Summary
Urinary incontinence (UI) is a common condition characterized by involuntary leakage of urine. Causes and representations are variable. Stress urinary incontinence (SUI), urgency urinary incontinence (UUI), and mixed urinary incontinence are the most common types. UI is more common in older individuals, and approximately twice as common in women than in men. The diagnosis can often be made based on a detailed medical history, a voiding diary, physical examination, and basic testing including urinalysis and measurement of postvoid residual (PVR). Advanced diagnostic studies may be required for patients with red flags in urinary incontinence or incontinence refractory to treatment. Management depends on the underlying cause and may involve conservative measures (e.g., management of comorbidities, pelvic floor exercises, bladder training), pharmacological treatment, minimally invasive procedures, or anti-incontinence surgery. Untreated UI can lead to skin irritation and urinary tract infection (UTI) and potentially result in negative effects on a patient's psychosocial well-being, mobility, and independence.
For the management of stress urinary incontinence and overactive bladder and urgency urinary incontinence, see the respective articles.
Epidemiology
-
Prevalence [1]
- Increases with age
- Up to 50% of women and up to 25% of men older than 65 years are affected.
-
Sex: ♀ > ♂ (2:1) [2]
- SUI and mixed incontinence are the most common types of incontinence in female patients.
- UUI is the most common type in male patients.
Epidemiological data refers to the US, unless otherwise specified.
Etiology
- Idiopathic
-
Neurological causes
- Multiple sclerosis
- Spinal injury
- Normal-pressure hydrocephalus
- Dementia
- Delirium
-
Genitourinary causes
- Trauma to the pelvic floor
- Intrinsic sphincter deficiency
- Urethral hypermobility in women
- Impaired detrusor contractility
- Bladder outlet obstruction
- Pelvic floor weakness
- Urogenital fistula
-
Transient causes of urinary incontinence
- Drugs (e.g., diuretics)
- UTI
- Postmenopausal atrophic urethritis
- Psychiatric causes (especially depression, delirium/confused state)
- Excessive urinary output (in conditions like hyperglycemia, hypercalcemia, CHF)
- Stool impaction
- Impaired mobility
-
General risk factors
- Recurrent UTI
- Obesity
- Caffeine
- Alcohol
To remember the reversible causes of acute urinary incontinence, think DIAPPERS: Delirium/confusion, Infection, Atrophic urethritis/vaginitis, Pharmaceutical, Psychiatric causes (especially depression), Excessive urinary output (hyperglycemia, hypercalcemia, CHF), Restricted mobility, Stool impaction.
Overview
| Overview of urinary incontinence [3][4][5] | |||
|---|---|---|---|
| Underlying mechanism | Clinical features | Treatment | |
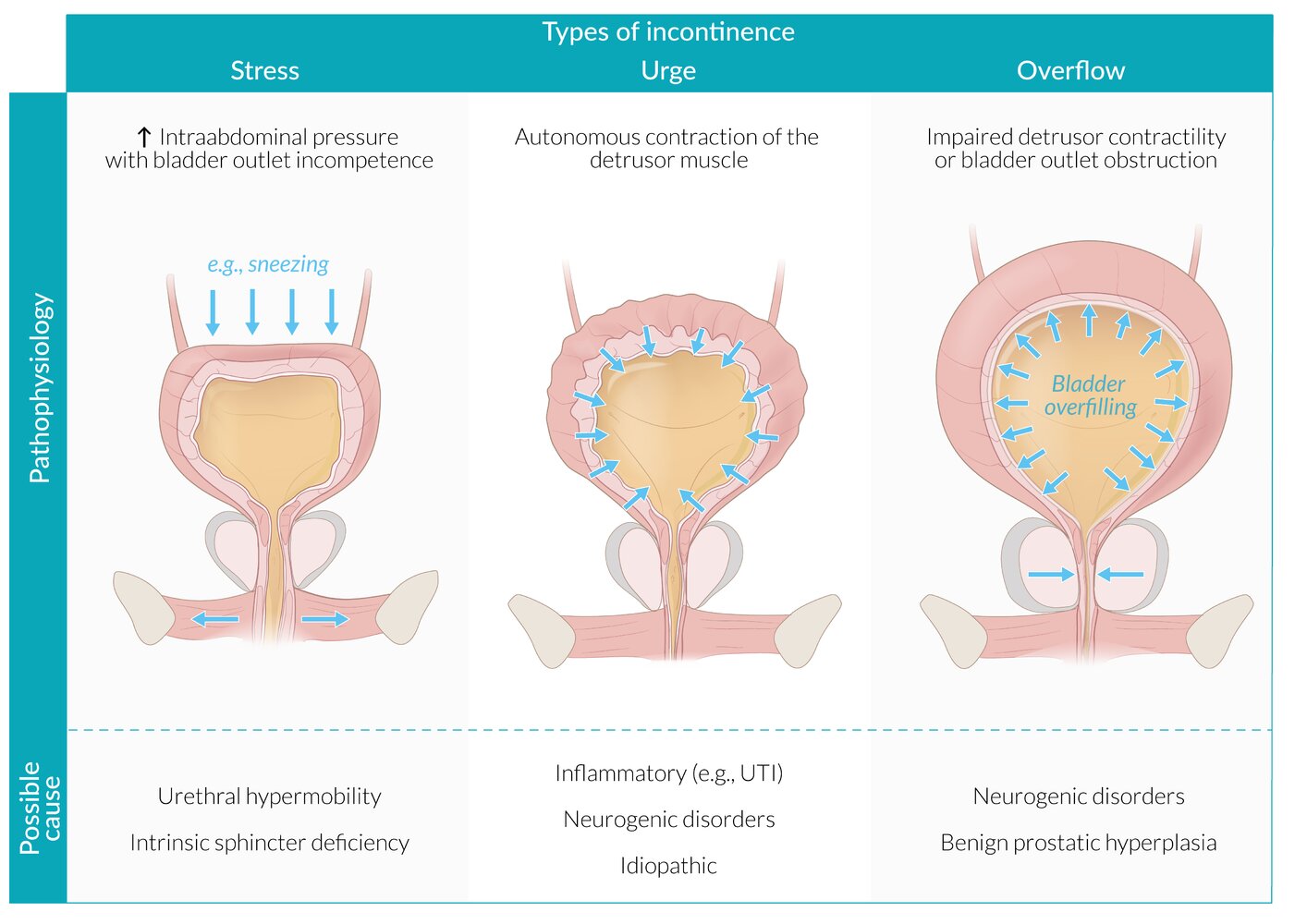
| Stress urinary incontinence |
|
|
|
| Urgency urinary incontinence [6] |
|
|
|
| Mixed incontinence |
|
|
|
| Total incontinence |
|
|
|
| Overflow incontinence (overflow bladder) [10] |
|
|
|
| Neurogenic lower urinary tract dysfunction [13][14][15] |
|
|
|
|
|
||
|
|
||
| Giggle incontinence [16] |
|
|
|
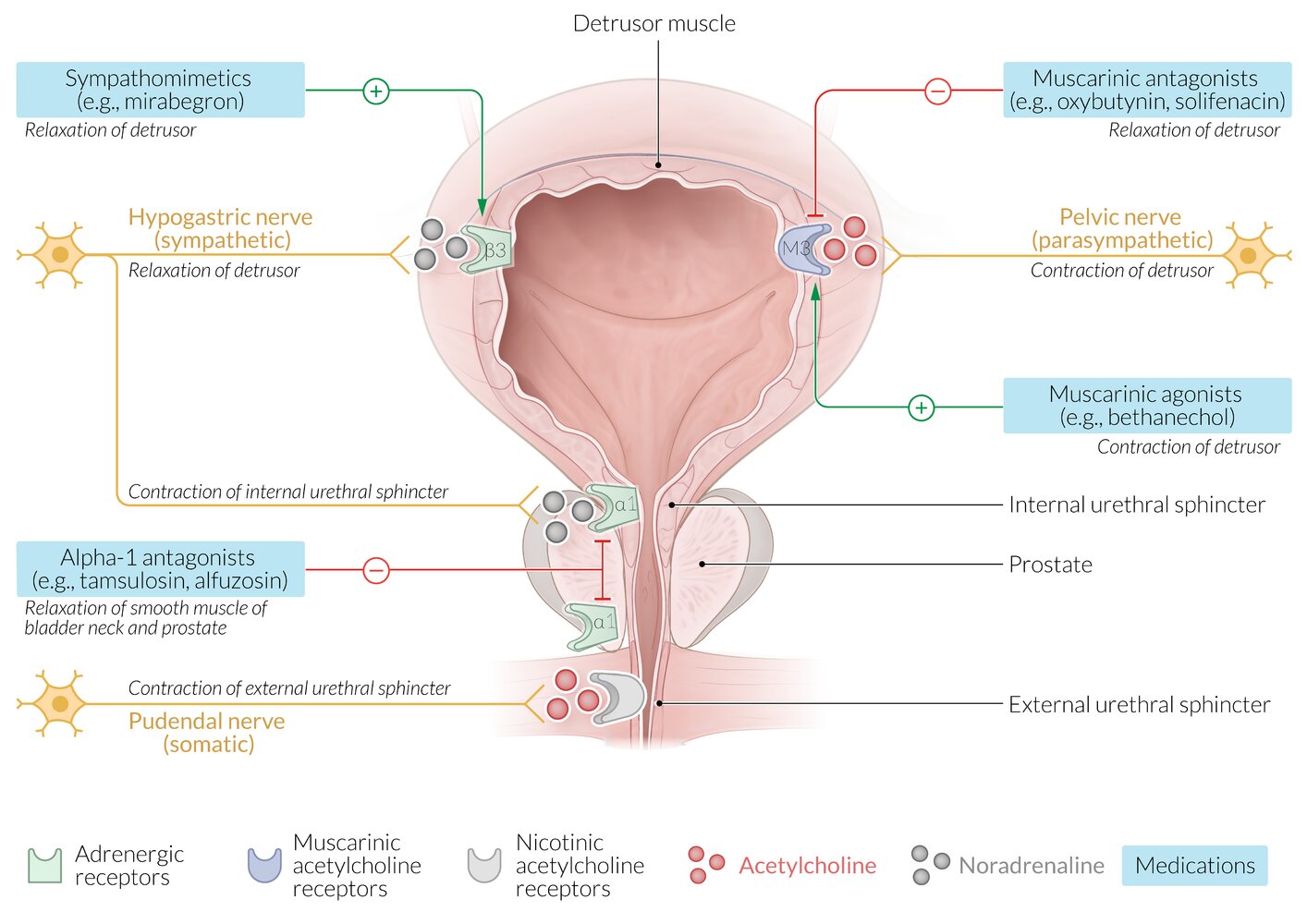
Neural control of micturition: parasympathetic nervous system → S2–S4 ventral root → inferior hypogastric plexus → contraction of the detrusor muscle → voluntary relaxation of the external urethral sphincter muscle via the pudendal nerve → micturition
SUI is caused by urethral dysfunction, while UUI is caused by bladder dysfunction. Mixed incontinence is a combination of both. [17]

")
")
© AMBOSS
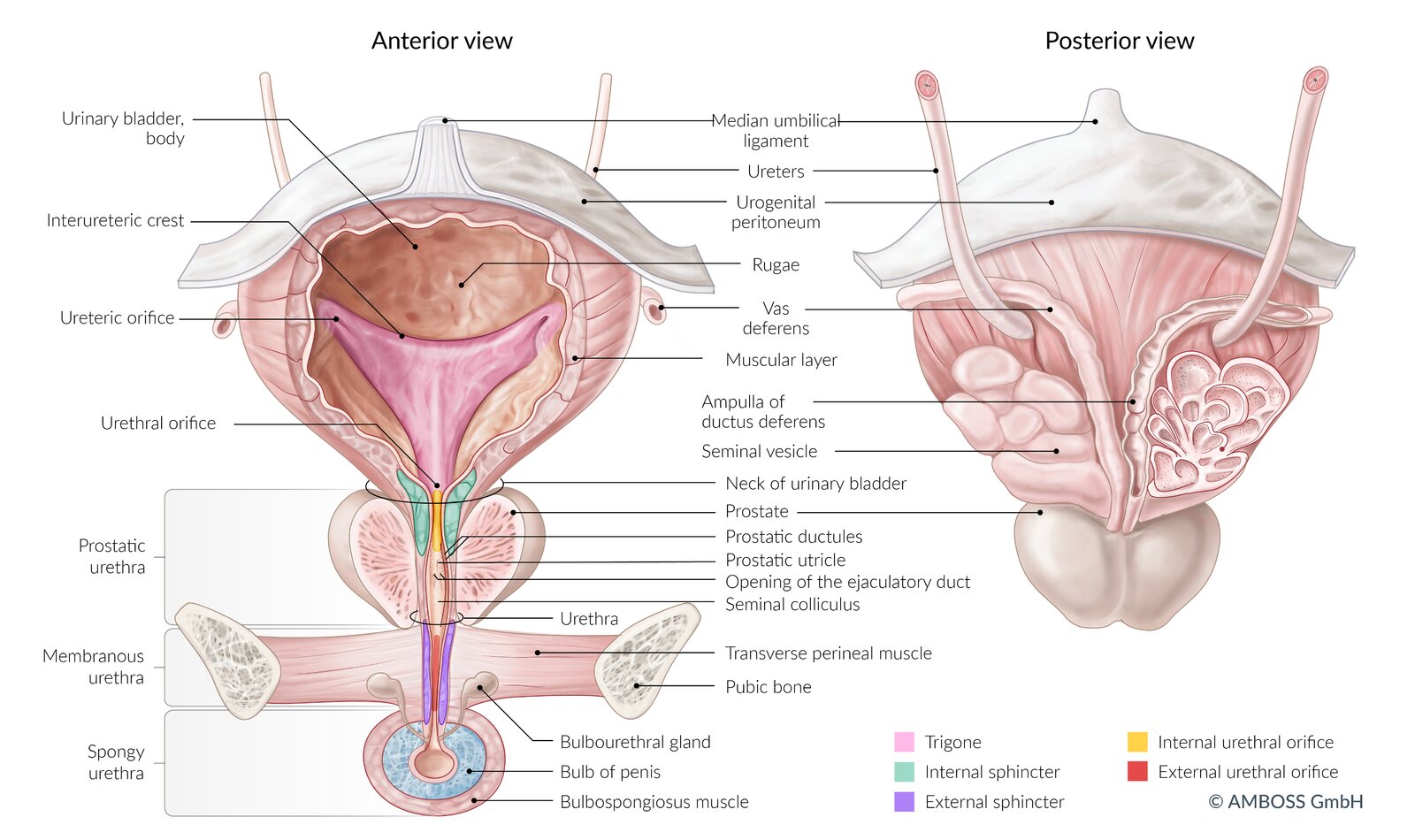
Left: ventral view of the bladder, urethra, prostate, and penis (coronal section)
Right: dorsal view of the bladder, seminal vesicles, terminal ureters, and prostate
The coronal section of the seminal vesicle and vas deferens is depicted on the right.
© AMBOSS
© AMBOSS
Diagnosis
Approach
- All patients
- Perform an initial evaluation for urinary incontinence.
- Screen for red flags in urinary incontinence.
- Suspected upper urinary tract involvement : Obtain renal ultrasound and laboratory studies.
- Red flags in urinary incontinence present or refractory incontinence: Refer to a specialist for advanced studies.
Red flags in urinary incontinence [3][5][17]
Refer to urology or urogynecology for specialist workup if any of the following features are present:
- Associated pain
- Persistent hematuria or proteinuria
- Elevated PVR
- Symptoms suggestive of obstruction
- Suspected fistula
- Pelvic organ prolapse
- Recurrent UTIs
- Incontinence after radiation, radical pelvic surgery, or previous incontinence surgery
Initial evaluation for urinary incontinence [3][4][18]
Focused history
- Use a validated incontinence questionnaire if possible. [3][5]
- Inquire about symptoms that occur with voiding.
- Assess for barriers to voiding (e.g., limited mobility, which may delay patients reaching the bathroom).
- Ask patients to record fluid intake and micturition for 3–5 days using a voiding diary.
- Obtain a relevant social and medical history, including:
- Transient causes of urinary incontinence
- Local causes (back, bowel, gynecologic, or bladder surgery; constipation; pelvic organ prolapse)
- Systemic conditions (congestive heart failure, chronic cough , neurological disease)
- Contributing dietary and lifestyle factors.
Physical examination [3][17]
- Lower abdominal examination: Evaluate for bladder distention and masses.
- Digital rectal examination: Assess for fecal impaction, prostatomegaly, masses, and decreased anal sphincter tone.
- Pelvic examination: Evaluate for pelvic organ prolapse, vaginal atrophy, masses, and vaginitis. [3]
- Cardiovascular examination: Assess for signs of fluid overload (may worsen urge incontinence).
-
Neurological examination: Both spinal and cerebral pathologies can cause incontinence (see “Etiology”).
- Assess motor function of the lower extremities and sensation of the sacral dermatomes.
- Consider cognitive testing.
Initial diagnostics
The following outlines a general approach for the workup of undifferentiated incontinence.
- Urinary stress test: performed for all patients to distinguish SUI from other types of UI [5]
-
Urinalysis
- Positive urinary nitrites and/or leukocyte esterase: suggestive of a UTI; send urine culture.
- Isolated microhematuria: obtain diagnostics for hematuria [19]
- Glucosuria: If present, screen for diabetes. [20]
-
Postvoid residual (PVR) [10]
- Indications [3][5][17]
- Suspected overflow incontinence
- Diagnostic uncertainty
- Patients being considered for specialist referral
- Findings: Elevated PVR suggests either decreased bladder contractility or urethral obstruction. [4][17]
- Indications [3][5][17]
-
Pad test: Consider to determine symptom severity. [21][22]
- Performed over a set period of time ranging from 1–24 hours
- Patients drink a set amount of fluids before performing specific activities while wearing preweighed incontinence pads.
- The pad is weighed again after the trial to determine the volume of incontinence.
Perform a urinary stress test in all patients to distinguish between SUI and UUI.
Differentiation between types of incontinence
| Diagnostic overview of types of incontinence [17] | |||
|---|---|---|---|
| Clinical history | Urinary stress test | Postvoid residual | |
| Stress urinary incontinence |
|
|
|
| Urgency urinary incontinence |
|
|
|
| Overflow incontinence |
|
|
|
| Functional urinary incontinence |
|
|
|
| Patients with features of both SUI and UUI have mixed incontinence. | |||
Upper urinary tract studies [3][23]
-
Renal ultrasound
- Indications include:
- Hematuria
- Neurogenic incontinence
- Elevated PVR
- Comorbid renal disease
- Findings may show:
- Hydronephrosis associated with overflow incontinence
- Urinary tract pathology, e.g., malignancy
- Indications include:
- Creatinine and BUN: may be elevated in patients with overflow incontinence
Only perform upper urinary tract studies if the initial assessment indicates a possible renal pathology and/or renal impairment due to urinary retention and vesicoureteral reflux. [5][23]
Advanced studies [3][4][24]
Advanced studies are performed under specialist guidance for patients with red flags in urinary incontinence or incontinence refractory to initial management.
- Micturating cystourethrogram: to detect vesicoureteral reflux and/or morphological abnormalities (e.g., diverticula, obstruction)
- Urodynamic studies: to determine detrusor and sphincter function
- Cystoscopy: to evaluate for tumors and vesicorectal and vesicovaginal fistulae
- Ultrasound pelvis : for suspected pelvic floor dysfunction
- MRI : to assess for pelvic floor defects, urinary tract anomalies, and masses
- CT with IV contrast: for suspected anatomical abnormalities, e.g., urinary tract masses, bladder wall thickening
Management
This section provides an overview of the management of UI. For specific information, see “Treatment of SUI,” “Treatment of UUI,” and “Treatment of urinary retention.”
Approach [3]
- Identify and manage:
- Transient causes of urinary incontinence (e.g., UTI, constipation)
- Barriers to voiding
- Risk factors for and causes of UI (see “Etiology of urinary incontinence”)
- Offer incontinence products to prevent dermatological complications and improve patient comfort.
- Educate patients on lifestyle recommendations for UI.
- Further management depends on the type of incontinence and can include:
- Pelvic floor physical therapy
- Pharmacological treatment
- Interventional management
- Refer patients with any of the following to urology or urogynecology for further management:
- Red flags in UI
- Neurogenic incontinence or total incontinence
- Refractory incontinence
Assess the impact of incontinence symptoms on the patient's daily activities and discuss their treatment goals; use shared decision-making to individualize treatment plans.
Conservative management of urinary incontinence [6][8]
Incontinence products [25]
- Offer to all patients to prevent skin breakdown and improve comfort.
- Products may be used alone or in combination and include:
- Pads and diapers
- Barrier creams
- External urinary catheters
- The following products may be considered by a specialist for refractory incontinence. [25]
- Urethral inserts
- Continence pessaries
- Penile clamps
- Indwelling catheters
Management of risk factors and causes
- Treat common comorbidities, e.g.:
- Management of obesity
- Management of diabetes mellitus
- Treatment of genitourinary syndrome of menopause [26]
- Advise smoking cessation.
- Reduce the dose of or discontinue contributing medications (e.g., diuretics).
- Refer patients with limited mobility to physical therapy and occupational therapy.
- Refer patients with SUI and UUI to pelvic floor physical therapy. [27]
Lifestyle recommendations for UI
- Limiting consumption of alcohol and caffeine (including carbonated drinks)
- Discuss appropriate fluid intake and timing throughout the day [5]
Bladder training
-
Scheduled voiding regimens and patient education are used to increase leak-free intervals. [4]
- Timed voiding: Intervals between voiding are sequentially increased until the goal of at least 3–4 hours is met.
- Relaxation and distraction techniques: used to suppress the urge to urinate
- Indications: UUI, but also effective for SUI and mixed incontinence
Pharmacological treatment
- Used in the management of UUI, urinary retention, or outlet obstruction
- Adverse effects and interactions may limit use (see “Pharmacotherapy in older adults”).
| Autonomic drugs used to treat bladder incontinence [3][4][5] | ||
|---|---|---|
| Drug group | Indications | Mechanism of action |
| Muscarinic antagonists e.g., oxybutynin |
|
|
| Beta-3 agonists (sympathomimetics) e.g., mirabegron |
|
|
| Muscarinic agonists e.g., bethanechol [10][12] |
|
|
| Alpha-1 antagonists e.g., tamsulosin |
|
|
The use of muscarinic agonists may lead to urinary urgency, while the use of sympathomimetics or muscarinic antagonists may lead to urinary retention, especially if there is an untreated outlet obstruction. [3]
No pharmacological treatments are FDA-approved for SUI; management is either conservative (e.g., physiotherapy) or surgical. [4]

Interventional management
- Minimally invasive procedures
- For SUI: periurtheral bulking
- For UUI: sacral neuromodulation, botulinum toxin injections, posterior tibial nerve stimulation
-
Anti-incontinence surgery
- Choice of procedure depends on type of incontinence
- See “Treatment of SUI,” “Treatment of UUI,” and “Treatment of urinary retention” for more information.
© AMBOSS
Special patient groups
Urinary incontinence in older adults [3]
Overview
- Management of older patients is similar to that of other populations but with some modifications.
- Functional incontinence due to cognitive or mobility impairment is more common than in younger patients.
- Comorbid conditions and polypharmacy can make pharmacological management challenging.
Modifications to diagnostics for UI
- Screen for transient causes of urinary incontinence.
- Consider cognitive testing and functional testing in all patients.
- Limit PVR measurement to patients with any of the following:
- Diabetes mellitus
- Recurrent UTIs
- History of prior urinary retention, high PVR, bladder outlet obstruction, or detrusor underactivity
- No improvement following pharmacological treatment of UUI
- Medication use that delays bladder emptying
- Severe constipation
Modifications to the management of UI
- Consider life expectancy, goals of care, and the patient's and/or caregiver's ability to manage therapy when planning treatment.
- Prompted voiding may be helpful for older patients with cognitive impairment. [3]
- Start any medications at the lowest dose possible and follow up frequently to assess for adverse effects.
- Consider specialist referral if conservative therapies fail or other chronic conditions need to be addressed (e.g., dementia, functional impairment).
Urinary incontinence in pregnancy [10]
- SUI is common during pregnancy; the incidence rises as gestation progresses. [10][28]
- Conservative management of UI is recommended during pregnancy and the early postpartum period. [28]
Prevention
Prevention [22]
- Lifestyle modifications may help reduce the risk of UI.
- Diet rich in fruits, vegetables, and whole grains
- Regular exercise
- Recommend pelvic floor muscle exercises for:
- Pregnant and postpartum individuals
- Individuals following prostatectomy
- Manage risk factors for and causes of UI.
Screening
- Consider screening all women for UI at the annual preventive care visit. [29][30]
- Ask patients if they have experienced symptoms of UI in the last year and how these impact their lives. [29]
- For patients reporting symptoms of UI, perform an initial evaluation for urinary incontinence.
There are currently no screening recommendations for urinary incontinence in men.
Complications
- Mental health: depression, psychosocial distress
- Dermatologic: dermatitis, skin infections, sores [31]
- Environmental: decreased independence
- Urinary tract: : increased risk of UTIs
We list the most important complications. The selection is not exhaustive.
External Resources
References
- Nitti VW. "The prevalence of urinary incontinence". Rev Urol. 3(Suppl 1). :S2-6. (2001)
- Gorina Y, Schappert S, Bercovitz A, et al. "Prevalence of Incontinence Among Older Americans". Vital Health Stat. 3(36). (2014)
- Abrams P, Andersson KE, Apostolidis A, et al. "6th International Consultation on Incontinence. Recommendations of the International Scientific Committee: Evaluation and Treatment of Urinary Incontinence, Pelvic Organ Prolapse and Faecal Incontinence". Neurourol Urodyn. 37(7). :2271-2272. (2018)
- Khandelwal C, Kistler C. "Diagnosis of urinary incontinence". Am Fam Physician. 87(8). :543-50. (2013)
- Hu JS, Pierre EF. "Urinary Incontinence in Women: Evaluation and Management". Am Fam Physician. 100(6). :339-348. (2019)
- Rizvi RM, Ather MH. "Assessment of Urinary Incontinence (UI) in Adult Patients". InTech. (2017). ISBN: 9789535129318
- American College of Obstetricians and Gynecologists. "Practice Bulletin No. 155: Urinary Incontinence in Women (Reaffirmed 2022)". Obstet Gynecol. 126(5). :e66-e81. (2015)
- Barocas DA, Boorjian SA, Alvarez RD, et al. "Microhematuria: AUA/SUFU Guideline". J Urol. 204(4). :778-786. (2020)
- Danforth KN, Townsend MK, Curhan GC, Resnick NM, Grodstein F. "Type 2 Diabetes Mellitus and Risk of Stress, Urge and Mixed Urinary Incontinence". J Urol. 181(1). :193-197. (2009)
- Abrams P, Cardozo L, Wagg A, Wein A. "Incontinence 6th Edition". International Continence Society. (2017). ISBN: 9780956960733
- Haylen BT, de Ridder D, Freeman RM, et al. "An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction". Int Urogynecol J. 21(1). :5-26. (2009)
- Cardozo L, Rovner E, Wagg A, Wein A, Abrams P. "Incontinence 7th Edition". International Continence Society. (2023). ISBN: 9780956960740
- Stoffel, John, et al. "Non-Neurogenic Chronic Urinary Retention: Consensus Definition, Management Strategies, and Future Opportunities". AUA White Paper. Linthicum, MD: American Urological Association. (2016)
- Khatri G, Bhosale PR, Robbins JB, et al. "ACR Appropriateness Criteria® Pelvic Floor Dysfunction in Females". J Am Coll Radiol. 19(5). :S137-S155. (2022)
- Lukacz ES, Santiago-Lastra Y, Albo ME, Brubaker L. "Urinary incontinence in women". JAMA. 318(16). :1592. (2017)
- Welk B, Baverstock RJ. "The management of mixed urinary incontinence in women". Canadian Urological Association Journal. 11(6S2). :121. (2017)
- Moore KN, Saltmarche B, Query A. "Urinary incontinence. Non-surgical management by family physicians". Can Fam Physician. 49. :602-10. (2003)
- "Choosing wisely: Don’t place an indwelling urinary catheter to manage urinary incontinence". https://web.archive.org/web/20220728141915/http://www.choosingwisely.org:80/clinician-lists/amda-indwelling-urinary-catheter/
- Lobo RA. "Treatment of the Postmenopausal Woman". Academic Press. (2007). ISBN: 9780123694430
- Gaitonde S, Malik RD, Christie AL, Zimmern PE. "Bethanechol: Is it still being prescribed for bladder dysfunction in women?". Int J Clin Pract. 73(8). :e13248. (2018)
- Ginsberg D. "The epidemiology and pathophysiology of neurogenic bladder". Am J Manag Care. 19(10 Suppl). :s191-6. (2013)
- Panicker JN. "Neurogenic Bladder: Epidemiology, Diagnosis, and Management". Semin Neurol. 40(05). :569-579. (2020)
- Ginsberg DA, Boone TB, Cameron AP, et al. "The AUA/SUFU Guideline on Adult Neurogenic Lower Urinary Tract Dysfunction: Treatment and Follow-up". J Urol. 206(5). :1106-1113. (2021)
- Fernandes L, Martin D, Hum S. "A case of the giggles: Diagnosis and management of giggle incontinence". Can Fam Physician. 64(6). :445-447. (2018)
- Farage MA, Miller KW, Berardesca E, Maibach HI. "Incontinence in the aged: contact dermatitis and other cutaneous consequences". Contact Dermatitis. 57(4). :211-217. (2007)
- Sangsawang B, Sangsawang N. "Stress urinary incontinence in pregnant women: a review of prevalence, pathophysiology, and treatment". Int Urogynecol J. 24(6). :901-12. (2013)
- Cameron AP, Jimbo M, Heidelbaugh JJ. "Diagnosis and office-based treatment of urinary incontinence in adults. Part two: treatment". Ther Adv Urol. 5(4). :189-200. (2013)
- Cody JD, Jacobs ML, Richardson K, Moehrer B, Hextall A. "Oestrogen therapy for urinary incontinence in post-menopausal women". Cochrane Database Syst Rev. (2012)
- John Schorge, Joseph Schaffer, Lisa Halvorson, et al. "Williams Gynecology". Wiley. 55(4). (2010). ISBN: 9780071472579
- Nancy O'Reilly, Heidi D. Nelson, Jeanne M. Conry, et al. "Screening for Urinary Incontinence in Women: A Recommendation From the Women's Preventive Services Initiative". Ann Intern Med. 169(5). :320-328. (2018)
- Heidi D. Nelson, Amy Cantor, Miranda Pappas, Liev Miller. "Screening for Urinary Incontinence in Women: A Systematic Review for the Women's Preventive Services Initiative". Ann Intern Med. 169(5). :311-319. (2018)