Summary
Thyroid nodules are abnormal growths within the thyroid gland. They are present in approximately 50% of the general population but only palpable in 5–10% of the population. They are more common in women, especially in iodine-deficient regions, and their incidence increases with age. Thyroid nodules are the clinical manifestation of various underlying thyroid diseases. The majority of them are benign (∼ 95%), with colloid cysts, follicular adenomas, and Hashimoto thyroiditis being the most common causes. Approximately 5% of thyroid nodules are malignant, with papillary carcinoma being the most common form of malignant disease. A thyroid incidentaloma is a nodule that is discovered during imaging for an unrelated cause and should be evaluated in the same way as other nodules. The initial evaluation of all thyroid nodules includes a TSH assay and thyroid ultrasound. Sonographic signs of thyroid cancer should be further evaluated with fine-needle aspiration cytology (FNAC). Identification of a follicular neoplasm on FNAC necessitates further diagnostic evaluation with either molecular testing or surgical excision and histopathology because cytology cannot reliably distinguish between a follicular adenoma and a follicular carcinoma. A radioiodine uptake scan (thyroid scintigraphy) is used to evaluate nodules in patients with low TSH levels. Based on their iodine uptake on radioiodine scans, thyroid nodules can be categorized as autonomous/hot (increased uptake) or nonfunctional/cold (decreased uptake). The most common hot nodules are toxic adenomas and dominant nodules of toxic multinodular goiters. With a 5–15% risk of malignancy, cold nodules are clinically significant. Treatment depends on the underlying etiology and includes, e.g., surgery (thyroidectomy) for malignant and autonomous nodules, aspiration for thyroid cysts, and observation for small, benign nodules.
Epidemiology
- Sex: ♀ > ♂ (4:1)
- Incidence: increases with age [1]
- Geographic distribution: most common in inland regions without iodine fortification programs, where iodine content in food and water is low
References:[2]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
Benign thyroid nodules (∼ 95% of cases)
-
Thyroid adenomas
- Follicular adenoma (most common)
- Hürthle cell adenoma
- Toxic adenoma
- Papillary adenoma (least common)
- Thyroid cysts
- Dominant nodules of multinodular goiters
- Hashimoto thyroiditis
Malignant thyroid nodules (∼ 5% of cases)
-
Types
- Thyroid carcinoma
- Thyroid lymphoma
- Metastatic cancer from breast/renal carcinoma (rare)
-
Red flags for thyroid cancer ; [3][4][5]
- Patient characteristics
- Male sex
- Age: < 14 years or > 70 years [3]
- History of radiation to the head or neck
-
Family history of:
- MEN2 syndrome
- Differentiated thyroid cancer (i.e., papillary, follicular, or medullary thyroid cancer)
- Gardner syndrome
- Symptoms
- Rapid growth of thyroid nodule
- Recent onset of persistent hoarseness, dysphagia, or dyspnea
- Palpatory findings
- Firm or hard nodule
- Fixed nodule
- Cervical lymphadenopathy
- Patient characteristics
In addition to red flags for thyroid cancer, a solid nodule on thyroid ultrasound or a cold nodule on thyroid scintigraphy should raise suspicion for thyroid cancer.
Diagnostics
Approach [3][6][7]
- All thyroid nodules (including thyroid incidentalomas) should be evaluated for malignancy. [8]
- Initial tests in all patients: TSH levels and thyroid ultrasound [9]
-
Subsequent tests
- Thyroid scintigraphy for patients with low TSH
- Cytology if ultrasound examination shows indications for FNAC in thyroid nodules
-
Additional tests
- Diagnostic workup of hyperthyroidism or hypothyroidism (e.g., fT4, total T3, thyroid antibodies)
- Thyroid cancer tumor markers (e.g., serum calcitonin for suspected medullary carcinoma) [3]

Initial evaluation [3][6][9]
-
Serum TSH: may be normal, elevated, or low
- Elevated TSH: associated with a higher risk of malignancy in thyroid nodules
- Low TSH: indication for thyroid scintigraphy
-
Thyroid ultrasound:
- Indicated in patients with palpable nodules or if there is clinical suspicion of malignancy
- Assess each nodule individually for risk features.
| Sonographic evaluation of thyroid nodules [6] | ||
|---|---|---|
| Overview | Risk pattern | Ultrasound findings |
| Sonographic signs of thyroid malignancy | High risk |
|
| Intermediate risk |
|
|
| Sonographic signs of benign thyroid nodules | Low risk |
|
| Very low risk |
|
|
| Benign |
|
|
Thyroid ultrasound is not a screening test for the general population. It is indicated as initial test for patients with palpable thyroid nodules or clinical suspicion for thyroid malignancy. [3]
Solid, hypoechoic nodules with irregular margins, microcalcifications, taller-than-wide shape, extrathyroidal growth, and/or cervical lymphadenopathy should raise suspicion for malignancy and require further evaluation with FNAC.



Subsequent evaluation
Thyroid scintigraphy [3][10]
- Indication: thyroid nodule(s) in a patient with low TSH
- Contraindications: pregnant and breastfeeding women
-
Findings and interpretation
- Cold nodule (hypofunctioning nodule): Evaluate for indications for FNAC of thyroid nodules with ultrasound.
-
Hot nodule (hyperfunctioning nodule): rarely malignant, FNAC not recommended [11]
- Solitary hot nodule: toxic adenoma
- Multiple hot nodules: toxic multinodular goiter [12]



Malignancy is rare in hyperfunctioning (hot) nodules. [11]
Fine-needle aspiration cytology (FNAC) [3][6]
-
Indications for FNAC of thyroid nodules
- Solid hypoechoic nodules ≥ 1 cm with/without additional sonographic signs of thyroid cancer
-
Consider for solid hypoechoic nodules < 1 cm if any of the following are present:
- Extrathyroidal growth
- Cervical lymphadenopathy
- Symptoms suggestive of distant metastases
- Patient preference for FNAC over observation
- Partly cystic, isoechoic, and hyperechoic nodules ≥ 1.5 cm (low-risk pattern)
- Consider in spongiform or partly cystic nodule ≥ 2 cm (very low-risk pattern).
-
Procedure
- Thyroid cells are obtained using a fine (e.g., 25-gauge) needle, and then observed under a microscope. [3]
- Multiple nodules may require FNAC depending on their sonographic appearance.
- Findings: categorized according to the Bethesda system for thyroid cytopathology
If thyroid scintigraphy is performed, sonographic features of thyroid nodules should be used to determine which cold nodules require FNAC. Cold nodules with a benign appearance on thyroid ultrasound do not routinely require FNAC.
| Bethesda system for thyroid cytopathology [13] | |
|---|---|
| Diagnostic category | Management [6] |
| I: Nondiagnostic or unsatisfactory |
|
| II: Benign |
|
| III: Atypia or follicular lesion of undetermined significance |
|
| IV: Follicular neoplasm or suspicious for follicular neoplasm |
|
| V: Suspicious for malignancy |
|
| VI: Malignant | |
TSH: thyroid-stimulating hormone
© AMBOSS
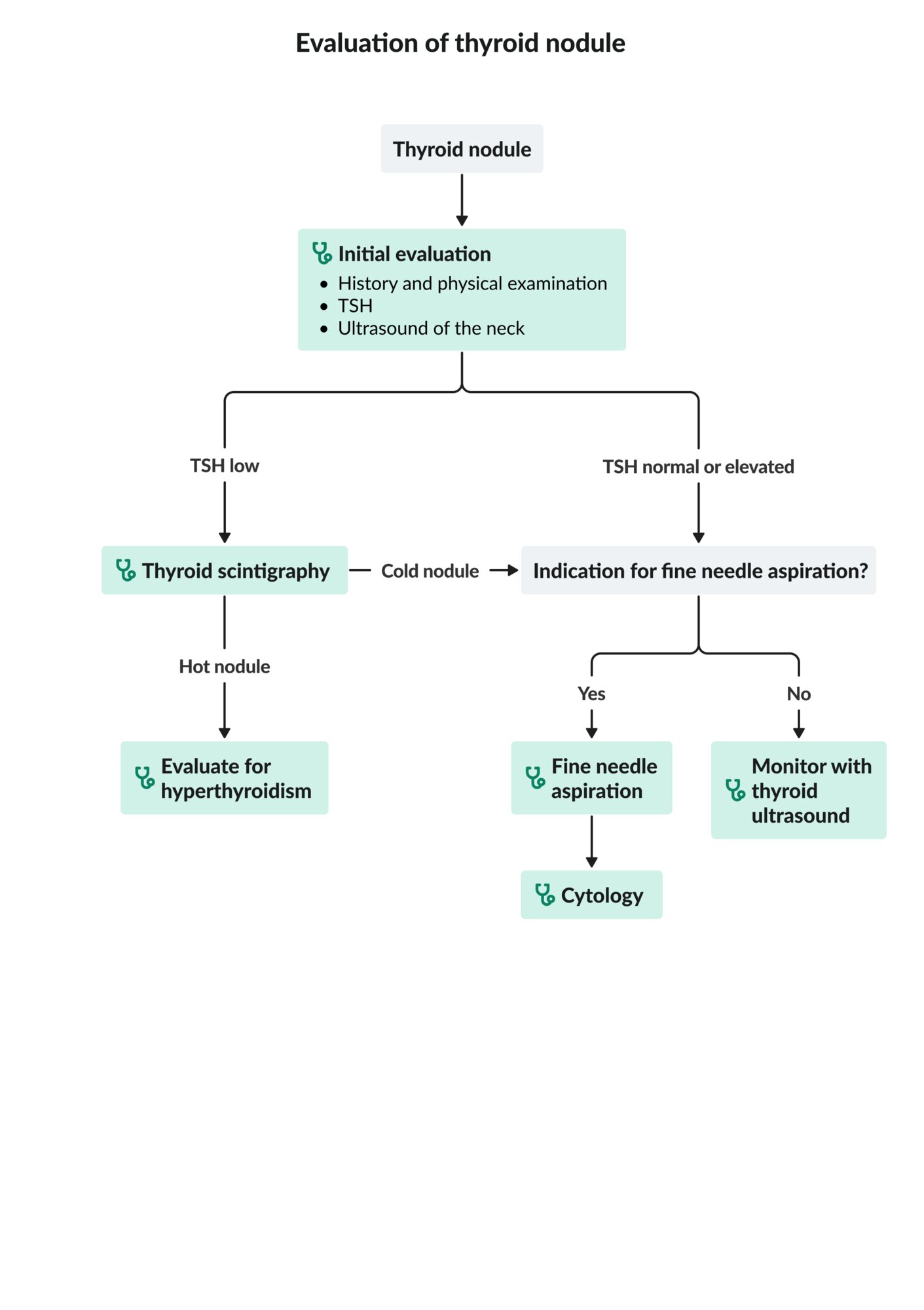
Ultrasound thyroid (left lobe; longitudinal plane)
A rounded mixed-echogenicity nodule with irregular (lobulated) margins contains hypoechoic (green overlay), isoechoic, and hyperechoic (hatched green overlay) components.
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
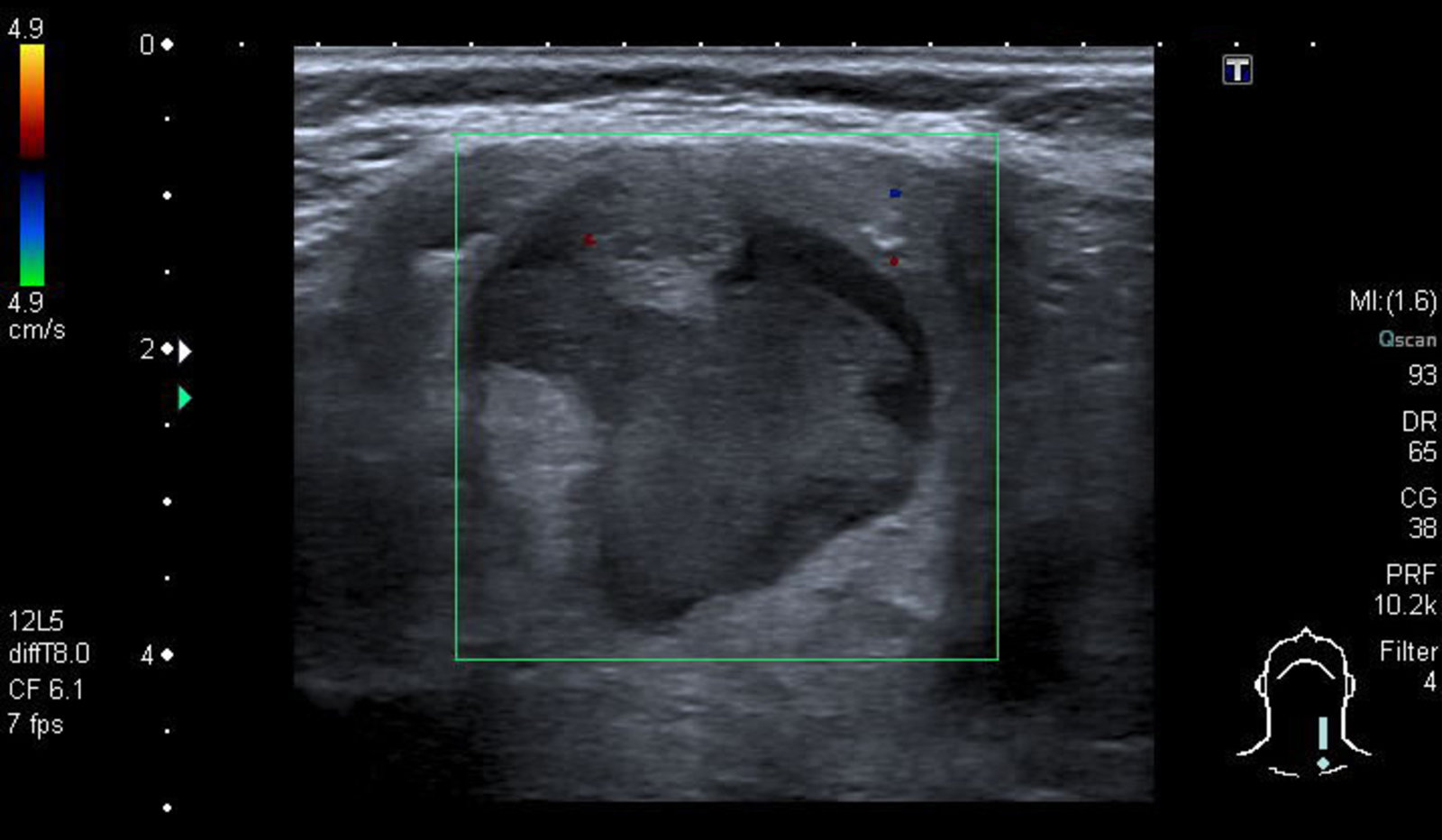
Ultrasound thyroid (left lobe; longitudinal plane; with color Doppler)
A solid circumscribed hypoechoic nodule is present in the left thyroid lobe. It does not contain microcalcifications. Color Doppler shows vascular flow. Fine needle aspiration (FNA) yielded a diagnosis of papillary carcinoma.
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
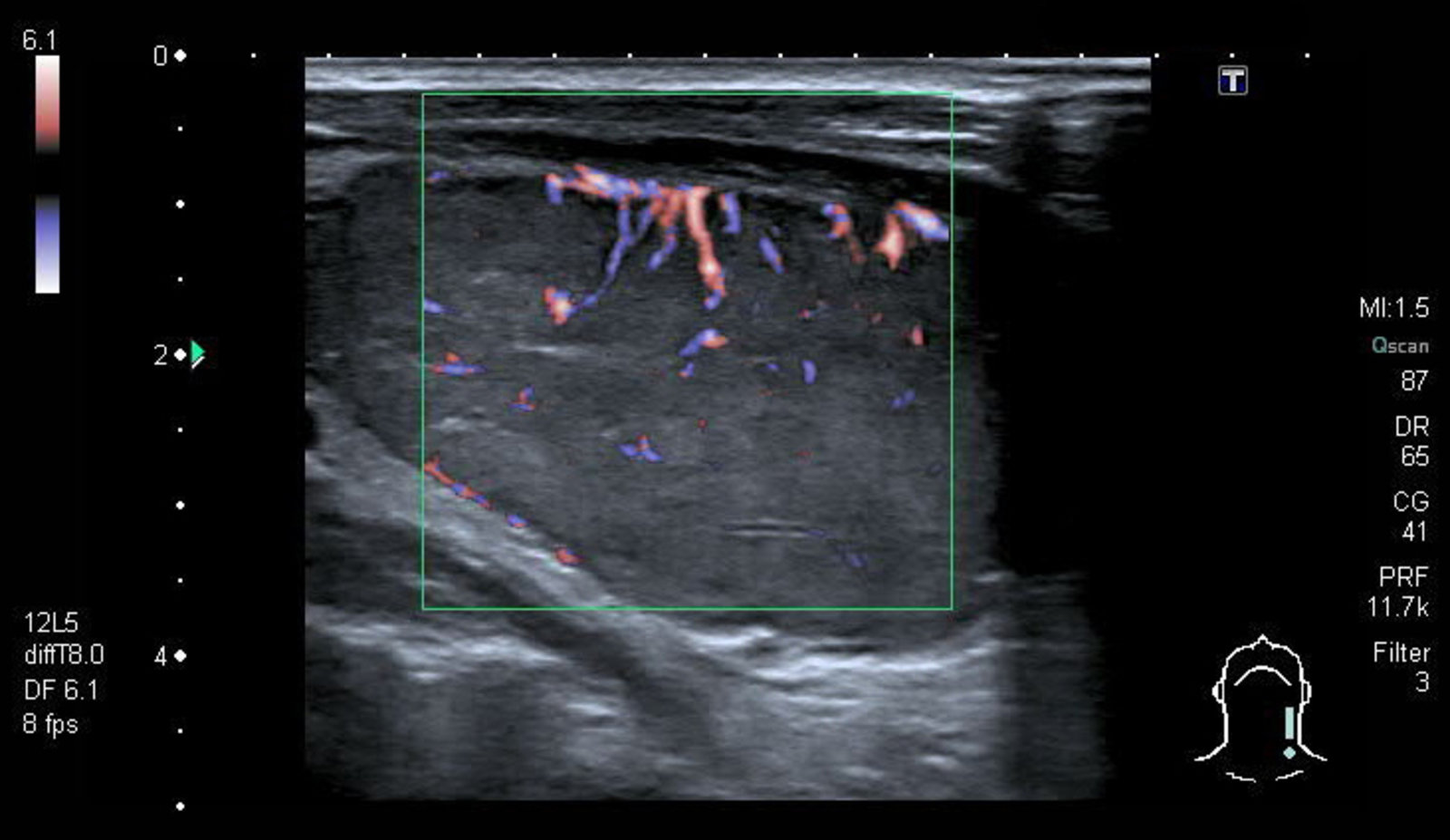
Ultrasound thyroid (right lobe; longitudinal plane)
A heterogeneous thyroid nodule (white overlay) has hypoechoic (red overlay) and slightly hyperechoic (green overlay) components. Microcalcifications (arrowheads) are present along the periphery of the hypoechoic component.
Features of this lesion are suspicious for malignancy; fine needle aspiration (FNA) is, therefore, required.
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
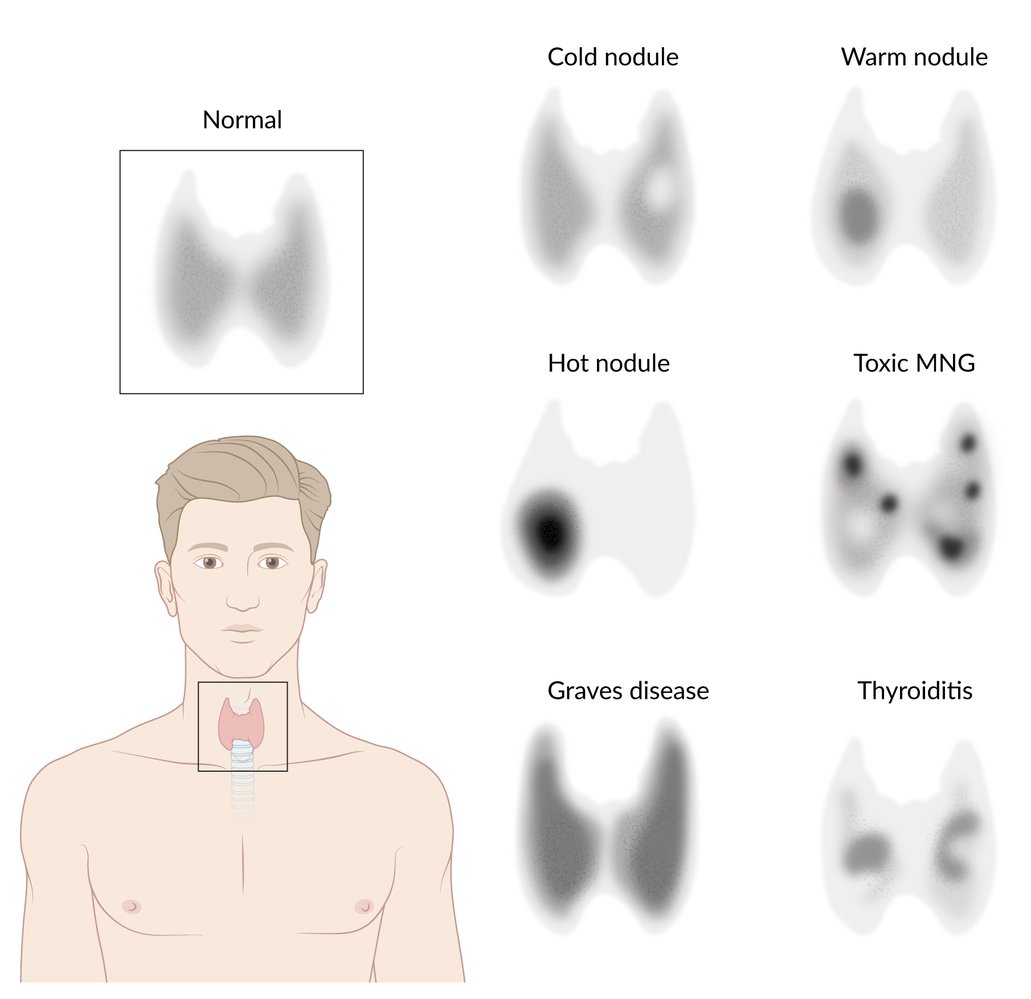
Overview of radioactive iodine uptake patterns in hyperthyroidism
Toxic MNG: Toxic multinodular goiter
© AMBOSS

Nuclear medicine thyroid scintigraphy (Tc-99m pertechnetate)
The rounded area in the right thyroid lobe represents a so-called hot thyroid nodule, which shows increased radioisotope uptake compared to the rest of the thyroid gland.
Source: “Figure 1. in: Papillary Thyroid Carcinoma Development after Radioactive Iodine Treatment for Toxic Adenoma” by El Bez I, Ben Sellem D, Bannour S, Mhiric A and Slim I, Clinics in Oncology, licensed under CC BY 4.0. Modifications: image cropped.
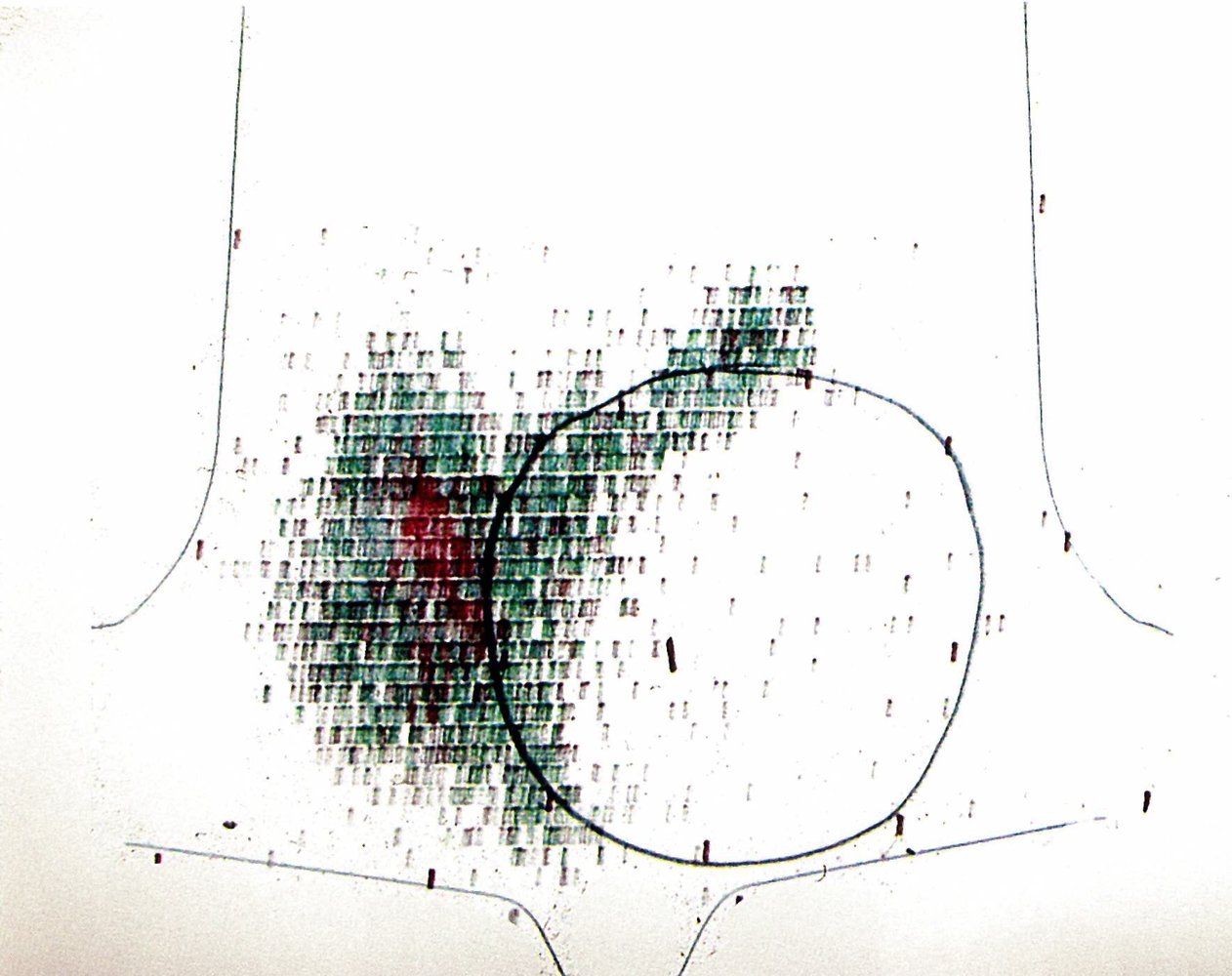
A large cold nodule (black circle) is visible within the left thyroid lobe as an area of decreased radiotracer uptake. Radiotracer uptake by the rest of the thyroid gland appears normal.
A cold nodule is associated with a higher risk of malignancy and warrants further workup (e.g., FNA if there are additional sonographic signs of malignancy on thyroid ultrasound).
Source: © IMPP
Follicular adenoma
Epidemiology
- Follicular adenoma is the most common type of thyroid adenoma. [9]
- 10–15% of follicular neoplasms are malignant.
Clinical features [9]
- Often presents as a slow-growing solitary nodule
- Patients are typically euthyroid.
- In rare cases, patients can manifest with clinical features of hyperthyroidism (∼ 1% of follicular adenomas develop into toxic adenomas). [14]
Diagnostics [6]
Follicular adenoma is a histopathological diagnosis. Cytology alone cannot distinguish between adenoma and carcinoma. For the initial workup, see “Diagnostic approach to thyroid nodules”.
- Thyroid function tests: TSH is typically normal.
- Thyroid ultrasound: may show sonographic signs of malignancy or appear benign
-
FNAC
- Follicular neoplasm or follicular lesion of undetermined significance
- Cannot distinguish between follicular adenoma and carcinoma
-
Confirmatory test
- Surgical excision (e.g., hemithyroidectomy) with histologic analysis [7][9]
- Findings: normal follicular structure with no tumor invasion into the surrounding tissues (e.g., capsule, blood vessels).

Treatment [9]
- Thyroid surgery is always indicated, both for definitive diagnosis and treatment.
- Initial surgical excision shows no evidence of cancer: no further treatment required
- If follicular cancer is identified on histopathology: completion thyroidectomy and adjuvant treatment of thyroid cancer as needed
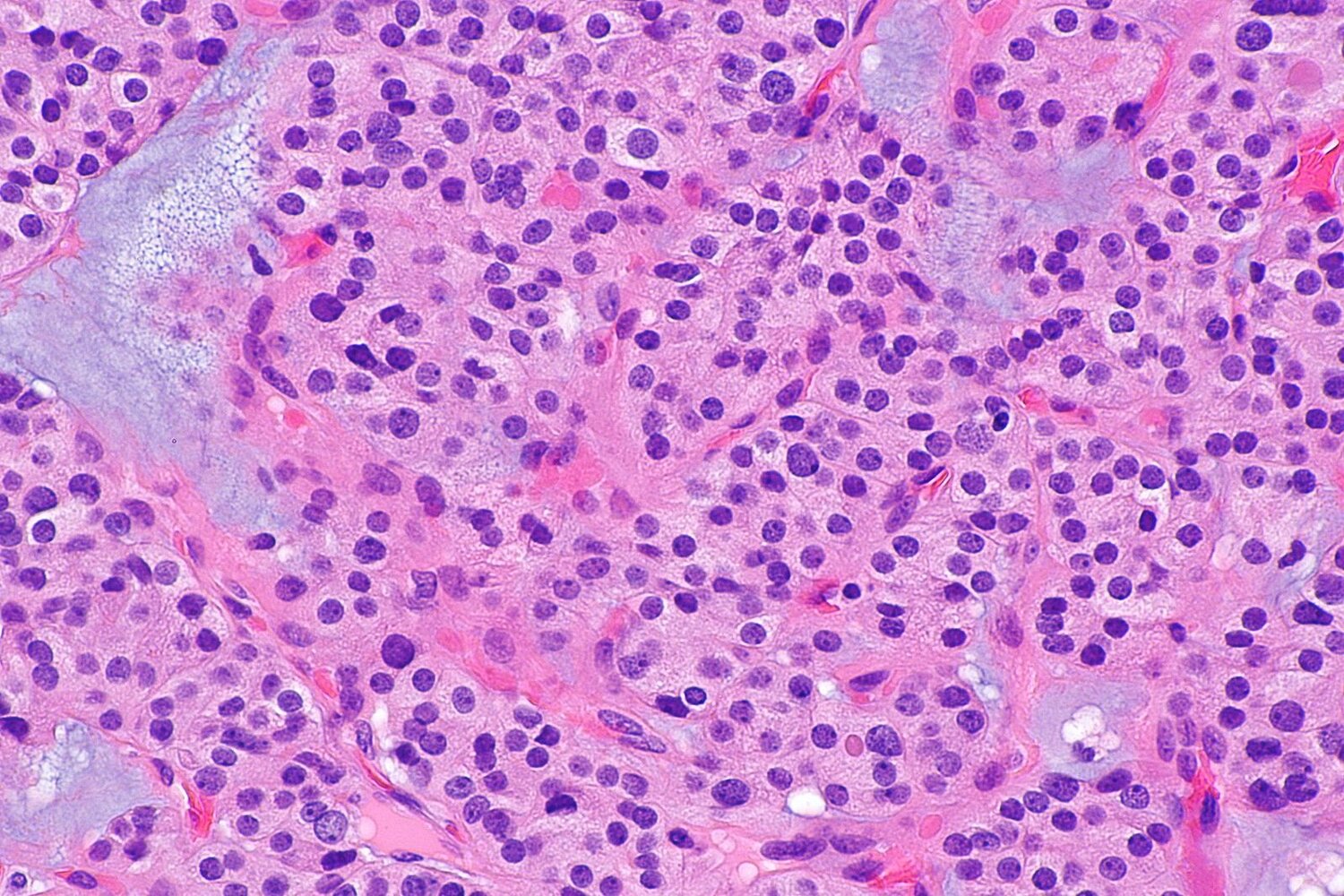
Photomicrograph of thyroid tissue (H&E stain; high magnification)
The closely packed follicular cells (examples indicated by green overlay) appear normal with round, uniform nuclei, and dense chromatin patterns. Significant hyperplasia of follicular cells has resulted in a loss of the normal follicular architecture, but neither capsular nor vascular invasion is visible.
These findings are suggestive of follicular adenoma of the thyroid.
Source: “Follicular adenoma -- high mag” by Nephron, Wikimedia Commons, licensed under CC BY-SA 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 4.0.
{kind=link}
Toxic adenoma
Epidemiology
- Third most common cause of hyperthyroidism
- Sex: ♀ > ♂ [15]
- Age: more common in individuals 30–50 years of age
Pathophysiology
- Gain-of-function mutations of TSH receptor gene; in a single precursor cell → autonomous functioning of the thyroid follicular cells of a single nodule → focal hyperplasia of thyroid follicular cells → toxic adenoma
- The autonomous thyroid nodule overproduces thyroid hormones → hyperthyroidism → decrease in pituitary TSH secretion → suppression of hormone production in the rest of the gland
Clinical features
- Palpable, usually painless nodule in otherwise normal gland
- Symptoms of thyrotoxicosis
Diagnostics [16]
For the initial workup, see “Diagnostic approach to thyroid nodules.”
- Thyroid function tests: : ↑ T3 and ↓ TSH
- Thyroid ultrasound: sonographic signs of a benign thyroid nodule; in some cases, increased perfusion
-
Thyroid scintigraphy
- Solitary, hot nodule
- Suppression of rest of the gland
- FNAC: Indicated not as a confirmatory test for toxic adenoma but to identify malignancy in suspicious nodules (see “Indications for FNAC of thyroid nodules”)
Treatment [10]
-
Initial management: treatment of hyperthyroidism
- Beta blockers for symptom control
- Antithyroid drugs to achieve euthyroidism
-
Definitive treatment options [9][17]
- Hemithyroidectomy or isthmusectomy for a solitary toxic adenoma
- Radioactive iodine ablation (RAIA) [16]
- Less invasive therapy (e.g., ethanol ablation, radiofrequency ablation, laser ablation) may be considered in patients who are neither candidates for surgery nor RAIA. [16][18]
Toxic multinodular goiter
Epidemiology [16]
- Sex: ♀ > ♂
- Age: often > 60 years
- Second most common cause of hyperthyroidism
- Develops in 10% of patients with a long-standing nodular goiter
- More prevalent in iodine-deficient regions
Pathophysiology
- Chronic iodine deficiency/thyroid dysfunction → decreased hormone production → increased hypothalamic TRH secretion → persistent TSH stimulation of the thyroid gland → hyperplasia of thyroid nodules, some more active than others → multinodular goiter (nontoxic MNG)
- Multiple somatic mutations of TSH receptor occur in long-standing goiters (> 60% of cases) → autonomous functioning of some nodules (toxic MNG) → hyperthyroidism (due to ↑ release of both T3 and T4)
Clinical features [16]
- Painless goiter with multiple palpable nodules
- Symptoms of thyrotoxicosis
Diagnostics [16]
For the initial workup of a nodular goiter, see “Diagnostic approach to thyroid nodules.”
- Thyroid function tests: ↑ T3 and ↓ TSH
- Thyroid ultrasound: multiple nodules within the thyroid parenchyma; increased perfusion
-
Thyroid scintigraphy [12]
- Increased radioiodine uptake by multiple hyperfunctioning (hot) nodules
- Decreased uptake (suppression) by the rest of the gland and intervening parenchyma
- Hypofunctioning or cold nodules may also be present in the multinodular gland.
- FNAC: not routinely required (see “Indications for FNAC of thyroid nodules”)
- Histopathology of resected tissue: patches of enlarged follicular cells distended with colloid and with flattened epithelium
Treatment [10][17]
-
Initial management: treatment of hyperthyroidism
- Beta blockers for symptom control
- Antithyroid drugs to achieve euthyroidism
-
Definitive treatment options [9]
- Total thyroidectomy or near-total thyroidectomy
- Radioactive iodine ablation
Thyroid cysts
Classification and etiology [7]
- Simple cysts are exclusively fluid-filled nodules lined by benign epithelial cells.
- Complex cysts are partly solid and partly cystic and carry a 5–10% risk of malignancy. [19]
- Most commonly due to cystic degeneration of thyroid tissue or involution of an adenoma
Clinical features
- Palpable thyroid nodule
- Hemorrhage into a cyst → pain and rapid enlargement of the nodule
- A large cyst or extensive hemorrhage can cause compression symptoms (e.g., hoarseness, dysphagia).
Diagnostics [6]
The initial workup is the same as that for other thyroid nodules (see “Diagnostic approach to thyroid nodules”).
- Thyroid function tests: typically normal
-
Thyroid ultrasound
- Cystic components appear anechoic.
- May be mixed with solid components
-
FNAC: based on FNAC indications for thyroid nodules [6][20]
- Purely cystic nodule: diagnostic FNAC not recommended
-
Partly cystic nodule
- Low risk pattern (eccentric solid component): FNAC if size is ≥ 1.5 cm
- Very low risk pattern: Consider FNAC if size is ≥ 2 cm.
Treatment [6]
-
Benign cysts
- Asymptomatic cysts: observation
- Large or symptomatic cysts (or patient preference)
- Aspiration with/without ethanol ablation [21]
- Surgery may be considered if aspiration is not effective.
- Malignant cysts: See “Thyroid cancer.”
Special patient groups
Pregnant patients [3]
Management of thyroid nodules in pregnancy is similar to those in nonpregnant patients, except for the following points.
-
Diagnostics
- In patients with low TSH, thyroid scintigraphy should be deferred until after pregnancy and cessation of breastfeeding.
- Newly symptomatic or growing thyroid nodules should be followed up with thyroid ultrasound.
- FNAC may be safely performed during pregnancy if indicated.
-
Treatment
- RAIA is contraindicated during pregnancy and breastfeeding.
- If thyroid cancer is suspected or diagnosed during pregnancy:
- Postpone surgery until after the pregnancy, unless there are signs of aggressive cancer or advanced growth; surgery is relatively safe during the second trimester.
- If surgery is deferred, consider administration of levothyroxine to maintain TSH at low to normal levels.
Children [3]
- Management is similar to that of thyroid nodules in adults.
- Thyroid nodules in children are more frequently malignant.
External Resources
- 2020 AAES Guidelines for the Definitive Surgical Management of Thyroid Disease in Adults
- 2016 AACE/ACE/AME Guidelines for Clinical Practice for the Diagnosis and Management of Thyroid Nodules
- 2015 ATA Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer
- US Preventative Service Task Force Recommendation (Thyroid Cancer Screening in Adults)
References
- "Multinodular Goiter"
- Sharma A, Stan MN. "Thyrotoxicosis: Diagnosis and Management". Mayo Clin Proc. 94(6). :1048-1064. (2019)
- Ross DS, Burch HB, Cooper DS, et al. "2016 American Thyroid Association Guidelines for Diagnosis and Management of Hyperthyroidism and Other Causes of Thyrotoxicosis". Thyroid. 26(10). :1343-1421. (2016)
- Porterfield JR Jr, Thompson GB, Farley DR, Grant CS, Richards ML. "Evidence-based management of toxic multinodular goiter (Plummer's Disease)". World J Surg. 32(7). :1278-84. (2008)
- Patel KN et al. "The American Association of Endocrine Surgeons Guidelines for the Definitive Surgical Management of Thyroid Disease in Adults". Ann Surg. 271(3). :e21-e93. (2020)
- Tarantino L, Francica G, Sordelli I, et al. "Percutaneous Ethanol Injection of Hyperfunctioning Thyroid Nodules: Long-Term Follow-Up in 125 Patients". American Journal of Roentgenology. 190(3). :800-808. (2008)
- Intenzo CM, Depapp AE, Jabbour S, et al. "Scintigraphic manifestations of thyrotoxicosis". Radiographics. 23(4). :857-869. (2003)
- Haugen BR, Alexander EK, Bible KC, et al. "2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer". Thyroid. 26(1). :1-133. (2016)
- Gharib H, Papini E, Garber JR, et al. "American Association of Clinical Endocrinologists, American College of Endocrinology, and Associazione Medici Endocrinologi Medical Guidelines for clinical practice for the diagnosis and management of thyroid nodules-2016 update". Endocr Pract. 22(5). :622-39. (2016)
- Gharib H, Papini E. "Thyroid nodules: clinical importance, assessment, and treatment". Endocrinol Metab Clin North Am. 36(3). :707-35, vi. (2007)
- Russ G, Leboulleux S, Leenhardt L, Hegedüs L. "Thyroid Incidentalomas: Epidemiology, Risk Stratification with Ultrasound and Workup". Eur Thyroid J. 3(3). :154-163. (2014)
- Mirfakhraee S, Mathews D, Peng L, Woodruff S, Zigman JM. "A solitary hyperfunctioning thyroid nodule harboring thyroid carcinoma: review of the literature". Thyroid Res. 6(1). :7. (2013)
- Cibas ES, Ali SZ. "The 2017 Bethesda System for Reporting Thyroid Cytopathology.". Thyroid. 27(11). :1341-1346. (2017)
- Dean DS, Gharib H. "Epidemiology of thyroid nodules". Best Pract Res Clin Endocrinol Metab. 22(6). :901-911. (2008)
- Welker MJ, Orlov D. "Thyroid Nodules". Am Fam Physician. 67(3). :559-567. (2003)
- Burman KD, Wartofsky L. "CLINICAL PRACTICE. Thyroid Nodules". N Engl J Med. 373(24). :2347-56. (2015)
- Welker MJ, Orlov D. "Thyroid nodules.". Am Fam Physician. 67(3). :559-66. (2003)
- McHenry CR, Phitayakorn R. "Follicular Adenoma and Carcinoma of the Thyroid Gland". Oncologist. 16(5). :585-593. (2011)
- Lee MJ, K, Kim EK, Kwak JY, Kim MJ. "Partially Cystic Thyroid Nodules on Ultrasound: Probability of Malignancy and Sonographic Differentiation". Thyroid. 19(4). :341-346. (2009)
- Tessler FN, Middleton WD, Grant EG, et al. "ACR Thyroid Imaging, Reporting and Data System (TI-RADS): White Paper of the ACR TI-RADS Committee". J Am Coll Radiol. 14(5). :587-595. (2017)
- Iñiguez-Ariza NM, Lee RA, Singh-Ospina NM, Stan MN, Castro MR. "Ethanol Ablation for the Treatment of Cystic and Predominantly Cystic Thyroid Nodules.". Mayo Clin Proc. 93(8). :1009-1017. (2018)
- Jameson JL, Fauci AS, Kasper DL, et al. "Harrison's Principles of Internal Medicine, Twentieth Edition (Vol.1 & Vol.2)". McGraw-Hill Education / Medical. (2018). ISBN: 9781259644030