Quick guide
Diagnostic approach
- Targeted clinical evaluation
- TWIST score
- POCUS and/or duplex US of scrotum
- Urinalysis
 score")
Red flag features
- Sudden, severe, unilateral testicular pain
- High-riding testis
- Transverse lie of testis
- Absent cremasteric reflex
- Negative Prehn sign
- TWIST score ≥ 6
Management checklist
- Analgesia
- Consult urology.
- Consider manual testicular detorsion.

This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
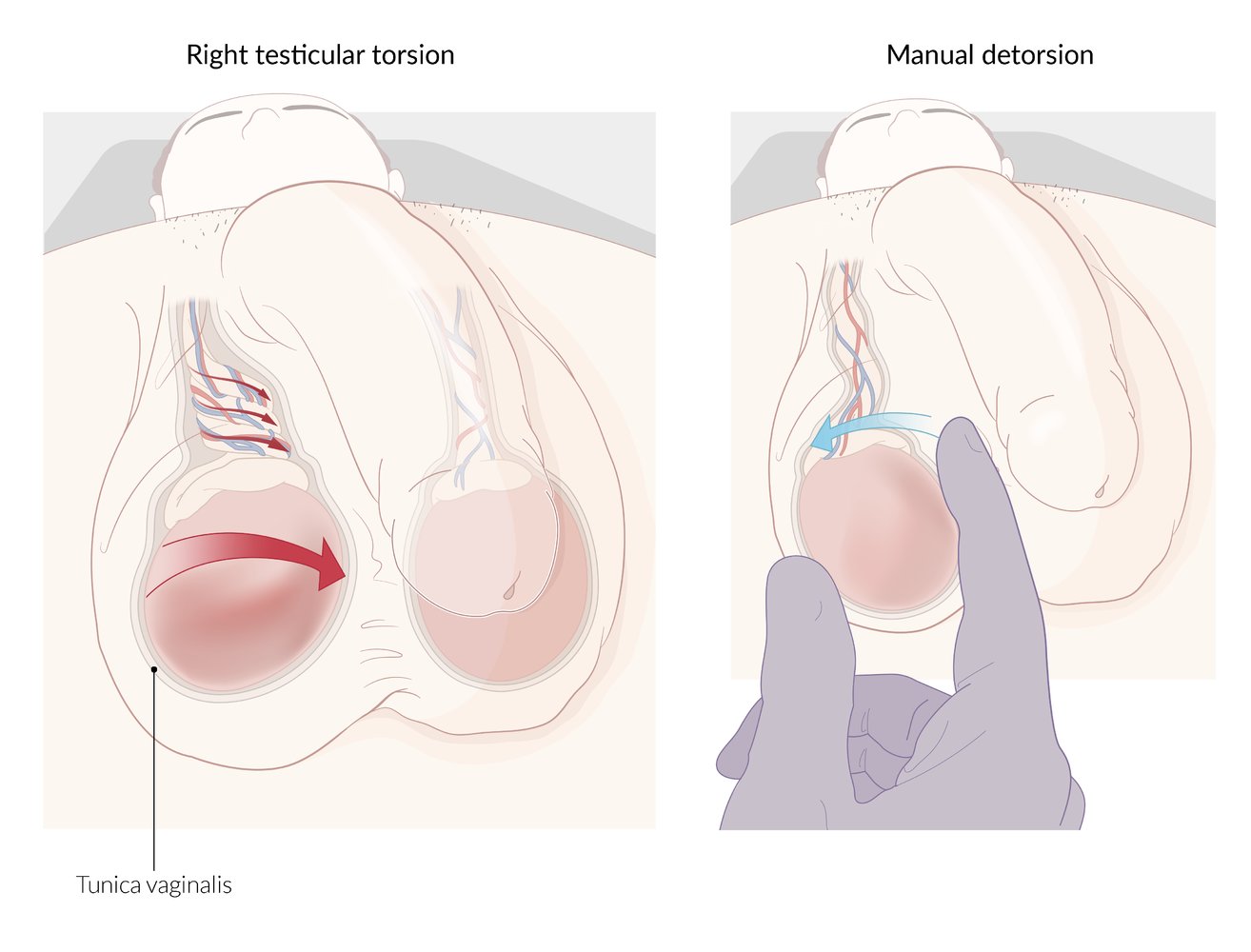
Testicular torsion is the twisting of the spermatic cord containing testicular blood vessels, leading to testicular ischemia. Testicular torsion most commonly occurs in the medial direction.
Manual detorsion may be attempted before definitive surgical therapy (orchidopexy) if the duration of symptoms is less than six hours. This involves untwisting the spermatic cord by rotating the testis in a lateral direction.
© AMBOSS
Summary
Testicular torsion is the sudden twisting of the spermatic cord within the scrotum. It most commonly affects neonates and young men. Because of the risk of ischemia and possible infarction of the testis, it is considered a urological emergency. Testicular torsion is characterized by sudden-onset unilateral testicular pain, which may radiate to the lower abdomen, with nausea and vomiting. Clinical findings include a high-riding testis with an absent cremasteric reflex. Imaging with duplex ultrasound of the scrotum may be required if the clinical diagnosis is in doubt. If testicular torsion is suspected, prompt surgical exploration within six hours of symptom onset is essential to salvage the testis. Important differential diagnoses, e.g., orchitis and epididymitis, should be ruled out before initiating treatment.
Epidemiology
- Peak incidence: neonatal period (first 30 days of life) and during puberty (10–14 years) [1]
-
Prevalence
- 3.8 per 100,000 male individuals under 18 years of age (two-thirds of cases occur between 12 and 18 years of age) [2]
- Accounts for 10–15% of acute scrotal illness in children within the United States [3]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
-
Idiopathic [3]
- Proposed causes include bell clapper deformity (intravaginal torsion; see "Pathophysiology" below) and a long mesorchium.
- In fetuses and neonates: extravaginal torsion of the entire tunica vaginalis
- Iatrogenic
- Occurs as a result of vigorous physical activity or trauma in very rare cases [4]
- Predisposing factors, especially in adults: testicular malignancy
Pathophysiology
- Testicular torsion is a sudden twisting of the spermatic cord (and vascular pedicle) associated with a poorly secured testis.
- Three mechanisms of testicular torsion may be identified:
- Intravaginal torsion: hypotheses suggest this occurs because of a congenital abnormality in which the tunica vaginalis attaches to the superior pole of the testis (bell-clapper deformity) → increased mobility of testis within tunica vaginalis, with possible abnormal transverse lie of testis → torsion of the testis (along the spermatic cord) [5]
- Extravaginal torsion: lack of fixation of the tunica vaginalis to the gubernaculum → concomitant torsion of the testis and tunica vaginalis (along the spermatic cord) [6]
- Long mesorchium : elongated mesorchium (thick band of connective tissue between the efferent ductules of the epididymis and the posterior surface of the testis) → torsion of the testis along the mesorchium [7]
- Torsion results in venous engorgement with consequent arterial compromise, tissue ischemia, and possible infarction.
- Irreversible damage occurs after 6–12 hours of torsion. [3]
Clinical features
- Abrupt onset of severe testicular pain and/or pain in the lower abdomen
- Typically swollen and tender testis and/or lower abdominal tenderness [8]
- Nausea and vomiting
-
Abnormal position of the testis
- Scrotal elevation (high-riding testis)
- Abnormal transverse position
- Possible undescended testes (predisposes to testicular torsion) [9]
- Absent cremasteric reflex
- Negative Prehn sign
- In neonates
- Possible absent testis
- Firm, painless scrotal mass
- Possible acute inflammation: swollen, erythematous (or blue discolored in venous engorgement), and tender hemiscrotum
Sudden, severe, unilateral scrotal pain in a patient with a tender, abnormally positioned testis on examination should be managed as testicular torsion until proven otherwise.
References:[3]
Initial management
Management of testicular torsion is time-sensitive.
- Perform rapid clinical evaluation of patients with acute scrotal pain as soon as possible.
- Record time from symptom onset.
- Consider differential diagnoses of scrotal pain.
- Consider using the TWIST score to supplement clinical judgment.
- Urgently refer the patient to urology as soon as torsion is suspected (e.g., high clinical likelihood, TWIST score ≥ 6–7). [10][11]
- Consider imaging if the diagnosis is uncertain, if this does not delay definitive treatment (see “Diagnostics”). [12]
- Color duplex ultrasonography is preferred over radionuclide imaging or MRI.
- Consider POCUS over formal ultrasound if trained personnel are available and can perform the examination more rapidly at the bedside.
- Obtain IV access and start pain management; consider a spermatic cord block.
- If surgery is not immediately available, consider performing manual testicular detorsion.
- Reassess pain frequently until the patient has been taken for exploratory surgery (see “Treatment”).
Do not delay urological referral to perform imaging or manual detorsion, especially if clinical suspicion is high, as there is a significant risk of infertility and/or testicular loss if definitive surgical management is delayed > 6 hours from symptom onset.
Clinical decision score [10][11][13]
The TWIST score may be used to help guide decisions on imaging prior to surgical exploration.
-
High-risk patients with a score of ≥ 6: extremely high likelihood of torsion
- Adult patient or child with Tanner stage ≥ 3: can refer patients directly for surgical exploration without prior imaging
- Child with Tanner stage < 3: Consider ultrasound before surgery.
- Low-risk patients (especially those with a score of 0): very low risk of torsion (ultrasound may not be required; however, this is controversial) [10][11][13]
- Medium-risk patients or clinical uncertainty: Obtain a scrotal ultrasound to help confirm diagnosis.
| Testicular workup for ischemia and suspected torsion score (TWIST score) [10][13] | |
|---|---|
| Clinical feature | Score if present |
| Swelling of the scrotum |
|
| Testis firm to palpation |
|
| Cremasteric reflex absent |
|
| Scrotal elevation (high-riding testis) |
|
| Nausea or vomiting |
|
Risk categories (from original derivation and validation cohort)
| |
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
Diagnosis
Testicular torsion is typically a clinical diagnosis. Do not delay definitive treatment for diagnostic workup if clinical suspicion is high.
Imaging
Imaging is not routinely indicated if there is high clinical suspicion but should be considered in patients with atypical clinical features.
Duplex ultrasound of the scrotum [11][14][15][16][17]
Either formal ultrasound or POCUS can be used to diagnose torsion, depending on operator skill and availability. [18]
- Indication: inconclusive clinical findings [14]
-
Characteristic findings [12][16]
- Enlarged testis
- Twisting of spermatic cord (whirlpool sign)
- Reduced or absent blood flow to/from the affected testis
- Heterogeneous appearance of testicular parenchyma indicates testicular necrosis. [16]

Other imaging modalities
These are typically time-consuming studies and may not be readily available in emergency situations.
-
Radionuclide imaging [3][19]
- Indications
- Inconclusive clinical findings
- Evaluate for epididymitis
- Characteristic findings
- Testicular torsion
- Areas that do not absorb radionuclide as a result of decreased blood flow to the affected testis (“cold spots”)
- Asymmetric blood flow
- Epididymitis: areas of increased radionuclide absorption as a result of increased blood flow in inflammation (“hot spots”)
- Testicular torsion
- Indications
- MRI with IV contrast: may be used as an alternative to radionuclide imaging [12]
Surgical intervention is recommended for suspected testicular torsion, regardless of radiological findings.
Laboratory studies
- Not routinely indicated
-
Urinalysis [14]
- Indications: rule out epididymitis
- Findings: Leukocytes and erythrocytes in the urine suggest epididymitis but do not exclude torsion (see “Epididymitis”).
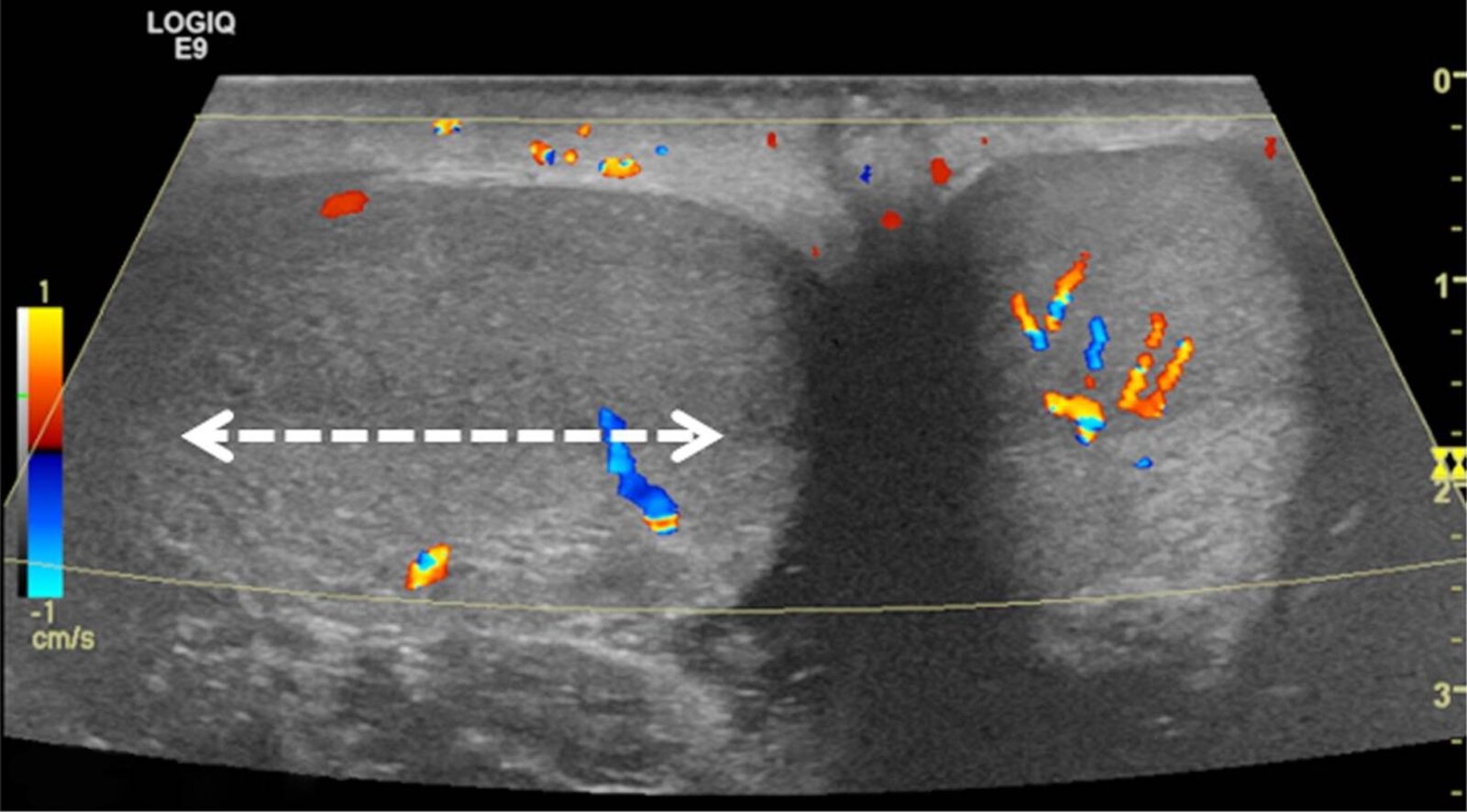
Color Doppler ultrasound of both testes (transverse plane) of a 14-year-old boy who woke up with acute right scrotal pain
The right testis lies in an abnormal horizontal position (white arrow), with intratesticular flow slightly reduced compared to the left testis.
These findings are consistent with intermittent testicular torsion. During orchiopexy, a bell clapper deformity was seen bilaterally determined to be the most likely cause.
Source: “Fig 5, In: Testicular torsion with preserved flow: key sonographic features and value-added approach to diagnosis” by Bandarkar AN, Blask AR, SpringerLink, licensed under CC BY 4.0. Modifications: image cropped & letter removed.
Differential diagnoses
Torsion of testicular appendage (hydatid of Morgagni) [20]
- Description: an embryological remnant on the upper pole of the testes or at the epididymis (the remnant of the Mullerian duct) that has the potential to rotate
-
Clinical features: Symptoms resemble acute testicular torsion.
- Typically seen in boys 7–14 years of age
- Insidious unilateral scrotal tenderness
- Blue dot sign (infarction of the hydatid of Morgagni that appears blue through the scrotal skin)
- Imaging: Doppler ultrasound may show an enlarged testicular appendix and/or mild hydrocele with preserved testicular blood flow.
-
Management
- A conservative approach with NSAIDs may be considered.
- If the diagnosis is in doubt, surgical intervention is required to examine the testes.
Other differential diagnoses
- Epididymitis
- Testicular tumor
- Complicated inguinal hernia
- Trauma (e.g., testicular rupture, scrotal hematocele)
- Nephrolithiasis
- Orchitis
- Fournier gangrene
- See also “Overview of scrotal abnormalities.”
The differential diagnoses listed here are not exhaustive.
Treatment
Testicular torsion is a medical emergency and should ideally be treated within 6 hours of the onset of symptoms for the best chance of testicular salvage. Manual detorsion in the emergency department may be attempted prior to surgery for immediate pain relief, but should not delay transferring the patient to the operating room.
Manual testicular detorsion [3][12]
- Indication: : may be attempted prior to surgery for immediate pain relief or if surgery is not immediately available
-
Procedure
- Consider performing under ultrasound guidance to increase the likelihood of success.
- Rotate the testis laterally toward the thigh ; two-thirds of torsions occur toward the midline.
- If lateral rotation does not provide symptom relief, rotate the testis toward the midline; one-third of torsions occur laterally. [21]
- Surgery should still be performed in all patients to resolve any possible degree of remaining torsion and to prevent recurrence. [14][14]
Because of the risk of infertility, surgical exploration of the scrotum is recommended in any patient suspected of having testicular torsion, even if manual detorsion has been attempted.
Exploratory surgery [3][14]
- Indication: suspected testicular torsion
- Timing: ideally, within 6 hours of symptom onset [3]
-
Procedure
- Immediate surgical exploration of the scrotum with reduction (untwisting) and orchiopexy of the affected testis
- Orchiopexy of the contralateral testis is recommended because the risk of testicular torsion on the contralateral side increases with previous or current testicular torsion. [3]
- Orchiectomy if the testis is grossly necrotic or nonviable
Testicular torsion is the twisting of the spermatic cord containing testicular blood vessels, leading to testicular ischemia. Testicular torsion most commonly occurs in the medial direction.
Manual detorsion may be attempted before definitive surgical therapy (orchidopexy) if the duration of symptoms is less than six hours. This involves untwisting the spermatic cord by rotating the testis in a lateral direction.
© AMBOSS
Prognosis
- Testicular salvage rates depend on the interval of time between symptom onset and restoration of testicular blood flow. [3][22][23]
- Within 6 hours: 90–100% [3]
- > 12 hours: 20–60%
- > 24 hours: up to 20%
- Late or absent surgical intervention → testicular ischemia (with/without necrosis) → disruption of the blood-testis barrier → formation of antisperm antibodies → infertility [22][23]
External Resources
References
- Huang W-Y, Chen Y-F, Chang H-C, et al. "The incidence rate and characteristics in patients with testicular torsion: a nationwide, population-based study". Acta Paediatr. 102(8). :e363-e367. (2013)
- William P. Adelman, MD, and Alain Joffe, MD, MPH. "The adolescent with a painful scrotum". Contemporary Pediatrics. (2000)
- Sharp VJ, Arlen AM. "Testicular Torsion: Diagnosis, Evaluation, and Management". Am Fam Physician. 88(12). :835-840. (2013)
- Ringdahl E, Teague L. "Testicular Torsion". Am Fam Physician. 74(10). :1739-1743. (2006)
- Riaz-ul-haq M, Mahdi DE, Elhassan EU. "Neonatal testicular torsion: a review article". Iran J Pediatr. 22(3). :281-289. (2012)
- Mano R, Livne PM, Nevo A, Sivan B, Ben-meir D. "Testicular torsion in the first year of life: characteristics and treatment outcome". Urology. 82(5). :1132-1137. (2013)
- Ta A et al. "Testicular torsion and the acute scrotum". Eur J Emerg Med. 23(3). :160-165. (2016)
- Liguori G et al. "Role of US in acute scrotal pain". World J Urol. 29(5). :639-643. (2011)
- McDowall J et al. "The ultrasonographic “whirlpool sign” in testicular torsion: valuable tool or waste of valuable time? A systematic review and meta-analysis". Emerg Radiol. 25(3). :281-292. (2018)
- Sheth KR, Keays M, Grimsby GM, et al. "Diagnosing Testicular Torsion before Urological Consultation and Imaging: Validation of the TWIST Score.". J Urol. 195(6). :1870-6. (2016)
- Wang CL, Aryal B, Oto A, et al. "ACR Appropriateness Criteria® Acute Onset of Scrotal Pain-Without Trauma, Without Antecedent Mass". J Am Coll Radiol. 16(5). :S38-S43. (2019)
- Blaivas M, Sierzenski P, Lambert M. "Emergency Evaluation of Patients Presenting with Acute Scrotum Using Bedside Ultrasonography". Acad Emerg Med. 8(1). :90-93. (2001)
- Walls R, Hockberger R, Gausche-Hill M. "Rosen's Emergency Medicine". Elsevier Health Sciences. (2018). ISBN: 9780323354790
- Wu H-C et al. "Comparison of Radionuclide Imaging and Ultrasonography in the Differentiation of Acute Testicular Torsion and Inflammatory Testicular Disease". Clin Nucl Med. 27(7). :490-493. (2002)
- Kadish HA, Bolte RG. "A retrospective review of pediatric patients with epididymitis, testicular torsion, and torsion of testicular appendages". Pediatrics. 102(1 Pt 1). :73-76. (1998)
- Lavallee ME, Cash J. "Testicular Torsion". Curr Sports Med Rep. 4(2). :102-104. (2005)
- Jacobsen FM, Rudlang TM, Fode M, et al. "The Impact of Testicular Torsion on Testicular Function". The World Journal of Men's Health. 37. (2019)
- Visser AJ, Heyns CF. "Testicular function after torsion of the spermatic cord". BJU Int. 92(3). :200-203. (2003)
- Sharp VJ, Kieran K, Arlen AM. "Testicular torsion: diagnosis, evaluation, and management.". Am Fam Physician. 88(12). :835-40. (2013)
- Bombiński P, Warchoł S, Brzewski M, et al. "Ultrasonography of Extravaginal Testicular Torsion in Neonates". Polish Journal of Radiology. 81. :469-472. (2016)
- Munden MM, Williams JL, Zhang W, et al. "Intermittent Testicular Torsion in the Pediatric Patient: Sonographic Indicators of a Difficult Diagnosis". American Journal of Roentgenology. 201(4). :912-918. (2013)
- Frohlich LC, Paydar-Darian N, Cilento BG, Lee LK. "Prospective Validation of Clinical Score for Males Presenting With an Acute Scrotum". Acad Emerg Med. 24(12). :1474-1482. (2017)
- Barbosa JABA, de Freitas PFS, Carvalho SAD, et al. "Validation of the TWIST score for testicular torsion in adults". Int Urol Nephrol. 53(1). :7-11. (2020)
- Kalfa N, Veyrac C, Lopez M, et al. "Multicenter assessment of ultrasound of the spermatic cord in children with acute scrotum". J Urol. 177(1). :297-301. (2007)
- Barbosa JA, Tiseo BC, Barayan GA, et al. "Development and initial validation of a scoring system to diagnose testicular torsion in children". J Urol. 189(5). :1859-1864. (2012)