Summary
Tibial and fibular fractures are common types of long bone injuries and are usually caused by direct trauma. Fractures may occur proximally, at the shaft, or distally. Since only a small amount of soft tissue covers the tibia and fibula, there is a high risk of open fractures. X-rays are the initial diagnostic test of choice. Initial management varies by fracture location and commonly involves consulting orthopedic surgery, splinting, and weight-bearing restrictions. Complications include common peroneal nerve injury and compartment syndrome.
For distal tibial or fibular fractures, see “Ankle fractures.” See also “Tibial stress fractures.”
Classification
-
Tibial fractures
- Tibial plateau fracture: a break in the superior surface of the tibia which articulates with the femoral condyles
- Isolated tibial shaft fracture
-
Fibular fractures
- Isolated proximal fibular fracture
- Isolated fibular shaft fracture
- Combined tibial and fibular shaft fractures (managed similarly to tibial shaft fracture)
- Distal tibial or fibular fractures: See “Ankle fractures.”
Clinical features
- Local pain, tenderness, and/or deformity
- Swelling, bruising, and/or hematoma
- Skin abnormalities, e.g., lacerations, tenting
- Signs of neurovascular injury, e.g.:
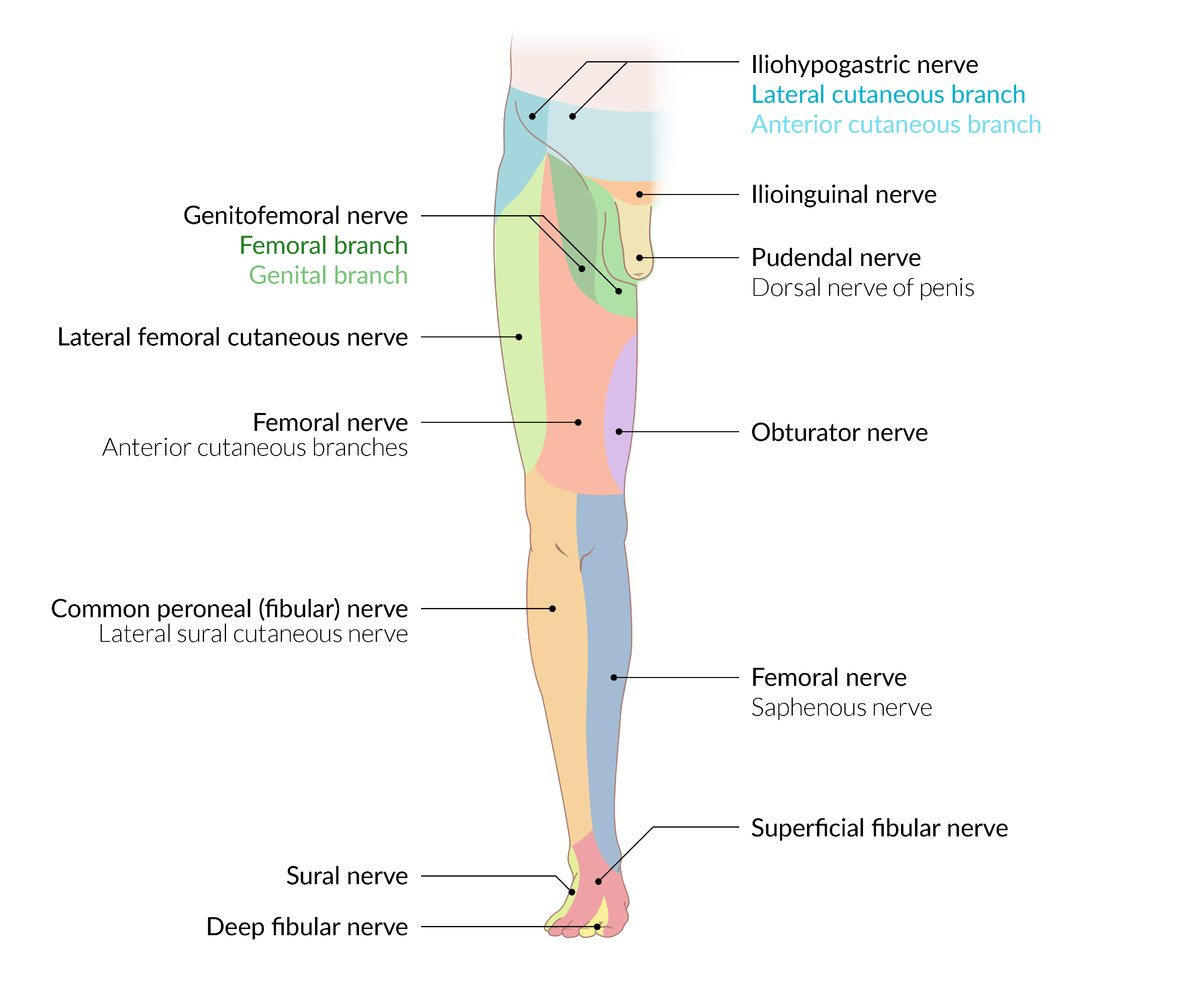
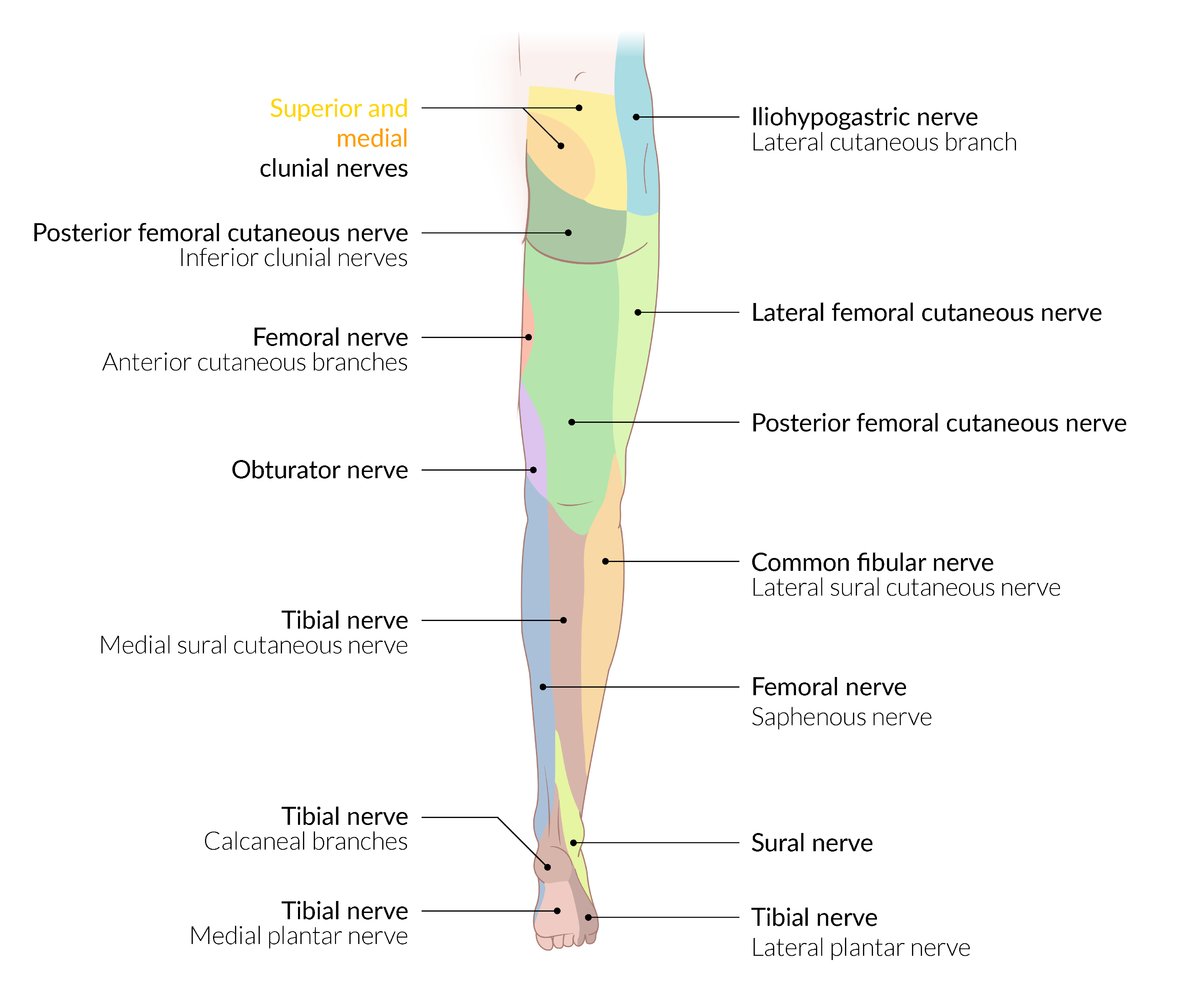
- Common peroneal nerve injury, e.g., foot drop, impaired foot eversion, sensory deficits
- Posterior tibial nerve injury, e.g., impaired plantar flexion, sensory deficit over the sole of foot
- Arterial injury, e.g., hard signs of extremity vascular injury, diminished distal pulses
- Signs of compartment syndrome
- See “Fracture signs.”
Tibial and fibular fractures are at high risk of open fractures due to minimal surrounding soft tissue. [1]
Diagnosis
Clinical evaluation [1]
Urgent orthopedic consultation is indicated for any findings that suggest neurovascular injury or an open fracture.
-
Neurovascular examination
- Assess dorsalis pedis and posterior tibial pulses and capillary refill time.
- Evaluate for peroneal nerve injury and posterior tibial nerve injury.
- Skin examination: Evaluate for laceration, tearing, and tenting.
")
")
X-ray [1][2]
Imaging for tibial and/or fibular fractures generally includes x-rays of the knee, tibia and fibula, and ankle.
-
Views
- Knee
- Anterioposterior (AP) and lateral views
- Intercondylar view for suspected tibial plateau fractures
- Tibia and fibula: AP and lateral views
- Ankle: AP, lateral, and mortise views
- Knee
-
Findings
- Radiographic fracture signs, fracture fragments, displacement, angulation, and/or dislocation
- In tibial plateau fractures, lipohemarthrosis may be visible as a fat-fluid level. [1]
- See also “Ankle fracture diagnostics.”
Evaluate for a Maisonneuve fracture in patients with a proximal fibular fracture, as Maisonneuve fractures are often unstable and require urgent orthopedic evaluation. [1]
")
")
")
")



Advanced imaging [1][2]
- CT: may be indicated for preoperative planning, fractures with intraarticular extension, or inconclusive x-rays with high clinical suspicion
- MRI: may be indicated for diagnosis of associated tendon and/or ligament injuries, e.g., meniscal injury associated with tibial plateau fracture [3]
In patients with acute traumatic knee pain, tibial tenderness, inability to bear weight, and nondiagnostic x-rays, obtain a CT to rule out a tibial plateau fracture. [1]
© AMBOSS
© AMBOSS

X-ray right knee (AP view)
An oblique fracture (red overlay) of the proximal fibula (Fi) shows slight medial displacement of the distal fragment. Lateral subluxation of the fibula at the tibiofibular joint and widening of the distance between tibia (T) and fibula (double arrow) indicate disruption of the tibiofibular ligaments.
Fe: femur
Source: © IMPP

X-ray right knee (lateral view)
The oblique proximal fibular fracture (red overlay) shows no appreciable anterior or posterior displacement of the distal fragment.
Fe: femur; Fi: fibula; T: tibia
Source: © IMPP

X-ray left knee (AP view)
A comminuted tibial plateau fracture (red lines) shows intraarticular extension and displacement of some fracture fragments. There is depression of the lateral tibial plateau. An extra-articular fracture (green line) of the proximal fibula (dashed line) is also visible.
Source: © IMPP

X-ray left knee (lateral view)
A comminuted tibial plateau fracture (red line) shows intraarticular extension. An extra-articular fracture (green lines) of the proximal fibula (dashed line) is also visible.
Source: © IMPP

X-ray knee (AP view) of patient with severe pain following fall onto knee
There is a depression fracture of the lateral tibial plateau (blue overlay). Rod and screw fixation of a prior femoral shaft fracture is also seen.
Dashed line: depressed lateral tibial plateau after fracture; arrow: direction of depression; line: lateral tibial plateau position before fracture
Source: © IMPP

X-ray lower right leg (lateral view) of patient involved in motor vehicle crash
Transverse mid tibial fracture (red overlay) with near half-shaft-width posterior displacement of the distal fracture fragment.
White outline: fibula
Our great thanks to PD Dr. M. Jergas (Center for Diagnostic and Interventional Radiology, St. Elizabeth Hospital, Cologne) for kindly providing this image.

X-ray left lower leg (AP view)
A fracture (red line) is present at the middle to distal third of the tibial diaphysis. No medial or lateral displacement of the fracture fragments is shown on this view; however, a lateral radiograph is not available to assess for anterior or posterior displacement. There is no callus formation.
Arrowheads: secondary fracture lines
Our great thanks to PD Dr. M. Jergas (Center for Diagnostic and Interventional Radiology, St. Elizabeth Hospital, Cologne) for kindly providing this image.
Management
Initial management by fracture type [1]
-
All patients
- Initiate general fracture care, including analgesia.
- Place patients on non-weight-bearing status.
- Identify fractures requiring urgent orthopedic consultation.
- Consider VTE prophylaxis in consultation with orthopedics. [1]
-
Tibial plateau fractures
- Apply a knee immobilizer.
- Arrange orthopedic follow-up within 1 week.
-
Tibial shaft fractures (with or without fibular shaft fracture)
- Perform closed reduction for displaced, deformed, or angulated fractures with neurovascular compromise.
- Immobilize in a posterior long-leg splint; consider adding a stirrup splint for open fractures.
- Consult orthopedics urgently.
-
Isolated proximal or midshaft fibular fractures
- Immobilize in a stirrup splint.
- Arrange orthopedic follow-up within 1–2 weeks.
- Distal tibial or fibular fractures: See “Ankle fractures.”
For proximal fibular fractures, rule out associated Maisonneuve fracture and common peroneal nerve injury. [1]
Identify and treat acute compartment syndrome in high-energy tibial and fibular fractures if present. [4]
Nonoperative management [1]
- Indicated for most nondisplaced closed fractures, e.g.:
- Tibial plateau fractures
- Isolated proximal or midshaft fibular fractures
- Options include knee immobilizers and posterior long-leg splints.
- See “Conservative treatment of fractures.”
Surgical management [1]
-
Fractures commonly requiring surgery include:
- Open fractures
- Displaced fractures
- Fractures with neurovascular injury
- Severe tibial plateau fractures (e.g., with comminution, significant articular step-off deformity, condylar widening, multiple condylar involvement) [4]
- Operative techniques include:
- Open reduction and internal fixation
- Closed reduction and internal fixation
- Intramedullary nailing
- External fixation

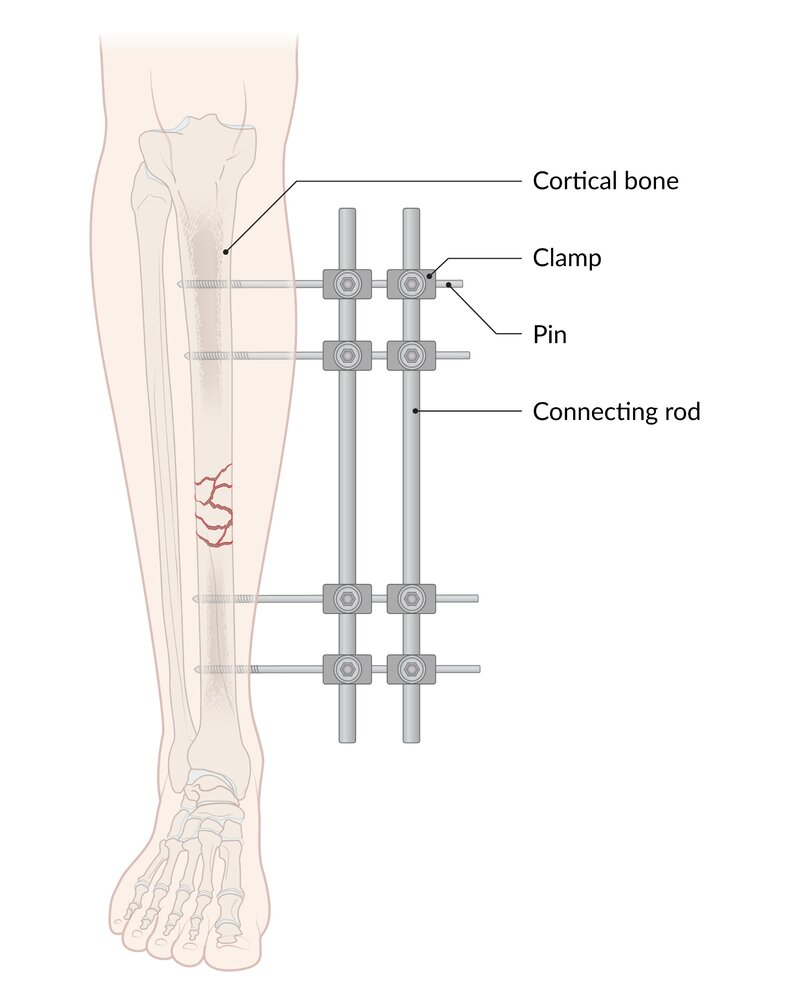
External fixation is a method of immobilizing a fracture using devices (e.g., pins, screws, etc) that are secured outside the skin (in contrast to internal fixation, in which the devices are placed completely inside the body).
© AMBOSS
Subtypes and variants
Toddler fracture [5][6]
- Definition: a nondisplaced fracture of the distal tibial shaft, usually following acute trauma (e.g., falling, tripping), causing rotation of the body around a fixed foot
- Epidemiology: : commonly seen in children between 9 months and 3 years of age [6]
- Etiology: trauma (e.g., low-energy fall from a chair or table, tripping while running)
-
Clinical features
- Irritability
- Abnormal gait (limping or inability to bear weight)
- Localized tenderness over the distal tibial shaft
-
Diagnostics
- Often goes undetected due to subtle clinical and radiographic findings
- Imaging
- AP, lateral, and oblique x-ray
- MRI and/or CT: indicated in cases of prolonged symptoms and suspicion of infection (e.g., osteomyelitis)
- Treatment: immobilization with a long cast, controlled ankle movement walker boot, short cast, or splint [7]


X-ray lower leg (AP view) of a child
A nondisplaced spiral fracture of the distal tibial diaphysis (arrows) is not accompanied by conspicuous periosteal reaction. The fibula is normal.
Toddler fractures are usually accidental injuries. They can be subtle and sometimes require additional views, follow-up radiographs, or bone scintigraphy for diagnosis. Ultrasound may also be useful.
Source: “Tibfracture.png” by Doc James, Wikimedia commons, licensed under CC BY-SA 3.0. Modifications: - arrow removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
Complications
- Patients with tibial fractures should be monitored for:
- High risk of compartment syndrome in any of the compartments, given that the tibia is surrounded by the anterior, lateral, and deep posterior compartments of the lower leg
- Fat embolism
- Peroneal nerve injury (foot drop)
- Deep vein thrombosis
- Nonunion
- Posttraumatic arthritis [8]
- See “Fracture complications.”
We list the most important complications. The selection is not exhaustive.
References
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904
- Dennan S. "Difficulties in the radiological diagnosis and evaluation of tibial plateau fractures". Radiography. 10(2). :151-158. (2004)
- Mustonen AOT, Koivikko MP, Lindahl J, Koskinen SK. "MRI of Acute Meniscal Injury Associated with Tibial Plateau Fractures: Prevalence, Type, and Location". Am J Roentgenol. 191(4). :1002-1009. (2008)
- Mthethwa J, Chikate A. "A review of the management of tibial plateau fractures". Musculoskelet Surg. 102(2). :119-127. (2017)
- Mehin R, O’Brien P, Broekhuyse H, Blachut P, Guy P. "Endstage arthritis following tibia plateau fractures: average 10-year follow-up". Canadian Journal of Surgery. 55(2). :7-94. (2012)
- Naranje S, Kelly DM, Sawyer JR. "A Systematic Approach to the Evaluation of a Limping Child.". Am Fam Physician. 92(10). :908-16. (2015)
- Yiqiao Wang, Meagan Doyle, Kevin Smit, Terry Varshney, Sasha Carsen. "The Toddler's Fracture". Pediatr Emerg Care. 38(1). :36-39. (2021)
- Bauer JM, Lovejoy SA. "Toddler's Fractures: Time to Weight-bear With Regard to Immobilization Type and Radiographic Monitoring.". J Pediatr Orthop. 39(6). :314-317. (2019)