and cardiac arrhythmias". Hellenic J Cardiol. 59(3). :140-149. (2018)
- Wang PJ, Estes NAM. "Supraventricular Tachycardia". Circulation. 106(25). (2002)
- Walls R, Hockberger R, Gausche-Hill M. "Rosen's Emergency Medicine". Elsevier Health Sciences. (2018). ISBN: 9780323354790
- Tisdale JE, Chung MK, Campbell KB, et al. "Drug-Induced Arrhythmias: A Scientific Statement From the American Heart Association.". Circulation. 142(15). :e214-e233. (2020)
- Desforges JF, Kastor JA. "Multifocal Atrial Tachycardia". N Engl J Med. 322(24). :1713-1717. (1990)
- Wang K. "Multifocal Atrial Tachycardia". Arch Intern Med. 137(2). :161. (1977)
- Bittar G, Friedman HS. "The Arrhythmogenicity of Theophylline". Chest. 99(6). :1415-1420. (1991)
- Santos-Ocampo CD, Sadaniantz A, Elion JL, et al. "Echocardiographic assessment of the cardiac anatomy in patients with multifocal atrial tachycardia: a comparison with atrial fibrillation.". Am J Med Sci. 307(4). :264-8. (1994)
- Kastor JA. "Multifocal Atrial Tachycardia". Card Electrophysiol Rev. 1(1/2). :71-75. (1997)
- Iseri LT, Fairshter RD, Hardemann JL, Brodsky MA. "Magnesium and potassium therapy in multifocal atrial tachycardia". Am Heart J. 110(4). :789-794. (1985)
- Neumar RW, Otto CW, Link MS, et al. "Part 8: Adult Advanced Cardiovascular Life Support: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care". Circulation. 122(18_suppl_3). :S729-S767. (2010)
- Stouffer G, Runge MS, Patterson C. "Netter's Cardiology E-Book". Elsevier Health Sciences. (2010). ISBN: 9781437736502
- Podrid P, MD P, Malhotra R, et al. "Podrid's Real-World ECGs: Volume 4A, Arrhythmias [Core Cases]". Cardiotext Publishing. (2014). ISBN: 9781935395263
- Munro J, Shen W-K, Srivathsan K. "Pre-excited tachycardia: Atrial tachycardia with a bystander left lateral accessory pathway". HeartRhythm Case Reports. 2(4). :334-338. (2016)
- H Heidbüchel. "How to ablate typical 'slow/fast' AV nodal reentry tachycardia". Europace. 2(1). :15-19. (2000)
- Alboni P, Tomasi C, Menozzi C, et al. "Efficacy and safety of out-of-hospital self-administered single-dose oral drug treatment in the management of infrequent, well-tolerated paroxysmal supraventricular tachycardia". J Am Coll Cardiol. 37(2). :548-553. (2001)
- Hanna Deschamps E, Hanna EB. "Atrioventricular Accessory Pathways: Mechanisms, Electrocardiograms, and Associated Arrhythmias". South Med J. 109(10). :670-676. (2016)
- Ali R, Tahir A, Nadeem M, Shakhatreh MI, Faulknier B. "Antidromic Atrioventricular Reentry Tachycardia with Wolff Parkinson White Syndrome: A Rare Beast". Cureus. (2018)
- Kylat RI, Samson RA. "Permanent junctional reciprocating tachycardia in infants and Children". J Arrhythm. 35(3). :494-498. (2019)
- Rao BNVR. "Clinical Examinations in Cardiology - E-Book". Elsevier Health Sciences. (2007). ISBN: 9788131231548
- Marini JJ, Wheeler AP. "Critical Care Medicine". Lippincott Williams & Wilkins. (2010). ISBN: 9780781798396
- Jayasinghe R. "ECG workbook - E-Book". Elsevier Health Sciences. (2012). ISBN: 9780729581097
- Roberts-Thomson KC, Kistler PM, Kalman JM. "Focal atrial tachycardia I: clinical features, diagnosis, mechanisms, and anatomic location.". Pacing Clin Electrophysiol. 29(6). :643-52. (2006)
- Kistler PM, Roberts-Thomson KC, Haqqani HM, et al. "P-Wave Morphology in Focal Atrial Tachycardia". J Am Coll Cardiol. 48(5). :1010-1017. (2006)
- Chen SA, Chiang CE, Yang CJ, et al. "Sustained atrial tachycardia in adult patients. Electrophysiological characteristics, pharmacological response, possible mechanisms, and effects of radiofrequency ablation.". Circulation. 90(3). :1262-1278. (1994)
- Buttà C, Tuttolomondo A, Giarrusso L, Pinto A. "Electrocardiographic Diagnosis of Atrial Tachycardia: Classification, P-Wave Morphology, and Differential Diagnosis with Other Supraventricular Tachycardias". Annals of Noninvasive Electrocardiology. 20(4). :314-327. (2014)
- Blomström-Lundqvist C, Scheinman MM, Aliot EM, et al. "ACC/AHA/ESC guidelines for the management of patients with supraventricular arrhythmias--executive summary. a report of the American college of cardiology/American heart association task force on practice guidelines and the European society of cardiology committee for practice guidelines (writing committee to develop guidelines for the management of patients with supraventricular arrhythmias) developed in collaboration with NASPE-Heart Rhythm Society.". J Am Coll Cardiol. 42(8). :1493-531. (2003)
- Medi C, Kalman JM, Haqqani H, et al. "Tachycardia-mediated cardiomyopathy secondary to focal atrial tachycardia: long-term outcome after catheter ablation.". J Am Coll Cardiol. 53(19). :1791-7. (2009)
- Walters TE, Kistler PM, Kalman JM. "Radiofrequency Ablation for Atrial Tachycardia and Atrial Flutter". Heart, Lung and Circulation. 21(6-7). :386-394. (2012)
- Roberts-Thomson KC, Kistler PM, Kalman JM. "Focal atrial tachycardia II: management.". Pacing Clin Electrophysiol. 29(7). :769-78. (2006)
- Chrispin J, Calkins H. "Accessory pathways-related tachycardias: Wolff–Parkinson–White syndrome and atrioventricular reentrant tachycardias". Oxford University Press. :2085-2091. (2018). ISBN: 9780198784906
- Fleisher LA, Roizen MF, Roizen J. "Essence of Anesthesia Practice E-Book". Elsevier Health Sciences. (2017). ISBN: 9780323395410
- Surawicz B, Knilans T. "Chou's Electrocardiography in Clinical Practice E-Book". Elsevier Health Sciences. (2008). ISBN: 9781437711028
- Crawford MH, DiMarco JP, Paulus WJ. "Cardiology E-Book". Elsevier Health Sciences. (2009). ISBN: 9780723436447
- Sidhu J, Roberts R. "Genetic basis and pathogenesis of familial WPW syndrome.". Indian Pacing Electrophysiol J. 3(4). :197-201. (2003)
- Zipes DP. "Braunwald's Heart Disease". Mosby. (2018). ISBN: 9780323463423
- Bergsma D. "Birth Defects Compendium". Springer. (2016). ISBN: 9781349051311
- Saksena S, Camm AJ. "Electrophysiological Disorders of the Heart E-Book". Elsevier Health Sciences. (2011). ISBN: 9781437709711
- Brugada J, Keegan R. "Asymptomatic Ventricular Pre-excitation: Between Sudden Cardiac Death and Catheter Ablation.". Arrhythm Electrophysiol Rev. 7(1). :32-38. (2018)
- Surawicz, B; C. Pratap Reddy, C; Prystowsky, EN. "Tachycardia". Springer Science & Business Media. (2012). ISBN: 9781461328278
- Adelmann GA. "Cardiology Essentials in Clinical Practice". Springer Science & Business Media. (2010). ISBN: 9781849963053
- Ziad I; Mille J. "Clinical Arrhythmology and Electrophysiology: A Companion to Braunwald's Heart Disease". Saunders. (2008). ISBN: 9781416059981
- Aehlert BJ. "ECGs Made Easy - E-Book". Elsevier Health Sciences. (2015). ISBN: 9780323391504
- Rosenbaum, MB; Elizari, MV. "Frontiers of Cardiac Electrophysiology: Volume 19 of Developments in Cardiovascular Medicine". Springer Science & Business Media. (2012). ISBN: 9789400967816
- Edhouse J. "ABC of clinical electrocardiography: Broad complex tachycardia---Part II". BMJ. 324(7340). :776-779. (2002)
- Wesley K. "Huszar's ECG and 12-Lead Interpretation - E-Book". Elsevier Health Sciences. (2016). ISBN: 9780323430104
- Huff J. "ECG Workout". Lippincott Williams & Wilkins. (2006). ISBN: 9780781782302
- Garmel GM. "Wide Complex Tachycardias: Understanding this Complex Condition Part 2 - Management, Miscellaneous Causes, and Pitfall". West J Emerg Med. 9(2). :97-103. (2008)
- Appelboam A, Reuben A, Mann C, et al. "Postural modification to the standard Valsalva manoeuvre for emergency treatment of supraventricular tachycardias (REVERT): a randomised controlled trial". Lancet. 386(10005). :1747-1753. (2015)
- Smith G, Boyle MJ. "The 10 mL syringe is useful in generating the recommended standard of 40 mmHg intrathoracic pressure for the Valsalva manoeuvre". Emerg Med Australas. 21(6). :449-454. (2009)
- Marshall SA, Ruedy J. "On Call Principles and Protocols E-Book". Elsevier Health Sciences. (2010). ISBN: 9780323081290
- Vincent J-L, Abraham E, Kochanek P, Moore FA, Fink MP. "Textbook of Critical Care E-Book". Elsevier Health Sciences. (2011). ISBN: 9781437715682
- Fleisher GR, Ludwig S. "Textbook of Pediatric Emergency Medicine ". Lippincott Williams & Wilkins. (2010). ISBN: 9781605471594
- Tintinalli JE, Stapczynski JS, Ma OJ, et al. "Tintinalli's Emergency Medicine: A Comprehensive Study Guide, 9th edition". McGraw Hill Professional. (2019). ISBN: 9781260019940
- Dale Dubin, MD. "Rapid Interpretation of EKG's". COVER, Inc.. :109. (2000). ISBN: 0912912065
- Al-Khatib SM, Page RL. "Ongoing Management of Patients With Supraventricular Tachycardia". JAMA Cardiology. 2(3). :332. (2017)
- Azeem T, Vassallo M, Samani NJ. "Rapid Review of ECG Interpretation". CRC Press. (2005). ISBN: 9781840765106
- Ferri FF. "Ferri's Clinical Advisor 2020 E-Book". Elsevier Health Sciences. (2019). ISBN: 9780323679770
- Fogoros RN, MD RN. "Electrophysiologic Testing". John Wiley & Sons. (2012). ISBN: 9781118399606
- Field JM. "The Textbook of Emergency Cardiovascular Care and CPR". Lippincott Williams & Wilkins. (2009). ISBN: 9780781788991
- Atlee JL. "Complications in Anesthesia". Elsevier Health Sciences. (2007). ISBN: 9781416022152
- Hollenberg SM, Heitner S. "Cardiology in Family Practice". Springer Science & Business Media. (2011). ISBN: 9781617793851
- Camm AJ, Ward D. "Clinical Aspects of Cardiac Arrhythmias". Springer Science & Business Media. (2012). ISBN: 9789400912892
- Hare M, Ramlakhan S. "Handstands: a treatment for supraventricular tachycardia?". Arch Dis Child. 100(1). :54-56. (2014)
- Bohnen M, Stevenson WG, Tedrow UB, et al. "Incidence and predictors of major complications from contemporary catheter ablation to treat cardiac arrhythmias". Heart Rhythm. 8(11). :1661-1666. (2011)
- Gupta A, Perera T, Ganesan A, et al. "Complications of Catheter Ablation of Atrial Fibrillation". Circulation: Arrhythmia and Electrophysiology. 6(6). :1082-1088. (2013)