Summary
The menstrual cycle is a highly regulated physiological process required for conception and pregnancy. From the start of menstruation (menarche) to its cessation (menopause), menstrual bleeding (menstruation) is regulated by the coordinated release of hormones from the hypothalamus, pituitary gland, and ovaries. These hormones trigger simultaneous changes in the ovaries (ovarian cycle) and the uterus (uterine cycle). Mittelschmerz is a physiological condition experienced by some individuals characterized by unilateral lower abdominal pain during ovulation; it may be initially misdiagnosed as appendicitis, ectopic pregnancy, or ovarian torsion in individuals who present with acute pelvic pain or acute abdomen. Management involves reassurance and nonopioid analgesics.
Menstrual cycle abnormalities include changes in the frequency and intensity of menstruation as well as symptoms such as pronounced abdominal discomfort, gastrointestinal issues, and psychiatric symptoms. Amenorrhea, dysmenorrhea, abnormal uterine bleeding, and premenstrual disorders are discussed separately.
Overview of the menstrual cycle
Menstrual cycle
- The menstrual cycle is a highly regulated physiological process in which the coordinated release of hormones from the hypothalamus, pituitary gland, and ovaries produces a mature oocyte and prepares the endometrium for blastocyst implantation.
- Average cycle duration: 28 days (24–38 days)
- First day of menstruation: day 1 of the cycle
- Average duration of menstruation: 5 days [3]
- Average blood loss: 35–50 mL
-
Simultaneous changes in the ovaries (ovarian cycle) and the uterus (uterine cycle)
-
Ovarian cycle: 3 phases, regulated by hormones released from the hypothalamus and pituitary gland
- Follicular phase: production and maturation of a dominant follicle
- Ovulation: release of the oocyte from the dominant follicle
- Luteal phase: formation and degeneration of the corpus luteum
-
Uterine cycle: 3 phases, regulated by hormones released from the ovary during the ovarian cycle
- Menstrual phase: endometrial desquamation
- Proliferative phase: regeneration of the functional layer of the endometrium
- Secretory phase: endometrial differentiation in preparation for possible blastocyst implantation
-
Ovarian cycle: 3 phases, regulated by hormones released from the hypothalamus and pituitary gland
Ovarian and uterine changes during the menstrual cycle
| Menstrual cycle changes | ||
|---|---|---|
| Phase | Mechanism | |
| Ovarian cycle |
|
|
|
|
|
|
|
|
| Uterine cycle |
|
|
|
|
|
|
|
|

")
")
© AMBOSS
© AMBOSS
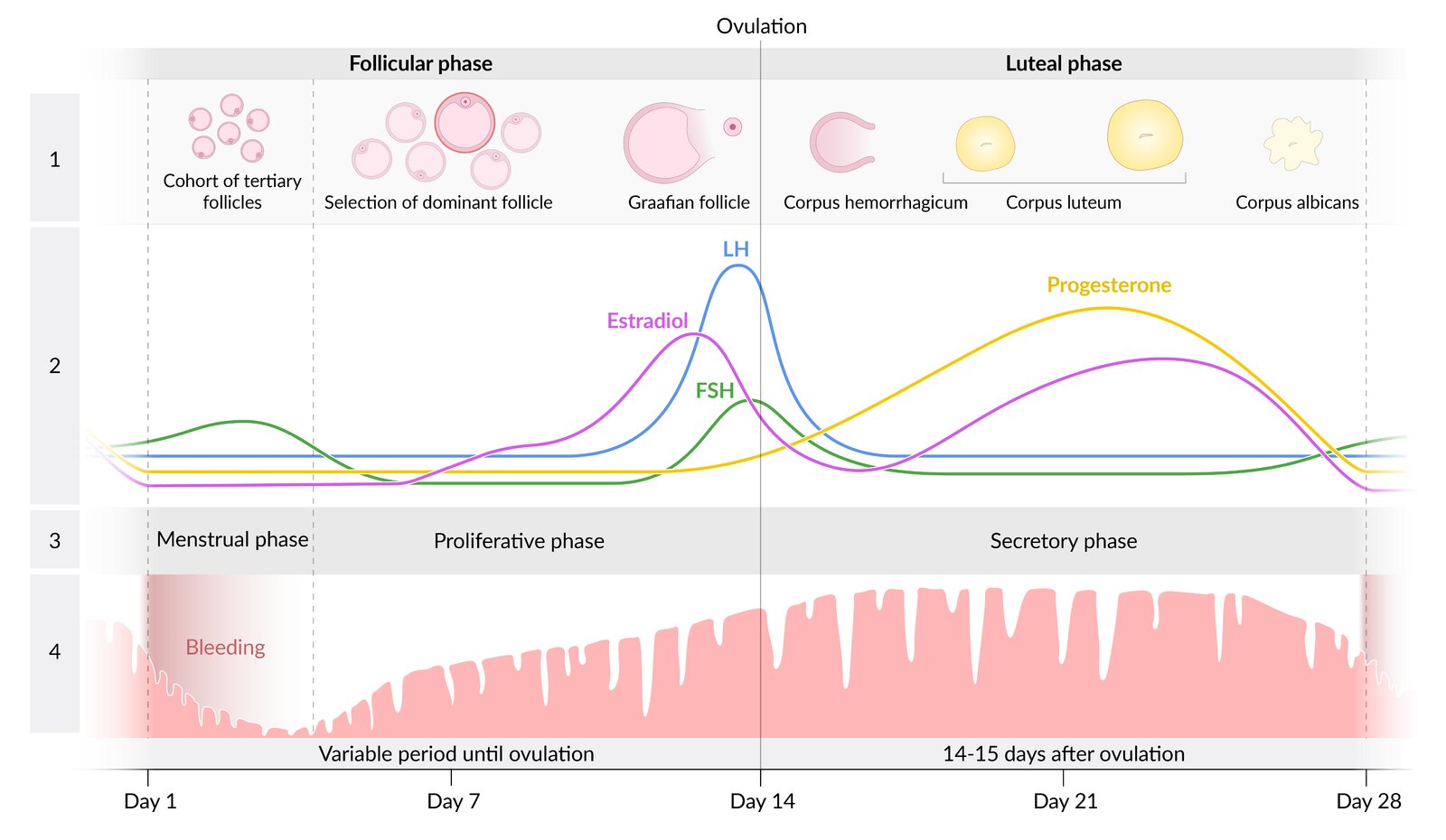
The menstrual cycle consists of two phases: the follicular and the luteal phase. The onset of menses marks the beginning of the follicular phase, which usually lasts 12–14 days but may be variable. The luteal phase begins on the day of ovulation and lasts 14 days.
During the follicular phase, FSH and LH stimulate the development of several follicles, one of which develops as the dominant follicle into the Graafian follicle. An LH surge initiates ovulation. As the oocyte reaches the fallopian tube, the ruptured follicle transforms into the corpus luteum, which produces progesterone. If no pregnancy occurs, the corpus luteum regresses and the progesterone level drops. This drop induces vasospasms in the uterine spiral arteries, ischemia, and sloughing off of the functional endometrial layer, which leads to menstrual bleeding (menstrual phase). During the proliferative phase, the endometrium is built up again in preparation for oocyte implantation during the secretory phase.
1: stages of follicle development; 2: hormone levels; 3: phases of the endometrial cycle; 4: development of the endometrium during the cycle
© AMBOSS
Ovarian cycle
-
Follicular phase (approx. day 1–14) ; [4]
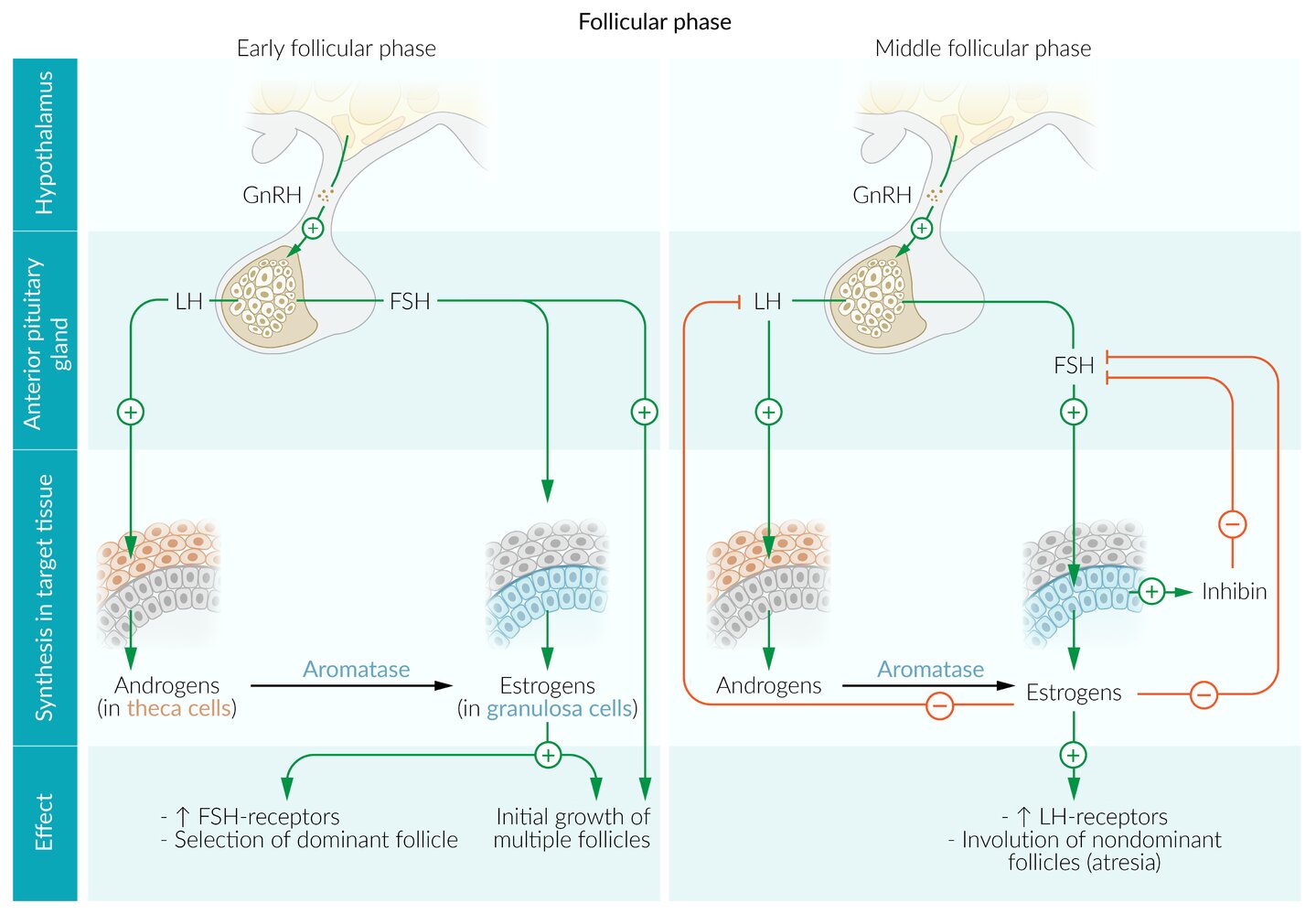
- The hypothalamus releases gonadotropin-releasing hormone (GnRH) in pulses, stimulating the anterior pituitary gland to release follicle-stimulating hormone (FSH) and luteinizing hormone (LH).
- FSH and LH stimulate the growth of a cohort of antral follicles.
- LH stimulates ovarian theca cells and induces the production of progesterone and androstenedione (substrates for estradiol synthesis in granulosa cells).
- FSH stimulates ovarian granulosa cells, which produce estradiol and inhibin.
- Estradiol and inhibin block the release of gonadotropins (negative feedback).
- Decreasing FSH levels lead to a regression of all follicles except one dominant follicle, which continues to develop despite falling FSH levels. [5]
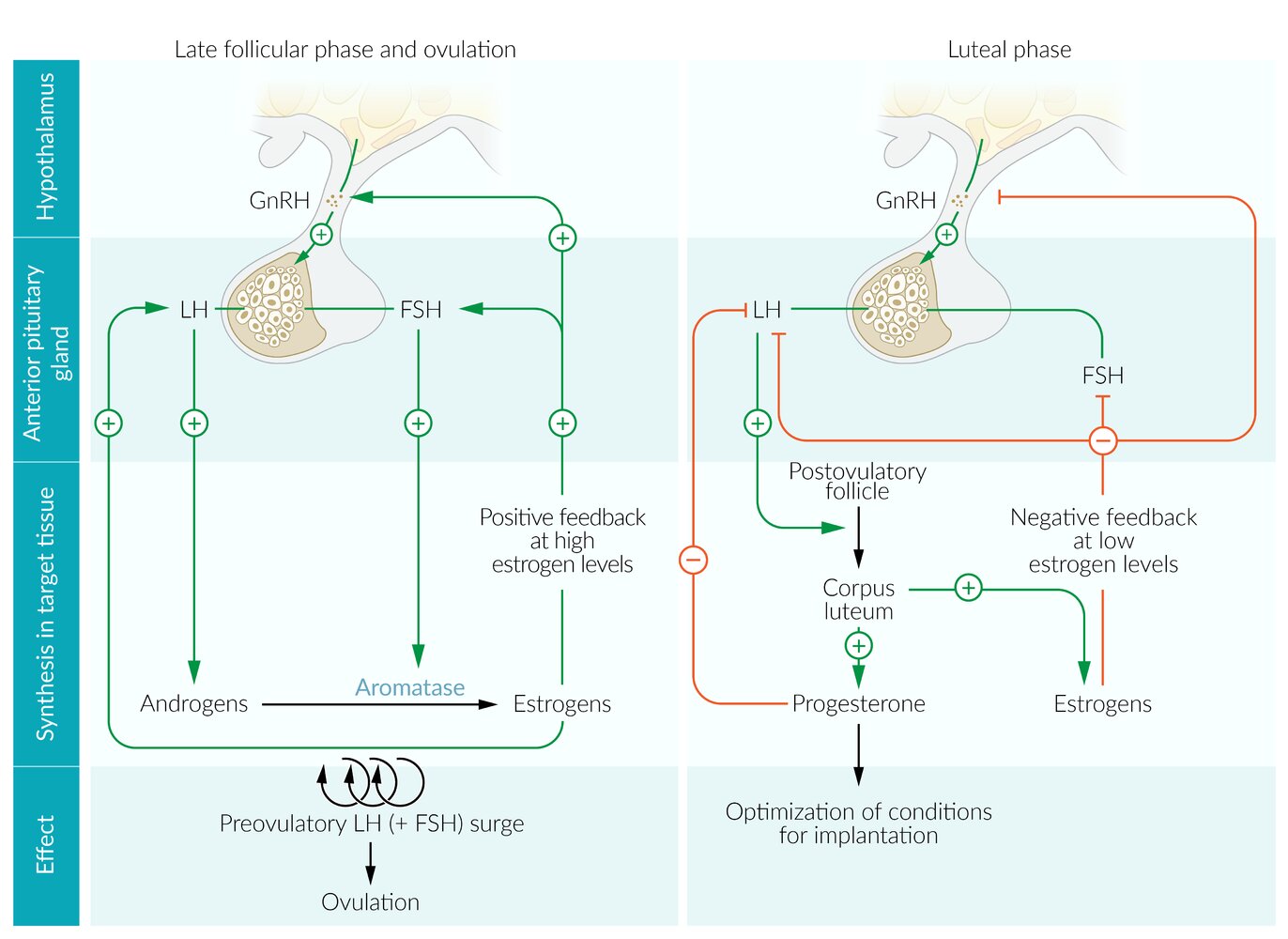
- The dominant follicle produces high levels of estradiol, which leads to a switch from negative to positive feedback in the hypothalamus and pituitary gland, resulting in a rapid increase in gonadotropin levels (LH surge). [6]
- Ovulation (approx. day 14): LH surge induces the release of the mature oocyte from the dominant follicle.
-
Luteal phase (for 14 days after ovulation) ; :
- The ruptured follicle transforms into the corpus luteum, primarily producing progesterone and some estradiol.
- Progesterone and estradiol inhibit gonadotropin release (switch back to negative feedback).
- In the absence of fertilization, falling LH levels lead to degeneration of the corpus luteum.
- Discontinuation of progesterone and estradiol production by the corpus luteum results in cessation of gonadotropin inhibition, initiating the follicular phase.
© AMBOSS
© AMBOSS
Uterine cycle
-
Menstrual phase (day 1 to approx. day 5)
- In the absence of fertilization, the corpus luteum degenerates.
- Decreasing progesterone and estradiol levels induce vasospasms and ischemia in the uterine spiral arteries and apoptosis of the functional layer of the endometrium. [7][8][9]
- These changes lead to shedding of the endometrial lining, which manifests as menstruation.
-
Proliferative phase of the menstrual cycle (approx. day 5–14): Estradiol produced by the growing follicles promotes endometrial proliferation.
- Uterine spiral arteries regenerate and extend two-thirds of the way into the endometrium.
- Stromal cells divide, enlarge, and accumulate glycogen.
- Endometrial glands become straight, tubular, and lined by simple columnar epithelium.
- Endometrial epithelial cells proliferate (cells have high mitotic activity).
-
Secretory phase (approx. day 14–28): Progesterone from the corpus luteum promotes endometrial differentiation and other changes that prepare the body for blastocyst implantation.
- Stromal cells become edematous and uterine spiral arteries extend the full length of the endometrium.
- Endometrial glands increase tortuosity and production of glycogen-rich secretions.
- Basal body temperature increases.
- Cervical mucus secretion increases, which protects the uterus from foreign substances and cells (e.g., sperm).
Physiological age-related changes in the menstrual cycle
- First few years after menarche: irregular menstrual cycles (due to immaturity of the hypothalamic-pituitary-gonadal axis)
- 25–30 years of age: Menstrual cycles are longest.
- Perimenopause: irregular menstrual cycles (due to fluctuating hormone levels)
Mittelschmerz
Mittelschmerz (also known as midcycle pain or ovulatory pain) is physiological pain experienced by some individuals during ovulation. [10][11]
Epidemiology
Mittelschmerz occurs at least once in > 50% of premenopausal individuals. [12]
Etiology [12]
- Unclear
-
Proposed etiologies include:
- Enlargement and rupture of the follicular cyst
- Spasms of the fallopian tubes or uterus
- Transient peritoneal irritation from follicular fluid or blood
Clinical features
-
Unilateral lower abdominal pain (often recurrent) [12][13]
- Pain occurs mid-cycle (days 14–16 of the menstrual cycle) in individuals with regular cycles.
- Usually located in the iliac fossa but may be generalized [13][14]
- Can last from minutes up to 48 hours [10][14]
- May be accompanied by ovulation bleeding: light bleeding or blood-stained discharge during the midpoint of the menstrual cycle [15]
-
Physical examination
- Lower abdominal pain on palpation [16]
- Possible referred pain and rebound tenderness [16]
- Adnexal tenderness or, rarely, a mass [14][17]
Diagnostics
- Clinical diagnosis [11][12]
- If there is diagnostic uncertainty, consider laboratory studies or imaging to rule out differential diagnoses of acute abdomen. [12][16]
-
Pelvic ultrasound (if performed) may show signs of ovulation, e.g.: [18]
- A small amount of intraperitoneal fluid
- Increased echogenicity in ovarian follicles
It may be difficult to distinguish between symptoms of mittelschmerz and those of acute appendicitis or other adnexal emergencies. [12][16]
Management
- Reassurance and ; nonopioid analgesics (e.g., NSAIDs) as needed [11][13]
- For recurrent episodes, consider hormonal contraception to suppress ovulation. [19]
Abnormalities of the menstrual cycle
Abnormal menstrual patterns include changes in the frequency, intensity, and/or onset of bleeding. Common manifestations of menstrual cycle abnormalities include:
- Dysmenorrhea (painful menstruation)
- Amenorrhea (absence of menstruation)
- Abnormal uterine bleeding (e.g., increased frequency and/or volume of menstruation)
- Premenstrual disorders (cyclical physical, psychological, and behavioral changes before menstruation)
-
Anovulatory cycle: The menstrual cycle may be irregular in adolescents during the first few months/years after menarche.
-
Immaturity of the hypothalamic-pituitary-gonadal axis → irregular secretion of gonadotropins → short luteal phase, and lack of progesterone → endometrium remains in the proliferative phase → irregular menses and heavy menstrual bleeding
- Does not require treatment because menses become regular as hypothalamic-pituitary-gonadal axis matures
-
Immaturity of the hypothalamic-pituitary-gonadal axis → irregular secretion of gonadotropins → short luteal phase, and lack of progesterone → endometrium remains in the proliferative phase → irregular menses and heavy menstrual bleeding
Related One-Minute Telegram
- One-Minute Telegram 64-2022-3/3: COVID-19-related stress may cause menstrual irregularity
Interested in the newest medical research, distilled down to just one minute? Sign up for the One-Minute Telegram in “Tips and links” below.
External Resources
References
- Kumar V, Abbas AK, Aster JC. "Robbins & Cotran Pathologic Basis of Disease". Elsevier Saunders. (2014). ISBN: 9781455726134
- Dutta DC, Konar H. "DC Dutta's Textbook of Gynecology". Jaypee Brothers Medical Publishers. (2013). ISBN: 9789351520689
- Dasharathy SS, Mumford SL, Pollack AZ, et al. "Menstrual Bleeding Patterns Among Regularly Menstruating Women". Am J Epidemiol. 175(6). :536-545. (2012)
- Scott M. Fishman. "Bonica's Management of Pain". Lippincott Williams & Wilkins. (2012). ISBN: 9781451161403
- Cameron P, Little M, Mitra B, Deasy C. "Textbook of Adult Emergency Medicine E-Book". Elsevier Health Sciences. (2019). ISBN: 9780702076251
- Baines PA, Allen GM. "PELVIC PAIN AND MENSTRUAL RELATED ILLNESSES". Emerg Med Clin North Am. 19(3). :763-780. (2001)
- Pamela Macintyre, David Rowbotham, Suellen Walker. "Clinical Pain Management Second Edition: Acute Pain, Band 1". CRC Press. (2008). ISBN: 9780340940099
- Wolfson AB, Hendey GW, Ling LJ, et al. "Harwood-Nuss' Clinical Practice of Emergency Medicine". Lippincott Williams & Wilkins. (2012). ISBN: 9781451153453
- Horsky J, Presl J. "Ovarian Function and its Disorders". Springer Science & Business Media. (2012). ISBN: 9789400981959
- Braen GR. "Manual of Emergency Medicine". Lippincott Williams & Wilkins. (2012). ISBN: 9781451153910
- Wheeler V, Umstead B, Chadwick C. "Adnexal Masses: Diagnosis and Management". Am Fam Physician. 108(6). :580-587. (2023)
- Su H, Yi Y, Wei T, Chang T, Cheng C. "Detection of ovulation, a review of currently available methods". Bioeng Transl Med. 2(3). :238-246. (2017)
- Rakel RE, Rakel D. "Textbook of Family Medicine". Elsevier Health Sciences. (2011). ISBN: 9781437711608
- Miro F, Aspinall LJ. "The onset of the initial rise in follicle-stimulating hormone during the human menstrual cycle". Human Reproduction. 20(1). :96-100. (2005)
- Woods DC, Johnson AL. "Regulation of Follicle-Stimulating Hormone-Receptor Messenger RNA in Hen Granulosa Cells Relative to Follicle Selection1". Biol Reprod. 72(3). :643-650. (2005)
- Kauffman AS. "Neuroendocrine mechanisms underlying estrogen positive feedback and the LH surge". Frontiers in Neuroscience. 16. (2022)
- Song J. "Hormonal regulation of apoptosis and the Fas and Fas ligand system in human endometrial cells". Mol Hum Reprod. 8(5). :447-455. (2002)
- Wei P, Jin X, Tao SX, Han CS, Liu YX. "Fas, FasL, Bcl-2, and Bax in the endometrium of rhesus monkey during the menstrual cycle". Mol Reprod Dev. 70(4). :478-484. (2005)
- Kelly RW, King AE, Critchley HOD. "Inflammatory mediators and endometrial function—focus on the perivascular cell". J Reprod Immunol. 57(1-2). :81-93. (2002)
- Tao Le, Vikas Bhushan, Deol M, Reyes G. "First Aid for the USMLE Step 2 CK, Tenth Edition". McGraw-Hill Education. (2018). ISBN: 9781260440294