Quick guide for cerebral toxoplasmosis
Diagnostic approach
- ABCDE survey
- Targeted clinical evaluation
- CBC
- BMP
- HIV testing
- IgM and IgG Toxoplasma serology
- CT or MRI brain with contrast
- Lumbar puncture
- CSF analysis
- CSF PCR for Toxoplasma
Red flag features
- Altered mental status
- Seizures
- Focal neurological deficits
- Signs of elevated ICP
- Immunocompromise
- Pregnancy
Management checklist
- Immediate hemodynamic support (e.g., IV fluids, vasopressors)
- Manage acute seizures.
- Manage elevated ICP.
- Initiate treatment of cerebral toxoplasmosis.
- Consult infectious disease.
Summary
Toxoplasmosis is a disease caused by the obligate intracellular parasite Toxoplasma gondii. Transmission occurs either through ingestion of cysts found, for example, in raw meat or cat feces, or from mother to fetus through the placenta. The clinical presentation depends on the patient's immune status: In immunocompetent individuals, 90% of cases are harmless and asymptomatic, with the remaining 10% displaying mild mononucleosis-like symptoms. In immunosuppressed patients (e.g., those who are HIV-positive), infection may result in cerebral toxoplasmosis (headache, confusion, focal neurological deficits) or toxoplasmic chorioretinitis (eye pain, reduced vision). Treatment is indicated for immunosuppressed patients, infected mothers, congenital toxoplasmosis, and immunocompetent patients with more severe symptoms. The treatment of choice is usually a combination of pyrimethamine, sulfadiazine, and leucovorin (folinic acid), with the exception of new infections during pregnancy, which are treated with spiramycin.
For the congenital variant and how to manage infection in pregnant women, see “Toxoplasmosis in pregnancy.”
Epidemiology
-
Prevalence
- In the US: ∼ 10% of adults
- In some tropical climates: up to 95%
References:[1]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
- Pathogen: : Toxoplasma gondii, an obligate intracellular, single-celled protozoan
-
Route of transmission
-
Oral ingestion: The oocysts are excreted in the feces of cats (final host) and are orally ingested by other mammals such as humans, hoofed animals, and birds (intermediate hosts). Primary modes of transmission include the following:
- Cat feces
- Raw or insufficiently cooked meat (most common)
- Unpasteurized milk (especially goat milk)
- Transplacental transmission: see toxoplasmosis in pregnancy
- Via organ transplantation or blood transfusion
-
Oral ingestion: The oocysts are excreted in the feces of cats (final host) and are orally ingested by other mammals such as humans, hoofed animals, and birds (intermediate hosts). Primary modes of transmission include the following:

References:[2]
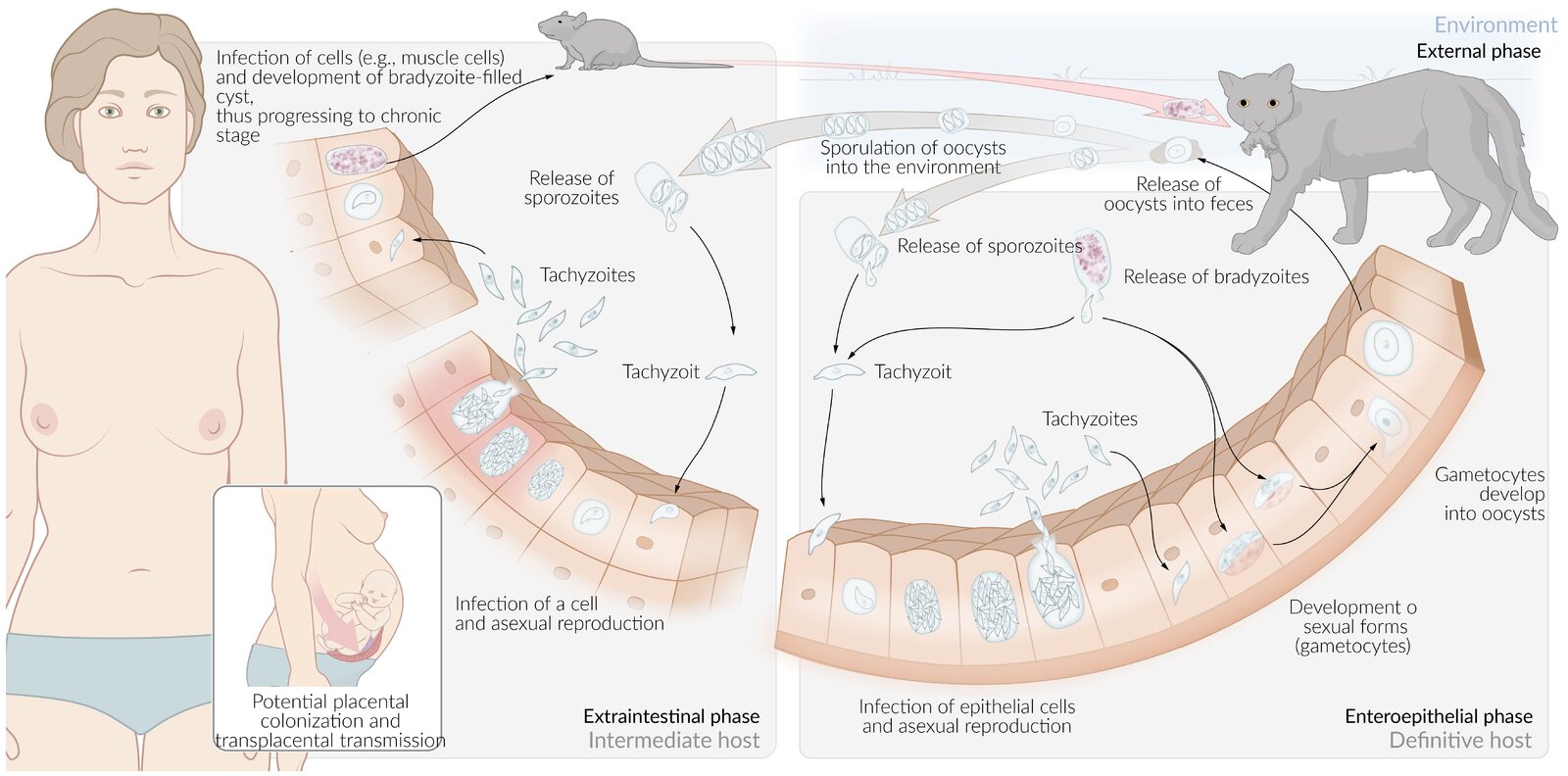
The life cycle of toxoplasmosis involves transmission to a human host through the ingestion of cat feces particulate that contains oocysts or ingestion of meat (i.e., pork) containing Toxoplasma cysts. Cross-placental transmission is possible after the initial infection of pregnant women.
© AMBOSS
Clinical features
- Incubation time: 5 days to 3 weeks [3]
-
Immunocompetent patients: typically primary infection [4][5]
- Mainly asymptomatic (∼ 90% of patients)
-
Symptomatic (< 10% of patients) [6]
- Mononucleosis-like symptoms with bilateral cervical adenopathy (but negative heterophile antibody test) [7]
- Rarely: ocular toxoplasmosis
- After initial infection, latent tissue cysts remain.
-
Immunosuppressed patients (e.g., patients with AIDS): primary infection or reactivation in previously infected individuals [4]
- Symptoms of encephalitis in cerebral toxoplasmosis
- Visual impairments and pain in ocular toxoplasmosis
- Other symptoms depend on affected organs (e.g., lungs, heart).
Diagnosis
Indications for testing may include uveitis or retinochoroiditis with no known history of congenital toxoplasmosis, organ transplantation, and a new diagnosis of HIV. [4][8]
-
Serology [4][9]
- IgM antibody test: positive within first week of acute infection [9]
- IgG antibody test; : positive 2 weeks following infection and remains positive for life
-
PCR using, e.g.:
- Amniotic fluid for suspected intrauterine disease
- CSF for suspected cerebral toxoplasmosis
-
Additional diagnostics, e.g.:
- CT/MRI of the brain for suspected cerebral toxoplasmosis
- Fundoscopy for suspected ocular toxoplasmosis
Treatment
- Indications include immunosuppression; , pregnancy, and severe infection (e.g., active ocular toxoplasmosis).
- Treatment of choice
- Pyrimethamine PLUS sulfadiazine PLUS leucovorin
- Spiramycin for toxoplasmosis in pregnancy before the 18th week [10][11][12]
- For details, including dosages, see:
- “Treatment of cerebral toxoplasmosis”
- “Treatment of ocular toxoplasmosis”
Immunocompetent patients do not usually require treatment.
Cerebral toxoplasmosis
Description [5][8][13]
- A necrotizing encephalitis affecting immunocompromised individuals that is caused by reactivation of T. gondii
-
The most common neurological disorder associated with AIDS
- Considered an AIDS-defining condition
- Typically occurs at CD4 count < 100/μL
Clinical features [8]
- Fever
- Headache
- Mental status changes
- Seizures
- Focal neurological deficits
Diagnostics [8][13]
A definitive diagnosis requires the presence of clinical features, biopsy findings of T. gondii, and ≥ 1 mass lesion seen on imaging. Empiric treatment is usually initiated based on typical clinical features and currently available imaging and serology results. [8][13]
-
Imaging: CT or MRI with contrast
- Multiple ring-enhancing lesions (brain abscesses)
- Lesions located predominantly in the basal ganglia and/or the subcortical white matter
- CSF: pleocytosis, ↑ protein, PCR positive for T. gondii [14]
- Serology: IgM and IgG antibody tests [4]
-
Biopsy: may be required if treatment fails and/or to differentiate from other diagnoses [4][8]
- Toxoplasma tachyzoites: parasites in their replicative state; predominant during active infection
- Toxoplasma bradyzoites: parasites in their dormant state with reduced metabolism
- Chronic inflammation and necrosis of brain tissue [4]





Treatment of cerebral toxoplasmosis [15][16]
See “Approach to undifferentiated neurological symptoms in patients with HIV” for initial management of this patient group.
-
Preferred regimen [15]
- Pyrimethamine
- PLUS sulfadiazine
- PLUS leucovorin
- Treatment duration: at least 6 weeks, followed by chronic maintenance therapy
-
Supportive treatment [8]
- Patients with a history of seizures: anticonvulsants during the acute therapy phase
- Patients with AIDS: Initiate ART within 2–3 weeks (if not already started).
- Consider glucocorticoids if there is concern for mass effect.
- Disposition: Admission, potentially to a critical care unit, is usually required.
Primary CNS lymphoma is a differential diagnosis of cerebral toxoplasmosis. Until this differential is ruled out, avoid glucocorticoids, as they can alter neuroimaging and biopsy findings and may delay a diagnosis.
Prophylaxis for HIV patients [15]
- Adequate HIV treatment (cART)
- Trimethoprim/sulfamethoxazole
- See: “Prevention of opportunistic infections in HIV”
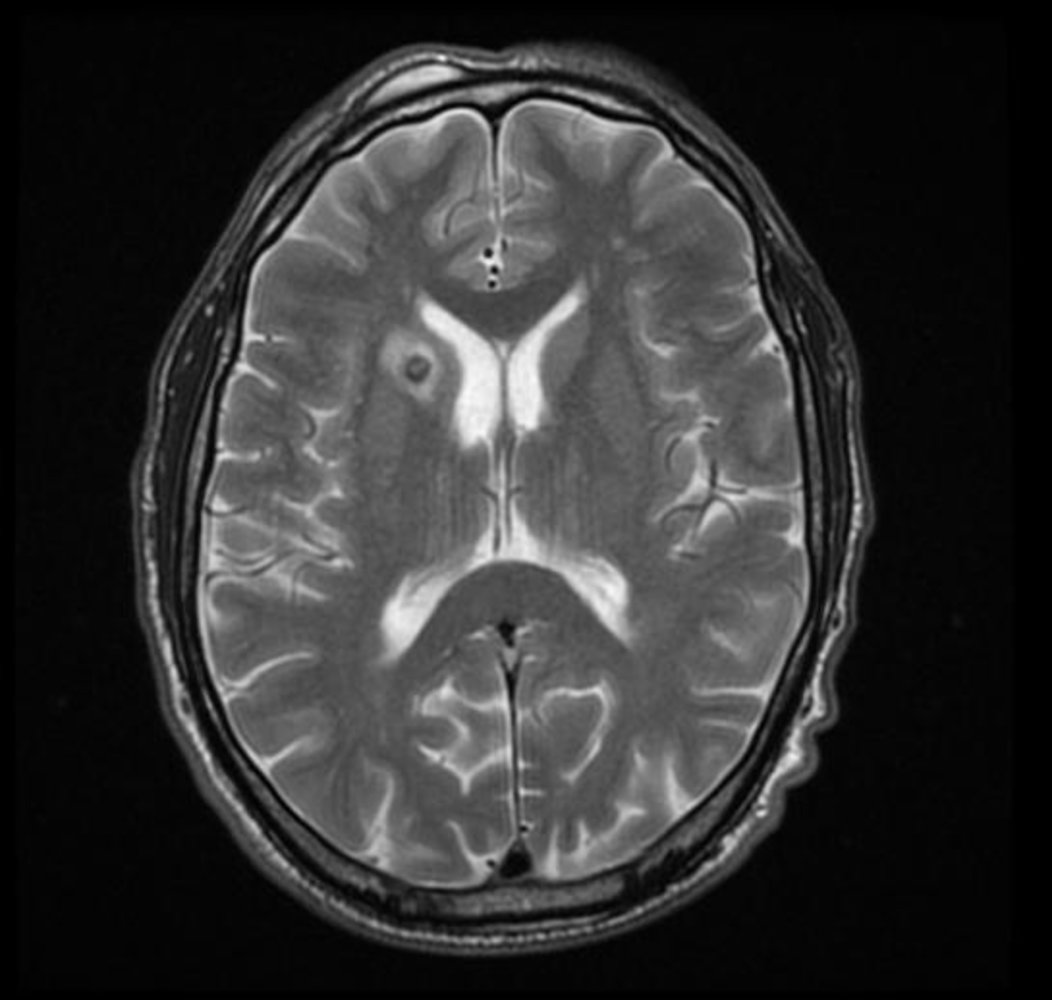
MRI head (T2-weighted; with contrast; axial plane) of a patient with cerebral toxoplasmosis
A small nodule (hatched overlay) in the right internal capsule is accompanied by hyperintense perilesional edema (solid overlay).
Neurotoxoplasmosis more commonly manifests with multiple lesions and it has a propensity for the corticomedullary junction, thalami, and basal ganglia. It is a leading cerebral opportunistic infection in patients with AIDS.
Source: “Intracranial toxoplasmosis 001.jpg” by Prashanth Saddala., Wikidoc, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
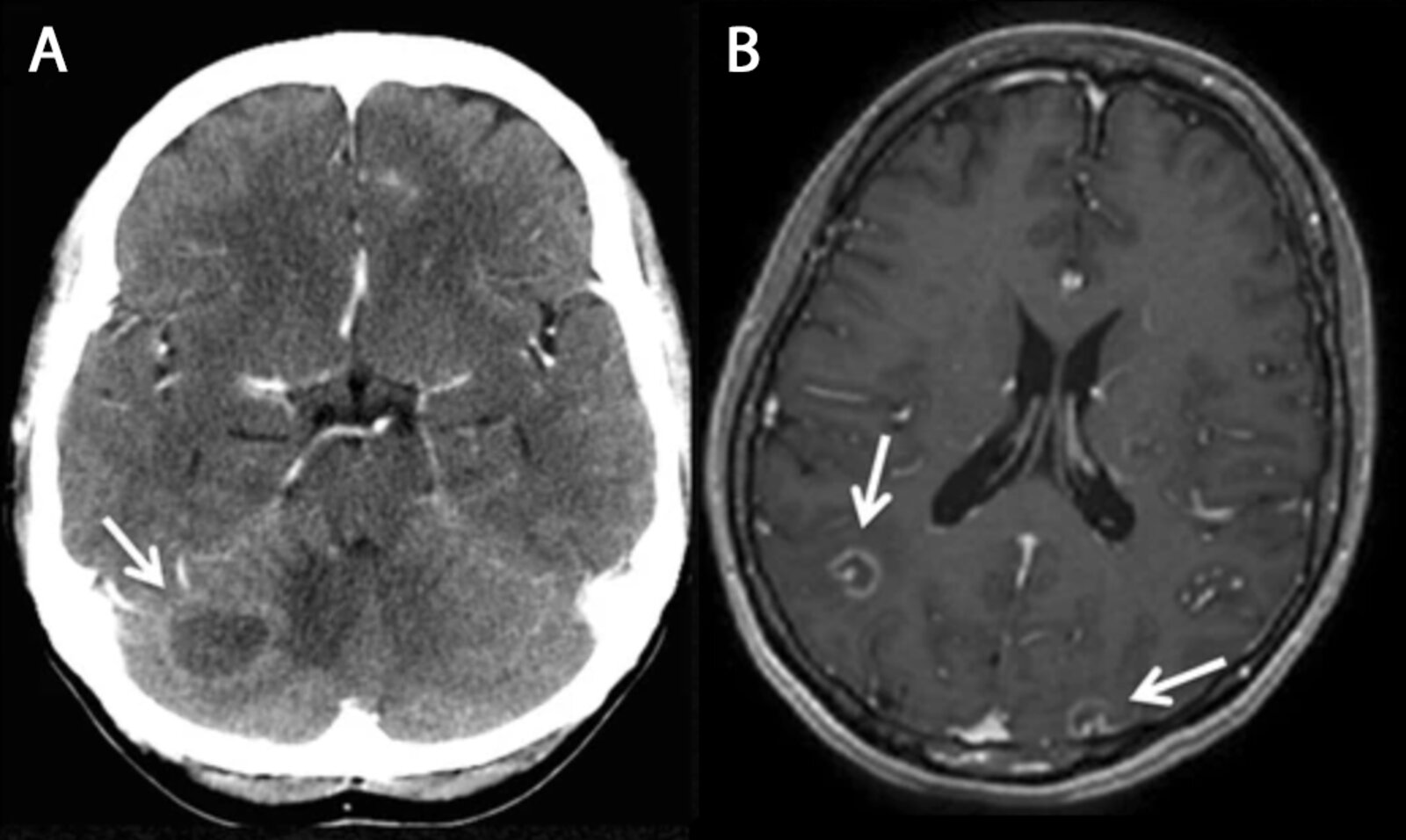
A: CT head (with contrast, axial plane); B: MRI head (with contrast, T1-weighted; axial plane) of a patient with AIDS
CT shows a ring-enhancing lesion (arrow) in the right cerebellar hemisphere. The two smaller cerebral lesions seen on MRI (arrows) contain eccentric enhancing nodules.
This appearance has been termed the “eccentric (or asymmetric) target sign” and is considered characteristic of toxoplasmosis.
Source: “Fig. 3, in: Unexpected hosts: imaging parasitic diseases” by Rodríguez Carnero, P., Hernández Mateo, P., Martín-Garre, S. et al., Insights Imaging, licensed under CC BY 4.0. Modifications: image cropped, letters replaced.
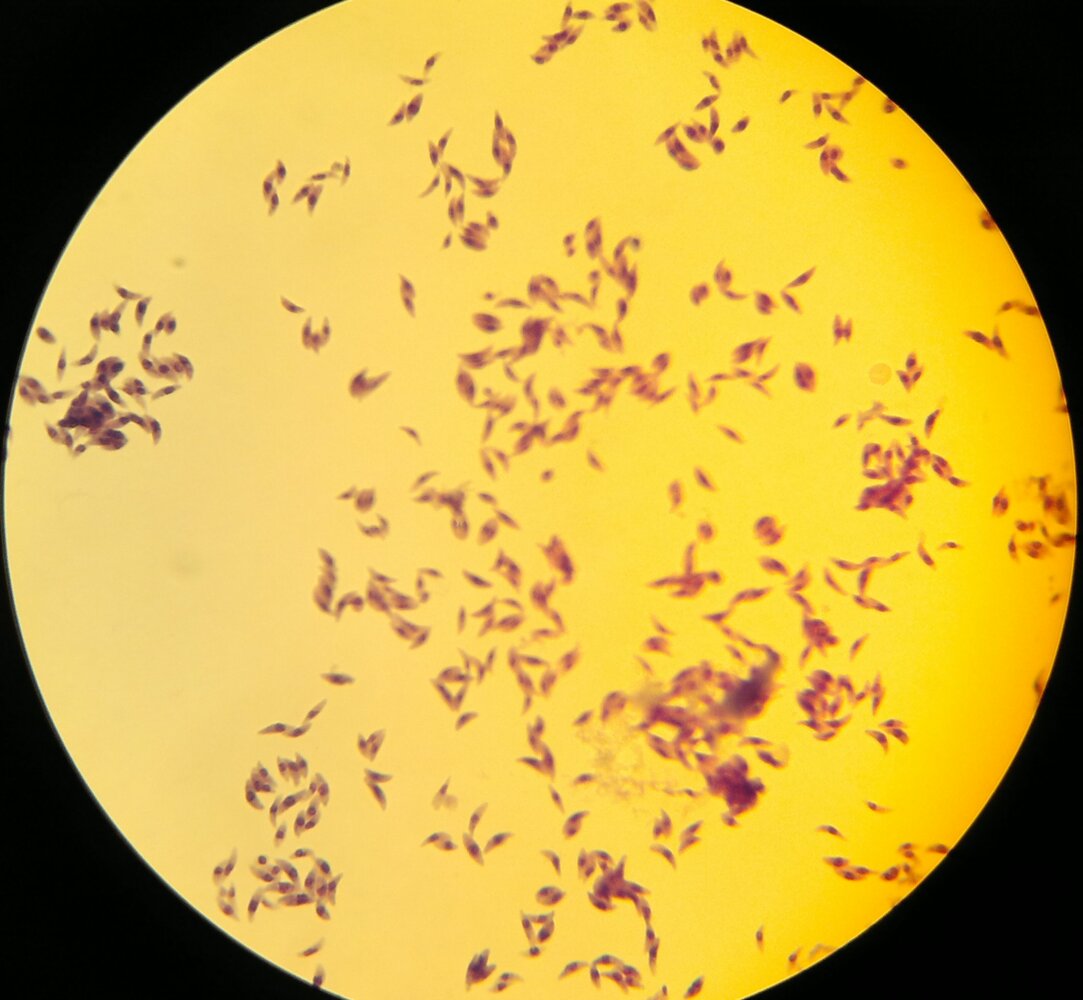
Photomicrograph of Toxoplasma gondii tachyzoites (Giemsa stain; 1000× magnification)
The tachyzoites have a crescent shape with a tapered anterior end and a large nucleus set centrally.
Source: “T. gondii tachyzoites” by Persian Microbiologist, Wikimedia Commons, licensed under CC BY-SA 4.0. Modifications: Image cropped.
{kind=link}
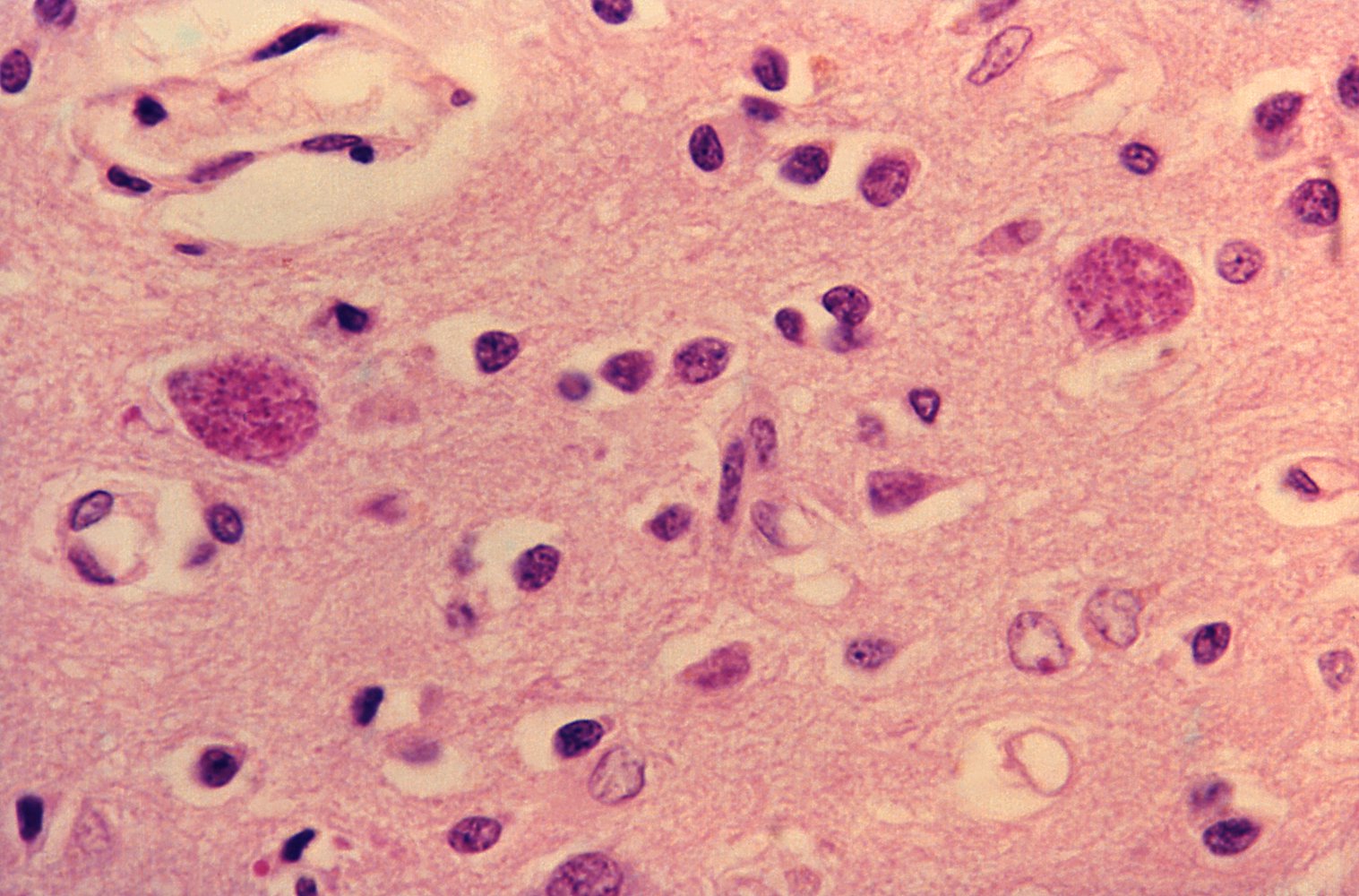
Photomicrograph of brain tissue specimen (H&E stain; very high magnification)
Two cystic structures (blue overlay) are visible, containing numerous Toxoplasma gondii pathogens (protozoan parasites, the causative organism of toxoplasmosis) in the bradyzoite stage.
In toxoplasmosis, CNS involvement is typically seen in severely immunocompromised patients.
Source: "14379", Jonathan W.M. Gold, M.D., Centers for Disease Control and Prevention (CDC) licensed under Public Domain
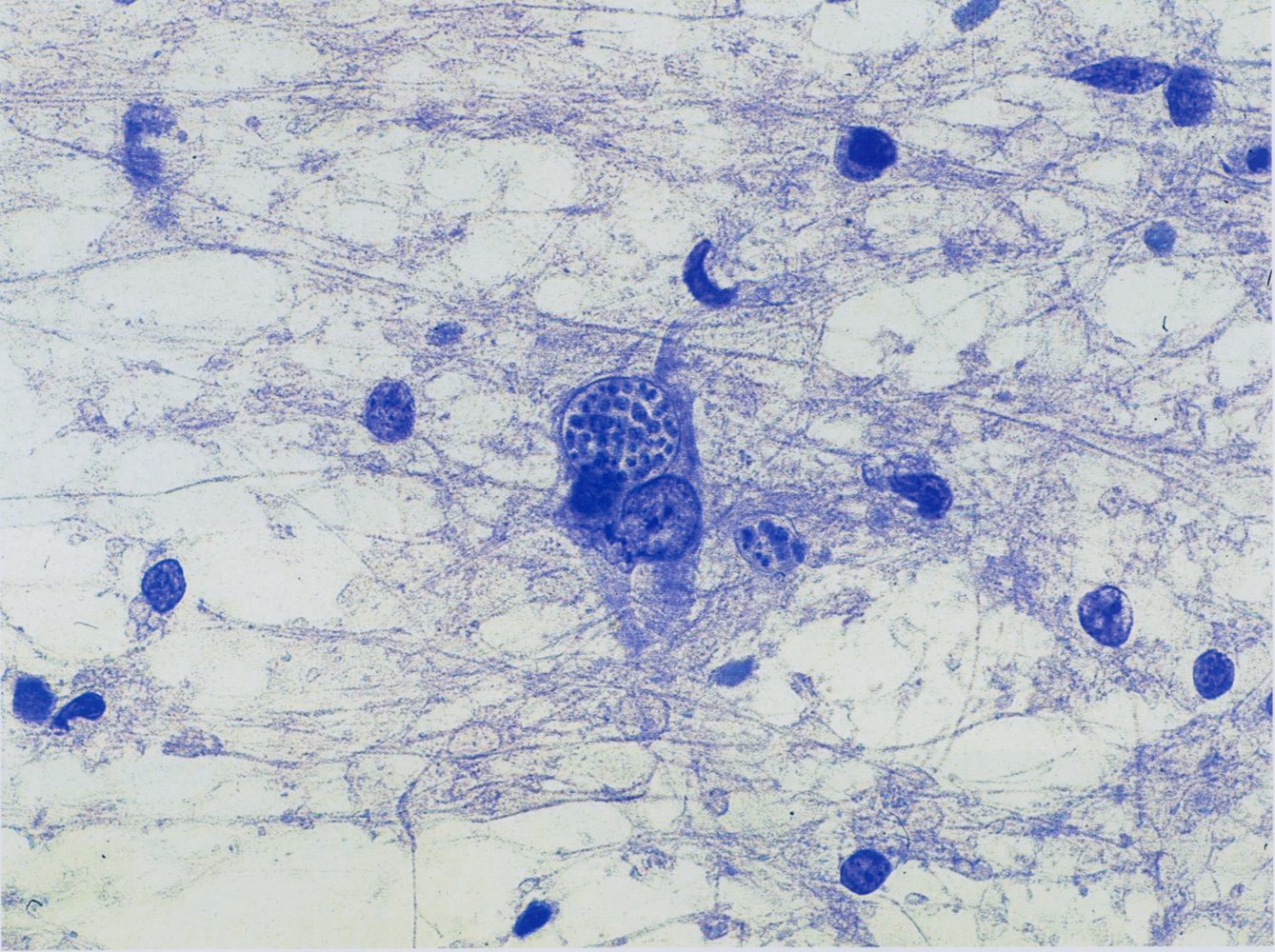
Photomicrograph of a stereotactic brain biopsy smear from a cerebral toxoplasmosis lesion (Giemsa stain; very high magnification)
The cystic structure in the center of the image (circled in green) is an intracellular (i.e., within a neuron) encapsulated colony of Toxoplasma gondii in the bradyzoite stage. There is necrotic tissue surrounding the neuron.
These microscopic findings are characteristic of cerebral toxoplasmosis.
Source: © IMPP
Ocular toxoplasmosis
Clinical features [17][18]
-
Chorioretinitis
- Visual impairment, floaters, scotomas
- Defects in the visual field at the site of inflammation
- Pain (but may be painless in some patients)
- Optic atrophy or macular scar formation can progress to blindness.
- Typically self-limited in immunocompetent patients
- Frequently recurrent in immunocompromised patients
- Retinochoroiditis juxtapapillaris (Jensen disease): visual field defects caused by retinochoroidal lesions adjacent to the optic disc [19]
Diagnostics [18]
Ocular toxoplasmosis is typically a clinical diagnosis.
-
Fundoscopy
-
Acute toxoplasmosis [20]
- Yellow-white retinal lesion
- Marked vitreous reaction: Severe vitritis may result in a "headlight in the fog” appearance.
- Concomitant vasculitis
-
Previous toxoplasmosis
- Formation of scars with white atrophic areas
- Dark, sharply defined retinal pigmentation
-
Acute toxoplasmosis [20]
- Adjunctive tests: PCR or antibody titers of ocular fluid if the diagnosis is uncertain

")

Treatment of ocular toxoplasmosis [18][21][22]
-
Preferred regimens
- Pyrimethamine PLUS sulfadiazine PLUS leucovorin
- OR trimethoprim/sulfamethoxazole (off-label)
- Treatment duration: 4–6 weeks
- Supportive treatment: Consider adding glucocorticoids after initial antibiotic therapy. [21]
Fundus photography of a right eye
There is a peripapillary zonal inflammatory lesion (green overlay) with vitreous infiltration (fundus details are slightly blurred).
M: macula; P: papilla (optic disc)
Source: © IMPP

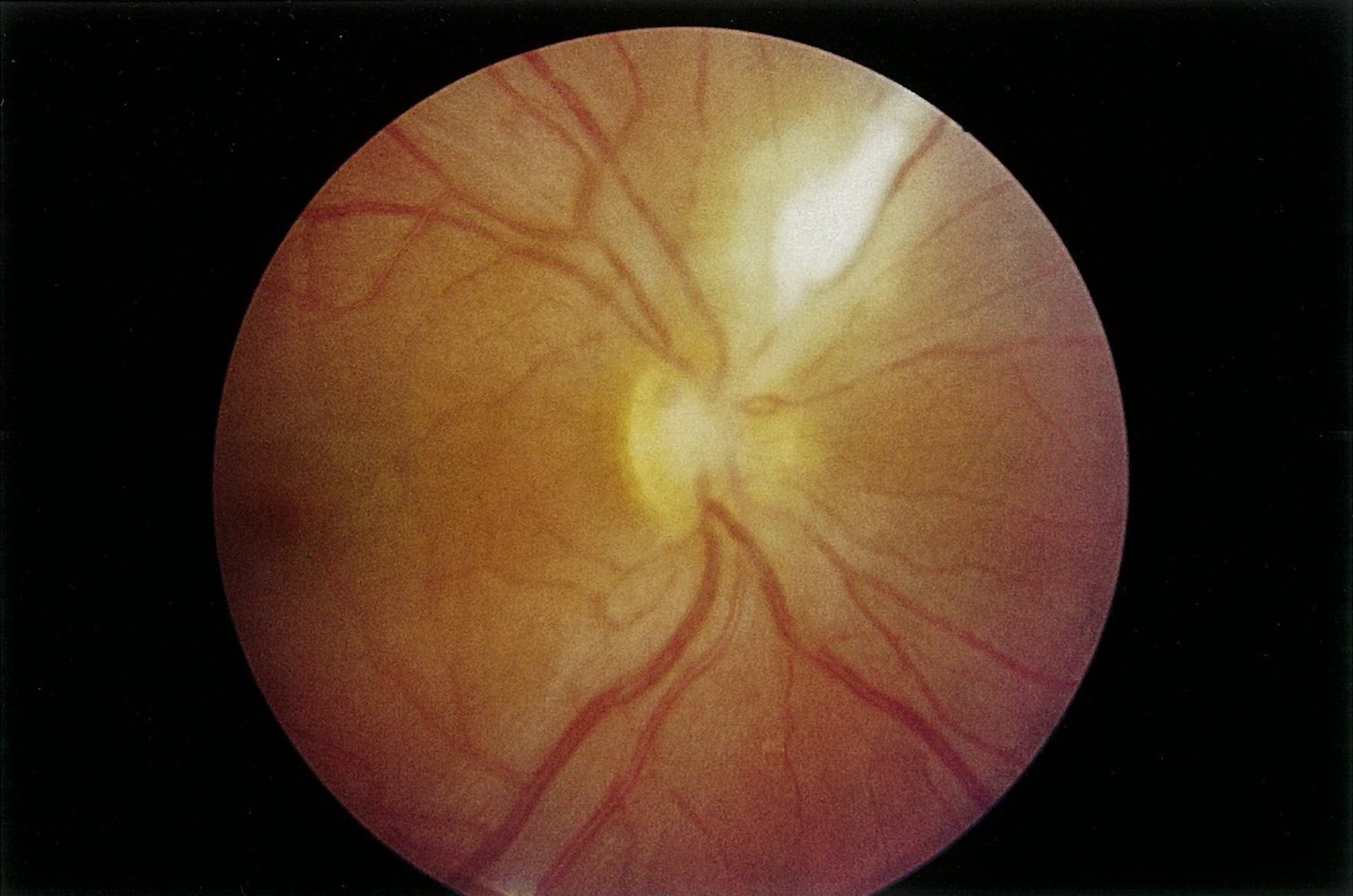
Fundus photography of a right eye
The image appears cloudy, which is consistent with vitreous opacity. There is a yellow-white, fluffy retinal lesion (blue overlay) at the temporal superior vascular arch. The pigmented scar (arrowhead) in the nasal area is most likely the remnant of a previous manifestation of toxoplasmosis. In addition, the optic disc (circle) appears blurred.
M: macula
Source: © IMPP
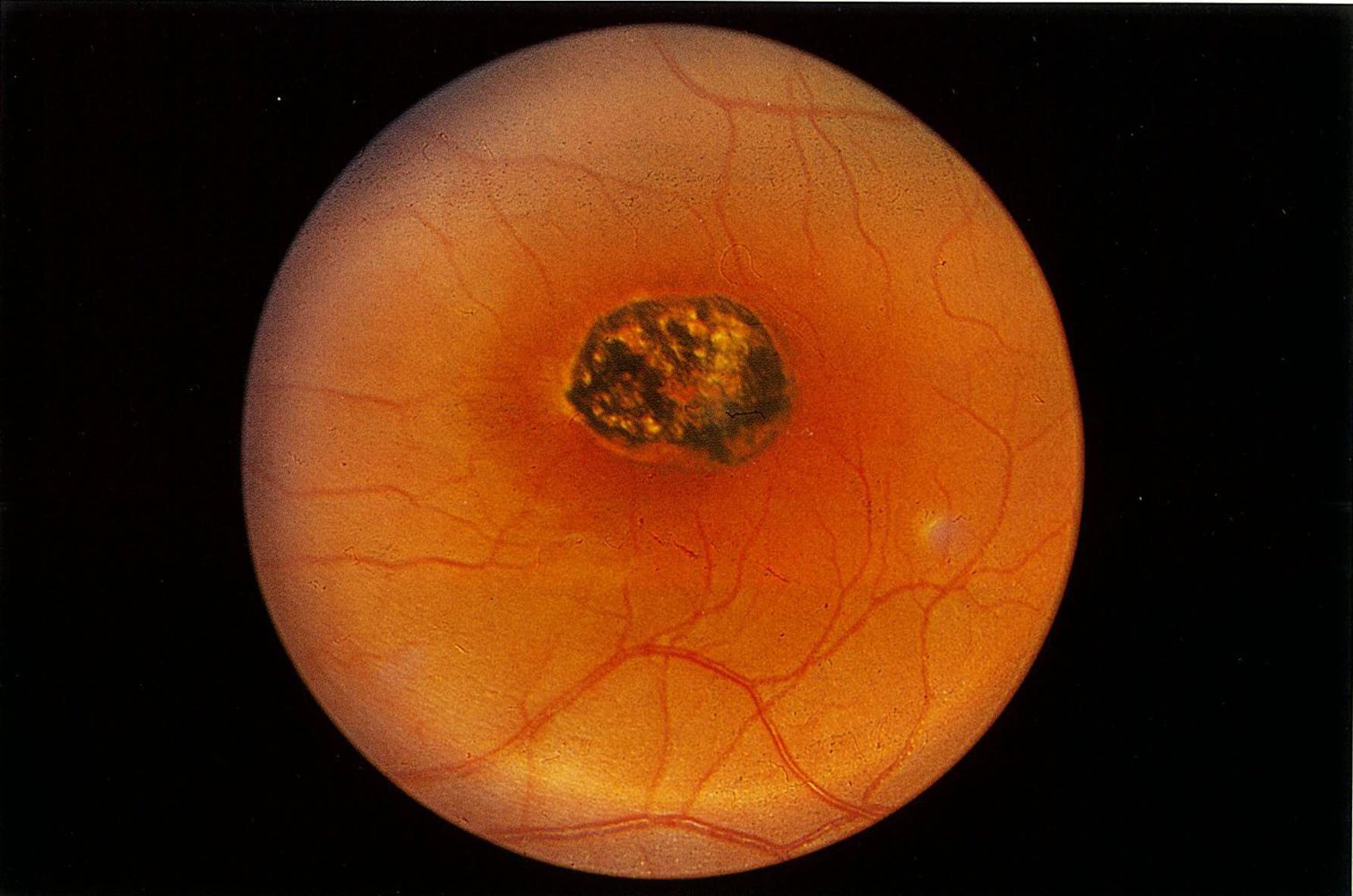
Fundus photography of the left eye of an infant (optic disc not shown)
The macular area shows a sharply demarcated scar with depigmentation and hyperpigmentation, affecting both the retina and choroid. This clinical finding is a typical sign of congenital toxoplasmosis.
Source: © IMPP
External Resources
References
- "Parasites - Toxoplasmosis (Toxoplasma infection): Epidemiology & Risk Factors". https://web.archive.org/web/20170527044503/https://www.cdc.gov/parasites/toxoplasmosis/epi.html. [2015-03-26]
- "Toxoplasma gondii: from animals to humans". https://www.ncbi.nlm.nih.gov/pubmed?term=11113252. [2000-11-01]
- Centers for Disease Control and Prevention. "CDC Yellow Book 2020". Oxford University Press, USA. (2019). ISBN: 9780190065973
- Robert-Gangneux F, Dardé ML. "Epidemiology of and Diagnostic Strategies for Toxoplasmosis". Clin Microbiol Rev. 25(2). :264-296. (2012)
- Jones JL, Parise ME, Fiore AE. "Neglected Parasitic Infections in the United States: Toxoplasmosis". Am J Trop Med Hyg. 90(5). :794-799. (2014)
- Goldman L, Schafer AI. "Goldman-Cecil Medicine, 2-Volume Set". Elsevier. (2019). ISBN: 9780323532662
- Furtado J, Smith J, Belfort R, Gattey D, Winthrop K. "Toxoplasmosis: A global threat". J Glob Infect Dis. 3(3). :281. (2011)
- "Guidelines for the Prevention and Treatment of Opportunistic Infections in Adults and Adolescents with HIV: 2021 update". https://web.archive.org//web/20220807093439/https://clinicalinfo.hiv.gov/sites/default/files/guidelines/documents/adult-adolescent-oi/guidelines-adult-adolescent-oi.pdf. [2021-06-22]
- Reiter-Owona I. "Laboratory diagnosis of toxoplasmosis – possibilities and limitations". J Lab Med. 29(6). :439-445. (2005)
- Konstantinovic N, Guegan H, Stäjner T, Belaz S, Robert-Gangneux F. "Treatment of toxoplasmosis: Current options and future perspectives". Food Waterborne Parasitol. 15. :e00036. (2019)
- "Clinical Care of Toxoplasmosis". https://web.archive.org/web/20250819094742/https://www.cdc.gov/toxoplasmosis/hcp/clinical-care/index.html. [2024-01-22]
- Cantey PT, Montgomery SP, Straily A. "Neglected Parasitic Infections: What Family Physicians Need to Know-A CDC Update". Am Fam Physician. 104(3). :277-287. (2021)
- Halonen SK, Weiss LM. "Toxoplasmosis". Handb Clin Neurol. :125-145. (2013)
- Brogi E, Cibas ES. "Cytologic Detection of Toxoplasma gondii Tachyzoites in Cerebrospinal Fluid". Am J Clin Pathol. 114(6). :951-955. (2000)
- "Guidelines for the Prevention and Treatment of Opportunistic Infections in Adults and Adolescents with HIV". https://web.archive.org/web/20240225045201/https://clinicalinfo.hiv.gov/en/guidelines/hiv-clinical-guidelines-adult-and-adolescent-opportunistic-infections/candidiasis. [2024-01-10]
- Vidal JE. "HIV-Related Cerebral Toxoplasmosis Revisited: Current Concepts and Controversies of an Old Disease". J Int Assoc Provid AIDS Care. 18. :232595821986731. (2019)
- Cunningham ET, Margolis TP. "Ocular Manifestations of HIV Infection". N Engl J Med. 339(4). :236-244. (1998)
- Ozgonul C, Besirli CG. "Recent Developments in the Diagnosis and Treatment of Ocular Toxoplasmosis". Ophthalmic Res. 57(1). :1-12. (2016)
- Eckert GU, Melamed J, Menegaz B. "Optic nerve changes in ocular toxoplasmosis". Eye. 21(6). :746-751. (2006)
- Aleixo AL, Curi AL, Benchimol EI, Amendoeira MR. "Toxoplasmic Retinochoroiditis: Clinical Characteristics and Visual Outcome in a Prospective Study". PLoS Negl Trop Dis. 10(5). :e0004685. (2016)
- Harrell M, Carvounis PE. "Current Treatment of Toxoplasma Retinochoroiditis: An Evidence-Based Review". J Ophthalmol. 2014. :1-7. (2014)
- "Clinical Care of Toxoplasmosis". https://web.archive.org/web/20240711152913/https://www.cdc.gov/toxoplasmosis/hcp/clinical-care/index.html. [2024-01-22]
- "Toxoplasmosis in the adult". https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1749356/pdf/bullnyacadmed00169-0109.pdf. [1974-02-01]