Summary
Thyroid cancer is a malignant tumor that arises from either the thyrocytes or the parafollicular cells of the thyroid gland. It is more common in women, especially between 30–50 years of age. The predominant risk factors for thyroid cancer are a history of childhood irradiation to the head and neck and a family history of thyroid cancer. Thyroid cancer typically manifests as firm to hard thyroid nodule (or nodules). Initial evaluation of all patients includes TSH assay and thyroid ultrasound. Sonographic signs of thyroid cancer include a solid, hypoechoic nodule(s) with irregular margins, microcalcifications, and evidence of local infiltration into adjacent structures or cervical lymph nodes. On thyroid scintigraphy, which should be obtained in patients with low serum TSH, a malignant nodule is typically “cold” or hypofunctional. Cytopathological analysis with FNAB is required to confirm the diagnosis. Depending on the cell of origin, thyroid cancer can be classified as papillary, follicular, medullary, or anaplastic thyroid cancer. Most thyroid cancers are treated surgically with total thyroidectomy (in some cases with hemithyroidectomy), followed by adjuvant therapy, which may include RAIA and TSH suppression therapy with L-thyroxine, radiation therapy, and chemotherapy. In advanced anaplastic carcinoma, only palliative care may be feasible. The prognosis depends on the type of thyroid cancer.
Epidemiology
- Incidence: ∼ 13.5 new cases per 100,000 per year [1]
-
Sex [2]
- Differentiated carcinoma (papillary and follicular): ♀ > ♂ (3:1)
- Poorly-differentiated carcinoma (medullary and anaplastic): ♀ ≈ ♂
- Age: See “Overview” below.
Epidemiological data refers to the US, unless otherwise specified.
Etiology
- Genetic factors
- Medullary carcinoma: associated with MEN2 (RET gene mutations) or familial medullary carcinoma
- Papillary carcinoma: associated with RET/PTC rearrangements and BRAF mutations
- Follicular carcinoma: associated with PAX8-PPAR-γ rearrangement and RAS mutation
- Undifferentiated/anaplastic carcinoma: associated with TP53 mutation
- Ionizing radiation; (particularly during childhood): mostly associated with papillary carcinoma
References:[3]
Overview
| Characteristic features of thyroid cancer [4] | |||||
|---|---|---|---|---|---|
| Tissue of origin | Carcinoma | Differentiation | Characteristics | Distribution | Peak incidence |
| Thyrocytes | Papillary thyroid carcinoma | Well differentiated |
|
|
|
| Follicular thyroid carcinoma |
|
|
|
||
| Anaplastic thyroid carcinoma | Poorly differentiated |
|
|
|
|
| Parafollicular cells (C cells) | Medullary thyroid carcinoma |
|
|
|
|





Papillary carcinoma is the most Prevalent type of thyroid cancer, it features Palpable lymph nodes, and it has the best Prognosis compared to all other types of thyroid cancer.
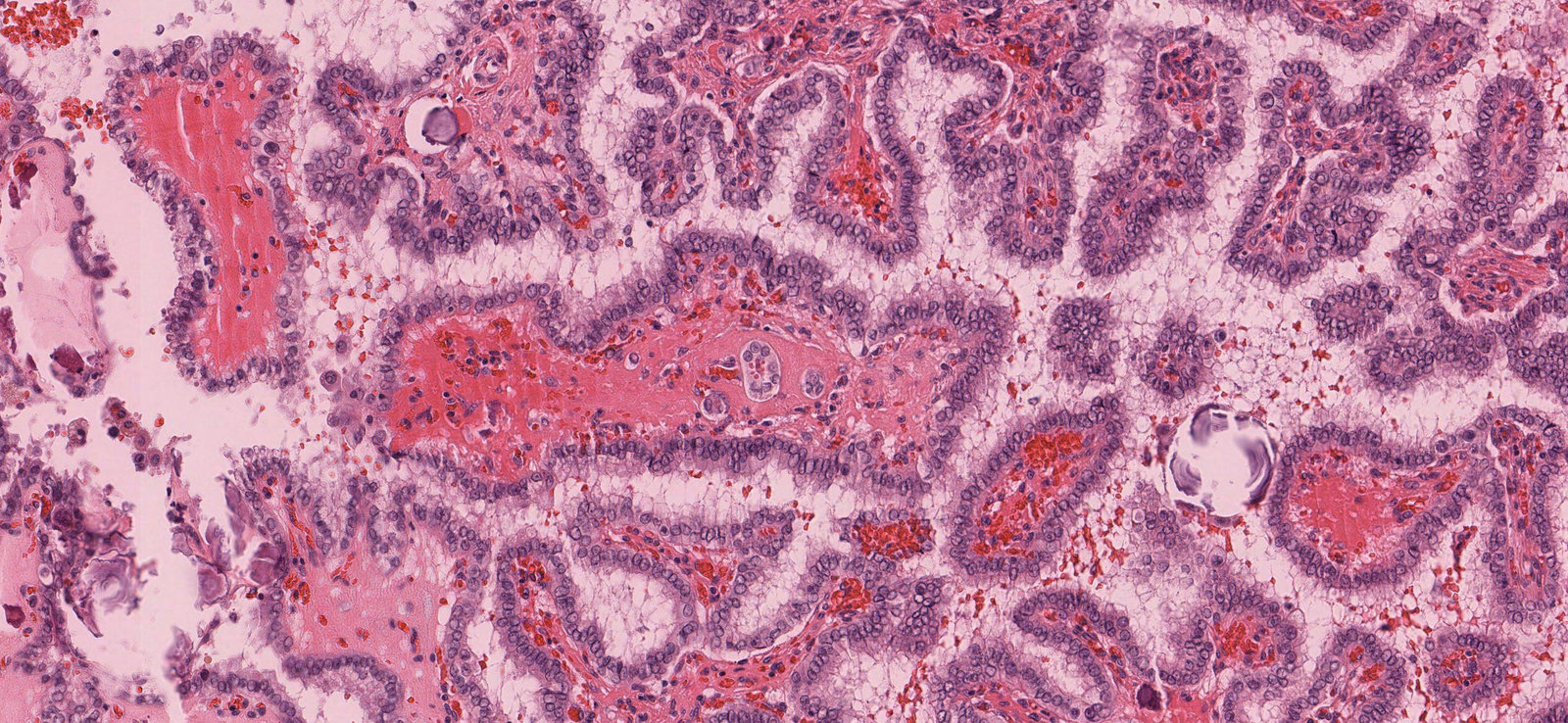
Micrograph image of thyroid tissue (H&E stain, 400x magnification)
Arrowheads: examples of pathological nuclei
Blue overlay: connective tissue core of papillae
Yellow dashed overlay: epithelial cancer cells covering the papillae
Yellow overlay: psammoma bodies
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. med. Alberto Perez Bouza, Facharzt für Pathologie
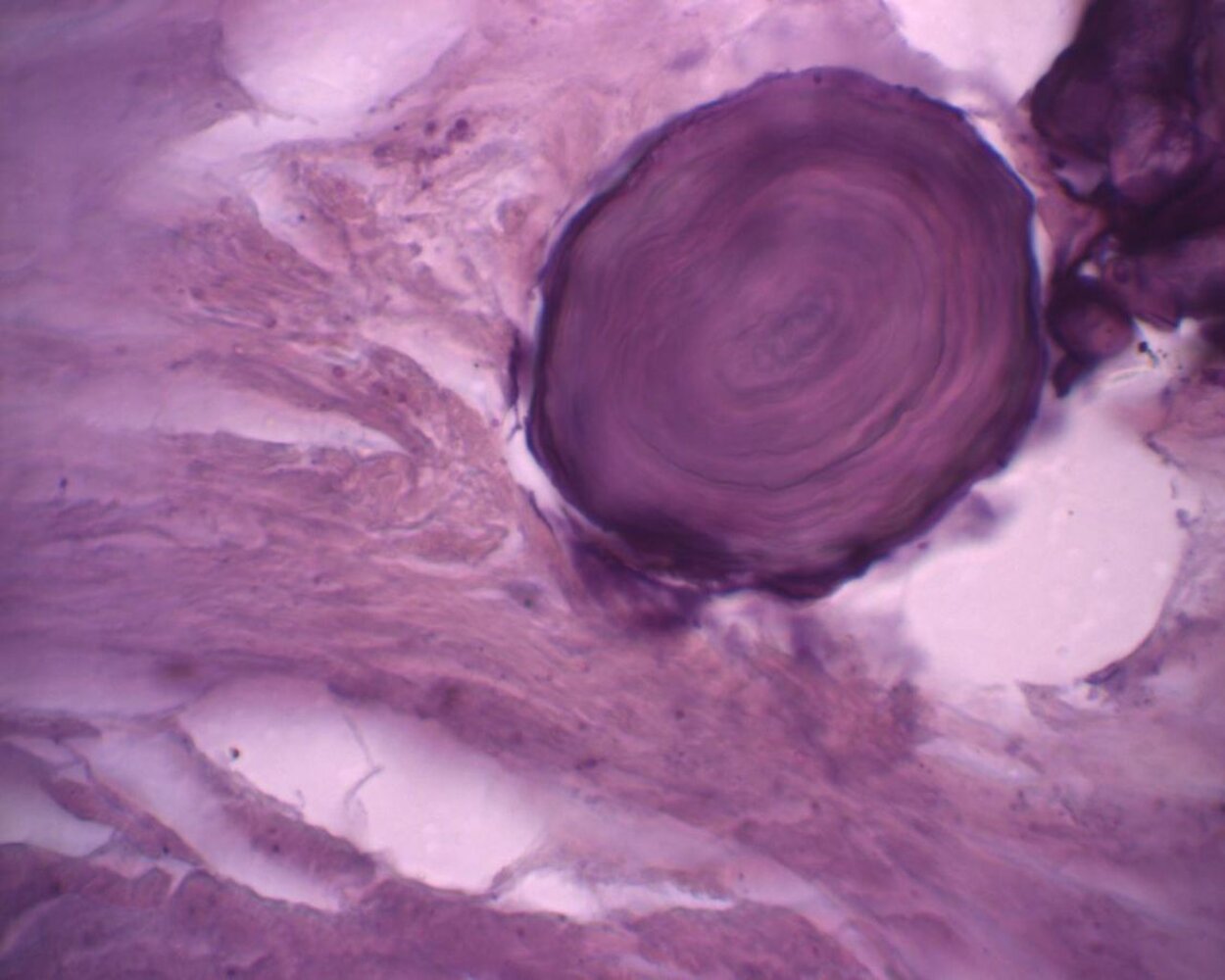
Photomicrograph of a thyroid tissue sample (H&E stain; high magnification)
Psammoma bodies are concentric lamellar calcifications that are often seen within papillary thyroid carcinomas.
Other tumors with frequent presence of psammoma bodies include serous carcinoma of the ovary, high-grade serous carcinoma of the uterus, and meningiomas.
Source: “Psammoma body Papillary thyroid carcinoma magnx400.jpg” by Eriugen, Wikimedia commons, licensed under CC BY-SA 4.0.
{kind=link}
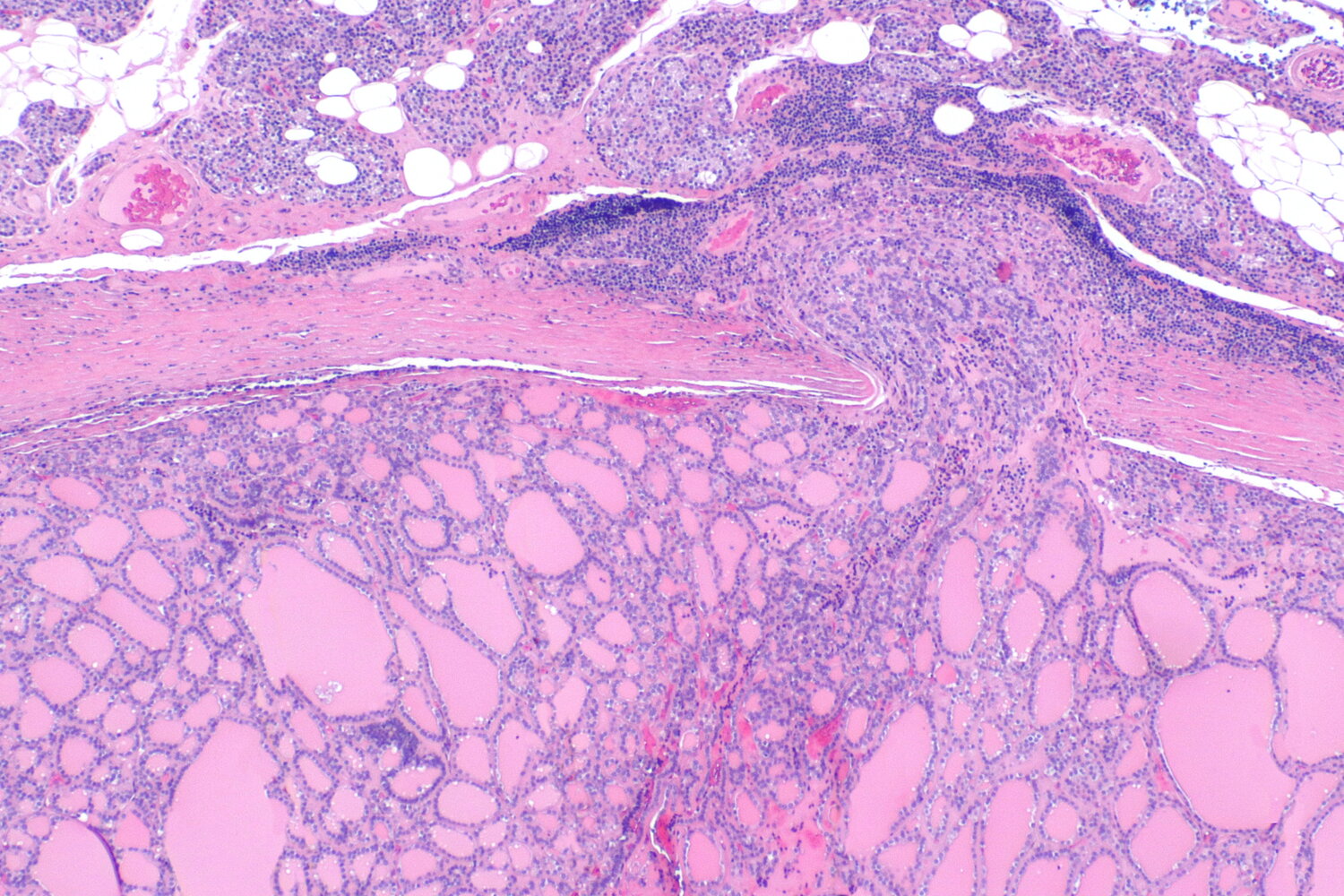
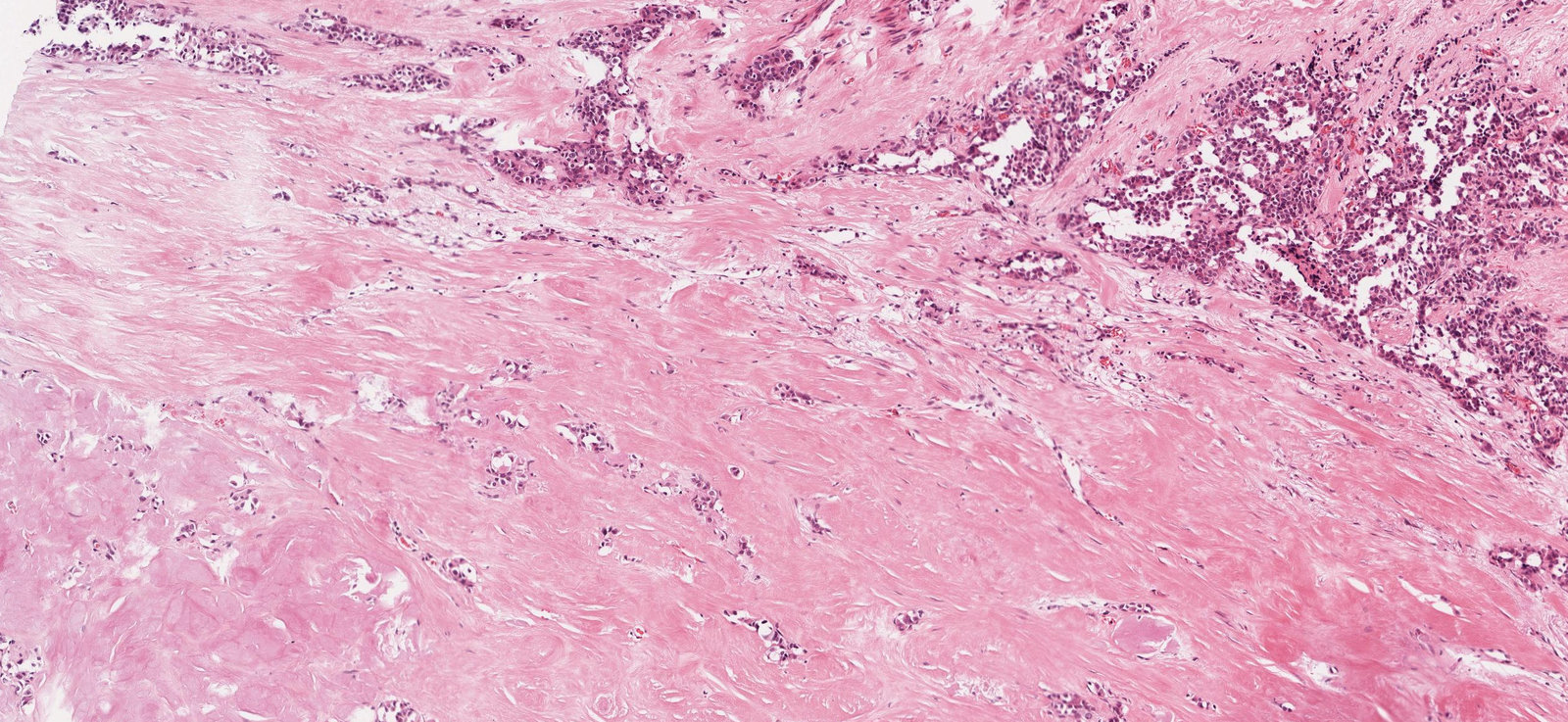
Photomicrograph of a thyroid tissue specimen (H&E stain; low magnification)
A partly encapsulated (capsule marked by hatched blue overlay) thyroid lesion comprised of follicles of varying size and shape (blue overlay) can be seen. Focally, this lesion displays a capsular invasion (yellow overlay), which is diagnostic of follicular thyroid carcinoma.
Source: “Follicular thyroid carcinoma 2 -- low mag” by Nephron, Wikimedia Commons, licensed under CC BY-SA 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 4.0.
{kind=link}
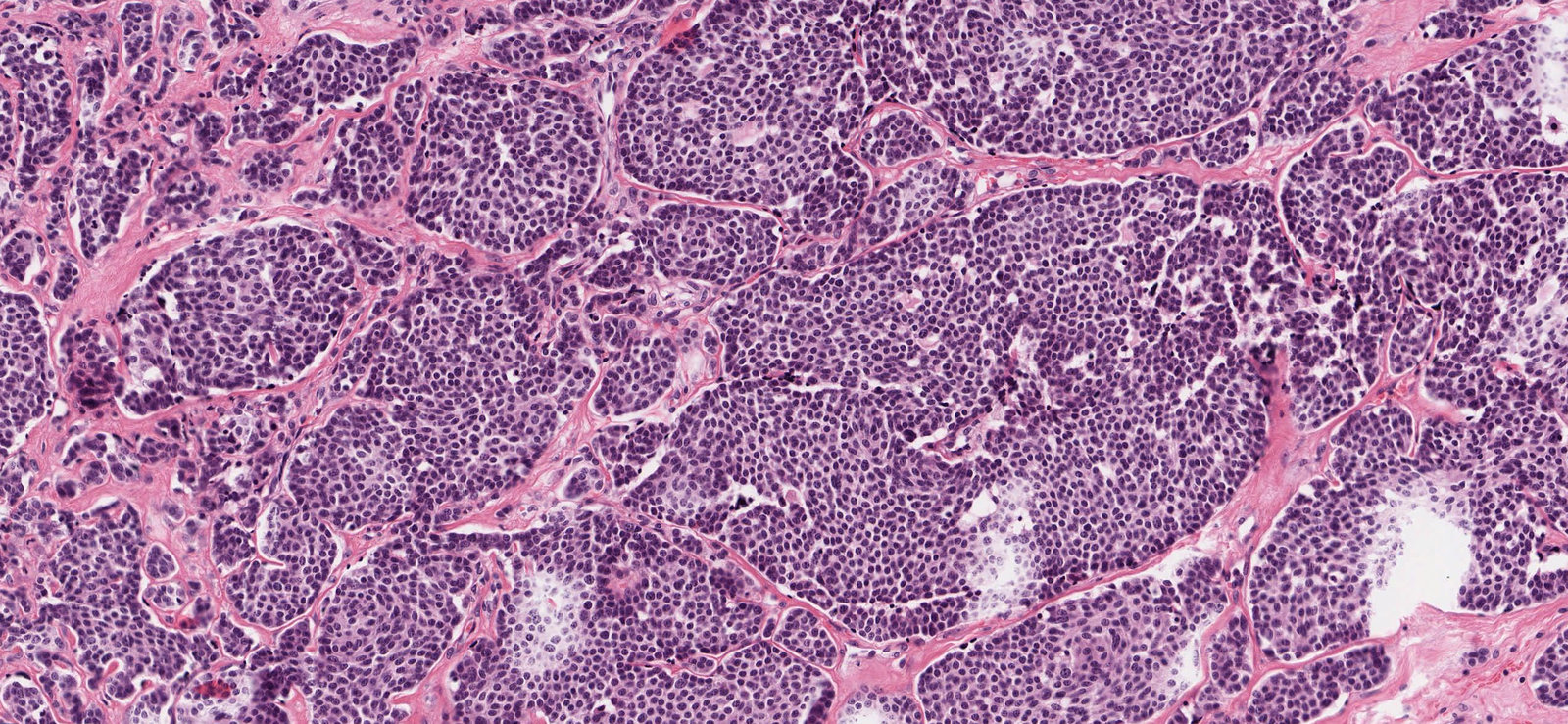
Photomicrograph of thyroid tissue (H&E stain, 300x magnification)
Green overlay: tumor cell nests
Black arrows: fibrous bands with prominent vascularity
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. med. Alberto Perez Bouza, Facharzt für Pathologie
Photomicrograph of thyroid tissue (H&E stain, 400x magnification)
Green overlay: amyloid deposits
Red: exemplary tumor cells
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. med. Alberto Perez Bouza, Facharzt für Pathologie
Subtypes and variants
-
Hurthle cell carcinoma
- 3–10% of all well-differentiated thyroid cancers
- Often classified as subtype of follicular carcinoma
-
Thyroid histopathology: hypercellularity with a predominance of Hurthle cells (large, polygonal epithelial cell with eosinophilic granular cytoplasm as a result of numerous altered mitochondria)
- Hurthle cells are nonspecific and also observed in Hashimoto thyroiditis, Graves disease, previously-irradiated thyroid glands, and in Hurthle cell adenoma (no vascular or capsular invasion; no metastasis)
- They are also found in the parathyroid glands, salivary glands, and kidneys
- B-cell lymphoma: usually develops from Hashimoto thyroiditis
- Sarcoma: rare
- Metastatic (e.g., breast, renal, melanoma): rare

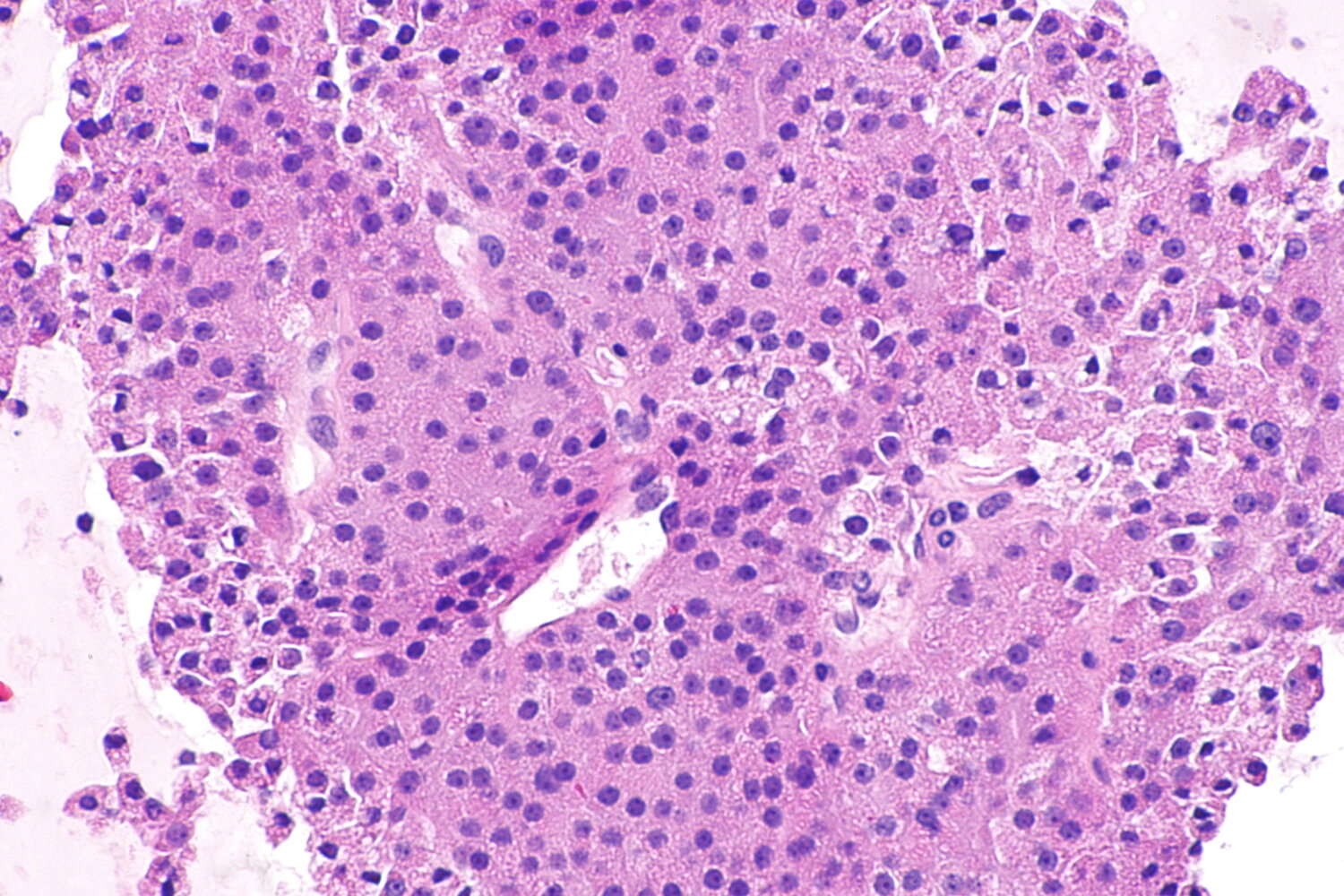
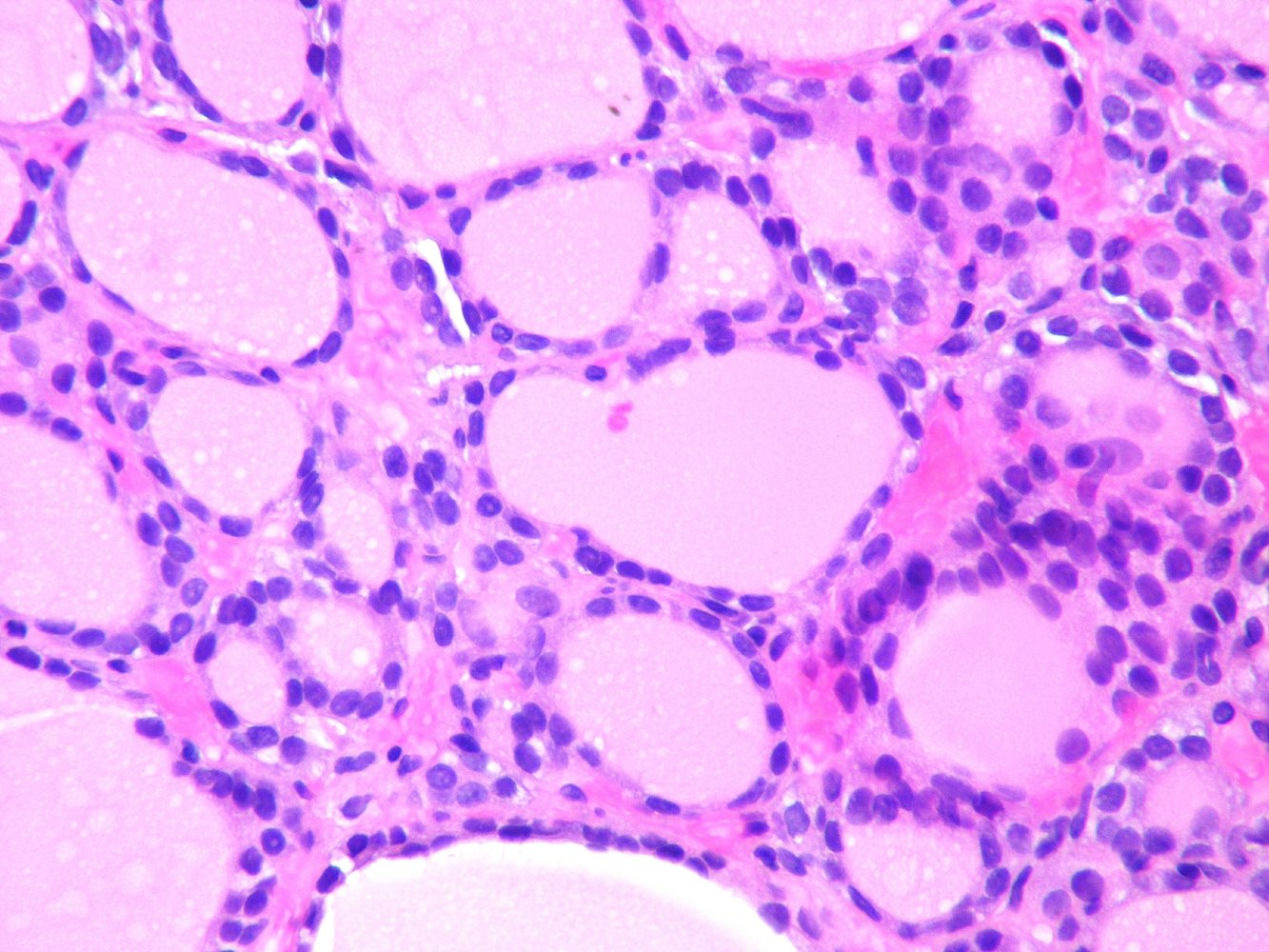
Photomicrograph of a thyroid tissue specimen (H&E stain; high magnification)
A cluster of cells with granular, eosinophilic cytoplasm is visible. The granular appearance is due to the large number of mitochondria. Nuclei (examples indicated by arrows) are round and centrally located, some with prominent nucleoli (examples indicated by arrowheads). The cells show no obvious signs of malignancy.
These features are characteristic of a Hurthle cell neoplasm (Hurthle cell adenoma or Hurthle cell carcinoma). Signs of invasion (e.g., capsular or vascular invasion, not shown in this picture) differentiate Hurthle cell carcinoma from adenoma.
Source: “File:Hurthle cell carcinoma -- high mag.jpg” by Librepath, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
{kind=link}
Clinical features
Thyroid carcinoma may be asymptomatic (e.g., thyroid incidentaloma) or manifest with any or all of the following clinical features: [10]
-
Thyroid nodule [11][12]
- Firm to hard consistency
- Typically painless
- See also “Red flags for thyroid cancer.”
-
Features of local infiltration or compression
- Fixed thyroid nodule [13][14]
- Recent onset of any of the following: [12]
- Hoarseness of voice (vocal cord paresis)
- Dyspnea
- Dysphagia
- Horner syndrome (rare) [15][16]
- Venous obstruction (very rare): IJV thrombosis, SVC syndrome [17][18]
-
Painless cervical lymphadenopathy [14]
- More common in papillary thyroid cancer and anaplastic thyroid cancer
- Less common in follicular thyroid cancer
-
Signs of distant metastasis [19]
- More common in follicular thyroid cancer and anaplastic thyroid cancer
- Less common in papillary thyroid cancer
- Examples include:
- Pulmonary metastases: coughing, hemoptysis, dyspnea
- Bone metastases: bone pain, pathologic fractures
- Brain metastases: focal neurologic deficit, seizures
- Paraneoplastic syndrome: diarrhea and facial flushing (typically seen in advanced medullary carcinoma) [8]




© AMBOSS
© AMBOSS

Photograph of the anterolateral aspect of the neck
The thyroid gland is diffusely enlarged in the region of the isthmus. A prominent nodule is visible in the right lateral aspect of the neck, which could be a nodule within the right lobe or a right lateral cervical lymphadenopathy.
Thyroid cancer typically manifests as a solitary, painless, firm to hard thyroid nodule with cervical lymphadenopathy. The diagnosis should be confirmed on cytological (i.e., fine-needle aspiration biopsy) or histopathological examination.
Source: "Thyroid cancer", John Campbell, Flickr licensed under Public Domain
Diagnosis
Approach [11][14]
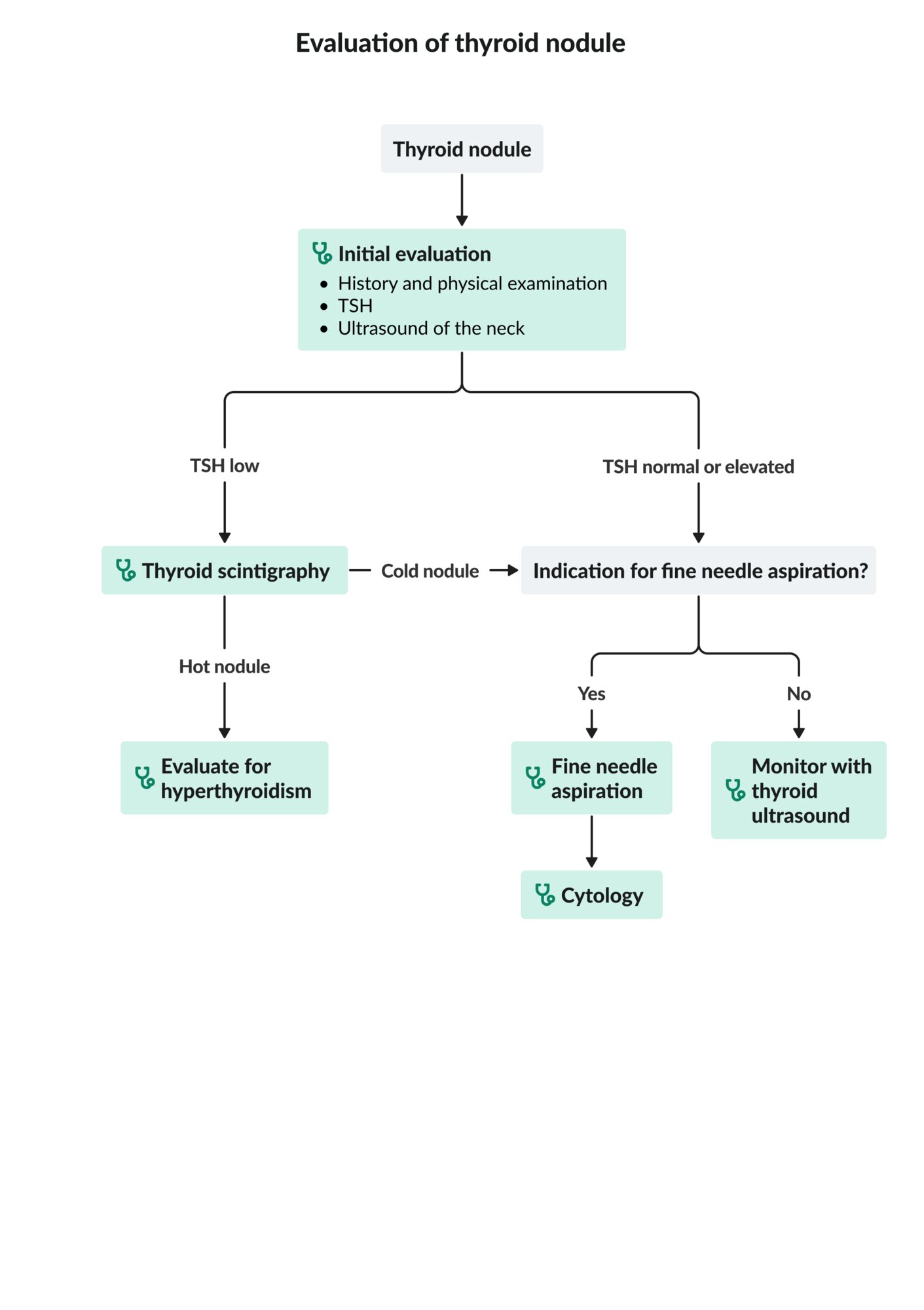
- For initial evaluation, follow the diagnostic approach to thyroid nodules.
- TSH, ultrasound, potentially scintigraphy
- Confirmation: fine-needle aspiration cytology (FNAC) or intraoperative frozen-section
-
Thyroid tumor markers help to estimate the prognosis and assess response to therapy.
- Differentiated thyroid cancer: serum thyroglobulin (Tg)
- Medullary carcinoma: serum calcitonin and carcinoembryonic antigen (CEA)
- Staging of lymph node and distant metastases
- Patients with medullary carcinoma require further assessment.
- Genetic testing for RET germline mutations [8]
- Screening of family members
- Screening for associated conditions (e.g., MEN2)

Initial evaluation
Laboratory studies and ultrasound
Serum TSH and ultrasound should be obtained in all patients with thyroid nodules.
- TSH: typically normal or mildly elevated [14]
-
Thyroid ultrasound: to assess for sonographic signs of thyroid malignancy ; [11][14]
- Solid or mostly solid hypoechoic nodule(s)
- Irregular margins
- Microcalcifications within nodules
- Nodules that are taller than wide
- Extrathyroidal growth





Thyroid scintigraphy [11]
-
Indications
- Thyroid nodule(s) with ↓ TSH levels
- Multinodular thyroids (to identify nodules that require FNAC)
- Prior to RAIA to evaluate eligibility for adjuvant treatment of well-differentiated thyroid cancer
- Contraindications: pregnant and breastfeeding women
- Supportive findings: decreased or no radiotracer uptake (i.e., hypofunctioning or nonfunctioning nodules, referred to as cold nodules) [20]


Nodules that appear hypoechoic on thyroid ultrasound and cold on thyroid scintigraphy should increase suspicion for malignancy.
Hyperfunctioning nodules (hot nodules) are rarely malignant and typically do not require further evaluation for malignancy. [11][21]
Confirmatory tests [11][14]
-
Fine-needle aspiration cytology (FNAC)
- Indications: sonographic signs of thyroid cancer detected on thyroid ultrasound (see “Indications for FNAC of thyroid nodules”)
- Supportive findings: typically reported as “malignant” or “suspicious for malignancy” according to the Bethesda system for thyroid cytopathology
- Intraoperative frozen-section: Consider if FNAC cannot reliably rule out malignancy in high-risk patients.
Additional studies after confirmed diagnosis
Thyroid cancer tumor markers
The specific tumor markers depend on the histological type of the cancer.
-
Follicular or papillary thyroid cancer
-
Thyroglobulin (Tg): precursor of thyroid hormones; produced exclusively by the thyroid gland [14]
- Indicated after total thyroidectomy or RAIA therapy
- Baseline (pretreatment) levels are not routinely indicated.
-
Thyroglobulin (Tg): precursor of thyroid hormones; produced exclusively by the thyroid gland [14]
-
Medullary carcinoma
-
Calcitonin: A hormone secreted by parafollicular cells, which is the tissue of origin of medullary carcinoma
- Indicated preoperatively if FNAC is suspicious for medullary carcinoma (supportive diagnostic marker) [8][11])
- Used to monitor response to therapy
- Carcinoembryonic antigen (CEA): nonspecific marker, used in combination with calcitonin to monitor response to therapy [8]
-
Calcitonin: A hormone secreted by parafollicular cells, which is the tissue of origin of medullary carcinoma
Elevation of tumor markers after total thyroidectomy or RAIA indicates persistent disease, recurrence, or metastasis.
Staging [14]
Staging includes evaluation for cervical lymph node metastases in all patients and of distant metastases as needed.
-
Preoperative assessment of cervical lymph nodes
- Neck ultrasound in all patients with confirmed diagnosis
- FNAC of lymph nodes with signs of metastases [14]
- Assessment of distant metastases: based on clinical suspicion [22]
- Chest x-ray or CT
- Bone scintigraphy
- CT or MRI head [23]
TSH: thyroid-stimulating hormone
© AMBOSS

Ultrasound thyroid (longitudinal plane)
A solid nodule in the upper pole has ill-defined margins and contains multiple microcalcifications.
The presence of microcalcifications increases suspicion for malignancy
Source: “Figure 1, in: Echogenic foci in thyroid nodules: diagnostic performance with combination of TIRADS and echogenic foci” by Su Min Ha, Yun Jae Chung, Hye Shin Ahn, Jung Hwan Baek, Sung Bin Park, BMC Medical Imaging, licensed under CC BY-SA 4.0. Modifications: removed arrow.
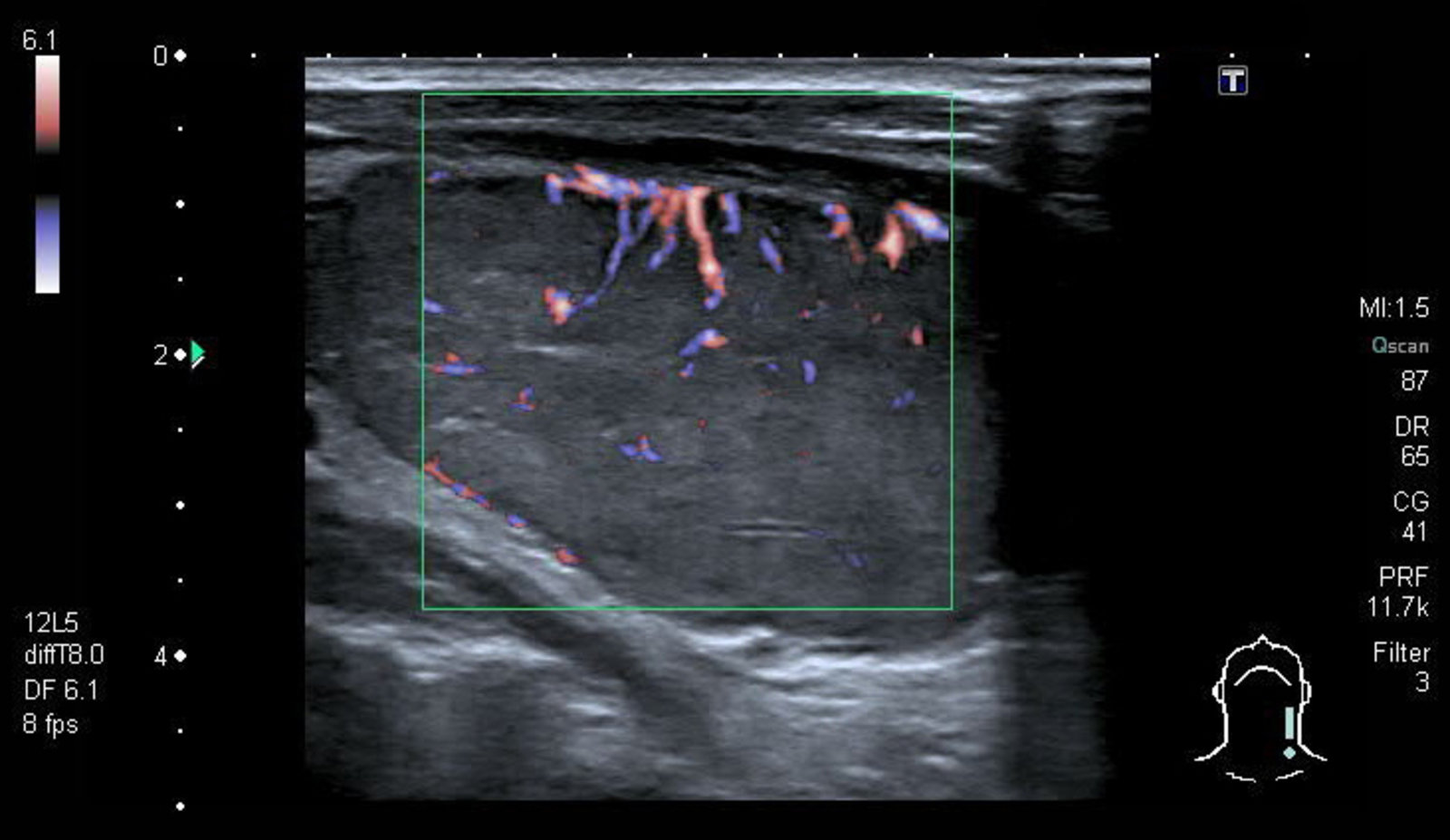
Ultrasound thyroid (left lobe; longitudinal plane; with color Doppler)
A solid circumscribed hypoechoic nodule is present in the left thyroid lobe. It does not contain microcalcifications. Color Doppler shows vascular flow. Fine needle aspiration (FNA) yielded a diagnosis of papillary carcinoma.
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
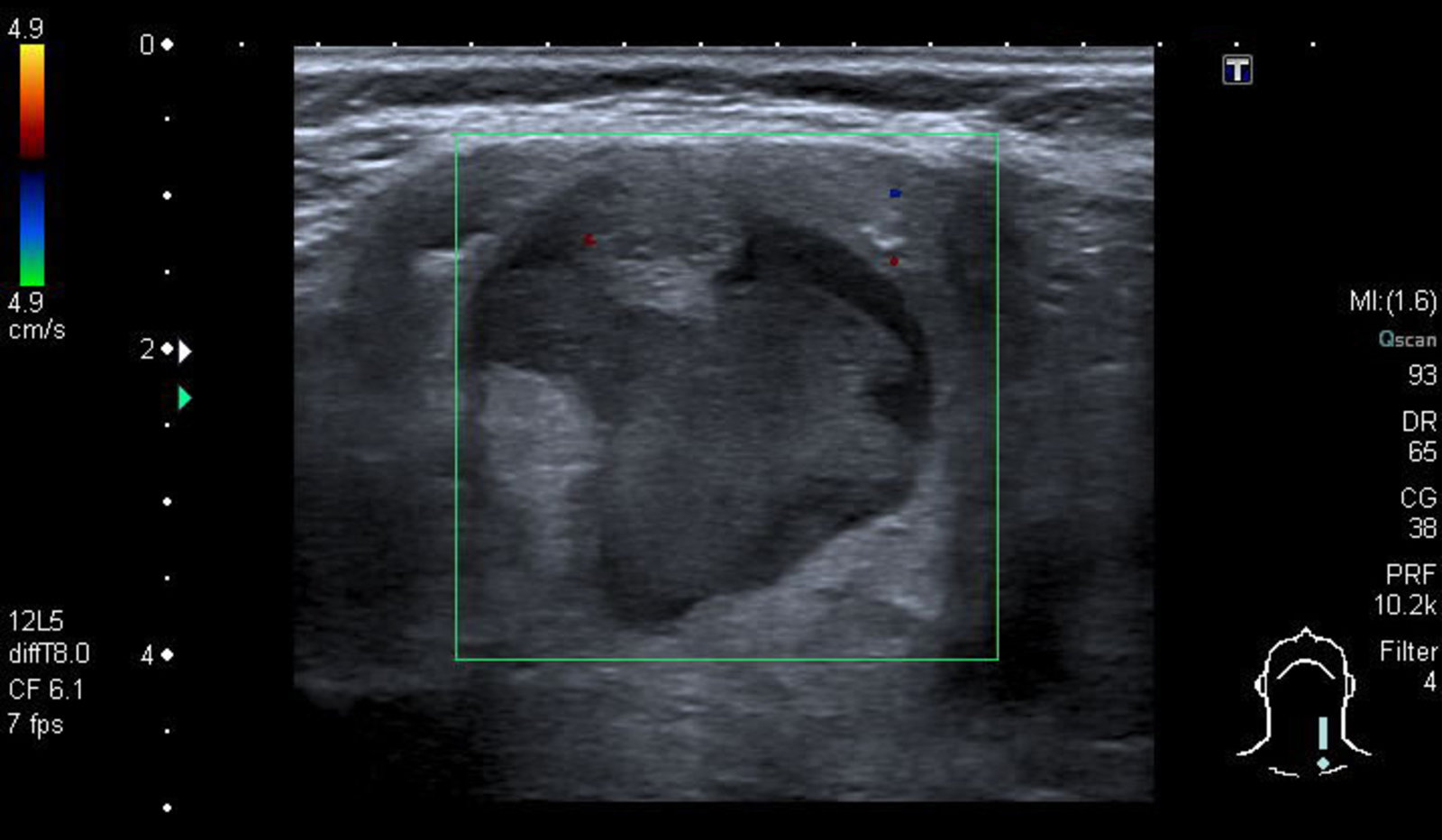
Ultrasound thyroid (left lobe; longitudinal plane)
A rounded mixed-echogenicity nodule with irregular (lobulated) margins contains hypoechoic (green overlay), isoechoic, and hyperechoic (hatched green overlay) components.
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
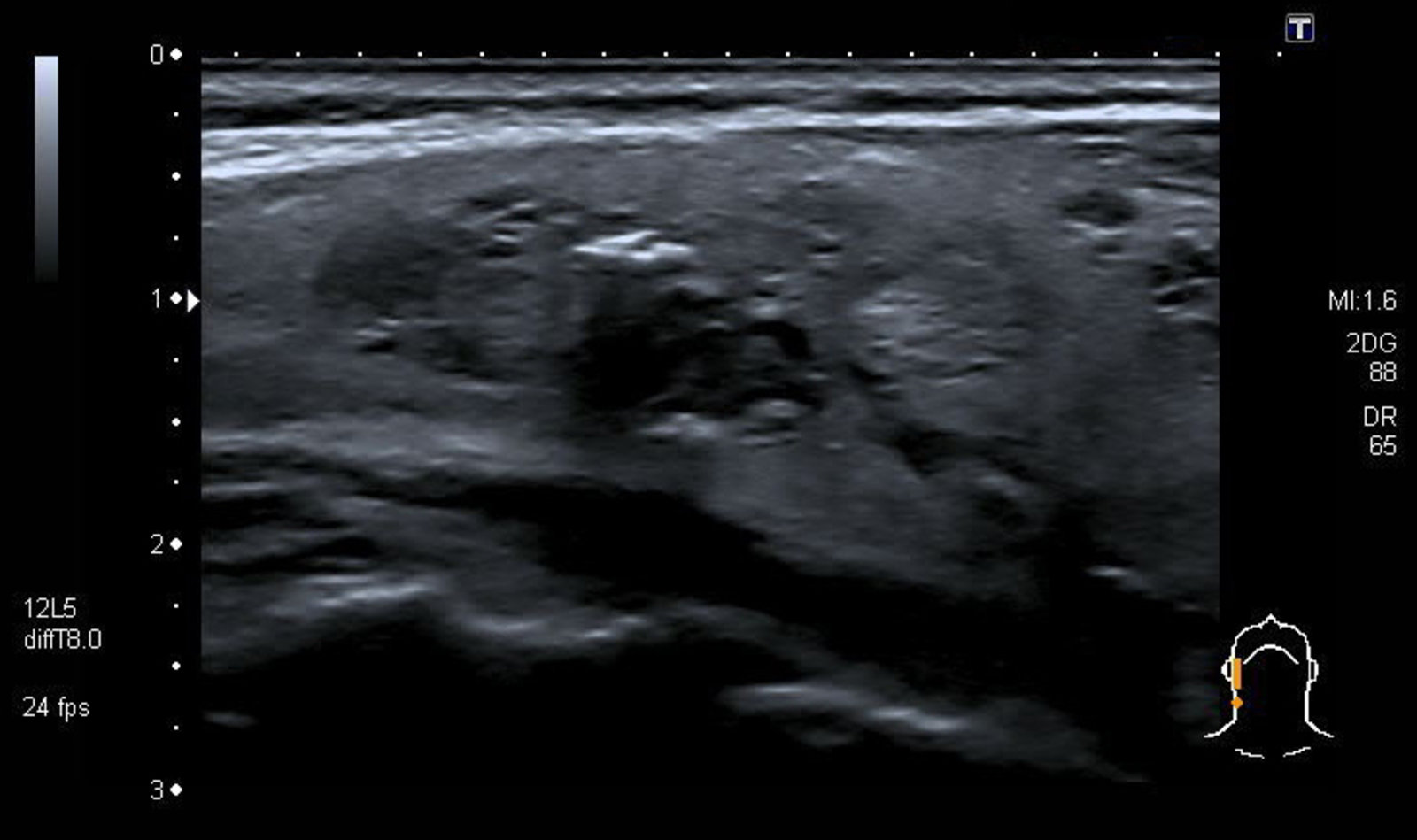
Ultrasound thyroid (right lobe; longitudinal plane)
A heterogeneous thyroid nodule (white overlay) has hypoechoic (red overlay) and slightly hyperechoic (green overlay) components. Microcalcifications (arrowheads) are present along the periphery of the hypoechoic component.
Features of this lesion are suspicious for malignancy; fine needle aspiration (FNA) is, therefore, required.
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
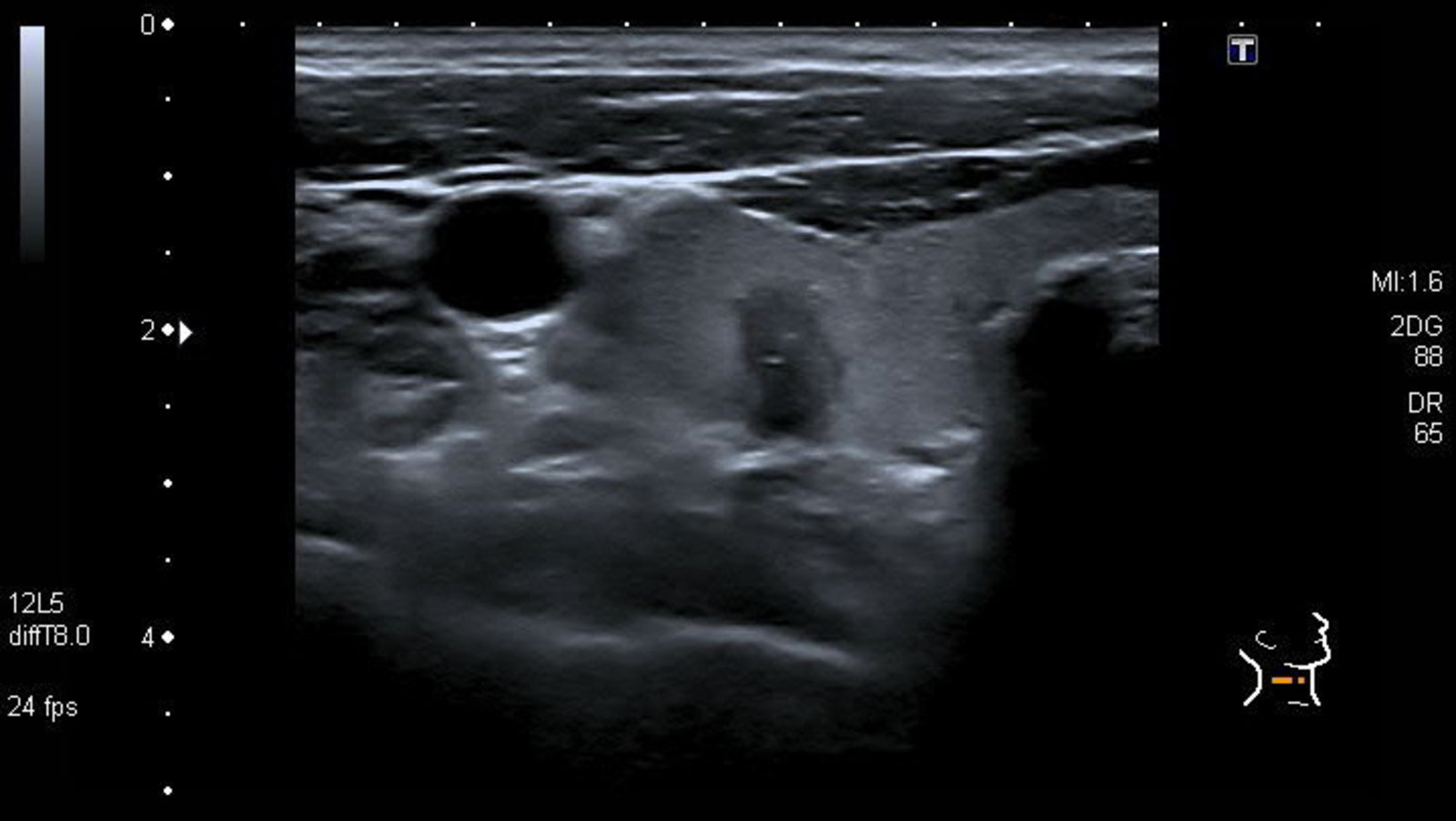
Ultrasound thyroid (right lobe; transverse plane)
An irregular hypoechoic nodule (green hatched overlay with green outline) with solid and cystic components is present in the mid-right lobe (white outline). The nodule is taller-than-wide and contains small echogenic microcalcifications (indicated by arrows and white overlays).
CCA: common carotid artery; T: trachea; I: isthmus
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
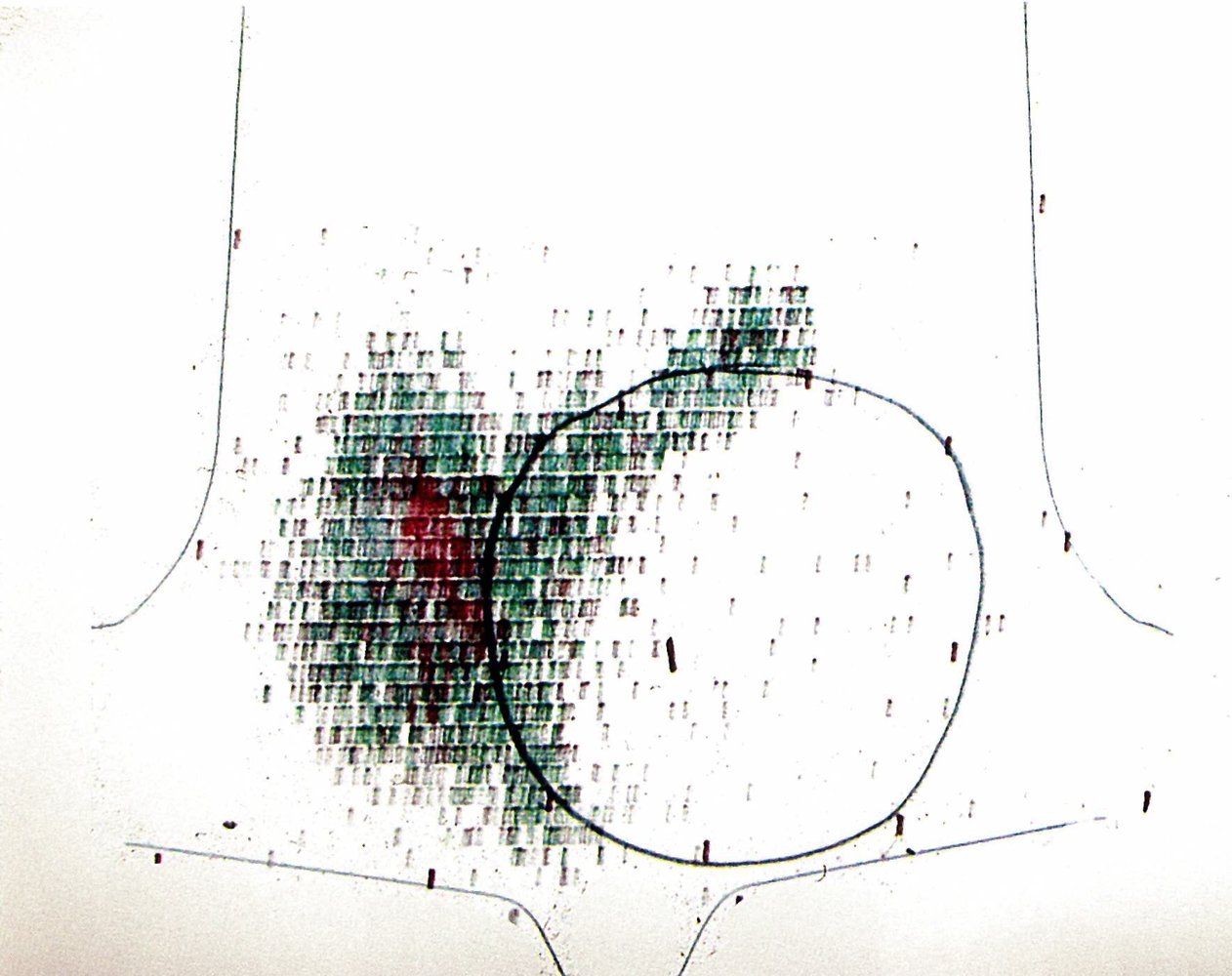
A large cold nodule (black circle) is visible within the left thyroid lobe as an area of decreased radiotracer uptake. Radiotracer uptake by the rest of the thyroid gland appears normal.
A cold nodule is associated with a higher risk of malignancy and warrants further workup (e.g., FNA if there are additional sonographic signs of malignancy on thyroid ultrasound).
Source: © IMPP
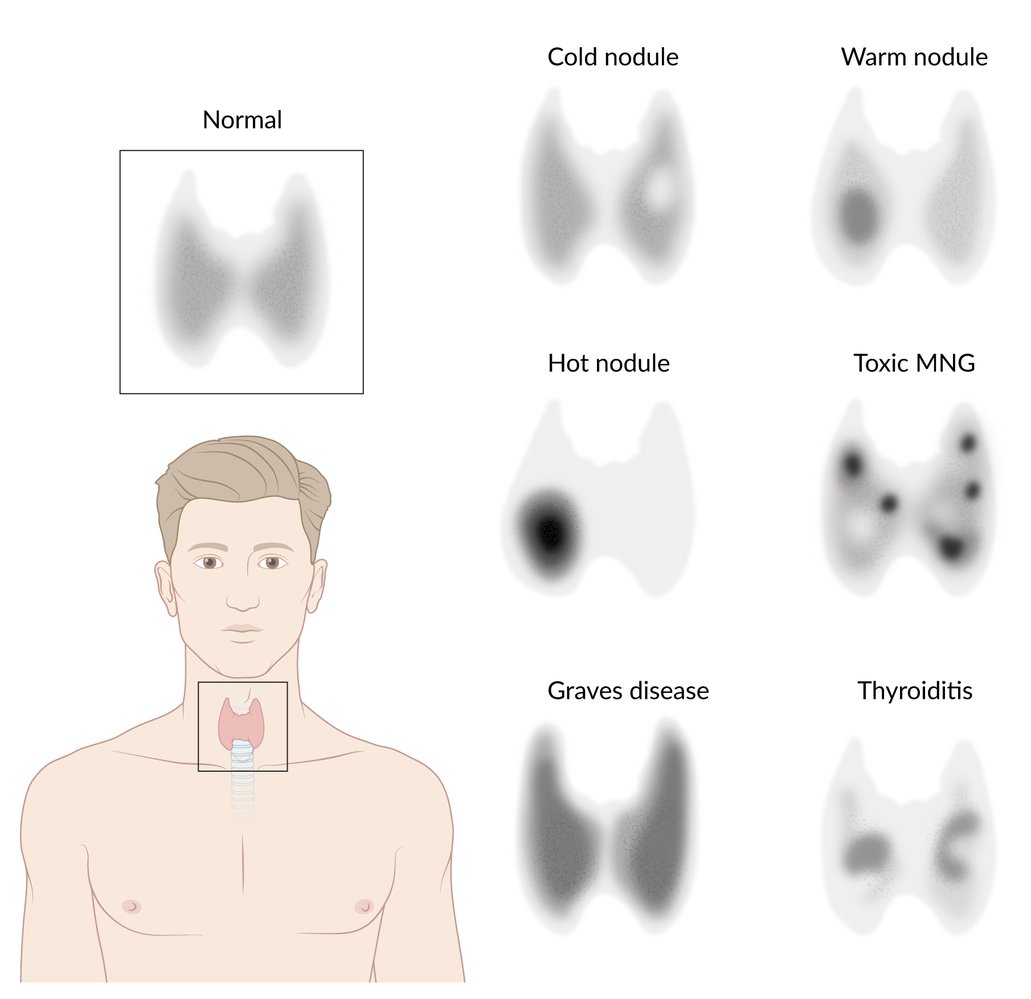
Overview of radioactive iodine uptake patterns in hyperthyroidism
Toxic MNG: Toxic multinodular goiter
© AMBOSS
Pathology
Papillary thyroid cancer
Psammoma bodies
- Morphology: concentric lamellar calcifications
-
Occurrence: seen in diseases associated with calcific degeneration
- Papillary thyroid carcinomas (evidence of psammoma bodies in thyroid tissue should always raise suspicion of malignancy)
- Serous papillary cystadenocarcinoma of ovary and endometrium
- Meningiomas
- Mesotheliomas

“Orphan Annie” eyes nuclei
- Morphology: empty-appearing large oval nuclei with central clearing
-
Occurrence
- Papillary thyroid carcinomas
- Autoimmune thyroiditis (e.g., Hashimoto disease, Grave disease)
Nuclear grooves [24]
- Morphology: longitudinal invaginations of nuclear bilayer
- Occurrence: papillary thyroid carcinomas
“Papi and Moma adopted Orphan Annie:” papillary thyroid cancer is histologically characterized by psammoma bodies and Orphan Annie-eye nuclei.

Follicular carcinoma
- Uniform follicles
- Vascular and/or capsular invasion

Medullary carcinoma
- Ovoid cells of C cell origin and therefore without follicle development
- Amyloid in the stroma (stains with Congo red)

Medullary carcinoma is composed of C-cells producing Calcitonin and is characterized by amyloid aCCumulation staining with Congo red.
Anaplastic thyroid carcinoma
- Undifferentiated giant cell (i.e., osteoclast-like cell)
- Areas of necrosis and hemorrhage

Histopathology slide of the ovary (H&E stain)
In addition to papillary tumor cells, there are two Psammoma bodies located in the lower left corner of the image (red overlay). Psammoma bodies are concentric, lamellar calcifications, which are characteristic for serous tumors of the ovary.
Source: © IMPP
Micrograph image of thyroid tissue (H&E stain, 400x magnification)
Arrowheads: examples of pathological nuclei
Blue overlay: connective tissue core of papillae
Yellow dashed overlay: epithelial cancer cells covering the papillae
Yellow overlay: psammoma bodies
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. med. Alberto Perez Bouza, Facharzt für Pathologie
Photomicrograph of a thyroid tissue sample (H&E stain; high magnification)
Psammoma bodies are concentric lamellar calcifications that are often seen within papillary thyroid carcinomas.
Other tumors with frequent presence of psammoma bodies include serous carcinoma of the ovary, high-grade serous carcinoma of the uterus, and meningiomas.
Source: “Psammoma body Papillary thyroid carcinoma magnx400.jpg” by Eriugen, Wikimedia commons, licensed under CC BY-SA 4.0.
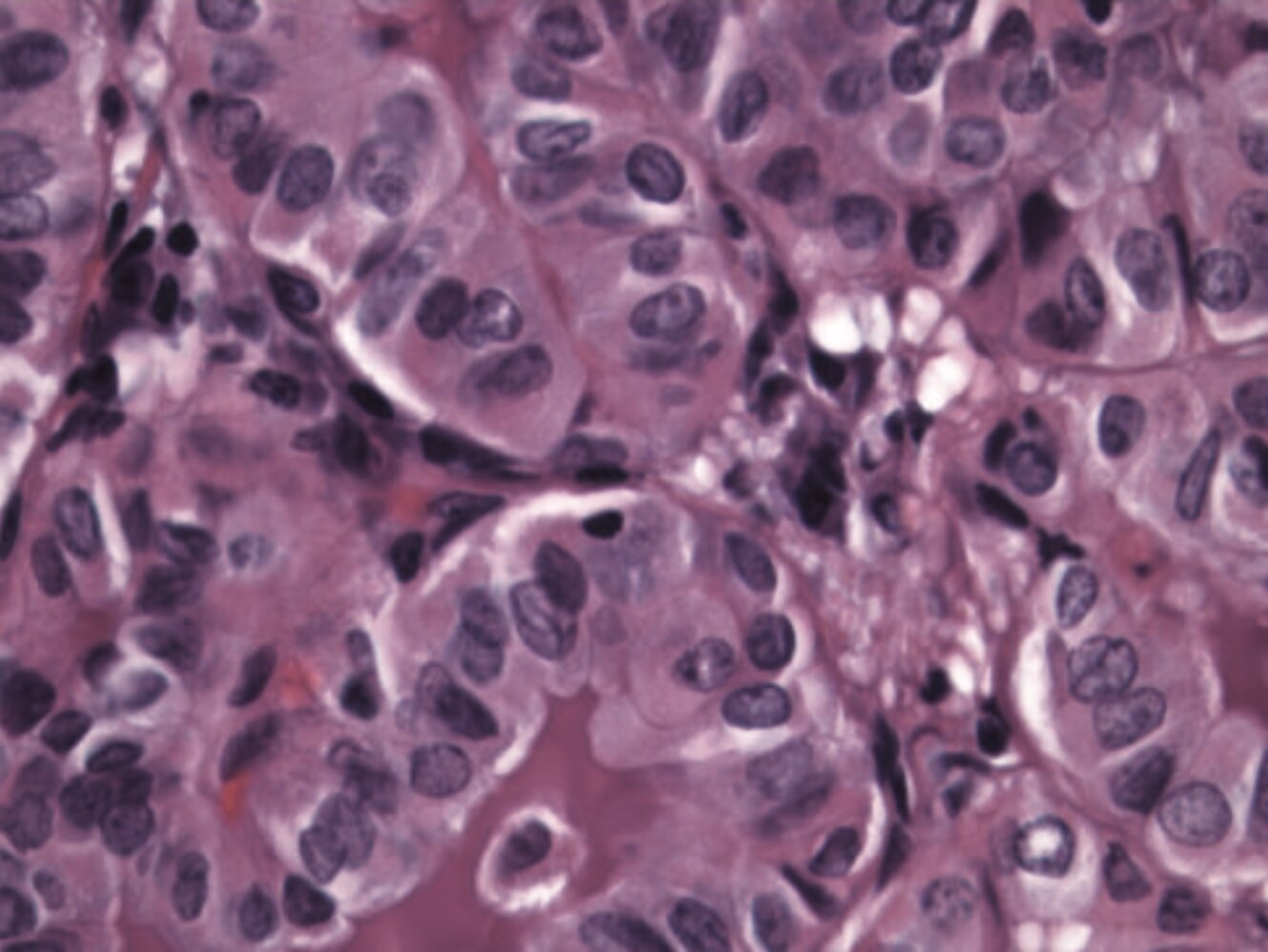
Photomicrograph of a thyroid tumor tissue sample (H&E stain; high magnification)
Cells arranged in a papillary architecture are visible (examples indicated by green overlay). Some cell nuclei appear invaginated (nuclear grooves), giving them a coffee-bean appearance (examples indicated by white lines). The nuclei in general show pale staining centrally and powdery chromatin in the periphery (Orphan Annie-eye nuclei; example highlighted by red overlay).
These nuclear changes in a thyroid tumor with papillary architecture confirm the diagnosis of papillary thyroid carcinoma.
Source: “Fig. 3, in: Papillary Thyroid Cancer in a Child with Progressive Transformation of Germinal Centers” by Suresh Mohan, Bradley DeNardo, Dariusz Stachurski, Jennifer Greene Welch, Jan C. Groblewski, Case Reports in Otolaryngology, vol. 2016, Article ID 6469073, 5 pages, 2016. https://doi.org/10.1155/2016/6469073, licensed under CC BY 4.0. Modifications: Image was cropped.. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Micrograph of a histological section of thyroid (H&E stain).
Multiple uniform follicles of similar sizes with an absence of papillary nuclear features. Additionally, these lesions must demonstrate capsular or vascular invasion.
This appearance is typical of a well differentiated follicular thyroid cancer.
Source: “Metastatic follicular thyroid carcinoma - Case 264” by Yale Rosen, Flickr, licensed under CC BY-SA 2.0.
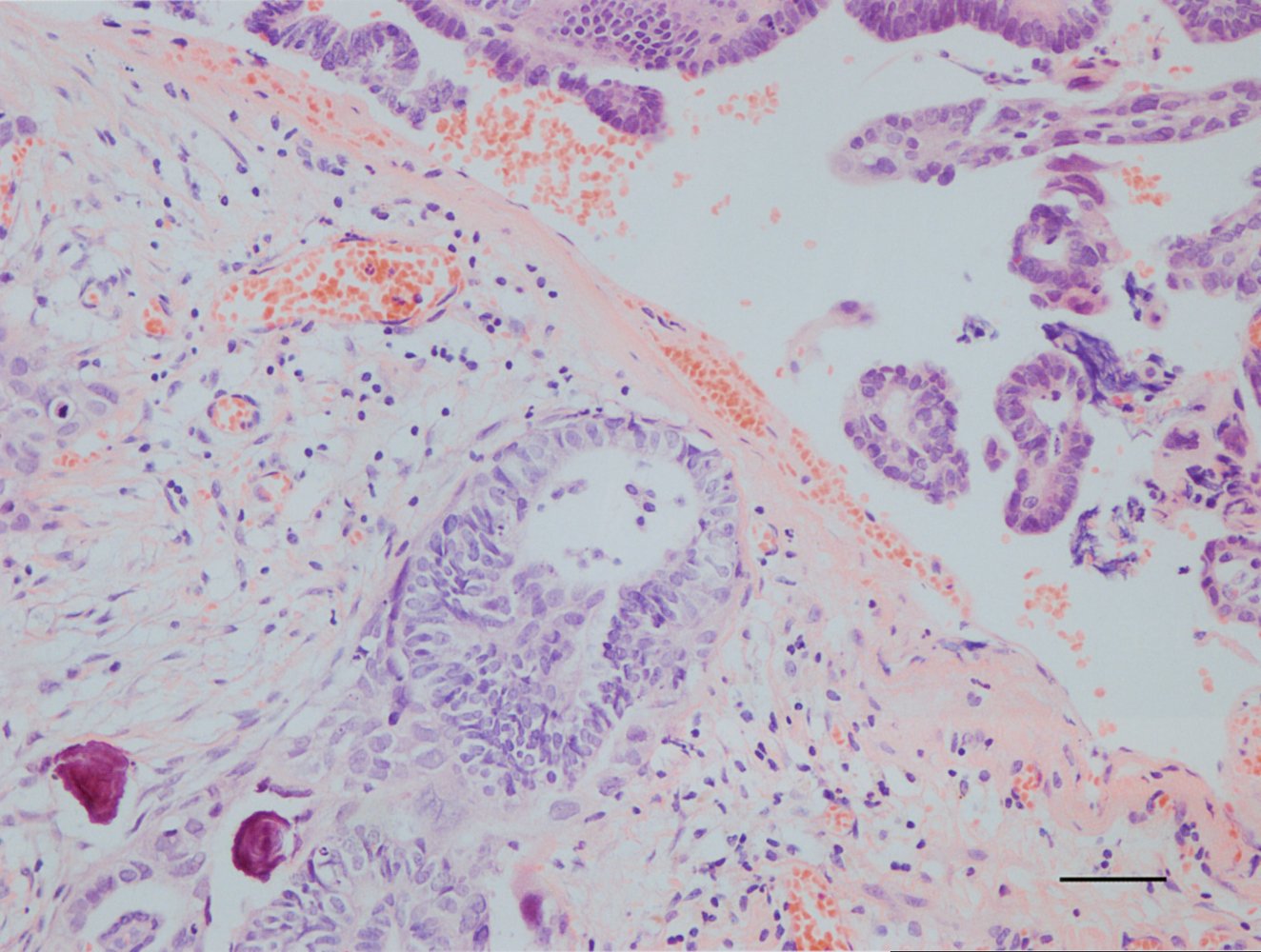
Photomicrograph of a thyroid tissue specimen (H&E stain; low magnification)
A partly encapsulated (capsule marked by hatched blue overlay) thyroid lesion comprised of follicles of varying size and shape (blue overlay) can be seen. Focally, this lesion displays a capsular invasion (yellow overlay), which is diagnostic of follicular thyroid carcinoma.
Source: “Follicular thyroid carcinoma 2 -- low mag” by Nephron, Wikimedia Commons, licensed under CC BY-SA 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 4.0.
Photomicrograph of thyroid tissue (H&E stain, 400x magnification)
Green overlay: amyloid deposits
Red: exemplary tumor cells
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. med. Alberto Perez Bouza, Facharzt für Pathologie
Photomicrograph of thyroid tissue (H&E stain, 300x magnification)
Green overlay: tumor cell nests
Black arrows: fibrous bands with prominent vascularity
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. med. Alberto Perez Bouza, Facharzt für Pathologie
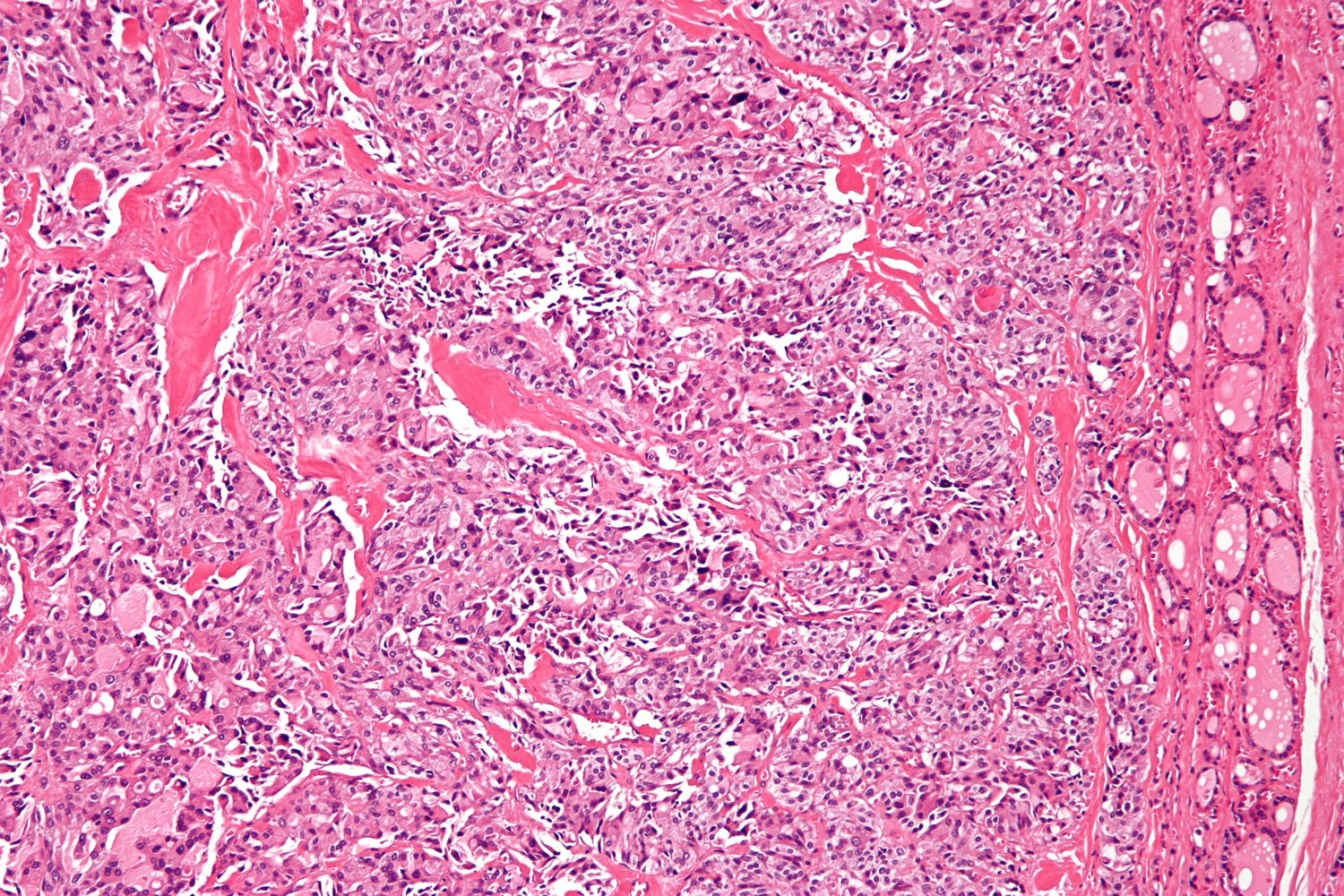
Photomicrograph of thyroid tissue (H&E stain)
There is a very dense conglomeration of parafollicular cells arranged in nests and clusters (examples indicated by dashed circles). Amyloid is visible in the stroma as amorphous, pink, hyaline material (examples indicated by green overlays).
These are typical histological findings in medullary thyroid carcinoma.
Source: “Medullary thyroid carcinoma - intermed mag” by Nephron, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
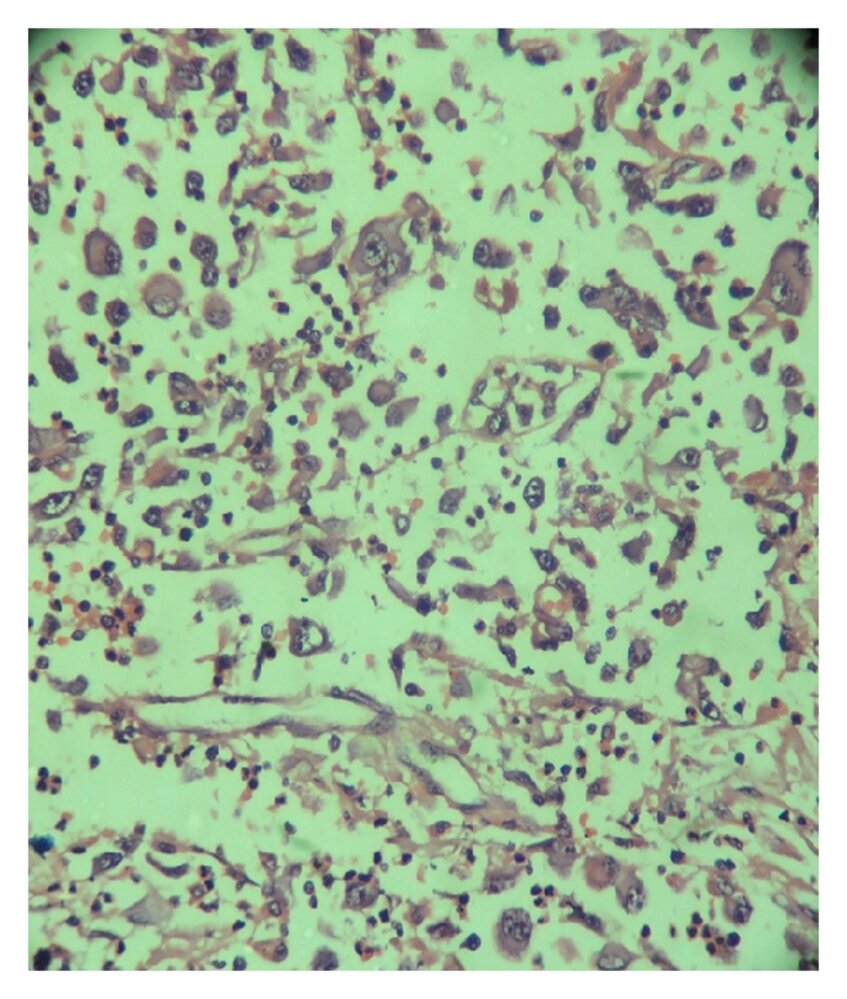
Photomicrograph of a fine-needle aspiration from a thyroid lesion (H&E stain; medium magnification)
Highly pleomorphic cells (examples indicated by blue overlay) with enlarged, irregular nuclei that have prominent nucleoli (examples indicated by arrows) are visible. Multinucleated tumor cells (examples indicated by yellow overlay) can also be seen. There are no follicular or papillary growth patterns.
The diagnosis of an anaplastic thyroid carcinoma is a diagnosis of exclusion. This patient's diagnosis was supported by immunohistochemical findings (negative for TTF-1, thyroglobulin, and calcitonin).
Source: “Figure 1, in: A Rare Case of a Synchronous Anaplastic Carcinoma Thyroid with Ductal Carcinoma Breast” by S. Ghosh, P. B. Ananda Rao, S. Sarkar, Hindawi - Case Reports in Oncological Medicine, licensed under CC BY 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Differential diagnoses
- See the article “Thyroid nodules.”
-
Thyroid cyst
-
Ultrasound findings
- Anechoic round mass
- In many cases, dorsal acoustic enhancement
- Relatively frequent and typically harmless
-
Ultrasound findings
The differential diagnoses listed here are not exhaustive.
Treatment
General principles [8][14][23]
-
Well-differentiated thyroid cancer [8][14]
- Standard management (regardless of nodal or distant metastases): total thyroidectomy (with neck dissection as needed) + RAIA + TSH suppression therapy
- Small cancers without nodal or distant metastases: Consider hemithyroidectomy + TSH suppression therapy.
- Papillary microcarcinoma in low-risk patients : Consider active surveillance.
-
Poorly-differentiated thyroid cancer
- Medullary carcinoma: total thyroidectomy + neck dissection ± radiation therapy and/or systemic chemotherapy as needed. [8]
-
Anaplastic carcinoma [23]
- Resectable cancer: total thyroidectomy + neck dissection + radiochemotherapy
- Unresectable or metastatic cancer: palliative care
RAIA and TSH suppression therapy are not useful in the management of medullary carcinoma or anaplastic thyroid cancer. [8][23]
Surgery [14]
Surgical resection is the primary treatment for thyroid cancer. For further information on preoperative testing and complications see “Thyroid surgery.”
Total thyroidectomy
-
Indications
-
Well-differentiated thyroid carcinoma
- Tumor size ≥ 4 cm
- Tumor size 1–4 cm (individual decision)
- With/without extrathyroidal extension
- With/without nodal or distant metastases [14]
- Medullary carcinoma [8]
- Resectable anaplastic thyroid cancer [23]
-
Well-differentiated thyroid carcinoma
-
Important considerations
- Total thyroidectomy should be combined with neck dissection as needed (e.g., in patients with regional lymph node spread).
-
Thyroid hormone replacement is required in all patients who undergo total thyroidectomy.
- Maintain TSH within the physiological range for poorly-differentiated thyroid cancer. [8]
- TSH-suppressive therapy is required for well-differentiated thyroid cancer. [14]
Hemithyroidectomy [14]
-
Indications
-
Small, well-differentiated thyroid carcinoma with all of the following characteristics:
- Intrathyroidal tumors (i.e., no evidence of extrathyroidal extension)
- No nodal or distant metastasis
- No high-risk patient factors such as age > 45 years, history of head and neck radiation, or family history of cancer
- Preferred option in tumors < 1 cm in size with all of the above characteristics
- An alternative to total thyroidectomy in tumors 1–4 cm in size with all of the above characteristics
-
Small, well-differentiated thyroid carcinoma with all of the following characteristics:
-
Contraindications
- Intrathyroidal tumor ≥ 4 cm
- Extrathyroidal spread
- Distant or nodal metastasis
- High-risk patient factors
Complications [25]
- Hypocalcemia: as a result of accidental removal of parathyroid glands [26]
-
Dysphonia (hoarseness) and/or dysphagia: as a result of transection of the superior and recurrent laryngeal nerve
- May occur during ligation of the superior laryngeal artery and inferior thyroid artery due to the proximity of the nerves to the arteries
- If only the external branch of the superior laryngeal nerve is damaged, complete loss of the voice is unlikely, but a loss of vocal range may occur (with potentially career-damaging consequences for, e.g., singers and actors).
- Vocal cord function should be assessed preoperatively with laryngoscopy.
Adjuvant therapy [14]
-
Well-differentiated thyroid cancer
- Radioactive iodine ablation (RAIA): conducted 4– 6 weeks after total thyroidectomy to destroy remaining thyroid tissue or metastases [11]
-
TSH suppression therapy:
- Administration of L-thyroxine to suppress serum TSH to subnormal levels to minimize the risk of tumor recurrence
- Administered after completion of RAIA in patients who have undergone total thyroidectomy
- L-thyroxine also serves as hormone replacement therapy after surgery and RAIA.
- Poorly differentiated thyroid cancer: adjuvant radiation therapy and/or chemotherapy as needed [8][23]
Nonoperative management
-
Active surveillance [14]
- Papillary microcarcinoma (i.e., a tumor < 1 cm in diameter) with no nodal or distant metastasis in low-risk patients [27]
- Multimorbid patients with high surgical risk or short life expectancy
- Palliative therapy: Palliative radiation therapy and/or chemotherapy may be considered for advanced anaplastic thyroid cancer. [23]
Follow-up
- Physical examination
- Biochemical tests
- Neck ultrasound
- Further imaging, if a relapse is suspected
References:[14]
Prognosis
| Thyroid cancer | 5-year survival rate |
|---|---|
| Papillary | > 90% |
| Follicular | 50–70% |
| Medullary | 50% |
| Anaplastic | 5–14% |
External Resources
- 2020 AAES Guidelines for the Definitive Surgical Management of Thyroid Disease
- 2016 AACE/ACE/AME Guidelines for the Diagnosis and Management of Thyroid Nodules
- 2015 ATA Guidelines for the Management of Thyroid Nodules and Differentiated Thyroid Cancer
- 2015 ATA Revised Guidelines for the Management of Medullary Thyroid Carcinoma
- 2021 ATA Guidelines for the Management of Anaplastic Thyroid Cancer
- US Preventive Services Task Force recommendations (Thyroid Cancer)
References
- "Cancer Stat Facts: Thyroid Cancer". https://seer.cancer.gov/statfacts/html/thyro.html. [2017-01-26]
- Rahbari R, Zhang L, Kebebew E. "Thyroid cancer gender disparity.". Future Oncol. 6(11). :1771-9. (2010)
- Veiga LH, Lubin JH, Anderson H, et al. "A pooled analysis of thyroid cancer incidence following radiotherapy for childhood cancer". Radiat Res. 178(4). :365-376. (2012)
- Russ G, Leboulleux S, Leenhardt L, Hegedüs L. "Thyroid Incidentalomas: Epidemiology, Risk Stratification with Ultrasound and Workup". Eur Thyroid J. 3(3). :154-163. (2014)
- Gharib H, Papini E, Garber JR, et al. "American Association of Clinical Endocrinologists, American College of Endocrinology, and Associazione Medici Endocrinologi Medical Guidelines for clinical practice for the diagnosis and management of thyroid nodules-2016 update". Endocr Pract. 22(5). :622-39. (2016)
- Durante C, Grani G, Lamartina L, et al. "The Diagnosis and Management of Thyroid Nodules: A Review". JAMA. 319(9). :914-924. (2018)
- Popoveniuc G, Jonklaas J. "Thyroid nodules.". Med Clin North Am. 96(2). :329-49. (2012)
- Haugen BR, Alexander EK, Bible KC, et al. "2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer". Thyroid. 26(1). :1-133. (2016)
- Donaldson JF, Rodriguez-Gomez IA, Parameswaran R. "Rapidly enlarging neck masses of the thyroid with Horner's syndrome: a concise clinical review". Surgeon. 13(2). :110-5. (2015)
- Broome JT, Gauger PG, Miller BS, Doherty GM. "Anaplastic thyroid cancer manifesting as new-onset Horner syndrome.". Endocr Pract. 15(6). :563-6
- Bukhari H, Ayad M, Rosenthal A, Block M, Cortelli M. "Superior vena cava syndrome secondary to thyroid cancer". J Surg Case Rep. 2011(7). :7. (2011)
- Hyer SL, Dandekar P, Newbold K, et al. "Thyroid cancer causing obstruction of the great veins in the neck". World J Surg Oncol. 6. :36. (2008)
- Nixon IJ, Whitcher MM, Palmer FL, et al. "The Impact of Distant Metastases at Presentation on Prognosis in Patients with Differentiated Carcinoma of the Thyroid Gland". Thyroid. 22(9). :884-889. (2012)
- Wells SA, Asa SL, Dralle H, et al. "Revised American Thyroid Association Guidelines for the Management of Medullary Thyroid Carcinoma". Thyroid. 25(6). :567-610. (2015)
- Gharib H, Papini E. "Thyroid nodules: clinical importance, assessment, and treatment". Endocrinol Metab Clin North Am. 36(3). :707-35, vi. (2007)
- Mirfakhraee S, Mathews D, Peng L, Woodruff S, Zigman JM. "A solitary hyperfunctioning thyroid nodule harboring thyroid carcinoma: review of the literature". Thyroid Res. 6(1). :7. (2013)
- King AD. "Imaging for staging and management of thyroid cancer". Cancer Imaging. 8(1). :57-69. (2008)
- Smallridge RC, Ain KB, Asa SL, et al. "American Thyroid Association guidelines for management of patients with anaplastic thyroid cancer". Thyroid. 22(11). :1104-39. (2012)
- Batistatou A, Scopa CD. "Review articles: Pathogenesis and diagnostic significance of nuclear grooves in thyroid and other sites". Int J Surg Pathol. 17(2). :107-110. (2008)
- Patel KN et al. "The American Association of Endocrine Surgeons Guidelines for the Definitive Surgical Management of Thyroid Disease in Adults". Ann Surg. 271(3). :e21-e93. (2020)
- Campos NS, Cardoso LP, Tanios RT, et al. "Risk factors for incidental parathyroidectomy during thyroidectomy". Brazilian Journal of Otorhinolaryngology. 78(1). :57-61. (2012)
- Bradly DP, Reddy V, Prinz RA, Gattuso P. "Incidental papillary carcinoma in patients treated surgically for benign thyroid diseases". Surgery. 146(6). :1099-1104. (2009)
- Nagaiah G, Hossain A, Mooney CJ, Parmentier J, Remick SC. "Anaplastic thyroid cancer: a review of epidemiology, pathogenesis, and treatment". J Oncol. (2011)
- Limaiem F, Rehman A, Mazzoni T. "Papillary Thyroid Carcinoma". StatPearls. (2021)
- Ashorobi D, Lopez PP. "Follicular Thyroid Cancer". StatPearls. (2021)
- Chintakuntlawar AV, Ryder M, Bible KC. "Anaplastic Thyroid Cancer and Primary Thyroid Lymphoma". Elsevier. :246-254.e3. (2021). ISBN: 9780323661270
- Stamatakos M, Paraskeva P, Stefanaki C, et al. "Medullary thyroid carcinoma: The third most common thyroid cancer reviewed.". Oncology letters. 2(1). :49-53. (2011)