Summary
Urinary tract cancer most commonly involves the bladder, although it may also occur in the renal pelvis, ureters, and, rarely, the urethra. The most common histological type of urinary tract cancer is urothelial carcinoma, followed by squamous cell carcinoma and adenocarcinoma. Symptomatic patients often present with painless gross hematuria and/or irritative voiding symptoms. Urinary tract cancer may also be diagnosed in patients with an incidental finding of microhematuria. All patients with unexplained gross hematuria should be evaluated for urinary tract carcinoma, while patients with microhematuria should undergo risk stratification to determine the need for further evaluation. Diagnostic evaluation includes laboratory studies, imaging, and direct visualization with collection of biopsy samples. Treatment selection is guided by histology, location, and tumor grade and stage. Upper urinary tract carcinomas (i.e., in the renal pelvis and/or ureters) and urethral carcinomas are rare, and there are no standardized treatment protocols. For bladder cancer, nonmuscle invasive disease is treated with transurethral resection of the bladder tumor (TURBT) and either intravesical chemotherapy or bacillus Calmette-Guérin (BCG). Muscle invasive bladder cancer is usually treated more aggressively with neoadjuvant chemotherapy followed by radical cystectomy. Metastatic bladder cancer is managed with palliative chemotherapy. Disease recurrence is common; therefore, close follow-up surveillance is required.
Renal cancer is covered separately in “Renal cell carcinoma.”
Epidemiology
- Sex: : ♂ > ♀ [1]
-
Race
- Transitional cell carcinoma: White individuals > African American (2:1) [2]
- Squamous cell carcinoma: most common in African Americans [3]
- Peak incidence: 60–70 years [3][4]
-
Cancer sites
- Bladder (90%)
- Renal pelvis and renal calyces (8%)
- Ureter and urethra (2%)
-
Histological types
- Transitional cell (urothelial) carcinoma: most common (∼ 95%) type of cancer of the bladder, ureter, renal pelvis, and proximal urethra in male individuals
- Squamous cell carcinoma: most common (∼ 60%) type of cancer of the distal urethra in male individuals and the entire urethra in female individuals
- Adenocarcinoma: the rarest type of urinary tract cancer (< 5%) [5][6]
")
")
References:[7]
Epidemiological data refers to the US, unless otherwise specified.
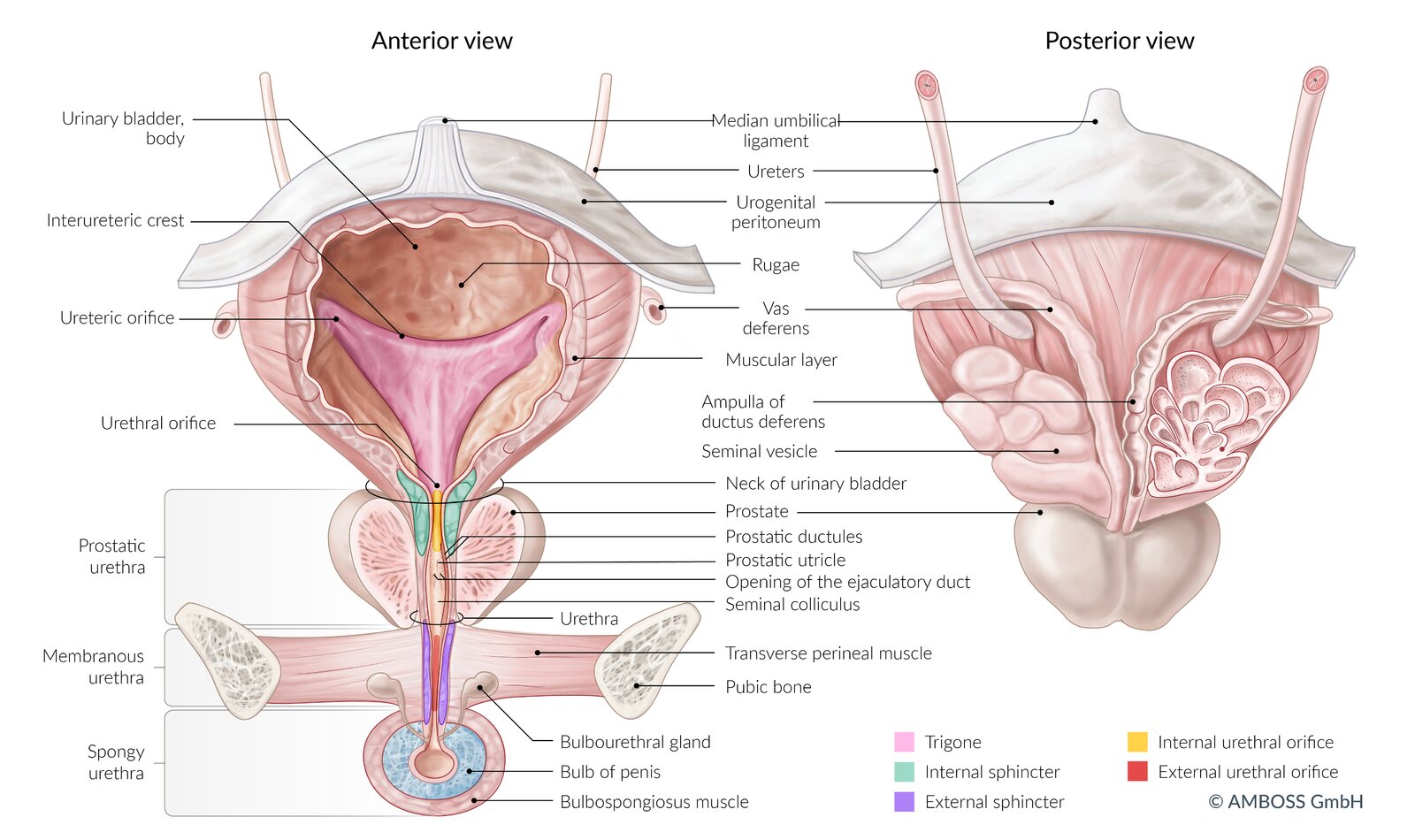
Left: ventral view of the bladder, urethra, prostate, and penis (coronal section)
Right: dorsal view of the bladder, seminal vesicles, terminal ureters, and prostate
The coronal section of the seminal vesicle and vas deferens is depicted on the right.
© AMBOSS
© AMBOSS
Risk factors
Transitional cell urothelial carcinoma [4][8][9][10]
-
Carcinogens
- Tobacco (esp. due to 2-naphthylamine in cigarette smoke)
- Aromatic amines (e.g., benzidine, aniline dye, azo dye, arylamines)
- Medications
- Cyclophosphamide
- Phenacetin
- High-dose, long-term pioglitazone treatment [11]
- Heavy metals (e.g., chlorine and arsenic content in drinking water) [12]
- Polycyclic aromatic hydrocarbons
-
Medical procedures
- Pelvic irradiation
- Augmentation cystoplasty [13]
- Kidney transplantation [14]
- Genetic predisposition: personal and family history of urothelial carcinoma (e.g., hereditary nonpolyposis colorectal cancer)
Squamous cell carcinoma [3][9][10]
-
Carcinogens
- Tobacco
- Medications: cyclophosphamide
-
Medical procedures
- Pelvic irradiation
- Previous intravesical bacillus Calmette-Guerin treatment
- Chronic indwelling bladder catheters [15]
-
Infection: chronic inflammation of the urinary tract that can lead to the transformation of urothelial cells into squamous epithelial cells (squamous metaplasia)
- Schistosomiasis (endemic throughout the Middle East and Africa, mainly in rural areas with poor sanitation near freshwater bodies)
- Chronic and/or recurrent UTIs
- Chronic nephrolithiasis and bladder calculi
- Gonococcal urethritis
Adenocarcinoma
-
Medical history
- Urachus remnant [16]
- Cystitis cystica
- Bladder exstrophy [17]
A carcinogen ACTS on the bladder: Aniline dye, Cyclophosphamide, Tobacco, Schistosomiasis
Clinical features
| Clinical features of urinary tract cancer | ||
|---|---|---|
| Location | Symptoms | Features of advanced/metastatic disease |
| Bladder carcinoma |
|
|
| Carcinoma of the renal pelvis and ureteral carcinoma |
|
|
| Urethral carcinoma |
|
|
Gross hematuria is more commonly associated with cancer than microhematuria is. [18][19]
References:[20][21][22]
Diagnosis
General principles [18][23][24]
- Follow a risk-based approach to hematuria.
- Confirm the diagnosis with imaging and direct visualization of the urinary tract.
- Staging studies for urinary tract cancer should be guided by a uro-oncologist.
Evaluate the entire urinary tract if malignancy is suspected. Use imaging to assess the renal pelvis and ureters and perform cystoscopy to assess the bladder and urethra.
Initial laboratory studies
Urine studies
- Urinalysis with microscopy: Obtain for all patients to confirm hematuria.
- Urine dipstick: high sensitivity but low specificity for hematuria [18]
Assessment of urine tumor markers is not recommended, as their diagnostic value is uncertain. [18][24]
Blood tests [18]
- Renal function tests
- Suspected metastatic disease: CBC and CMP
Imaging [19][23][24]
-
Modalities
- Preferred: CT urography [18][25]
- Alternative
- MR urography [25][26]
- Renal bladder ultrasound [24]
-
Findings
- Filling defects
- Hydronephrosis (suggestive of intraluminal tumor obstruction)
- Mural thickening
- Visualization of masses
- Evidence of disease spread (e.g., lymphadenopathy)
Perform urinary tract imaging prior to direct visualization as inflammation from instrumentation/biopsy can make radiological interpretation challenging. [18]



Direct visualization (cystoscopy/ureteroscopy) [23][24][27]
TURBT may be performed during cystoscopy if lesions are detected.
-
Indications [23][24][27]
-
Cystoscopy
- Gross hematuria
- Unexplained urinary symptoms
- Known upper urinary tract cancer: to evaluate for concurrent lesions
- Microhematuria, depending on risk stratification for microhematuria
-
Ureteroscopy
- Upper urinary tract lesion identified on imaging
- Normal results on cystoscopy but high suspicion for malignancy
-
Cystoscopy
-
Characteristic findings [20][28][29]
- Single or multiple lesions [28]
- Appearance may be a:
- Papillary, sessile, or nodular mass [29][30]
- Flat erythematous area (carcinoma in situ) [29]
- Areas of necrosis may be visible. [29]
Direct visualization is the gold standard for diagnosing urinary tract cancer. [24][31]
During cystoscopy, TURBT can allow for simultaneous diagnosis and treatment.

Pathology studies
Biopsy [24][31]
- Not routinely required: Histology is usually performed on tissue removed during TURBT.
- Image-guided or endoscopic biopsy may be used as an alternative.
- For findings, see “Pathology of urinary tract cancers.”
Urine cytology [24]
- Indication: an adjunct study for patients with gross hematuria [18][23][24]
- Findings: can detect sloughed malignant cells, especially from high-grade urothelial tumors [23]
Staging studies for urinary tract cancer [32][33][34]
- First line
- Chest x-ray and/or CT chest with IV contrast
- CT abdomen/pelvis with and without IV contrast (if not already performed)
- Consider additional studies.
- Bone scan [34]
- FDG-PET/CT scan [34]
Examination under anesthesia may be used to determine locoregional extension. [32]

CT urography (with contrast; axial plane) of a patient with transitional cell carcinoma
A hypodense mass (green overlay) is visible within the posterior bladder. Layering (red line) hyperdense contrast (C) outlines the mass.
Source: “TransCellCaMark” by James Heilman, MD, Wikimedia Commons, licensed under CC BY-SA 4.0. Modifications: removed red arrow. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 4.0.
{kind=link}
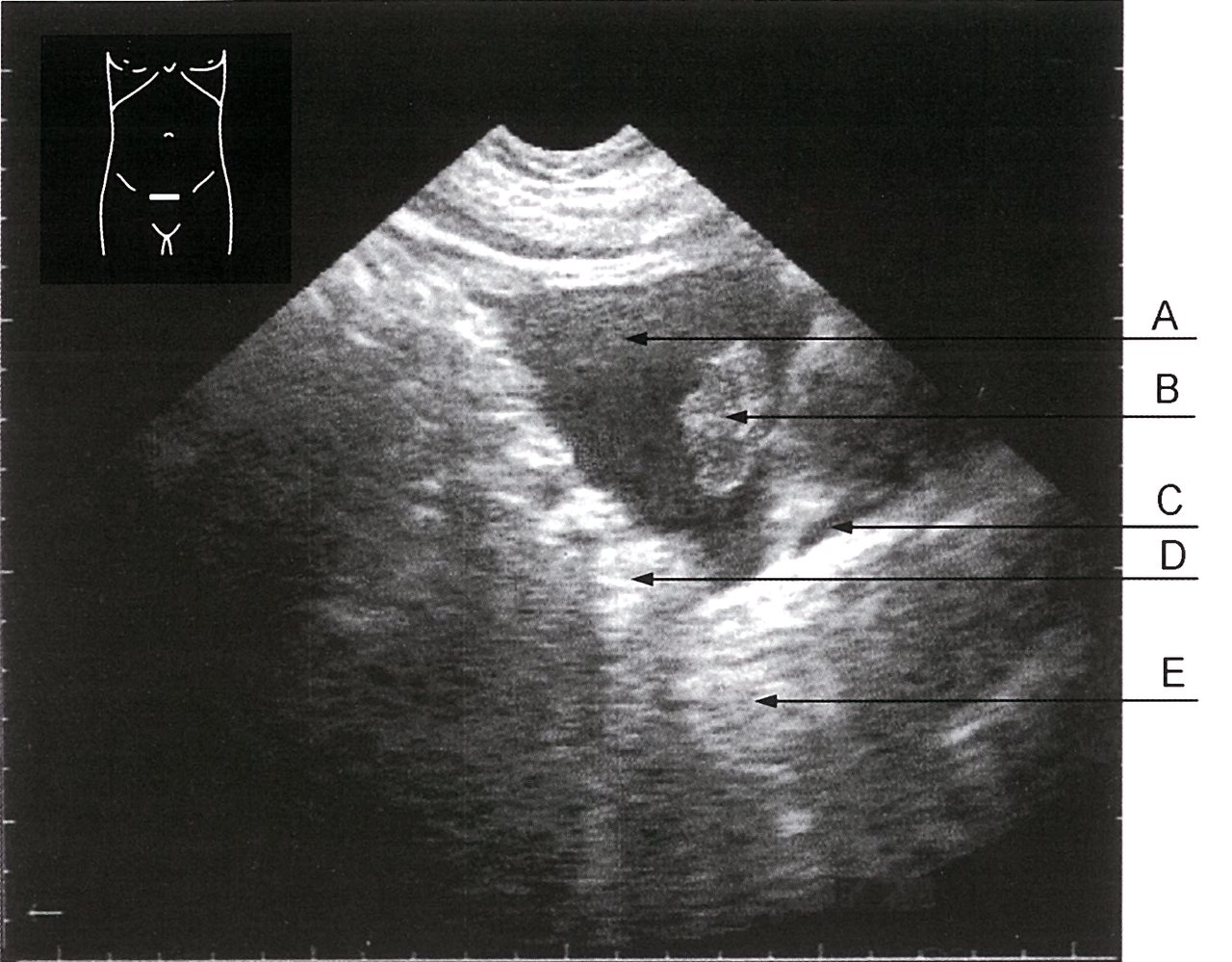
Ultrasound, transversal section of the bladder
A: hypoechoic bladder content (urine)
B: papillary urothelial carcinoma
C: thin, hypoechoic structure, likely to be the filled seminal vesicle or vessels
D: hyperechoic structure, likely to be the enlarged wall of the bladder or fat tissue
E: hyperechoic structure below the bladder (prostate gland)
Source: © IMPP
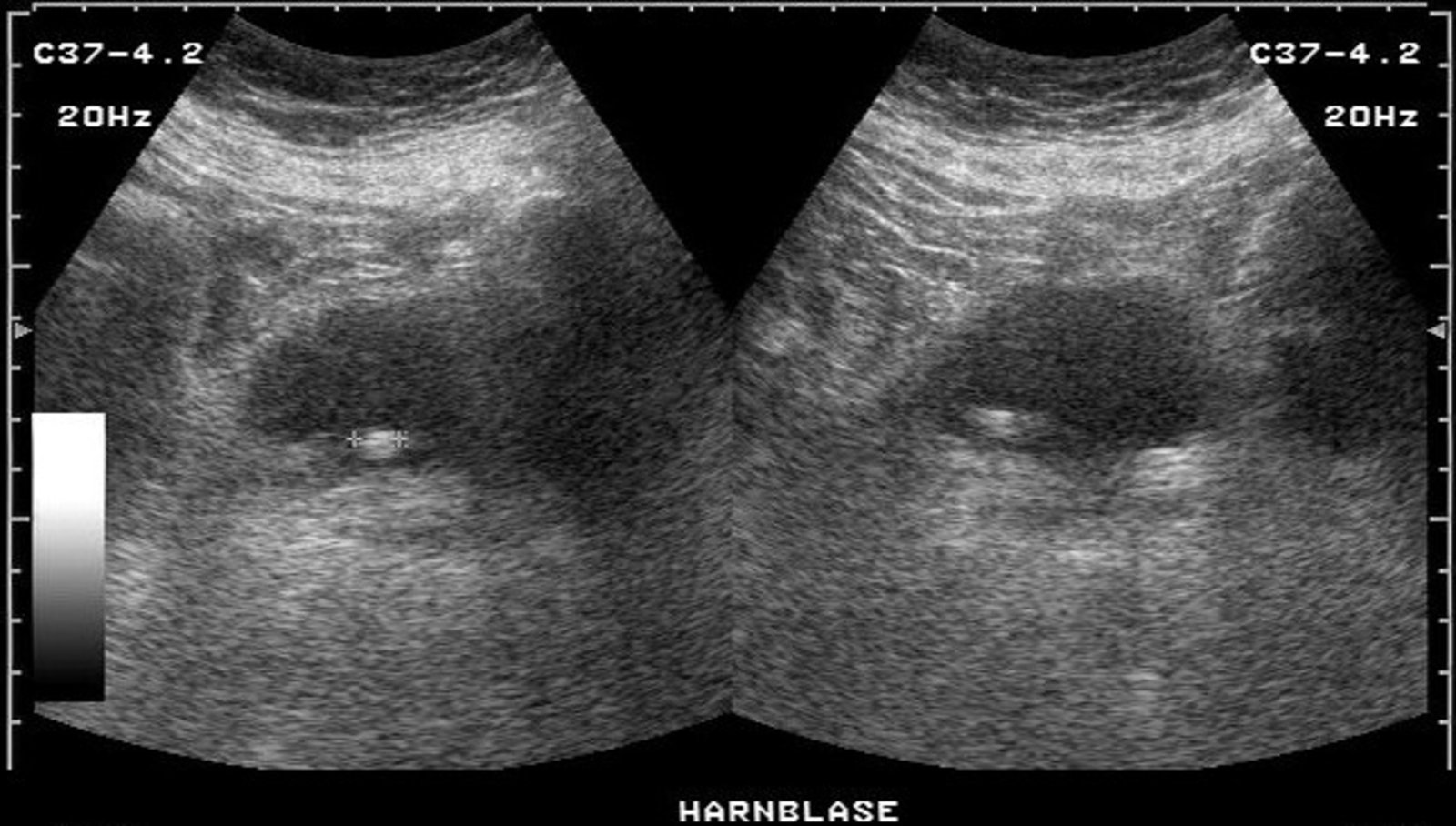
Ultrasound of the bladder (sagittal plane, left; transverse plane, right)
The urinary bladder (white dashed border) shows an hyperechoic oval mass (green overlay).
Possible diagnoses include a bladder stone or a urinary bladder polyp or tumor with an exophytic growing pattern.
Our great thanks to Dr. Kissig (Center for Diagnostic and Interventional Radiology, Hedwigshöhe, St. Hedwig, Berlin, and St. Josefs Hospital, Potsdam) for kindly providing this image.

Endoscopic view of the bladder
A lateral bladder wall lesion is visible during bipolar transurethral resection.
Source: “Figure 2, in: NBI cystoscopy and bipolar electrosurgery in NMIBC management – An overview of daily practice” by Geavlete B, Stănescu F, Moldoveanu C et al., Journal of Medicine and Life, licensed under CC BY 4.0.
Pathology
-
Papillary urothelial carcinoma
- A thick papilla with a fibrovascular core
- CIS: focal or diffuse erythematous, flat, velvety lesion(s) in the bladder mucosa [29]
- Low-grade tumors: usually pedunculated with a papillary surface; and noninvasive [29][30]
- High-grade tumors: usually sessile and nodular/solid; and invasive (invading lamina propria or deeper tissues) [29][30]
-
Squamous cell carcinoma
- Chronic inflammatory stimuli (e.g., schistosomiasis, chronic cystitis) can lead to transformation of urothelial cells into squamous epithelial cells (squamous metaplasia)
- Squamous epithelial cells that are constantly exposed to urine are prone to dysplasia and squamous cell carcinoma


")


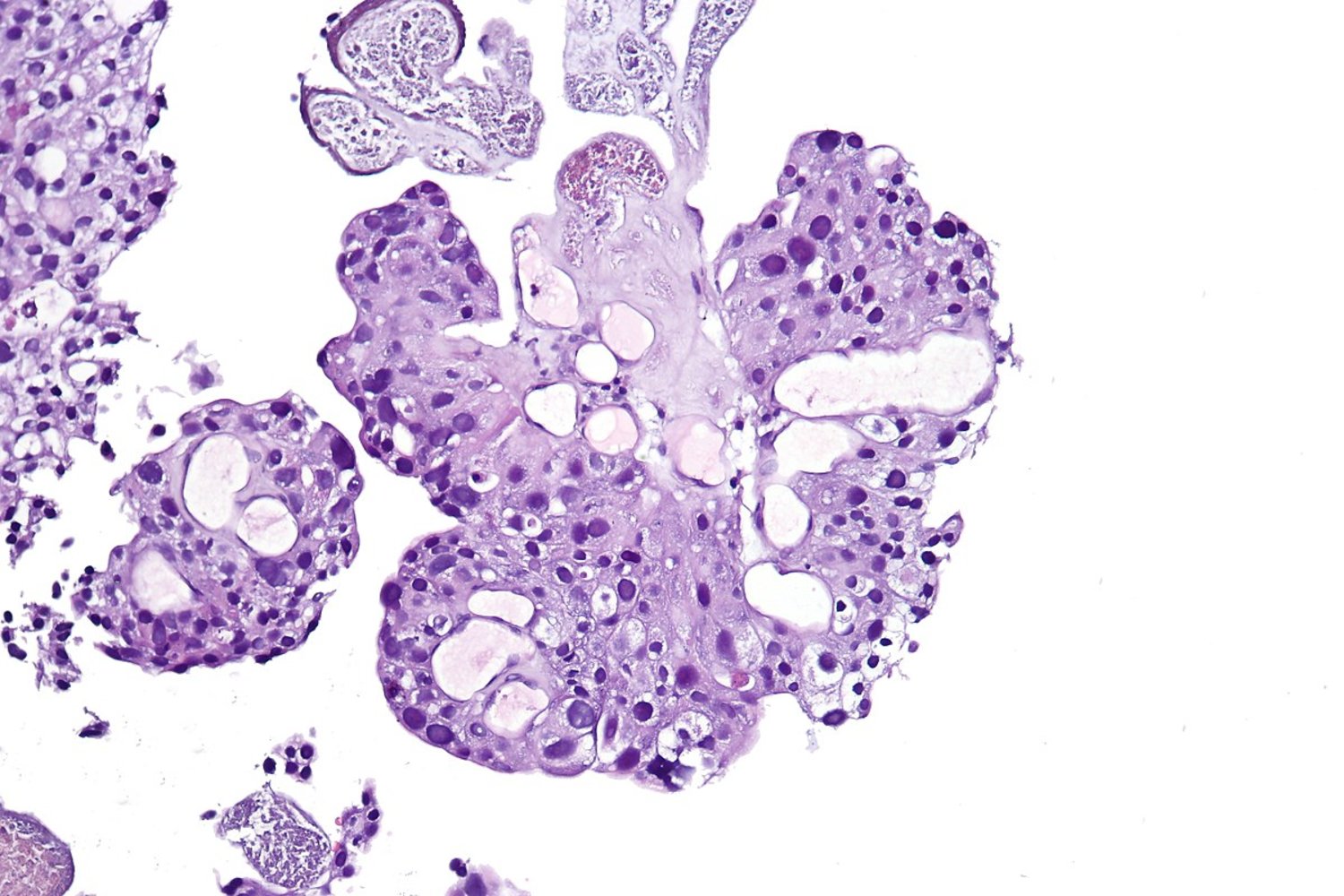
Photomicrograph of a bladder tumor biopsy specimen (H&E stain)
A thick papilla with a fibrovascular core (red overlay) can be seen in the center.
The urothelium (green overlay) appears hyperplastic and the normal stratification of the urothelial cells is absent.
The nuclei of the urothelial cells are large and deeply staining (nuclear atypia).
The basal cells of the urothelium are not in contact with the basement membrane (loss of polarity).
These features are characteristic of papillary urothelial carcinoma.
Source: “Papillary urothelial carcinoma (high-grade), high mag.2” by CoRus13, Wikimedia Commons, licensed under CC0 1.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
,_high_mag.2.jpg){kind=link}
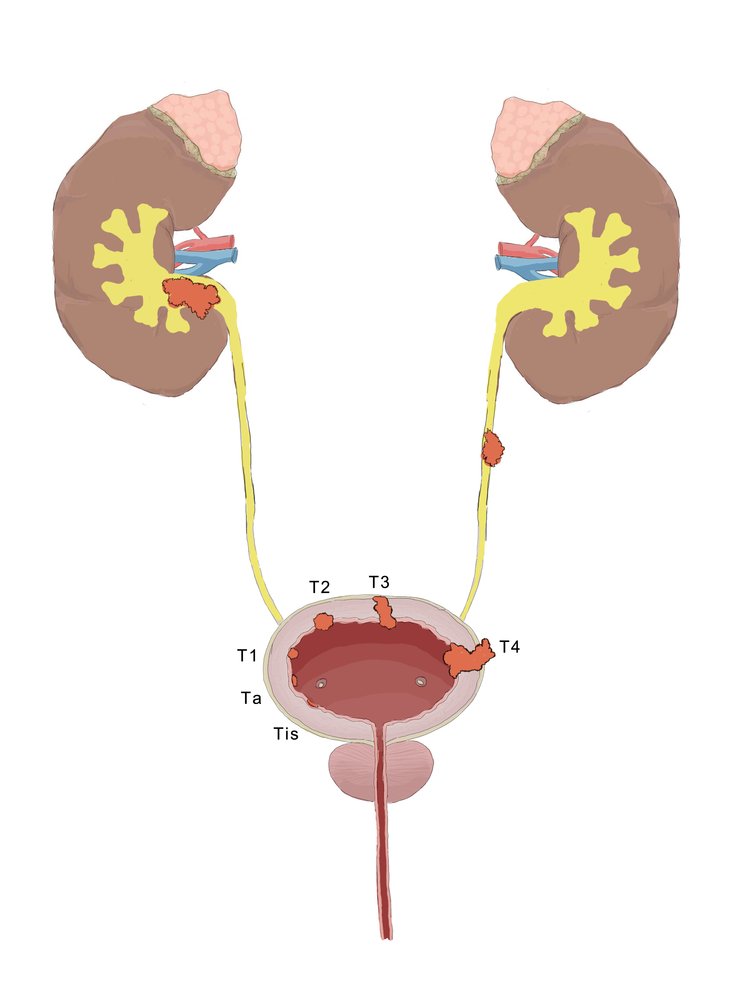
Ta: non-invasive papillary carcinoma; Tcis: carcinoma in situ (flat tumor); T1: tumor invades the lamina propria to the subepithelial connective tissue (lamina submucosa); T2: tumor invades the lamina muscularis; T3: tumor invades the perivesical fat; T4: tumor invades adjacent organs
© AMBOSS
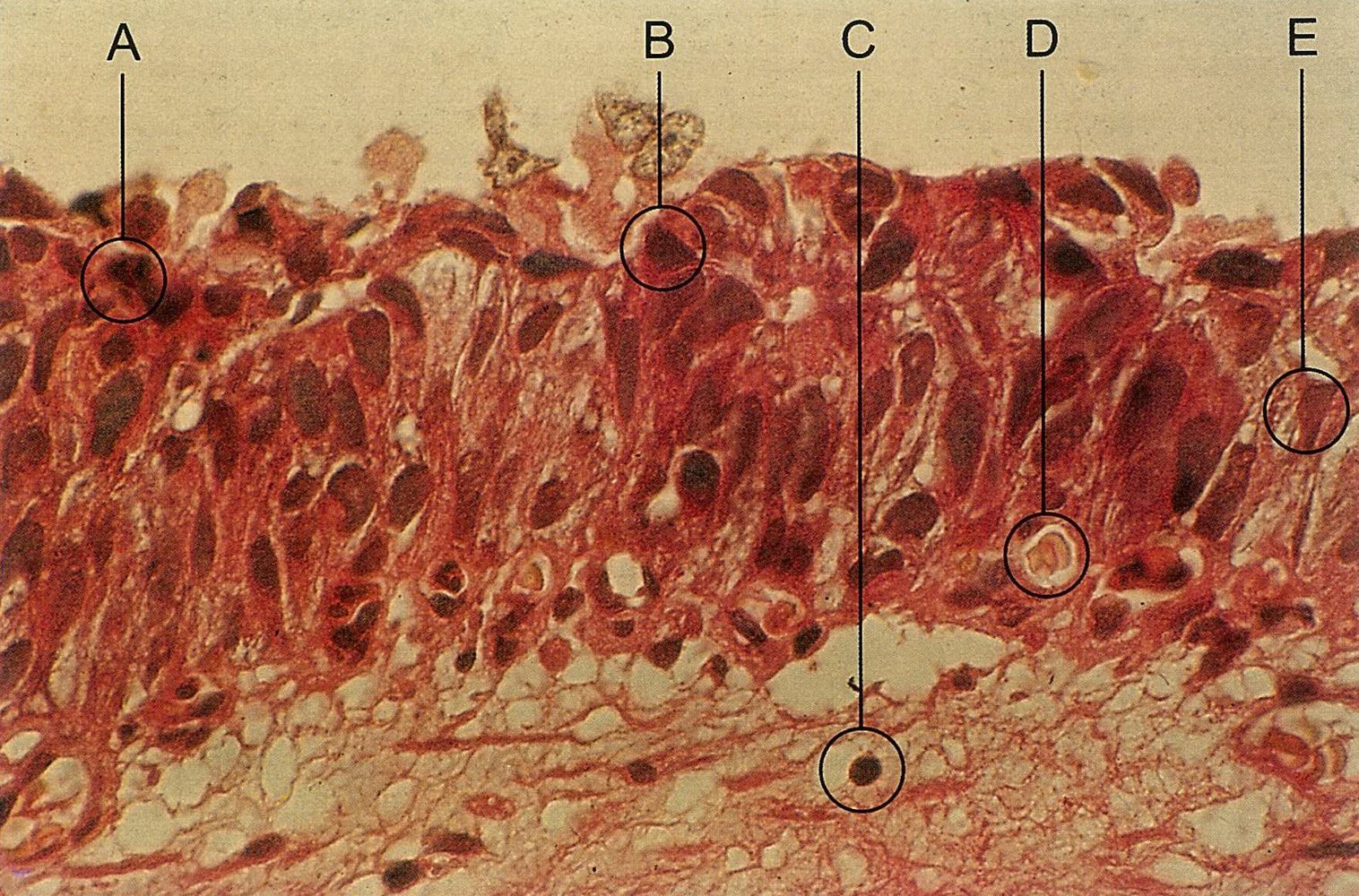
Photomicrograph of urothelial tissue (H&E stain; 750x magnification)
Papillary urothelial carcinoma with lamina propria infiltration, moderately differentiated.
A) Mitotic figure
B) Urothelial cell with severe nuclear atypia; no mitotic figure
C) Small, round lymphocytes; no mitotic figure
D) Structure with a nucleus
E) Atypical urothelial cell; no mitotic figure
Source: © IMPP
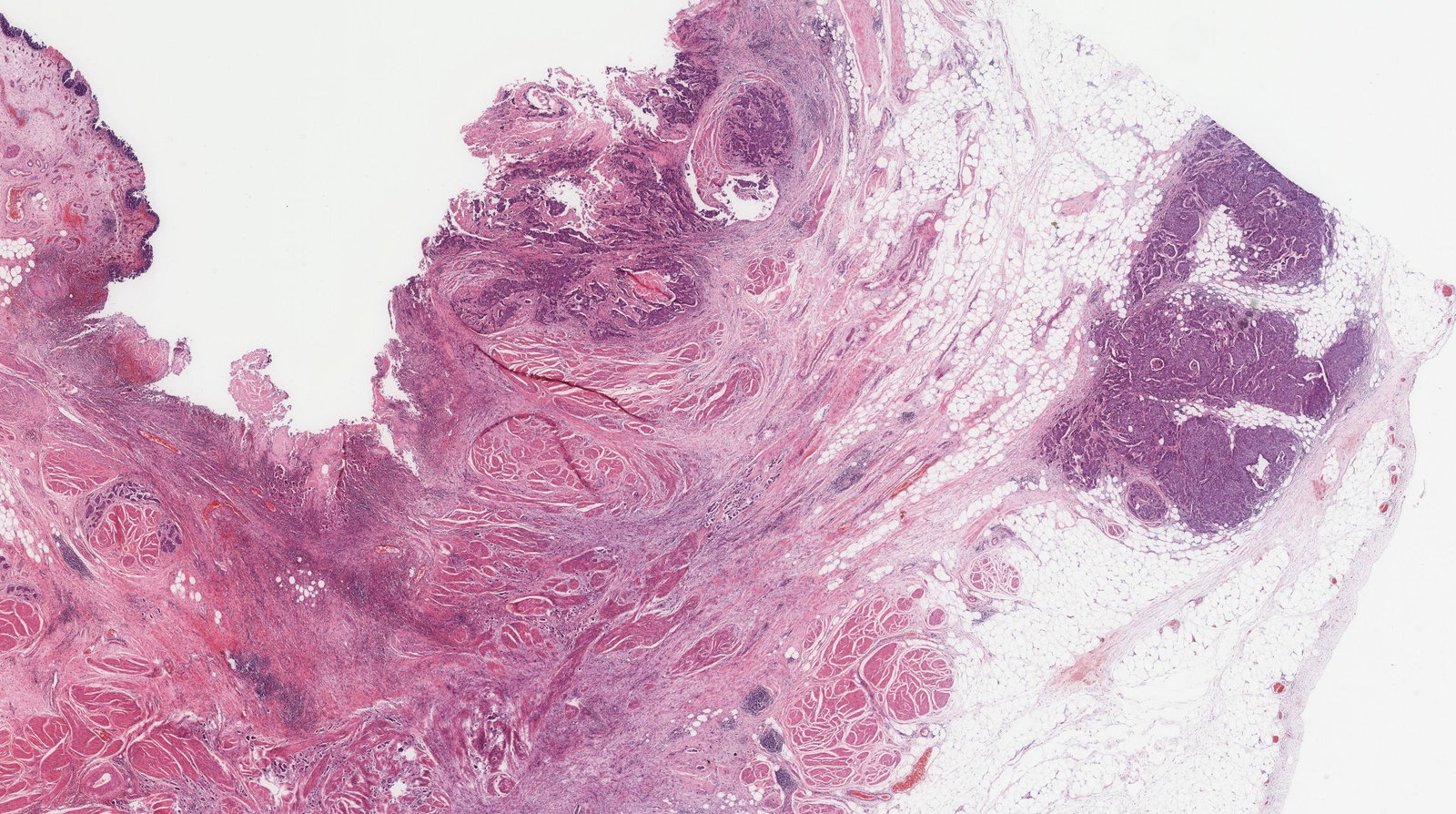
Photomicrograph of bladder tissue (H&E stain, 75x magnification)
Green overlay: deepest invasive tumor front
Black arrow: urothelium
White arrow: bladder muscularis of bladder
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. med. Alberto Perez Bouza, Facharzt für Pathologie
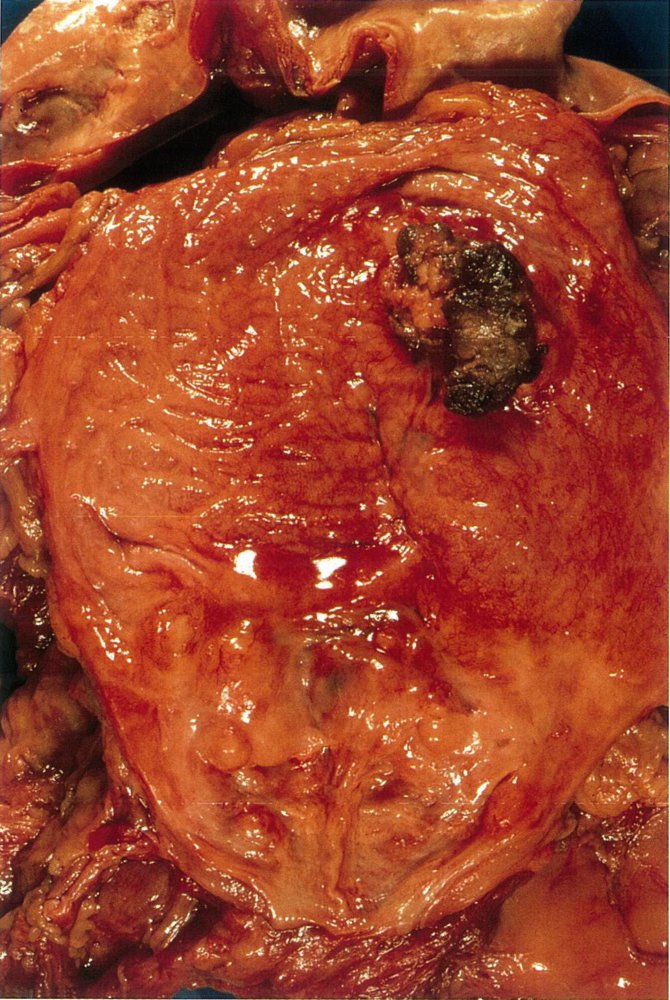
A prepared and open bladder of a 70-year-old patient with urothelial cancer
An exophytic tumor with a black necrotic surface (green shaded area) originating from the urothelium can be seen.
Source: © IMPP
Differential diagnoses
Other causes of hematuria and flank pain
- Urolithiasis
- Infections: cystitis, urethritis
- Renal cell carcinoma
- Glomerular disease, nephropathies
- Systemic disease (e.g., SLE, GPA, IgA vasculitis)
- Coagulopathy
- Trauma (see “Traumatic injuries of the kidney and bladder”)
- Physical strain, rhabdomyolysis
References:[35][36]
The differential diagnoses listed here are not exhaustive.
Treatment
This article primarily discusses treatment options for urothelial carcinoma, as squamous cell carcinoma and adenocarcinoma of the urinary tract are less common and protocols are less established.
General principles
- Treatment usually consists of surgical resection along with neoadjuvant chemotherapy and/or radiation therapy.
- Metastatic disease is managed with palliative systemic chemotherapy, and, in some cases, palliative surgery (e.g., removal of urethral obstructions).
Treatment of bladder cancer
Bladder cancer is the most common urothelial cancer; treatment differs based on the presence of muscular invasion and/or metastases.
Nonmuscle invasive [37]
-
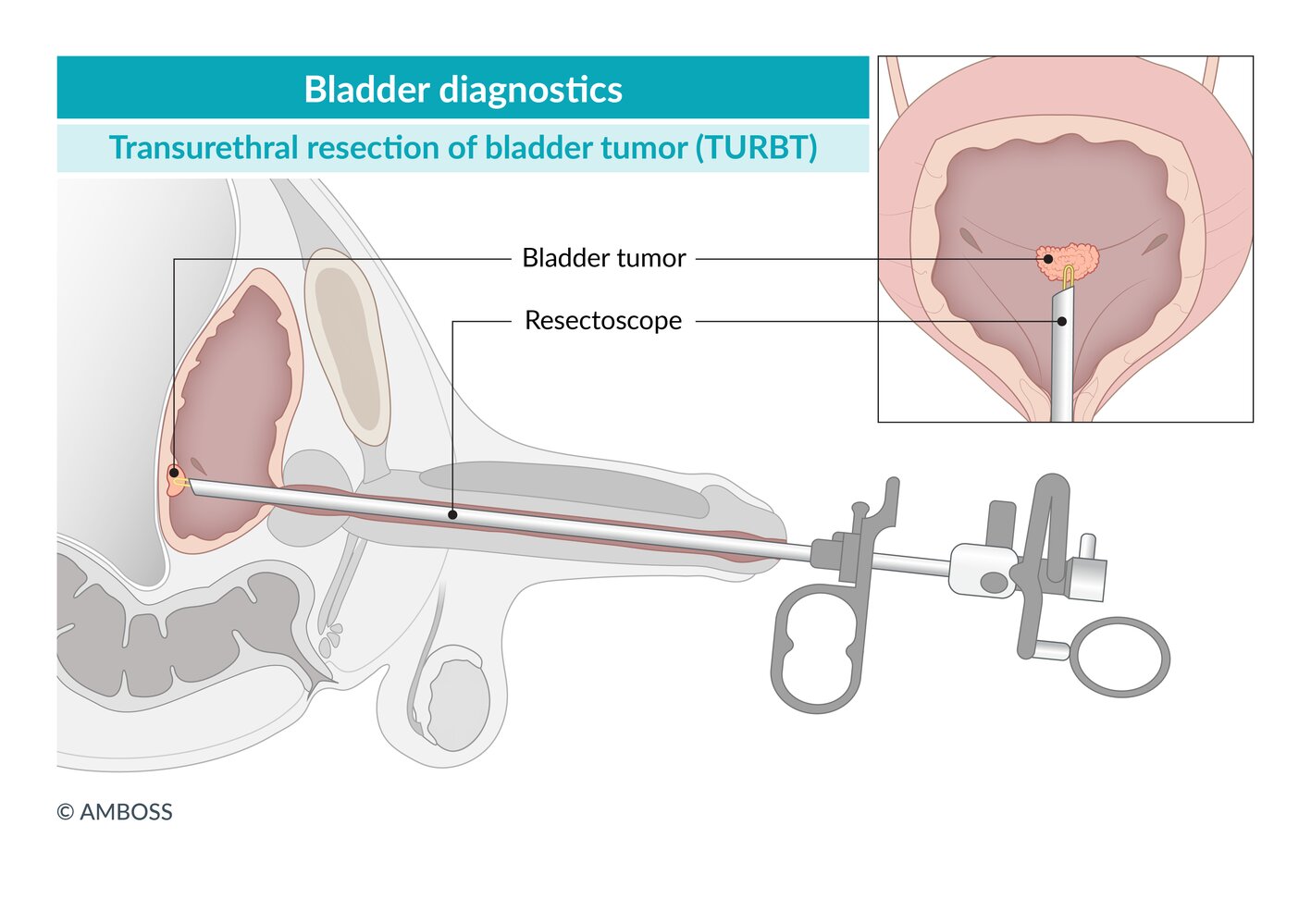
First line: transurethral resection of bladder tumor (TURBT)
- Indicated in all patients with visible bladder tumors on cystoscopy
- Visible tumors are resected using an electrocautery resectoscope.
- May be repeated after 4–6 weeks for high-grade or incompletely resected lesions
- Additional treatments include:
- Intravesical adjuvant chemotherapy (e.g., mitomycin C or epirubicin) [37]
- Immunotherapy with intravesical bacillus Calmette-Guérin (BCG) [37][38]
- Radical cystectomy: for refractory lesions, lymphovascular invasion, selected variants [37]

Nonmetastatic muscle invasive [32]
-
First-line treatment
- Neoadjuvant chemotherapy (cisplatin-based combination regimens)
- AND radical cystectomy with bilateral pelvic lymph node dissection and urinary diversion [32]
- For patients who are ineligible for radical cystectomy or prefer to retain their bladder, bladder-preserving treatment involves a combination of:
- Maximal debulking TURBT [39]
- Chemotherapy
- Radiation therapy [32]
Metastatic disease [40]
- First line: palliative cisplatin-based systemic chemotherapy [40]
- Palliative immunotherapy, radiation therapy, and/or surgery may also be used. [23]
Treatment of carcinoma of the renal pelvis and ureters [27]
- Upper urinary tract cancer is rare and there are no standardized treatment protocols.
- Surgical treatments include:
- Radical nephroureterectomy with or without regional lymphadenectomy: gold standard for high-grade tumors [27]
-
Kidney-sparing alternatives
- Consider for some low-grade cancers or if radical nephroureterectomy is contraindicated.
- Options include endoscopic resection or ablation, segmental ureteral resection, and distal ureterectomy.
- Medical treatments include:
- Neoadjuvant and/or adjuvant systemic chemotherapy
- Others: adjuvant topical chemotherapy or immunotherapy
Treatment of urethral carcinoma [5][41][42]
- Urethral cancer is rare and there are no standardized treatment protocols.
- Treatment is overseen by a specialist using a combination of the following:
- Surgical resection or ablation
- Radiation therapy (e.g., external beam radiotherapy, brachytherapy)
- Systemic chemotherapy
Monitoring [27][32][37]
- Urothelial carcinoma commonly recurs; therefore, close monitoring for recurrence and progression is required. [27]
- Surveillance studies may include repeat cystoscopy, imaging, and laboratory studies (e.g., urine cytology).
- The frequency of surveillance depends on patient characteristics and disease features (e.g., tumor grade and stage).
© AMBOSS
Prognosis
- 5-year survival of bladder, ureteral, and pelvic cancer is 90–95% for noninvasive disease and ∼ 12% for metastatic disease.
- Prognosis of urethral cancer is poorer (5-year survival of ∼ 45%).
References:[43]
Prevention
Routine screening for bladder cancer in asymptomatic adults is not recommended
References:[44]
External Resources
- 2020 AUA/SUFU Microhematuria Guideline
- 2020 Update to the EAU Guidelines on Upper Urinary Tract Urothelial Carcinoma
- 2017 AUA/ASCO/ASTRO/SUO Guideline for the Treatment of Non-Metastatic Muscle-Invasive Bladder Cancer
- 2016 AUA/SUO Guideline for the Diagnosis and Treatment of Non-Muscle Invasive Bladder Cancer
- 2016 ASCO Endorsement of EAU Guideline on Guideline on Muscle-Invasive and Metastatic Bladder Cancer
References
- Deltourbe L, Lacerda Mariano L, Hreha TN, Hunstad DA, Ingersoll MA. "The impact of biological sex on diseases of the urinary tract". Mucosal Immunology. 15(5). :857-866. (2022)
- Al-Husseini MJ, Kunbaz A, Saad AM, et al. "Trends in the incidence and mortality of transitional cell carcinoma of the bladder for the last four decades in the USA: a SEER-based analysis". BMC Cancer. 19(1). (2019)
- Martin JW, Carballido EM, Ahmed A, et al. "Squamous cell carcinoma of the urinary bladder: Systematic review of clinical characteristics and therapeutic approaches". Arab Journal of Urology. 14(3). :183-191. (2016)
- Soria F, Shariat SF, Lerner SP, et al. "Epidemiology, diagnosis, preoperative evaluation and prognostic assessment of upper-tract urothelial carcinoma (UTUC)". World J Urol. 35(3). :379-387. (2016)
- Rabbani F. "Prognostic factors in male urethral cancer". Cancer. 117(11). :2426-2434. (2010)
- Dadhania V, Czerniak B, Guo CC. "Adenocarcinoma of the urinary bladder". Am J Clin Exp Urol. 3(2). :51-63. (2015)
- Kalayci OT, Bozdag Z, Sonmezgoz F, Sahin N. "Squamous cell carcinoma of the renal pelvis associated with kidney stones: radiologic imaging features with gross and histopathological correlation". J Clin Imaging Sci. 3. :14. (2013)
- DeGeorge KC, Holt HR, Hodges SC. "Bladder Cancer: Diagnosis and Treatment". Am Fam Physician. 96(8). :507-514. (2017)
- Wolfman DJ, Marko J, Nikolaidis P, et al. "ACR Appropriateness Criteria® Hematuria". J Am Coll Radiol. 17(5). :S138-S147. (2020)
- Lerner SP, Schoenberg M, Sternberg C. "Textbook of Bladder Cancer". Taylor & Francis. (2006). ISBN: 1841843822
- Kawashima A, Sandler CM, Wasserman NF, et al. "Imaging of urethral disease: a pictorial review". Radiographics. 24(Suppl 1). :S195-216. (2004)
- Zhang M, Adeniran AJ, Vikram R, et al. "Carcinoma of the urethra". Hum Pathol. 72. :35-44. (2018)
- Lenis AT, Lec PM, Chamie K, MSHS M. "Bladder Cancer". JAMA. 324(19). :1980. (2020)
- Barocas DA, Boorjian SA, Alvarez RD, et al. "Microhematuria: AUA/SUFU Guideline". J Urol. 204(4). :778-786. (2020)
- Silverman SG, Leyendecker JR, Amis ES. "What Is the Current Role of CT Urography and MR Urography in the Evaluation of the Urinary Tract?". Radiology. 250(2). :309-323. (2009)
- Leyendecker JR, Barnes CE, Zagoria RJ. "MR Urography: Techniques and Clinical Applications". RadioGraphics. 28(1). :23-46. (2008)
- Rouprêt M, Babjuk M, Compérat E, et al. "European Association of Urology Guidelines on Upper Urinary Tract Urothelial Carcinoma: 2017 Update". Eur Urol. 73(1). :111-122. (2018)
- Wong-You–Cheong JJ, Woodward PJ, Manning MA, Sesterhenn IA. "Neoplasms of the Urinary Bladder: Radiologic-Pathologic Correlation". RadioGraphics. 26(2). :553-580. (2006)
- Hansel DE, McKenney JK, Stephenson AJ, Chang SS. "The Urinary Tract: A Comprehensive Guide to Patient Diagnosis and Management". Springer Science & Business Media. (2012). ISBN: 9781461453208
- III MG, Bagley DH. "Upper Urinary Tract Urothelial Carcinoma". Springer. (2015). ISBN: 9783319138695
- Vashistha V, Shabsigh A, Zynger DL. "Utility and Diagnostic Accuracy of Ureteroscopic Biopsy in Upper Tract Urothelial Carcinoma". Arch Pathol Lab Med. 137(3). :400-407. (2013)
- Chang SS, Bochner BH, Chou R, et al. "Treatment of Non-Metastatic Muscle-Invasive Bladder Cancer: AUA/ASCO/ASTRO/SUO Guideline". J Urol. 198(3). :552-559. (2017)
- Jinzaki M, Kikuchi E, Akita H, et al. "Role of computed tomography urography in the clinical evaluation of upper tract urothelial carcinoma". Int J Urol. 23(4). :284-298. (2016)
- van der Pol CB, Sahni VA, Eberhardt SC, et al. "ACR Appropriateness Criteria ® Pretreatment Staging of Muscle-Invasive Bladder Cancer". J Am Coll Radiol. 15(5). :S150-S159. (2018)
- "Diagnosis, Evaluation, and Follow-Up of Asymptomatic Microhematuria (AMH) in Adults: AUA Guideline". http://www.auanet.org/education/guidelines/asymptomatic-microhematuria.cfm. [2012-05-01]
- Li Y, Ding YU, Chen D, et al. "Renal cell carcinoma growing into the renal pelvis and mimicking transitional cell carcinoma: A case report and literature review". Oncol Lett. 9(4). :1869-1872. (2015)
- Chang SS, Boorjian SA, Chou R, et al. "Diagnosis and Treatment of Non-Muscle Invasive Bladder Cancer: AUA/SUO Guideline". J Urol. 196(4). :1021-1029. (2016)
- Kapoor R, Vijjan V, Singh P. "Bacillus Calmette-Guérin in the management of superficial bladder cancer". Indian J Urol. 24(1). :72-76. (2008)
- Russell CM, Lebastchi AH, Borza T, Spratt DE, Morgan TM. "The Role of Transurethral Resection in Trimodal Therapy for Muscle-Invasive Bladder Cancer". Bladder Cancer. 2(4). :381-394. (2016)
- Milowsky MI, Rumble RB, Booth CM, et al. "Guideline on Muscle-Invasive and Metastatic Bladder Cancer (European Association of Urology Guideline): American Society of Clinical Oncology Clinical Practice Guideline Endorsement". J Clin Oncol. 34(16). :1945-1952. (2016)
- Farrell MR, Xu JT, Vanni AJ. "Current Perspectives on the Diagnosis and Management of Primary Urethral Cancer: A Systematic Review". Res Rep Urol. Volume 13. :325-334. (2021)
- Gakis G, Bruins HM, Cathomas R, et al. "European Association of Urology Guidelines on Primary Urethral Carcinoma—2020 Update". Eur Urol Oncol. 3(4). :424-432. (2020)
- "Survival Rates for Bladder Cancer". https://www.cancer.org/cancer/bladder-cancer/detection-diagnosis-staging/survival-rates.html. [2016-05-23]
- Moyer VA, U.S. Preventive Services Task Force. "Final Recommendation Statement Bladder Cancer in Adults: Screening". Ann Intern Med. 155(4). :246-251. (2011)
- "Non-muscle-invasive Bladder Cancer". https://uroweb.org/guidelines/non-muscle-invasive-bladder-cancer/chapter/epidemiology-aetiology-and-pathology
- "Urothelial and Kidney Cancers". http://www.cancernetwork.com/cancer-management/urothelial-and-kidney-cancers. [2016-06-01]
- "Bladder cancer: Risks and causes". http://about-cancer.cancerresearchuk.org/about-cancer/bladder-cancer/risks-causes. [2015-07-20]
- Tuccori M, Filion KB, Yin H, et al. "Pioglitazone use and risk of bladder cancer: population based cohort study". BMJ. :i1541. (2016)
- Di Giovanni P, Di Martino G, Scampoli P, et al. "Arsenic Exposure and Risk of Urothelial Cancer: Systematic Review and Meta-Analysis". Int J Environ Res Public Health. 17(9). :3105. (2020)
- Biardeau X, Chartier-Kastler E, Rouprêt M, Phé V. "Risk of malignancy after augmentation cystoplasty: A systematic review". Neurourol Urodyn. 35(6). :675-682. (2015)
- Yan L, Chen P, Chen EZ, Gu A, Jiang ZY. "Risk of bladder cancer in renal transplant recipients: a meta-analysis". Br J Cancer. 110(7). :1871-1877. (2014)
- Ho CH, Sung KC, Lim SW, et al. "Chronic Indwelling Urinary Catheter Increase the Risk of Bladder Cancer, Even in Patients Without Spinal Cord Injury". Medicine. 94(43). :e1736. (2015)
- "Urachal Cancer". https://rarediseases.org/rare-diseases/urachal-cancer/#general-discussion
- Altan M, Çıtamak B, Haberal HB, et al. "Invasive Squamous Carcinoma and Adenocarcinoma of an Unreconstructed Exstrophic Bladder with HPV Infection". Current Urology. 9(2). :109-112. (2016)