Summary
Tetanus (lockjaw) is an acute disease caused by neurotoxins from the bacterium Clostridium tetani. C. tetani is ubiquitous in spore form and enters the body through broken skin (e.g., deep puncture wounds). Its toxins then cause uncontrolled activation of alpha motor neurons, leading to muscular rigidity and spasms. Patients classically present with a triad of trismus, risus sardonicus, and opisthotonus. Tetanus is a clinical diagnosis, but diagnostic testing may help confirm the diagnosis. Treatment includes airway management, wound debridement, immunoglobulin therapy (e.g., human tetanus immune globulin), antibiotics (e.g., metronidazole), and pharmacological management of severe muscle spasms. Prevention of tetanus involves routine immunization with tetanus vaccines and administering postexposure prophylaxis for wounds.
Etiology
-
Pathogen
- Clostridium tetani: a gram-positive, obligate anaerobic, spore-forming rod
- Produces neurotoxins tetanospasmin and tetanolysin
- Ubiquitous (especially animal feces and soil)
-
Route of infection
- Clostridial spores contaminate a wound (e.g., through dirt, saliva, feces).
- Localized ischemia, necrosis, foreign bodies and/or coinfection with other bacteria predispose to infection.
- Wounds with compromised blood supply create anaerobic conditions that are required for the germination and multiplication of C. tetani.
- Deep, penetrating wounds (e.g., knife, gunshot, animal bites)
- Open fractures
- Surgical procedures (e.g., bowel, biliary tract, or dental surgery)
- Burns
- Umbilical stump infections
- Septic abortion
- Groups with a higher risk: : non-immunized individuals, those with diabetes, neonates, people who inject drugs (PWID), certain patient groups (i.e., postsurgical, obstetric, dental)
Pathophysiology
Ubiquitous C. tetani spores contaminate a wound → bacterial reproduction under anaerobic conditions → production of the neurotoxins tetanospasmin and tetanolysin
-
Tetanospasmin: reaches the CNS through retrograde axonal transport
- Toxin binds to receptors of peripheral nerves and is then transported to interneurons (Renshaw cells) in the CNS via vesicles. [1][2]
- Acts as protease that cleaves synaptobrevin, a SNARE protein → prevention of inhibitory neurotransmitters (i.e., GABA and glycine) release from Renshaw cells in the spinal cord → uninhibited activation of alpha motor neurons → muscle spasms, rigidity, and autonomic instability
- Tetanolysin: causes hemolysis and has cardiotoxic effects
Neurotoxins (not the pathogen itself) cause tetanic contractions.
Tetanospasmin causes tetanic spasms.
Clinical features
- Incubation period: 3–21 days (average: ∼ 10 days)
-
Generalized tetanus: painful muscle spasms and rigidity
- Trismus: lockjaw due to spasms of jaw musculature (commonly the first tetanus-specific symptom)
- Risus sardonicus: sustained facial muscle spasm that causes a characteristic, apparently sardonic grin and raised eyebrows
- Opisthotonus: backward arching of spine, neck, and head caused by spasms of the back muscles
- Neck stiffness
- Abdominal rigidity
-
Life-threatening complications
- Laryngospasm and/or respiratory muscles spasms → respiratory failure [3]
- Autonomic dysfunction → circulatory arrest and shock [1][3]

 in tetanus")

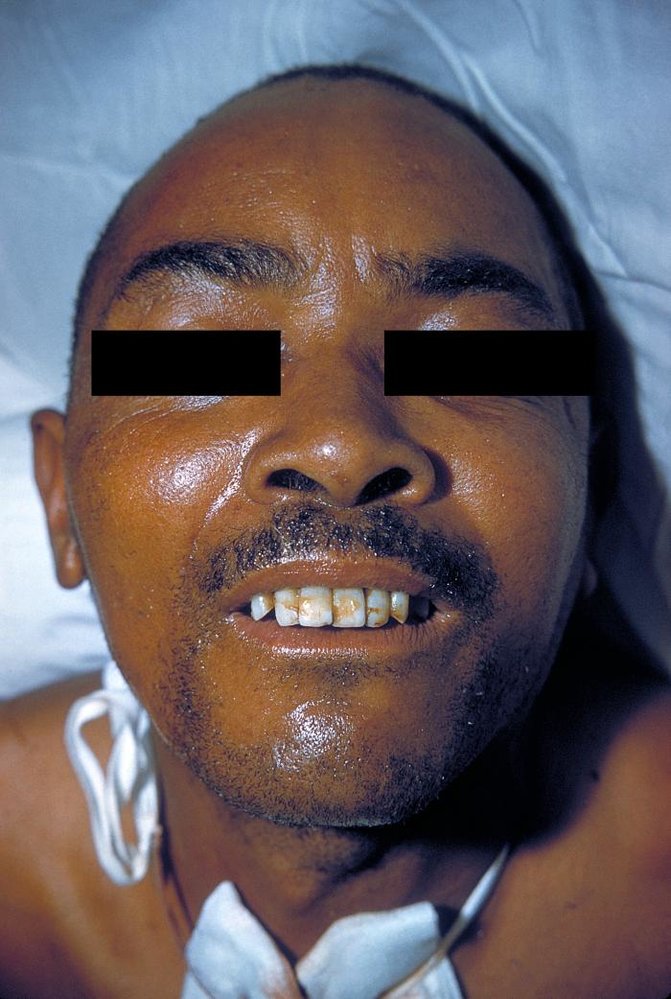
Sustained spasm of the facial muscles has resulted in trismus and the characteristic grinning appearance.
Source: "ID: 2857", CDC/Dr. Thomas F. Sellers, Centers for disease control and prevention licensed under Public Domain
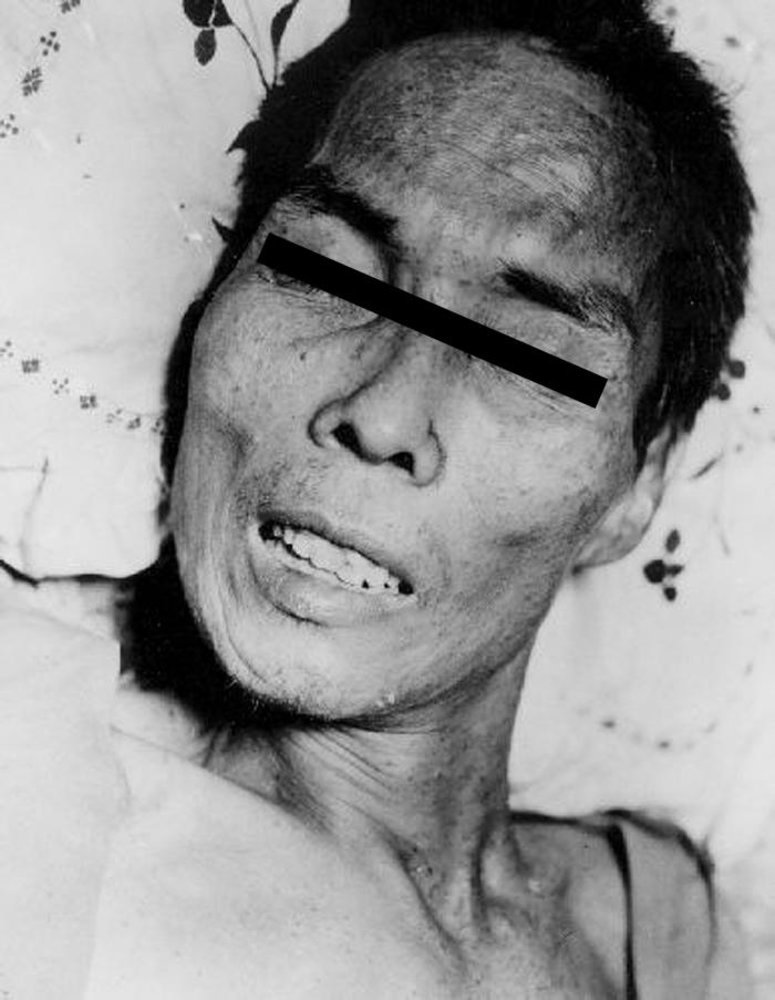
Photograph showing the characteristic facial muscle spasm of tetanus, with the appearance of a distorted grin and raised eyebrows.
Source: "ID#: 1657", CDC/ Armed Forces Institute of Pathology (AFIP)/ C. Farmer, Centers for Disease Control and Prevention, Atlanta, USA licensed under Public Domain
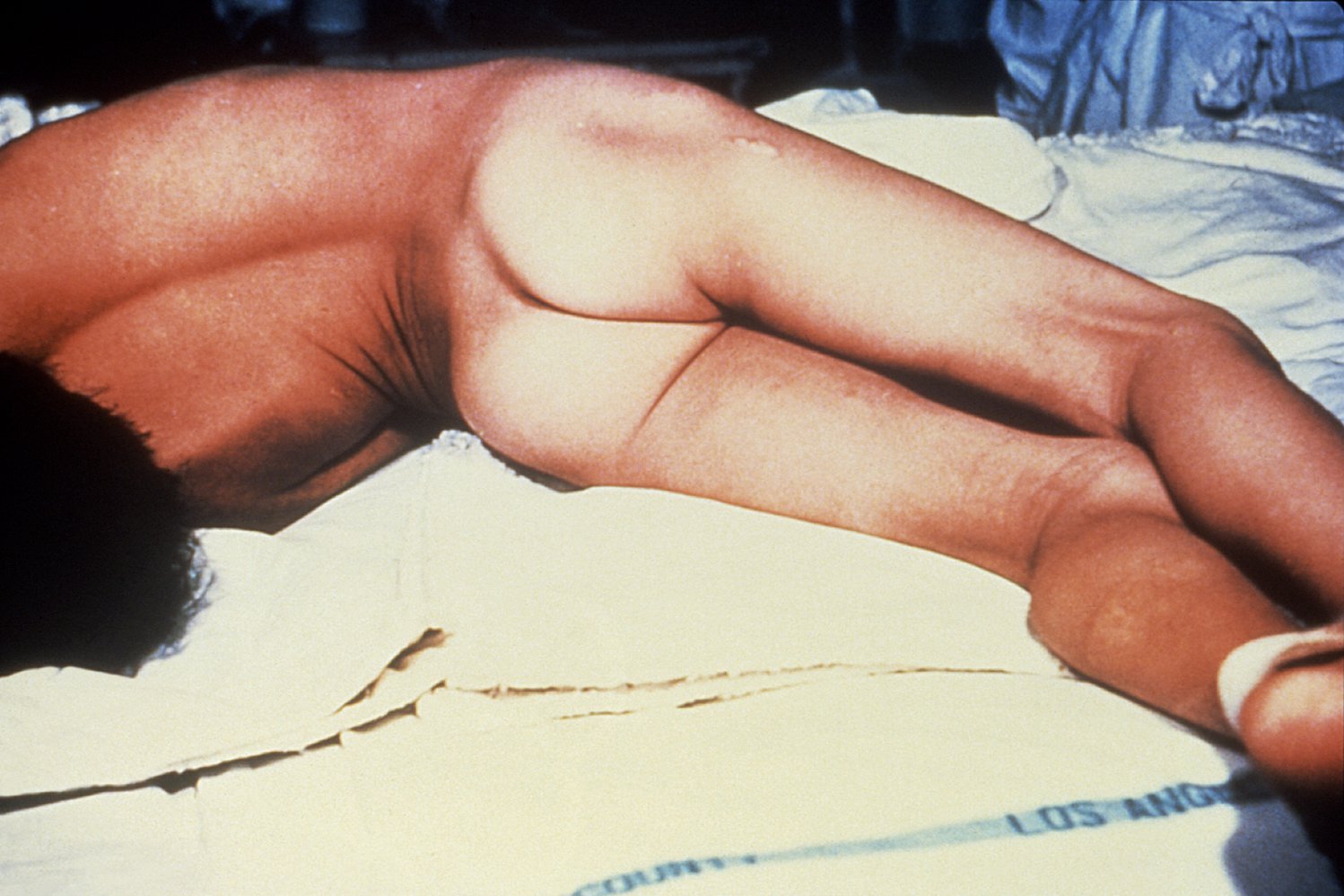
This young patient shows hyperextension of his head, neck and back (hyperlordosis), a position which is referred to as opisthotonus. Opisthotonus is characteristic of lockjaw (tetanus).
Source: "ID#: 6373", CDC, Centers for Disease Control and Prevention (CDC) licensed under Public Domain
Subtypes and variants
Neonatal tetanus
- Occurs in infants of inadequately immunized mothers after unsterile management of the umbilical stump
- Typically occurs 5–8 days after birth, but the incubation period can take up to several weeks
- Typically a rapid onset of symptoms as axonal length in infants is shorter than in adults [4]
- Symptoms
- Difficulty opening the mouth and feeding due to trismus and risus sardonicus
- Muscle stiffness and opisthotonus
- Clenched hands
Other types [5]
- Localized tetanus: Patients present with painful muscle contractions in areas surrounding the injury site only.
-
Cephalic tetanus
- In patients with open head or neck injuries.
- Initially only affects cranial nerves (especially flaccid paralysis of CN VII), which can be mistaken for stroke
Diagnosis
- Tetanus is a clinical diagnosis based on muscle spasms and rigidity associated with an entry point for bacteria and inadequate immunization. [6]
- Wound culture and serology may confirm the diagnosis but have low sensitivity and specificity.
Treatment
The following relates to the treatment of clinically apparent tetanus. See "Tetanus prophylaxis after injury" for preventing tetanus in individuals with acute wounds.
Approach [7][8][9][10]
- Immediately manage life-threatening and severe symptoms (see “Acute stabilization”).
- Administer passive immunization, e.g., human tetanus immunoglobulin, as soon as possible.
- Manage acute wounds, e.g., wound irrigation and debridement
- Initiate antibiotics, preferably PO metronidazole.
- Admit all patients with suspected tetanus infection.
- ICU admission is often required. [11][12][13]
- Follow standard precautions. [14]
- Begin active immunization; with the tetanus vaccine once the patient is improving.
Wound care and antibiotics decrease bacterial load and toxin production. Immunoglobulin therapy neutralizes free toxins. [9][13]
Acute stabilization [7][8][9][10]
- Laryngospasm or respiratory muscle spasms: airway management with rapid sequence intubation (RSI) [13]
- Cardiac instability: immediate hemodynamic support
- Severe muscle spasms: benzodiazepines and/or paralytics; , potentially in combination with mechanical ventilation [8][13]
Prepare for difficult airway management and consider early RSI, as trismus and laryngospasm can limit successful intubation.
Prolonged mechanical ventilation is often required; consider early tracheostomy. [13]
Antibiotics [7][8][9][10]
- Preferred: PO metronidazole (off-label) [7][10][13]
- Alternative: penicillin G [7][9]
Immunization [7][8][9][10]
-
Passive immunization: immunoglobulin therapy [7][8]
- First-line: IM human tetanus immunoglobulin (HTIG) [7][8]
- Consider infiltrating part of the HTIG dose into the affected wound. [7][8]
- HTIG unavailable: Consider intravenous immunoglobulin (off-label) . [7][11][15]
- HTIG and IVIG unavailable (e.g., resource-limited settings): Equine tetanus immunoglobulin may be considered. [7][16]
- Active immunization: tetanus vaccine administered at a separate site from HTIG [7][8][9]
Following immunoglobulin therapy, live vaccines (e.g., MMR vaccine, varicella vaccine) should not be given for 3–8 months (see “Contraindications to live vaccines”). [7]
Prevention
Tetanus vaccine [17][18]
Routine immunization is recommended for all individuals.
- Active component: denatured tetanus toxin
-
Available vaccines
- Children < 7 years of age
- DTaP (diphtheria, tetanus, and acellular pertussis) vaccines
- DT (diphtheria, tetanus) if acellular pertussis vaccines are contraindicated [19]
-
Children ≥ 7 years of age and adults
- Tdap (tetanus, diphtheria, pertussis): routinely, at age 11 years [8]
- Td (tetanus, diphtheria) OR Tdap boosters every 10 years
- Children < 7 years of age
- Schedule: See “ACIP immunization schedule” for details.
Boosters with Td or Tdap are recommended every 10 years for all adolescents and adults who have completed the primary Tdap and DTaP series. See “ACIP immunization schedule” for details. [18][20][21]
Acellular pertussis-containing vaccines are contraindicated in patients who previously developed unexplained encephalopathy within a week after receiving an acellular pertussis vaccine (i.e., DTaP or Tdap). [19]
Tetanus prophylaxis after injury [7][8][9][22]
- Management is based on:
- Tetanus vaccine history
- Wound assessment
- Immune status (e.g., immunocompromised state, HIV infection) [9]
-
Tetanus-prone wounds include:
- Dirty wounds
- Deep injuries
- Thermal injuries
| Postexposure tetanus prophylaxis [8][9][22] | ||
|---|---|---|
| Tetanus vaccine history | Clean and minor wounds | Tetanus prone wounds |
| Unknown or < 3 doses |
|
|
| ≥ 3 doses |
|
|
Administer HTIG to patients with severe immunodeficiency or HIV infection and a tetanus-prone wound regardless of tetanus vaccine history. [9]
External Resources
References
- Moss. "Handbook of Natural Toxins: Bacterial Toxins and Virulence Factors in Disease, Band 8". Marcel Dekker, Inc. . (1995). ISBN: 0824793811
- "Tetanus toxin: direct evidence for retrograde intraaxonal transport.". http://www.ncbi.nlm.nih.gov/pubmed/49080. [1975-05-30]
- "Epidemiology and Prevention of Vaccine-Preventable Diseases". https://web.archive.org/web/20160921090606/https://www.cdc.gov/vaccines/pubs/pinkbook/tetanus.html#complications. [2015-09-08]
- Andrew Michael Taylor, FRCA. "Tetanus". 6(3). :101-104. (2006)
- AAP Committee on Infectious Diseases. "Red Book: 2021–2024 Report of the Committee on Infectious Diseases". American Academy of Pediatrics. (2021). ISBN: 9781610025218
- Hall E, Wodi AP, Hamborsky J, et al. "Epidemiology and Prevention of Vaccine-Preventable Diseases 14th ed". Public Health Foundation. (2021). ISBN: 9780578969695
- Nemhauser JB. "CDC Yellow Book 2024". Oxford University Press. (2023). ISBN: 9780197570944
- "Current recommendations for treatment of tetanus during humanitarian emergencies". https://web.archive.org/web/20230816195511/https://www.who.int/publications/i/item/current-recommendations-for-treatment-of-tetanus-during-humanitarian-emergencies. [2010-01-11]
- "Tetanus: For Clinicians". https://web.archive.org/web/20230817153618/https://www.cdc.gov/tetanus/clinicians.html#treatment. [2022-08-29]
- Freshwater-Turner D, Udy A, Lipman J, et al. "Autonomic dysfunction in tetanus – what lessons can be learnt with specific reference to alpha-2 agonists?". Anaesthesia. 62(10). :1066-1070. (2007)
- Rodrigo C, Fernando D, Rajapakse S. "Pharmacological management of tetanus: an evidence-based review". Crit Care. 18(2). :217. (2014)
- Siegel JD, Rhinehart E, Jackson M, Chiarello L. "2007 Guideline for Isolation Precautions: Preventing Transmission of Infectious Agents in Health Care Settings". Am J Infect Control. 35(10). :S65-S164. (2007)
- Lee DC, Lederman HM. "Anti-Tetanus Toxoid Antibodies in Intravenous Gamma Globulin: An Alternative to Tetanus Immune Globulin". J Infect Dis. 166(3). :642-645. (1992)
- Orenstein W, Orenstein W, MD W, et al. "Plotkin's Vaccines". Elsevier. (2023). ISBN: 9780323790581
- "Tetanus (Lockjaw) Vaccination: What Everyone Should Know". https://web.archive.org/web/20160905114929/https://www.cdc.gov/vaccines/vpd-vac/tetanus/public/index.html. [2016-02-03]
- "Child and Adolescent Immunization Schedule. Recommendations for Ages 18 Years or Younger, United States, 2023". https://web.archive.org/web/20230324163634/https://www.cdc.gov/vaccines/schedules/hcp/imz/child-adolescent.html. [2023-02-10]
- "CDC Diphtheria, Tetanus, and Pertussis Vaccine Recommendations". https://web.archive.org/web/20230809155621/https://www.cdc.gov/vaccines/vpd/dtap-tdap-td/hcp/recommendations.html#:~:text=You%20should%20not%20administer%20acellular,of%20DTP%2C%20DTaP%2C%20or%20Tdap. [2023-03-10]
- "Catch-up Immunization Schedule for Children and Adolescents Who Start Late or Who Are More than 1 Month Behind Recommendations for Ages 18 Years or Younger, United States, 2023". https://web.archive.org/web/20230324164753/https://www.cdc.gov/vaccines/schedules/hcp/imz/catchup.html. [2023-02-10]
- "Adult Immunization Schedule by Age Recommendations for Ages 19 Years or Older, United States, 2023". https://web.archive.org/web/20230324184103/https://www.cdc.gov/vaccines/schedules/hcp/imz/adult.html. [2023-02-10]
- Liang, et al. "Prevention of Pertussis, Tetanus, and Diphtheria with Vaccines in the United States: Recommendations of the Advisory Committee on Immunization Practices (ACIP)". MMWR Recomm Rep. (2018)
- Roper MH, Vandelaer JH, Gasse FL. "Maternal and neonatal tetanus". 370(9603). :1947-59. (2007)
- "Tetanus: For Clinicians". https://web.archive.org/web/20201126130433/https://www.cdc.gov/tetanus/clinicians.html. [2020-01-23]
- Brown. "Nerve Cells and Nervous Systems: An Introduction to Neuroscience". Springer Science & Business Media. (2012). ISBN: 9783540760900
- Hinfey PB, Brusch JL. "Tetanus Clinical Presentation". WebMD. http://emedicine.medscape.com/article/229594-clinical#b2. [2016-06-16]
- Hinfey PB. "Tetanus Treatment & Management". WebMD. http://emedicine.medscape.com/article/229594-treatment#d9. [2016-06-16]