Summary
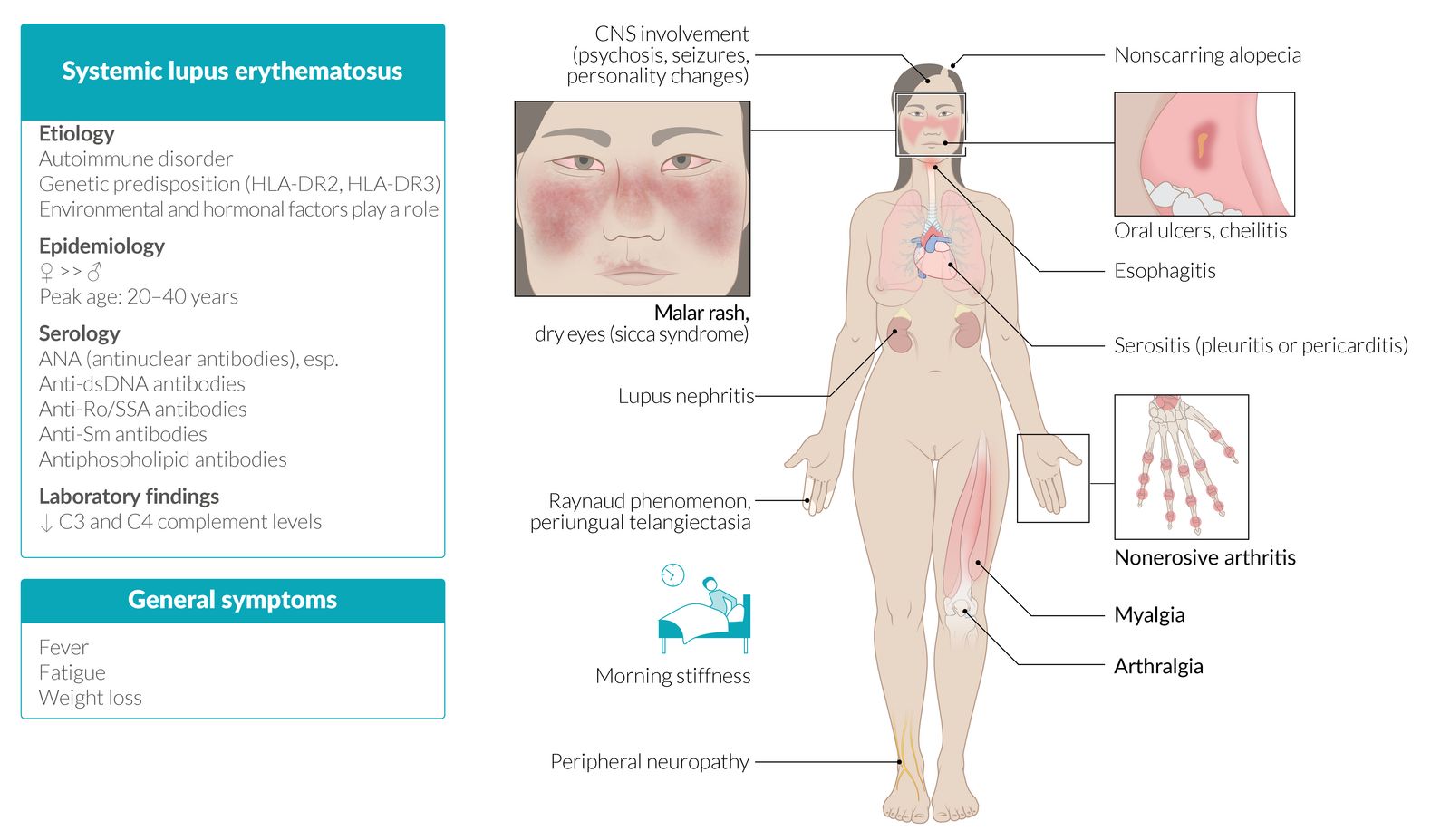
Systemic lupus erythematosus (SLE) is a multisystem autoimmune disease that predominantly affects women of childbearing age and is the most common form of lupus. The exact cause is still unknown, but hormonal and immunological features and genetic predisposition are considered likely etiological factors. Disease presentation is variable but is usually characterized by phases of remission and relapse. Symptoms can range from mild and localized to life-threatening systemic disease. SLE can affect any organ, but typical findings include arthritis, a malar rash (facial butterfly rash), and constitutional symptoms such as fever and fatigue. Involvement of the kidneys is common and can lead to lupus nephritis. Potential manifestations of SLE include cutaneous lupus erythematosus (CLE) and neuropsychiatric systemic lupus erythematosus (NPSLE); however, they can also occur independently from SLE. Other forms of lupus in addition to SLE include drug-induced lupus erythematosus (DILE) and neonatal lupus. The diagnosis of lupus is based on clinical findings and is further supported by laboratory studies, including the presence of antinuclear antibodies (ANAs) and antigen-specific ANAs (i.e., anti-dsDNA, anti-Sm). The 2019 EULAR/ACR classification criteria for SLE do not need to be fulfilled to make a diagnosis but may further support it. Management consists of general measures, such as avoiding sun exposure, and lifestyle modifications for ASCVD prevention. Long-term immunosuppressive therapy depends on disease severity and organ involvement; hydroxychloroquine is typically used, as it has been shown to reduce flares and decrease mortality. In severe cases, additional immunosuppressants (e.g., mycophenolate, azathioprine) or biological agents may be given. Cardiovascular, neurological, and renal disease (lupus nephritis), together with infections, are the main causes of death in patients with SLE.

© AMBOSS
Epidemiology
- Sex: : ♀ > ♂ (10:1) [1]
-
Peak incidence and prevalence [1][2]
- Age of onset
- Women: 15–44 years
- Men: no particular age
- Race: highest in populations of African descent
- Age of onset
Epidemiological data refers to the US, unless otherwise specified.
Etiology
The exact etiology is unknown, but several predisposing factors have been identified.
-
Genetic predisposition [3]
- HLA-DR2 and HLA-DR3 are commonly present in individuals with SLE.
- Genetic deficiency of classical pathway complement proteins (C1q, C2, C4) in approx. 10% of affected individuals
- Hormonal factors: Hyperestrogenic states (e.g., due to oral contraceptive use, postmenopausal hormonal therapy, endometriosis) are associated with an increased risk of SLE. [4]
-
Environmental factors [3][4]
- Cigarette smoking and silica exposure increase the risk of developing SLE.
- UV light and EBV infection may trigger disease flares, but there is insufficient evidence on whether they cause SLE.
- Drugs such as procainamide or hydralazine (see “Drug-induced lupus erythematosus”)
Pathophysiology
The exact pathomechanism of SLE is not fully understood, but the following two processes are the most widely accepted hypotheses: [5]
- Autoantibody development: deficiency of classical complement proteins (C1q, C4, C2) → failure of macrophages to phagocytose immune complexes and apoptotic cell material (i.e., plasma and nuclear antigens) → dysregulated, intolerant lymphocytes targeting normally hidden intracellular antigens → autoantibody production (e.g., ANA, anti-dsDNA)
-
Autoimmune reactions
- Type III hypersensitivity (most common in SLE) → antibody-antigen complex formation in microvasculature → complement activation and inflammation → damage to skin, kidneys, joints, small vessels
- Type II hypersensitivity → IgG and IgM antibodies directed against antigens on cells (e.g., red blood cells) → cytopenia
Clinical features
SLE is a systemic disease characterized by phases of remission and relapse. Some individuals only experience mild symptoms, while others experience severe symptoms and rapid disease progression. SLE can affect any organ.
Common [6]
- Constitutional: : fatigue, fever, weight loss
-
Joints (> 90% of cases) [3]
- Arthritis and arthralgia
- Distal symmetrical polyarthritis: most commonly affects the joints of the fingers, carpal joints, and the knee
-
Skin (85% of cases) [3][7]
- Malar rash (butterfly rash): flat or raised fixed erythema over both malar eminences (nasolabial folds tend to be spared)
- Raynaud phenomenon
- Photosensitivity → maculopapular rash
- Discoid rash
- Oral ulcers (usually painless)
- Nonscarring alopecia (except with discoid rashes)
- Periungual telangiectasia
Both rheumatoid arthritis and SLE arthritis affect the MCP and PIP joints, but SLE does not usually lead to deformities.







Less common [3]
- Hematological: : petechiae; , pallor, or recurrent infections due to cytopenias
- Musculoskeletal: myalgia
- Serositis: : pleuritis and pericarditis → effusions
- Kidneys: nephritis with proteinuria (see “Lupus nephritis”)
-
Heart
- Pericarditis, myocarditis, endocarditis (Libman-Sacks endocarditis)
- Aortic valve lesions
- Coronary artery disease
-
Lungs
- Pneumonitis
- Interstitial lung disease
- Pulmonary hypertension
-
Vascular
- Vasculitis
- Thromboembolism (see “Antiphospholipid syndrome”)
-
Neurological
- Seizures
- Psychosis
- Personality changes
- Lupus cerebritis
- Aseptic meningitis
- Polyneuropathy
- Eyes: keratoconjunctivitis sicca [8]
SLE can cause LSE (Libman-Sacks Endocarditis).

An erythematous macular rash with adherent keratotic scaling is visible over the nasal bridge, cheek (malar eminence), brow, and chin. The rash has spared the nasolabial fold. Mild cheilitis is also visible.
This is the characteristic appearance of the malar rash typically seen in systemic lupus erythematosus. Because this rash typically affects both malar eminences symmetrically, resembling butterfly wings, it is also referred to as a "butterfly rash."
Source: © IMPP

Hyperpigmented areas measuring approx. 3–4 cm are visible over the patient's cheeks with sparing of the nasolabial folds.
This appearance suggests a malar rash, which is typically seen in lupus erythematosus.
Source: “Figure 1, in: Systemic Lupus Erythematosus in India: A Clinico-Serological Correlation” by Mathur, R., Deo, K., Raheja, A., Cureus, licensed under CC BY 4.0.

An erythematous maculopapular rash is visible on the lateral aspect of the arm.
This is the characteristic appearance of the macular rash in systemic lupus erythematosus, and it typically occurs on sun-exposed areas of the skin.
Source: © IMPP

Several sharply-defined, partially confluent, erythematous, annular (discoid) lesions are visible. The center of the lesions appears atrophic. Follicular plugging (hyperkeratotic follicles appearing as white spots within the lesions), and scarred, hyperpigmented borders can also be seen.
These are the characteristic features of discoid lupus erythematosus (DLE), a chronic, scarring variant of cutaneous lupus erythematosus. DLE lesions are typically pruritic and have a propensity to first appear on the face and neck.
Source: © IMPP

Back of a patient with Takayasu arteritis
Several annular (discoid), sharply-demarcated, erythematous lesions can be seen. The center of the lesions appears atrophic.
These are characteristic features of discoid systemic lupus erythematosus.
Source: “Figure 1, in: Takayasu’s Arteritis with Systemic Lupus Erythematosus: A Rare Association” by Dhrubajyoti Bandyopadhyay, Vijayan Ganesan, Debarati Bhar, Diptak Bhowmick, Sibnarayan Sasmal, Cankatika Choudhury, Sabyasachi Mukhopadhyay, Adrija Hajra, Manas Layek, Partha Sarathi Karmakar, Hindawi, licensed under CC BY 3.0.
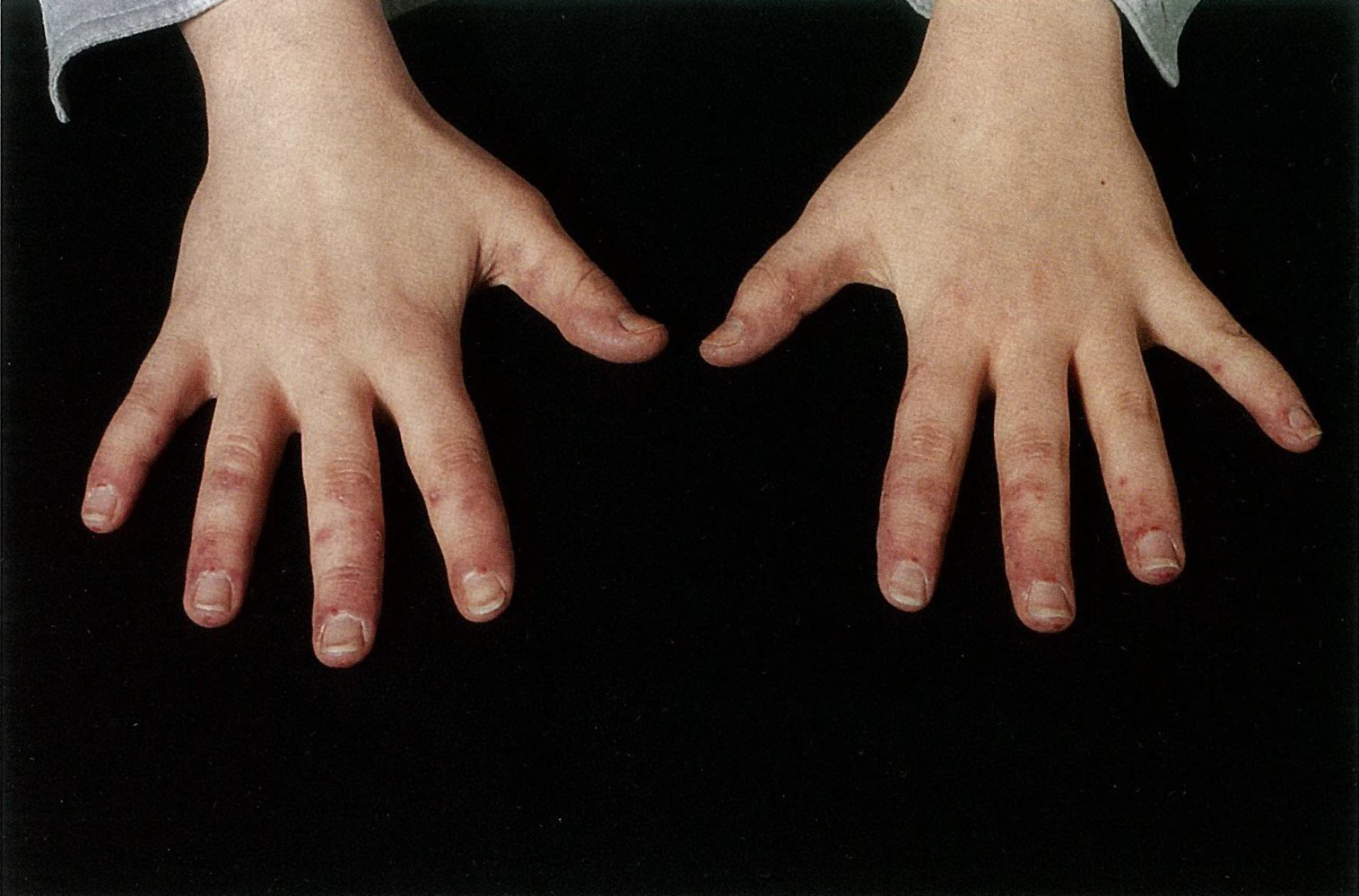
Several dilated capillaries (examples circled) are visible on the periungual skin of the second to fourth fingers of both hands.
These findings are consistent with systemic lupus erythematosus but are also seen in other connective tissue diseases.
Source: © IMPP

21-year old woman with history of SLE and Lupus nephritis
The characteristic butterfly rash, an erythematous, mildly scaly, macular rash with nasolabial sparing on buccal area, is visible (A). Mixed hyperpigmented and hypopigmented scaly skin area on lateral forearm with some erythema consistent with photosensitivity reaction of lupus are visible (B).
Source: “Fig. 1a/b, in: Seizure as an Initial Presentation for Posterior Reversible Encephalopathy Syndrome in Undiagnosed Systemic Lupus Erythematosus and Lupus Nephritis: A Case Report” by Ethan N. Hartman, Kubra Tuna, Elio Monsour, Karthikram Komanduri, Aneta Tarasiuk-Rusek, Cureus, licensed under CC BY 4.0.
Diagnosis
General principles [9][10]
-
SLE is a clinical diagnosis.
- Consider a diagnosis of SLE in patients with constitutional symptoms and features involving ≥ 2 organs or systems.
- Rule out alternative diagnoses to avoid unnecessary and potentially harmful interventions (e.g., immunosuppressants).
- Diagnostic studies support the diagnosis and serve as markers of disease activity and/or organ damage.
- Rheumatology consultation is advised for all patients with suspected SLE.
The 2019 EULAR/ACR classification criteria for SLE may be considered to further support the diagnosis, but do not need to be fulfilled to establish a diagnosis of SLE. [6][9][10]
“SOAP BRAIN, MD:” Serositis, Oral and/or nasal ulcers, Arthritis, Photosensitivity, Blood disorders, Renal involvement, ANAs, Immunological phenomena (anti-dsDNA, anti-Sm, antiphospholipid antibodies), Neurological disorders, and Malar or Discoid rash are the features of SLE.
Laboratory studies [9][10]
The following studies are commonly part of a minimum diagnostic workup if SLE is clinically suspected. [9]
-
Antinuclear antibodies (ANAs)
- Positive titers of ≥ 1:80 have ∼ 98% sensitivity for SLE (entry criterion for the 2019 EULAR/ACR classification criteria for SLE).
- If negative, consider differential diagnoses and/or follow-up with the patient regularly.
-
Antigen-specific ANAs: Request only if ANAs are positive.
-
Anti-dsDNA antibodies
- Autoantibodies against double-stranded DNA
- Positive in 60–70% of patients
- Highly specific for SLE
- Levels correlate with disease activity (especially lupus nephritis activity).
-
Anti-Sm antibodies
- Autoantibodies against Smith antigens (nonhistone nuclear proteins)
- Positive in < 30% of patients, but highly specific for SLE
-
Anti-dsDNA antibodies
- Antiphospholipid antibodies: Screen all patients for antiphospholipid syndrome.
-
Laboratory markers of disease activity and/or organ damage in SLE
- Complement levels: ↓ C3 and/or ↓ C4 in patients with active disease
-
Inflammatory markers [11]
- ESR: may be elevated in patients with active disease
- CRP: often normal (may be elevated in patients with serositis, arthritis, or infections)
- CBC: may show leukopenia, thrombocytopenia, and/or autoimmune hemolytic anemia or anemia of chronic disease
- CMP: may show ↑ BUN and/or creatinine, and/or electrolyte abnormalities
- Urinalysis and urine microscopy: may show proteinuria; , hematuria, and/or urinary casts
ANAs have the highest sensitivity but low specificity for SLE. Anti-dsDNA and anti-Sm antibodies are the most specific antibodies for SLE.
RPR and VDRL are usually used to test for syphilis but may also be positive in SLE.
 casts in urine sediment")
Classification criteria for SLE [6][12]
The classification criteria for SLE were originally developed for research purposes (not as diagnostic criteria). Nevertheless, these criteria are often used in clinical practice to support the diagnosis of SLE.
- Indication: Use in patients who have an ANA titer of ≥ 1:80; (i.e., entry criterion; for the classification criteria). [6]
-
Further considerations
- Consider other, more likely diagnoses before attributing a criterion to SLE.
- Criteria do not need to occur simultaneously.
- The occurrence of any criterion at least once is sufficient.
| 2019 EULAR/ACR classification criteria for SLE [6][12] | ||||
|---|---|---|---|---|
| Domain | Criteria | Weight | ||
| Clinical |
|
|
|
|
|
|
|
||
|
|
|||
|
|
|||
|
|
|
||
|
|
|||
|
|
|||
|
|
|
||
|
|
|||
|
|
|||
|
|
|||
|
|
|
||
|
|
|||
|
|
|
||
|
|
|
||
|
|
|||
|
|
|||
| Immunological |
|
|
|
|
|
|
|
||
|
|
|||
|
|
|
||
SLE classification requires all of the following to be met:
| ||||
Additional diagnostics [9]
Request additional tests based on suspected organ involvement (see also “Specific clinical manifestations” and “Clinical features”).
Imaging studies
Imaging studies can help in the assessment of organ or joint involvement.
- X-ray joints: Perform in patients with articular symptoms.
- X-ray or CT chest: Perform in patients with symptoms of pulmonary involvement (e.g., interstitial lung disease, pleuritis).
- Echocardiography: Consider in patients with suspected pericardial effusion or Libman-Sacks endocarditis.
Histopathology [13]
-
Skin biopsy
- Consider in patients with atypical dermatologic presentation or no response to initial therapy.
- Lupus band test (LBT): a direct immunofluorescence staining technique used to detect immunoglobulin and complement component deposits along the dermoepidermal junction in affected and unaffected skin in patients with SLE [14]
- See also “Cutaneous lupus erythematosus.”
- Kidney biopsy: in case of suspected lupus nephritis
Biopsy of an affected organ (e.g., skin, kidney) can be performed to support the diagnosis but is not required for all patients.

ASCVD risk assessment [9]
- Recommended in all patients with SLE (ASCVD risk-enhancing factor). [10]
- Includes diabetes mellitus screening, screening for lipid disorders, and a risk calculation using the 2013 ACC/AHA pooled cohort equation
Patients with SLE have double the cardiovascular risk compared to patients without SLE. Cardiovascular disease is among the most common causes of death in patients with SLE. [10]
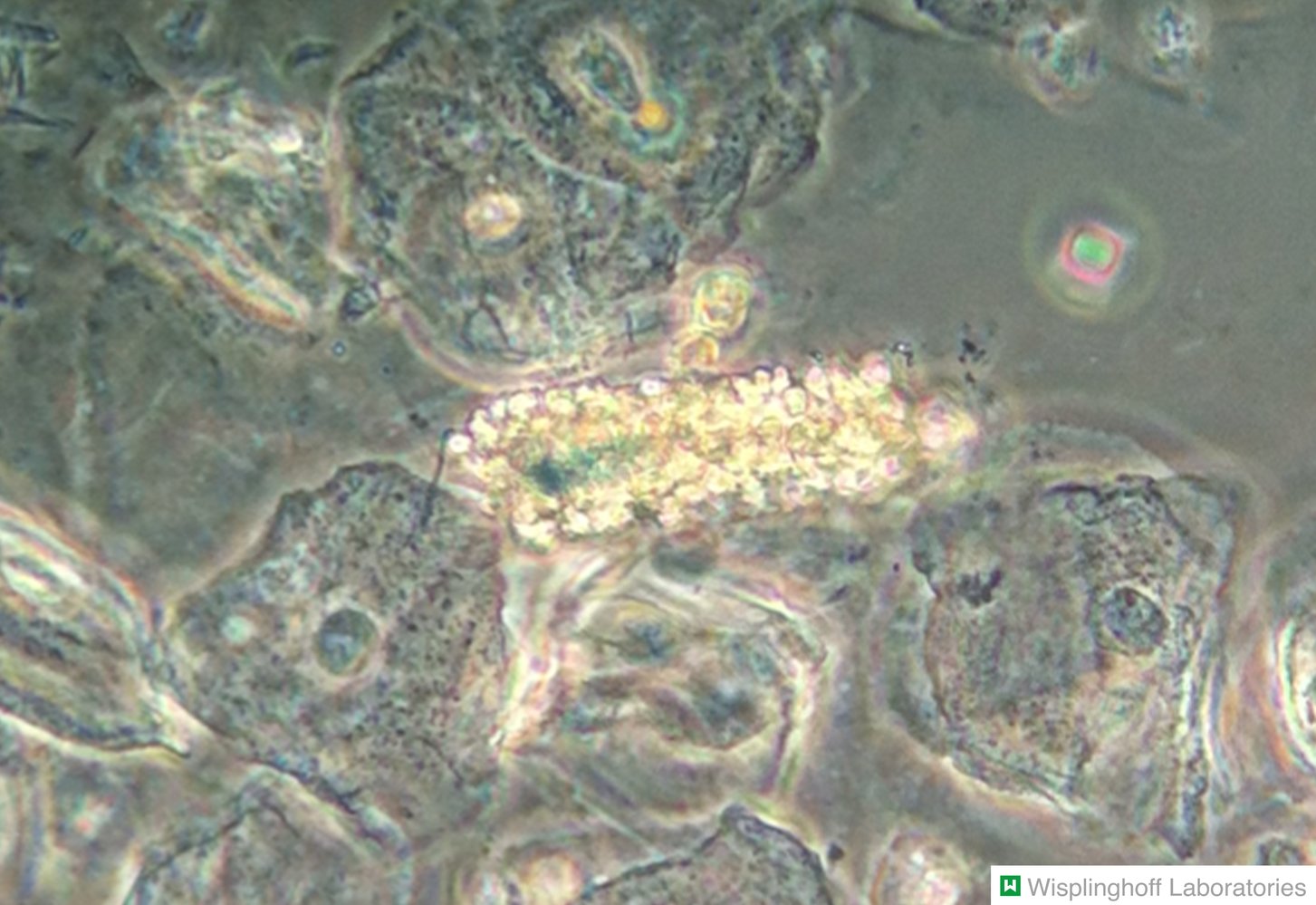
Photomicrograph of urine sediment (phase-contrast microscopy)
A tubular cast (blue overlay) is visible in the center of the image. The cast is composed of numerous RBCs, identifiable by their characteristic biconvex shape (examples outlined in yellow), in a matrix of fibrin and plasma proteins. Several epithelial cells surrounding the RBC cast are also visible.
RBC casts in urinary sediment are typically seen in glomerulonephritis.
Our great thanks to Dr. Wisplinghoff (Dr. Wisplinghoff's laboratory) for kindly providing this image.
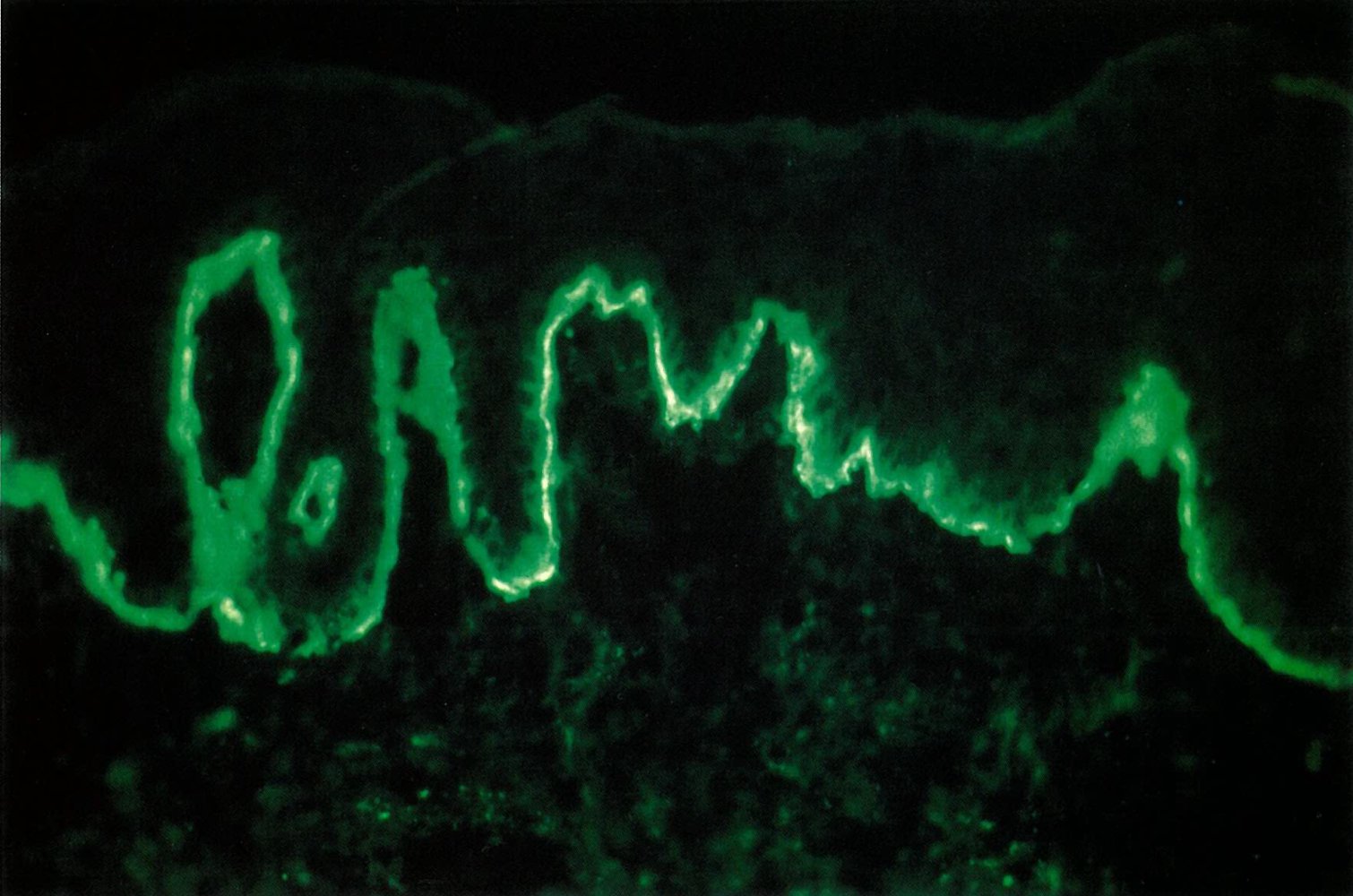
Fluorescence photomicrograph of skin tissue (immunofluorescence staining)
A sharp well-defined band of green immunofluorescence is visible at the dermoepidermal junction.
This indicates a positive lupus band test caused by the deposition of immunoglobulins and complement at the dermoepidermal junction. A positive lupus band test is seen in patients with lupus erythematosus.
Source: © IMPP
Treatment
General principles [10][13][15]
Specialist consultation is advised, i.e., rheumatology and other departments based on the patient's clinical presentation.
-
Patients with SLE usually require life-long immunosuppressants.
- Management is guided by disease severity and the systems or organs affected (see also “Specific clinical manifestations”).
- Patients should be frequently monitored for medication-induced adverse effects.
- NSAIDs can provide symptomatic relief. [9]
- Nonpharmacological measures include:
- Lifestyle modifications for ASCVD prevention (e.g., smoking cessation, aerobic exercise)
- Avoidance of UV light
- If applicable, optimize management of ASCVD and offer preconception counseling (see also “SLE and pregnancy”). [10]
Admit patients with SLE and unexplained fever, severe disease (e.g., lupus nephritis, alveolar hemorrhage, NPSLE), or complications (e.g., sepsis, thrombosis), as these features are associated with increased mortality.
Disease severity
Disease severity can be classified based on the presence of clinical features and laboratory markers of disease activity and/or organ damage in SLE.
- Mild disease (no vital organs affected): e.g., constitutional symptoms, mild arthritis rash and/or cytopenias
- Moderate disease (no vital organs affected): e.g., cutaneous vasculitis, serositis, RA-like arthritis, moderate rash and/or cytopenias , or no response to standard therapy
- Severe or organ-threatening disease: e.g., nephritis, myelitis, pneumonitis, mesenteric vasculitis, severe cytopenias
Management should be guided by disease severity, the patient's safety (e.g., childbearing potential, adverse effects), and medication cost. Therapy may be modified further based on the main organs affected.
Pharmacotherapy [9][12][13]
Depending on the systems or organs affected (e.g., skin, kidneys), a specialist may decide on a different pharmacological approach.
- All patients: Hydroxychloroquine is the cornerstone of therapy (regardless of disease activity). [13][16]
- Mild to moderate disease: (no vital organs affected): Consider the addition of oral glucocorticoids with or without other immunosuppressive agents to achieve remission.
-
Severe or organ-threatening disease
-
Induction therapy
- High-dose IV glucocorticoids and other immunosuppressive agents
- Used until symptom remission or low disease activity is achieved
-
Maintenance of remission
- Hydroxychloroquine with or without lower-dose glucocorticoids
- AND/OR immunosuppressants or biological agents
-
Induction therapy
- Disease flares: Adjust therapy based on the severity of organ involvement.
| Overview of the recommended pharmacological treatment for patients with non-renal SLE [9][13] | ||||
|---|---|---|---|---|
| Disease severity | ||||
| Mild to moderate | Severe | |||
| Standard therapy (for all patients) |
|
|||
| Additional therapy | Glucocorticoids |
|
|
|
| Other immunosuppressive agents |
|
|
||
Prevention and monitoring for medication-induced adverse effects [9][10][13]
- All patients: Offer influenza and pneumococcus immunizations. [9]
-
Glucocorticoids and immunosuppressants
- Consider studies for the diagnosis of latent TB at baseline in selected patients.
- Assess for infection before starting high-dose glucocorticoids.
- Monitor for side effects of glucocorticoid therapy.
- Hydroxychloroquine: request ophthalmologic screening at baseline, after 5 years, and yearly thereafter. [13]
Administer glucocorticoids at the lowest effective dose and only for short periods of time to reduce the risk of adverse effects (e.g., hyperglycemia, atherosclerosis, myopathy).
Offer vaccinations before initiating pharmacological therapy based on the patient's individual risk and potential adverse effects of the prospective agent, and perform laboratory studies.
Specific clinical manifestations
The specific manifestations of SLE are classified based on the systems affected.
Cutaneous lupus erythematosus (CLE)
Some patients with lupus present with predominantly cutaneous manifestations. Cutaneous manifestations are classified based on their chronicity (acute, subacute, or chronic).
Acute cutaneous lupus erythematosus (ACLE) [6][17][18]
- General information: frequently associated with active SLE
- Epidemiology: most common in individuals 20–30 years of age
-
Clinical features
- Malar rash
- Maculopapular rash (also called maculopapular rash of lupus and photosensitive lupus dermatitis)
-
Diagnostics
- Diagnosis is clinical.
- Consider a biopsy in patients with atypical clinical presentation.
- Serum studies
- Positive ANAs in 95% of patients [17]
- Levels of anti-dsDNA and anti-Sm antibodies are often positive.
ACLE is frequently associated with systemic disease.
Subacute cutaneous lupus erythematosus (SCLE) [3][17]
-
General information
- An uncommon variant
- May be associated with systemic disease
-
Clinical features
- Extreme photosensitivity
- Begins as a papular eruption or small scaly plaques that develop into either annular or psoriasiform lesions
- Lesions heal without scarring but may cause hypopigmentation.
- Usually affects the neck, shoulders, and upper limbs, but spares the face
-
Diagnostics
- Based on a combination of patient history, clinical examination, and histology
- Patients often have positive ANAs and anti-Ro/SSA antibodies.


Discoid lupus erythematosus (DLE) [7][17]
-
General information
- Most common form of chronic CLE
- Rarely associated with systemic disease
-
Epidemiology
- ♀ > ♂ (3:1)
- Most common in women 30–50 years of age
-
Clinical features
- Erythematous, inflammatory scaly plaques that are painful to remove
- The plaques heal, but cause scarring alopecia, atrophy, peripheral hyperpigmentation, and central depigmentation.
- Typically affects the face, neck, and head (triggered by exposure to UV light)
-
Diagnostics
- Based on a combination of patient history and clinical examination
- Autoantibodies ; (i.e., ANAs and antigen-specific ANAs) are usually negative.
-
Skin biopsy: Consider in patients with atypical clinical presentation. [13]
- Vacuolar degeneration of basal cells (interface dermatitis) with lymphocytic infiltrates
- Follicular hyperkeratosis or plugging may be seen on the scalp and mucin deposition may be seen in long-standing lesions.
- Lupus band test: can help differentiate DLE from SLE [14]
- Differential diagnosis: For details, see “Overview of annular skin lesions.”
-
Prognosis
- The prognosis for patients with DLE is better than the prognosis for those with SLE.
- The risk of developing SLE is < 10%.
DLE is the most common form of chronic CLE; it is rarely associated with systemic disease.


Management of CLE [9][13]
-
General recommendations
- Wear sunblock with SPF ≥ 50 and protective clothing.
- See also “General principles” in the “Treatment” section.
-
Pharmacological treatment (in consultation with a specialist)
- First-line treatment: Hydroxychloroquine
- PLUS topical glucocorticoids (e.g., fluocinonide) AND/OR topical calcineurin inhibitors (e.g., pimecrolimus) [9][13]
- With or without systemic glucocorticoids (e.g., prednisone)
- Second-line treatment (in consultation with a dermatologist)
- Topical therapy: i.e., intralesional steroids for chronic skin lesions
- Systemic therapy: e.g., methotrexate, retinoids, dapsone, thalidomide, belimumab, or rituximab
- First-line treatment: Hydroxychloroquine
Lupus nephritis
Description [19]
- Most dangerous specific manifestation because of its high morbidity and mortality
- Can manifest as nephritic syndrome and/or nephrotic syndrome; See also "Nephritic-nephrotic syndrome" in “Glomerular diseases."
- Common: found in up to 50% of individuals with SLE at presentation [9]
Pathophysiology [19]
- Mesangial and/or subendothelial deposition of immune complexes (e.g., anti-dsDNA antibodies, anti-Sm antibodies) → expansion and thickening of mesangium, capillary walls, and/or glomerular basement membrane
Clinical features
- Hypertension
- Edema
- Hematuria
Diagnostics [9]
-
Laboratory studies
- BMP: ↑ creatinine
- Urinalysis: proteinuria, hematuria, cellular casts (RBCs, hemoglobin, granular, tubular, or mixed)
- Spot urine protein:creatinine ratio: proteinuria ≥ 0.5 g/g
-
Kidney biopsy
- Indicated in patients with either: [9]
- Unexplained ↑ creatinine
- Proteinuria ≥ 1.0 g/g
- Proteinuria ≥ 0.5 g/g and hematuria or cellular urinary casts
- Findings: immune complex-mediated glomerulonephritis
- Indicated in patients with either: [9]
| Abbreviated histopathologic classification of lupus nephritis [20] | |
|---|---|
| Class I |
|
| Class II |
|
| Class III |
|
| Class IV |
|
| Class V |
|
| Class VI |
|
Perform regular urinalysis follow-up in patients with SLE, as early detection and treatment of renal disease can prevent progression to severe disease.
Management of lupus nephritis [13]
-
General principles
- Consult a nephrologist.
- Induction and maintenance therapy is generally indicated in patients with class III or IV lupus nephritis.
- All patients should receive standard therapy for lupus and individualized management of CKD.
-
Pharmacological management
-
Induction therapy
- IV glucocorticoids (e.g., methylprednisolone)
- PLUS other immunosuppressants (e.g., mycophenolate or cyclophosphamide)
-
Maintenance of remission
- Oral prednisone
- PLUS mycophenolate OR azathioprine
- Refractory or relapsing disease: Rituximab may be considered.
-
Induction therapy
Patients with class I, II, or V lupus nephritis do not usually require specific immunosuppressive therapy. [9][13]
Neuropsychiatric systemic lupus erythematosus (NPSLE) [21]
- Description: the presence of neurological and psychiatric symptoms in patients with SLE that cannot be attributed to another condition [22]
- Epidemiology: found in ∼ 40% of patients with SLE [21]
- Classification: The American College of Rheumatology has identified 19 NPSLE syndromes. [22]
| Neuropsychiatric systemic lupus erythematosus syndromes [22] | |
|---|---|
| Central nervous system | Peripheral nervous system |
|
|
-
Diagnostics [21]
- General principles
- Rule out other common etiologies (e.g., infections, malignancy, adverse drug effects).
- Consult a neurologist if NPSLE is suspected.
- Imaging studies
- First-line studies: MRI brain (T1/T2-weighted) may detect NPSLE and also rule out other neurosurgical lesions and infections.
- Consider other studies (e.g., EEG, SPECT) depending on clinical features.
-
Laboratory studies
- CSF examination: Request for patients with a suspected neurological infection.
- Serology: antiphospholipid antibodies, ANAs
- See also the “Diagnostics” section.
- General principles
-
Treatment: depends on the underlying cause [21]
- Antithrombotic and/or antiplatelet therapy for ischemic, embolic, or thrombotic manifestations
- Immunosuppressive treatment for inflammatory manifestations: See also the “Treatment” section.
An erythematous macular rash with adherent keratotic scaling is visible over the nasal bridge, cheek (malar eminence), brow, and chin. The rash has spared the nasolabial fold. Mild cheilitis is also visible.
This is the characteristic appearance of the malar rash typically seen in systemic lupus erythematosus. Because this rash typically affects both malar eminences symmetrically, resembling butterfly wings, it is also referred to as a "butterfly rash."
Source: © IMPP
Hyperpigmented areas measuring approx. 3–4 cm are visible over the patient's cheeks with sparing of the nasolabial folds.
This appearance suggests a malar rash, which is typically seen in lupus erythematosus.
Source: “Figure 1, in: Systemic Lupus Erythematosus in India: A Clinico-Serological Correlation” by Mathur, R., Deo, K., Raheja, A., Cureus, licensed under CC BY 4.0.
An erythematous maculopapular rash is visible on the lateral aspect of the arm.
This is the characteristic appearance of the macular rash in systemic lupus erythematosus, and it typically occurs on sun-exposed areas of the skin.
Source: © IMPP

Symmetrical erythematous plaques are visible on the lateral aspect of the arm, shoulder, and torso. These annular plaques are well-circumscribed and scaly.
The appearance of this psoriasiform rash in subacute cutaneous lupus erythematosus is often triggered by exposure to UV light. It typically affects the neckline, upper back, arms, and scalp, but spares the face.
Source: © IMPP

Numerous partially confluent erythematous macules and plaques are visible over the entire upper back of this patient.
Source: © IMPP
Several sharply-defined, partially confluent, erythematous, annular (discoid) lesions are visible. The center of the lesions appears atrophic. Follicular plugging (hyperkeratotic follicles appearing as white spots within the lesions), and scarred, hyperpigmented borders can also be seen.
These are the characteristic features of discoid lupus erythematosus (DLE), a chronic, scarring variant of cutaneous lupus erythematosus. DLE lesions are typically pruritic and have a propensity to first appear on the face and neck.
Source: © IMPP

Multiple annular (discoid), sharply demarcated, erythematous plaques, 0.5–3 cm in diameter with central atrophy and scaling are visible underneath the right ear. Additional scaly plaques are located on the lobe, helix, and antihelix of the ear.
These are the characteristic features of discoid lupus erythematosus (DLE), a chronic, scarring variant of cutaneous lupus erythematosus. DLE lesions are typically pruritic and have a propensity to first appear on the face and neck.
Source: © IMPP
Back of a patient with Takayasu arteritis
Several annular (discoid), sharply-demarcated, erythematous lesions can be seen. The center of the lesions appears atrophic.
These are characteristic features of discoid systemic lupus erythematosus.
Source: “Figure 1, in: Takayasu’s Arteritis with Systemic Lupus Erythematosus: A Rare Association” by Dhrubajyoti Bandyopadhyay, Vijayan Ganesan, Debarati Bhar, Diptak Bhowmick, Sibnarayan Sasmal, Cankatika Choudhury, Sabyasachi Mukhopadhyay, Adrija Hajra, Manas Layek, Partha Sarathi Karmakar, Hindawi, licensed under CC BY 3.0.
Fluorescence photomicrograph of skin tissue (immunofluorescence staining)
A sharp well-defined band of green immunofluorescence is visible at the dermoepidermal junction.
This indicates a positive lupus band test caused by the deposition of immunoglobulins and complement at the dermoepidermal junction. A positive lupus band test is seen in patients with lupus erythematosus.
Source: © IMPP

© Massachusetts Medical Society. All rights reserved. AMBOSS SE, exclusive licensee.
Photomicrograph of urine sediment (phase-contrast microscopy)
A tubular cast (blue overlay) is visible in the center of the image. The cast is composed of numerous RBCs, identifiable by their characteristic biconvex shape (examples outlined in yellow), in a matrix of fibrin and plasma proteins. Several epithelial cells surrounding the RBC cast are also visible.
RBC casts in urinary sediment are typically seen in glomerulonephritis.
Our great thanks to Dr. Wisplinghoff (Dr. Wisplinghoff's laboratory) for kindly providing this image.
Differential diagnoses
Drug-induced lupus erythematosus (DILE) [9][23]
- Description: : lupus-like symptoms triggered by medication
-
Epidemiology
- ♂ = ♀
- DILE accounts for ∼ 10% of all SLE cases.
- Most common in white populations
- Most common in individuals 50–70 years of age
-
Etiology
- Genetic susceptibility
- Presence of a genetic mutation that causes decreased acetyltransferase activity, which results in the slow acetylation of drugs
- Presence of HLA-DR2, HLA-DR3, HLA-DR4, or an unexpressed C4 complement allele
- Drug triggers [23]
- High risk: procainamide and hydralazine
- Low risk: sulfa drugs; and certain nonsulfa drugs, (e.g., isoniazid, methyldopa, minocycline, phenytoin, TNF-α inhibitors)
- Genetic susceptibility
-
Clinical features (usually manifest ≥ 1 month after medication initiation)
- Constitutional: fatigue, fever, and weight loss
- Musculoskeletal: myalgia and symmetrical polyarthralgia
- Skin lesions (e.g., malar rash)
- Serositis
-
Diagnostics [9][23]
- ANAs are positive in nearly all patients.
-
Antihistone antibodies
- Antihistone antibodies are seen in 90–95% of patients.
- Nonspecific: They may also be present in ∼ 75% of patients with SLE.
- Anti-dsDNA antibodies: uncommon in patients with DILE
-
Treatment
- Stop the triggering drug.
- If necessary, start temporary pharmacotherapy (see the “Treatment” section).
- Prognosis: Most cases resolve within a few weeks after the causative medication has been discontinued.
“My Two HIPS”: Methyldopa/Minocycline, TNF-α inhibitors, Hydralazine, Isoniazid, Procainamide/Phenytoin, and Sulfa drugs are triggers for DILE.
DILE can manifest with various features that are also seen in idiopathic SLE (e.g., fever, arthritis, malar rash, serositis) but typically does not affect the CNS or kidneys, unlike SLE.
Undifferentiated connective tissue disease (UCTD)
- Definition: a term used to describe a clinical entity that manifests with features of autoimmunity without fulfilling the criteria for any specific connective tissue disease
-
Classification criteria [24]
- Clinical features that suggest a systemic autoimmune disease
- Positive ANAs on two separate occasions
- Disease duration of ≥ 3 years
-
Approach to management [24]
- Provide the patient with clear information on the diagnosis.
- Refer to a rheumatologist for periodical follow-up.
- No specific therapy is required; consider symptomatic management.
- Prognosis: Up to 25% of patients with UCTD progress to an identifiable systemic autoimmune disease within 1–3 years. [24]
In patients with UCTD, the presence of serositis, fever, and/or anti-Sm or anti-dsDNA antibodies has been associated with progression to SLE. [25]
The differential diagnoses listed here are not exhaustive.
Special patient groups
SLE and pregnancy
-
General [26][27]
- While fertility is not affected by SLE, it may be affected by immunosuppressive drugs.
- Pregnancy may trigger flares in disease activity.
- Increased severity of maternal disease correlates with increased risk of maternal and fetal complications during pregnancy (see “Complications” below).
-
Risk assessment [26][27]
- Cardiac, lung, and kidney screening [27]
- Serological profile
- Anti-Ro/SSA and anti-La/SSB are associated with an increased risk of neonatal lupus.
- Anticardiolipin antibodies and lupus anticoagulant: ↑ risk of miscarriage and thrombosis-related complications (see “Antiphospholipid syndrome”)
-
Management [15][27]
- Pregnancy planning and counseling [26]
- Medical treatment should not be discontinued but the drug regimen may be changed.
- Preconception, pregnancy, and breastfeeding: hydroxychloroquine and/or azathioprine
- Disease flares: hydroxychloroquine and/or prednisolone
- Low-dose aspirin from 12 weeks' gestation reduces the risk of preeclampsia. [27]
- Teratogenic immunosuppressive drugs (e.g., methotrexate, mycophenolate, cyclophosphamide) should be avoided.
-
Complications [27]
- Maternal
- SLE flares
- Hypertension, preeclampsia
- Venous thromboembolism
-
Fetal-neonatal
- Neonatal lupus syndrome
- Miscarriage
- Intrauterine growth restriction
- Fetal AV block [26]
- Preterm delivery
- Maternal
Avoid estrogen-containing hormonal contraceptives in patients with antiphospholipid syndrome because of the increased risk of thrombosis.
Educate patients of reproductive age about contraceptive methods, planned pregnancy, and the potential teratogenic effects of pharmacological treatment.
Neonatal lupus syndrome [26][27]
- General: rare (has a high mortality rate)
- Etiology: associated with the transfer of maternal antibodies (anti-Ro/SSA and anti-La/SSB)
-
Clinical features
- First- to third-degree congenital AV block
- Periorbital or diffuse rash (often presents in the first weeks after birth)
- Cytopenia
- Hepatitis, elevated liver enzymes
-
Diagnostics
-
The following two criteria must be present at birth:
- Antibodies (anti-Ro/SSA or anti-La/SSB) in either the mother or child
- Heart block, characteristic rash, and/or hematologic/hepatic involvement with no identifiable cause in the newborn/fetus
-
The following two criteria must be present at birth:
- Treatment: directed at specific organ involvement
- Prognosis: Symptoms usually resolve within a few months.


Face of a newborn with erythematous rash
Multiple ring-shaped erythematous patches can be seen around the lips, eyelids, and on the forehead. Neither nose or cheeks are affected by the rash.
These findings are typical of neonatal lupus syndrome.
Source: “Fig. 1, in: Neonatal lupus erythematosus: a cutaneous cases based update” by Francesco Savino, Serena Viola, Valentina Tarasco, Emanuela Locatelli, Alberto Ricagni, Paola Coppo, BMC, licensed under CC BY 4.0.
Complications
Infections [13][28]
- Responsible for 25–50% of deaths in patients with SLE [28]
- Most common infections
- Bacterial: skin, lungs, and urinary tract
- Viral: varicella zoster virus, cytomegalovirus, and human papillomavirus
Patients with SLE are at increased risk of developing infections because of disease-related factors (e.g., pancytopenia) and/or immunosuppressive treatment.
Cardiovascular disease [15]
- ↑ Risk of thrombosis; in all patients with SLE (especially if secondary antiphospholipid syndrome is present)
- ↑ Risk of myocardial infarction and stroke because of accelerated atherosclerosis
Other comorbidities [3][29]
- Libman-Sacks endocarditis
- Pancytopenia
- Non-Hodgkin lymphoma [30]
- Osteonecrosis of long-bone epiphyses (e.g., osteonecrosis of the femoral head) [31]
- Interstitial lung disease, pulmonary hypertension
- Medication-induced adverse effects
- Pregnancy-related adverse effects (see “SLE and pregnancy” in “Special patient groups” below)
We list the most important complications. The selection is not exhaustive.
Prognosis
- Mortality: 10-year survival rate is ∼ 90% [3][29]
-
Causes of death [3]
- In early disease
- High disease activity with renal or neurological complications
- Infections due to disease-related factors and immunosuppressive therapy
- In late disease
-
Cardiovascular disease [29]
- Complications due to atherosclerosis
- Coronary artery disease
- Most common cause of death in SLE [32]
- End-stage renal disease [19]
- Adverse effects of long-term medication
-
Cardiovascular disease [29]
- In early disease
“Redness In Cheeks” (malar rash): Renal disease, Infections, and Cardiovascular complications are the three most common causes of death in SLE.
Damage to the kidneys or nervous system is associated with a poor prognosis.
External Resources
References
- Stojan G, Petri M. "Epidemiology of systemic lupus erythematosus: an update.". Curr Opin Rheumatol. 30(2). :144-150. (2018)
- "Systemic Lupus Erythematosus (SLE)". https://web.archive.org/web/20200807193142/https://www.cdc.gov/lupus/facts/detailed.html. [2018-10-17]
- Feather A, Randall D, Waterhouse M. "Kumar and Clark's Clinical Medicine". Elsevier. (2020). ISBN: 9780702078682
- Barbhaiya, Costenbader. "Environmental Exposures and the Development of Systemic Lupus Erythematosus". Current Opinion in Rheumatology. 28(5). (2016)
- Aringer M, Costenbader K, Daikh D, et al. "2019 European League Against Rheumatism/American College of Rheumatology Classification Criteria for Systemic Lupus Erythematosus". Arthritis & Rheumatology. 71(9). :1400-1412. (2019)
- Uva L, Miguel D, Pinheiro C, et al. "Cutaneous manifestations of systemic lupus erythematosus". Autoimmune Dis.. 2012. :834291. (2012)
- Shoughy SS, Tabbara KF. "Ocular findings in systemic lupus erythematosus". Saudi Journal of Ophthalmology. 30(2). :117-121. (2016)
- Kiriakidou M, Ching CL. "Systemic Lupus Erythematosus". Ann Intern Med. 172(11). :ITC81-ITC96. (2020)
- Gergianaki I, Bertsias G. "Systemic Lupus Erythematosus in Primary Care: An Update and Practical Messages for the General Practitioner". Front Med (Lausanne). 5. (2018)
- Littlejohn E, Marder W, Lewis E, et al. "The ratio of erythrocyte sedimentation rate to C-reactive protein is useful in distinguishing infection from flare in systemic lupus erythematosus patients presenting with fever". Lupus. 27(7). :1123-1129. (2018)
- Kaul A, Gordon C, Crow MK, et al. "Systemic lupus erythematosus". Nature Reviews Disease Primers. 2(1). (2016)
- Fanouriakis A, Kostopoulou M, Alunno A, et al. "2019 update of the EULAR recommendations for the management of systemic lupus erythematosus". Ann Rheum Dis. 78(6). :736-745. (2019)
- Reich A, Marcinow K, Bialynicki-Birula R. "The lupus band test in systemic lupus erythematosus patients". Ther Clin Risk Manag. 24(7). :27-32. (2011)
- Vu Lam et al. "Systemic Lupus Erythematosus: Primary Care Approach to Diagnosis and Management". American Family Physician. 94(4). :284-294. (2016)
- Ruiz-Irastorza G, Ramos-Casals M, Brito-Zeron P, Khamashta MA. "Clinical efficacy and side effects of antimalarials in systemic lupus erythematosus: a systematic review". Ann Rheum Dis. 69(01). :20-28. (2008)
- Jung JY, Suh CH. "Infection in systemic lupus erythematosus, similarities, and differences with lupus flare". Korean J Intern Med. 32(3). :429-438. (2017)
- Justiz Vaillant AA, Goyal A, Bansal P, et al. "Systemic Lupus Erythematosus (SLE)". StatPearls. (2020)
- Wang LH, Wang WM, Lin SH, Shieh CC. "Bidirectional relationship between systemic lupus erythematosus and non-Hodgkin’s lymphoma: a nationwide population-based study". Rheumatology. 58(7). :1245-1249. (2019)
- Caramaschi P, Biasi D, Dal Forno I, Adami S. "Osteonecrosis in Systemic Lupus Erythematosus: An Early, Frequent, and Not Always Symptomatic Complication". Autoimmune Diseases. 2012. :1-7. (2012)
- Iozza I, Cianci S, Di Natale A, et al. "Update on systemic lupus erythematosus pregnancy". J Prenat Med. 4(4). :67-73. (2010)
- Knight C, Nelson-Piercy C. "Management of systemic lupus erythematosus during pregnancy: challenges and solutions". Open Access Rheumatol. 9. :37-53. (2017)
- Thomas G, Mancini J, Jourde-Chiche N, et al. "Mortality Associated With Systemic Lupus Erythematosus in France Assessed by Multiple-Cause-of-Death Analysis". Arthritis Rheumatol. 66(9). :2503-2511. (2014)
- Rosalie M. Sterner, Stella P. Hartono, and Joseph P. Grande. "The Pathogenesis of Lupus Nephritis". Journal of Clinical and Cellular Immunology. (2014)
- Mok CC, Lau CS. "Pathogenesis of systemic lupus erythematosus". J Clin Pathol. 56(7). :481-490. (2003)
- Okon LG, Werth VP. "Cutaneous Lupus Erythematosus: Diagnosis and Treatment". Best Pract Res Clin Rheumatol. 27(3). :391-404. (2013)
- Aringer M, Leuchten N, Johnson SR. "New Criteria for Lupus". Curr Rheumatol Rep. 22(6). :18. (2020)
- Weening JJ, D’agati VD, et al. "The classification of glomerulonephritis in systemic lupus erythematosus revisited". Kidney Int. 65(2). :521-530. (2004)
- Bertsias GK, Ioannidis JPA, Aringer M, et al. "EULAR recommendations for the management of systemic lupus erythematosus with neuropsychiatric manifestations: report of a task force of the EULAR standing committee for clinical affairs". Ann Rheum Dis. 69(12). :2074-2082. (2010)
- The American College of Rheumatology. "The American College of Rheumatology nomenclature and case definitions for neuropsychiatric lupus syndromes". Arthritis & Rheumatism. 42(4). :599-608. (1999)
- Pretel M, Marquès L, España A. "Drug-Induced Lupus Erythematosus". Actas Dermo-Sifiliogr. (English Edition). 105(1). :18-30. (2014)
- Antunes M, Scirè CA, Talarico R, et al. "Undifferentiated connective tissue disease: state of the art on clinical practice guidelines". RMD Open. 4(Suppl 1). :e000786. (2019)
- West SG. "Rheumatology Secrets". Elsevier Mosby. (2014). ISBN: 9780323037006