Summary
Ulcerative colitis is a type of chronic inflammatory bowel disease (IBD) characterized by mucosal inflammation of the colon that typically starts in the rectum and may extend proximally affecting the distal colon or the entire colon up to the cecum. The most common clinical feature is bloody diarrhea, often accompanied by abdominal pain, fecal urgency, and tenesmus. Extraintestinal manifestations such as arthritis, uveitis, erythema nodosum, and primary sclerosing cholangitis can also occur. Diagnosis is confirmed by ileocolonoscopy with biopsy, while laboratory (e.g., ESR, CRP) and stool studies (e.g., fecal calprotectin) help assess disease severity. Treatment depends on disease severity, ranging from 5-ASA preparations for mild disease to systemic immunomodulatory medications for severe disease. Major complications include toxic megacolon, perforation, and an increased risk of colorectal cancer, which necessitates regular endoscopic screening. A restorative proctocolectomy is a curative surgical option for patients with refractory disease or complications.

© AMBOSS
Epidemiology
-
Prevalence
- Approx. 1.2 million adults in the US are affected by ulcerative colitis.[1]
- Ethnicity
- Higher in White populations than in Black, Hispanic, or Asian populations
- Highest among individuals of Ashkenazi Jewish descent
-
Incidence
- Peak incidence: 20–30 years of age [1]
- Another smaller peak may be observed in individuals > 55 years of age. [2]
- Childhood onset occurs in > 10% of patients; see “IBD in children.” [3]
- ♂=♀ [4]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
Risk factors [2][5][6]
- Genetic predisposition (e.g., HLA-B27 association)
- Ethnicity (White populations, individuals of Ashkenazi Jewish descent)
- Family history of inflammatory bowel disease
- History of intestinal infections
- Increased fat intake (especially saturated fat and animal fat)
- Oral contraceptive use
- NSAIDs may exacerbate ulcerative colitis.
Protective factors [5][6]
- Appendectomy
- Smoking
Classification
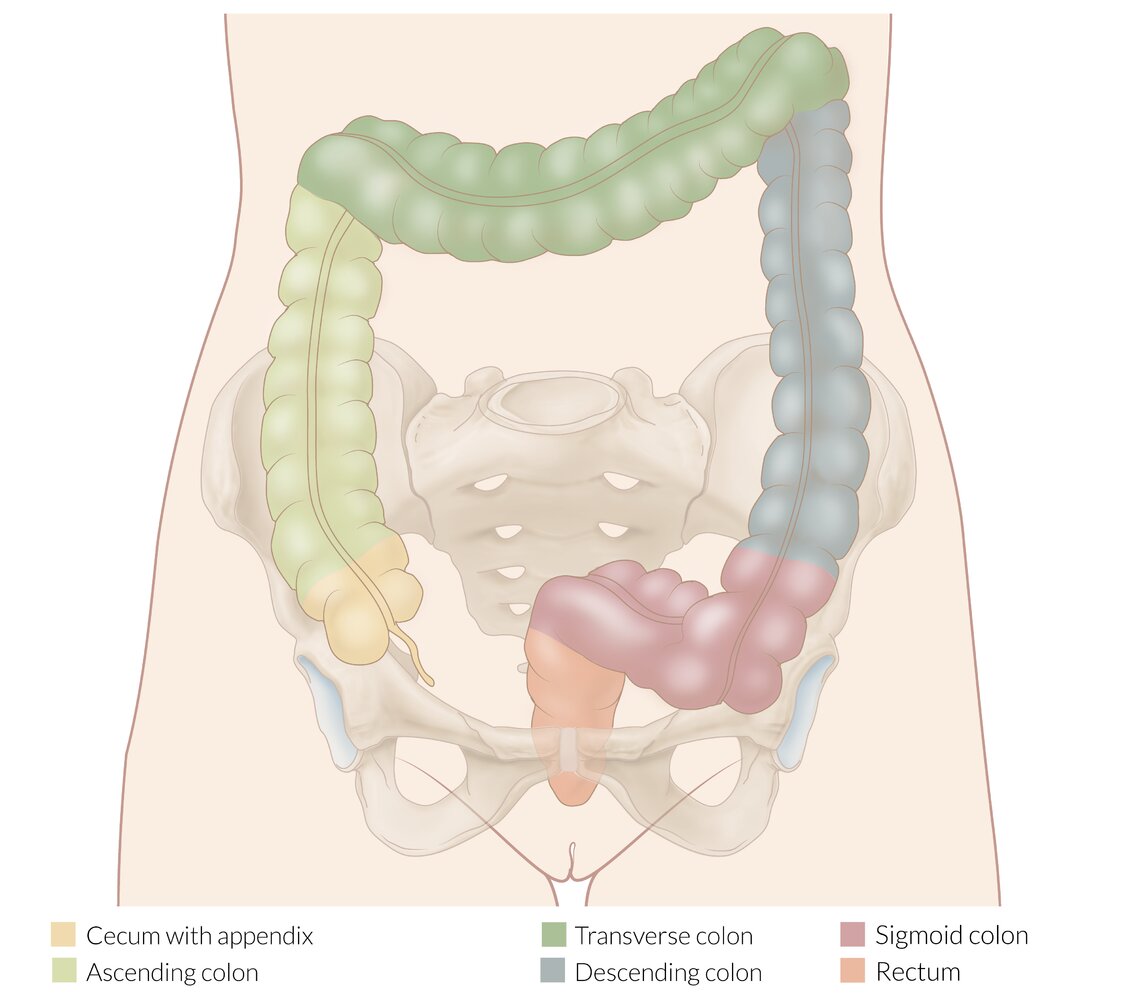
Classification of ulcerative colitis by disease extent [1]
The extent of disease is classified based on endoscopic findings.
| Montreal classification for the extent of ulcerative colitis [1] | ||
|---|---|---|
| Disease extent | Mucosal involvement | |
| Ulcerative proctitis (E1) | Limited to the rectum (≤ 15 cm) | |
| Left-sided ulcerative colitis (E2) | Limited to the colon distal to the splenic flexure | |
| Extensive ulcerative colitis (E3) | Extends proximal to the splenic flexure | |
Classification of ulcerative colitis by severity [1]
There are several classification systems that can be used to assess disease severity. There is significant overlap among the criteria used. Criteria include:
-
Endoscopic findings
- Ulcerative colitis endoscopic index of severity (UCEIS)
- Mayo endoscopic score (MES)
-
Clinical presentation
- Simple clinical colitis activity index (SCCAI)
- Truelove and Witts severity index for ulcerative colitis
-
A combination of both endoscopic findings and clinical presentation
- Mayo score for ulcerative colitis activity
- American College of Gastroenterology (ACG) ulcerative colitis activity index
- Other: response to medication, disease course, patient's quality of life
-
Remission (ACG ulcerative colitis activity index): all of the following [1]
- Absence of diarrhea, blood in stools, and fecal urgency
- Fecal calprotectin < 150–200 mcg/g; normal Hb, ESR and CRP [1]
- Normal endoscopy
| American College of Gastroenterology ulcerative colitis activity index [1] | |||
|---|---|---|---|
| Criteria | Severity of ulcerative colitis | ||
| Mild ulcerative | Moderate-to-severe | Fulminant | |
| Stools per day | < 4 | > 6 | > 10 |
| Frequency of blood in stool | Intermittent | Frequent | Continuous |
| Fecal urgency | Mild, occasional | Often | Continuous |
| Hemoglobin | Normal | < 75% of normal | Transfusion required |
| ESR | < 30 mm/hour | > 30 mm/hour | |
| CRP | Elevated | ||
| Fecal calprotectin | > 150–200 mcg/g | ||
| Mayo endoscopy score | 1 | 2–3 | 3 |
| Ulcerative colitis endoscopic index of severity | 2–4 | 5–8 | 7–8 |
| Truelove and Witts severity index [7][8] | ||
|---|---|---|
| Criteria | Mild | Severe |
| Bowel movements per day | ≤ 4 | ≥ 6 |
| Amount of blood in stool | Small amount | Macroscopic blood |
| Temperature | No fever | ≥ 37.8°C (≥ 100°F) |
| Heart rate | No tachycardia | > 90 bpm |
| Hemoglobin | No severe anemia | ≤ 75% of normal |
| ESR | ≤ 30 mm/hour | > 30 mm/hour |
Treatment recommendations by the ACG are based on their ulcerative colitis activity index, while recommendations by the American Gastroenterological Association (AGA) are based on the Truelove and Witts severity index and the Mayo score for ulcerative colitis activity.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
Pathophysiology
The exact mechanism is unknown but studies suggest that ulcerative colitis is caused by abnormal interactions between host immune cells and commensal bacteria. [5][6]
-
Dysregulation of intestinal epithelium: increased permeability for luminal bacteria → activation of macrophages and dendritic cells → antigen presentation to macrophages and naive CD4+ cells leads to:
- Secretion of proinflammatory cytokines (IL-6, IL-12, TNF-α) and chemokines (CXCL1, CXCL3, and CXCL8) → recruitment of other immune cells (e.g., neutrophils) to the site
- Differentiation of naive CD4+ cells to Th2 effector cells
- Recruitment of natural killer cells
-
Dysregulation of the immune system: upregulation of lymphatic cell activity (T cells, B cells, plasma cells) in bowel walls → enhanced immune reaction and cytotoxic effect on colonic epithelium → inflammation with local tissue damage (ulcerations, erosions, necrosis) in the submucosa and mucosa
- Autoantibodies (pANCA) against cells of the intestinal epithelium
- Th2 cell-mediated response
-
Pattern of involvement
- Ascending inflammation that begins in the rectum and spreads continuously proximally throughout the colon
- Inflammation is limited to the mucosa and submucosa.
The rectum is always involved in ulcerative colitis.
© AMBOSS
Clinical features
Intestinal features
- Bloody diarrhea with mucus (hematochezia)
- Fecal urgency
- Increased stool frequency
- Abdominal pain and cramps
- Tenesmus
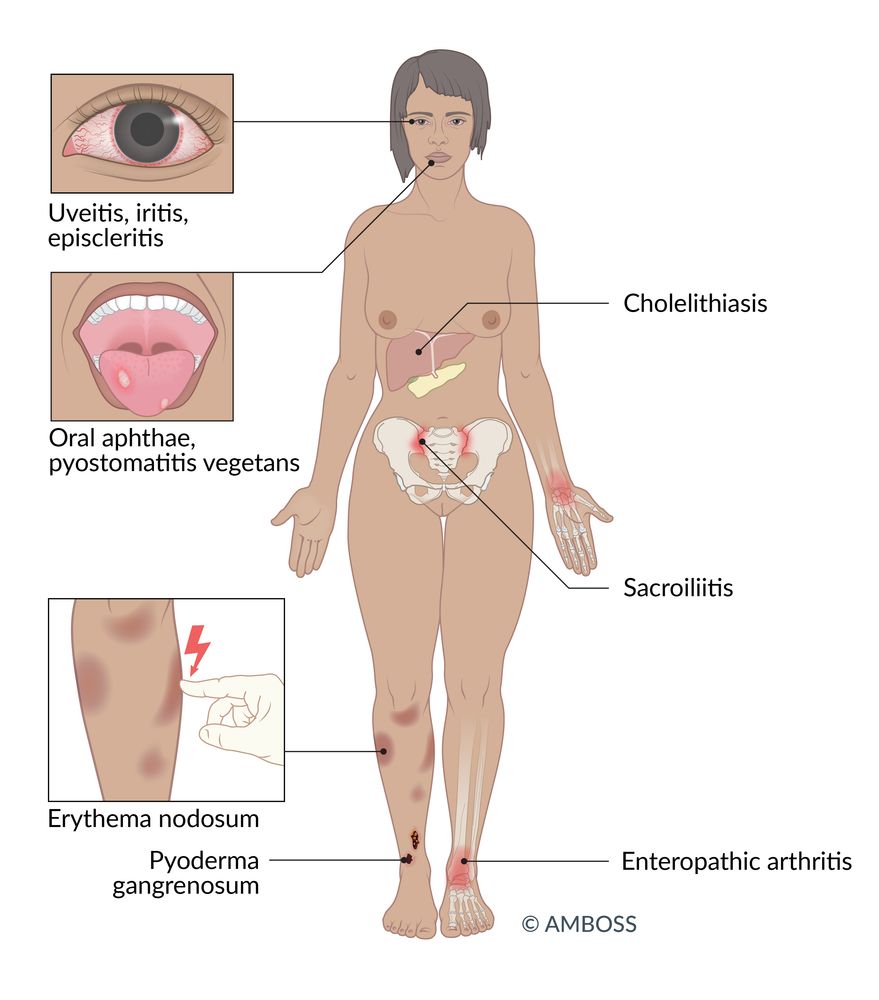
Extraintestinal features of ulcerative colitis
- General: fatigue, fever
- Skeletal: (most common extraintestinal feature of ulcerative colitis): arthritis, ankylosing spondylitis, sacroiliitis [9][10]
- Ocular: uveitis, episcleritis, iritis
- Biliary: primary sclerosing cholangitis (it is rare for patients with ulcerative colitis to develop PSC, but up to 90% of all patients with PSC will also have ulcerative colitis)
-
Cutaneous
- Erythema nodosum
- Pyoderma gangrenosum
- Aphthous stomatitis
-
Pyostomatitis vegetans
- A very rare condition that is associated with other cutaneous diseases and inflammatory bowel disease, particularly ulcerative colitis
- Manifests with multiple aphthae and pustules of the oral mucosa
PSC is often associated with inflammatory bowel disease, especially ulcerative colitis. However, only approximately 4% of patients with inflammatory bowel disease develop PSC.
“ULCCCERS:” Ulcers, Large intestine, Continuous/Colon cancer/Crypt abscesses, Extends proximally, Red diarrhea, and Sclerosing cholangitis are the characteristics of ulcerative colitis.

Disease course
-
Chronic intermittent
- Most common course
- Exacerbation is followed by complete remission.
-
Chronic continuous
- Complete remission does not occur.
- Disease severity varies.
-
Acute fulminant (i.e., acute severe ulcerative colitis)
- Sudden onset
- Severe diarrhea, dehydration, shock
© AMBOSS
Subtypes and variants
Backwash ileitis
- Definition: inflammation of the terminal ileum in the context of ulcerative colitis
- Epidemiology: affects approximately 10–20% of all patients diagnosed with ulcerative colitis
- Localization: typically affects an area a few centimeters proximal to the ileocecal valve
- Pathophysiology: The pathological mechanism is not fully understood.
- Differential diagnosis: Clinically, backwash ileitis is hardly relevant but its presence makes it harder to differentiate between ulcerative colitis and Crohn disease.
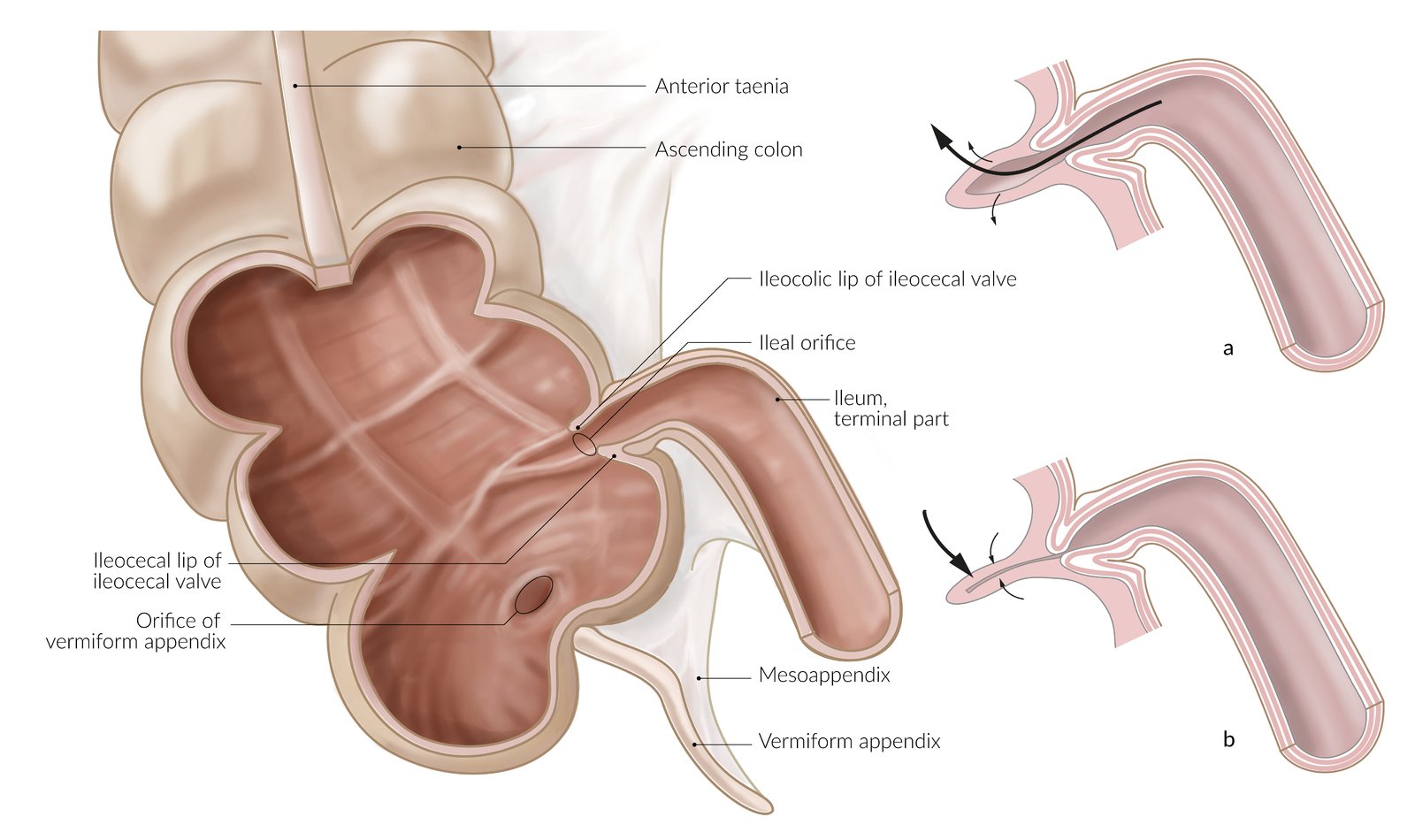
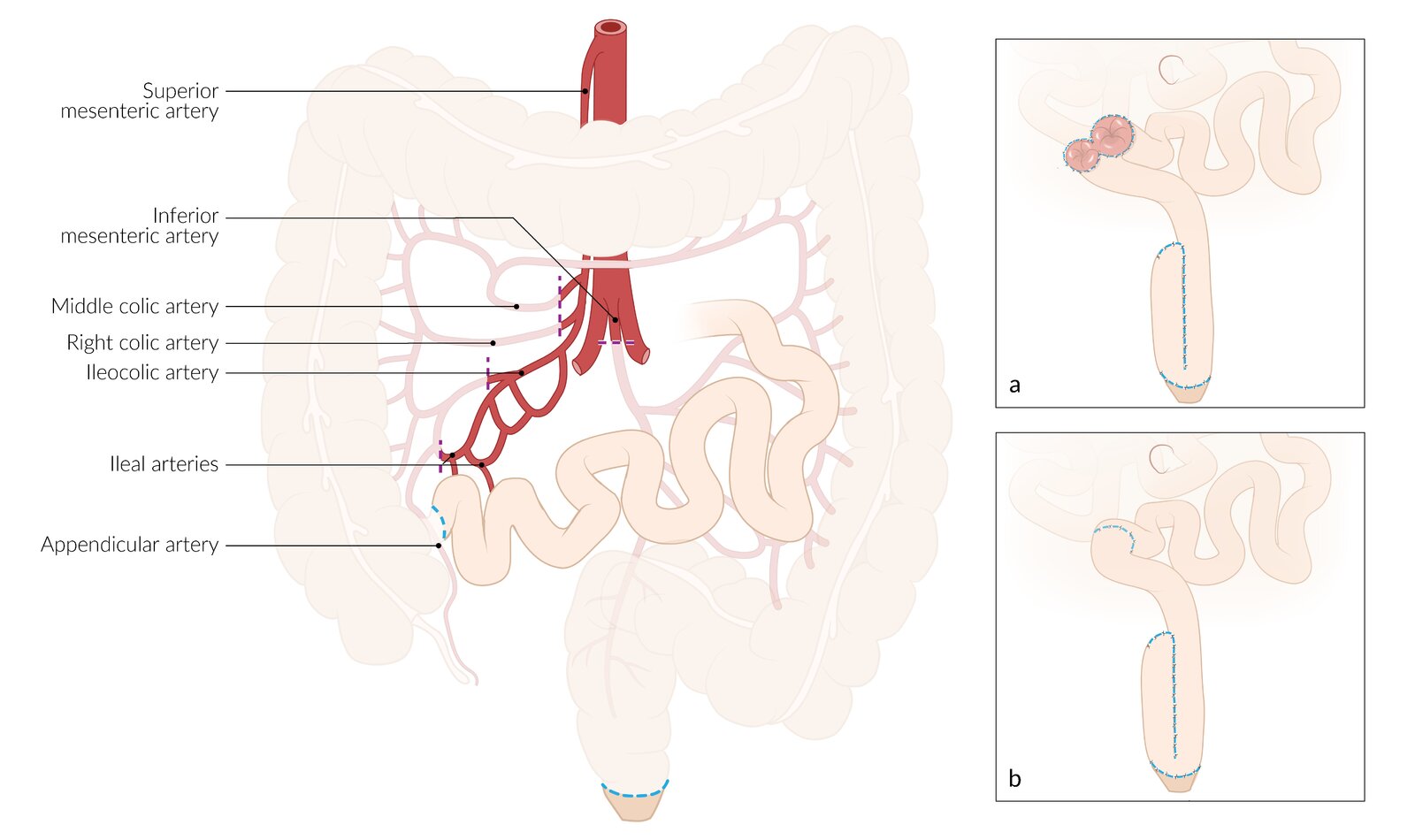
The ileum invaginates into the cecum at the junction of the small and large intestine, forming the ileocecal valve. The valve consists of an ileocolic and an ileocecal lip. This enables flow from the ileum to the cecum (a) and prevents backflow of cecal contents, esp. bacteria (b). A defective valve may result in bacterial overgrowth of the small intestine.
© AMBOSS
Diagnosis
Approach [1]
The diagnosis is based on clinical features, endoscopic and pathology findings. [1]
- Suspect ulcerative colitis in patients with hematochezia, increased stool frequency, and fecal urgency.
- Assess for extraintestinal features of ulcerative colitis.
- Order laboratory studies to:
- Rule out infectious gastroenteritis
- Assess disease severity (e.g., baseline levels of CRP, fecal calprotectin) [11]
- Consult gastroenterology for an ileocolonoscopy with biopsy to:
- Confirm the diagnosis of ulcerative colitis
- Determine the extent of disease in ulcerative colitis and severity of ulcerative colitis
- Assess disease severity
- See "Classification of ulcerative colitis by severity."
- Identify patients with acute severe ulcerative colitis (ASUC).
- Consider CT or MRI abdomen if endoscopy is contraindicated.
Laboratory studies [1]
Stool testing for infectious gastroenteritis is indicated in all patients. Blood tests are not required for diagnosis, but help assess disease activity and severity.
-
Blood tests
- CBC: anemia, leukocytosis, thrombocytosis [4]
- ESR, CRP: Elevated levels may indicate active ulcerative colitis and often correlate with disease severity.
- Hypoalbuminemia: associated with a poor prognosis and more severe disease
- ALP, GGT: elevated in patients with concurrent PSC
-
pANCA
- Not recommended to establish diagnosis, monitor disease activity, or determine prognosis [1]
- Elevated in up to 70% of patients with ulcerative colitis [1]
-
Stool diagnostic studies [1][11]
- Stool test for Clostridioides difficile infection [1][11]
- Fecal calprotectin: to monitor disease activity and response to therapy [1][11]
- GI PCR panel: Consider based on clinical features and risk factors for diarrhea. [11]
- Stool culture and microscopy: to assess for bacteria, ova, and parasites if a GI PCR panel is not available
CRP, ESR, or hemoglobin levels are not required for the diagnosis of ulcerative colitis; they help determine disease severity.
Hypoalbuminemia and ↑ CRP are significant poor prognostic factors. Other factors include age < 40 years at diagnosis, extensive ulcerative colitis, and severe disease on endoscopic evaluation scores. [1]
Endoscopy [1]
-
Ileocolonoscopy
- Recommended method for diagnosis and disease monitoring [1]
- Severe disease is a relative contraindication. [1]
- See "Histopathology findings" in "Pathology".
| Endoscopic findings in ulcerative colitis | |
|---|---|
| Early stages | Chronic disease |
|
|
-
Sigmoidoscopy [1]
- Indications
- Initially used as an alternative to ileocolonoscopy, e.g., in ASUC
- Monitoring treatment response
- Findings are similar to ileocolonoscopy findings.
- Indications
- EGD: recommended for patients with upper GI symptoms to rule out Crohn disease [1]
There is a high risk for colonic perforation in severe ulcerative colitis; caution should be used when performing biopsies.











Imaging studies [1]
- Not routinely recommended for diagnosis
- Adjunct to endoscopy, particularly for the detection of complications; , or if endoscopy is not possible. [1]
Abdominal x-rays [1]
- Indication: initial and serial evaluation of suspected ASUC
-
Findings
- Typically normal in mild-to-moderate disease
- Severe disease
- Loss of colonic haustra (lead pipe appearance)
- Increased bowel wall thickness
- May show signs of complications, e.g.:
- Toxic megacolon: massive distention
- Ulceration: segmental dilation with irregular edges outlined by gas [12]
- Perforation: pneumoperitoneum [13]


CT or MRI abdomen [1][13]
-
Indications
- Abdominal symptoms unexplained by endoscopic findings [1]
- Evaluation of proximal disease involvement when endoscopy is not feasible
- Suspected complications (e.g., bowel perforation)
- Differentiation from other conditions, e.g., Crohn disease [1]
-
Findings
- Loss of haustra
- Increased bowel wall thickness
- Mural hyperenhancement
- Signs of complications (similar to abdominal x-ray findings)
Barium enema radiography [12]
The role of barium enema is limited, as it is less sensitive than other imaging modalities and is contraindicated in patients with active disease.
- Indication: Colonoscopy is contraindicated and other cross-sectional imaging (e.g., CT, MRI) is not available.
-
Findings
- Granular appearance of the mucosa
- Deep ulcerations
- Loss of haustra
- Pseudopolyps that appear as filling defects
Abdominal ultrasound [1]
- Indication: monitoring disease activity and treatment response
- Findings: increased bowel wall thickness



Endoscopic view of the rectum
An inflamed, edematous mucosa with active bleeding is visible.
These findings are characteristic of ulcerative colitis.
Source: © IMPP
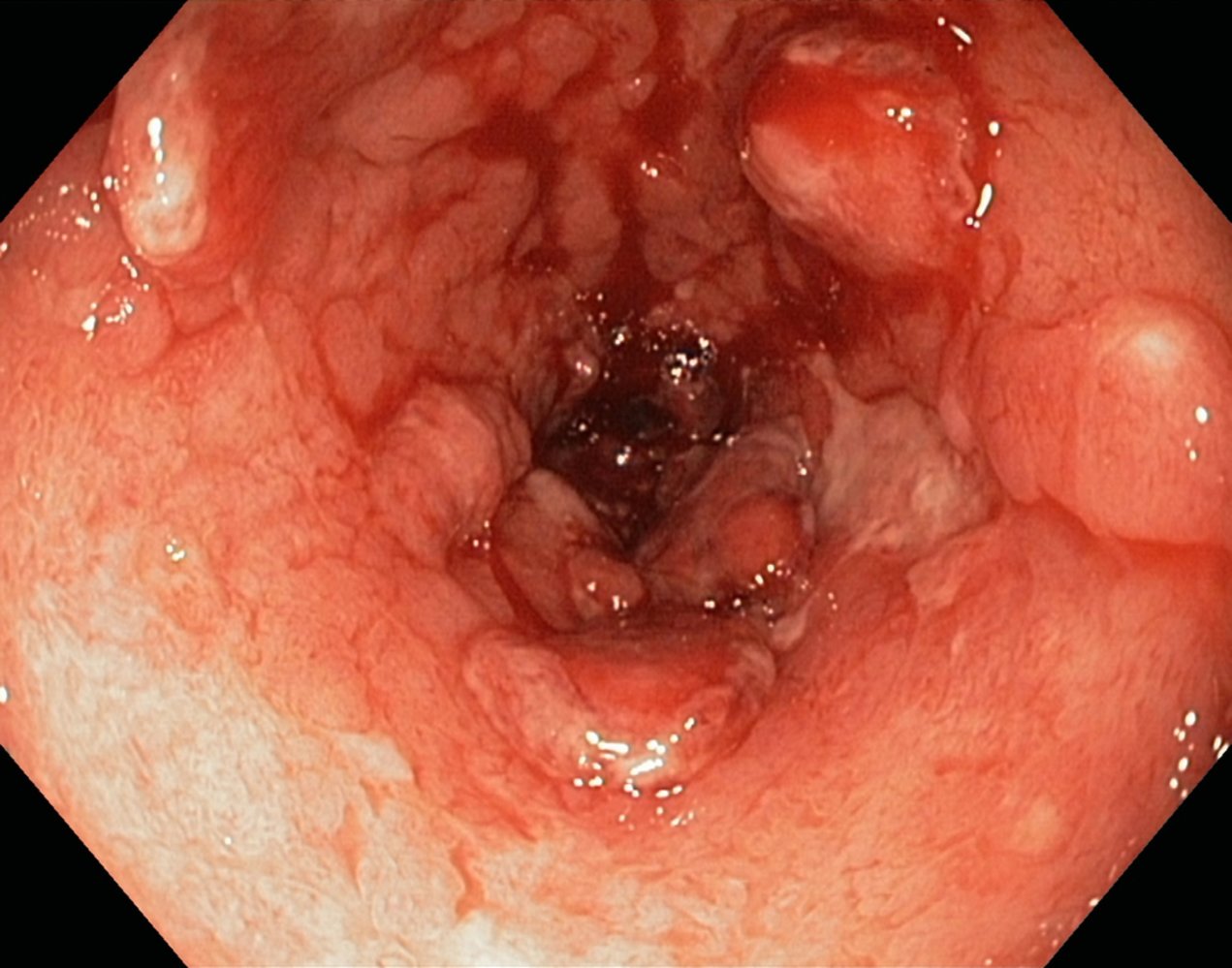
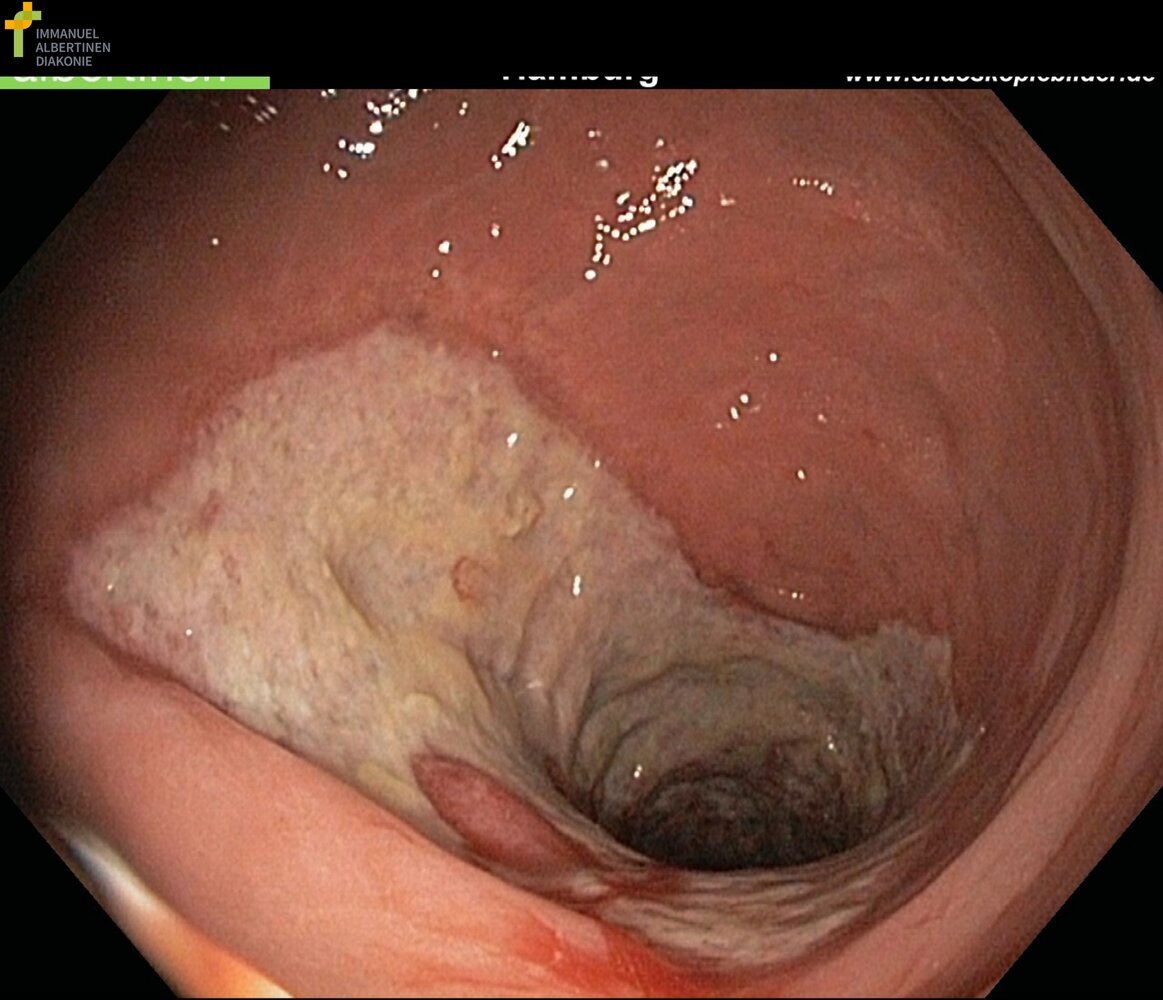
Endoscopic view of the colon
The mucosa appears erythematous and edematous, indicating active inflammation. The vascular pattern has been lost and minor spontaneous hemorrhage is visible. A fibrin-covered ulceration (blue overlay) and several pseudopolyps (indicated by dashed lines) are visible.
These features are characteristic of active ulcerative colitis.
Original title: “CU floride entzuendl”. Created by: Dr. J. Guntau. Organization providing image: endoskopiebilder.de - Innere Medizin des Albertinen-Krankenhauses Hamburg.
{kind=link}
Endoscopic view of the sigmoid colon
The mucosa is erythematous and edematous. There is a loss of superficial vascular markings. Several linear, semi-confluent ulcerations (green overlay) are visible.
These findings are characteristic of acute ulcerative colitis.
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
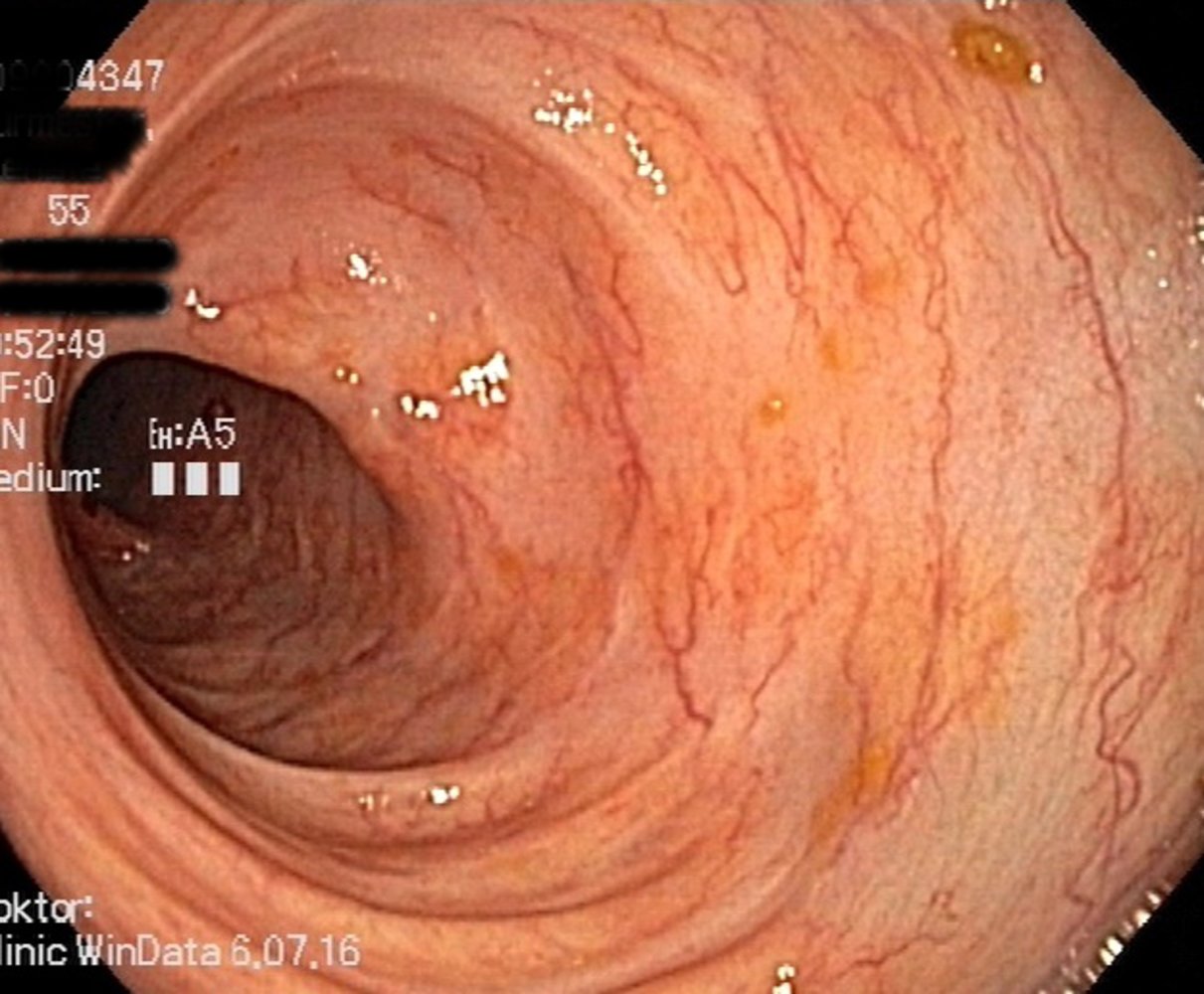
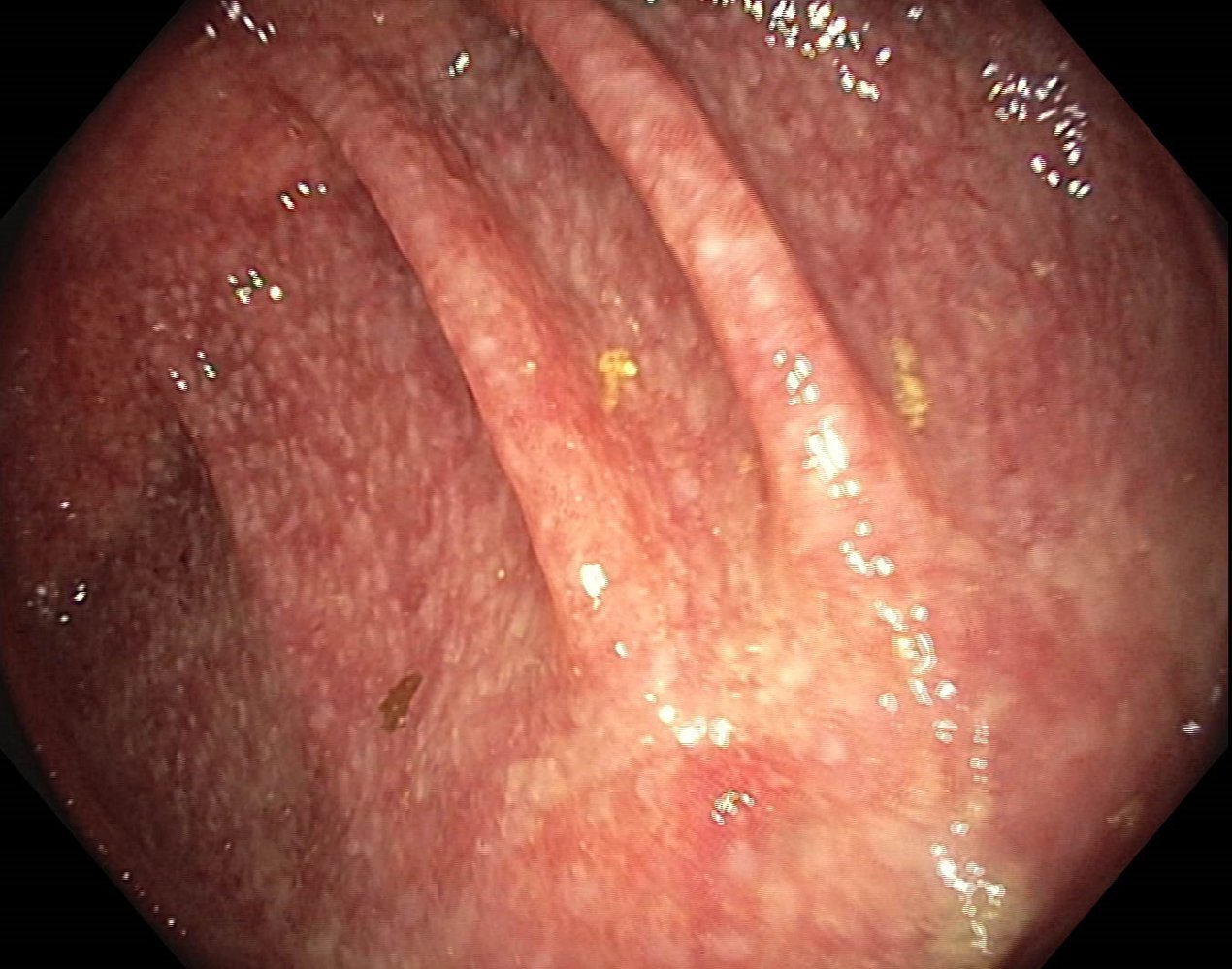
Endoscopic view of the colon in a patient with ulcerative colitis
The right side of the colon shows a loss of haustra and a diminished vascular pattern, both of which indicate previous exacerbations. On the left side of the colon, the haustral folds and vascular pattern are normal. There are no signs of active inflammation.
This appearance is consistent with ulcerative colitis in remission.
Original title: “Ausgebrannte CU Sigma”. Created by: Dr. J. Guntau. Organization providing image: endoskopiebilder.de - Innere Medizin des Albertinen-Krankenhauses Hamburg.
{kind=link}

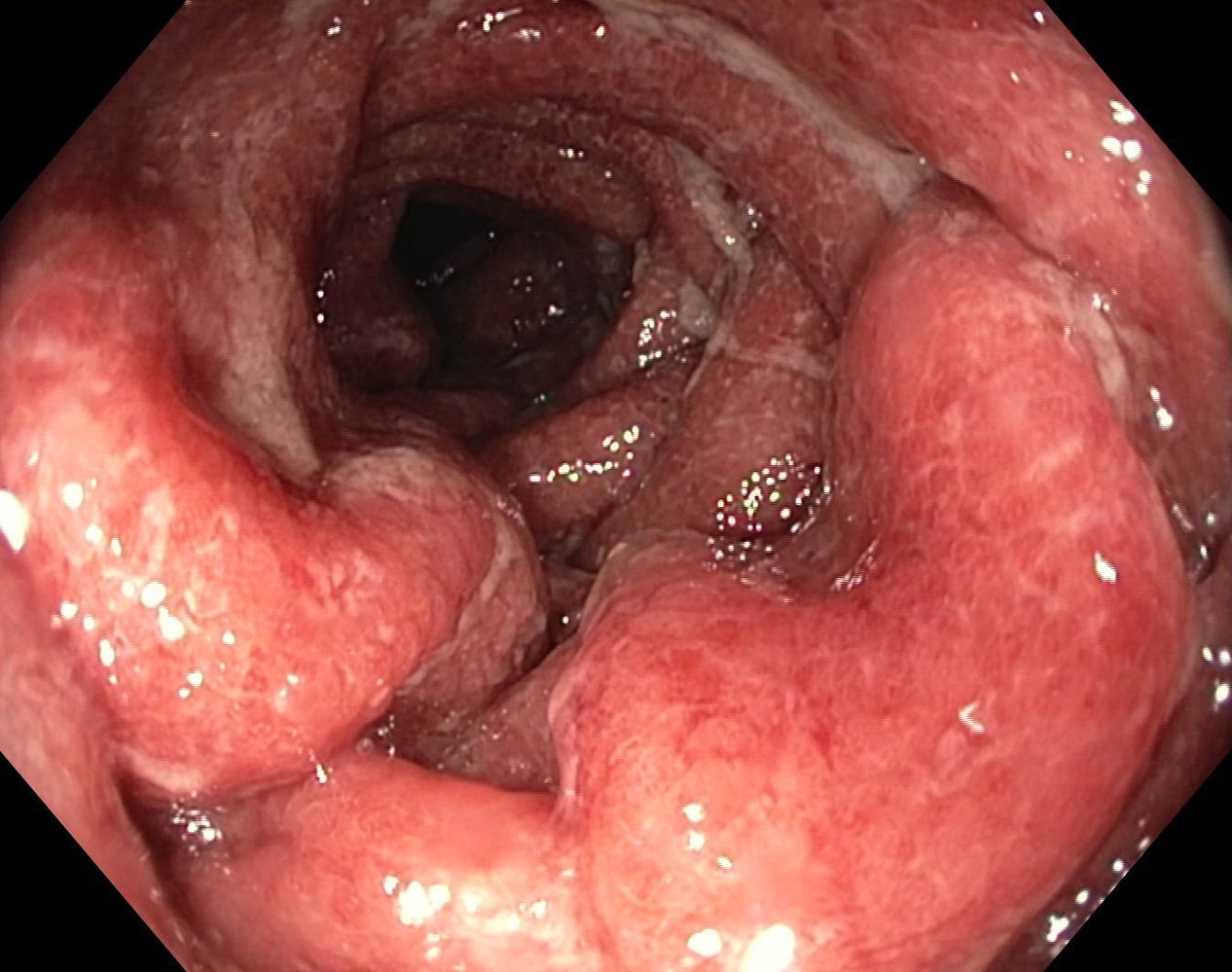
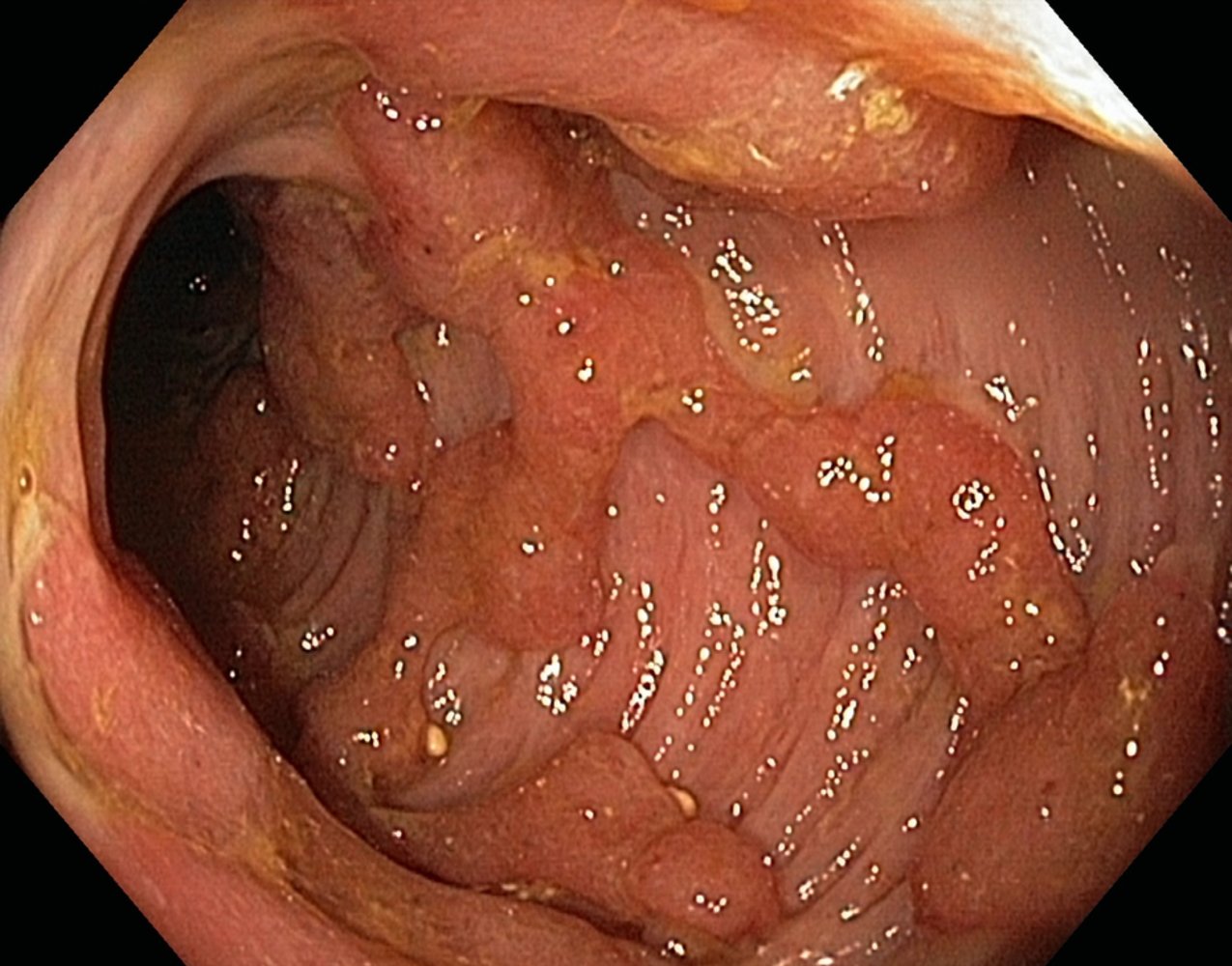
Endoscopic view of the colon
There are multiple raised areas of normal mucosal tissue resulting from mucosal regeneration and hyperplasia.
These findings are characteristic of pseudopolyps in advanced ulcerative colitis.
Original title: “Entzündliche Pseudopolypen”. Created by: Dr. J. Guntau. Organization providing image: endoskopiebilder.de - Innere Medizin des Albertinen-Krankenhauses Hamburg.
{kind=link}
Endoscopic view of the colon
There are multiple prominent, raised areas of normal mucosa resulting from mucosal regeneration and hyperplasia.
These findings are characteristic of pseudopolyps in advanced ulcerative colitis.
Original title: “Pseudopolypen gross Pankolitis”. Created by: Dr. J. Guntau. Organization providing image: endoskopiebilder.de - Innere Medizin des Albertinen-Krankenhauses Hamburg.
{kind=link}

Endoscopic view of the colon
The mucosa appears edematous and several pseudopolyps are beginning to form. There is a loss of superficial vascular markings with a central area of spotty bleeding.
These findings are characteristic of active ulcerative colitis.
Source: © IMPP
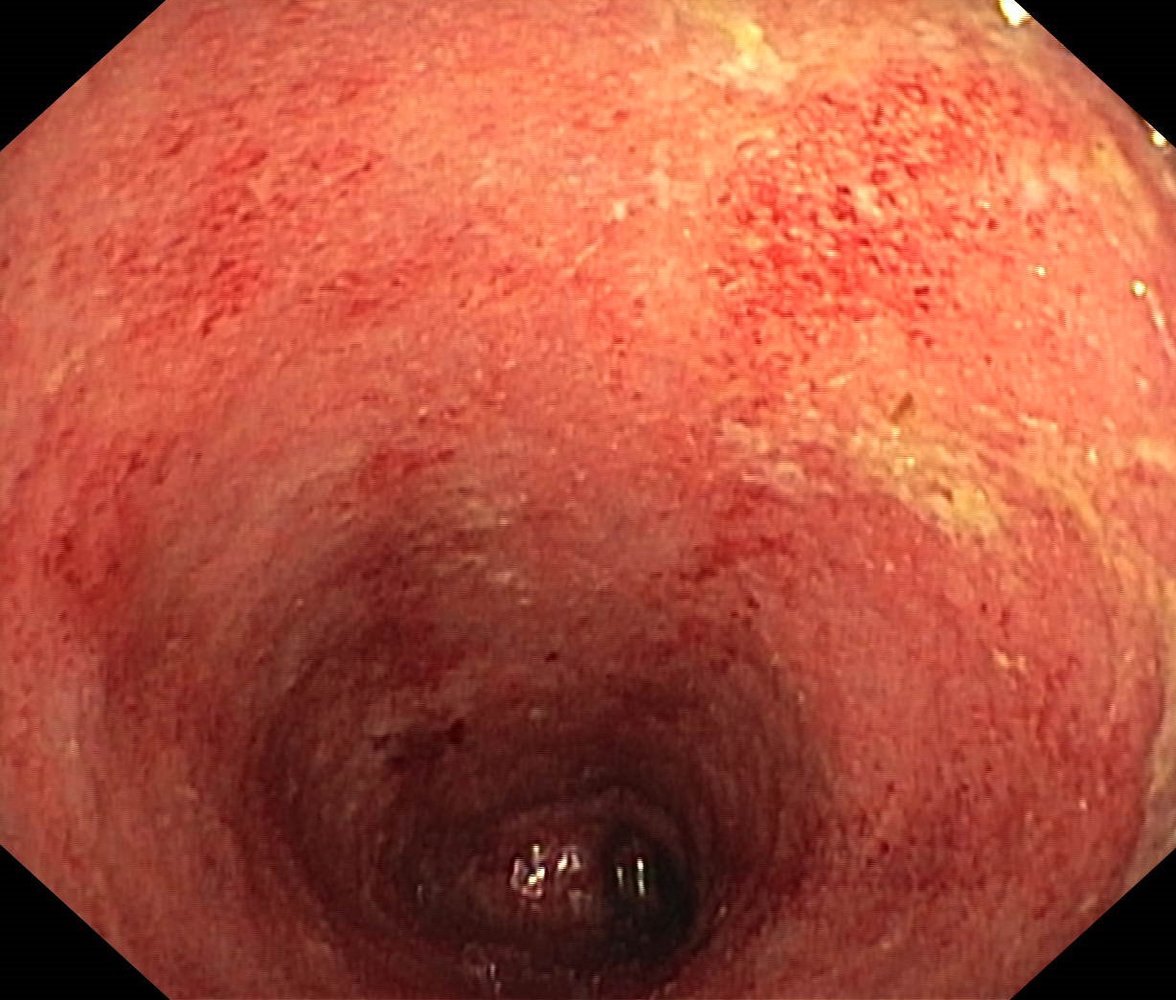
Endoscopic view of the colon
The mucosa is erythematous and edematous. There is a loss of superficial vascular markings. Mucosal granularity and ulcerations (examples indicated by green overlay) are visible.
These findings are characteristic of acute ulcerative colitis.
Original title: “CU floride nah”. Created by: Dr. J. Guntau. Organization providing image: endoskopiebilder.de - Innere Medizin des Albertinen-Krankenhauses Hamburg.
{kind=link}
Endoscopic view of the colon
The mucosa appears inflamed and shows several fibrin deposits (examples indicated by green overlay). The normal vascular pattern and haustral folds of the colon are no longer visible.
These features are characteristic of active ulcerative colitis.
© AMBOSS

Endoscopic view of the colon in a patient with ulcerative colitis
The mucosa shows light, line-shaped scars with a loss of the normal vascular pattern indicating previous ulcerations (blue overlay). There are no signs of active inflammation.
These findings are consistent with ulcerative colitis in remission.
Original title: “Narben CU Sigma”. Created by: Dr. J. Guntau. Organization providing image: endoskopiebilder.de - Innere Medizin des Albertinen-Krankenhauses Hamburg.
{kind=link}

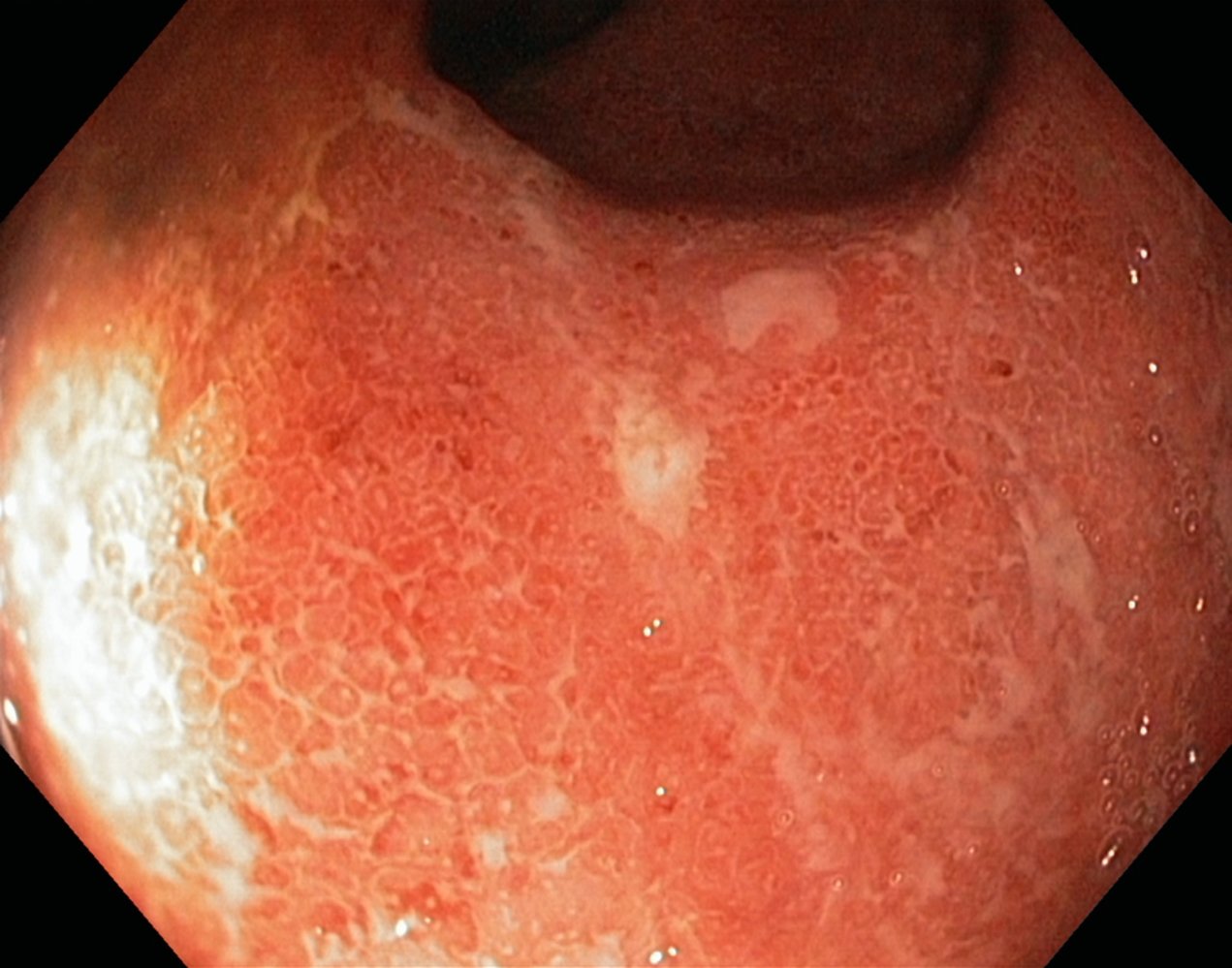
Endoscopic view of the colon in a patient with ulcerative colitis
The colonic mucosa shows a reticulated pattern due to scarring. The typical vascular pattern and haustral folds are missing. There are no signs of active inflammation.
These findings are consistent with ulcerative colitis in remission after a prolonged course of disease activity.
Original title: “CU Narben”. Created by: Dr. J. Guntau. Organization providing image: endoskopiebilder.de - Innere Medizin des Albertinen-Krankenhauses Hamburg.
{kind=link}

X-ray abdomen (AP view) of a patient with ulcerative colitis
A lack of haustral markings in the descending colon has resulted in a smooth cylindrical appearance (lead-pipe sign; green overlay).
The lead-pipe sign has been described as a characteristic barium enema finding in longstanding ulcerative colitis. The sign is also visible on conventional radiography, CT, and MRI and has been observed in other inflammatory bowel diseases (e.g, Crohn disease, cathartic colon, tuberculosis).
Source: “Colitis ulcerosa - Haustrenverlust - Fahrradschlauch” by Hellerhoff, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
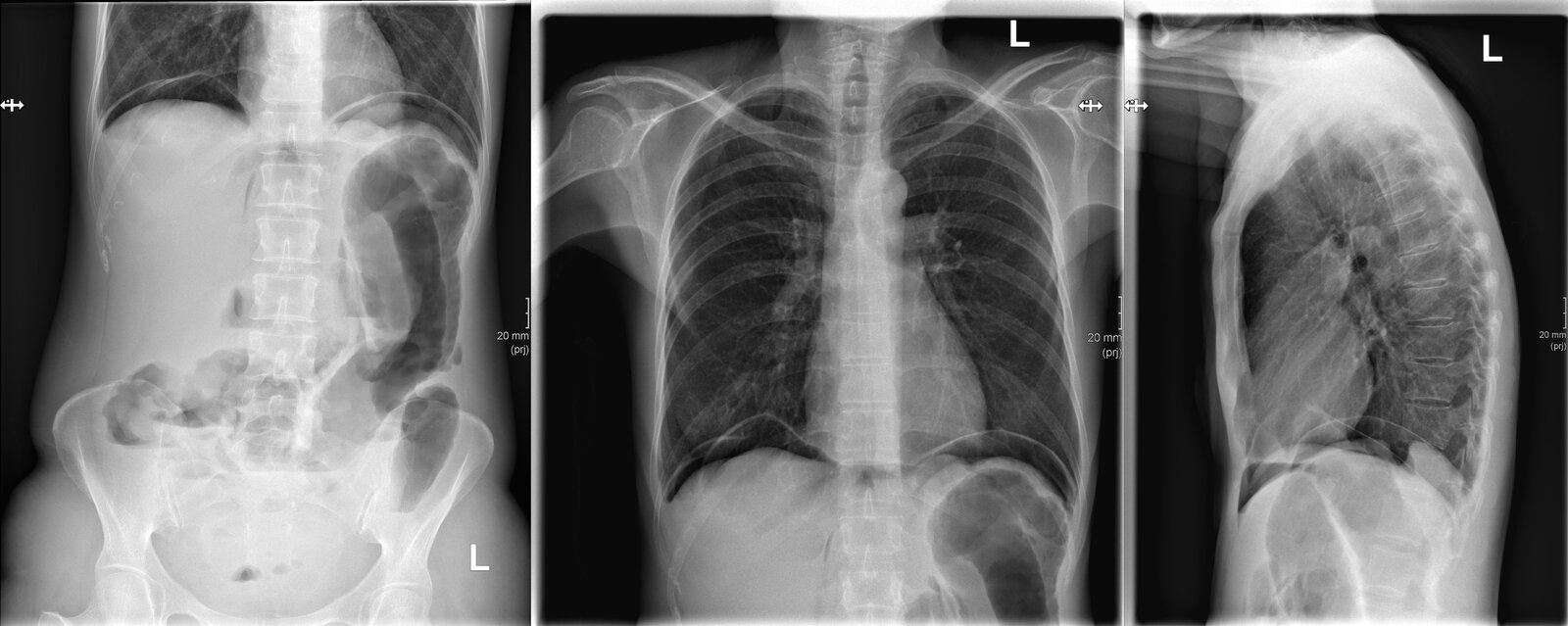
X-ray abdomen (AP erect view) and chest (PA and lateral views)
Multiple air-fluid levels are seen in the colon and small bowel (examples indicated by black lines). Some dilated segments of left colon are seen and gas is present in the peritoneal space as a result of bowel perforation. Gas is primarily located beneath the diaphragms (green overlay) because of the erect positioning of the patient. Additional gas has dissected into the retroperitoneum (examples indicated by red overlay) and is visible as linear collections parallel to the spine.
Our great thanks to Kerstin Bohse, MD (Klinikum Pfeiffersche Stiftungen), for kindly providing this case.
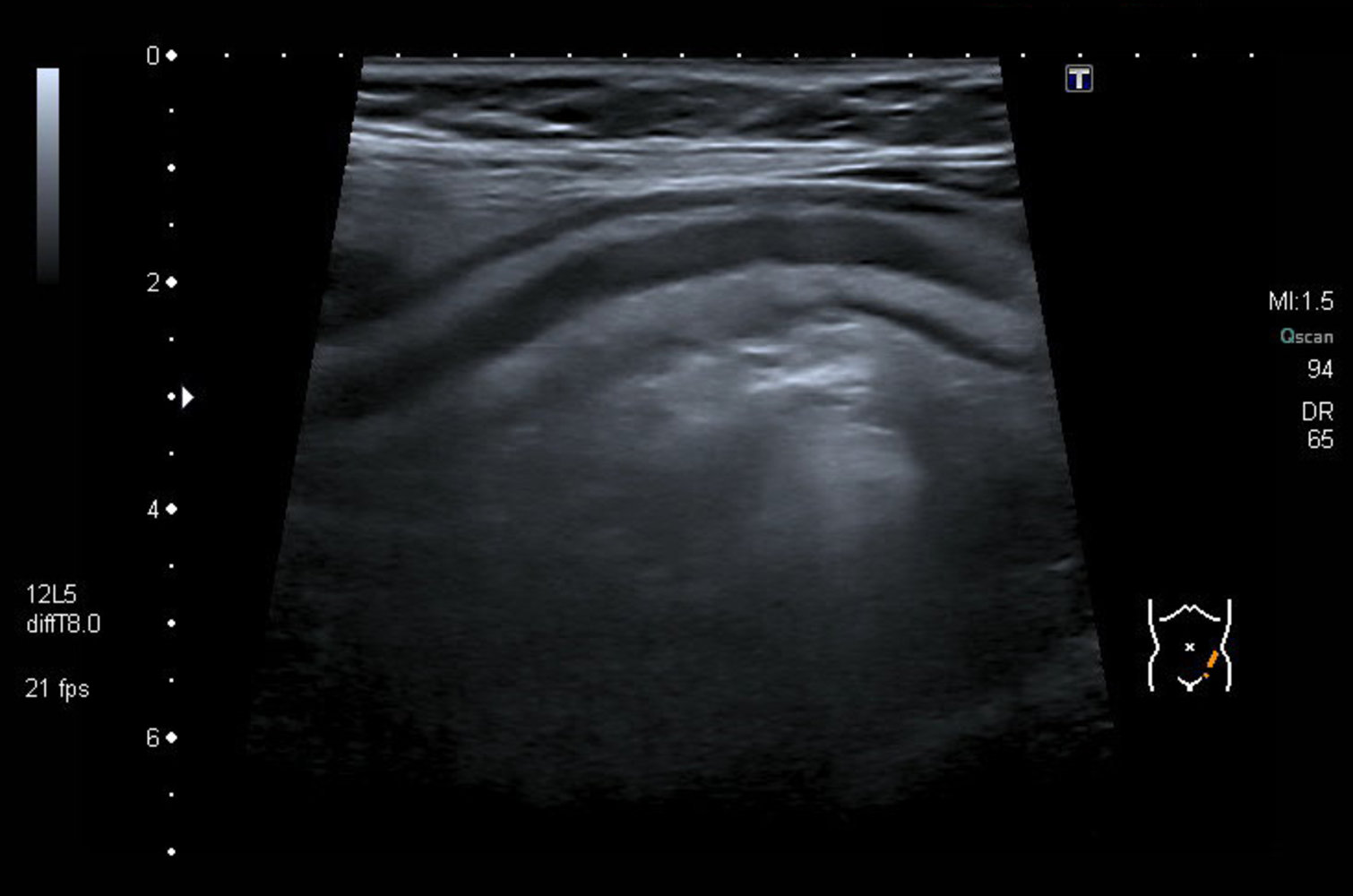
Transabdominal ultrasound of the descending colon
The four layers of the intestine remain distinguishable (despite thickening of the intestinal wall) in ulcerative colitis as only the mucosa and submucosa are affected. The intestinal lumen also appears hypoechoic due to acute inflammation.
S: serosa; Mp: muscularis propria; Sm: submucosa; M: mucosa
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
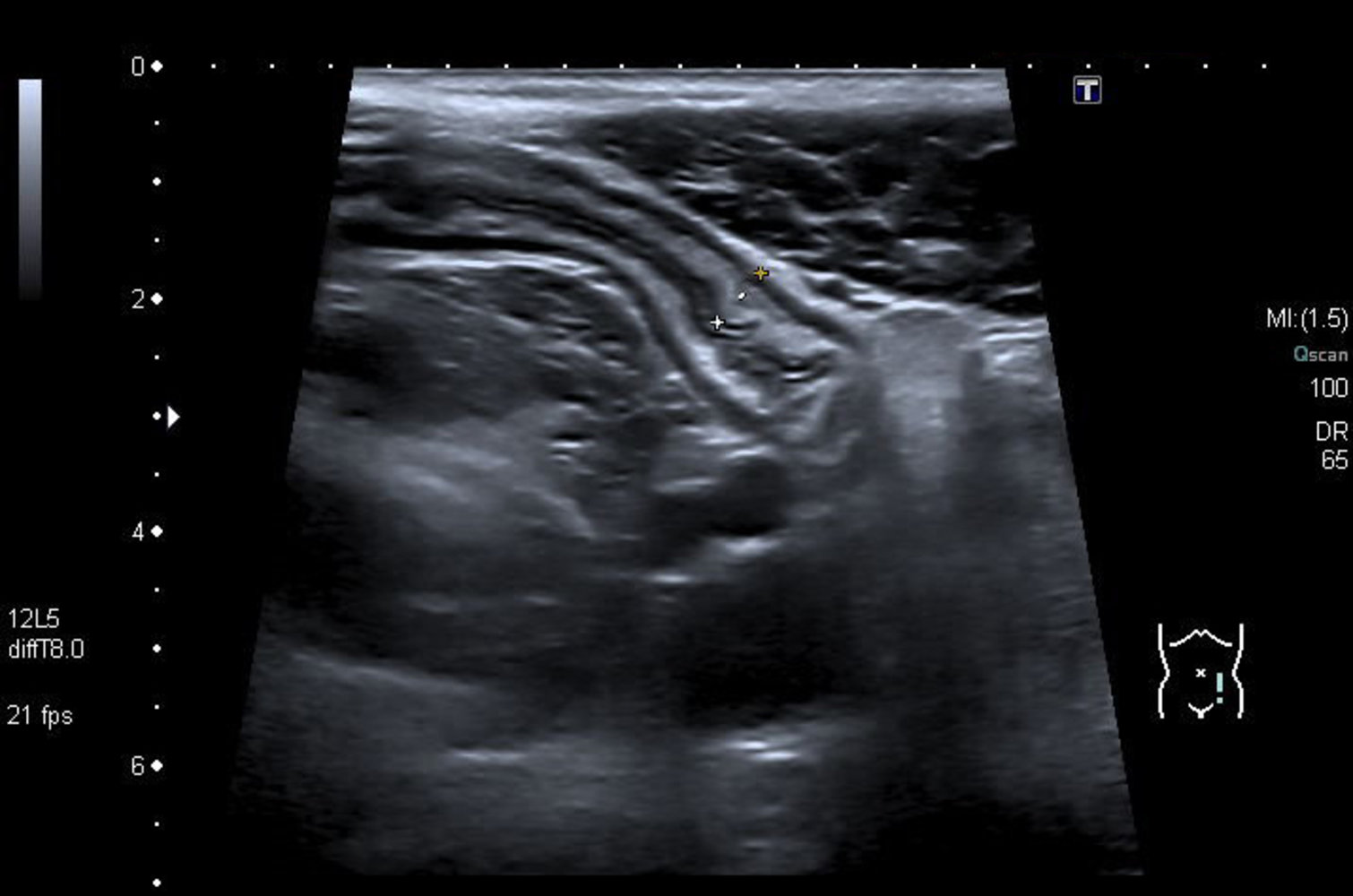
Transabdominal ultrasound of the descending colon
The intestinal layers remain distinguishable (despite thickening of the intestinal wall) in ulcerative colitis as the mucosa and submucosa are affected.
S: serosa; Mp: muscularis propria; Sm: submucosa; M: mucosa; Lr: luminal reflection
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
Pathology
Gross pathology
See “Endoscopic findings in ulcerative colitis” in “Diagnostics.”
Histopathology findings
-
Early stages
- Granulocyte (neutrophil) infiltration: limited to mucosa and submucosa
- Crypt abscesses: an infiltration of neutrophils into the lumen of intestinal crypts due to a breakdown of the crypt epithelium
-
Chronic disease
- Lymphocyte infiltration
- Mucosal atrophy
-
Altered crypt architecture
- Branching of crypts
- Irregularities in size and shape
- Epithelial dysplasia
In ulcerative colitis, the extent of intestinal inflammation is limited to the mucosa and submucosa. In contrast, Crohn disease shows a transmural pattern of intestinal involvement.
Noncaseating granulomas are seen in Crohn disease but are not a feature of ulcerative colitis!


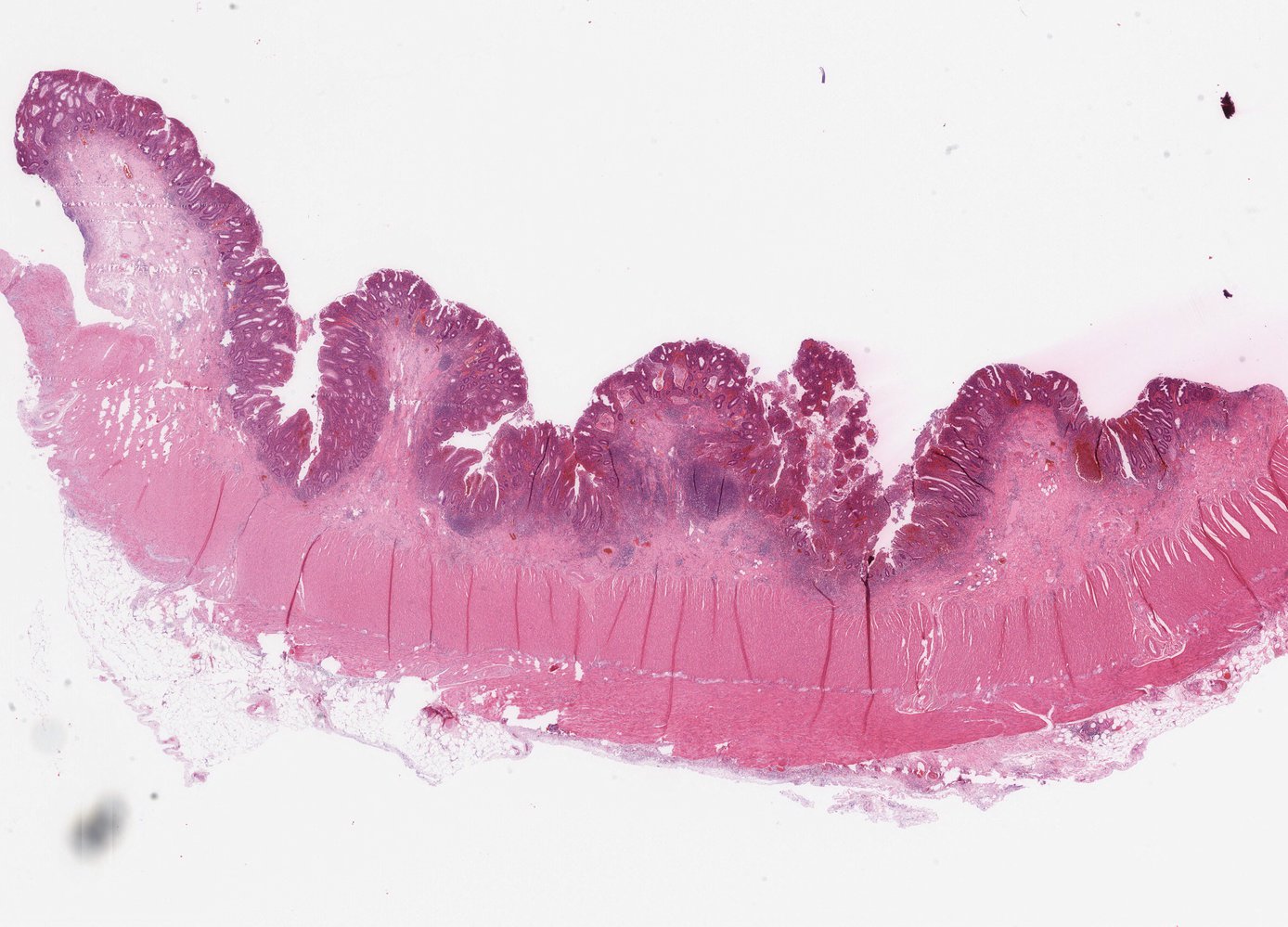
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. Alberto Perez Bouza
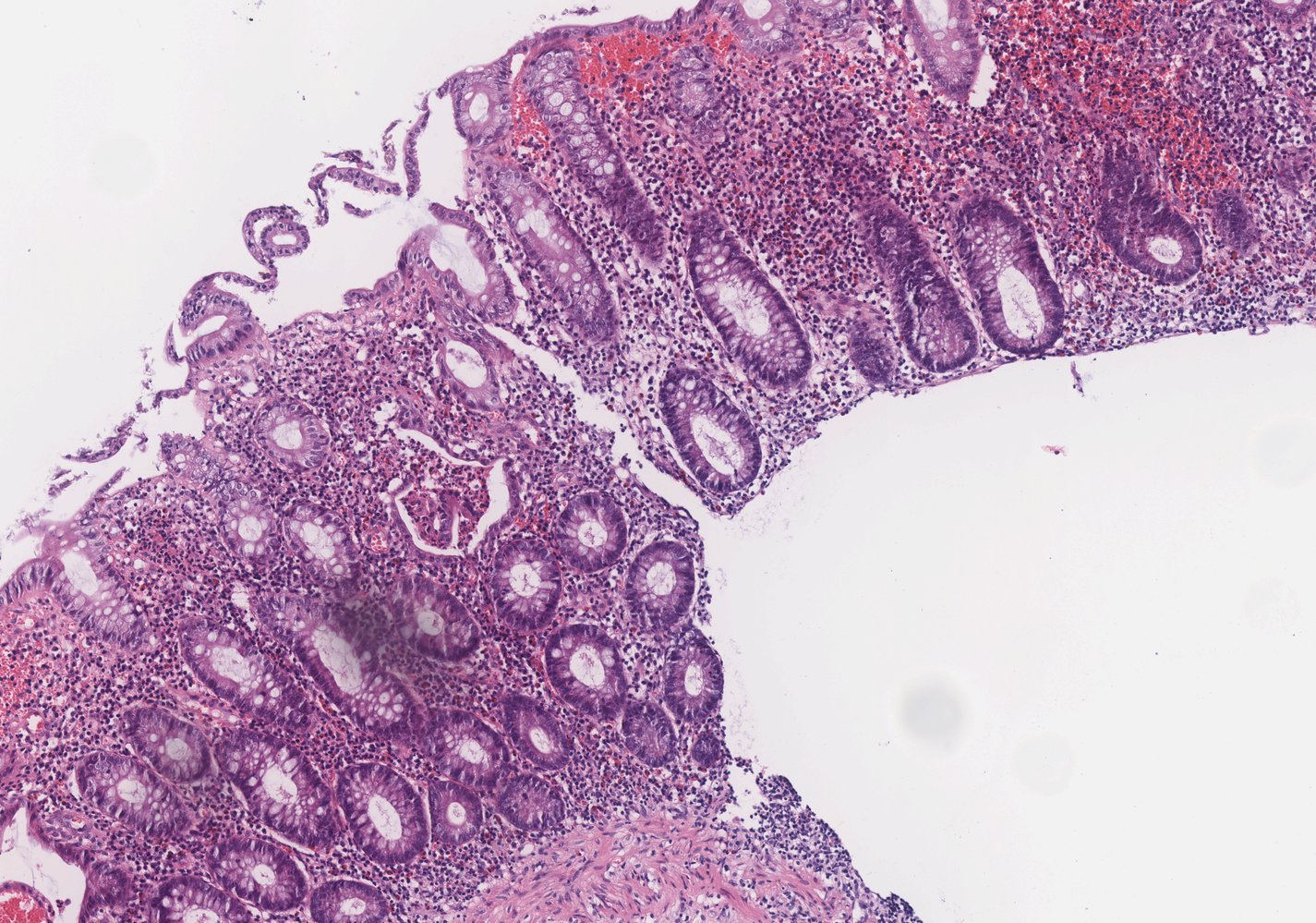
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. Alberto Perez Bouza
Differential diagnoses
Differential diagnosis considerations
- Crohn disease (see “Differential diagnostic considerations: Crohn disease and ulcerative colitis”)
- Exudative-inflammatory diarrhea
- Diverticular disease
- Appendicitis
- Ischemic colitis
-
Infectious colitis
- C. difficile colitis
- Shigella dysenteriae
- Salmonella enterocolitis
- Escherichia coli colitis
- Campylobacter enterocolitis
- Yersiniosis
- Tuberculosis
- CMV colitis
- Microscopic colitis
- Radiation colitis
- Celiac disease
- Inflammatory diarrhea
- Indeterminate colitis


The differential diagnoses listed here are not exhaustive.
Endoscopic view of the colon
A large fibrin-covered ulceration (green overlay) is visible. The surrounding mucosa appears fragile and edematous, with a loss of the colonic vascular pattern.
These findings are consistent with ischemic colitis.
Our great thanks to Albertinen Krankenhaus, Hamburg, Germany, for kindly providing this case.
Endoscopic view of the colon
Erythematous mucosa with multiple small fibrinous spots can be seen. The semilunar folds and haustra are normal and the vascular pattern remains recognizable. The brown and yellow deposits are residual bowel contents.
These findings are consistent with infectious colitis.
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
© AMBOSS
Management
General principles [1]
The goal of treatment is clinical and endoscopic remission.
- Consult gastroenterology before starting management.
- Provide supportive care measures for all patients.
- Choice of pharmacological therapy is based on the classification of ulcerative colitis by severity and patient-specific prognostic factors.
- Surgical management should be considered if medical therapy is unsuccessful or complications occur.
- Long-term management includes:
- Monitoring for complications related to the disease and its treatment.
- Screening for colorectal cancer and other common comorbidities (e.g., depression and anxiety).
While most cases of ulcerative colitis can be managed in an outpatient setting, patients with ASUC should be admitted for management.
Supportive care [1]
-
Pain management
- Nonpharmacological measures, e.g., heating pads
- Consider acetaminophen, anxiolytics, and sedatives.
- Avoid opioids and NSAIDs.
-
Nutritional support
- Assess for and manage malnutrition.
- Avoid parenteral nutrition unless required to improve nutritional status prior to colectomy.
- Probiotics: There is insufficient evidence to support their use.
Surgical management [1]
Surgical treatment is curative for ulcerative colitis and reduces the risk of colorectal cancer. [1]
-
Indications
-
Complications of ASUC
- Toxic megacolon
- Bowel perforation
- Severe hematochezia
- Multiorgan failure
- Refractory ulcerative colitis; (i.e., no response after 3–5 days of medical management and/or glucocorticoid dependence) [1]
- Dysplasia or carcinoma
-
Complications of ASUC
-
Procedure: restorative proctocolectomy with an ileal pouch-anal anastomosis (J pouch)
- Resection of the entire colon and rectal mucosa while sparing the anal sphincters.
- Loops of small intestine (serving as the pouch) are used to create an artificial rectum, resulting in a continence-conserving connection between the ileum and anus.
-
Complications of surgery
- Early (≤ 30 days): anastomotic leak, pelvic sepsis
- Late: bowel stricture, bowel obstruction, fertility issues, sexual dysfunction [4]
- Most common late postoperative issue: pouchitis (increased stool frequency, malaise, and possibly incontinence caused by bacterial overgrowth)
Nutritional status should be optimized before colectomy to improve patient outcomes.

Long-term management of ulcerative colitis
-
Disease monitoring
- Flexible sigmoidoscopy: 3–6 months after starting a new treatment [4]
- Clinical assessment: every 3 months until remission, then every 6–12 months [4]
- Follow-up after symptomatic remission
- Symptom assessment
- Inflammation biomarkers (i.e., fecal calprotectin, fecal lactoferrin, and/or serum CRP) [1][11]
-
Colorectal cancer screening [14][15]
- Start screening 8–10 years after the initial diagnosis or at the time of diagnosis of primary sclerosing cholangitis.
- Modality: ileocolonoscopy with biopsies
- Interval: every 1–5 years
-
Additional measures [16][17]
- Annual LFTs to monitor for primary sclerosing cholangitis [16][18]
- See also “Preventive care in IBD.”
© AMBOSS
Acute severe ulcerative colitis
Definition
The presence of both of the following indicates acute severe ulcerative colitis (ASUC): [1]
- ≥ 6 bowel movements daily
- ≥ 1 sign of systemic toxicity (e.g., tachycardia, fever, hemoglobin < 10.5 g/dL, ESR > 30 mm/hour) [1]
Management of ASUC [1]
- Consult gastroenterology for urgent flexible sigmoidoscopy (ideally within 24 hours).
- Obtain a stool test for CDI.
- Obtain cross-sectional imaging (e.g., CT scan) if there is concern for extraluminal complications or perforation.
- Initiate treatment with IV glucocorticoids (e.g., methylprednisolone, hydrocortisone)
- Provide supportive care with IV fluid resuscitation and electrolyte repletion as needed.
- Consider empiric antibiotics only in patients with signs of sepsis and/or concern for extraluminal complications.
- Closely monitor for:
- Complications: Order serial abdominal examinations and abdominal x-rays.
- Treatment response: based on clinical features (i.e., rectal bleeding and stool frequency), vital signs, physical examination findings, and serial CRP
- Assess for concomitant CMV colitis in patients with ASUC who do not improve with glucocorticoid therapy; see “Antiviral therapy for CMV.” [1]
- Consult surgery if:
- Complications arise (e.g., toxic megacolon, bowel perforation, hemorrhage, sepsis)
- There is no improvement after 3 days of medical management
Avoid NSAIDs, opioids, and anticholinergic medications in patients with ASUC.
Neither total parenteral nutrition nor empiric antibiotics are routinely indicated in ASUC.
Pharmacological therapy for ulcerative colitis
General principles [1]
-
The goal of pharmacological therapy is to induce and maintain disease remission.
- 5-ASA monotherapy are first-line in mild-to-moderate ulcerative colitis.
- Oral glucocorticoids are indicated for induction of remission of ulcerative colitis resistant to 5-ASA monotherapy.
-
Systemic immunomodulators (e.g., anti-TNF agents) should be considered for: [1][19]
- Patients with moderate-to-severe ulcerative colitis
- Patients with poor prognosis factors:
- Age < 40 years at diagnosis
- ↑ CRP, hypoalbuminemia
- Extensive colitis, severe disease on endoscopy
- Hospitalization for colitis
Glucocorticoids should only be used for induction of remission and then gradually tapered. Glucocorticoid-sparing agents are preferred for maintenance of remission. [1]
Induction of remission [1]
| Pharmacological treatment for induction of remission in ulcerative colitis [1][19] | ||
|---|---|---|
| Disease severity | Agents | |
| Mild-to-moderate [1] |
|
|
| Moderate-to-severe [1] |
|
|
| Acute severe ulcerative colitis |
|
|
For induction of remission, azathioprine may be considered in combination with anti-TNF agents, not as monotherapy. [14]
Maintenance of remission
- The same agents used for induction should be continued for maintenance of remission, except for glucocorticoids.
- Thiopurine (e.g., azathioprine) monotherapy may be considered if remission was achieved with glucocorticoids alone.[19]
Overview of 5-ASA and 5-ASA derivatives [14][20]
| 5-ASA and 5-ASA derivatives | |||
|---|---|---|---|
| Description | Mechanism of action | Adverse effects | |
| Mesalamine |
|
|
|
| Olsalazine |
|
||
| Sulfasalazine |
|
|
|
Complications
-
↑ Risk of cancer (see “Long-term management of ulcerative colitis” for screening protocol)
- Risk increases with duration and/or extent of disease (e.g., pancolitis).
- Colorectal carcinoma risk is not significantly increased in patients with mild ulcerative colitis.
- Toxic megacolon
- Fulminant colitis: severe bowel inflammation that typically causes > 10 stools per day, lower gastrointestinal bleeding, abdominal pain, and abdominal distention
- Gastrointestinal bleeding (both acute and chronic)
- Perforation → peritonitis (see “Gastrointestinal perforation”)
- Colonic stricture
- Amyloidosis
References:[23]
We list the most important complications. The selection is not exhaustive.
Special patient groups
Inflammatory bowel disease in children [3][24][25]
Epidemiology
- The incidence of IBD in children is rising, especially very early onset IBD (before 6 years of age). [3][26]
- Prevalence: 77 per 100,000 [3]
Clinical features [3][25]
The clinical features of IBD are similar in adults and children. Additionally, in children, IBD is characterized by: [3]
- Delayed onset of puberty
- Growth stunting (more commonly associated with Crohn disease) [16]
- Increased risk of extraintestinal symptoms [24][25]
- Extraintestinal symptoms may precede gastrointestinal symptoms by months or years.
- Approx. 25% of children have extraintestinal symptoms at diagnosis. [24]
- See “Extraintestinal symptoms of Crohn disease” and “Extraintestinal symptoms of ulcerative colitis.”
- Increased risk of severe disease and complications
Red flags for IBD in children [3]
Any of the following features in a child with chronic (≥ 4 weeks) abdominal pain and/or diarrhea should prompt evaluation for IBD.
-
Major red flags for IBD in children
- Rectal bleeding
- Perianal findings (e.g., perianal fistula, perianal abscess, perianal ulcers)
-
Minor red flags for IBD in children
- First-degree relative with IBD
- Unplanned weight loss
- Extraintestinal symptoms of ulcerative colitis or extraintestinal symptoms of Crohn disease
Diagnosis of IBD in children [3][24][25][27]
- Assess for red flags for IBD in children.
- Obtain CBC, inflammatory markers (CRP, ESR), liver chemistries, and stool studies. [28]
- Normal laboratory findings do not rule out IBD.
- See “Laboratory studies” in “Diagnostics for ulcerative colitis” or “Diagnostics for Crohn disease” for details.
- Refer for ileocolonoscopy and EGD as indicated. [25][29]
- Major red flags for IBD in children: Refer for endoscopy.
-
Minor red flags for IBD in children: Consider a risk-stratified approach based on fecal calprotectin levels to determine the need for endoscopy. [3]
- Fecal calprotectin > 250 mcg/g: Refer for endoscopy.
- Fecal calprotectin 50–250 mcg/g: Consider endoscopy based on shared decision-making.
- Fecal calprotectin < 50 mcg/g: IBD is excluded; consider other causes of abdominal pain in children.
- Imaging is indicated as an adjunctive diagnostic modality to determine the extent and severity of bowel involvement. [24][25][29]
- Small bowel imaging is recommended for all patients (unless endoscopic and histology findings are characteristic of ulcerative colitis). [25]
- MR enterography is the preferred imaging modality. [25][27][30]
- Wireless capsule endoscopy may be considered if conventional endoscopy or imaging is not feasible. [25][30]
Fecal calprotectin < 50 mcg/g excludes IBD. [3]
Management[3][24]
Multidisciplinary management (including a pediatric gastroenterologist, nutritionist, primary care physician, and psychologist) is recommended. [3]
- Treatment of ulcerative colitis is similar in children and adults, except thiopurines are not recommended for induction of remission in children. [3][16][31][32]
-
Treatment of Crohn disease is similar in children and adults, with the following exceptions for children: [3][27]
- Early initiation of anti-TNF therapy may be considered if prognostic indicators are poor.
- Exclusive enteral nutrition for 6–8 weeks (instead of glucocorticoids) may be considered to induce remission in selected patients.
- Long-term management of IBD is similar for children and adults.
- See “Long-term management of ulcerative colitis” and “Long-term management of Crohn disease” for details.
- In children, also monitor for growth faltering and delayed onset of puberty. [16]
- See also “Preventive care in IBD” for details on vaccination and screening for other complications.
The transition from a pediatric to an adult care team must be well coordinated to avoid disease complications and/or relapse. [3]
Inflammatory bowel disease in pregnancy [33][34]
Fertility and preconception counseling
- Fertility is not affected in women with IBD in remission and no history of abdominal surgery.
- Women with active disease have decreased fertility rates.
- Pharmacological therapy for IBD does not impact fertility.
- Active disease at conception increases the risk of persistently active disease during gestation.
- Active disease is associated with an increased risk of preterm birth and low birth weight.
- Patients who wish to conceive should be on appropriate pharmacological therapy to maintain disease remission.
- With the exception of methotrexate, all other treatments can be continued at conception.
Disease management during pregnancy
- Most medications used in the treatment of IBD are considered safe during pregnancy.
- Glucocorticoids; are indicated for disease flares but should be avoided as maintenance therapy because of the increased risk of gestational diabetes, preterm birth, and low birth weight.
- 5-ASA, 5-ASA derivatives, immunomodulators, and biopharmaceuticals can be used during pregnancy.
- Monotherapy is preferred for maintenance treatment to reduce the risk of adverse effects.
Prognosis
- On average, the life expectancy of patients with ulcerative colitis is normal.
- Poor prognosis factors include: [1]
- Laboratory studies: hypoalbuminemia and ↑ CRP
- Age < 40 years at diagnosis
- Extensive ulcerative colitis
- Severe disease on endoscopic evaluation scores
External Resources
- 2025 ACG Clinical Guideline Update: Ulcerative Colitis in Adults
- 2024 AGA Living Clinical Practice Guideline on Pharmacological Management of Moderate-to-Severe Ulcerative Colitis
- 2023 AGA Clinical Practice Guideline on the Role of Biomarkers for the Management of Ulcerative Colitis
- 2019 AGA Clinical Practice Guidelines on the Management of Mild-to-Moderate Ulcerative Colitis
References
- Rubin DT, Ananthakrishnan AN, Siegel CA, et al. "ACG Clinical Guideline Update: Ulcerative Colitis in Adults". Am J Gastroenterol. 120(6). :1187-1224. (2025)
- Peppercorn MA, Cheifetz AS. "Definition, epidemiology, and risk factors in inflammatory bowel disease". UpToDate. UpToDate. https://www.uptodate.com/contents/definition-epidemiology-and-risk-factors-in-inflammatory-bowel-disease. [2016-11-08]
- Bouhuys M, Lexmond WS, van Rheenen PF. "Pediatric Inflammatory Bowel Disease". Pediatrics. 151(1). (2022)
- Ungaro R, Mehandru S, Allen PB, Peyrin-Biroulet L, Colombel J-F. "Ulcerative colitis". The Lancet. 389(10080). :1756-1770. (2017)
- Pabla BS, Schwartz DA. "Assessing Severity of Disease in Patients with Ulcerative Colitis". Gastroenterol Clin North Am. 49(4). :671-688. (2020)
- Truelove SC, Witts LJ. "Cortisone in Ulcerative Colitis". BMJ. 2(4947). :1041-1048. (1955)
- Ordas et al. "Ulcerative colitis". The Lancet. 380(9853). :1606-1619. (2012)
- Kasper DL, Fauci AS, Hauser S, et al. "Harrisons Principles of Internal Medicine ". McGraw-Hill Medical Publishing Division. 19. (2016). ISBN: 9780071802154
- Rothfuss et al. "Extraintestinal manifestations and complications in inflammatory bowel diseases". World Journal of Gastroenterology. 12(30). :4819. (2006)
- Feuerstein and Cheifetz. "Ulcerative Colitis". Mayo Clinic Proceedings. 89(11). :1553-1563. (2014)
- Singh S, Ananthakrishnan AN, Nguyen NH, et al. "AGA Clinical Practice Guideline on the Role of Biomarkers for the Management of Ulcerative Colitis". Gastroenterology. 164(3). :344-372. (2023)
- Dignass A, Eliakim R, Magro F, et al. "Second European evidence-based consensus on the diagnosis and management of ulcerative colitis Part 1: Definitions and diagnosis". Journal of Crohn's and Colitis. 6(10). :965-990. (2012)
- Panes J, Bouhnik Y, Reinisch W, et al. "Imaging techniques for assessment of inflammatory bowel disease: Joint ECCO and ESGAR evidence-based consensus guidelines". Journal of Crohn's and Colitis. 7(7). :556-585. (2013)
- Rubin et al. "ACG Clinical Guideline: Ulcerative Colitis in Adults". Am J Gastroenterol. 114(3). :384-413. (2019)
- Murthy SK, Feuerstein JD, Nguyen GC, Velayos FS. "AGA Clinical Practice Update on Endoscopic Surveillance and Management of Colorectal Dysplasia in Inflammatory Bowel Diseases: Expert Review". Gastroenterology. 161(3). :1043-1051.e4. (2021)
- Turner D, Ruemmele FM, Orlanski‐Meyer E, et al. "Management of Paediatric Ulcerative Colitis, Part 1". J Pediatr Gastroenterol Nutr. 67(2). :257-291. (2018)
- Farraye FA, Melmed GY, Lichtenstein GR, et al. "ACG Clinical Guideline Update: Preventive Care in Inflammatory Bowel Disease". Am J Gastroenterol. 120(7). :1447-1473. (2025)
- Mertz A, Nguyen NA, Katsanos KH, Kwok RM. "Primary sclerosing cholangitis and inflammatory bowel disease comorbidity: an update of the evidence". Ann Gastroenterol.. 32(2). :124-133. (2019)
- Adams SM, Bornemann PH. "Ulcerative Colitis". Am Fam Physician. 87(10). :699-705. (2013)
- Rubalcava NS, Gadepalli SK. "Inflammatory Bowel Disease in Children and Adolescents". Adv Pediatr. 68. :121-142. (2021)
- Levine A, Koletzko S, Turner D, et al. "ESPGHAN Revised Porto Criteria for the Diagnosis of Inflammatory Bowel Disease in Children and Adolescents". J Pediatr Gastroenterol Nutr. 58(6). :795-806. (2014)
- Kelsen JR, Sullivan KE, Rabizadeh S, et al. "North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition Position Paper on the Evaluation and Management for Patients With Very Early‐onset Inflammatory Bowel Disease". J Pediatr Gastroenterol Nutr. 70(3). :389-403. (2020)
- Veauthier B, Hornecker JR. "Crohn's Disease: Diagnosis and Management". Am Fam Physician. 98(11). :661-669. (2018)
- Cuda SE, Censani M. "Assessment, differential diagnosis, and initial clinical evaluation of the pediatric patient with obesity: An Obesity Medical Association (OMA) Clinical Practice Statement 2022". Obes Pillars. 1. :100010. (2022)
- Rosen MJ, Dhawan A, Saeed SA. "Inflammatory Bowel Disease in Children and Adolescents". JAMA Pediatr. 169(11). :1053-60. (2015)
- Moore MM, Gee MS, Iyer RS, et al. "ACR Appropriateness Criteria® Crohn Disease-Child". J Am Coll Radiol. 19(5). :S19-S36. (2022)
- Turner D, Ruemmele FM, Orlanski‐Meyer E, et al. "Management of Paediatric Ulcerative Colitis, Part 2". J Pediatr Gastroenterol Nutr. 67(2). :292-310. (2018)
- Cabrera JM, Sato TT. "Medical and Surgical Management of Pediatric Ulcerative Colitis". Clinics in colon and rectal surgery. 31(2). :71-79. (2018)
- Mahadevan U, Robinson C, Bernasko N, et al. "Inflammatory Bowel Disease in Pregnancy Clinical Care Pathway: A Report From the American Gastroenterological Association IBD Parenthood Project Working Group.". Gastroenterology. 156(5). :1508-1524. (2019)
- Magro F, Gionchetti P, Eliakim R, et al. "Third European Evidence-based Consensus on Diagnosis and Management of Ulcerative Colitis. Part 1: Definitions, Diagnosis, Extra-intestinal Manifestations, Pregnancy, Cancer Surveillance, Surgery, and Ileo-anal Pouch Disorders.". Journal of Crohn's & colitis. 11(6). :649-670. (2017)
- Singh S, Loftus EV, Limketkai BN, et al. "AGA Living Clinical Practice Guideline on Pharmacological Management of Moderate-to-Severe Ulcerative Colitis". Gastroenterology. 167(7). :1307-1343. (2024)
- Ko CW, Singh S, Feuerstein JD, et al. "AGA Clinical Practice Guidelines on the Management of Mild-to-Moderate Ulcerative Colitis". Gastroenterology. 156(3). :748-764. (2019)
- Cantarini L, Tinazzi I, Biasi D, Fioravanti A, Galeazzi M. "Sulfasalazine-induced immune thrombocytopenia". Postgrad Med J. 83(980). :e1-e1. (2007)
- Farr M, Symmons D, Blake D, Bacon P. "Neutropenia in patients with inflammatory arthritis treated with sulphasalazine.". Ann Rheum Dis. 45(9). :761-764. (1986)