Summary
Thyroid surgery is a procedure commonly performed to treat benign and malignant thyroid disorders. Total thyroidectomy entails the removal of the entire thyroid gland and is indicated in the management of thyroid cancer or benign thyroid conditions that affect the entire gland (e.g., Graves disease, multinodular goiter). A small cuff of tissue adjacent to the tracheoesophageal groove is spared in near-total and subtotal thyroidectomy in order to protect the parathyroid glands and the adjacent nerves. Lobectomy (removal of a single lobe) or hemithyroidectomy (removal of a single lobe with the isthmus) is performed for unilateral benign thyroid disorders (e.g., toxic adenoma, recurrent thyroid cysts) and for small, low-risk differentiated thyroid cancers. Postoperative complications include hematoma formation, hypoparathyroidism, nerve palsy (recurrent/superior laryngeal nerve), and hypothyroidism. The greater the extent of resection, the greater the risk of complications. However, the most extensive resections (total thyroidectomy) are associated with the lowest rates of recurrent disease.
Thyroid gland anatomy
See thyroid gland and parathyroid glands.
- Nerves in close proximity to the thyroid gland
- Recurrent laryngeal nerve (close to the inferior thyroid artery)
- Superior laryngeal nerve (close to the superior thyroid artery)



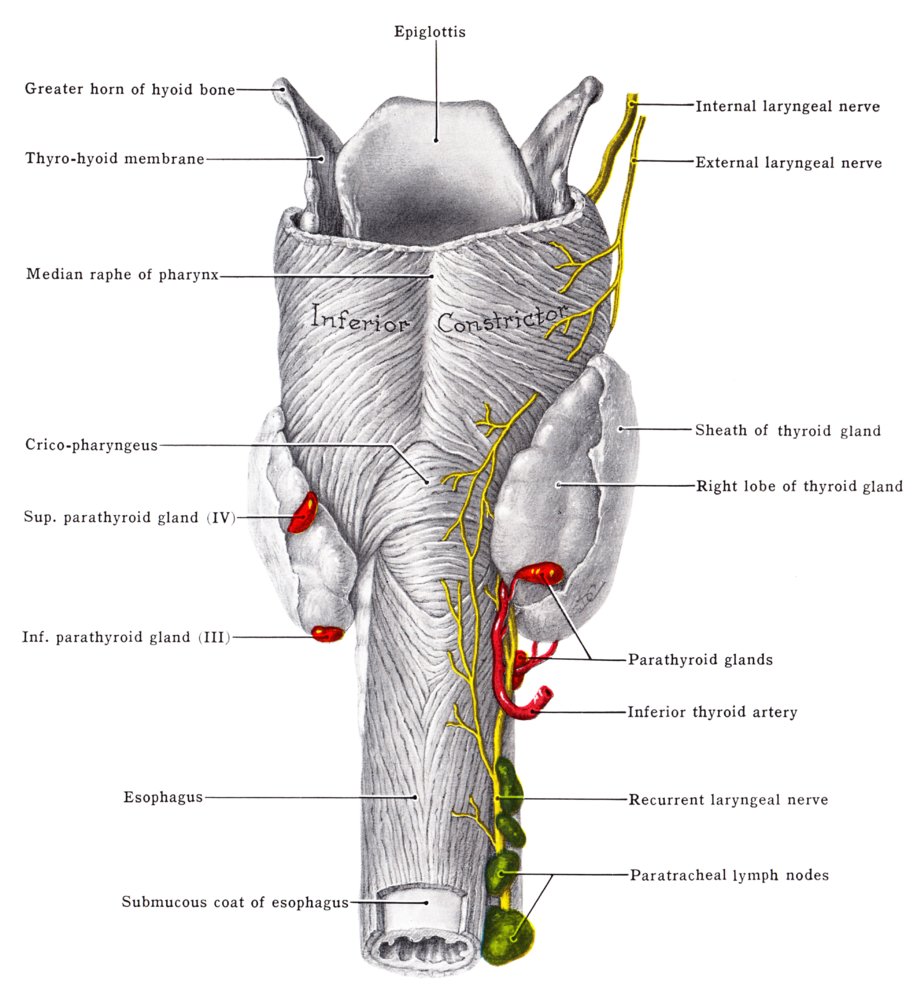
Topographic anatomy of the pharynx (dorsal view)
The parathyroid glands are located adjacent to the trachea at the left and right posterior edges of the thyroid gland. Also note the course of the internal, external, and recurrent laryngeal nerves.
Source: "Thyroid Gland, the Parathyroid Glands, and the Three Laryngeal Nerves, from behind", Grant, John Charles Boileau, Wikimedia Foundation licensed under Public Domain
{kind=link}
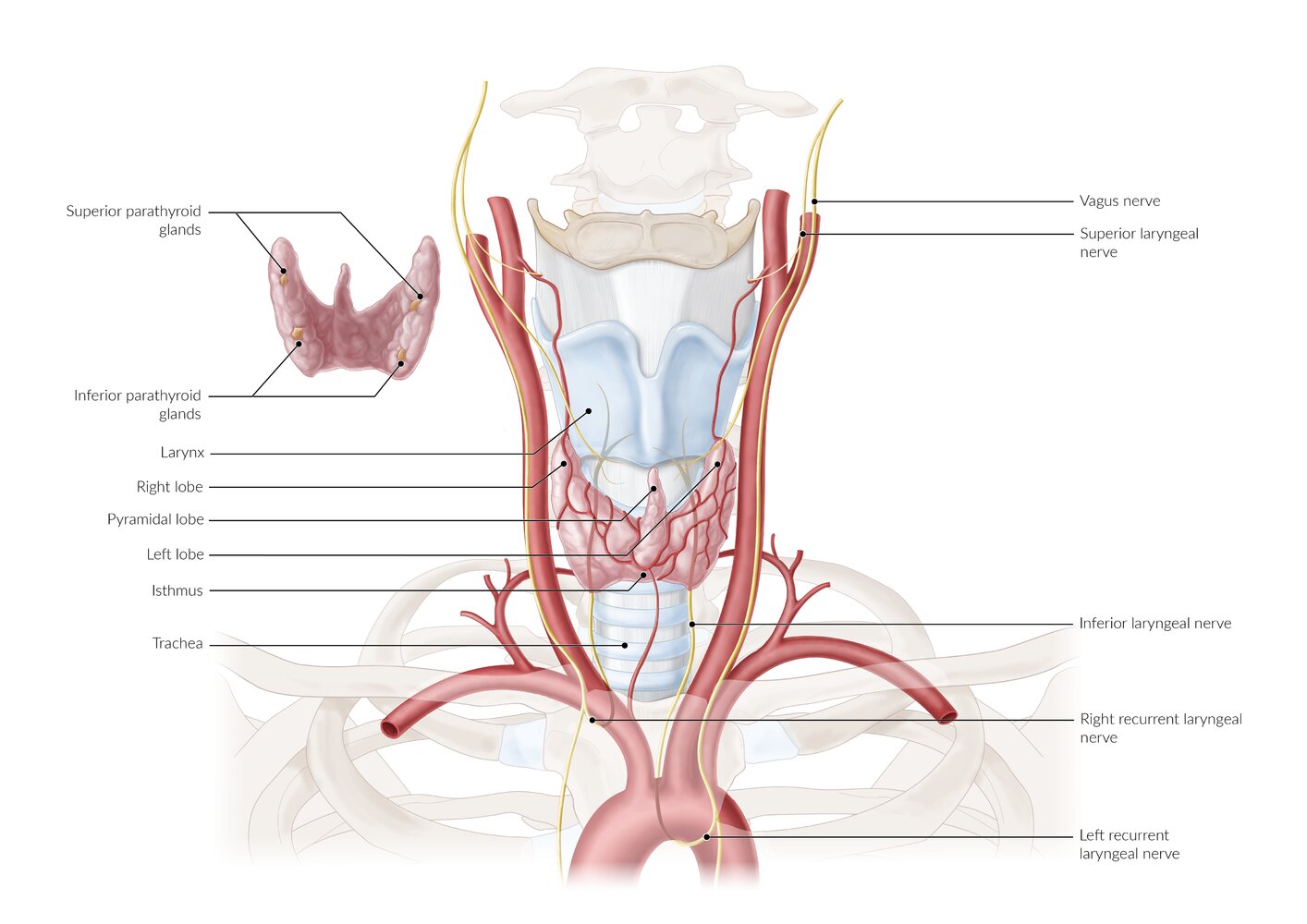
The thyroid gland is located in front of the trachea in the lower neck and consists of two lobes connected by an isthmus. A third pyramidal lobe extending from the isthmus is present in 50% of patients. This third lobe is a remnant of the thyroglossal duct.
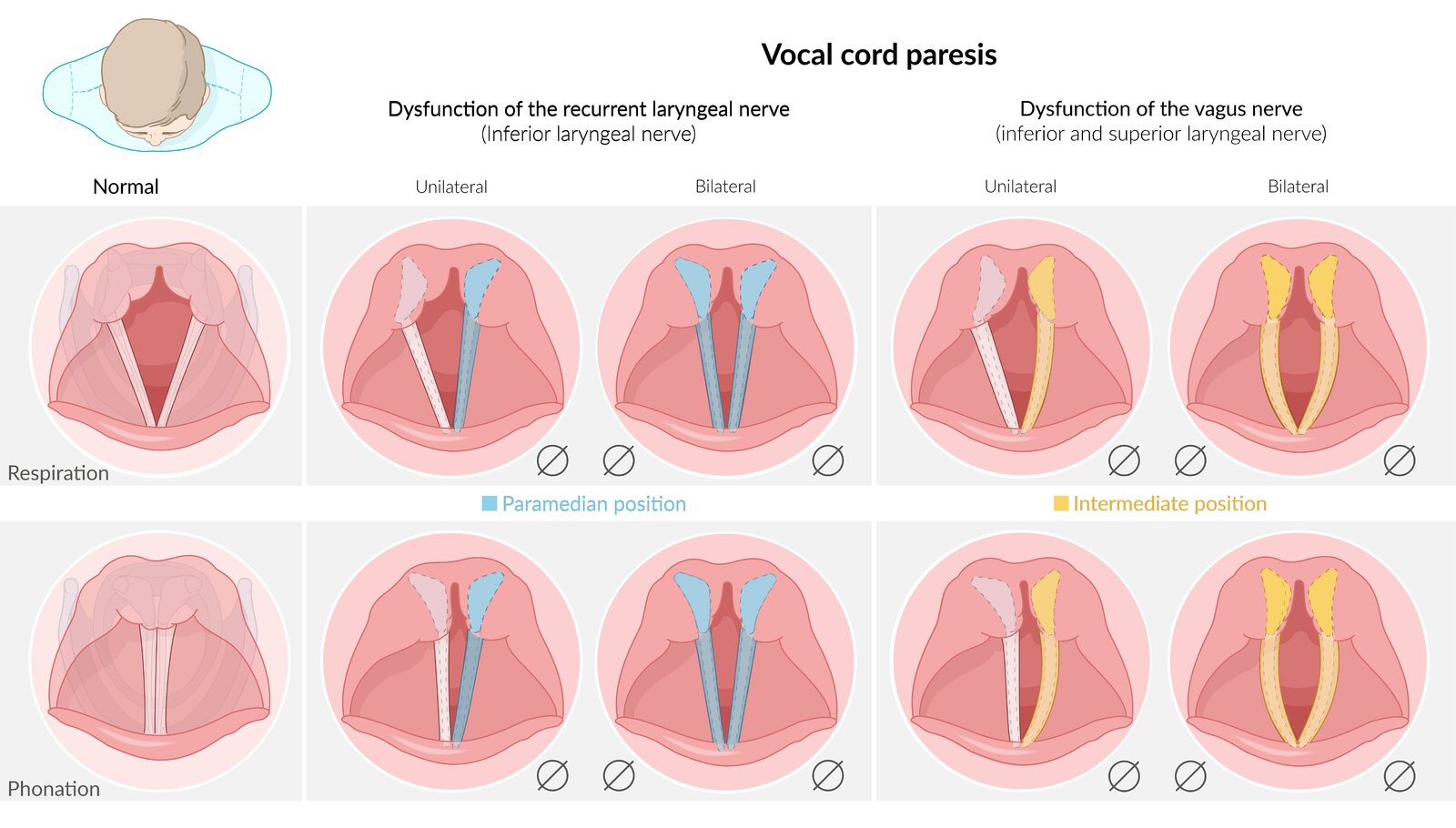
The parathyroid glands are located posterior to the thyroid gland; they may vary in number and location. The recurrent laryngeal nerves (RLN) branch off from the vagus nerve; the left RLN loops under the aortic arch, and the right RLN passes beneath the subclavian artery. Both RLNs are vulnerable to injury during thyroid surgery as they ascend to the larynx behind the thyroid gland. Unilateral RLN injury may result in hoarseness, and bilateral RLN injury may cause dyspnea and stridor.
© AMBOSS
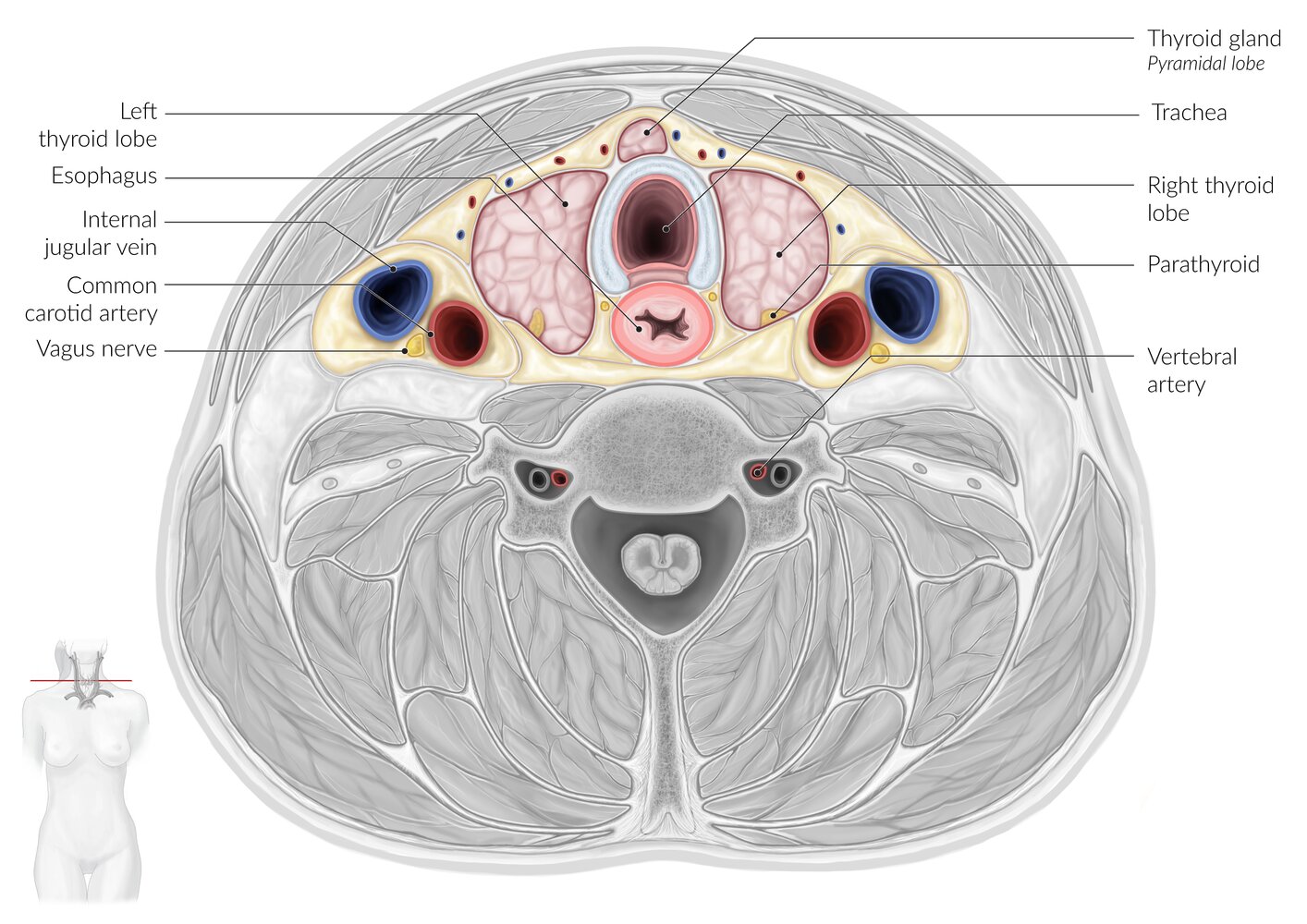
Transverse section of the neck at the level of C7 (cranial view)
The thyroid gland is located in the anterior neck and overlaps the anterior aspect of the cricoid cartilage and the upper tracheal rings. The thyroid consists of two lobes connected by an anterior isthmus. The pyramidal lobe (if present) projects from the isthmus and lies in front of the trachea.
Surrounding structures (by location)
– Anterior to the thyroid: infrahyoid muscles
– Posteromedial to the thyroid: recurrent laryngeal nerves, which lie in the tracheoesophageal groove; trachea; esophagus
– Posterolateral to the thyroid: carotid sheath (contains the common carotid artery, internal jugular vein, and vagus nerve)
– Posterior to the thyroid: parathyroid glands
© AMBOSS
Preparation
-
Achieve euthyroid status preoperatively.
- In hyperthyroidism to minimize the risk of thyroid storm
- Thioamides
- Iodides (potassium iodide)
- Beta blockers (e.g., propranolol)
- In hypothyroidism: thyroid hormone replacement
- In hyperthyroidism to minimize the risk of thyroid storm
- Preoperative oral calcium and vitamin D supplementation
- Preoperative direct/indirect laryngoscopy
References:[1][2][3][4][5][6]
Technique/steps
| Procedure | Description | Indication |
|---|---|---|
| Total thyroidectomy |
|
|
| Near-total thyroidectomy |
|
|
| Subtotal thyroidectomy |
|
|
| Thyroid lobectomy |
|
|
| Hemithyroidectomy |
|

")

References:[1][7][8][9][10][11]

A patient in Kocher's position (supine with a pad placed under the shoulders to enable neck extension and adequately expose the thyroid gland). A slight (15°) inclination of the operating table with the head-end raised (reverse Trendelenburg position) facilitates surgery by reducing blood flow to the gland. However, this position also increases the risk of air embolism by creating negative pressure in the vasculature.
Source: “Struma Lagerung” by THWZ, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}

A pen has been used to mark Kocher's incision: a transverse skin crease incision, which transects the thyroid isthmus, ~2–3 cm above the clavicular heads. The epidermis, dermis, subcutaneous fat, and the platysma are incised.
Note: A Kocher's incision is also in abdominal surgery.
Source: “Struma Schnittfuehrung” by THWZ, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}
The incision is made two finger widths above the jugulum, resulting in a symmetrical, curved, horizontal incision. Indication: thyroid, mediastinal, or tracheal surgery
© AMBOSS
Complications
- Transient/permanent postoperative hypoparathyroidism (most common) or hypothyroidism
- Hematoma
- Transient/permanent RLN palsy
- Superior laryngeal nerve palsy → paralysis of cricothyroid muscle → easy voice fatigability; change in the timbre of voice
- Thyroid storm: if the surgery was performed in inadequately treated patients with hyperthyroidism (see "complications" of hyperthyroidism for further details)
| Unilateral RLN palsy | Bilateral RLN palsy | |
|---|---|---|
| Clinical features |
|
|

References:[1][7][12]
We list the most important complications. The selection is not exhaustive.
© AMBOSS
References
- Wang TS, Richards ML, Sosa JA. "Initial thyroidectomy". UpToDate. UpToDate. https://www.uptodate.com/contents/initial-thyroidectomy?source=search_result&search=Thyroid%20surgery&selectedTitle=1~150#H27. [2017-01-03]
- "Endocrine Disease (Anesthesia Text)". https://www.openanesthesia.org/endocrine_disease_anesthesia_text/. [2017-03-21]
- Kay-rivest E, Mitmaker E, Payne RJ, et al. "Preoperative vocal cord paralysis and its association with malignant thyroid disease and other pathological features". J Otolaryngol Head Neck Surg. 44(1). :35. (2015)
- Yeung P, Erskine C, Mathews P, Crowe PJ. "Voice changes and thyroid surgery: is pre-operative indirect laryngoscopy necessary?". Aust N Z J Surg. 69(9). :632-634. (1999)
- Randolph GW. "The importance of pre- and postoperative laryngeal examination for thyroid surgery". Thyroid. 20(5). :453-458. (2010)
- "Kaplan E, Mercier F, Applewhite M, Angelos P, Grogan RH"
- "Surgery of the thyroid". http://www.thyroidmanager.org/chapter/chapter-21surgery-of-the-thyroid/. [2015-09-25]
- Rayes N, Seehofer D, Neuhaus P. "The surgical treatment of bilateral benign nodular goiter: balancing invasiveness with complications". Dtsch Arztebl Int. 111(10). :171-178. (2014)
- Vaiman M, Nagibin A, Hagag P, et al. "Subtotal and near total versus total thyroidectomy for the management of multinodular goiter". World J Surg. 32(7). :1546-1551. (2008)
- Hanks JB, Inabnet III WB. "Controversies in Thyroid Surgery". Springer International Publishing. (2015). ISBN: 9783319205236
- Mazzaferri EL. "Management of low-risk differentiated thyroid cancer". Endocr Pract. 13(5). :498-512. (2007)
- Carroll TL. "Unilateral Vocal Fold Paralysis". WebMD. http://emedicine.medscape.com/article/863779-overview. [2015-03-29]