Summary
Transfusion of whole blood or fractionated blood components is a widely used method for managing numerous conditions. Packed red blood cells (pRBCs), the most commonly transfused products, are primarily used for the treatment of acute and chronic blood loss. RBC transfusion elevates hemoglobin (Hb) levels and helps maintain organ perfusion and tissue oxygenation. The decision to transfuse RBCs is based on the patient's Hb level, hemodynamic status, and comorbidities (e.g., cardiovascular disease). Fresh frozen plasma (FFP), cryoprecipitate, platelet, and clotting factor transfusions are also available. Pretransfusion testing must be performed, unless in an emergency situation, to minimize the risk of transfusing incompatible RBCs and subsequent transfusion reactions. Testing involves blood typing (ABO and Rhesus) of the recipient's blood, RBC antibody screening of the recipient's serum or plasma, and compatibility testing (crossmatching recipient serum or plasma and donor RBCs).
See also “Transfusion reactions.”
Blood type systems
There are more than 250 antigens on the RBC surface, which are classified into several antigen-antibody systems or blood groups. Blood type is most commonly communicated as a combination of ABO blood type and Rhesus blood type (e.g., O- for blood type O Rh-negative blood products and AB+ for blood type AB Rh-positive blood products). [1]
ABO blood type system [1]
- Consists of the presence or absence of 2 antigens
- A (A antigen)
- B (B antigen)
- O (without antigen)
- Newborns have a lower occurrence of A and B antigens on RBCs than adults.
-
Inheritance pattern
- A and B are codominant
- O is recessive
- 6 genotypes give rise to 4 phenotypes
- Anti-A and/or anti–B antibodies
- Typically form spontaneously in antigen-negative individuals, i.e., without prior exposure to antigen-positive RBCs
- Can trigger acute hemolytic transfusion reactions upon an individual's first contact with ABO-incompatible RBCs
| ABO blood types [2] | ||||
|---|---|---|---|---|
| Type | Blood type O | Blood type A | Blood type B | Blood type AB |
| Prevalence | ∼ 45% | ∼ 40% | ∼ 10% | ∼ 5% |
| Antigens on RBCs | No antigens | A antigen | B antigen | A and B antigens |
| Antibodies in plasma | Anti-A and anti-B antibodies | Anti-B antibodies | Anti-A antibodies | No antibodies |
| Can receive RBCs from | O | A, O | B, O | AB, A, B, O (universal RBC recipients) |
| Can donate RBCs to | O, A, B, AB (universal RBC donors) | A, AB | B, AB | AB |
| Can receive FFP from | O, A, B, AB (universal FFP recipients) | A, AB | B, AB | AB |
| Can donate FFP to | O | A, O | B, O | AB, A, B, O (universal FFP donors) |
Individuals with blood type O can only receive RBCs from other blood type O donors. RBCs from donors of any other type (e.g., A, B, or AB) can cause acute hemolytic transfusion reactions.





Rhesus blood type system [1]
- Consists of > 45 Rhesus (Rh) antigens of which Rh(D) antigen is the most immunogenic and clinically significant [2]
- The Rh(D) antigen is dominant over other Rhesus antigens.
- In clinical practice, Rh status typically refers to the presence or absence of Rh(D) antigen, despite the existence of other Rh antigens (see “Extended RBC antigens”).
- Anti-Rh antibodies
- Usually only form in antigen-negative individuals after exposure to antigen-positive RBCs, e.g., transfusion, fetomaternal hemorrhage
- Can lead to hemolytic disease of the fetus and newborn (HDFN) and/or delayed hemolytic transfusion reactions (DHTR) in sensitized individuals
| Rh blood types [2] | ||
|---|---|---|
| Type | Rh-negative | Rh-positive |
| Prevalence | 1–15% [2] | 85–99% [2] |
| Rh(D) antigen on RBCs | Absent | Present |
| Antibodies in plasma | Anti-Rh antibodies can form after sensitization | No anti-Rh antibodies |
| Can receive RBCs from | Rh negative (preferably) | Rh positive, Rh negative |
| Can donate RBCs to | Rh negative, Rh positive | Rh positive |
In Rh-negative women of childbearing age, exposure to Rh-positive RBCs (e.g., by transfusion or fetomaternal hemorrhage) can trigger maternal Rh alloimmunization, which can cause HDFN in subsequent pregnancies. Rh-negative donor blood is therefore preferred in these patients, however, Rh-positive blood is acceptable if an emergency transfusion is required.
FFP transfusions do not need to be Rh-compatible as the risk of transfusion reactions and/or subsequent alloimmunization is low. [3]









Extended RBC antigen systems [4]
Several other antigen groups can trigger antibody formation in antigen-negative individuals after exposure to antigen-positive RBCs. Only some cause clinically significant hemolytic anemias and/or transfusion reactions.
- Rhesus antigen system: Most non-D Rh antigens, e.g., Rh(C) and Rh(E), are less frequent and typically considered among the spectrum of extended RBC antigens. [2]
-
Kell antigen system
- A group of RBC antigens, which includes K (K1), k (K2), Kpa, Kpb, Jsa, and Jsb antigens
- A homozygote for the Ko allele expresses no Kell antigens
- Responsible for up to 10% of severe cases of HDFN and capable of causing hemolytic transfusion reactions
-
Duffy antigen system [5]
- A group of six glycoprotein receptors found on RBCs that are encoded on chromosome 1
- Plasmodium vivax binds to Duffy antigens to invade RBCs and cause malaria.
- Antibodies against Duffy antigen can also cause transfusion reactions and hemolytic disease of the newborn.
-
Kidd antigen system [6]
- A rare group of three RBC antigens: Jka (JK1), Jkb (JK2), and JK3
- Also expressed in the epithelium of descending vasa recta, where they play an important role as urea transporters
-
MNS antigen system [7]
- A group of more than 40 RBC antigens, including M, N, S, s, and U antigens
- MNS antigens are carried on glycophorin A and B and are fully developed at birth.
- Less likely to be clinically significant than other antigen-antibody systems [1]
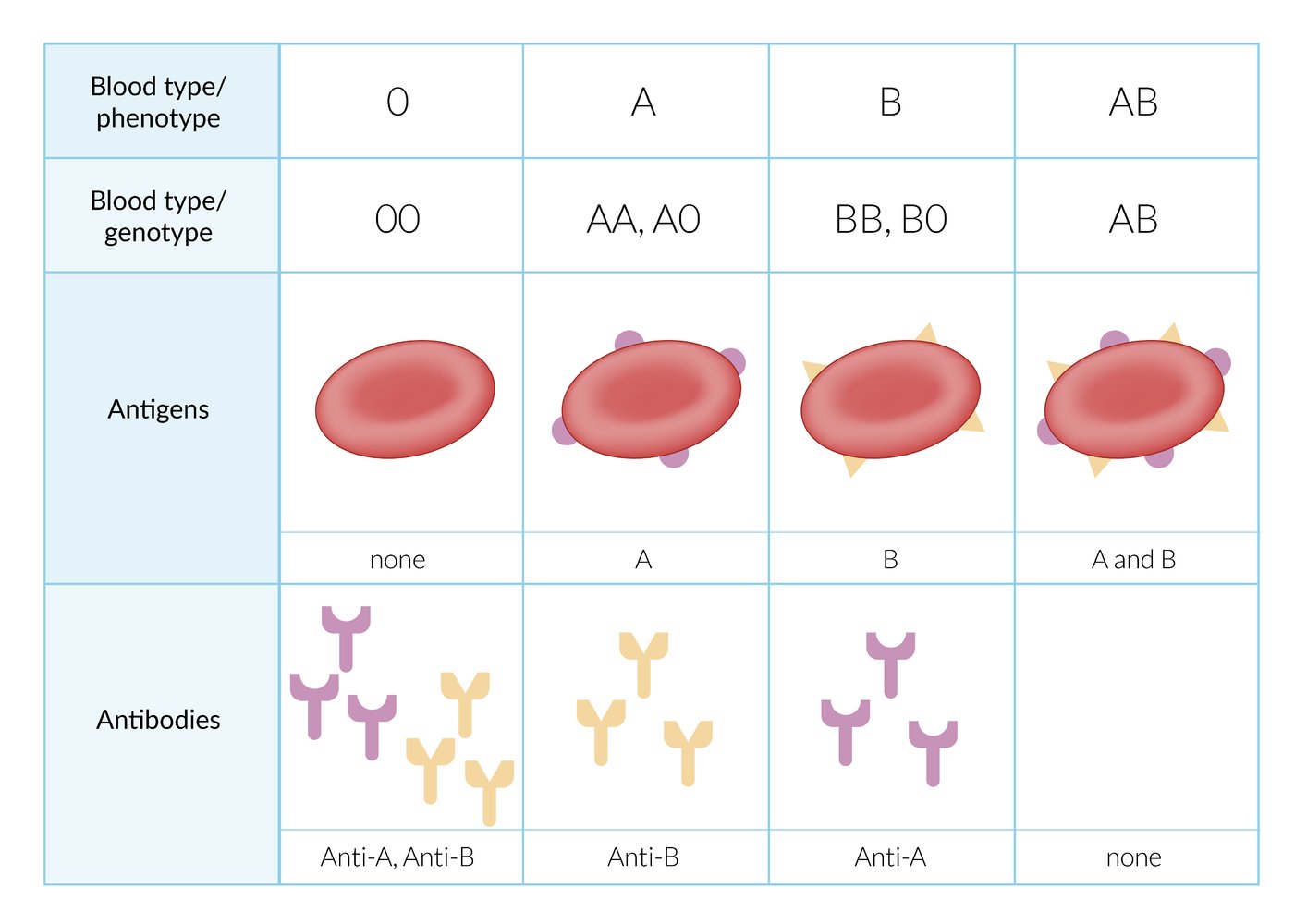
The ABO blood group system classifies four blood types (ABO phenotypes): O, A, B, and AB. These blood types are determined by the presence of antigens A and/or B on the surface of RBCs and the presence of antibodies against the antigens that are absent from the surface of an individual's RBC. Specific genes (ABO genotype) determine the expression of A and B surface antigens. ABO antibodies can cause potentially life-threatening agglutination and hemolysis upon contact with their corresponding antigen (e.g., the anti-A antibody will react with antigen A).
© AMBOSS
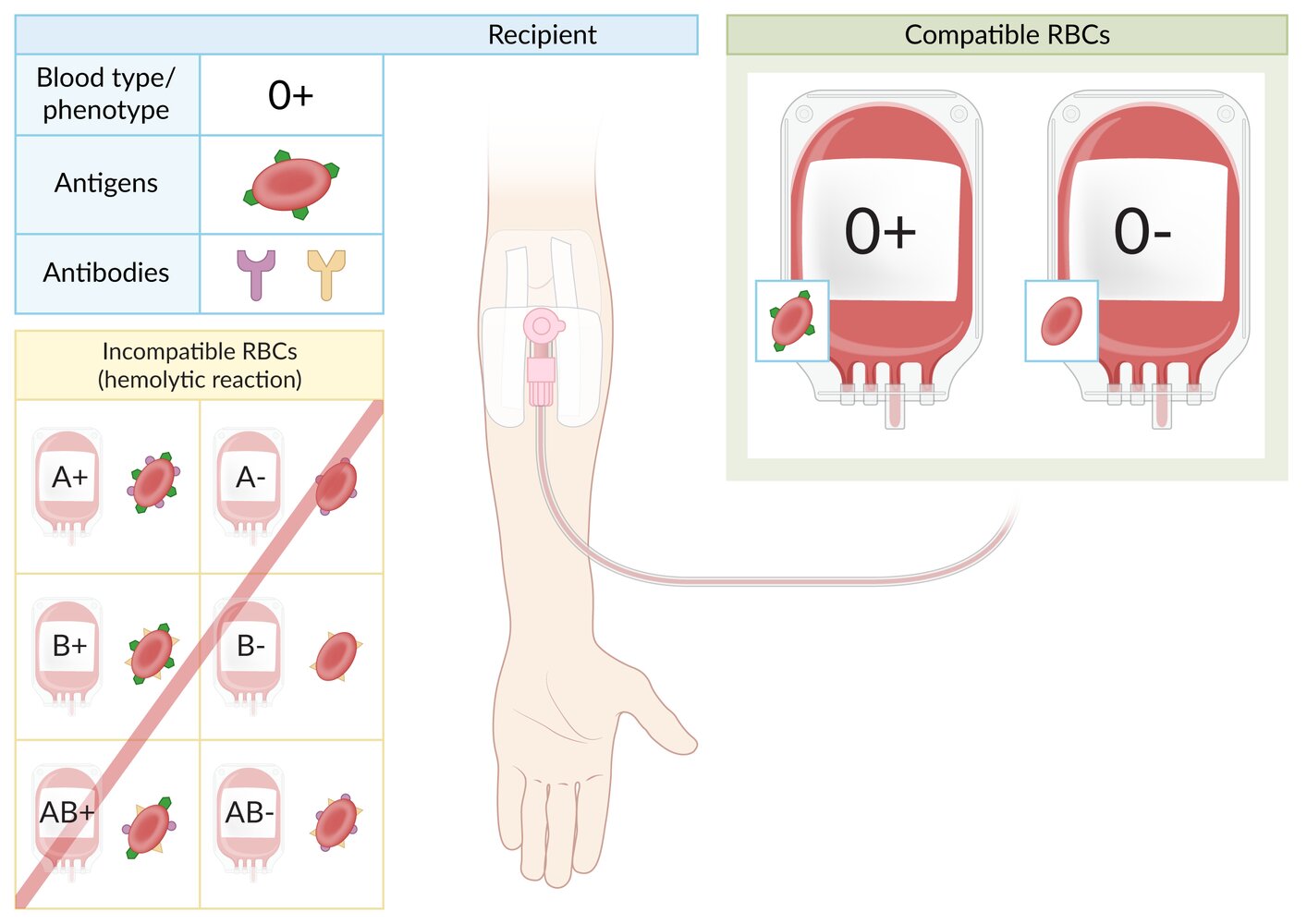
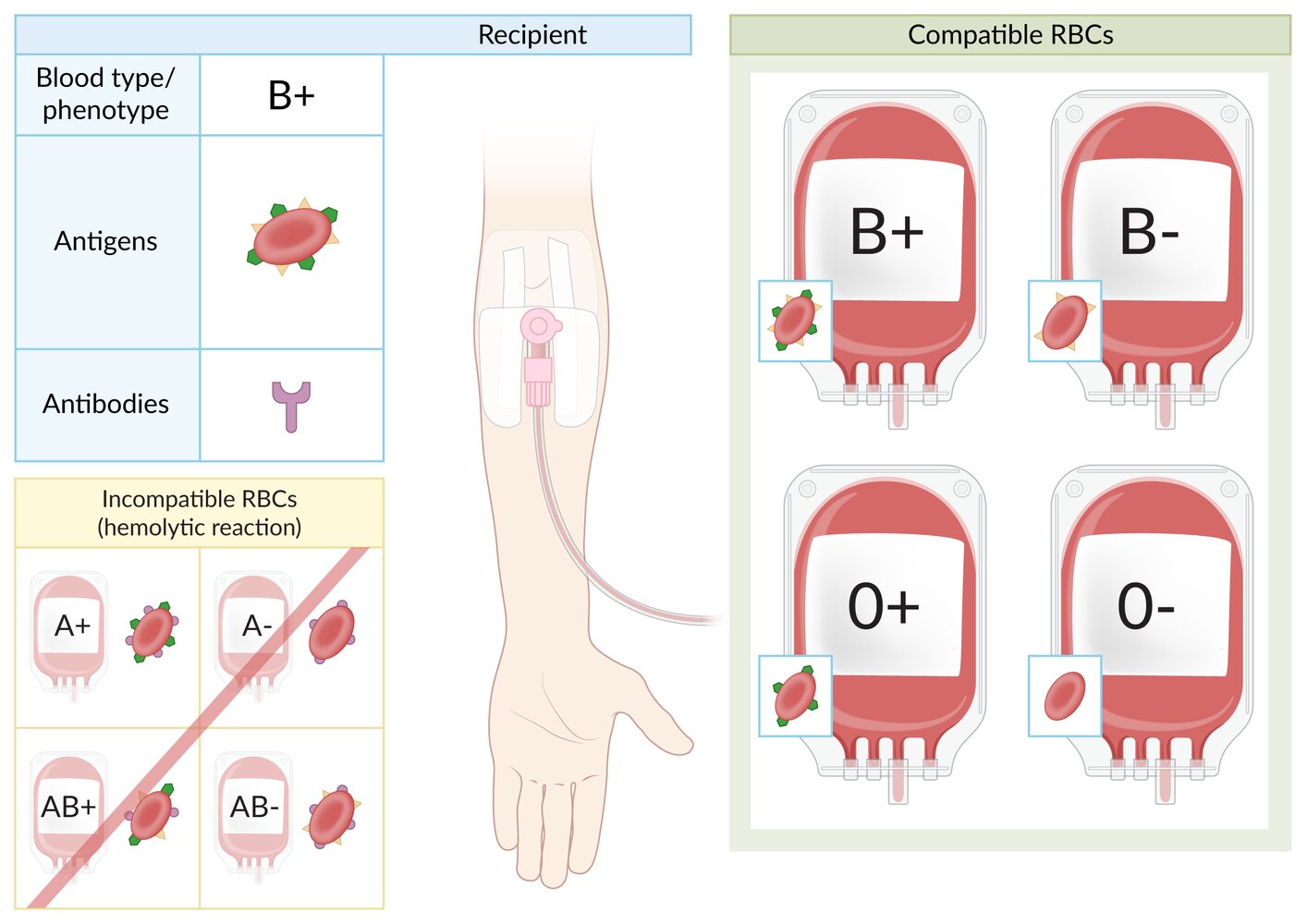
Individuals with blood type O+ have Rh factor antigens (green) on the surface of red blood cells (RBCs) and anti-A antibodies (purple) and anti-B antibodies (yellow) in the plasma.
O+ individuals can receive O+ or O- packed RBCs. They cannot receive A, B, or AB RBCs, regardless of Rh status, because they contain A and/or B antigens, which will trigger a hemolytic reaction.
© AMBOSS
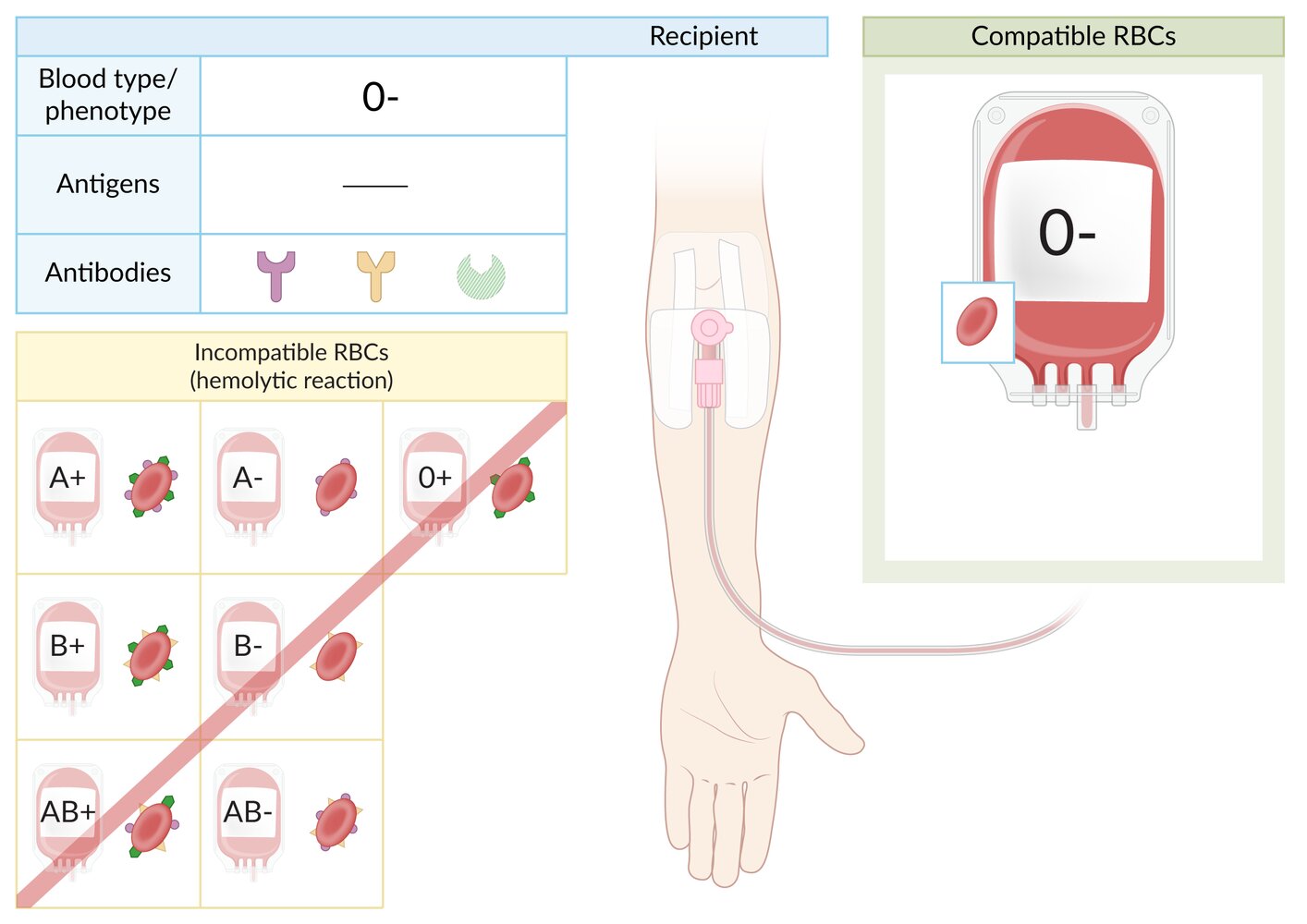
Individuals with blood type O- have no antigens on the surface of red blood cells (RBCs) and are therefore universal donors of packed RBCs, and have anti-A antibodies (purple) and anti-B antibodies (yellow) in the plasma. They may have anti-Rh antibodies (green) if they were previously exposed to Rh+ blood (Rh sensitization).
O- individuals can only receive O- packed RBCs. They cannot receive A, B, or AB RBCs, regardless of Rh status, because they contain A and/or B antigens, which will trigger a hemolytic reaction. They also should not receive O+ RBCs because they contain Rh antigens, which may trigger Rh sensitization or hemolysis in previously sensitized individuals.
Note: In case of emergency and no prior Rh sensitization, O- individuals may receive O+ RBCs.
© AMBOSS
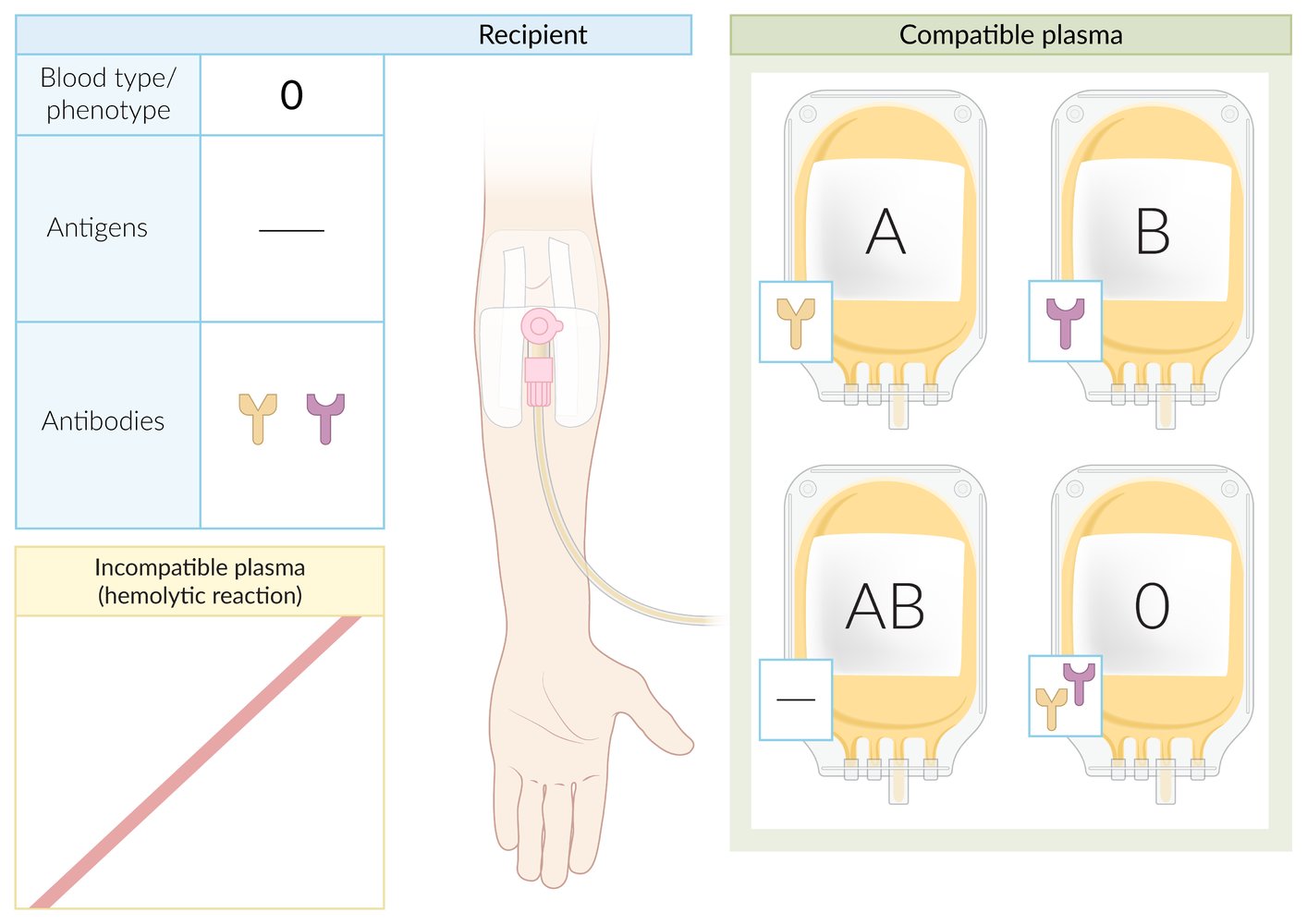
Individuals with blood type O have no blood type antigens on the surface of red blood cells and have anti-A and anti-B antibodies in the plasma. Blood type O individuals can receive plasma from donors of any blood type (i.e., blood type O individuals are universal plasma recipients).
Note: Rh factor compatibility is not relevant to plasma transfusions.
© AMBOSS
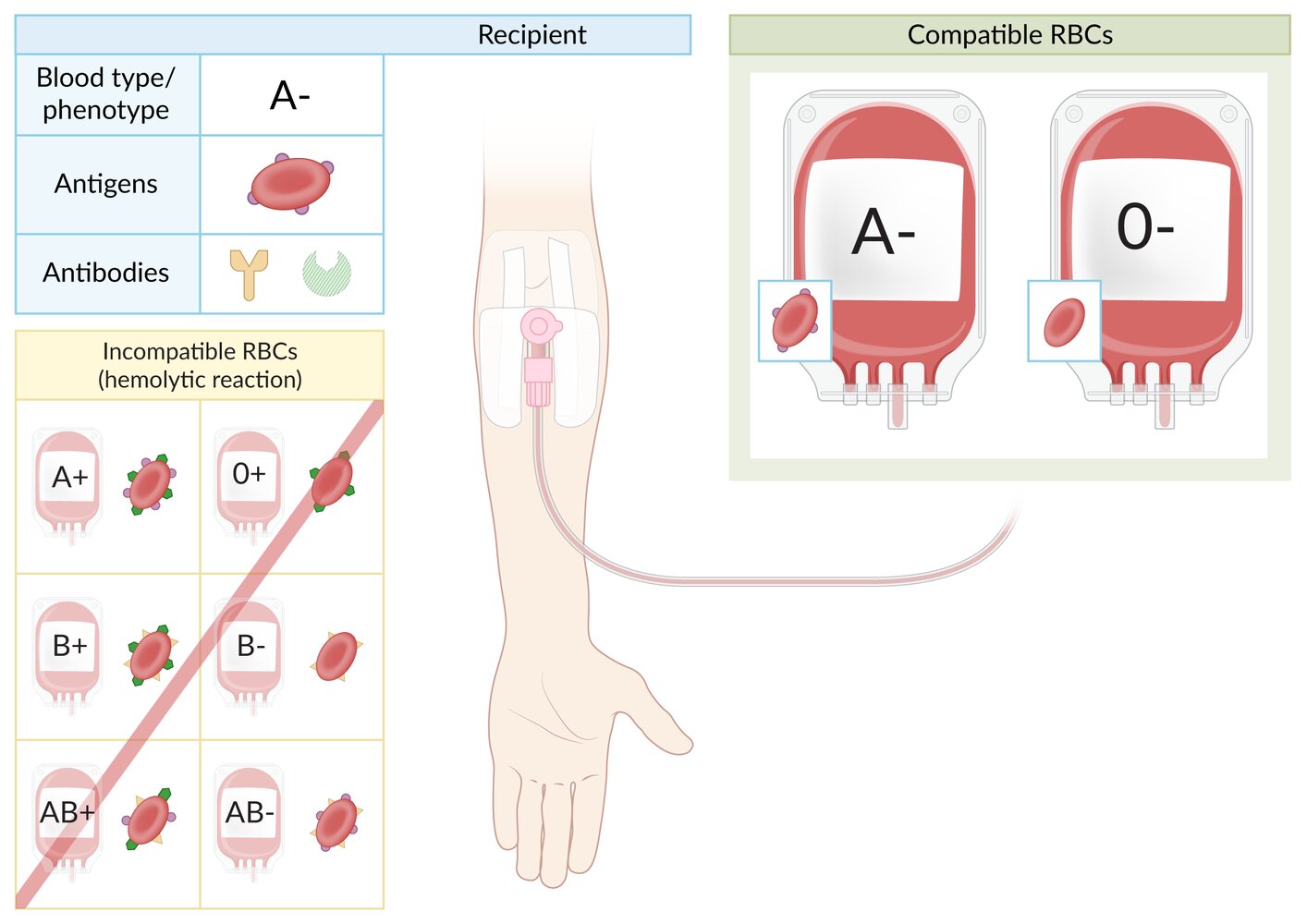
Individuals with blood type A- have A antigens (purple) on the surface of red blood cells (RBCs) and anti-B antibodies (yellow) in the plasma. They may have anti-Rh antibodies (green) if they were previously exposed to Rh+ blood (Rh sensitization).
A- individuals can receive A- or O- packed RBCs. They cannot receive B or AB RBCs, regardless of Rh status, because they contain B antigens, which will trigger a hemolytic reaction. They also should not receive A+ or O+ RBCs because they contain Rh antigens, which may trigger Rh sensitization or hemolysis in previously sensitized individuals.
Note: In case of emergency and no prior Rh sensitization, A- individuals may receive A+ or O+ RBCs.
© AMBOSS
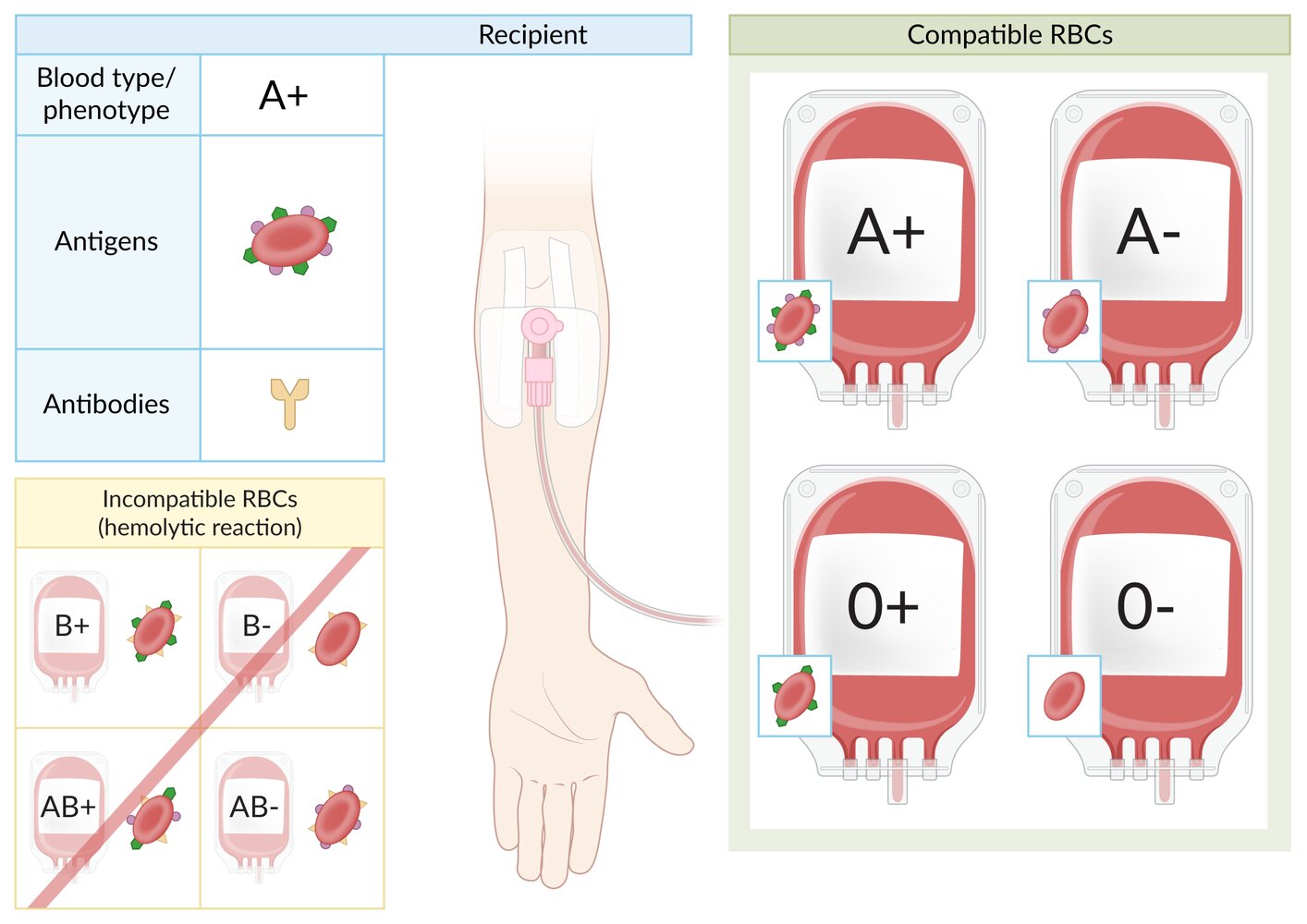
Individuals with blood type A+ have A antigens (purple) and Rh factor antigens (green) on the surface of red blood cells (RBCs) and anti-B antibodies (yellow) in the plasma.
A+ individuals can receive A+/- and O+/- packed RBCs. They cannot receive B or AB RBCs, regardless of Rh status, because they contain B antigens, which will trigger a hemolytic reaction.
© AMBOSS
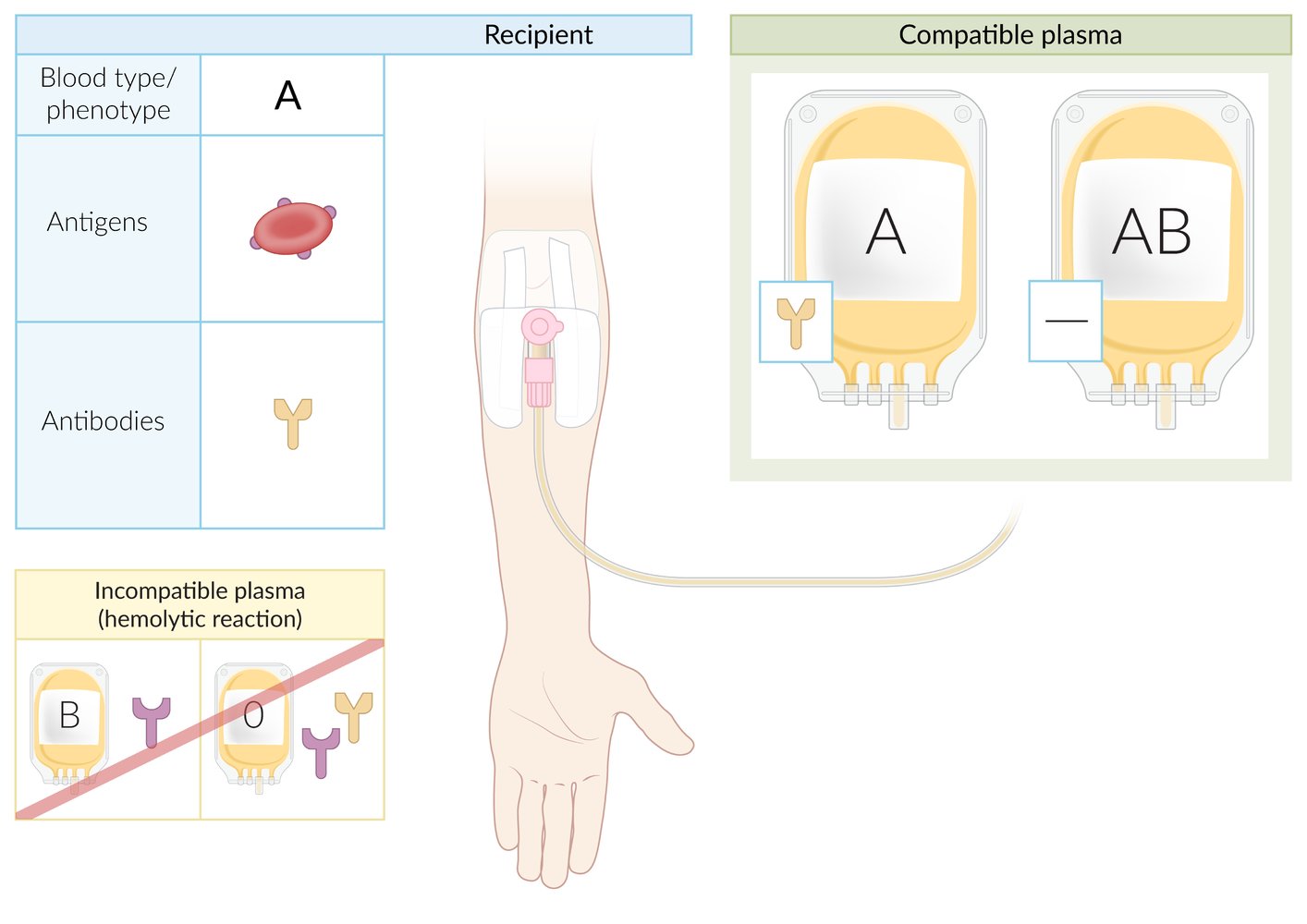
Individuals with blood type A have A antigens on the surface of red blood cells (RBCs) and anti-B antibodies in the plasma. Blood type A individuals can receive plasma from donors with blood types A or AB (blood type AB is a universal plasma donor because it lacks anti-A and anti-B antibodies).
Blood type A is not compatible with donations of blood types B and O because both contain anti-A antibodies, which can trigger a hemolytic reaction in blood type A recipients.
Note: Rh factor compatibility is not relevant to plasma transfusions.
© AMBOSS
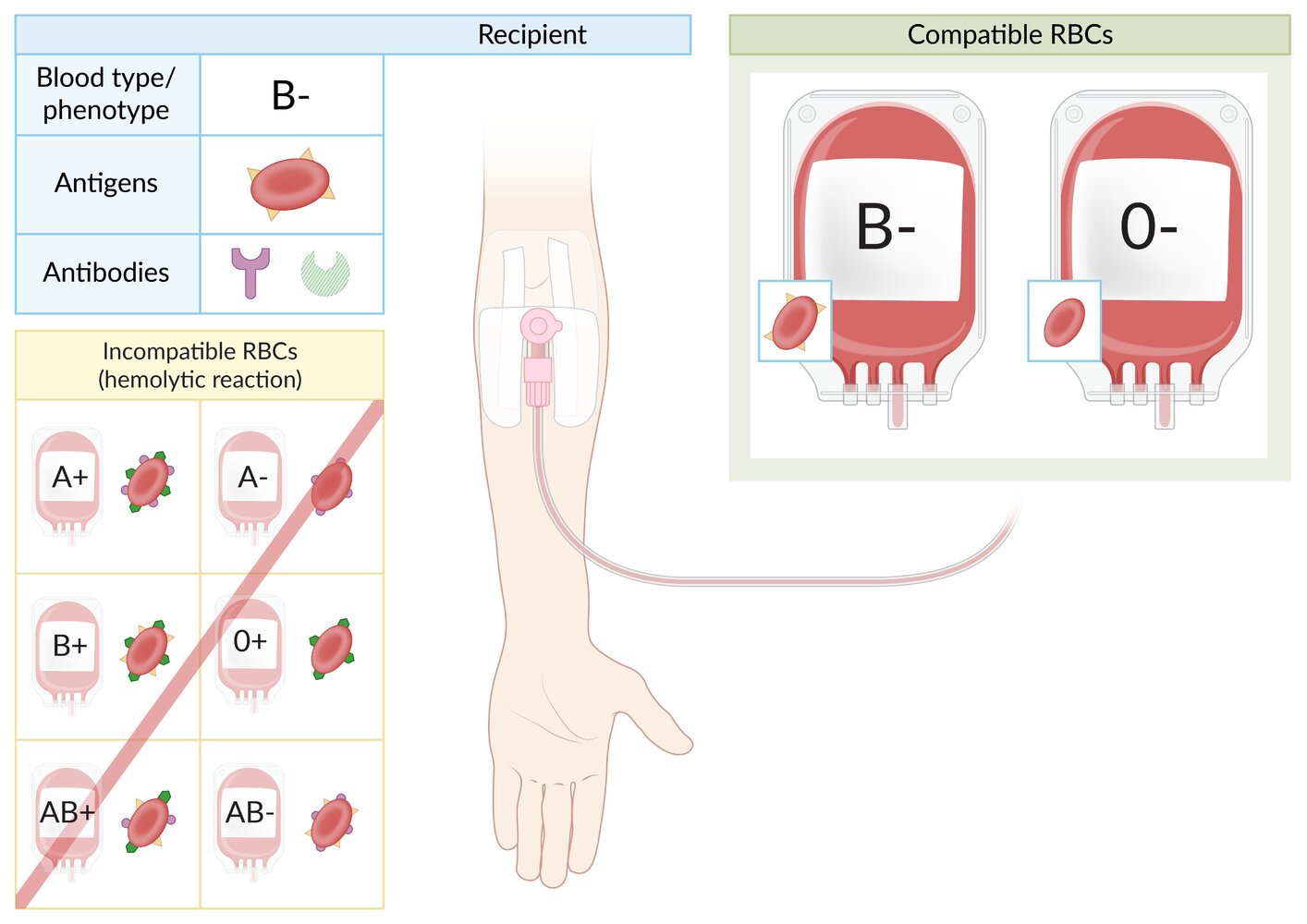
Individuals with blood type B- have B antigens (yellow) on the surface of red blood cells (RBCs) and anti-A antibodies (purple) in the plasma. They may have anti-Rh antibodies (green) if they were previously exposed to Rh+ blood (Rh sensitization).
B- individuals can receive B- or O- packed RBCs. They cannot receive A or AB RBCs, regardless of Rh status, because they contain A antigens, which will trigger a hemolytic reaction. They also should not receive B+ or O+ RBCs because they contain Rh antigens, which may trigger Rh sensitization or hemolysis in previously sensitized individuals.
Note: In case of emergency and no prior Rh sensitization, B- individuals may receive B+ or O+ RBCs.
© AMBOSS
Individuals with blood type B+ have B antigens (yellow) and Rh factor antigens (green) on the surface of red blood cells (RBCs) and anti-A antibodies (purple) in the plasma.
B+ individuals can receive B+/- and O+/- packed RBCs. They cannot receive A or AB RBCs, regardless of Rh status, because they contain A antigens, which will trigger a hemolytic reaction.
© AMBOSS
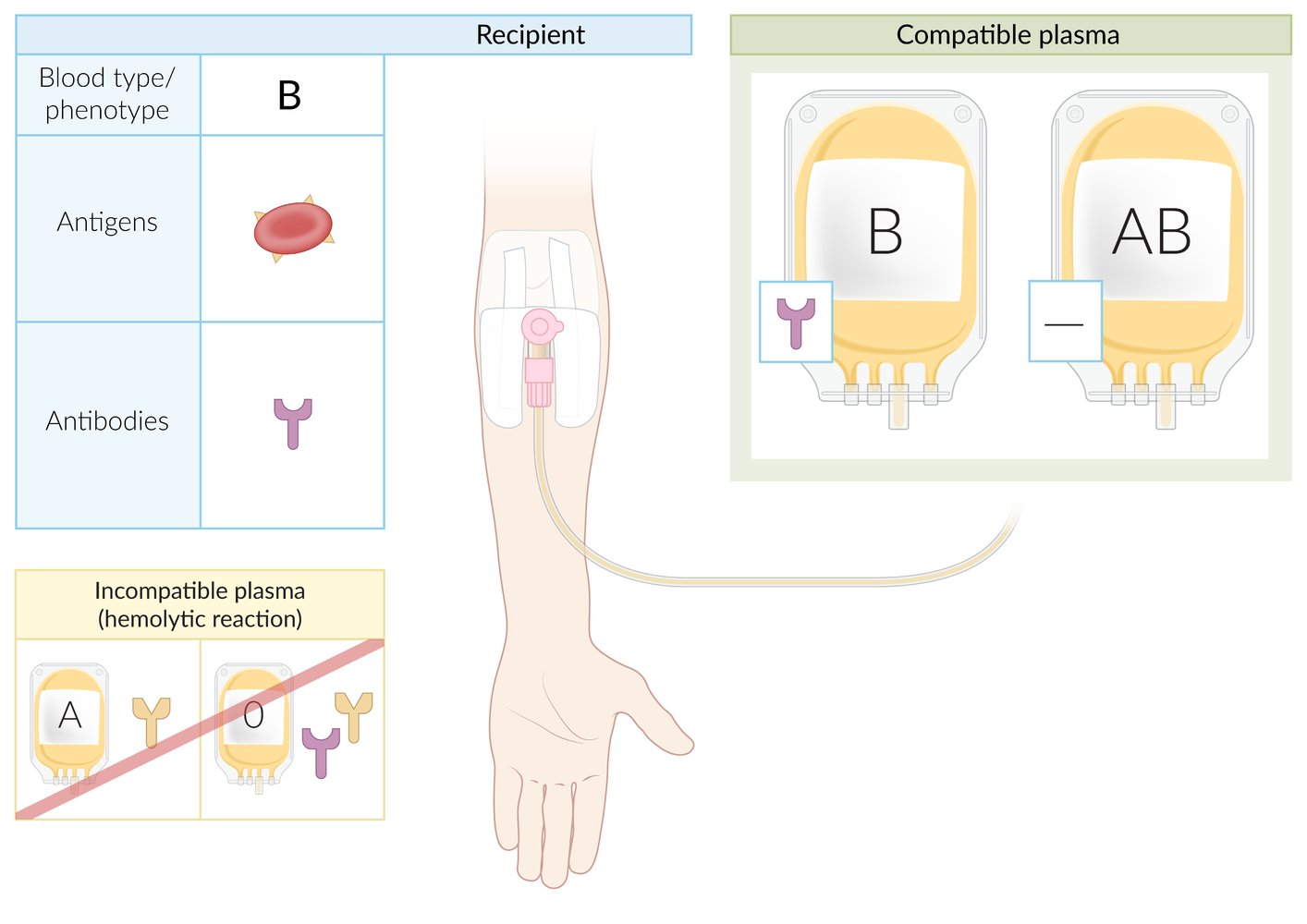
Individuals with blood type B have B antigens on the surface of red blood cells (RBCs) and anti-A antibodies in the plasma. Blood type B individuals can receive plasma from donors with blood types B or AB (blood type AB is a universal plasma donor because it lacks anti-A and anti-B antibodies).
Blood type B is not compatible with plasma donations from blood types A and O because both contain anti-B antibodies, which can trigger a hemolytic reaction in blood type B recipients.
Note: Rh factor compatibility is not relevant to plasma transfusions.
© AMBOSS
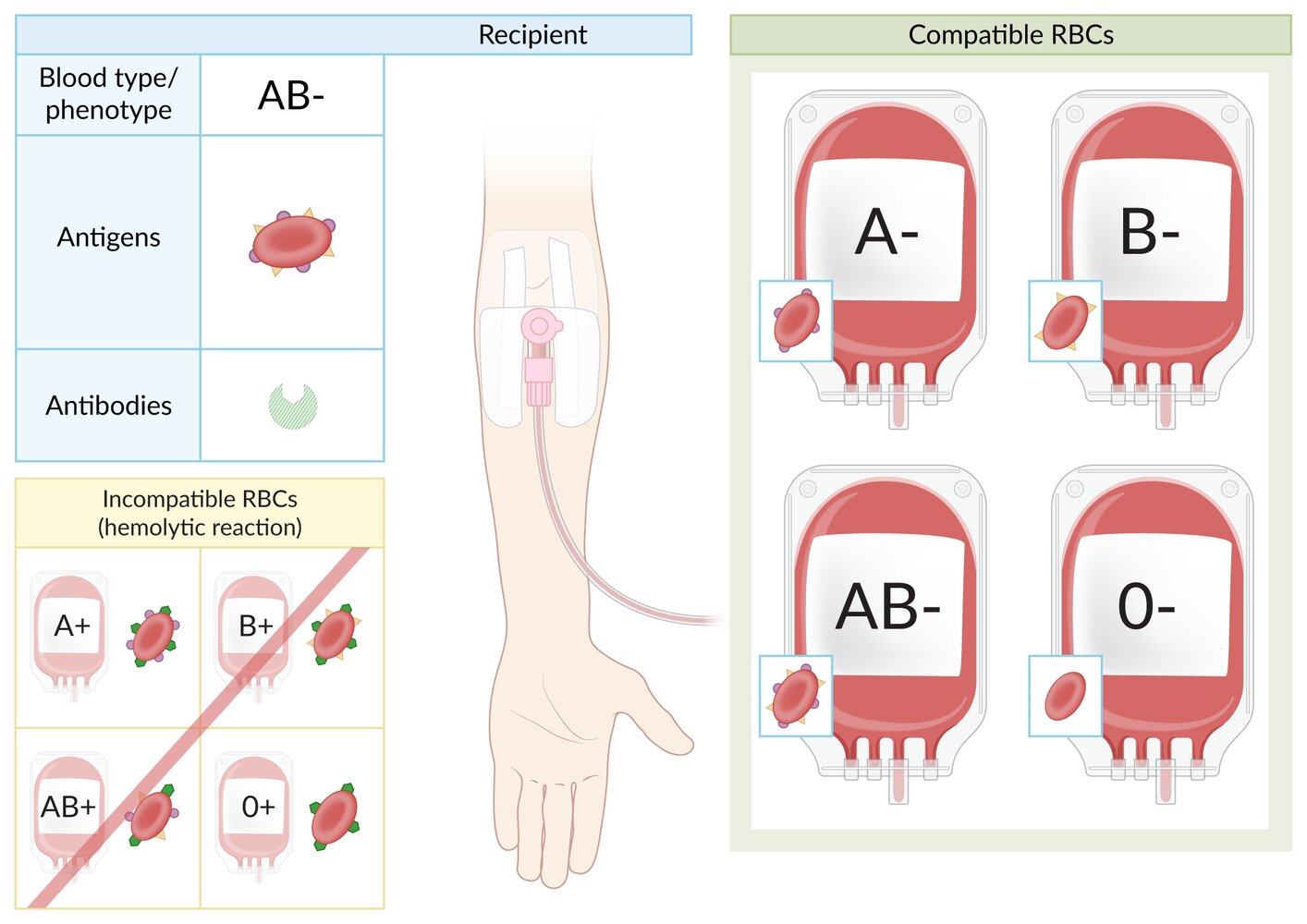
Individuals with blood type AB- have A antigens (purple) and B antigens (yellow) on the surface of red blood cells (RBCs) and no anti-A or anti-B antibodies in the plasma. They may have anti-Rh antibodies (green) if they were previously exposed to Rh+ blood (Rh sensitization).
AB- individuals can receive packed RBCs of any Rh- ABO system type, i.e., A-, B-, AB-, or O-. They should not receive Rh+ RBCs regardless of ABO type, as they contain Rh antigens, which may trigger Rh sensitization or hemolysis in previously sensitized individuals.
Note: In case of emergency and no prior Rh sensitization, AB- individuals may receive RBCs of any Rh+ ABO system type, i.e., A+, B+, AB+, or O+.
© AMBOSS
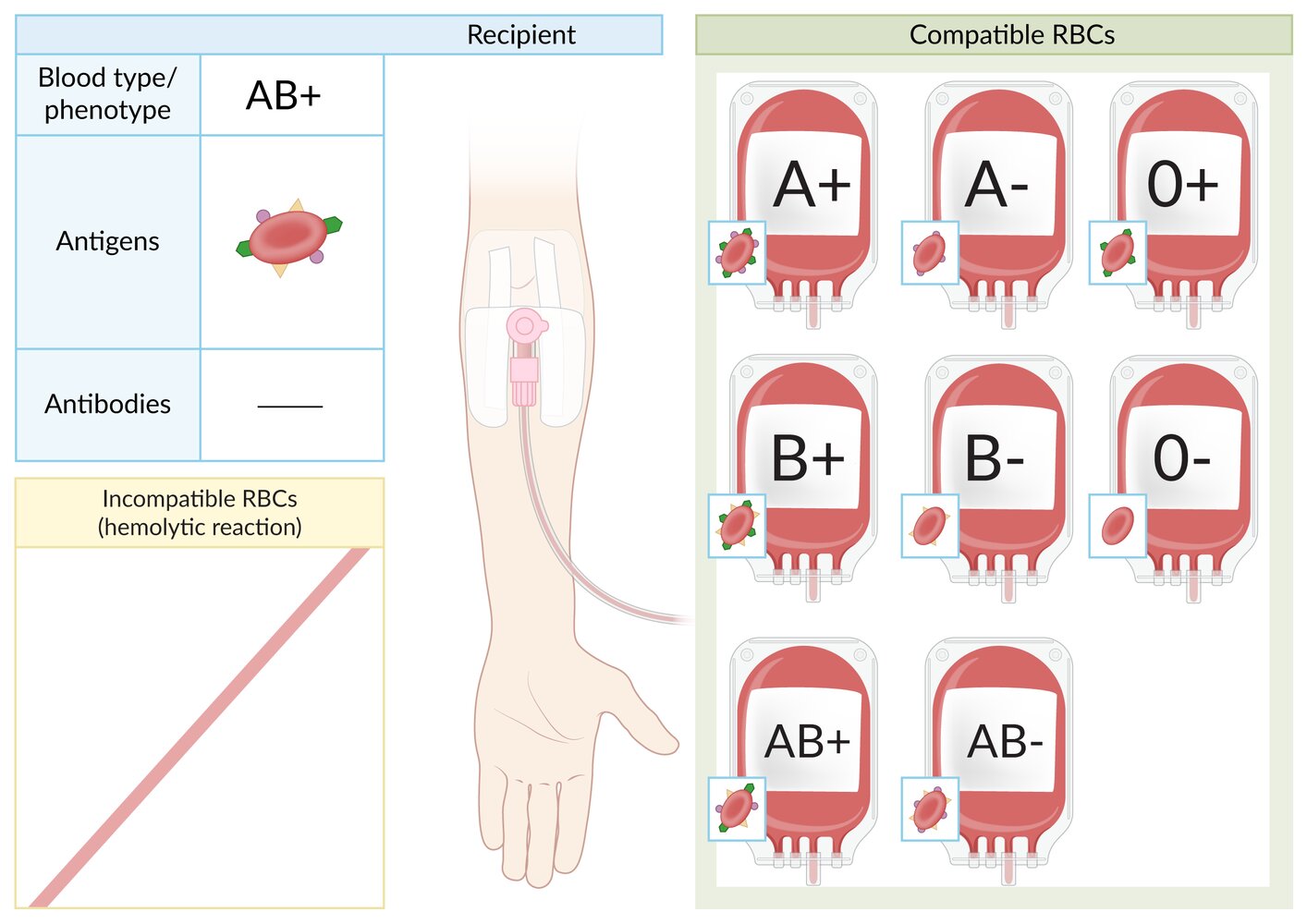
Individuals with blood type AB+ have A antigens (purple), B antigens (yellow), and Rh factor antigens (green) on the surface of red blood cells (RBCs) and no anti-A, anti-B, or anti-Rh antibodies in the plasma.
AB+ individuals can receive packed RBCs of any ABO system type, regardless of Rh status (i.e., AB+ individuals are universal recipients of packed RBCs).
© AMBOSS
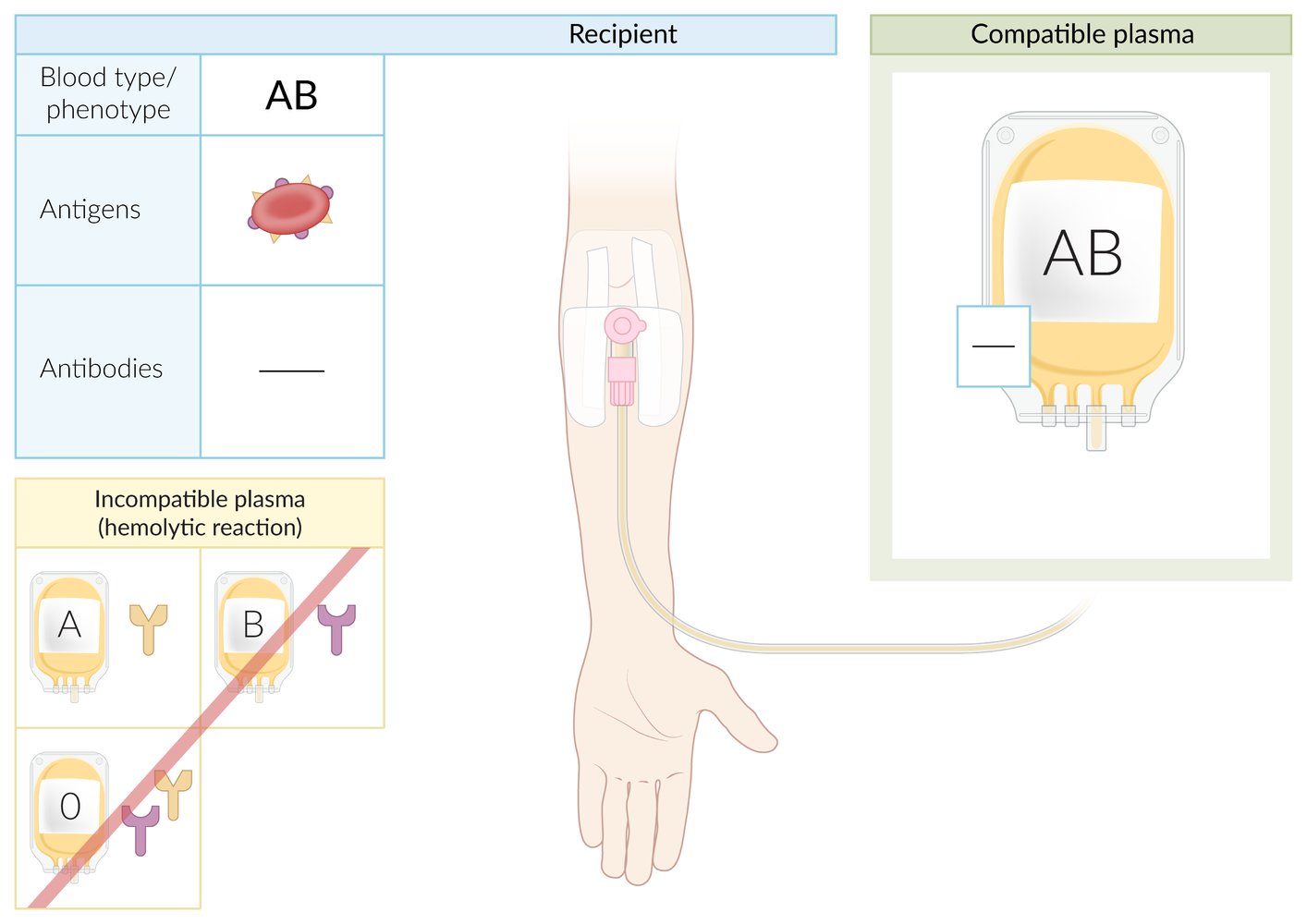
Individuals with blood type AB have both A and B antigens on the surface of red blood cells and no anti-A or anti-B antibodies in the plasma. Therefore, AB individuals can only receive plasma from AB blood type donors.
Blood types A, B, and O are not compatible plasma donors for blood type AB because they contain anti-A and/or anti-B antibodies, which can trigger a hemolytic reaction in blood type AB recipients.
Note: Due to their lack of anti-A and anti-B antibodies, individuals with blood type AB are universal plasma donors. Rh factor compatibility is not relevant to plasma transfusions.
© AMBOSS
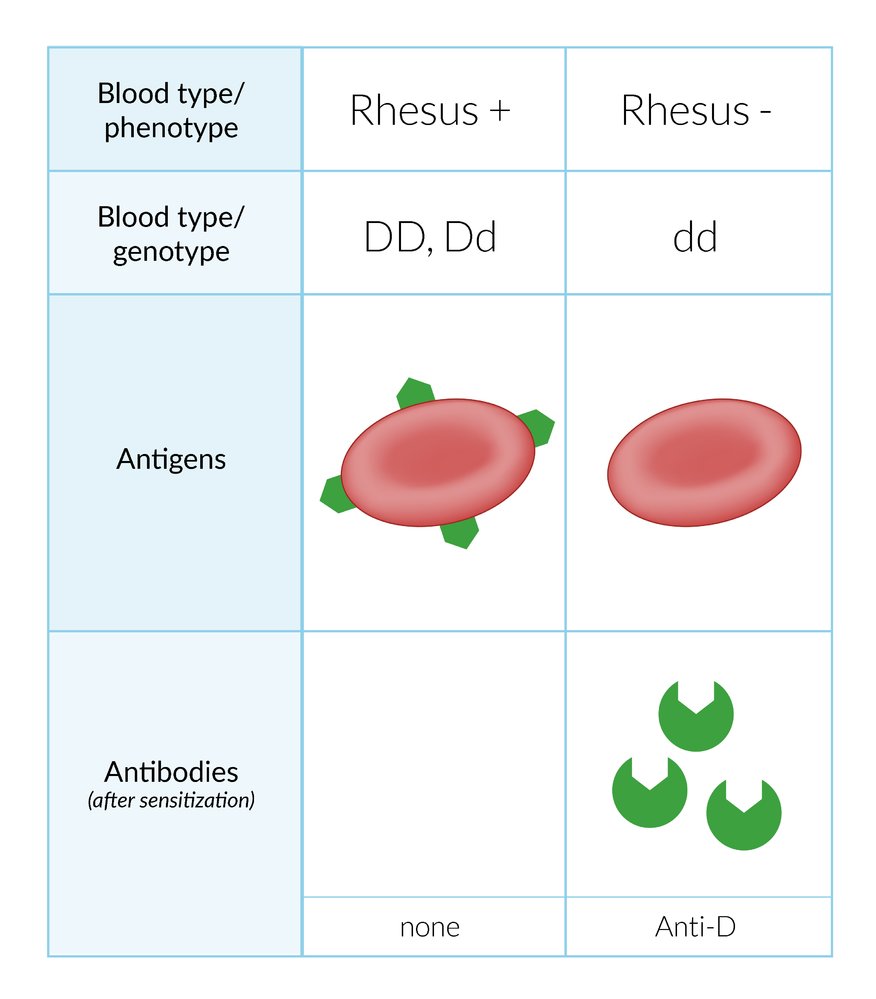
The Rh blood group system classifies blood phenotypes as Rh+ and Rh- based on the presence or absence of the RhD protein on the surface of RBCs, respectively. The expression of the D antigen on the surface of RBCs is determined genetically. Rh+ individuals have D antigen on the surface of their RBCs, and Rh- individuals have anti-D antibodies in their serum. The anti-D antibodies can cause potentially life-threatening agglutination and hemolysis upon contact with RBCs expressing the D antigen.
© AMBOSS
Transfusion safety measures
Blood bank measures
- Blood products for transfusion can be allogeneic (i.e., from a donor) or autologous (i.e., retransfusion of the patient's own blood products)
- Systemic measures are taken by blood banks and blood donation services prior to release for transfusion to reduce risks associated with individual donor units.
- Allogeneic donor blood is tested to determine blood type, screened for common infectious diseases, and then leukoreduced.
- Some blood donations undergo additional processing to further reduce the risk of complications in high-risk groups.
- Blood for autologous transfusion typically undergoes minimal processing intraoperatively prior to retransfusion (e.g., the addition of anticoagulant, filtering for debris and clots, saline washing) [8]
- All prospective blood donors in the United States undergo screening via a donor history questionnaire (DHQ), e.g., to identify infectious risk (see “Blood donation infection screening”) and high-risk medications (e.g., antiplatelet agents) and/or noninfectious conditions (e.g., cancer). [9][10][11]
Infection control
-
Leukoreduction: filtration of leukocytes out of cellular blood products ; [12]
- Reduces the risk of nonhemolytic febrile transfusion reactions; , HLA alloimmunization, and transmission of CMV, HTLV-1/2, and EBV via leukocytes
- Prolongs the lifespan of pRBC in storage
-
Blood donation infection screening
- DHQ screening may exclude donors for a variable or indefinite period if they meet specific criteria, e.g., certain behavioral risk factors for bloodborne infections, history or active features of transmissible illnesses, and/or time spent in endemic areas for specific pathogens, e.g., vCJD, malaria. [13][14][15]
- Laboratory screening: performed on all units received for blood donation
- Routine screening in the United States [16]
- HIV, hepatitis B, hepatitis C, and HTLV
- West Nile virus
- Zika virus
- Syphilis (Treponema pallidum)
- Chagas disease (Trypanosoma cruzi) [17]
- Additional screening in endemic regions
- Babesiosis (Babesia spp.)
- Hepatitis A and hepatitis E
- Malaria
- Routine screening in the United States [16]
Additional processing
Blood products for patients with certain preexisting conditions may require further processing to reduce the risk of complications.
-
Irradiation [18]
- Radiation exposure inactivates lymphocytes to reduce the risk of transfusion-associated graft-versus-host disease (ta-GvHD)
- Indicated in patients at risk of ta-GvHD.
-
Washing [19]
- Replaces plasma in cellular blood products with an alternative solution to reduce the risk of an allergic reaction
- Indicated in patients with a history of IgA deficiency or severe allergic reaction to blood products
-
Volume reduction [20]
- Decreases the amount of plasma and storage solution in cellular blood products to prevent volume overload during transfusion
- Indicated in patients at risk of transfusion-associated circulatory overload (TACO)
Pretransfusion safety practices [17][21]
- Consider transfusion therapy when benefits outweigh the risks and alternatives to blood transfusion have been excluded.
- Choose condition-specific transfusion thresholds and indications tailored to individual patient needs, for example:
- Preexisting conditions (e.g., heart disease, hematological malignancy)
- Specific clinical circumstances (e.g., trauma, critical illness)
- Functional status and desired level of care
- Whenever possible:
- Obtain informed consent.
- Complete pretransfusion testing.
- Follow compatibility requirements for each blood product issued.
- Ensure that the right blood product is being transfused to the right patient at the right time.
- Do not delay life-saving transfusions.
- Only defer life-saving blood transfusions if a clear and valid advance directive prohibits their use or an individual with decision-making capacity declines transfusion after an informed discussion.
Emergency-issued blood products (e.g., uncrossmatched RBCs) can be given under implied consent and without pretransfusion testing in life-threatening situations.
Patients who do not wish to accept blood transfusions (e.g., Jehovah's witnesses) are advised to carry an advance directive card. However, in life-threatening situations, if the patient cannot be consulted and clear advance directives are not available, blood products should be given.
Pretransfusion checklist
Ensure the following whenever possible:
- Check patient records to identify any special transfusion requirements.
- Discuss transfusion risks, benefits, and alternatives to blood transfusion in detail with patients or surrogate decision-makers.
- Document informed consent.
- Order pretransfusion testing as indicated by transfusion product: e.g., type and screen, crossmatching.
- Transfuse blood products within normal working hours for all nonurgent transfusions. [22]
- Use fully crossmatched blood products as soon as they are available.
Requests and prescriptions
Ensure the following are appropriately labeled, documented, and communicated:
- Two independent patient identifiers (e.g., full name and unique medical record number)
- Reasons for transfusion
- Type and number of units of the blood product to be transfused
- Rate or duration of transfusion
- Special requirements (e.g., washed or irradiated products)
- Name and contact details of the requesting clinician
Safety check prior to administration [17]
- Confirm the patient's identity.
- Check if the correct blood products have been issued.
- Ensure blood product containers are undamaged and contents appear normal.
Compare patient and blood product identifiers immediately prior to transfusion. Do not transfuse if there is any discrepancy!
Transfusion administration [17]
See “Fractionated blood components” for component-specific administration instructions.
-
Equipment
- Give blood component transfusions through a standard blood infusion set.
- Use blood-warming devices in patients with cold agglutinins or those requiring multiple transfusions.
-
Rate of administration
- When possible, transfuse at a slower rate for the first 15 minutes.
- Complete all transfusions within 4 hours of removing the blood product from temperature-controlled storage. [23]
-
Cautions
- Do not administer any other medication or solution (except normal saline) through the same tubing.
- Do not routinely use antipyretics, antihistamines, or steroids to prevent transfusion reactions. [24]
Diuretics are often used in clinical practice to help maintain a normal volume status in patients requiring multiple transfusions but have not been shown to reduce the risk of transfusion-associated circulatory overload. [24]
Monitoring [17][22]
- Check clinical status and vital signs for every unit transfused:
- Before initiation
- 15 minutes after starting the transfusion
- Within 60 minutes of completion
- If any symptoms or signs of a possible transfusion reaction (e.g., dyspnea, chills, pruritus) develop
- Monitor for signs of fluid overload, especially in patients requiring multiple transfusions.
- Observe inpatients for 24 hours after transfusion.
Follow the initial management of acute transfusion reactions for any patient who has a change in vital signs or becomes acutely unwell during or in the hours following a transfusion.
Pretransfusion testing
- Goal: Ensure compatibility between recipient and donor blood products and avoid hemolytic transfusion reactions.
- Methods: A variety of test strategies that mostly rely on hemagglutination (i.e., clumping of erythrocytes) induced by antibodies binding to RBC antigens (see “Overview of pretransfusion testing” for more specific methods.)
-
Standard testing requirements: vary by blood product and institutional policy
- RBC: Blood typing, RBC antibody screen, and crossmatching are typically required.
- FFP: Blood typing is typically required.
- Platelet and/or cryoprecipitate: Blood typing may be required.
-
Turnaround times [1][25][26]
- Blood typing alone: up to 25 minutes
- Type and screen: up to 75 minutes
- Type and screen and crossmatch: up to 120 minutes
-
Routine testing: Order advance pretransfusion testing based on anticipated transfusion requirements. [1][25][26]
- High probability during admission: Consider type and screen on arrival.
- High probability within the next few hours (e.g., need for major surgery): Consider immediate type and screen PLUS crossmatch.
-
Extended RBC phenotype matching: matches donor units to the recipient based on their extended RBC antigens profile [22][27]
- Involves detailed serological and genetic profiling of extended RBC antigens to select compatible donor units followed by serologic crossmatching (turnaround time can be several days)
- Performed early in patients with anticipated long-term or recurrent transfusion needs (e.g., due to sickle cell disease, thalassemia) to prevent alloimmunization and transfusion reactions.
Transfuse blood products with complete pretransfusion testing whenever possible. If life-saving transfusion is required before pretransfusion testing is complete, use emergency-issued blood products until fully tested blood products are available.
| Overview of pretransfusion testing [25][26][28] | ||||
|---|---|---|---|---|
| Objectives | Method | Results | ||
| 1. Type and screen [25][28] | Blood typing |
|
|
|
| RBC antibody screen |
|
|
|
|
| 2. Crossmatching [25][28] | Electronic crossmatch |
|
|
|
| Serologic crossmatch |
|
|
|
|

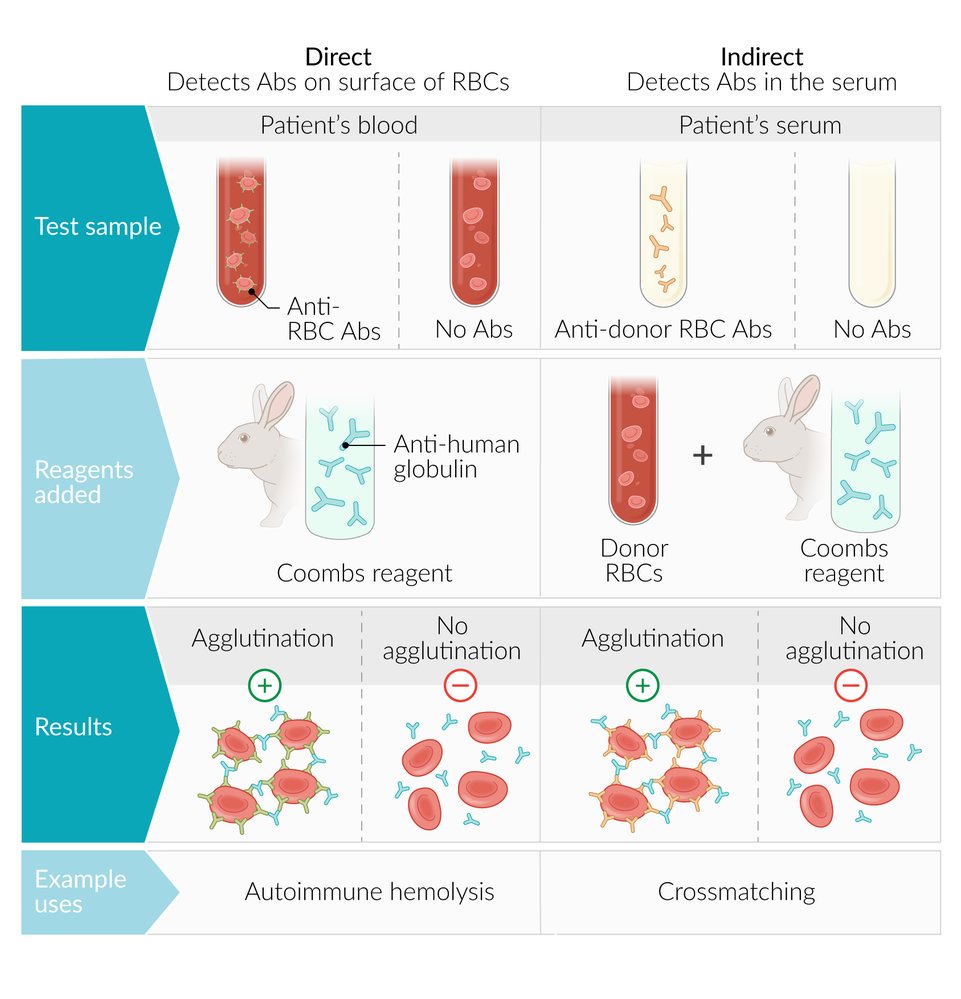
A test used to detect hemolytic antibodies bound to RBCs (direct Coombs test) or freely circulating in the serum (indirect Coombs test).
1. The direct Coombs test is used to detect hemolytic antibodies or complement bound to the surface of a patient's erythrocytes. It is used to differentiate between autoimmune and nonimmune hemolytic anemias and to diagnose hemolytic diseases of the fetus and newborn.
2. The indirect Coombs test is used to detect hemolytic anti-RBC IgG antibodies (against foreign RBC antigens) present in a patient's serum. It is used to screen for maternal anti-D IgG antibodies (detection of hemolytic disease of the newborn) and to crossmatch blood before transfusions.
© AMBOSS
Transfusion products
Recommendations in this article are consistent with the American Association of Blood Banks (AABB) guidelines for transfusing red blood cells (2023), platelets (2025), and plasma (2010). [29][30][31]
Whole blood [32]
- Content: all blood components
- Indications
- Planned surgery (autologous blood)
- Management of traumatic massive hemorrhage, as an alternative to fixed transfusion ratios
Whole blood is rarely used, as most patients require just one blood component, e.g., pRBCs to treat anemia.
Fractionated blood components
Fractionated blood components are prepared by separating whole blood into its constituent elements and storing each under ideal conditions.
- Packed red blood cells
- Platelet transfusion
- Fresh frozen plasma (FFP)
- Cryoprecipitate
- Plasma derivatives
Packed red blood cells
Recommendations in this section are consistent with the 2023 Association for the Advancement of Blood & Biotherapies (AABB) guideline for red cell transfusion. [17][24][30][33]
Content
- RBCs
- A preservative, typically citrate-based [34]
- Unit volume: ∼200–350 mL [22]
Compatibility requirements
See “ABO blood type system” and “Rhesus blood type system.”
- Must be ABO compatible
- Give Rh(D)-negative recipients Rh(D)-negative pRBCs if possible.
- See also “Type and screen” and “Crossmatching.”
Common indications for pRBC transfusion
The decision to transfuse should be made on a case-by-case basis. [24][30]
- Hemorrhagic shock or ongoing rapid blood loss (regardless of initial Hb level)
-
Severe anemia (even if asymptomatic)
- Hb < 7 g/dL for most patients [30]
- Hb ≤ 7.5 g/dL if the patient is due to undergo cardiac surgery [30]
- Hb ≤ 8 g/dL if the patient is due to undergo orthopedic surgery or has preexisiting cardiovascular disease [30]
-
Moderate anemia, in any of the following situations:
- Symptoms of anemia [26]
- Increased risk of complications, e.g., acute onset , significant comorbidities, older age
- Signs of hypoxia
- Planned surgery
- Acute myocardial infarction (AMI): Hb < 10 g/dL [35]
- Conditions requiring exchange transfusion, e.g., methemoglobinemia
Indications for RBC transfusion are not determined solely by Hb value, but rather by an assessment of the clinical circumstances and the patient's overall condition.
Restrictive transfusion thresholds (i.e., Hb 7–8 g/dL) in hemodynamically stable patients are associated with similar clinical outcomes and less blood use and adverse effects compared to liberal thresholds (Hb 9–10 g/dL). [30]
Administration
- Dose [24]
- Give the minimum number of units required to relieve symptoms and/or restore Hb to above transfusion thresholds.
- In the absence of active bleeding, reassess the patient clinically after each unit and check their CBC.
- Usual rate: 90–120 minutes per unit [33]
Effect
- ↑ Hb and oxygen-carrying capacity of the blood
- 1 unit of pRBCs increases Hb value by ∼ 1 g/dL and hematocrit value by ∼ 3%.
- Intravascular volume expansion roughly equivalent to unit volume
Complications
- Repeated transfusions can lead to iron overload.
- See also “Transfusion reactions.”
Platelets
Content [22][36]
- Platelets suspended in plasma or platelet additive solution [36]
- Typically provided as either of the following: [36]
- Single donor apheresis platelets (SDAP) unit: derived from 1 unit of whole blood from a single donor and contains ∼ 310,000/mm3 platelets in ∼ 300 mL
- Random donor pooled platelets (RDP) pack: derived from 4–6 units of whole blood from various donors and contains ∼ 280,000/mm3 platelets in ∼ 200 mL
Compatibility requirements [17][36]
Compatible donor platelets may not be available due to limited supply. The risks of incompatible platelet transfusion are lower than those of incompatible pRBCs. [37]
- ABO compatibility: preferred but not required for routine transfusions [1][37]
- Rh(D) matching: Rh(D)-negative platelets are preferred in Rh(D)-negative recipients to prevent alloimmunization. [22]
- Consider donor plasma compatibility when transfusing multiple units. [38]
Indications for platelet transfusion [24][29][36]
| Category | Indication | Platelet threshold |
|---|---|---|
| Active bleeding | General | Follow local protocols |
| Trauma-induced coagulopathy [39] | < 50,000/mm3 | |
| Nonoperative intracranial hemorrhage | ≤ 100,000/mm3 | |
| Qualitative platelet disorders (e.g., Bernard-Soulier syndrome) | Regardless of platelet count | |
| Massive hemorrhage | No specific threshold (part of balanced resuscitation) | |
| Prophylactic platelet transfusion | Severe hypoproliferative thrombocytopenia in patients actively receiving chemotherapy or undergoing allogeneic stem cell transplant | < 10,000/mm3 |
| Preterm neonates | < 25,000/mm3 | |
| Adults with consumptive thrombocytopenia due to critical illness | < 10,000/mm3 | |
| Before invasive procedures | Central venous catheter placement | < 10,000/mm3 |
| Diagnostic lumbar puncture | < 20,000/mm3 | |
| Neurosurgery [38] | < 100,000/mm3 | |
| Low-risk interventional radiology procedures | < 20,000/mm3 | |
| High-risk interventional radiology procedures (e.g., percutaneous liver biopsy) | < 50,000/mm3 | |
| Major nonneuraxial surgery | < 50,000/mm3 | |
| Childbirth | < 50,000/mm3 |
Cautions [24][29][36]
Prophylactic platelet transfusion is generally not recommended in the following situations:
- Hypoproliferative thrombocytopenia in patients undergoing autologous stem cell transplant or with aplastic anemia
- Dengue-related consumptive thrombocytopenia without major bleeding
- Patients undergoing cardiovascular surgery (including cardiopulmonary bypass) in the absence of major hemorrhage
- Spontaneous or traumatic, nonoperative intracranial hemorrhage if platelet count is > 100,000/mm3 (including those receiving antiplatelet agents)
- HIT
- TTP/HUS
- ITP
- Vaccine-induced immune thrombotic thrombocytopenia (VITT)
Platelet transfusion in patients with HIT or TTP is associated with higher rates of arterial thrombosis and mortality compared to no transfusion. [40]
Administration
- Dose
- Transfuse 1 unit of apheresis platelets or 1 pack of pooled platelets to prevent bleeding due to severe thrombocytopenia (platelets < 10,000/mm3). [41]
- In massive hemorrhage, follow the ratio recommended in the massive transfusion protocol.
- For other indications, use the minimum dose required to restore platelets to the recommended transfusion thresholds. [29]
- Usual rate: 30–60 minutes per apheresis platelets unit/pooled platelets pack [22][33]
Effect
- 1 unit of apheresis platelets or 1 pack of pooled platelets increases the platelet count by 20,000–60,000/mm3. [17]
- Intravascular volume expansion roughly equivalent to unit/pack volume
Complications [24]
- Multiple platelet transfusions may lead to platelet transfusion refractoriness. [36]
- See also “Transfusion reactions.”
Do not use platelet transfusions to treat severe thrombocytopenia due to ITP, TTP, HUS, or HIT unless there is major bleeding.
FFP and cryoprecipitate
Fresh frozen plasma [17][24][31][33]
Recommendations in this section are consistent with the 2010 AABB guideline for plasma transfusion. [31]
-
Content
- Plasma, including all coagulation factors and plasma proteins
- All cellular components are removed from the transfusion product.
- Unit volume: ∼200–300 mL [17][22]
-
Compatibility requirements: See “ABO blood type system.”
- ABO compatibility must be considered. [1]
- Rh(D) matching: not required [22]
-
Indications [17][24]
-
Management of coagulopathy in patients with multiple clotting factor deficiencies (e.g., due to liver cirrhosis, DIC)
- Usually considered for patients with INR ≥ 2.0 who have active bleeding or require invasive procedures.
- Not recommended for correction of mild INR elevations (i.e., INR = 1.1–1.9) [42]
- Prevention of dilutional coagulopathy in massive transfusion
- Plasma exchange transfusion, e.g., in TTP [43]
- Management of some coagulation factor deficiencies if no specific concentrate for treatment exists
- Alternative therapy for:
- Management of plasma protein deficiencies if recombinant products are unavailable
- Immediate reversal of warfarin in patients with life-threatening bleeding or intracranial hemorrhage if 4-factor PCC is unavailable [24]
-
Management of coagulopathy in patients with multiple clotting factor deficiencies (e.g., due to liver cirrhosis, DIC)
-
Administration
- Dose: 10–20 mL/kg [42]
- Usual rate: 10–20 mL/kg/hour [33]
-
Effect
- Correction of both isolated and multiple coagulation factor deficiencies
- Intravascular volume expansion roughly equivalent to unit volume
- Complications: See “Transfusion reactions.”
4-factor PCC is preferred over FFP for the immediate reversal of vitamin K antagonists. [24]
Cryoprecipitate [17][24]
- Content: clotting factors (fibrinogen, factor VIII, factor XIII), vWF, and fibronectin
-
Compatibility requirements
- ABO compatibility: preferred but not required [17]
- Rh(D) matching: not required [22]
-
Indications
- Bleeding associated with fibrinogen deficiency (e.g., due to DIC, liver disease): typically performed if serum fibrinogen is < 100–150 mg/dL [24]
- Alternative therapy for deficiencies in clotting factors; , including vWF, factor VIII, and factor XIII
- Treatment of uremic bleeding syndrome
-
Administration
- Dose: typically 1 unit per 7–10 kg of the patient's body weight [17]
- Usual rate: 10–20 mL/kg/hour [33]
- Effect: 1 unit of cryoprecipitate per 7–10 kg of the patient's body weight increases serum fibrinogen by ∼ 50–75 mg/dL . [17]
-
Complications
- Rarely, transfusion of large volumes of ABO-incompatible cryoprecipitate may lead to a mild hemolytic transfusion reaction.
- See also “Transfusion reactions.”
Cryoprecipitate is primarily used to treat bleeding associated with fibrinogen deficiency.
Only consider cryoprecipitate in the management of vWD, hemophilia A, or factor XIII deficiency if single-factor concentrates and recombinant synthetic factors are unavailable. [17]
Plasma derivatives
Clotting factors
Prothrombin complex concentrate (PCC) [44]
-
Composition
- Vitamin K-dependent clotting factors: factors II, VII, IX, and X [44]
- Anticoagulants: protein C, protein S, antithrombin, and/or heparin
-
Indications
- Vitamin K antagonist-associated major bleeding: 4-factor PCC is given with IV vitamin K (see “Warfarin reversal” for further information). [45]
- Treatment and prevention of bleeding in patients with rare clotting factor deficiencies if specific factor preparations are not available [46][47]
- Consider for the reversal of DOACs in life-threatening bleeding. [48][49]
-
Adverse effects
- Thrombotic complications (e.g., VTE, myocardial infarction)
- HIT
- Hypersensitivity reactions (e.g., anaphylaxis)
Do not use PCC or FFP to reverse vitamin K antagonists unless there is an emergency indication (e.g., life-threatening bleeding, emergency surgery). [24]
Single-factor concentrates [22]
- Composition: specific clotting factors that have been pooled from multiple donors
- Indications: specific clotting factor deficiencies (e.g., factor VIII and factor IX are used for the treatment of hemophilia A and hemophilia B) if recombinant factors are not available
When possible, use recombinant synthetic factors over blood-derived clotting factors, as they are not associated with any risk of infection transmission. [22]
Antithrombin III
- Composition: : human antithrombin III; , which is synthesized in the liver and inhibits coagulation factors IXa, Xa, XIa, and XIIa, and thrombin
-
Indications
- Patients with hereditary antithrombin III deficiency to optimize thrombosis prophylaxis with heparin
- Patients on cardiopulmonary bypass who are experiencing heparin resistance [50]
- DIC, in select cases [51]
- Effect: increases the effects of heparin
Albumin
- Composition: human albumin, which is produced exclusively in the liver
- Indications: after paracentesis or in the setting of therapeutic plasmapheresis
-
Effect
- Maintains colloid osmotic pressure
- Increases intravascular volume
- Functions as transport protein for various substances (e.g., drugs, hormones, enzymes)
Emergency transfusion
General principles [1]
- Emergency-release blood components can be issued from the blood bank in < 5 minutes but are associated with an increased risk of hemolytic transfusion reactions. [1][52]
- Unknown recipient blood type: Give universal donor blood products (blood products that could potentially be safely transfused to any recipient regardless of their ABO blood type, including blood type O negative packed RBCs, blood type AB plasma, and blood type AB platelets)
- Known recipient ABO type and Rhesus status: Give type-specific blood products.
Pretransfusion testing takes up to 120 minutes; emergency transfusion can occur prior to pretransfusion testing using uncrossmatched products. [1]
Blood product selection [1][26][36]
-
Unknown recipient blood type
- pRBCs: Uncrossmatched blood type O; (universal RBC donor) pRBCs (Rhesus D negative if possible)
- FFP: Blood type AB (universal plasma donor) FFP
- Platelets: Ideally use blood type AB platelets (preferably Rh(D)-negative) but platelets of any blood type may be used.
-
Known recipient blood type
- pRBCs: Uncrossmatched ABO and RhD-compatible pRBCs
- FFP: ABO-compatible FFP
-
Platelets
- ABO-compatible platelets are preferred but platelets of any blood type may be used.
- Rh(D)-negative platelets are preferred for Rh(D)-negative recipients. [22][36]
Massive transfusion
Definition
- The replacement of a large volume of blood in response to massive hemorrhage
- There is no universal threshold for a massive transfusion; proposed values include: [53][54]
- Complete replacement of a patient's blood volume (∼ 10 units of RBCs) within 24 hours
- Replacement of ≥ 50% of a patient's blood volume (∼ 5 units of RBCs) within 3 hours
- Blood loss replacement at a rate of > 150 mL/minute
- Transfusion of ≥ 3 units of pRBCs within 1 hour
Risks [55]
Giving patients large volumes of blood products, especially if unbalanced or given rapidly, risks the following massive transfusion-associated complications:
- Acidosis
- Hypothermia
- Coagulopathy [56]
- Electrolyte imbalances
- Citrate toxicity
- Transfusion-related lung injury
- Transfusion-associated circulatory overload
Judicious use of blood products to avoid overtransfusion is the best way to prevent massive transfusion-associated complications!
Massive transfusion protocols (MTP) [57]
- Goal: mitigate the risks of massive transfusion [58][59]
- Clinical application: activated for patients with large volume transfusion requirements, e.g., due to trauma, major surgery, obstetric complications, GI bleeding
-
Protocol components
- Multidisciplinary instructions to expedite transfusion
- A series of laboratory studies to perform on the patient's blood
- A set ratio of blood products to be given
- May include antifibrinolytics, e.g., tranexamic acid, in patients with ongoing bleeding
- Initial approaches: Consider a fixed ratio approach or whole blood approach for patients with ongoing hemorrhage prior to laboratory results.
- Subsequent approach: Consider targeted transfusion regimen once laboratory results become available and/or hemostatic control is achieved.
The optimal approach to blood component transfusion for massive hemorrhage remains unknown. Follow local hospital protocol under specialist guidance.
Fixed ratio approach [22][58]
- Transfusion of RBCs, FFP, and platelets at predefined ratios
- Intended for prophylaxis and empiric treatment of coagulopathy
-
Ratios vary by local protocols. Examples include:
- RBC, FFP, and platelet units in a 1:1:1 ratio
- RBC, FFP, and platelet units in a 6:4:1 ratio
Whole blood approach [32]
- Initial transfusion of whole blood (limited availability).
- Used as an alternative to the fixed ratio approach in the treatment of massive traumatic hemorrhage
- Type O blood with low anti-A and anti-B antibody titers is used in emergency transfusions to minimize the risk of hemolytic transfusion reactions.
Targeted transfusion regimen [58][60]
- Requires frequent laboratory monitoring (e.g., every 1–2 hours)
- Thresholds and dosing vary by local protocols
- Consult transfusion services if available.
| Suggested thresholds for targeted transfusion in massive hemorrhage [22] | ||
|---|---|---|
| Blood components | Indications | Dosage |
| RBCs |
|
|
| FFP |
|
|
| Platelets |
|
|
| Cryoprecipitate |
|
|
Massive transfusion protocol checklist [58]
- Activate the MTP, following local hospital guidance.
- Start monitoring, including continuous telemetry.
- Place 2 large-bore peripheral IV catheters.
- Obtain routine baseline massive transfusion studies, including CBC, PT, aPTT, serum fibrinogen, ionized calcium, BMP, and blood gases.
- Consider using point-of-care thromboelastography if available.
- Start transfusing blood through blood-warming equipment.
- Regularly reassess the patient to assess for signs of fluid overload and/or respiratory distress.
- Repeat massive transfusion studies, including arterial blood gases, at regular intervals.
Related One-Minute Telegram
- One-Minute Telegram 131-2025-1/3: To transfuse or not to transfuse? A new guideline for AMI
- One-Minute Telegram 125-2025-2/3: We’re clot kidding! New AABB/ICTMG guidelines favor restricting platelet transfusions
- One-Minute Telegram 88-2023-3/3: A heart-racking dilemma: transfusions in myocardial infarction and anemia
Interested in the newest medical research, distilled down to just one minute? Sign up for the One-Minute Telegram in “Tips and links” below.
External Resources
- 2025 AABB and ICTMG International Clinical Practice Guidelines on Platelet Transfusion
- 2023 AABB International Guidelines on Red Blood Cell Transfusion
- 2010 AABB Evidence-based Practice Guidelines for Plasma Transfusion
- 2018 British Society for Haematology Guideline for the administration of blood components
- 2023 AABB Donor History Questionnaire and Related Materials Toolkit (Version 4.0)
- Sign up for the One-Minute Telegram
References
- Yazer MH. "The blood bank "black box" debunked: pretransfusion testing explained.". CMAJ : Canadian Medical Association journal = journal de l'Association medicale canadienne. 174(1). :29-32. (2006)
- "Blood Groups and Red Cell Antigens". https://www.ncbi.nlm.nih.gov/books/NBK2261/. [2005-01-01]
- O’Shaughnessy DF, Atterbury C, et al. "Guidelines for the use of fresh-frozen plasma, cryoprecipitate and cryosupernatant". Br J Haematol. 126(1). :11-28. (2004)
- "Blood Grouping"
- de Carvalho GB, de Carvalho GB. "Duffy Blood Group System and the malaria adaptation process in humans.". Revista brasileira de hematologia e hemoterapia. 33(1). :55-64. (2011)
- Hamilton JR. "Kidd blood group system: outwardly simple with hidden complexity". ISBT Science Series. 14(1). :3-8. (2018)
- Wheeler M, Frazar C, Lannert K, et al. "Prediction of MNS Blood Group Antigens Using Next Generation Sequencing". Blood. 128(22). :1458-1458. (2016)
- Metcalf RA, Nahirniak S, Guyatt G, et al. "Platelet Transfusion". JAMA. (2025)
- Carson JL, Stanworth SJ, Guyatt G, et al. "Red Blood Cell Transfusion". JAMA. 330(19). :1892. (2023)
- Roback JD, Caldwell S, Carson J, et al. "Evidence-based practice guidelines for plasma transfusion.". Transfusion (Paris). 50(6). :1227-39. (2010)
- Cap AP, Beckett A, Benov A, et al. "Whole Blood Transfusion". Mil Med. 183(suppl_2). :44-51. (2018)
- Goel R, Tobian AAR, Shaz BH. "Noninfectious transfusion-associated adverse events and their mitigation strategies". Blood. 133(17). :1831-1839. (2019)
- "Red Blood Cell Transfusion: a pocket guide for the clinician"
- Solves Alcaina P. "Platelet Transfusion: And Update on Challenges and Outcomes". Journal of Blood Medicine. Volume 11. :19-26. (2020)
- Norfolk D. "Handbook of transfusion medicine, 5th edition". United Kingdom Blood Services. (2013). ISBN: 9780117068469
- Boisen ML, Collins RA, Yazer MH, Waters JH. "Pretransfusion testing and transfusion of uncrossmatched erythrocytes.". Anesthesiology. 122(1). :191-5. (2015)
- Chou ST, Alsawas M, Fasano RM, et al. "American Society of Hematology 2020 guidelines for sickle cell disease: transfusion support". Blood Adv. 4(2). :327-355. (2020)
- White J. "Pre-transfusion testing". ISBT Sci Ser. 4(1). :37-44. (2009)
- Vanderlinde ES. "Autologous transfusion". BMJ. 324(7340). :772-775. (2002)
- "Full-Length Donor History Questionnaire (DHQ) v2.1"
- "Implementation of acceptable full length and abbreviated donor history questionnaires and accompanying materials for use in screening donors of blood and blood components". https://www.fda.gov/media/124193/download. [2020-05-01]
- "Medication Deferral List v2.1"
- Pertinhez TA, Casali E, Baroni F, et al. "A Comparative Study of the Effect of Leukoreduction and Pre-storage Leukodepletion on Red Blood Cells during Storage". Front Mol Biosci. 3. (2016)
- Wilson K, Atkinson K, Keelan J. "Three decades of MSM donor deferral policies. What have we learned?". International Journal of Infectious Diseases. 18. :1-3. (2014)
- "Blood Donor Educational Material v2.1"
- "DHQ Flowcharts with PrEP, PEP, ART v2.1"
- "Infectious Disease, HLA and ABO Donor Qualification Testing". https://www.redcrossblood.org/biomedical-services/blood-diagnostic-testing/blood-testing.html
- "Circular of information for the use of human blood and blood components"
- Tormey CA, Hendrickson JE. "Irradiation of Red Blood Cells and Alloimmunization". Lab Med. 48(2). :172-177. (2017)
- Cardigan R, New HV, Tinegate H, Thomas S. "Washed red cells: theory and practice". Vox Sang. 115(8). :606-616. (2020)
- Bosboom JJ, Klanderman RB, Migdady Y, et al. "Transfusion-Associated Circulatory Overload: A Clinical Perspective". Transfus Med Rev. 33(2). :69-77. (2019)
- Murphy MF, Stanworth SJ, Yazer M. "Transfusion practice and safety: current status and possibilities for improvement". Vox Sang. 100(1). :46-59. (2010)
- Ramirez-Arcos S, Mastronardi C, Perkins H, et al. "Evaluating the 4-hour and 30-minute rules: effects of room temperature exposure on red blood cell quality and bacterial growth". Transfusion. 53(4). :851-859. (2012)
- Raval JS, Griggs JR, Fleg A. "Blood Product Transfusion in Adults: Indications, Adverse Reactions, and Modifications". Am Fam Physician. 102(1). :30-38. (2020)
- Kaur P, Basu S, Kaur G, Kaur R. "Transfusion protocol in trauma". J Emerg Trauma Shock. 4(1). :103. (2011)
- Savage SA, Sumislawski JJ, Zarzaur BL, et al. "The new metric to define large-volume hemorrhage". Journal of Trauma and Acute Care Surgery. 78(2). :224-230. (2015)
- Sihler KC, Napolitano LM. "Complications of Massive Transfusion". Chest. 137(1). :209-220. (2010)
- Thomas D, Wee M, Clyburn P, et al. "Blood transfusion and the anaesthetist: management of massive haemorrhage". Anaesthesia. 65(11). :1153-1161. (2010)
- DeSimone RA, Goss CA, Hsu Y-MS, Haas T, Cushing MM. "Massive Transfusion Protocols: Indications, Ratios and Mortality in the Non-Trauma Setting". Blood. 126(23). :2348-2348. (2015)
- "American College of Surgeons, Trauma Quality Improvement Program, Massive transfusion in trauma guidelines". https://www.facs.org/Quality-Programs/Trauma/TQP/center-programs/TQIP/Best-Practice. [2014-10-01]
- Sommer N, Schnüriger B, Candinas D, Haltmeier T. "Massive transfusion protocols in nontrauma patients". Journal of Trauma and Acute Care Surgery. 86(3). :493-504. (2019)
- Waters JH. "Role of the massive transfusion protocol in the management of haemorrhagic shock". Br J Anaesth. 113. :ii3-ii8. (2014)
- Zielinski MD, Wilson GA, Johnson PM, et al. "Ideal hemoglobin transfusion target for resuscitation of massive-transfusion patients". Surgery. 160(6). :1560-1567. (2016)
- Robinson S, Harris A, Atkinson S, et al. "The administration of blood components: a British Society for Haematology Guideline". Transfus Med. 28(1). :3-21. (2018)
- García-Roa M, Vicente-Ayuso M del C, Bobes AM, et al. "Red blood cell storage time and transfusion: current practice, concerns and future perspectives". Blood Transfus. (2017)
- Pagano MB, Stanworth SJ, Dennis J, et al. "Red Cell Transfusion in Acute Myocardial Infarction: AABB International Clinical Practice Guidelines". Ann Intern Med. (2025)
- Dunbar NM. "Does ABO and RhD matching matter for platelet transfusion?". Hematology. 2020(1). :512-517. (2020)
- Estcourt LJ, Birchall J, Allard S, et al. "Guidelines for the use of platelet transfusions". Br J Haematol. 176(3). :365-394. (2016)
- Stanworth SJ, Shah A. "How I use platelet transfusions". Blood. 140(18). :1925-1936. (2022)
- Goel R, Ness PM, Takemoto CM, et al. "Platelet transfusions in platelet consumptive disorders are associated with arterial thrombosis and in-hospital mortality". Blood. 125(9). :1470-1476. (2015)
- Kaufman RM, Djulbegovic B, Gernsheimer T. "Platelet Transfusion: A Clinical Practice Guideline From the AABB". Ann Intern Med. 162(3). :205-213. (2015)
- Szczepiorkowski ZM, Dunbar NM. "Transfusion guidelines: when to transfuse". Hematology Am Soc Hematol Educ Program. 2013(1). :638-644. (2013)
- Pereira A. "Efficacy of different plasma sources in the treatment of thrombotic thrombocytopenic purpura". ISBT Science Series. 4(1). :111-117. (2009)
- Rodgers GM. "Prothrombin complex concentrates in emergency bleeding disorders". Am J Hematol. 87(9). :898-902. (2012)
- Holbrook A, Schulman S, Witt DM, et al. "Evidence-Based Management of Anticoagulant Therapy". Chest. 141(2). :e152S-e184S. (2012)
- Dean M, Sung V. "Review of deutetrabenazine: a novel treatment for chorea associated with Huntington's disease". Drug Design, Development and Therapy. Volume 12. :313-319. (2018)
- Franchini M, Lippi G. "Prothrombin complex concentrates: an update". Blood Transfusion. (2010)
- Piran S, Khatib R, Schulman S, et al. "Management of direct factor Xa inhibitor–related major bleeding with prothrombin complex concentrate: a meta-analysis". Blood Advances. 3(2). :158-167. (2019)
- Hoffman M, Dickneite G. "Reversing the new oral anticoagulants with prothrombin complex concentrates (PCCs): what is the evidence?". Thromb Haemost. 111(02). :189-198. (2014)
- Spiess BD. "Treating Heparin Resistance With Antithrombin or Fresh Frozen Plasma". Ann Thorac Surg. 85(6). :2153-2160. (2008)
- Kim Y-J, Ko BS, Park SY, et al. "Effect of High-dose Antithrombin Supplementation in Patients with Septic Shock and Disseminated Intravascular Coagulation". Sci Rep. 9(1). (2019)
- Le T, Bhushan V. "First Aid for the USMLE Step 1 2015". McGraw-Hill Education. (2014). ISBN: 9780071840071
- "Blood Types". https://bloodcenter.stanford.edu/education/blood_types.php?education/blood_types.html. [2017-02-19]
- "Blood typing". https://medlineplus.gov/ency/article/003345.htm. [2016-11-02]
- Carson JL, Guyatt G, Heddle NM, et al. "Clinical Practice Guidelines From the AABB: Red Blood Cell Transfusion Thresholds and Storage". JAMA. 316(19). :2025. (2016)
- Bux J, Sachs UJ. "The pathogenesis of transfusion-related acute lung injury (TRALI).". Br J Haematol. 136(6). :788-99. (2007)
- Toy P, Lowell C. "TRALI – Definition, mechanisms, incidence and clinical relevance". Best Practice & Research Clinical Anaesthesiology. 21(2). :183-193. (2007)
- Rafei H, Yunus R, Nassereddine S. "Post-Transfusion Purpura: A Case Report of an Underdiagnosed Phenomenon". Cureus. (2017)
- Harewood J, Ramsey A, Master SR. "Hemolytic Transfusion Reaction". StatPearls. (2020)