Quick guide
Diagnostic approach
- ABCDE survey (primary survey in TBI)
- Continuous monitoring of vitals, SpO2, and capnography
- Serial neurological exams and assessment for signs of ↑ ICP
- Measure GCS and pupillary response.
- Noncontrast head CT (e.g., if GCS ≤ 12 or criteria for neuroimaging in mTBI)
- POC glucose
- Blood alcohol level
- Utox
- BMP
- ABG analysis
- Coagulation panel for suspected coagulopathy
- Imaging of other potential sites of injury (e.g., CT C-spine)
- eFAST if hypotensive
")
GCS ≤ 12 indicates a need for emergency neuroimaging with noncontrast head CT after stabilization regardless of other potential causes for mental obtundation (e.g., alcohol intoxication).
Red flag features
- GCS ≤ 12
- Focal neurologic deficits (e.g., unequal pupils)
- Deteriorating neurological status
- Decorticate posturing or decerebrate posturing
- Altered mood and behavior (e.g., aggressive behavior)
- Dizziness, nausea, vomiting
- Cushing triad
- Cerebral herniation
- SBP < 90 mm Hg
- CSF rhinorrhea or otorrhea
- Battle sign or raccoon eyes
- Hemotympanum
- Seizures
Management checklist
- C-spine immobilization as needed
- Maintain SpO2 > 92–94% and PaO2 > 60 mm Hg.
- Maintain PaCO2 35–45 mm Hg.
- Maintain SBP 90–180 mm Hg.
- 2L isotonic saline bolus for hypotension
- Maintain blood glucose 80–180 mg/dL.
- Consider intubation if GCS ≤ 8.
- Consider tranexamic acid (off-label) if GCS 9–12 and < 3 hours since injury.
- Consult neurosurgery urgently if GCS ≤ 12.
- Reverse anticoagulation if indicated.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
Summary
Traumatic brain injury (TBI) is defined as a structural injury to the brain or a disruption in the normal functioning of the brain as a result of a blunt or penetrating head injury. Head injury refers to trauma to the head that may or may not be associated with TBI, soft tissue injury, or skull fractures. Primary brain injury occurs as an immediate consequence of head injury at the time of the trauma. Secondary brain injury is indirect and results from physiological changes triggered by the initial impact and/or acute management measures; it is preventable to a certain degree. TBI is most frequently seen in young children, teenagers, and individuals older than 65 years, with falls and motor vehicle accidents being the leading causes. The Glasgow coma scale (GCS) is a commonly used scoring system used to assess the severity of TBI and guide management. Clinical features of TBI depend on the severity, type, and location of brain injury. Impaired consciousness is common in severe TBI, whereas patients with mild TBI may only present with transient confusion and headache. Neuroprotective measures to prevent or minimize secondary brain injury should be the main focus of initial management of all patients with TBI. Patients with moderate TBI or severe TBI should be transferred to a neurocritical care unit at the earliest. After initial resuscitation, a head CT without contrast should be obtained to identify the type and extent of injury. Definitive management varies depending on the type and severity of injury.
The specific management of mild TBI (concussion), elevated intracranial pressure and brain herniation, EDH, SDH, SAH, and ICH is discussed in separate articles.
Definitions
- Traumatic brain injury (TBI): structural or physiological disruption of the brain resulting from a head injury [1][2]
-
Head injury: trauma to the head that may or may not be associated with soft tissue injury, skull fractures, and TBI [3]
- Closed head injury (most common): head injury with intact dura mater
- Open head injury: head injury with a breach in the dura mater exposing the cranial contents to the environment; associated with skull fractures
Epidemiology
- Incidence: ∼ 800/100,000
- Age: especially children 0–4 years, teenagers and young adults 15–24 years, and adults > 65 years
- Sex: ♂ > ♀
References: [4][5][6]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
-
Blunt head injury (common): injury caused by blunt force trauma to the head
- Falls: leading cause of TBI; more common in children, adolescents, and the elderly [7]
- Motor vehicle accidents: second most common cause of TBI [7]
- Contact sports (e.g., football)
-
Penetrating head injury (less common): injury caused by penetrative trauma to the head [8]
- High-velocity missile injury: gunshot wounds
- Low-velocity nonmissile injury: assault or accidental injury with a penetrating foreign body to the head or face (e.g., knife, screwdriver, nail gun) [9][10]
- Blast injuries: injury caused by the high pressure wave (blast wave) generated from an explosion; common in active military or war zones [11]
Pathophysiology
TBI is categorized pathophysiologically into primary and secondary brain injury depending on whether the brain injury is a direct or indirect result of the inciting trauma.
Primary brain injury [12][13]
- Definition: brain injury that occurs at the time of the trauma as an immediate consequence of head injury
-
Focal primary brain injury
-
Intracranial hemorrhage
- Epidural hemorrhage (EDH)
- Subdural hemorrhage (SDH)
- Subarachnoid hemorrhage (SAH)
- Intracerebral hemorrhage (ICH)
- Cerebral contusion: focal area of heterogeneous brain injury, varying from a bruise to a focal area of necrosis [14]
-
Coup-contrecoup injury
- Coup injury: injury on the side of an impact
- Contrecoup injury: additional injury (typically a contusion) on the opposite side of impact
- Brain parenchymal lacerations
- Intracerebral or intracerebellar hematomas
-
Intracranial hemorrhage
-
Diffuse primary brain injury
- Mild traumatic brain injury (concussion)
- Cerebral edema
-
Diffuse axonal injury (DAI)
- Multifocal shearing tears and disruption of the axons of the brain due to rotational acceleration-deceleration trauma of the head; typically seen in high-impact road traffic accidents. [15][16]
- Commonly results in severe neurological injury (e.g., coma, persistent vegetative state)



Secondary brain injury [12][13]
- Definition: indirect brain injury resulting from physiological changes following acute CNS insults and/or their treatment
- Examples: disrupted blood-brain barrier, hypoxic-ischemic encephalopathy (see “Pathophysiology” in “Secondary brain injury” for details)
Secondary brain injury is preventable. Neuroprotective measures to prevent or minimize secondary brain injury should be initiated as early as possible in all patients with acute neurological insults.
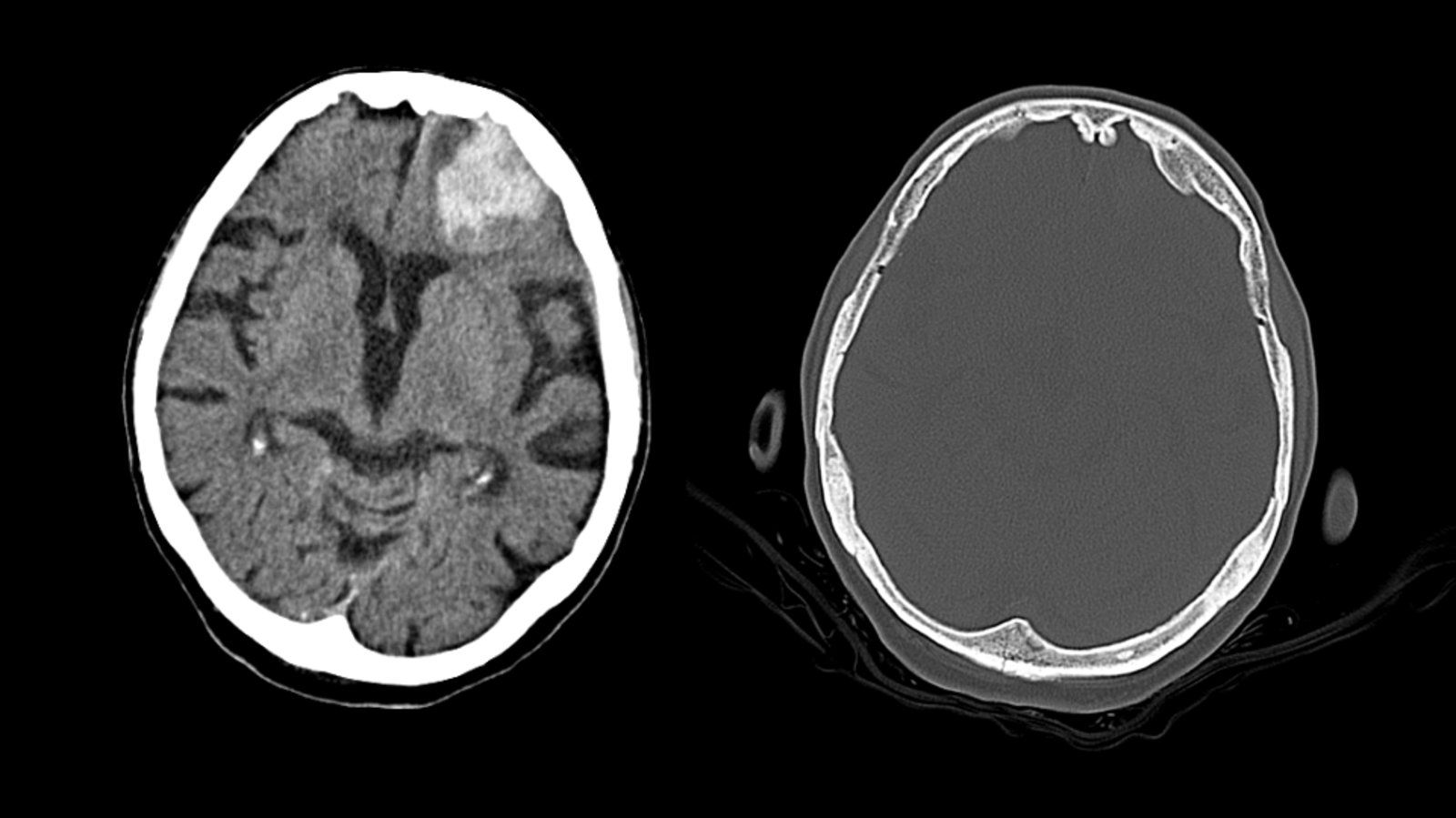
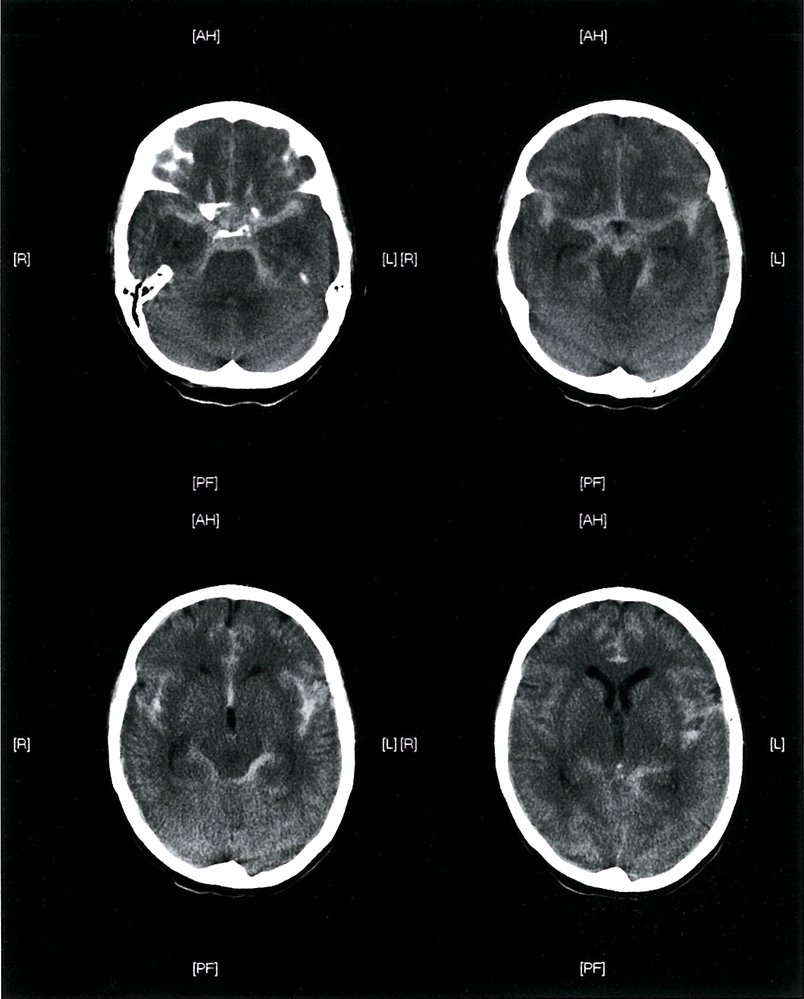
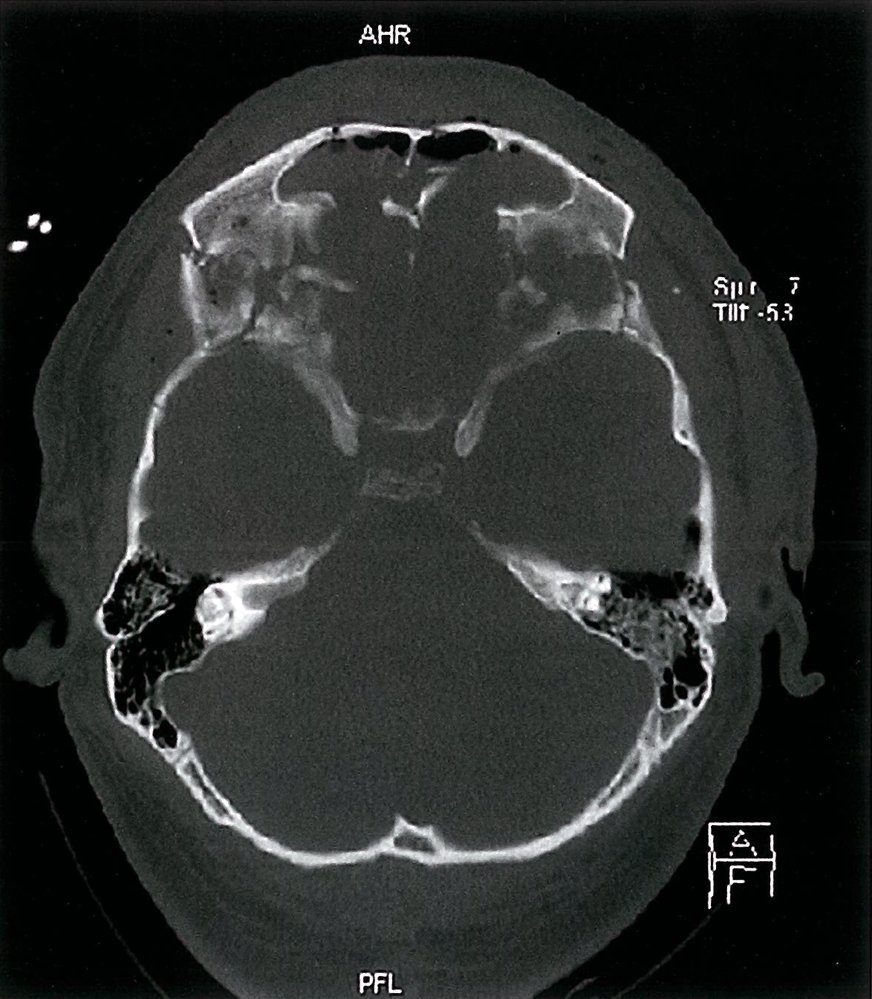
CT head (axial section; without IV contrast)
Brain window (left): A contusion is visible within the left frontal lobe as a well-defined heterogeneous lesion (blue overlay) surrounded by edema (hypodense rim; yellow overlay).
Bone window (right): A fracture of the skull in the occipital region (red overlay) can be seen.
These features are characteristic of a coup-contrecoup injury wherein the impact of the external force to the back of the head resulted in a cerebral contusion in the frontal lobe.
Our great thanks to PD Dr. M. Jergas (Center for Diagnostic and Interventional Radiology, St. Elizabeth Hospital, Cologne) for kindly providing this image.
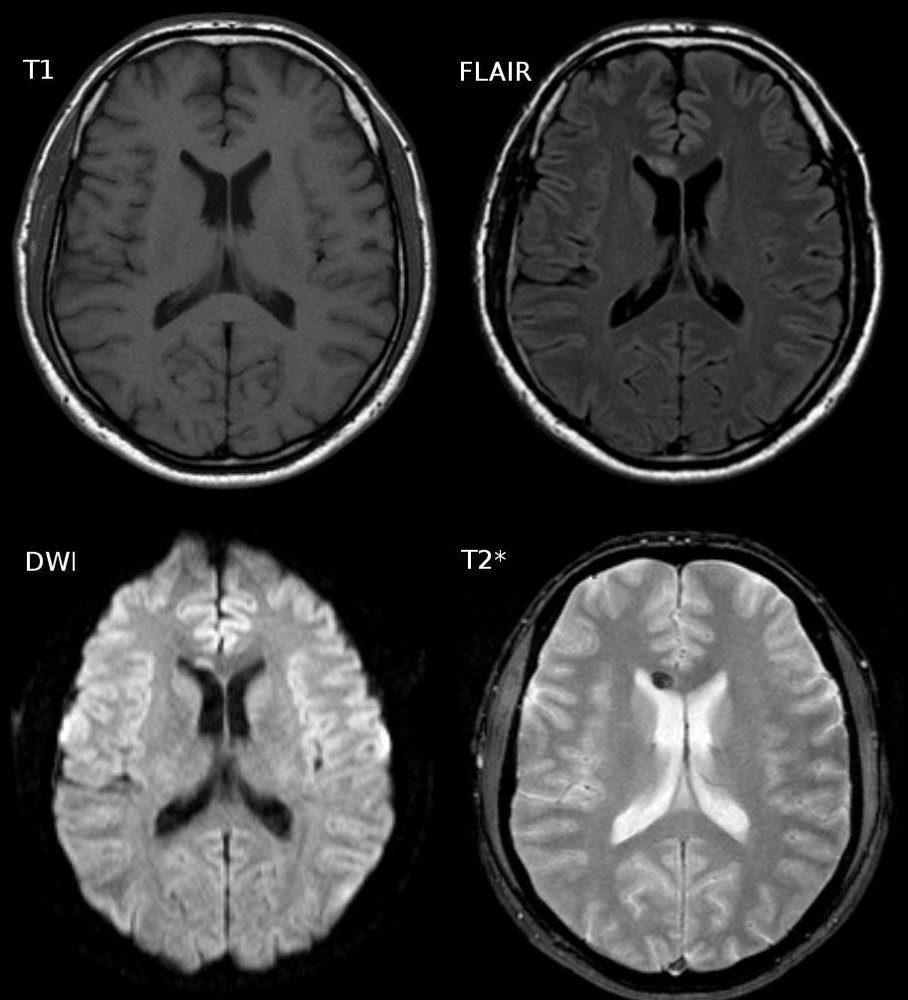
MRI head (axial section; T1, FLAIR, DWI and T2* [GRE])
An abnormal lesion (green overlay) is visible in the corpus callosum ventral to the frontal horn of the lateral ventricle in the FLAIR, DWI and T2* (GRE) images. The T2* (GRE) sequence is very sensitive for the detection of intracranial blood breakdown products.
The combination of the findings is consistent with the diagnosis of diffuse axonal injury.
Source: “Diffuse axonal injury- cMRT nach 3 Tagen” by Hellerhoff, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
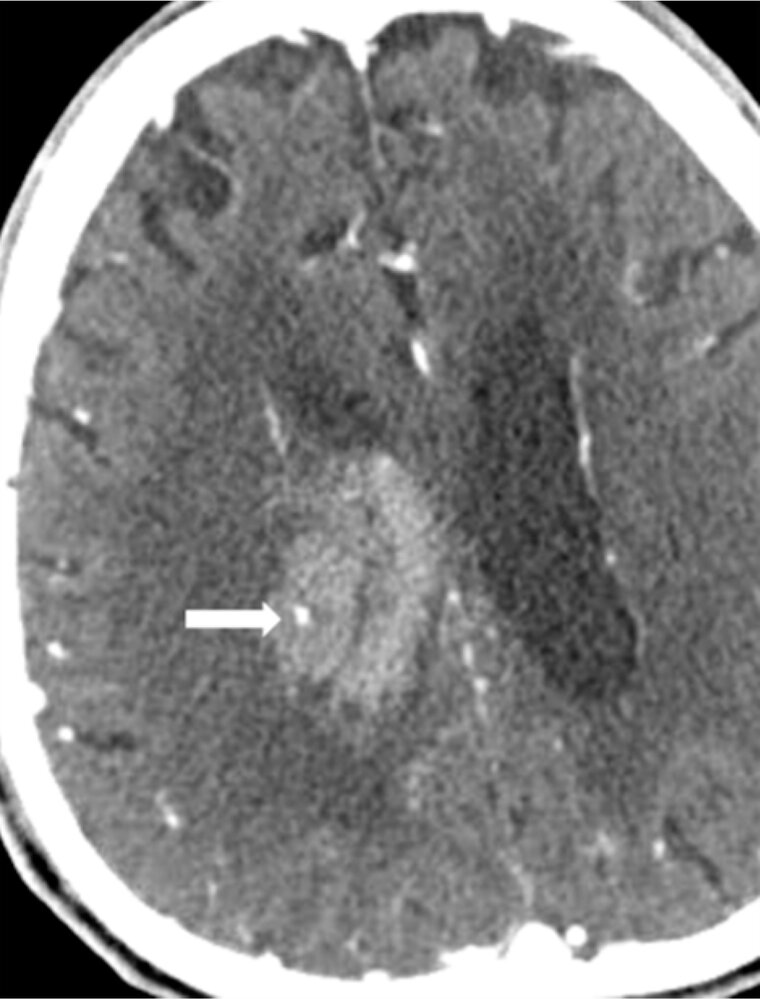
CT angiography head (second phase; axial plane)
A hyperdense area representing a hematoma (red overlay) is visible in the right basal ganglia and produces mass effect on the right lateral ventricle. The hematoma was seen on a precontrast study (first phase, not shown), but the dot-like hyperdensity within it (arrow; spot sign) was only visible postcontrast (second phase). The spot was not continuous with a normal enhanced blood vessel on multiplanar formatted images.
Contrast extravasation presenting as a positive spot sign indicates active bleeding and predicts hematoma expansion.
Source: “Fig. 4, in: Correlation between Spot Sign and Intracranial Hemorrhage Expansion on Dual-Phase CT Angiography” by Kim H, Goo JH, Kwak HS, Hwang SB, Chung GH, MDPI, licensed under CC BY 4.0. Modifications: Image was cropped. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Clinical features
Clinical features vary depending on the severity, location, and type of TBI. Patients require neurological examination and assessment of sensorium and cognition. For details see “Clinical features” in “EDH”, “SDH”, “SAH”, “ICH” and “Mild TBI”.
General symptoms
-
Global neurological symptoms
- Loss of consciousness or altered consciousness (e.g., confusion, disorientation), possibly with a lucid interval
- Headache
- Amnesia
-
Symptoms of increased intracranial pressure (ICP)
- Altered mood and behavior (e.g., aggressive behavior)
- Dizziness, nausea, vomiting
- Cushing triad
- Cerebral herniation syndromes
-
Focal neurologic deficits: depending on the affected brain region (see “Stroke symptoms by affected region”)
- Contralateral hemiparesis or hemiplegia
- Contralateral sensory loss
- Cranial nerve palsies (e.g., diplopia, blurred vision, unequal pupils, anosmia)
- Slurred and/or disorganized speech
- Impaired coordination
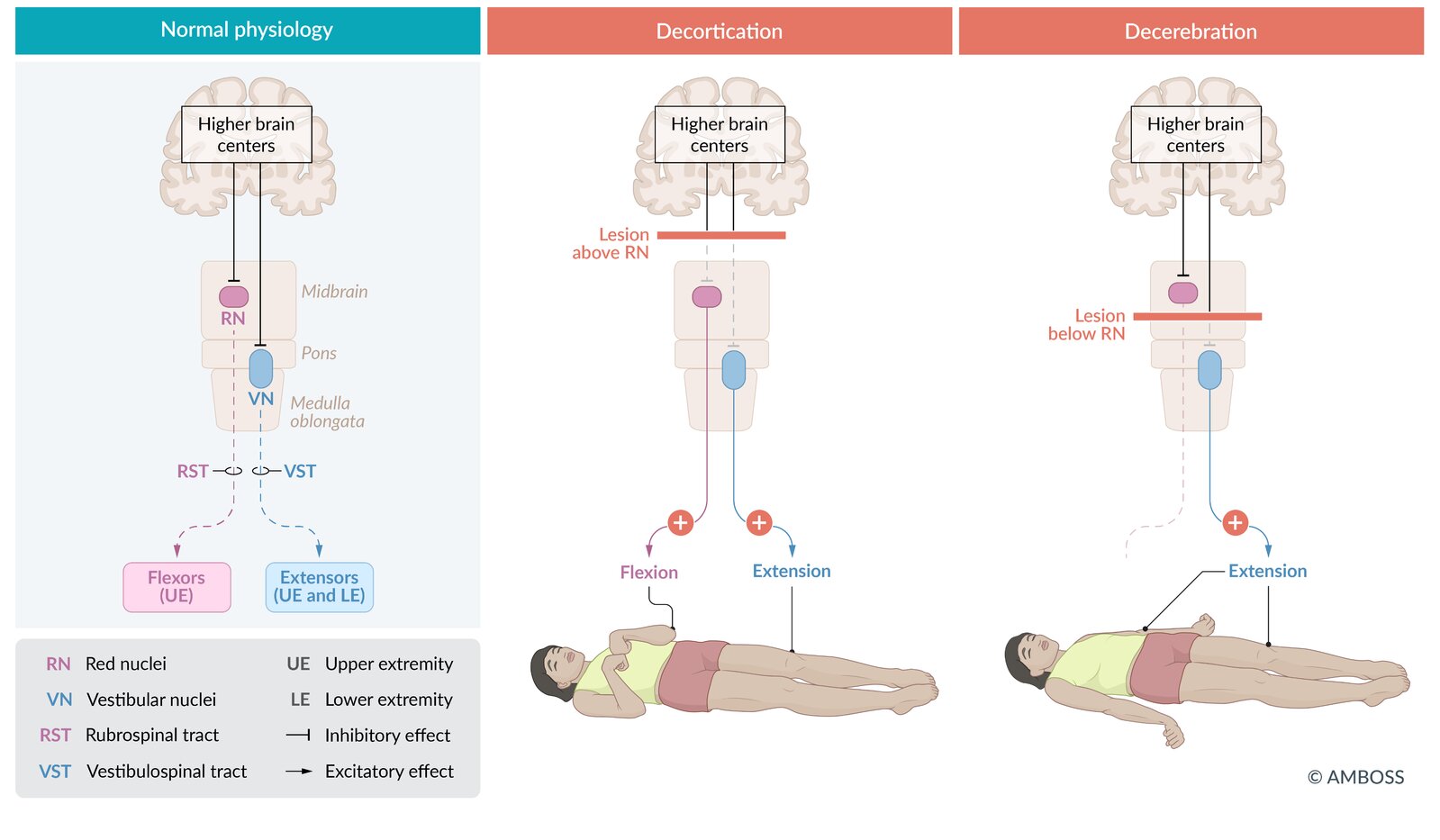
- Abnormal posturing: characteristic posture of the limbs that typically signifies severe brain injury (most commonly involving the brainstem) [17][18]
| Abnormal posturing | ||
|---|---|---|
| Decorticate posturing (flexor posturing) | Decerebrate posturing (extensor posturing) | |
| Description |
|
|
| Site of injury |
|
|
| Overactive tract |
|
|
| Prognosis |
|
|
In deCORticate posture, the arms are flexed towards the CORe of the body.

Symptoms of associated injuries
-
General symptoms of skull fractures [19][20]
- Hematoma; , local swelling, and laceration of the scalp
-
Liquorrhea: leakage of CSF from the subarachnoid space through an external opening
- Due to a dural tear immediately or within the first few days after the trauma
- May show a halo sign: rapidly-expanding clear ring of fluid surrounding blood
-
Basilar skull fractures
-
Anterior basilar skull fracture
- CSF rhinorrhea
- Raccoon eyes
- Palsies of cranial nerves I, V, VI, VII, and/or VIII
-
Posterior basilar skull fracture
- CSF otorrhea
- Hemotympanum
- Battle sign [21]
- Palsies of cranial nerves VI, VII, and/or VIII palsies
-
Anterior basilar skull fracture
- Facial fractures: hematomas, facial and/or nasal swelling, epistaxis, visible deformity
- C-spine injuries: See “Clinical features of C-spine injuries.”
Skull fractures, (worsening) neurological impairment, repeated vomiting, and seizures are indicative of more severe trauma or intracranial hemorrhage.



© AMBOSS

Face of a 54-year-old man after a fall on the back of his head 2 days earlier
Bilateral, symmetrical, dark purplish discoloration around the eye sockets is visible.
This appearance, also referred to as "raccoon eyes," is a typical sign of basilar skull fractures involving the anterior fossa and typically develops 1–3 days after injury. Nontraumatic causes include neuroblastoma, plasma cell proliferative disorders (e.g., amyloidosis), and hematological malignancies. Periorbital ecchymosis may occur unilaterally or bilaterally.
Source: “Fig 1, In: A man with panda eyes after a fall” by Mahdi D, Yosief LS, Butt U et al., Wiley Online Library, licensed under CC BY 4.0.

Otoscopic image of the tympanic membrane
The tympanic membrane is intact with a blue hue (instead of the normal pearly white color) and appears to be bulging outward.
These features are characteristic of hemotympanum. In patients with head injury, hemotympanum is strongly suggestive of a fracture of the temporal bone.
Source: © IMPP
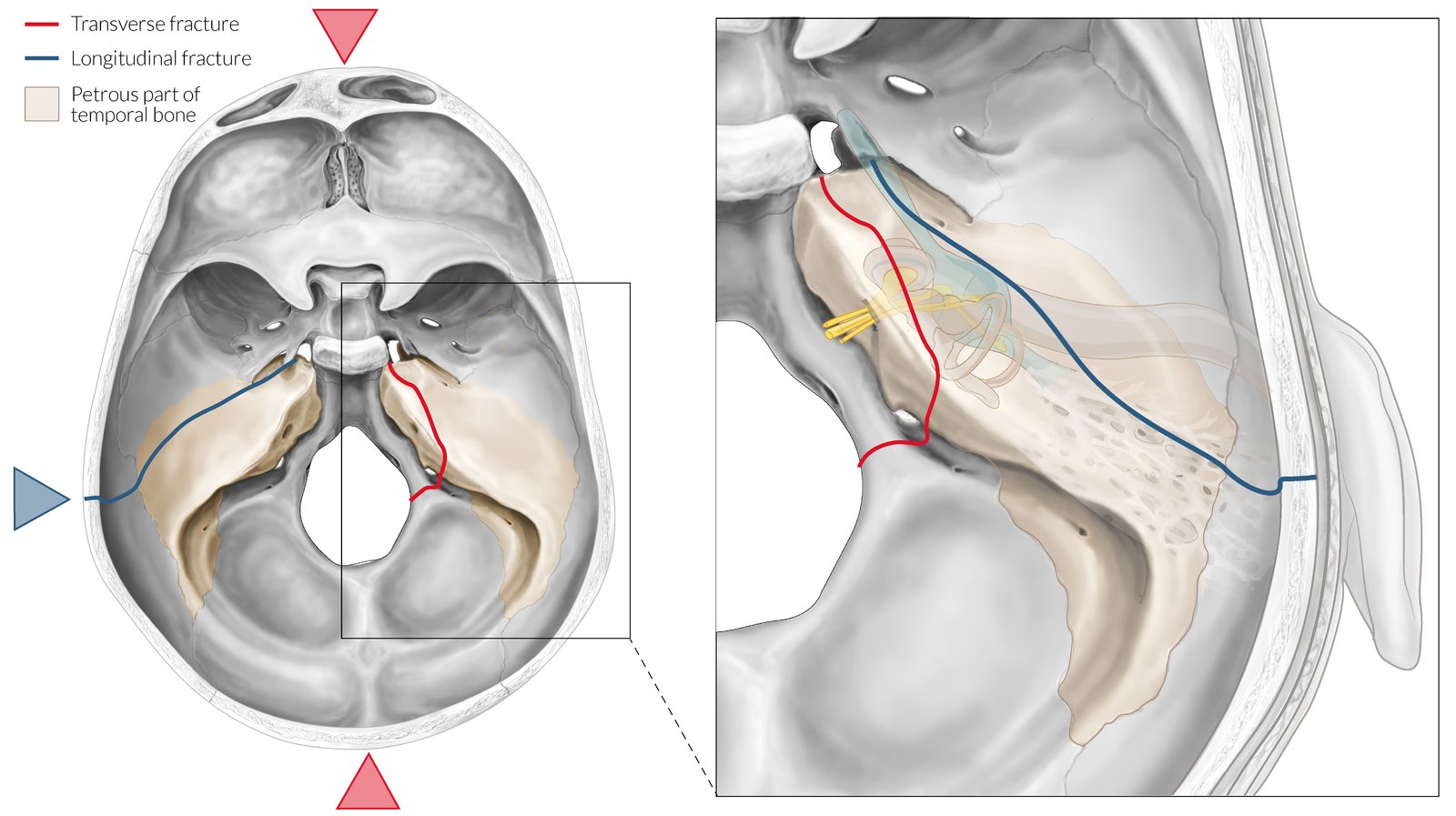
Temporal bone fractures are classified according to the fracture line through the petrous part of the temporal bone.
Longitudinal fractures (blue line) are more common and result from lateral or temporal force (blue arrow). Clinical features are due to damage to the middle ear and involve injury to the tympanic membrane, bleeding from the auditory canal, conductive hearing loss, and potentially cerebrospinal fluid (CSF) leakage from the ear in the event of dural laceration. Peripheral facial paralysis occurs in 20% of cases.
Transversal fractures (red line) are rare and result from frontal or occipital force (red arrows). Clinical features are due to damage to the inner ear and include sensorineural hearing loss and involvement of the otic capsule, leading to vertigo, nausea, and spontaneous nystagmus. CSF leak from the nose may occur. Otoscopy shows an intact tympanic membrane, which may appear blue because of the hemotympanum. Peripheral facial paralysis occurs in 50% of cases.
© AMBOSS
Initial management
Approach [22][23][24]
-
Start primary survey (ABCDE survey) with simultaneous neuroprotective measures.
- Additional prehospital trauma care (e.g., spine immobilization, analgesics)
- Maintain or achieve normoxia, normocapnia, blood pressure control, and euglycemia.
- Begin initial management of C-spine injuries, if indicated.
- Measure GCS and pupillary response.
- Classify TBI by severity based on GCS.
- Transfer to a neurocritical care unit if needed.
- Diagnostics and imaging (usually noncontrast CT) if indicated
- Treatment and further management based on severity scores and CT findings
Resuscitative measures to achieve normoxia, normocapnia, normotension, and euglycemia take precedence in the acute management of TBI and should not be delayed for diagnostic steps.
Neuroimaging should not delay transfer to centers that can provide definitive neurosurgical care if required. [24]
Hypotension in TBI significantly worsens the prognosis and should be identified and treated. Permissive hypotension is harmful in TBI. [23]
Primary survey [24]
The primary survey should follow the ATLS algorithm (ABCDE). The goal is to identify and treat any life-threatening conditions and avoid secondary brain injury.
| Key aspects for primary survey in TBI [22][23][24] | |
|---|---|
| Airway |
|
| Breathing |
|
| Circulation |
|
| Disability |
|
| Exposure |
|
Patients with moderate or severe TBI (GCS ≤ 12) require emergency neuroimaging with noncontrast head CT after stabilization even if potential additional causes for mental obtundation are present (e.g., alcohol intoxication).
Secondary survey
-
Focused history
- SAMPLE history
- Mechanism/time of injury
- Presence/duration of amnesia
- Presence of seizures/headache
- Use of anticoagulant medication
- Physical examination: thorough head-to-toe examination and complete neurological examination
-
Continuous monitoring
- Vitals, SpO2
- Serial neurological examination: GCS, pupillary exam, lateralizing signs
-
Emergency consults
- Neurosurgery (if GCS ≤ 12 or deteriorating)
- Trauma surgery for additional major trauma
- Transfer: If GCS ≤ 12, transfer to a trauma center or neurocritical care unit if unavailable at current site
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
Classification
Severity classification using Glasgow coma scale (GCS) [33][34][35]
-
Clinical applications of GCS in TBI [12]
- Assessing the level of consciousness objectively
- Guiding targeted therapies [12]
- Estimating patient prognosis
- Monitoring therapy
- Evaluating AMS or coma of concurrent etiologies (e.g., stroke, intoxication)
-
Scoring of GCS
- Eye opening (E): spontaneous (4); to verbal instruction (3); to pain (2); unresponsive (1)
- Verbal response (V): oriented (5); confused (4); inappropriate words (3); incomprehensible sounds (2); unresponsive (1)
- Motor response (M): follows instruction (6); localizes pain (5); withdraws from pain (4); decorticate posturing (3); decerebrate posturing (2); unresponsive (1)
-
Interpretation of GCS
- GCS 3 (minimum score): deeply comatose or imminent brain death
- GCS 15 (maximum score): fully conscious
-
TBI severity
- Mild TBI (mTBI): GCS 13–15; includes concussion; may or may not be associated with neuroimaging findings [24]
- Moderate TBI: GCS 9–12; usually associated with structural brain lesions on neuroimaging
- Severe TBI: GCS ≤ 8; usually an indication for intubation
-
Important considerations
- Record the score of each criterion individually (e.g., GCS 11, E(3) V(4) M(4)).
- The score is invalid if any parameter is nontestable.
- Alcohol and certain drugs (e.g., analgesics, antidepressants, anesthetics) may affect initial score.
- Significant hypotension (SBP < 90 mm Hg) alters GCS. [24]
GCS is the standard for initial evaluation and classification of patients with traumatic brain injury.
Significant hypotension alters GCS. Reassess GCS after correction of hypotension [24]
Other classifications
-
By mechanism of injury, e.g.:
- Primary brain injury vs. secondary brain injury
- Due to closed head injury or open head injury
- Associated with blunt head injury, penetrating head injury, or blast injury
- By type of injury (usually seen on neuroimaging): e.g., EDH, SDH, traumatic SAH, traumatic ICH, traumatic IVH, DAI, cerebral contusion
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
Diagnosis
General principles [24]
-
Head CT without IV contrast is the first-line diagnostic modality.
- Mild TBI: imaging only required for patients fulfilling criteria for neuroimaging in mTBI
- Moderate/severe TBI: emergency neuroimaging after stabilization
- The goal of diagnostics is timely identification of lesions that require neurosurgical intervention.
- Imaging should not delay transfer to centers that can provide definitive neurosurgical care if required.
- Obtain imaging of other potential sites of injury, e.g., diagnostics for C-spine injury.
Possible traumatic brain injury should always be considered in a patient with a decreased or altered consciousness.
Neuroprotective measures take precedence over diagnostics.
Imaging [23][24][36]
Head CT without IV contrast
-
Indications: preferred first-line imaging modality in patients with TBI [24][37]
- Moderate or severe TBI (GCS ≤ 12)
- Mild TBI (GCS ≥ 13): only if any criteria for neuroimaging in mTBI are present
- Open head injury
- Depressed skull fracture
- Short-term follow-up of TBI in patients with rapid deterioration of neurological symptoms
-
Supportive findings
- On brain window
- Usually normal in mTBI [38]
- Intracranial hemorrhage or hematoma: hyperdense lesions (see “Differential diagnosis of intracranial hemorrhage” for a comparison of CT findings)
-
Mass effect
- Compression of cerebral parenchyma adjacent to hematoma
- Midline shift to the contralateral side of the hematoma
- Brain herniation: displacement of brain tissue from one compartment to another [36]
- Diffuse axonal injury (DAI): can be normal in mild DAI; multiple punctate hyperdensities indicating small hemorrhages typically at the junction of gray and white matter, brainstem, internal capsule, and corpus callosum [23][36]
- Cerebral contusion: heterogeneous lesion (mixed hemorrhagic, necrotic, and edematous tissue) surrounded by cerebral edema [23]
- Cerebral edema: compression of ventricles, loss of defined sulci and gyri, and effacement of basal cisterns [36]
- On bone window
- Evidence of skull fractures: linear, depressed, or basilar skull fractures
- Pneumocephalus: air within the cranium; typically associated with an open skull fracture
- On brain window
-
Scrollable CT imaging examples
- EDH and SDH
- SDH
- Traumatic ICH










MRI head without IV contrast [37]
-
Indications
- Acute TBI with symptoms unexplained by CT (in hemodynamically stable patients) [24][36]
- Short-term follow-up of acute TBI in patients with rapid deterioration of neurological symptoms (alternative to CT)
- Subacute or chronic TBI with new, persistent, or worsening of neurological or cognitive deficits (preferred modality) [36][37]
- Supportive findings: Microhemorrhages, DAI, and contusions are better visualized on MRI than on CT.
Additional imaging [36][37]
Consider additional imaging based on the patient's history and clinical features or if initial imaging modality findings are inconsistent with neurological symptoms.
- CT cervical spine: obtain if C-spine injury is suspected (see “Diagnostics for C-spine injury” for details). [39]
- CT maxillofacial and/or temporal bone without IV contrast: in suspected CSF leak
-
CT or MR angiography: in suspected intracranial arterial injury [37]
- CTA spot sign
- Signs of BCVI and penetrating injuries [36]
- CT or MR venography: suspected cerebral venous thrombosis: [37]
Laboratory studies [23][24]
- In patients with altered consciousness
- Blood glucose
- Blood alcohol level
- Urine toxicology screen
- Serum electrolyte levels
- ABG analysis
- In patients with suspected coagulopathies : coagulation panel
- In patients with moderate TBI, severe TBI, and/or extensive blood loss from other injuries : blood type and screen
- In women of childbearing age: urine/serum pregnancy test
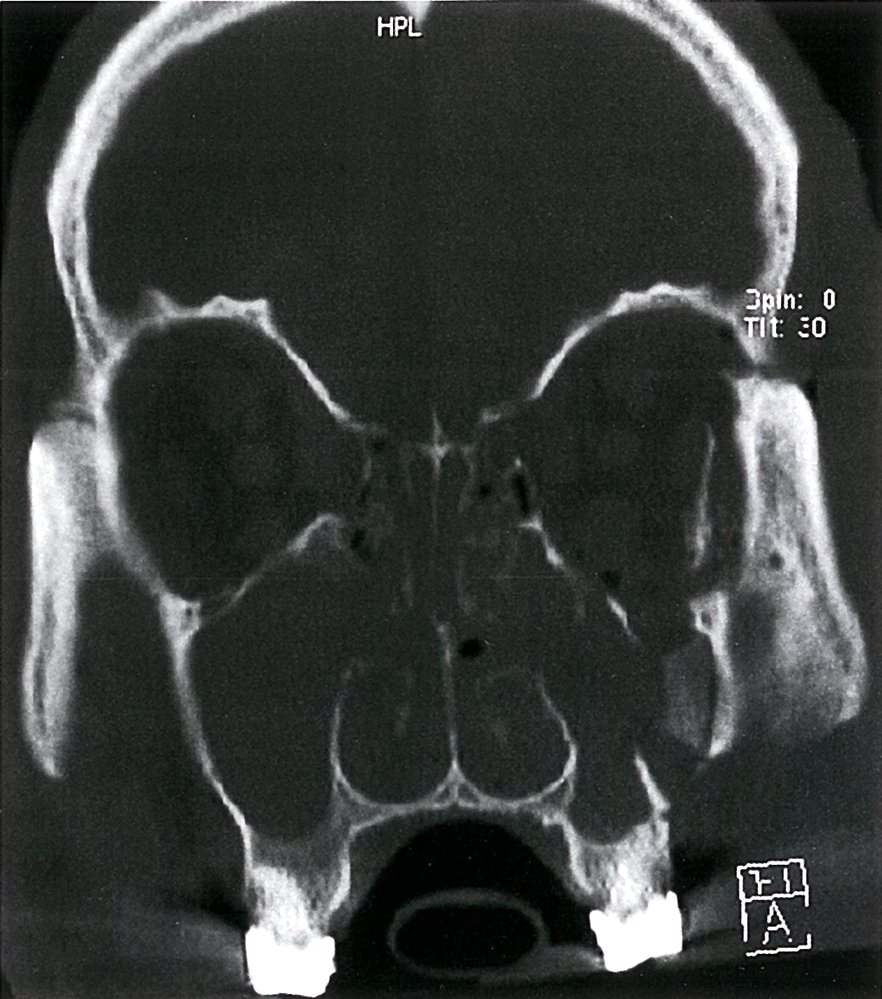
CT facial bones and orbits (coronal plane; bone window)
Fractures involve the left maxillary sinus and lateral and inferior walls of the left orbit (green arrows). There is diastasis of the left zygomaticofrontal suture (red arrow). The maxillary and ethmoid sinuses are opacified by blood (blue overlay).
Source: © IMPP
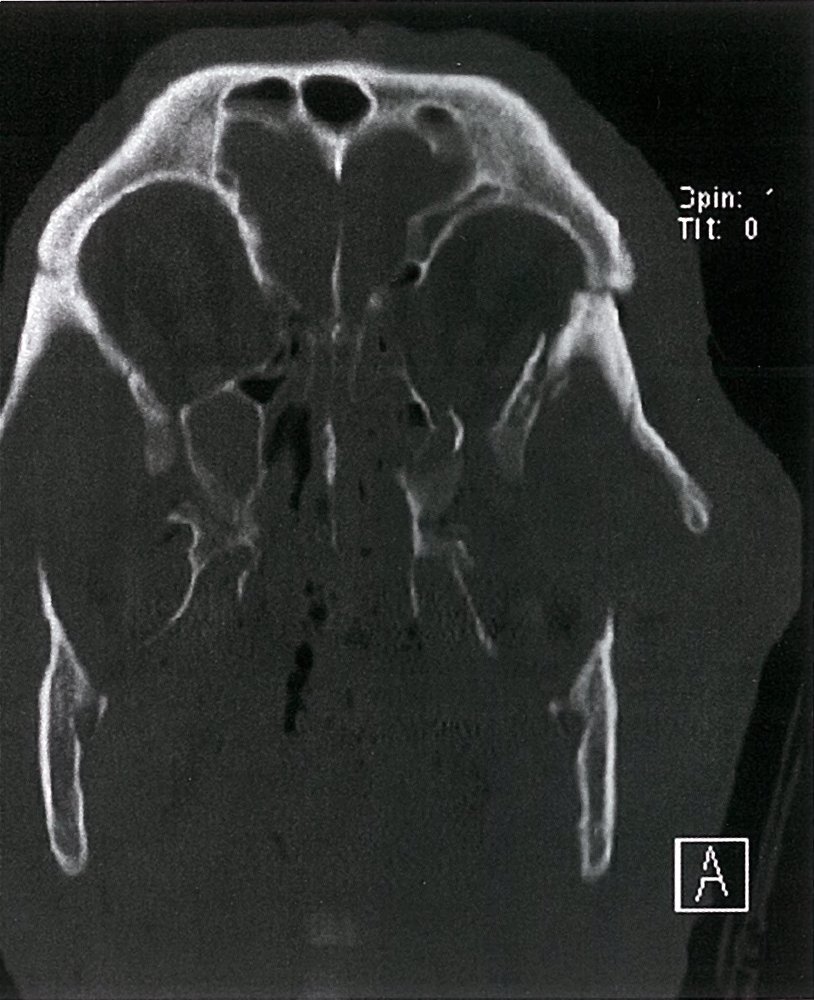
CT facial bones (coronal oblique plane; bone window)
There are fractures through the left zygomaticofrontal suture (red arrow) and orbital wall (green arrows). The left zygomatic arch is depressed (white arrow). The ethmoid sinuses are nearly completely opacified (blue overlay) and an air-fluid level (green overlay) is seen in the frontal sinus.
Source: © IMPP
Click on the overlay icon below the taskbar on the left to toggle the overlay on and off.
CT head (brain window: axial and coronal planes; bone window: axial plane)
A biconvex epidural hematoma (green overlay) with mass effect is seen in the left frontal region, adjacent to which is a small frontotemporal subdural hematoma (red overlay). A calvarial fracture (arrowheads) involves the left temporal and parietal bones.
Created by: Nándor Faluhelyi. Organization providing image: University of Pécs, Medical School. Further notes: Our great thanks to Nándor Faluhelyi (University of Pécs, Medical School) for kindly providing this case.

Click on the overlay icon below the taskbar on the left to toggle the overlay on and off.
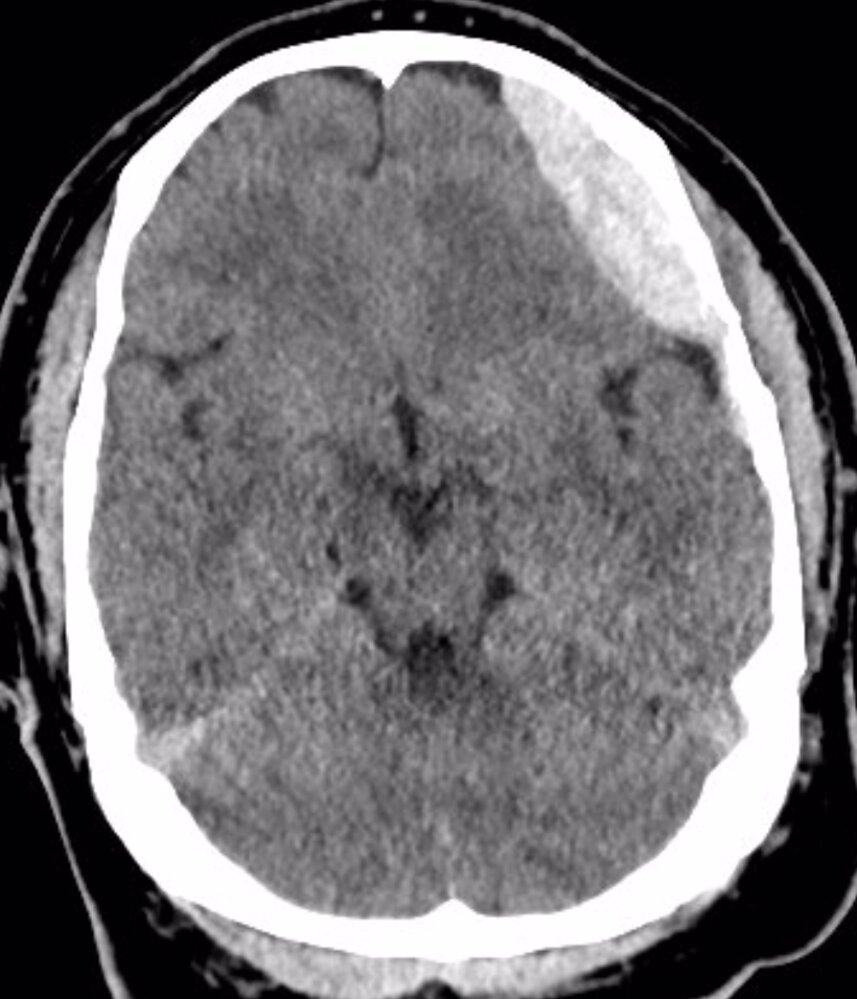
CT head (without contrast; axial plane)
The hyperdense, crescent-shaped, extra-axial collection (green overlay) visible along the left frontal convexity is compatible with an acute subdural hematoma.
Additional findings of dilated ventricles and sulci indicate generalized cerebral atrophy. The periventricular hyperlucencies are consistent with cerebral small vessel disease.
Original title: “Subdurales Hämatom”. Created by: Dr. med. Kerstin Bohse. Organization providing image: Clinic Pfeiffersche Stiftungen. Further notes: Our great thanks to Dr. med. Kerstin Bohse (Clinic Pfeiffersche Stiftungen) for kindly providing this case.
Click on the overlay icon below the taskbar on the left to toggle the overlay on and off.
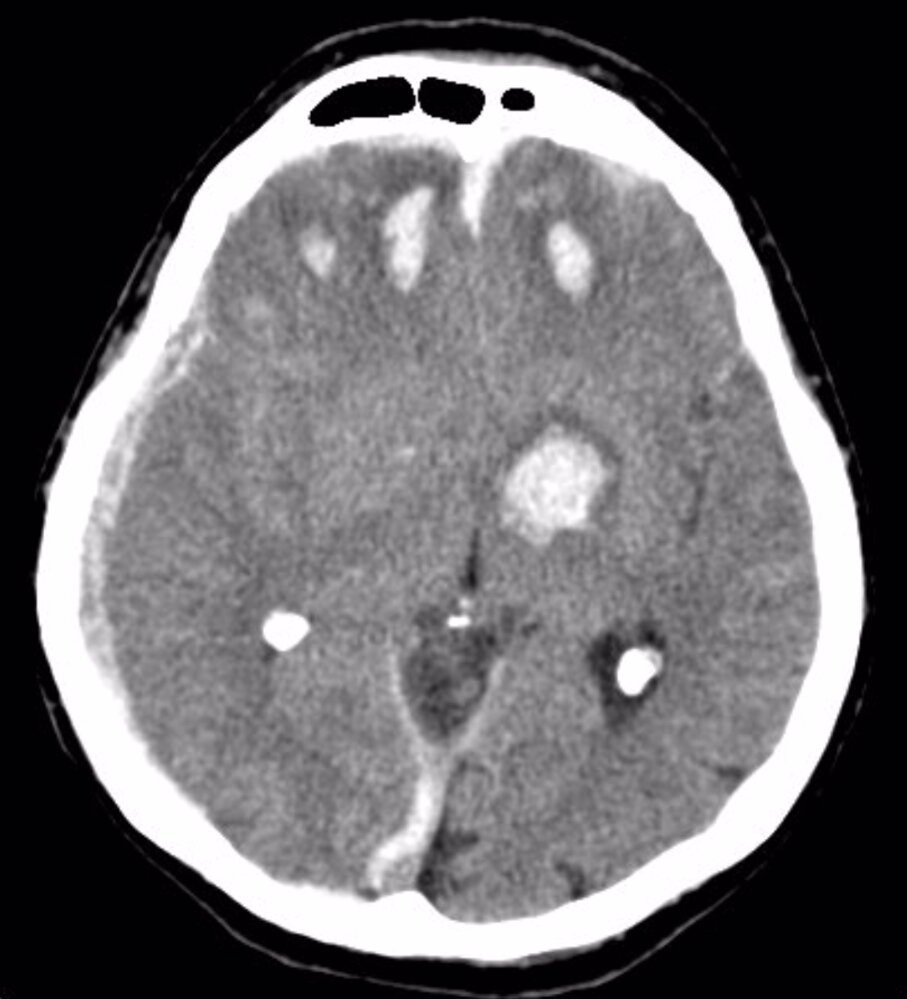
CT head (without contrast; brain and bone windows; axial plane) of a 47-year-old patient after head trauma
Brain window images show multiple sites of parenchymal contusion in the frontal lobes (green overlay). Additional hemorrhage involves the left basal ganglia and internal capsule (yellow overlay). Scattered areas of subarachnoid hemorrhage (examples indicated by blue overlay) are present, and a subdural hematoma (red overlay) along the right cerebral convexity has caused mass effect with contralateral shift (dashed white line) of the midline. Hemorrhage extends along the falx cerebri, which appears hyperdense and thickened (especially dorsally).
Bone window images show a calvarial fracture (green overlay) that extends from the frontal bone into the sagittal suture. Zygomatic (red circle) and nasal bone (green circle) fractures are also seen, and there is extensive hemosinus (example indicated by hatched green overlay).
Created by: Nándor Faluhelyi. Organization providing image: University of Pécs, Medical School. Further notes: Our great thanks to Nándor Faluhelyi (University of Pécs, Medical School) for kindly providing this case.
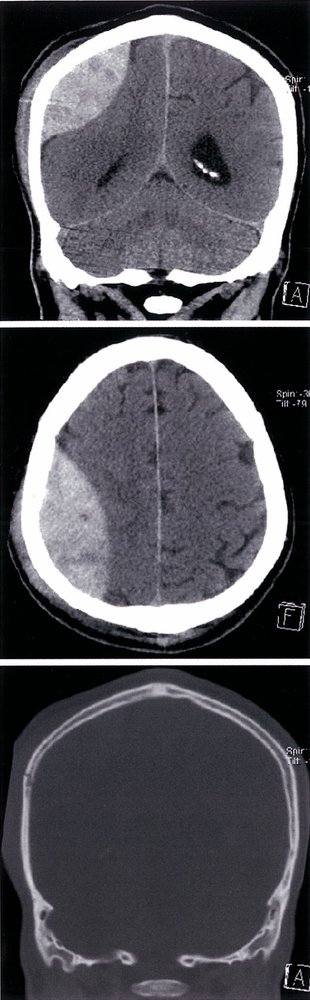
CT head (without IV contrast; top: brain window, coronal plane; middle: brain window, axial plane; bottom: bone window, axial plane)
An epidural hematoma (EDH) is visible as a biconvex, heterogeneous, hyperdense extra-axial collection (green overlay) in the right hemicranium. Mass effect on the adjacent cerebral parenchyma and right lateral ventricle (yellow overlay) has produced contralateral midline shift (indicated by dashed line). The hematoma does not cross the coronal or the lambdoid suture. A scalp hematoma is present (red overlay), and a fracture of the underlying right parietal bone (green circle) is visible on the bone window image.
A biconvex hyperdense extra-axial collection limited by skull suture lines is the characteristic presentation of an EDH. The majority of patients with an EDH have an associated skull fracture.
Source: © IMPP
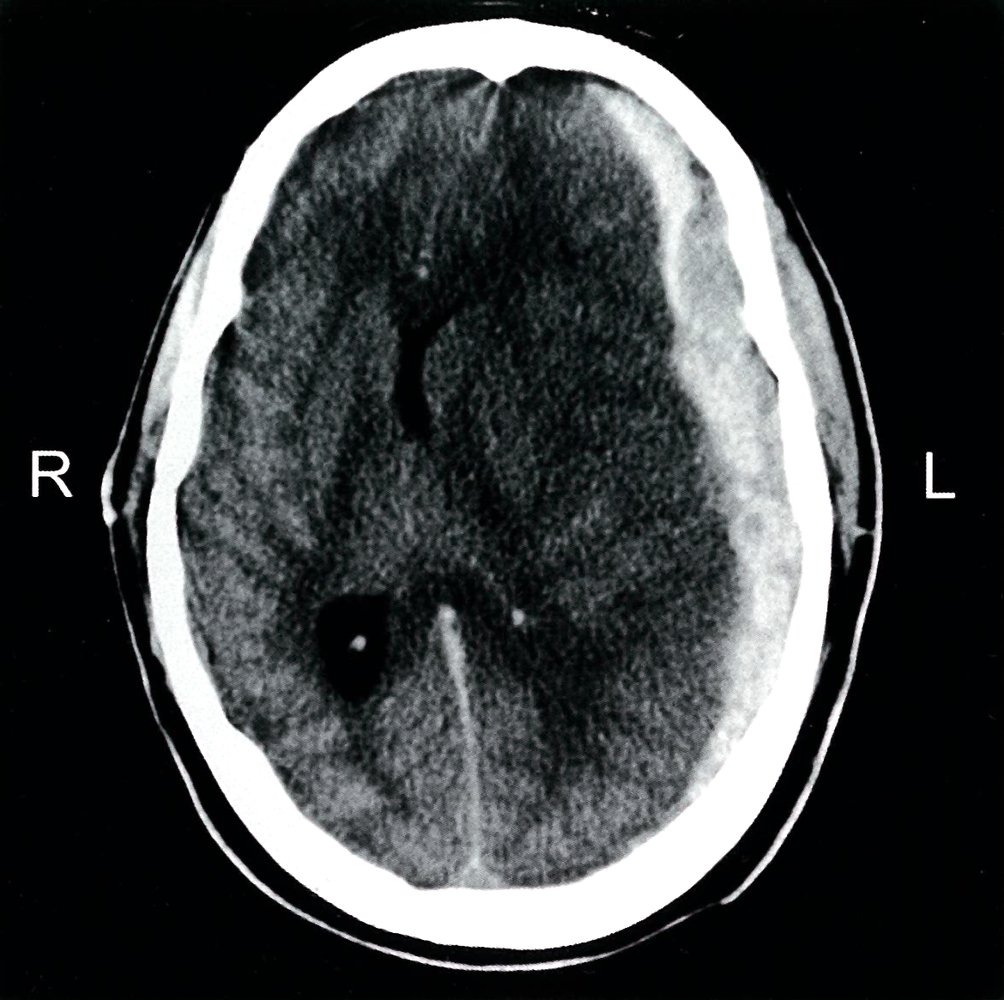
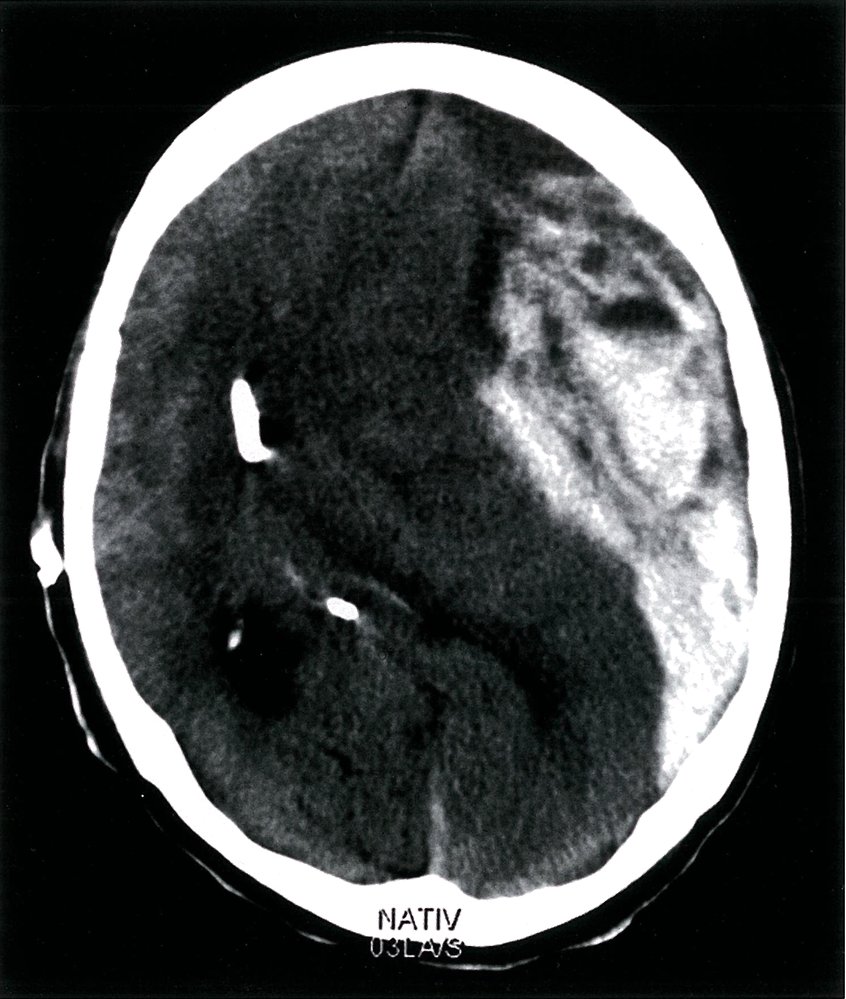
CT head (without IV contrast; axial section; brain window) of a patient with a history of trauma
A large acute subdural hematoma is visible as a hyperdense crescent-shaped lesion along the lateral aspect of the left hemisphere (red overlay). It is accompanied by an extracranial soft tissue hematoma (hatched red overlay). There is extensive hypodense left cerebral edema (gray overlay), with sulcal effacement and shift of midline structures (green line) to the right. The anterior horns of the lateral ventricles (hatched green overlay) are compressed and the posterior horn of the right lateral ventricle (red circle) is dilated.
Source: © IMPP

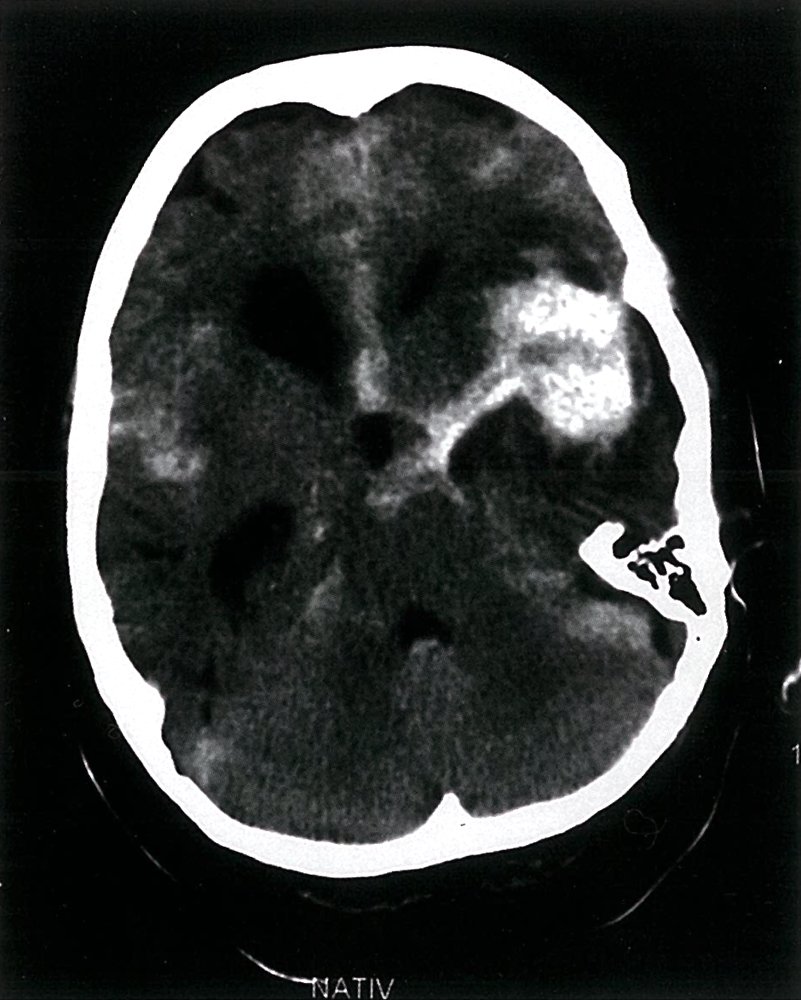
CT head (axial section; without IV contrast: brain window)
There are multiple intraparenchymal hyperdensities (green overlay) in the left frontotemporal lobes and right frontal lobe, indicating multiple intracerebral hemorrhages. Hyperdensities (green lines) in the interhemispheric region and the interpeduncular region of the basal cistern are identifiable. These are consistent with a subarachnoid hemorrhage. A fracture line (green arrow) is visible in the right frontal bone and pneumocehalus, visualized as hypodense air (circled) within the soft tissue overlying the fracture segment, indicates an open fracture. The extracranial hyperdense region in the anterolateral aspects of the scalp indicates a large subgaleal hemorrhage (hatched green overlay).
Source: © IMPP
CT head (without contrast; axial plane)
Multiple areas of high attenuation in the basal cisterns, Sylvian fissures, and sulci (examples indicated by green overlay) are characteristic of extensive subarachnoid hemorrhage.
Source: © IMPP
CT head (axial section; without IV contrast)
Brain window (left): A contusion is visible within the left frontal lobe as a well-defined heterogeneous lesion (blue overlay) surrounded by edema (hypodense rim; yellow overlay).
Bone window (right): A fracture of the skull in the occipital region (red overlay) can be seen.
These features are characteristic of a coup-contrecoup injury wherein the impact of the external force to the back of the head resulted in a cerebral contusion in the frontal lobe.
Our great thanks to PD Dr. M. Jergas (Center for Diagnostic and Interventional Radiology, St. Elizabeth Hospital, Cologne) for kindly providing this image.
CT head (axial plane; bone window)
Multiple fractures (red lines) involve the anterior skull base and anterior wall of the frontal sinus. Air and swelling (green overlay) are present in the extracranial soft tissues.
Source: © IMPP
MRI head (axial section; T1, FLAIR, DWI and T2* [GRE])
An abnormal lesion (green overlay) is visible in the corpus callosum ventral to the frontal horn of the lateral ventricle in the FLAIR, DWI and T2* (GRE) images. The T2* (GRE) sequence is very sensitive for the detection of intracranial blood breakdown products.
The combination of the findings is consistent with the diagnosis of diffuse axonal injury.
Source: “Diffuse axonal injury- cMRT nach 3 Tagen” by Hellerhoff, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
Management
Overview
- After the initial management of TBI, the severity of injury and neuroimaging findings determine further management.
- The goal is to prevent secondary brain injury and provide surgical treatment if necessary.
- Arrange for definitive management of C-spine injuries, if present.
- For surgical management of intracranial lesions see “Treatment” in “EDH”, “SDH”, “SAH”, “ICH”, and “Elevated intracranial pressure and brain herniation”.
| Overview of TBI management [23][24] | ||
|---|---|---|
| Severity of TBI | Treatment | Supportive care |
| Mild (GCS ≥ 13) |
|
|
| Moderate TBI (GCS 9–12) |
|
|
| Severe TBI (GCS ≤ 8) |
|
|
Moderate and severe TBI
Surgical treatment [23][24]
Consult neurosurgery and initiate treatment as needed based on the underlying condition (see “Treatment” in “EDH”, “SDH”, “SAH”, and “ICH” for details).
-
Skull fracture surgery can be indicated for depressed skull fracture with one of the following:
- Open fracture with dural penetration or significant depression
- Significant cranial hematoma
- Frontal sinus involvement
- Gross contamination/wound infection
- Pneumocephalus
- Major cosmetic deformity
-
Craniotomy and evacuation of hematomas
- EDH and acute SDH meeting criteria for surgery should have evacuation done as soon as possible.
- See “SDH” and “EDH” for details on indications and methods.
- Surgical management of ↑ ICP (See “ICP management” for details.)
- Extraventricular drain (EVD)
-
Decompressive craniectomy [26]
- Indicated in traumatic intraparenchymal hemorrhages and posterior fossa hemorrhages with:
- Mass effect
- Neurological deterioration attributable to the lesion
- High ICP refractory to medical therapy
- Approach (e.g., suboccipital, subtemporal, frontotemporoparietal) depends on lesion location.
- Indicated in traumatic intraparenchymal hemorrhages and posterior fossa hemorrhages with:
Additional treatment and monitoring
-
Antifibrinolytic therapy: Consider TXA.
- Moderate TBI: Consider TXA (off-label) if < 3 hours have elapsed since the injury [40][41][42][43][44]
- Severe TBI: benefit of TXA unlikely because of potentially extensive intracranial hemorrhage at presentation [40]
-
Supportive care:
- ICP management
- Intubated patients: See “Adjunctive care of ventilated patients”.
- Pain management: Treat pain and agitation with analgesics and sedatives.
- Antiemetics (in patients with significant nausea/vomiting)
-
Monitoring
- Continuous or frequent monitoring of vitals.
- Frequent assessment of GCS
- Frequent monitoring of blood glucose and serum electrolyte levels as needed.
- Consider invasive ICP monitoring in patients with risk factors for elevated ICP, including:
- GCS ≤ 8 and signs of high ICP on CT scan
- Normal CT scan and ≥ 2 of the following:
- Age > 40 years
- Unilateral or bilateral motor posturing
- SBP < 90 mm Hg
- Pain: Use self-reported or behavior-based pain scales.
- Sedation: Use standardized scales to assess agitation and level of sedation (e.g., RASS).
-
Follow-up neuroimaging
-
Moderate TBI: consider after 12–24 hours or before discharge if any of the following are present: [45][46]
- Clinical deterioration
- Initial neuroimaging showed abnormalities
- Elevated ICP
- Coagulopathy
- Hypotension
- Severe TBI: usually obtained 6 hours after initial neuroimaging [47]
-
Moderate TBI: consider after 12–24 hours or before discharge if any of the following are present: [45][46]
- Disposition: admission/urgent transfer to definitive neurosurgical care or neurocritical care unit
Continuing neuroprotective measures to avoid secondary brain injury is crucial for the management of moderate and severe TBI.
Pain and agitation increase SBP and ICP and contribute to secondary brain injury and should be managed adequately (see ICP management). [49]
Prevention of complications in brain injuries
Secondary bleeding or hematoma expansion
-
Anticoagulant reversal [50][51]
- Indication: all patients with intracranial hemorrhage who are on anticoagulant medication
- Contraindication: concomitant cerebral venous thrombosis [50]
- Target INR: ≤ 1.4 [24]
- Treatment
- Stop further doses of anticoagulants.
- Administer anticoagulant reversal.
- Resumption of anticoagulant therapy should be individualized. [52][53]
-
Antiplatelet therapy, thrombocytopenia, and platelet dysfunction [2][23]
- Stop further doses of antiplatelet agents.
- Patients planned for neurosurgery or invasive procedures: Consider platelet transfusion if platelet count is 80,000–100,000/μL. [31][54]
- Resumption of antiplatelet therapy should be individualized.
- DIC monitoring: repeat INR, platelets, and hemoglobin
Additional prophylactic measures
-
DVT prophylaxis [26]
- Mechanical prophylaxis: recommended in patients with an active intracranial bleed
- Pharmacological prophylaxis: consider LMWH or low-dose unfractionated heparin in stable TBI after individual risk-benefit evaluation
-
Antibiotic prophylaxis [26][51]
- Not routinely recommended
- Consider in select patients with open head injuries.
- See “CNS infection prophylaxis for open head injury” for details.
-
Seizure prophylaxis and treatment
- Prophylaxis [23][26]
- Indicated in severe TBI for 7 days postinjury to prevent early post-traumatic seizures
- Preferably with phenytoin or levetiracetam [2][26][48]
- See “Seizure prophylaxis after TBI” for dosages.
- Treat acute seizures.
- Prophylaxis [23][26]
- Maintenance of vitals and nutrition: See neuroprotective measures.
Complications
- Cerebral edema
- Post-concussion syndrome
- Coma
-
Seizures [55]
- Early post-traumatic seizure: occurs within one week of inciting trauma
- Late post-traumatic seizure: occurs a week after the inciting trauma
- Permanent focal neurological deficits, including persistent vegetative state
- Acute traumatic coagulopathy
- Chronic CSF rhinorrhea
- Intracranial infection (e.g., meningitis, encephalitis, brain abscess secondary to open head injury or neurosurgery) [56]
- Surgical site infections (e.g., bone flap osteomyelitis, shunt infections in patients who undergo neurosurgery) [57]
- Irreversible loss of brain function (brain death)
We list the most important complications. The selection is not exhaustive.
Paroxysmal sympathetic hyperactivity (PSH)
Definition
- A complication of acute brain injury characterized by recurrent episodes of excessive sympathetic activity.
Pathophysiology
- Loss of cortical inhibition of the sympathetic system subsequent to acute brain injury → exaggerated sympathetic response to stimulation
Causes
- Traumatic brain injury (most common)
- Anoxic brain injury
- Stroke
- Patient repositioning or extraction of endotracheal tube
- Brain tumors
- Infections (e.g., encephalitis)
- Hydrocephalus
Clinical features
- Usually occur 1 week after the injury
- Recurrent episodes of excessive sympathetic activity (e.g., fever, tachycardia, tachypnea, hypertension)
- Rapid onset; typically last up to 30 minutes then self-resolve
- Muscle spasms and, possibly, dystonia with posturing
Diagnostics
- Clinical diagnosis
- EEG and imaging (head CT/MRI) to rule out other conditions
Treatment [58]
- Supportive care (e.g., antipyretics for fever, adequate hydration, analgesia, remove or reduce stimuli that may trigger symptoms)
- Pharmacological
- Depends on patient symptoms
- Abortive and preventive agents
- Opioids (e.g., morphine, fentanyl)
- Sympatholytics (e.g., clonidine, propranolol)
- Benzodiazepines (e.g., diazepam, lorazepam)
- Muscle relaxants (e.g., dantrolene, baclofen)
References: [59][60]
Prognosis
- Mild TBI: Most (80–90%) patients make a full recovery within 2 weeks [23][61]
-
Moderate TBI [24][62]
- 90% patients improve but ∼ 44% have moderate disability.
- 10% deteriorate to severe TBI.
- Severe TBI: mortality rate of approx. 35% [63]
Special patient groups
When evaluating children and infants with TBI, a number of special issues must be observed.
-
Causes
- Falls (most common)
- The possibility of physical child abuse must always be considered.
- Clinical features: : esp. bulging anterior fontanelle (↑ ICP)
-
Diagnosis: cranial CT without contrast
- Identify patients with significant TBI but avoid unnecessary radiographic testing
- CT recommended for signs of skull fractures, ↑ ICP, major neurologic symptoms (e.g., impaired consciousness, seizures), suspected child abuse
- Consider CT: if less severe symptoms (e.g., changes in behavior, self-limited vomiting) are present.
- See also “Criteria for neuroimaging in children with mTBI.”
-
Management
-
Inpatient observation indications
- Skull fracture > 3 mm separation or depressed
- Evidence of traumatic brain injury on imaging (e.g.., intracranial hemorrhage)
- Signs of ↑ ICP (e.g., headache, altered mental status)
- Suspected physical child abuse
- Caregivers who are unreliable or unable to return if neurological deficits develop within 24 hours after release.
-
Release and at-home observation for 24 hours
- Patients without neurological deficits and non-depressed linear skull fracture < 3 mm separation
- Requires a caregiver who can reliably recognize new clinical neurological deficits and return the patient to the hospital if such manifestations arise
- See also “C-spine injuries in children.”
-
Inpatient observation indications
References:[64][65]
Overview of common brain lesions
| Overview of common brain lesions | ||||
|---|---|---|---|---|
| Location of lesion | Clinical features | |||
| Cortex | Frontal lobe |
|
||
| Frontal eye fields |
|
|||
| Parietal lobe |
|
|||
| Occipital lobe |
|
|||
| Temporal lobe |
|
|||
| Watershed border-zone |
|
|||
| Posterior limb of the internal capsule |
|
|||
| Thalamus |
|
|||
| Basal ganglia | Putamen |
|
||
| Substantia nigra |
|
|||
| Striatum |
|
|||
| Subthalamic nucleus |
|
|||
| Hippocampus (bilateral) |
|
|||
| Mammillary bodies (bilateral) |
|
|||
| Amygdala (bilateral) |
|
|||
| Medial longitudinal fasciculus |
|
|||
| Paramedian pontine reticular formation |
|
|||
| Dorsal midbrain |
|
|||
| Red nucleus |
|
|||
| Reticular activating system |
|
|||
| Cerebellum | General |
|
||
| Cerebellar vermis |
|
|||
| Cerebellar hemisphere |
|
|||
| Pons | Lateral spinothalamic tract |
|
||
| Middle and inferior cerebellar peduncles |
|
|||
| Spinal trigeminal nerve nucleus |
|
|||
| Facial nerve nuclei |
|
|||
| Vestibulocochlear nerve nuclei |
|
|||
| Sympathetic fibers |
|
|||
| Pyramidal tracts |
|
|||
| Abducens nerve |
|
|||
| Facial nerve |
|
|||
| Ventral pons |
|
|||
| Medulla oblongata | Nucleus and fibers of the hypoglossal nerve |
|
||
| Corticospinal tract |
|
|||
| Medial lemniscus |
|
|||
| Nucleus ambiguus (CN IX, X, XI) |
|
|||
| Vestibular nuclei |
|
|||
| Lateral spinothalamic tract |
|
|||
| Spinal trigeminal nucleus |
|
|||
| Inferior cerebellar peduncle |
|
|||
| Sympathetic fibers |
|
|||
Discrete brain lesions are typically caused by nontraumatic events, especially hemorrhagic, embolic, and neoplastic processes.







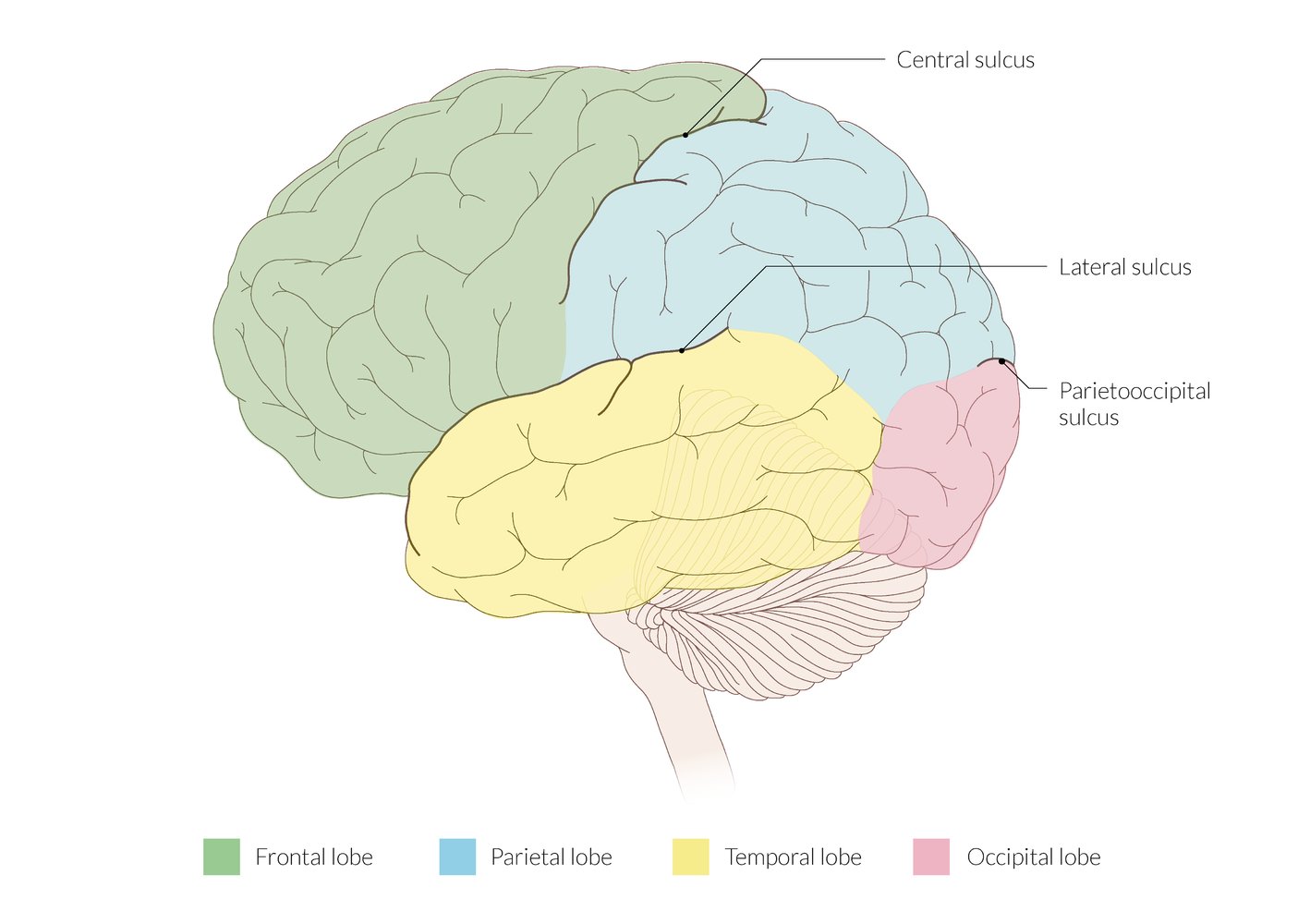
The 4 lobes of each cerebral hemisphere are separated by 3 main sulci:
–The central sulcus separates the frontal lobe from the parietal lobe.
–The lateral sulcus separates the temporal lobe from the frontal lobe and the parietal lobe.
–The parieto-occipital sulcus separates the parietal lobe from the occipital lobe.
© AMBOSS
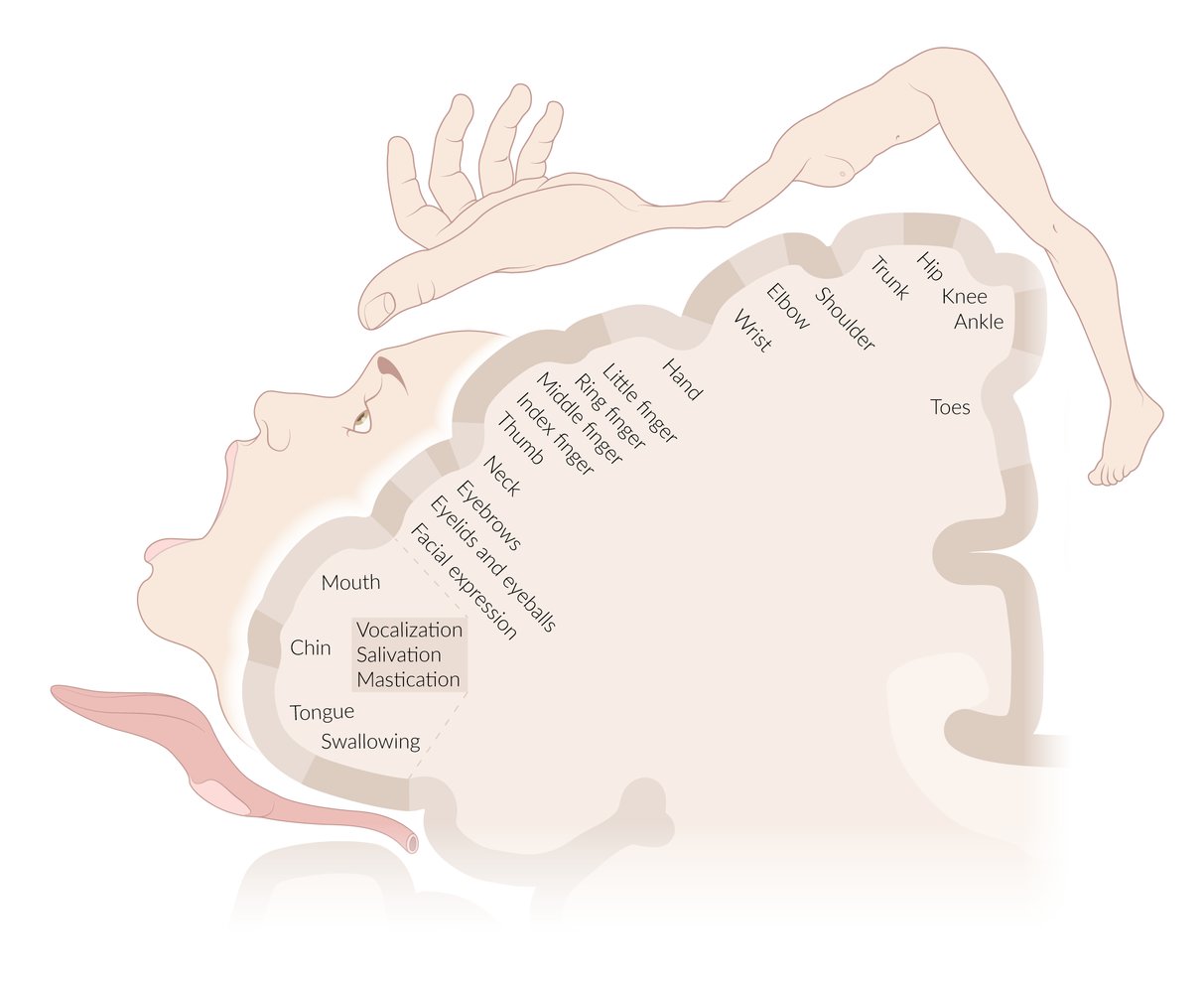
The motor homunculus is a map of the primary motor cortex (located in the precentral gyrus of the frontal lobes) that illustrates which areas of the brain process the motor output to which part of the body. The distorted representation of the body and the size of the correspondingly labeled cortical areas illustrate the proportional amount of motor output sent to the individual parts of the body. Accordingly, since areas like the tongue, face, and hands receive most motor innervation, these areas are represented as disproportionately large compared to other areas, like the trunk and lower limbs.
© AMBOSS
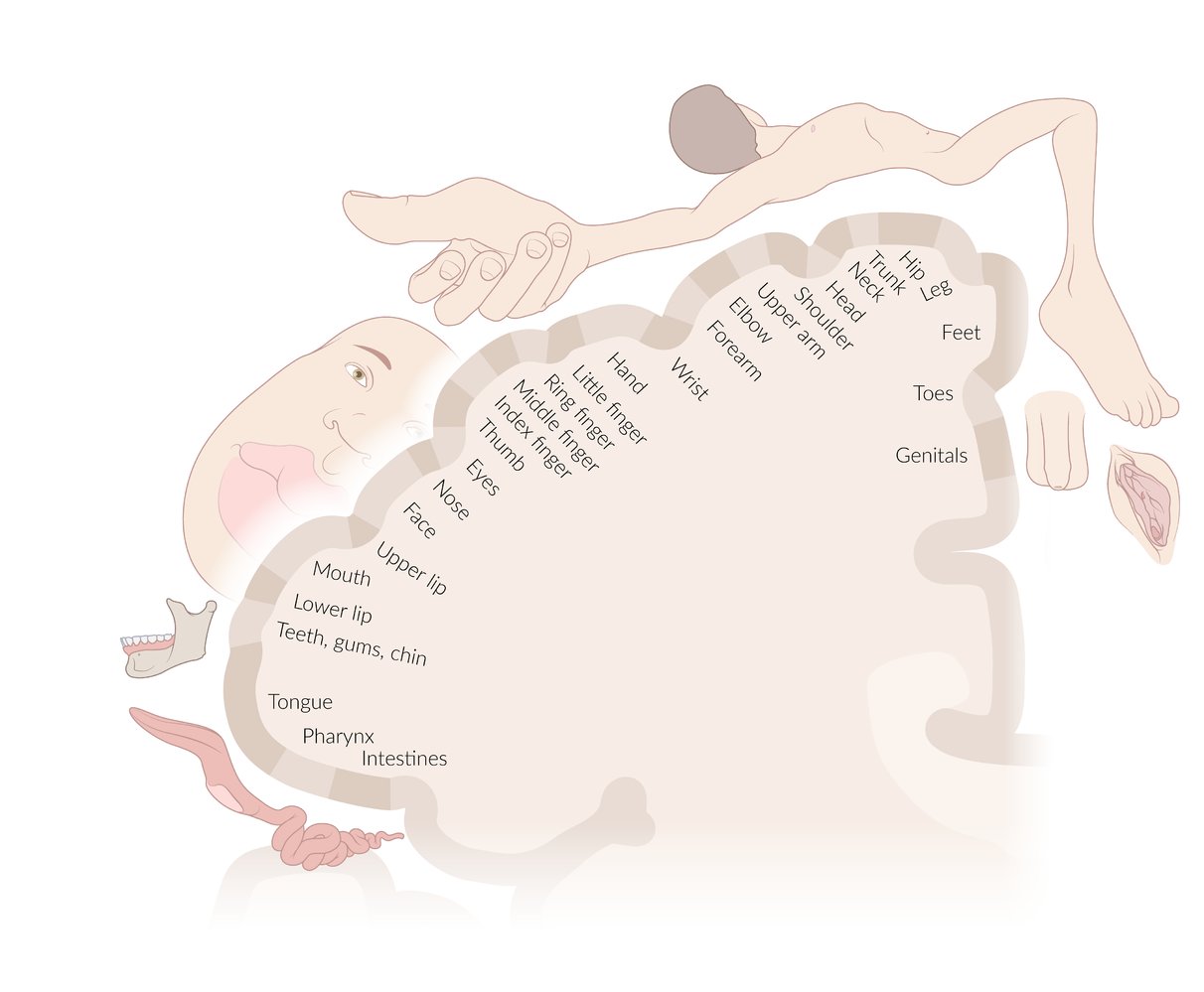
The sensory homunculus is a map of the primary somatosensory cortex (located in the postcentral gyrus of the parietal lobes) that illustrates which areas of the brain process the sensory input from which part of the body. The distorted representation of the body and the size of the correspondingly labeled cortical areas illustrate the proportional amount of sensory input received from the individual parts of the body. Accordingly, since the sensory nerves arriving from, e.g., the face and hands, terminate over larger areas of the brain than, e.g., those of the arms and legs, these parts of the body are represented as disproportionately large.
© AMBOSS
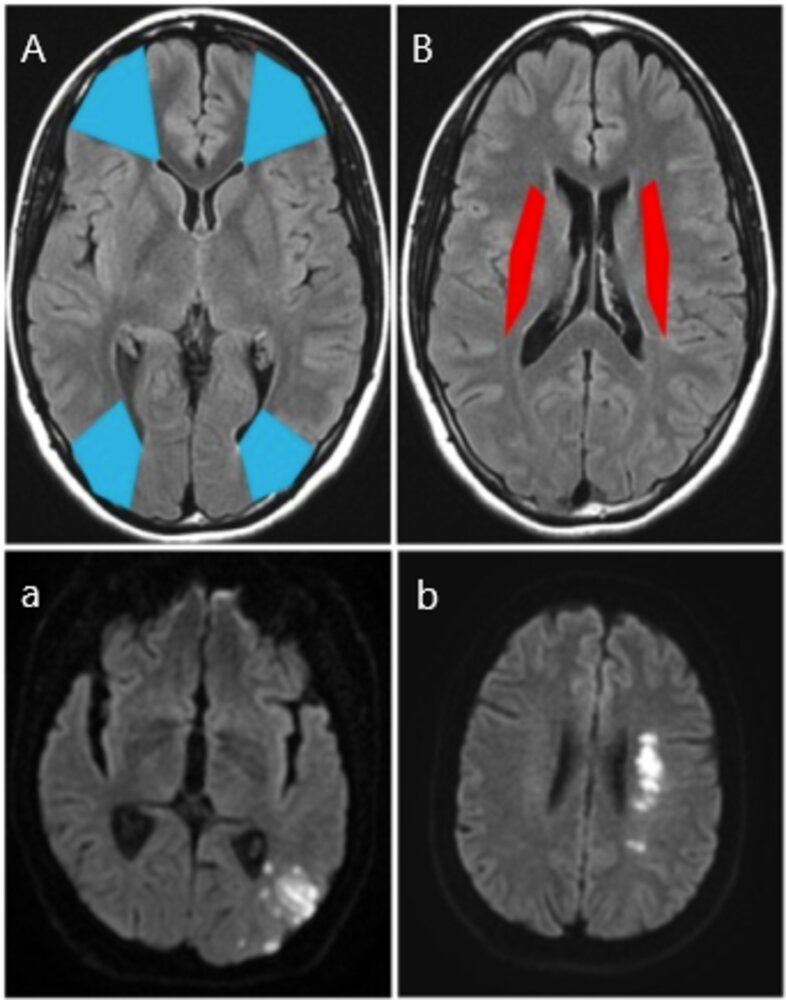
MRI head (A and B: FLAIR; a.and b.; DWI)
Cortical border zones, or watershed areas (A; blue), are located between the ACA and MCA territories and the PCA and MCA territories. A left occipital infarct (a; white) is shown at the boundary between the middle and posterior cerebral territories.
Internal border zones (B; red) are located between the superficial and deep branches of the MCA. A left internal watershed infarct (b; white) is shown.
FLAIR: fluid-attenuated inversion recovery; DWI: diffusion-weighted imaging; ACA: anterior cerebral artery; MCA: middle cerebral artery; PCA: posterior cerebral artery
Source: “Figure 1, in: Relationship between Watershed Infarcts and Recent Intra Plaque Haemorrhage in Carotid Atherosclerotic Plaque” by Isabel C et al., Plos One, licensed under CC BY 4.0. Modifications: Image cropped, labels changed.
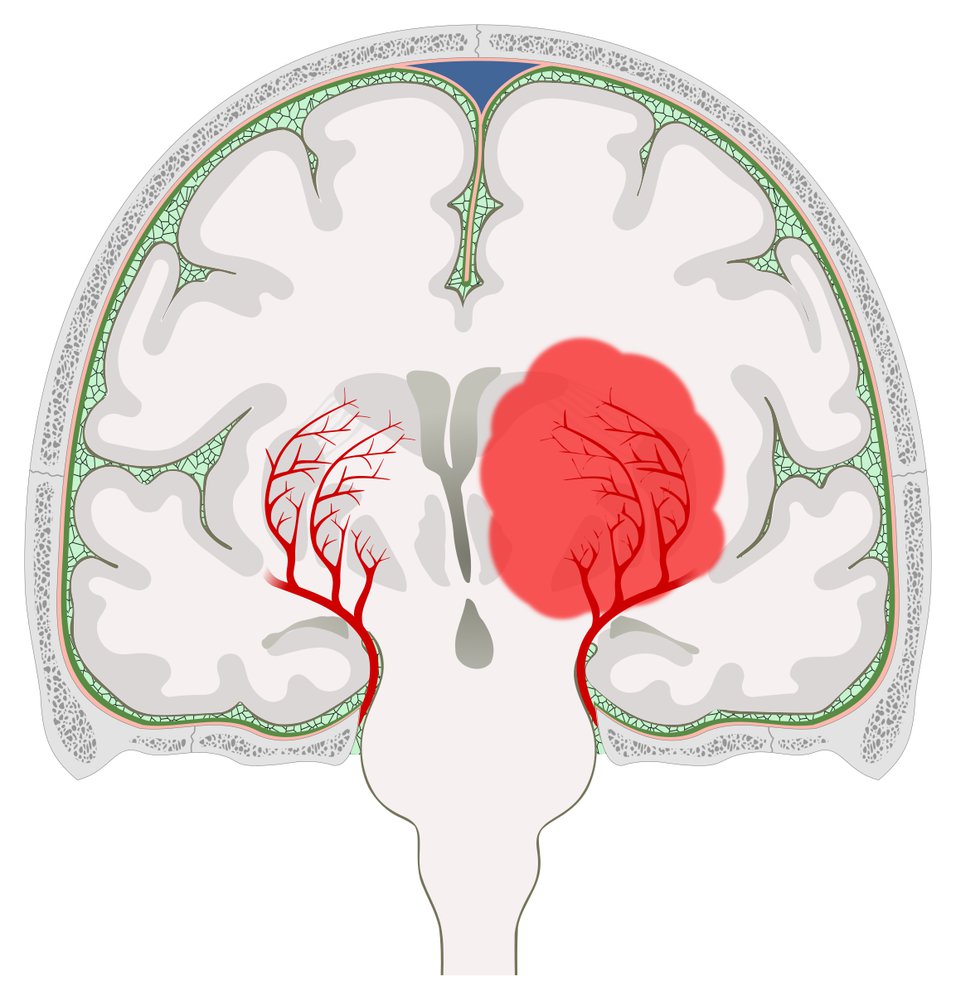
Hemorrhage in the region of the left basal ganglia causing a midline shift to the right
The basal ganglia are supplied by the lenticulostriate arteries, which arise from the middle cerebral artery. Hemorrhage from a lenticulostriate artery (e.g., due to poorly controlled hypertension or rupture of a Charcot-Bouchard microaneurysm) leads to a basal ganglia hemorrhage.
© AMBOSS
© AMBOSS
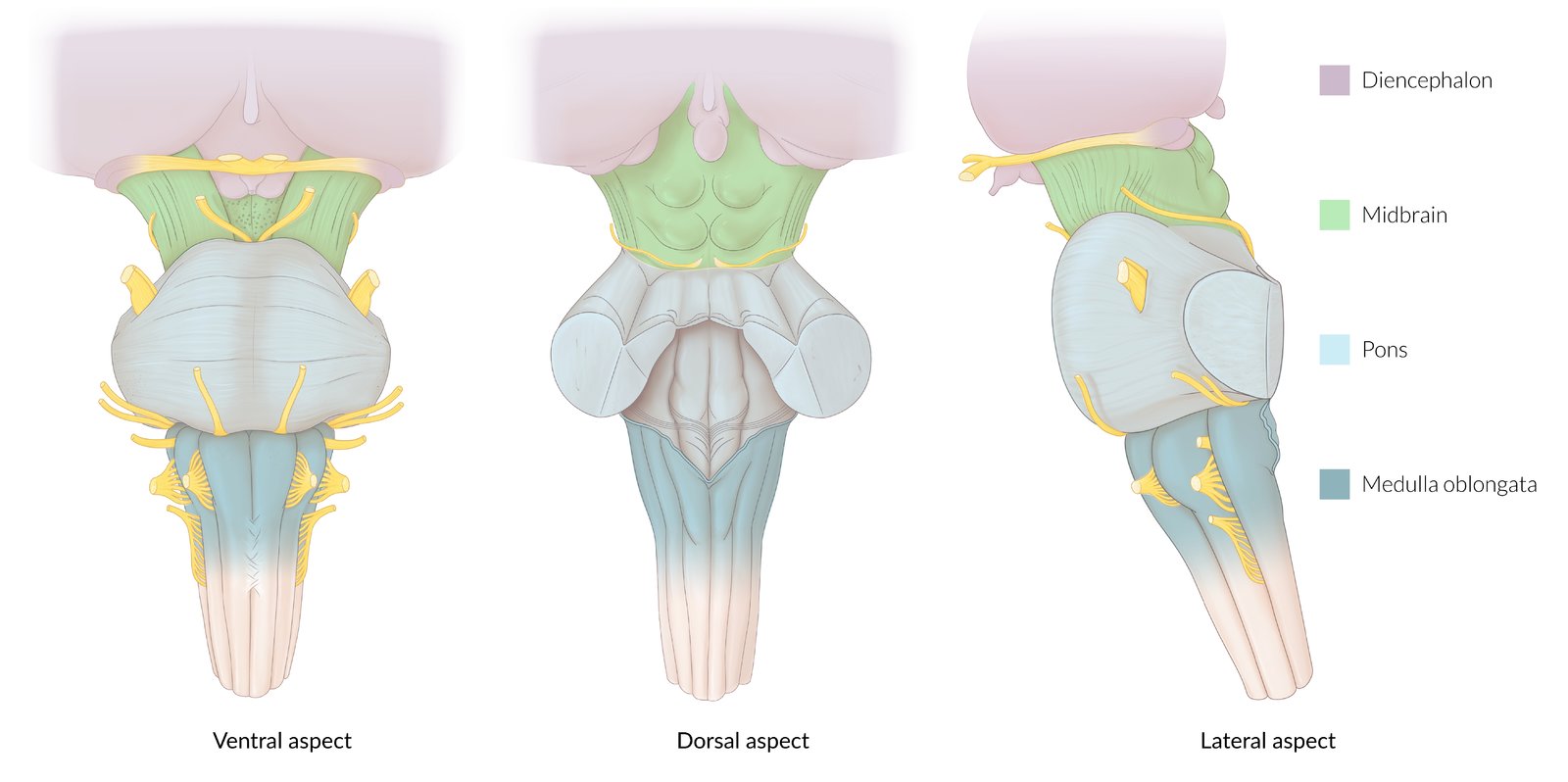
Ventral, dorsal, and lateral aspects of the brainstem (medulla oblongata, pons, midbrain) and the diencephalon. The points of entry/exit and course of various cranial nerves are shown as well.
© AMBOSS
Overview of intracranial hemorrhage
The following table focuses on traumatic causes of intracranial hemorrhage, which all have nontraumatic causes as well. See “Overview of stroke” for a comparison of nontraumatic cerebral ischemia and intracranial hemorrhage.
| Overview of intracranial hemorrhage | ||||
|---|---|---|---|---|
| Epidural hematoma | Subdural hematoma | Subarachnoid hemorrhage | Intracerebral hemorrhage | |
| Etiology |
|
|
|
|
| Characteristic clinical features |
|
|
|
|
| Typical findings on noncontrast CT head |
|
|
|
|
| Management |
|
|||
|
|
|
||




{kind=link}
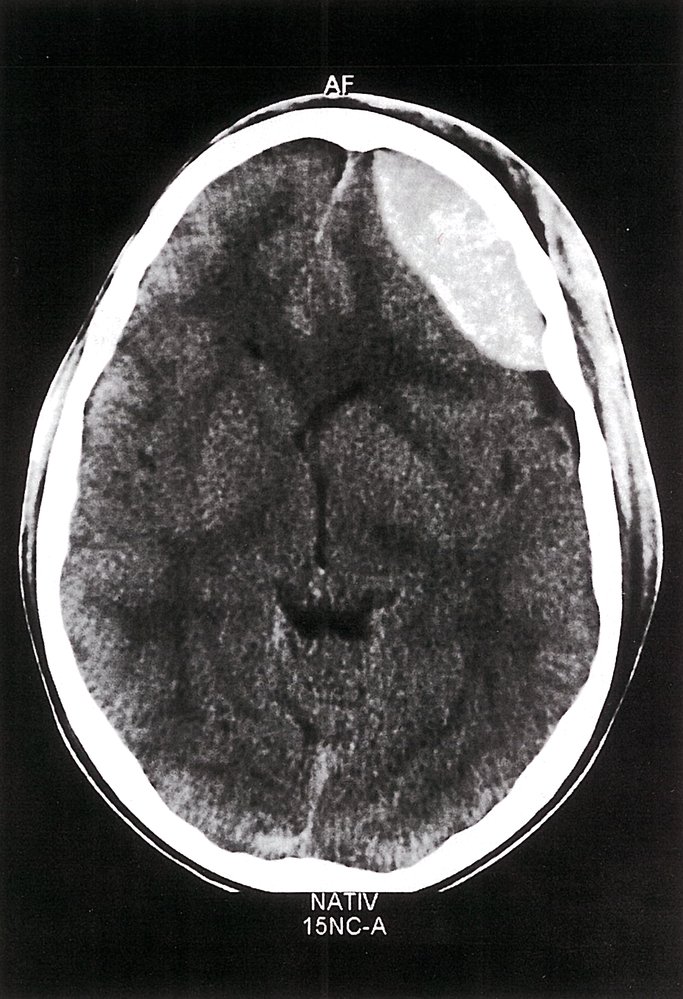
CT head (axial section; noncontrast)
An epidural hematoma is visible as a solitary biconvex hyperdense lesion in the left frontotemporal region (green overlay), causing a midline shift to the contralateral side (indicated by lines and arrows). The soft tissue of the scalp overlying the lesion also appears hyperdense, indicating a scalp hematoma (red overlay).
Source: © IMPP
CT head (without IV contrast; axial section; brain window)
There is a crescent-shaped, hyperdense lesion (green overlay) over the left cerebral hemisphere that crosses cranial sutures. There is a midline shift to the right (dotted line and arrows).
These findings are characteristic of an acute subdural hematoma.
Source: © IMPP
CT head (without contrast; axial plane)
A rounded area of high attenuation (1) in the left frontoparietal region indicates intracerebral hemorrhage from a ruptured left middle cerebral artery aneurysm. Extensive subarachnoid hemorrhage is present in the basal cisterns (2), interhemispheric fissure (3), right Sylvian fissure (4), left frontal lobe fissures (5), and posterior fossa (6). Ventricular dilatation (green overlay) is the result of obstruction of CSF drainage.
Source: © IMPP

CT head (without contrast; axial plane)
A large hyperdense hematoma (green overlay) in the posterior aspect of the left cerebral hemisphere is accompanied by hypodense edema (red overlay), effacement of the occipital horn of the left lateral ventricle, and midline shift (dashed line and arrowheads).
ROH: right occipital horn
Source: © IMPP
Related One-Minute Telegram
- One-Minute Telegram 106-2024-1/2: Liberal vs. restrictive transfusion strategy in traumatic brain injury
Interested in the newest medical research, distilled down to just one minute? Sign up for the One-Minute Telegram in “Tips and links” below.
External Resources
- One-Minute Telegram
- 2020 ACR Appropriateness Criteria for Imaging in Head Trauma
- 2016 Brain Trauma Foundation Guidelines for severe TBI (Fourth Edition)
- 2015 NCS Recommendations for the Management of Devastating Brain Injury
- 2015 NCS/SCCM Guideline for Reversal of Antithrombotics in ICH
- 2010 EAST Guidelines for the Management of BCVI
- 2014 Summary Statement of the International Consensus Conference on Monitoring in Neurocritical Care
References
- Menon DK, Schwab K, Wright DW, Maas AI. "Position Statement: Definition of Traumatic Brain Injury". Arch Phys Med Rehabil. 91(11). :1637-1640. (2010)
- Abdelmalik PA, Draghic N, Ling GSF. "Management of moderate and severe traumatic brain injury". Transfusion (Paris). 59(S2). :1529-1538. (2019)
- AAOS). "Advanced Assessment and Treatment of Trauma". Jones & Bartlett Learning. (2009). ISBN: 9780763751319
- "CDC Surveillance Report of Traumatic Brain Injury-related Emergency Department Visits, Hospitalizations, and Deaths—United States, 2014."
- Kazim SF, Shamim MS, Tahir MZ, Enam SA, Waheed S. "Management of penetrating brain injury.". Journal of emergencies, trauma, and shock. 4(3). :395-402. (2011)
- Harrington BM, Gretschel A, Lombard C, Lonser RR, Vlok AJ. "Complications, outcomes, and management strategies of non-missile penetrating head injuries". J Neurosurg. :1-9. (2020)
- Savitri QM, Putri CP, Gunawan KJ, et al. "Localized asymptomatic cerebellar abscess after penetrating brain injury by wooden foreign object with adequate antibiotics administration: A case report". International Journal of Surgery Case Reports. 72. :85-90. (2020)
- Wolf SJ, Bebarta VS, Bonnett CJ, Pons PT, Cantrill SV. "Blast injuries". The Lancet. 374(9687). :405-415. (2009)
- Teasdale G, Jennett B. "Assessment of coma and impaired consciousness. A practical scale.". Lancet (London, England). 2(7872). :81-4. (1974)
- Hoffer ME, Balaban C. "Neurosensory Disorders in Mild Traumatic Brain Injury". Academic Press. (2019). ISBN: 9780128123447
- Teasdale G, Maas A, Lecky F, et al. "The Glasgow Coma Scale at 40 years: standing the test of time.". The Lancet. Neurology. 13(8). :844-54. (2014)
- Saatman KE, Duhaime A-C, Bullock R, et al. "Classification of Traumatic Brain Injury for Targeted Therapies". J Neurotrauma. 25(7). :719-738. (2008)
- American College of Surgeons and the Committee on Trauma. "ATLS Advanced Trauma Life Support". American College of Surgeons. (2018). ISBN: 9780996826235
- Ahmed HM, Aquina CT, Gracias VH, et al. "Decorticate/Decerebrate Posturing". Springer Berlin Heidelberg. :674-676. (2012). ISBN: 9783642004179
- Bateman DE. "Neurological assessment of coma.". J Neurol Neurosurg Psychiatry. 71 Suppl 1. :i13-7. (2001)
- Ernst A, Herzog M, Seidl RO. "Head and Neck Trauma". Georg Thieme Verlag. (2006). ISBN: 9783131400017
- Ellenbogen RG, Abdulrauf SI, Sekhar LN. "Principles of Neurological Surgery E-Book". Elsevier Health Sciences. (2012). ISBN: 9781455727674
- Watanabe K, Kida W. "Images in clinical medicine: Battle's sign". N Engl J Med. 367(12). :1135. (2012)
- Walls R, Hockberger R, Gausche-Hill M. "Rosen's Emergency Medicine". Elsevier Health Sciences. (2018). ISBN: 9780323354790
- Lolli V, Pezzullo M, Delpierre I, Sadeghi N. "MDCT imaging of traumatic brain injury". Br J Radiol. 89(1061). :20150849. (2016)
- Shetty VS, Reis MN, et al. "ACR Appropriateness Criteria Head Trauma". Journal of the American College of Radiology. (2015)
- Borg J, Holm L, Cassidy JD, et al. "Diagnostic procedures in mild traumatic brain injury: results of the who collaborating centre task force on mild traumatic brain injury". Journal of Rehabilitation Medicine. 36. :61-75. (2004)
- Holly LT, Kelly DF, Counelis GJ, et al. "Cervical spine trauma associated with moderate and severe head injury: incidence, risk factors, and injury characteristics". J Neurosurg. 96(3). :285-291. (2002)
- The CRASH-3 trial collaborators. "Effects of tranexamic acid on death, disability, vascular occlusive events and other morbidities in patients with acute traumatic brain injury (CRASH-3): a randomised, placebo-controlled trial". The Lancet. 394(10210). :1713-1723. (2019)
- Slomski A. "Tranexamic Acid Improves Outcomes in TBI". JAMA. 322(24). :2375. (2019)
- Zehtabchi S, Abdel Baki SG, Falzon L, Nishijima DK. "Tranexamic acid for traumatic brain injury: a systematic review and meta-analysis.". Am J Emerg Med. 32(12). :1503-9. (2014)
- Lawati KA, Sharif S, Maqbali SA, et al. "Efficacy and safety of tranexamic acid in acute traumatic brain injury: a systematic review and meta-analysis of randomized-controlled trials". Intensive Care Med. 47(1). :14-27. (2020)
- Maas AIR, Steyerberg EW, Citerio G. "Tranexamic acid in traumatic brain injury: systematic review and meta-analysis trumps a large clinical trial?". Intensive Care Med. 47(1). :74-76. (2020)
- Kaups KL, Davis JW, Parks SN. "Routinely repeated computed tomography after blunt head trauma: does it benefit patients?". J Trauma. 56(3). :475-80; discussion 480-1. (2004)
- Connon FF, Namdarian B, Ee JL, Drummond KJ, Miller JA. "Do routinely repeated computed tomography scans in traumatic brain injury influence management? A prospective observational study in a level 1 trauma center.". Ann Surg. 254(6). :1028-31. (2011)
- Brown CV, Zada G, Salim A, et al. "Indications for routine repeat head computed tomography (CT) stratified by severity of traumatic brain injury.". J Trauma. 62(6). :1339-44; discussion 1344-5. (2007)
- Carney N, Totten AM, O’Reilly C, et al. "Guidelines for the Management of Severe Traumatic Brain Injury, Fourth Edition". Neurosurgery. 80(1). :6-15. (2016)
- Yerram S, Katyal N, Premkumar K, Nattanmai P, Newey CR. "Seizure prophylaxis in the neuroscience intensive care unit". Journal of Intensive Care. 6(1). :17. (2018)
- Englander J, Cifu DX, Diaz-Arrastia R. "Information/education page. Seizures and traumatic brain injury.". Arch Phys Med Rehabil. 95(6). :1223-4. (2014)
- Lin C, Zhao X, Sun H. "Analysis on the risk factors of intracranial infection secondary to traumatic brain injury". Chinese Journal of Traumatology. 18(2). :81-83. (2015)
- Kourbeti IS, Vakis AF, Papadakis JA, et al. "Infections in traumatic brain injury patients". Clinical Microbiology and Infection. 18(4). :359-364. (2012)
- Dawodu ST. "Traumatic Brain Injury (TBI): Definition and Pathophysiology". WebMD. http://emedicine.medscape.com/article/326510. [2015-09-22]
- Hemphill JC III. "Traumatic brain injury: Epidemiology, classification, and pathophysiology". UpToDate. UpToDate. https://www.uptodate.com/contents/traumatic-brain-injury-epidemiology-classification-and-pathophysiology. [2016-11-08]
- "Report to Congress: Traumatic Brain Injury In the United States: Epidemiology and Rehabilitation"
- Kinoshita K. "Traumatic brain injury: pathophysiology for neurocritical care". Journal of Intensive Care. 4(1). (2016)
- V. Schapira AH. "Neurology and Clinical Neuroscience E-Book". Elsevier Health Sciences. (2006). ISBN: 9780323070539
- Rincon S, Gupta R, Ptak T. "Imaging of head trauma". Elsevier. :447-477. (2016). ISBN: 9780444534859
- Lerner JT, Giza CC. "Traumatic Brain Injury in Children". Elsevier. :781-793. (2017). ISBN: 9780323371018
- McCrory P, Meeuwisse WH, Aubry M, et al. "Consensus statement on concussion in sport: the 4th International Conference on Concussion in Sport held in Zurich, November 2012". Br J Sports Med. 47(5). :250-258. (2013)
- Einarsen CE, van der Naalt J, Jacobs B, et al. "Moderate Traumatic Brain Injury: Clinical Characteristics and a Prognostic Model of 12-Month Outcome". World Neurosurgery. 114. :e1199-e1210. (2018)
- Prabhakaran K, Petrone P, Lombardo G, et al. "Mortality rates of severe traumatic brain injury patients: impact of direct versus nondirect transfers.". J Surg Res. 219. :66-71. (2017)
- Schutzman S. "Minor head trauma in infants and children: Evaluation". UpToDate. UpToDate. https://www.uptodate.com/contents/minor-head-trauma-in-infants-and-children-evaluation. [2016-07-20]
- Eiff MP, Hatch RL. "Fracture Management for Primary Care Updated Edition E-Book". Elsevier Health Sciences. (2017). ISBN: 9780323548458
- Rabinstein AA, Benarroch EE. "Treatment of paroxysmal sympathetic hyperactivity". Curr Treat Options Neurol. 10(2). :151-157. (2008)
- Meyer K. "Understanding paroxysmal sympathetic hyperactivity after traumatic brain injury". Surgical Neurology International. 5(14). :490. (2014)
- Totikov A, Boltzmann M, Schmidt SB, Rollnik JD. "Influence of paroxysmal sympathetic hyperactivity (PSH) on the functional outcome of neurological early rehabilitation patients: a case control study". BMC Neurol. 19(1). (2019)
- Bullock MR, Chesnut R, Ghajar J, et al. "Surgical Management of Acute Subdural Hematomas". Neurosurgery. 58(suppl_3). :S2-16-S2-24. (2006)
- Van Gijn J, Rinkel GJE. "Subarachnoid haemorrhage: diagnosis, causes and management". Brain. 124(2). :249-278. (2001)
- Quigley MR, Chew BG, Swartz CE, Wilberger JE. "The clinical significance of isolated traumatic subarachnoid hemorrhage". J Trauma Acute Care Surg. 74(2). :581-584. (2013)
- Vella MA, Crandall ML, Patel MB. "Acute Management of Traumatic Brain Injury". Surg Clin North Am. 97(5). :1015-1030. (2017)
- Hatchimonji JS, Dumas RP, Kaufman EJ, et al. "Questioning dogma: does a GCS of 8 require intubation?". Eur J Trauma Emerg Surg. (2020)
- Thompson M, McIntyre L, Hutton B, et al. "Comparison of crystalloid resuscitation fluids for treatment of acute brain injury: a clinical and pre-clinical systematic review and network meta-analysis protocol". Systematic Reviews. 7(1). (2018)
- Mistri AK, Robinson TG, Potter JF. "Pressor Therapy in Acute Ischemic Stroke". Stroke. 37(6). :1565-1571. (2006)
- Robertson CS, Hannay HJ, Yamal J-M, et al. "Effect of Erythropoietin and Transfusion Threshold on Neurological Recovery After Traumatic Brain Injury". JAMA. 312(1). :36. (2014)
- Hébert PC, Wells G, Blajchman MA, et al. "A Multicenter, Randomized, Controlled Clinical Trial of Transfusion Requirements in Critical Care". N Engl J Med. 340(6). :409-417. (1999)
- Stolla M, Zhang F, Meyer MR, Zhang J, Dong J. "Current state of transfusion in traumatic brain injury and associated coagulopathy". Transfusion (Paris). 59(S2). :1522-1528. (2019)
- Lelubre C, Bouzat P, Crippa IA, Taccone FS. "Anemia management after acute brain injury". Critical Care. 20(1). (2016)
- Rangel-Castilla L, Gopinath S, Robertson CS. "Management of intracranial hypertension.". Neurol Clin. 26(2). :521-41, x. (2008)
- Frontera JA, Lewin III JJ, Rabinstein AA, et al. "Guideline for Reversal of Antithrombotics in Intracranial Hemorrhage". Neurocrit Care. 24(1). :6-46. (2015)
- Le Roux P, Menon DK, Citerio G, et al. "Consensus Summary Statement of the International Multidisciplinary Consensus Conference on Multimodality Monitoring in Neurocritical Care". Neurocrit Care. 21(S2). :1-26. (2014)
- Albrecht JS, Liu X, Baumgarten M, et al. "Benefits and Risks of Anticoagulation Resumption Following Traumatic Brain Injury". JAMA Internal Medicine. 174(8). :1244. (2014)
- Puckett Y, Zhang K, Blasingame J, et al. "Safest Time to Resume Oral Anticoagulation in Patients with Traumatic Brain Injury.". Cureus. 10(7). :e2920. (2018)
- Kaufman RM, Djulbegovic B, Gernsheimer T. "Platelet Transfusion: A Clinical Practice Guideline From the AABB". Ann Intern Med. 162(3). :205-213. (2015)
- Hemphill JC, Greenberg SM, Anderson CS et al. "Guidelines for the Management of Spontaneous Intracerebral Hemorrhage". Stroke. 46(7). (2015)
- Qureshi AI, Palesch YY, Barsan WG, et al. "Intensive Blood-Pressure Lowering in Patients with Acute Cerebral Hemorrhage". N Engl J Med. 375(11). :1033-1043. (2016)
- Fomchenko EI, Gilmore EJ, Matouk CC, Gerrard JL, Sheth KN. "Management of Subdural Hematomas: Part I. Medical Management of Subdural Hematomas". Curr Treat Options Neurol. 20(8). (2018)
- Mild Traumatic Brain Injury Committee of the Head Injury Interdisciplinary Special Interest Group of the American Congress of Rehabilitation Medicine. "Definition of mild traumatic brain injury". J Head Trauma Rehabil. 8(3). :86-87. (1993)
- McInnes K, Friesen CL, MacKenzie DE, Westwood DA, Boe SG. "Mild Traumatic Brain Injury (mTBI) and chronic cognitive impairment: A scoping review". PLoS ONE. 12(4). :e0174847. (2017)
- Bullock MR, Chesnut R, Ghajar J, et al. "Guidelines for the Surgical Management of Traumatic Brain Injury Author Group". Neurosurgery. 58(3). :S2-vi-S2-vi. (2006)
- Crompton EM, Lubomirova I, Cotlarciuc I, et al. "Meta-Analysis of Therapeutic Hypothermia for Traumatic Brain Injury in Adult and Pediatric Patients". Crit Care Med. 45(4). :575-583. (2017)
- Andrews PJ, Sinclair HL, Rodríguez A, et al. "Therapeutic hypothermia to reduce intracranial pressure after traumatic brain injury: the Eurotherm3235 RCT". Health Technol Assess (Rockv). 22(45). :1-134. (2018)
- Watson HI, Shepherd AA, Rhodes JKJ, Andrews PJD. "Revisited: A Systematic Review of Therapeutic Hypothermia for Adult Patients Following Traumatic Brain Injury". Crit Care Med. 46(6). :972-979. (2018)
- Nyquist P, Bautista C, Jichici D, et al. "Prophylaxis of Venous Thrombosis in Neurocritical Care Patients: An Evidence-Based Guideline: A Statement for Healthcare Professionals from the Neurocritical Care Society". Neurocrit Care. 24(1). :47-60. (2015)
- Souter MJ, Blissitt PA, Blosser S, et al. "Recommendations for the Critical Care Management of Devastating Brain Injury: Prognostication, Psychosocial, and Ethical Management". Neurocrit Care. 23(1). :4-13. (2015)
- Krishnamoorthy V, Chaikittisilpa N, Kiatchai T, Vavilala M. "Hypertension After Severe Traumatic Brain Injury". J Neurosurg Anesthesiol. 29(4). :382-387. (2017)
- Paiva W, de Andrade AF, MONACO, et al. "Serum sodium disorders in patients with traumatic brain injury". Ther Clin Risk Manag. :345. (2011)
- Ratilal BO, Costa J, Pappamikail L, Sampaio C. "Antibiotic prophylaxis for preventing meningitis in patients with basilar skull fractures". Cochrane Database of Systematic Reviews. 4. :CD004884. (2015)
- Winn HR. "Youmans and Winn Neurological Surgery". Elsevier. (2016). ISBN: 9780323287821
- Brommeland T, Helseth E, Aarhus M, et al. "Best practice guidelines for blunt cerebrovascular injury (BCVI)". Scand J Trauma Resusc Emerg Med. 26(1). :90. (2018)
- Bromberg WJ, Collier BC, Diebel LN, et al. "Blunt cerebrovascular injury practice management guidelines: the Eastern Association for the Surgery of Trauma.". J Trauma. 68(2). :471-7. (2010)
- Franz RW, Willette PA, Wood MJ, Wright ML, Hartman JF. "A Systematic Review and Meta-Analysis of Diagnostic Screening Criteria for Blunt Cerebrovascular Injuries". J Am Coll Surg. 214(3). :313-327. (2012)
- Harmon LA, Haase DJ, Kufera JA, et al. "Infection after penetrating brain injury". Journal of Trauma and Acute Care Surgery. 87(1). :61-67. (2019)
- Rosenfeld JV, Bell RS, Armonda R. "Current Concepts in Penetrating and Blast Injury to the Central Nervous System". World J Surg. 39(6). :1352-1362. (2014)
- Aarabi B, Alden TD, Chesnut R, et al. "Guidelines for the management of penetrating brain injury". J Trauma. 51(2 Suppl). :S34-40. (2001)
- Lee B, Newberg A. "Neuroimaging in traumatic brain imaging.". NeuroRx. 2(2). :372-83. (2005)
- Lin DJ, Lam FC, Siracuse JJ, Thomas A, Kasper EM. ""Time is brain" the Gifford factor - or: Why do some civilian gunshot wounds to the head do unexpectedly well? A case series with outcomes analysis and a management guide". Surgical Neurology International. 3(1). :98. (2012)
- Wada R, Aviv RI, Fox AJ, et al. "CT Angiography “Spot Sign” Predicts Hematoma Expansion in Acute Intracerebral Hemorrhage". Stroke. 38(4). :1257-1262. (2007)
- Yang Y, Zheng F, Xu X, Wang X. "Levetiracetam Versus Phenytoin for Seizure Prophylaxis Following Traumatic Brain Injury: A Systematic Review and Meta-Analysis.". CNS Drugs. 30(8). :677-88. (2016)
- Xu JC, Shen J, Shao WZ, et al. "The safety and efficacy of levetiracetam versus phenytoin for seizure prophylaxis after traumatic brain injury: A systematic review and meta-analysis.". Brain injury. 30(9). :1054-61. (2016)
- Bakr A, Belli A. "A systematic review of levetiracetam versus phenytoin in the prevention of late post-traumatic seizures and survey of UK neurosurgical prescribing practice of antiepileptic medication in acute traumatic brain injury.". Br J Neurosurg. 32(3). :237-244. (2018)
- Abend NS, MD NS, Helfaer MA, MD MA. "Pediatric Neurocritical Care". Demos Medical Publishing. (2012). ISBN: 9781617050695
- Tahir R, Pabaney A. "Therapeutic hypothermia and ischemic stroke: A literature review". Surg Neurol Int. 7(15). :381. (2016)
- Lewis SR, Evans DJ, Butler AR, Schofield-Robinson OJ, Alderson P. "Hypothermia for traumatic brain injury". Cochrane Database Syst Rev. (2017)
- Klingbeil KD, Koch S, Dave KR. "Potential link between post-acute ischemic stroke exposure to hypoglycemia and hemorrhagic transformation". Int J Stroke. :174749301774379. (2017)
- Zhu C, Chen J, Pan J, Qiu Z, Xu T. "Therapeutic effect of intensive glycemic control therapy in patients with traumatic brain injury". Medicine. 97(30). :e11671. (2018)
- Madan A. "Correlation between the levels of SpO2 and PaO2.". Lung India. 34(3). :307-308. (2017)
- Spencer MP. "Ultrasonic Diagnosis of Cerebrovascular Disease". Springer Science & Business Media. (2012). ISBN: 9789400943056
- Nentwich LM, Jr BGM, Kahn JH. "Acute Ischemic Stroke, An Issue of Emergency Medicine Clinics - E-Book". Elsevier Health Sciences. (2012). ISBN: 9781455747627
- Elisha S, Nagelhout JJ, Heiner JS. "Current Anesthesia Practice - E-Book". Elsevier Health Sciences. (2019). ISBN: 9780323483858
- Besmertis, L; Bonovich, DC; and Hemphill, JC. "The Role of Hypotension in Secondary Brain Injury after Intracerebral Hemorrhage". Stroke. Vol 32, Issue suppl_1. :358. (2001)
- Appleton JP, Sprigg N, Bath PM. "Blood pressure management in acute stroke". BMJ. 1(2). :72-82. (2016)
- Moore AJ, Newell DW. "Tumor Neurosurgery". Springer Science & Business Media. (2010). ISBN: 9781846282942
- El-Fawal BM, Badry R, Abbas WA, Ibrahim AK. "Stress hyperglycemia and electrolytes disturbance in patients with acute cerebrovascular stroke". Egypt J Neurol Psychiatry Neurosurg. 55(1). (2019)
- Pin-on P, Saringkarinkul A, Punjasawadwong Y, Kacha S, Wilairat D. "Serum electrolyte imbalance and prognostic factors of postoperative death in adult traumatic brain injury patients". Medicine. 97(45). :e13081. (2018)
- Fisher M. "Stroke". Elsevier Health Sciences. (2009). ISBN: 9780444520043
- Frankenfield DC, Ashcraft CM. "Description and prediction of resting metabolic rate after stroke and traumatic brain injury". Nutrition. 28(9). :906-911. (2012)
- Wirth R, Smoliner C, et al. "Guideline clinical nutrition in patients with stroke". Exp Transl Stroke Med. 5(1). (2013)
- Perel P, Yanagawa T, Bunn F, Roberts IG, Wentz R. "Nutritional support for head-injured patients". Cochrane Database Syst Rev. (2006)
- Mazer L, Tapper EB, Piatkowski G, Lai M. "The need for antibiotic stewardship and treatment standardization in the care of cirrhotic patients with spontaneous bacterial peritonitis - a retrospective cohort study examining the effect of ceftriaxone dosing.". F1000Research. 3. :57. (2014)
- Levine Z. "Mild traumatic brain injury: part 1: determining the need to scan.". Can Fam Physician. 56(4). :346-9. (2010)
- Peng W-J, Reis C, Reis H, Zhang J, Yang J. "Predictive Value of CTA Spot Sign on Hematoma Expansion in Intracerebral Hemorrhage Patients". BioMed Research International. 2017. :1-9. (2017)
- Lascarrou J-B, Merdji H, Le Gouge A, et al. "Targeted Temperature Management for Cardiac Arrest with Nonshockable Rhythm". N Engl J Med. 381(24). :2327-2337. (2019)
- Bradshaw K, Smith M. "Disorders of sodium balance after brain injury". Continuing Education in Anaesthesia Critical Care & Pain. 8(4). :129-133. (2008)
- Saxena MK, Taylor C, Billot L, et al. "The Effect of Paracetamol on Core Body Temperature in Acute Traumatic Brain Injury: A Randomised, Controlled Clinical Trial.". PLoS ONE. 10(12). :e0144740. (2015)
- Kuczynski AM, Demchuk AM, Almekhlafi MA. "Therapeutic hypothermia: Applications in adults with acute ischemic stroke.". Brain circulation. 5(2). :43-54. (2019)
- Powers WJ, Rabinstein AA, Ackerson T, et al. "Guidelines for the Early Management of Patients With Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association". Stroke. 50(12). (2019)
- Zhang M, Wang H, Zhao J, et al. "Drug-induced hypothermia in stroke models: does it always protect?". CNS Neurol Disord Drug Targets. 12(3). :371-80. (2013)
- Yu S, Lee J, Zhang J. "Neuroprotective mechanisms and translational potential of therapeutic hypothermia in the treatment of ischemic stroke". Neural Regeneration Research. 12(3). :341. (2017)
- Sun YJ, Zhang ZY, Fan B, Li GY. "Neuroprotection by Therapeutic Hypothermia.". Frontiers in neuroscience. 13. :586. (2019)
- Kurisu K, Yenari MA. "Therapeutic hypothermia for ischemic stroke; pathophysiology and future promise". Neuropharmacology. 134. :302-309. (2018)
- Vavilala MS, Sharma D. "Neuroprotection with phenylephrine in traumatic brain injury". Crit Care Med. 40(8). :2515-2517. (2012)
- Feinstein AJ, Patel MB, Sanui M, et al. "Resuscitation with Pressors after Traumatic Brain Injury". J Am Coll Surg. 201(4). :536-545. (2005)
- Sookplung P, Siriussawakul A, Malakouti A, et al. "Vasopressor Use and Effect on Blood Pressure After Severe Adult Traumatic Brain Injury". Neurocrit Care. 15(1). :46-54. (2010)
- Chang JJ, Sanossian N. "Pre-Hospital Glyceryl Trinitrate: Potential for Use in Intracerebral Hemorrhage.". Journal of neurological disorders. 2(1). (2013)
- Rabinstein AA. "Optimal Blood Pressure After Intracerebral Hemorrhage". Stroke. 49(2). :275-276. (2018)
- Chu S, Sansing L. "Evolution of blood pressure management in acute intracerebral hemorrhage.". F1000Research. 6. :2035. (2017)
- Hill MD, Muir KW. "INTERACT-2". Stroke. 44(10). :2951-2952. (2013)
- Rostami E. "Glucose and the injured brain-monitored in the neurointensive care unit.". Frontiers in neurology. 5. :91. (2014)
- Haddad SH, Arabi YM. "Critical care management of severe traumatic brain injury in adults". Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine. 20(1). :12. (2012)
- Prince C, Bruhns ME. "Evaluation and Treatment of Mild Traumatic Brain Injury: The Role of Neuropsychology.". Brain sciences. 7(8). (2017)
- Sorrentino E, Diedler J, Kasprowicz M, et al. "Critical thresholds for cerebrovascular reactivity after traumatic brain injury.". Neurocrit Care. 16(2). :258-66. (2012)