CME information and disclosures
To see contributor disclosures related to this article, hover over this reference: [1]
Physicians may earn CME/MOC credit by reading information in this article to address a clinical question, and then completing a brief evaluation, in which they will identify their question and report the impact of any information learned on their clinical practice.
AMBOSS designates this Internet point-of-care activity for a maximum of 0.5 AMA PRA Category 1 Credit(s)™. Physicians should claim only credit commensurate with the extent of their participation in the activity.
For answers to questions about AMBOSS CME, including how to redeem CME/MOC credit, see "Tips and Links" at the bottom of this article.
Summary
A urinary tract infection (UTI) is an infection of the bladder, urethra, ureters, and/or kidneys and is a common infection in infancy and childhood. Risk factors include congenital anomalies of the kidneys and urinary tract (CAKUT), female sex, lack of circumcision in young boys, and bladder and bowel dysfunction. As in adults, the most common causative pathogen is Escherichia coli. Children and adolescents often present with classic symptoms of UTI (e.g., dysuria, urinary frequency). However, nonverbal and/or young children often have nonspecific symptoms, which may include fever, irritability, poor feeding, and new-onset urinary incontinence. Diagnosis is based on symptoms and urinalysis and urine culture results. Imaging is not routinely required for diagnosis but is used to evaluate for suspected acute complications (e.g., renal abscess) and underlying structural anomalies, such as vesicoureteral reflux (VUR). The first-line imaging modality is renal and bladder ultrasound (RBUS); voiding cystourethrography (VCUG) or voiding urosonography (VUS) is performed if there is concern for structural anomalies. Treatment of pediatric UTIs involves antibiotics (oral or IV) and management of any underlying causes. Recurrent UTIs are common in children, and patients and/or their caregivers should be educated on preventive measures. Complications of pediatric UTIs, especially if severe or recurrent, include pediatric sepsis, renal scarring, chronic kidney disease, and hypertension.
UTI in adults is discussed in a separate article; see “Urinary tract infections.”
Epidemiology
- UTIs are common in children: Up to 7% of girls and 2% of boys are diagnosed with a UTI by 6 years of age. [2]
- < 12 months of age: ♂ > ♀ [3]
- ≥ 12 months of age: ♀ >> ♂ [3]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
Pathogens [3][4]
-
Bacterial
- E. coli (in up to 90% of cases)
- Klebsiella pneumoniae
- Proteus mirabilis [3]
- Enterococcus faecalis
- Enterobacter species
- Rarely: Pseudomonas aeruginosa, group B Streptococcus, Staphylococcus aureus [4]
-
Nonbacterial
- Viral: adenovirus, Enterovirus, Echovirus, Coxsackievirus. [4]
- Fungal (rare): Candida, Cryptococcus neoformans, Aspergillus [4]
UTIs caused by a pathogen other than E. coli are considered atypical pediatric UTIs. [5][6]
Risk factors for pediatric UTI [3]
-
All ages
- Female sex
- Personal or family history of CAKUT or VUR
- Known renal scarring
- Bowel and bladder dysfunction (e.g., chronic constipation) [2][7]
- Instrumentation of the urinary tract [3]
-
Children ≤ 24 months of age
- Uncircumcised boys [8][9][10]
- Age < 12 months
-
Children > 24 months of age and adolescents
- Kidney stones
- Diabetes
- Sexual activity
Although uncircumcised young boys are at an increased risk for UTIs, the preventative effect of circumcision on UTI development is not considered sufficient to recommend circumcision for all patients. [11]
Classification
By location
- Lower UTI: infection of the bladder (cystitis) and/or urethra
- Upper UTI: infection of a kidney (pyelonephritis) and/or ureter
By severity
- Uncomplicated UTI: a UTI that follows a typical clinical course, responds to antibiotics within 72 hours of administration, and occurs in a patient without existing urinary tract abnormalities or chronic medical conditions [3]
-
Atypical pediatric UTI: a UTI in a patient with features suggesting an underlying pathology or complicated infection [2][3][6]
- UTI in a neonate
- Severe symptoms (e.g., pediatric sepsis, poor urine stream, ↑ creatinine)
- Identified pathogen is not E. coli
- Persistent symptoms despite 48–72 hours of antibiotics
- Associated complication (e.g., renal abscess)
- Personal or family history of urinary tract abnormalities (e.g., high-grade VUR, other CAKUT, renal scarring) [3]
- Abdominal or bladder mass
Clinical features
-
Features of lower UTI
- Urinary frequency
- Dysuria
- Urinary urgency
- Suprapubic pain
-
Features of upper UTI
- Flank pain
- Fever [2][3]
-
Nonspecific symptoms (may be reported by caregivers of young children) [2][3][12]
- New-onset urinary incontinence (if toilet trained)
- Irritability
- Crying when urinating
- Poor feeding
- Malodorous urine
- Neonates: jaundice, hypothermia [8][13]
Symptoms of a pediatric UTI may be nonspecific; fever may be the only sign, particularly in infants. Neonates may present with hypothermia. [2][3]
Subtypes and variants
Acute pyelonephritis in children (APN) [3]
Etiology
- Ascending infection from lower UTI
- Most common route of spread
- Causative pathogens: typically bacterial; most commonly E. coli
- Hematogenous spread
- May occur in chronically ill and/or immunocompromised individuals
- Causative pathogens: Staphylococcus spp., fungi
Clinical features
- APN is more common in young children.
- Upper UTI symptoms, often with lower UTI symptoms
- See “Clinical features of pediatric UTI” for nonspecific symptoms.
Diagnosis
Diagnostic criteria
APN in children is typically diagnosed based on the following:
- Clinical features of upper UTI
- Bacteriuria [3]
- Pyuria
Some patients present with low bacterial colony counts and no pyuria; diagnosis may be made clinically. [3]
Diagnostic studies
- ↑ CRP and/or procalcitonin suggest APN but are not diagnostic. [3][14]
-
Imaging in pediatric UTI is not routinely indicated for acute infection but may be obtained to exclude complications or underlying pathology; findings include: [3]
- RBUS: normal or nonspecific renal edema and hyperemia
- Dimercaptosuccinic acid scan (DMSA scan): renal cortical defects
- Assessment for chronic complications: DMSA scan 4–6 months after infection may reveal renal scarring. [3]
RBUS cannot diagnose APN. [3]
Treatment [3]
- Start a third-generation cephalosporin; see “Treatment of pediatric UTI” for dosing.
- Clinical improvement (e.g., fever resolution) within 48–72 hours: Continue antibiotics for 7–10 days. [3]
- No response within 48–72 hours
- Obtain renal ultrasound to exclude complications (e.g., renal abscess) that require a longer duration of antibiotics. [3]
- Consider specialist consultation (e.g., nephrology, urology, infectious diseases) for advanced diagnostics.
Diagnosis
Approach [2][3]
UTIs are typically diagnosed using urinalysis abnormalities (i.e., pyuria and/or visualized bacteria) and urine culture to confirm bacteriuria.
- Perform urinalysis if indicated based on age and clinical features.
- Send urine culture if urinalysis suggests UTI or if normal but clinical suspicion for UTI is high.
- Obtain imaging for UTI in children with:
- Age ≤ 6 years and first febrile UTI [15]
- Atypical pediatric UTI
- Recurrent UTI
Diagnosis may also be made clinically (e.g., in patients with suggestive clinical features but low colony counts and/or no pyuria). [2][3]
Urine studies [2][3]
Collection methods [3]
-
Not toilet trained
- Preferred: sterile collection (e.g., transurethral catheterization or suprapubic aspiration)
- Alternatives: clean-catch urine sample or bagged urine sample (not suitable for culture) [2][16]
- Toilet trained: clean-catch urine sample
")
")


Urinalysis [3]
Indications
- Age < 2 months: any ill-appearing and/or febrile infant (see "Approach to suspected neonatal bacterial infection" and “Fever in infants ≤ 60 days of age”) [16]
-
Age 2–24 months: Consider the following features or use risk stratification tools (e.g., UTICalc) to determine need for urinalysis. [17]
- Fever: ≥ 39°C (102.2°F), lasting ≥ 48 hours, and/or with no other apparent source [18]
- Clinical features of pediatric UTI
- History of prior UTI
- Presence of risk factors for pediatric UTI
- Age > 24 months with clinical features of pediatric UTI
Findings
- On dipstick urinalysis [3]
- Positive urinary nitrites: suggests bacteriuria
- Positive leukocyte esterase: suggests pyuria
- On microscopy
- Presence of bacteria on Gram stain and/or pyuria suggests UTI. [3]
- Normal findings on urinalysis generally rule out a UTI, but some uropathogens do not cause pyuria or bacteriuria. [3]
 test strip")

Urine culture [2][3]
Indications
- Urinalysis positive for pyuria and/or bacteruria
- Normal urinalysis but high clinical suspicion for UTI
Some uropathogens may not cause detectable pyruia. In patients with significant urinary symptoms and/or risk factors for pediatric UTI, obtain culture for a definitive diagnosis even in the absence of pyuria.[3]
Findings
- Significant bacteriuria confirms the diagnosis.
-
Thresholds vary based on collection method and across guidelines; follow local protocols.
- Clean-catch urine sample: > 100,000 CFU/mL [2][3][6]
- Transurethral catheterization: > 50,000 CFU/mL [3]
- Suprapubic aspiration: 1000 CFU/mL [3]
Imaging for pediatric UTI
Imaging is indicated in selected patients to evaluate for urinary tract anomalies (e.g, VUR, posterior urethral valves) and/or complications of UTI (e.g., renal abscess, APN).
-
Initial imaging for first febrile UTI in children [2][3][15]
- Infants aged < 2 months: RBUS ± either VCUG or VUS [15]
- Infants and children aged 2 months–6 years: RBUS [3]
- Children aged > 6 years: Imaging is not recommended. [15]
-
Imaging for atypical pediatric UTI and/or recurrent UTI [2][3][15]
- Atypical pediatric UTI at any age: RBUS and either VCUG or VUS
- Recurrent UTI: RBUS and, if ≥ 2 febrile UTIs, VCUG [15]
If RBUS and/or VCUG are abnormal, a specialist may recommend additional imaging. [3][15]
RBUS [2][3][15]
-
Indications
- First febrile UTI in children aged ≤ 6 years
- Atypical pediatric UTI or recurrent UTI at any age
-
Timing [3]
- Severe presentation and/or failure to respond to 48–72 hours of antibiotics: during acute infection
- Uncomplicated clinical course: after resolution of infection; typically within 6 weeks
-
Potential findings
- Features suggestive of UTI
- Lower UTI: normal or thickened bladder wall with bladder debris [3]
- Upper UTI: normal or nonspecific kidney edema and/or hyperemia [3]
- Renal parenchyma changes (not sensitive)
- Conditions that predispose to UTI
- Congenital anomalies of the kidneys
- Abdominal masses affecting the urinary system
- Secondary signs of vesicoureteral reflux (VUR) [2][3]
- Nephrolithiasis
- Complications (e.g., renal abscess)
- Features suggestive of UTI
RBUS is typically the initial imaging modality for pediatric UTIs, as it can detect most structural abnormalities and does not involve radiation. [3][15]


VCUG or VUS [2][3][15]
VUS is less invasive than VCUG and does not involve radiation.
-
Indications
- Abnormal RBUS
- Atypical pediatric UTI
- Recurrent febrile UTIs
-
Potential findings
- Visualization of VUR (see “Diagnostics of VUR”) [2][3]
- Obstructive uropathy (e.g., stenosis, hydronephrosis)
")
")



Advanced imaging [3][7][15]
- Nuclear medicine cystography: may be used to evaluate for VUR
-
Dimercaptosuccinic acid scan (DMSA scan) [3]
- Acute findings: renal cortical defects in acute pyelonephritis
- Nonacute findings (e.g., 4–6 months after acute infection) : gold standard for identification of renal scarring [3]

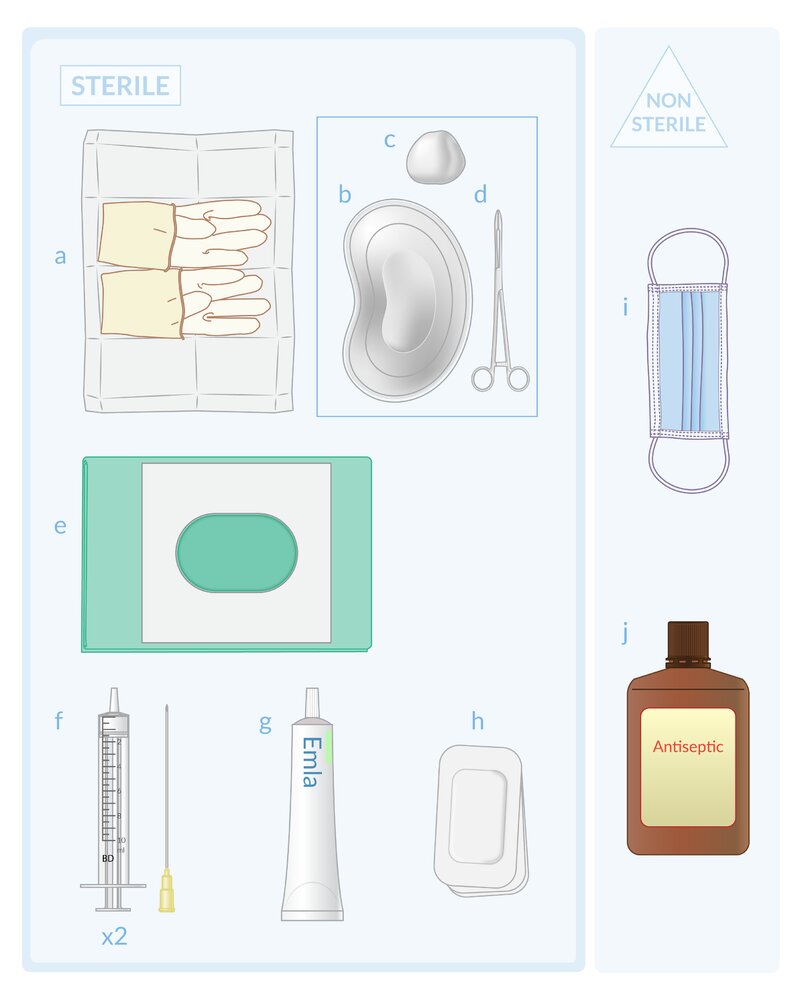
Sterile materials: (a) gloves; (b) tray; (c) gauze; (d) forceps; (e) fenestrated drape; (f) 5-mL syringe and 22-gauge needle; (g) EMLA topical anesthetic cream; (h) occlusive dressing
Nonsterile materials: (i) surgical mask; (j) antiseptic solution
© AMBOSS
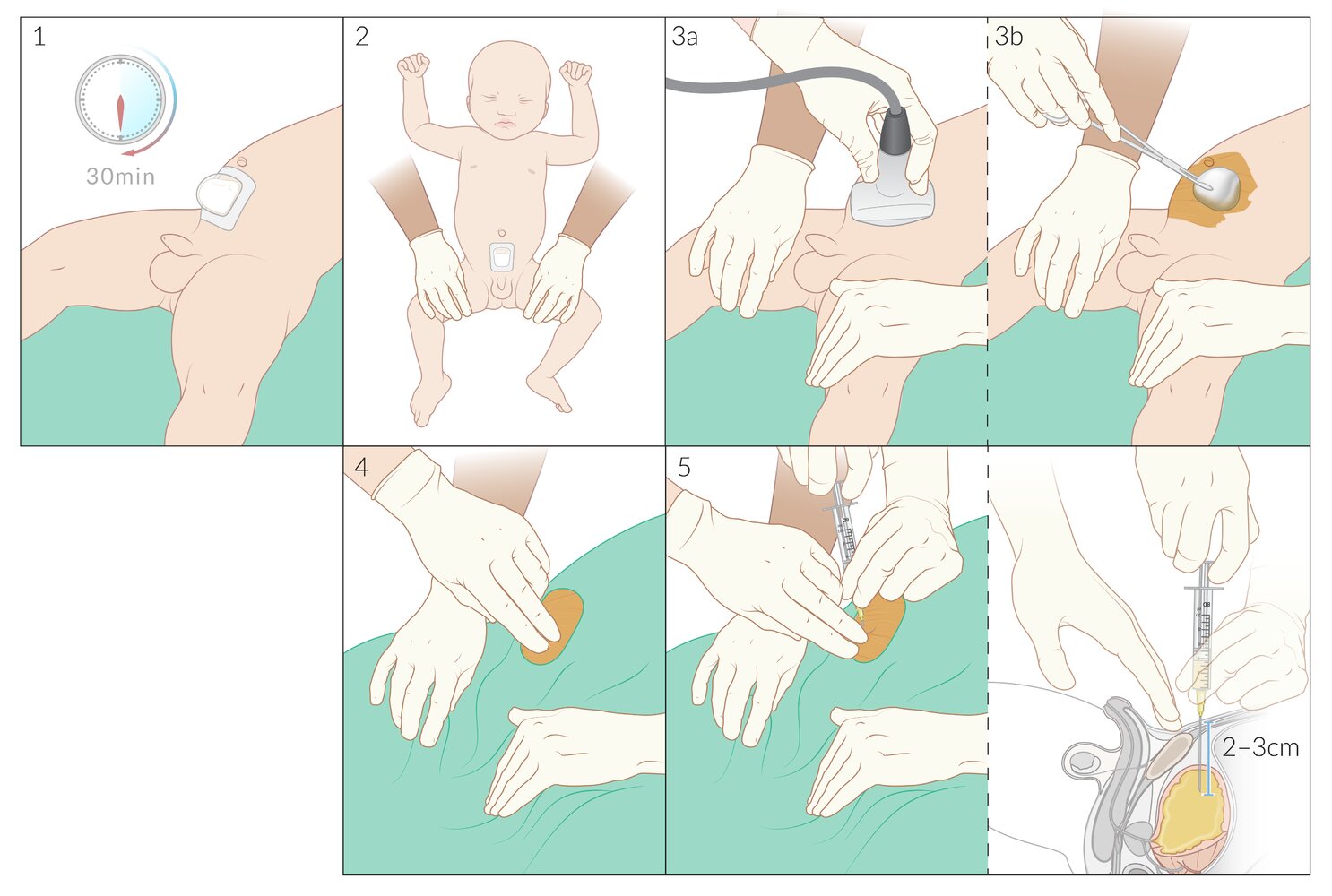
1) A topical anesthetic (e.g., EMLA cream) is applied to the aspiration site, in the midline approx. 1 to 2 cm cranial to the pubic symphysis. The area is covered with an occlusive dressing (e.g., Tegaderm), and the anesthetic is allowed to act for approximately 30 minutes before proceeding.
2) An assistant holds the infant's legs in a frog-legged position (i.e., hips and knees are flexed and hips are externally rotated).
3a) After removal of the occlusive dressing and wiping away the remaining anesthetic (not pictured), ultrasound is used to confirm bladder location. Note that needle insertion may also be performed under real-time ultrasound guidance, in which case a sterile cover is required for the ultrasound probe.
3b) Using sterile forceps and sterile gauze soaked in an antiseptic solution, the skin is cleaned from the pubic symphysis to the umbilicus and the antiseptic is allowed to air dry.
4) The cleaned area is covered with a sterile fenestrated drape. The aspiration site is marked by placing two fingers above the pubic symphysis (this may be done by a second assistant as shown here, or by the clinician themselves).
5) The clinician inserts a 22-gauge needle attached to a 5-mL syringe perpendicular to the abdominal wall (this usually means aiming approx. 10-20 degrees caudally from true vertical due to the slope of the abdominal wall).
6) While aspirating, the needle is advanced 2-3 cm until urine appears in the syringe. A minimum of 2 mL of urine should be collected.
Following the procedure, the needle and syringe are withdrawn, the needle safely removed from the syringe, and the urine emptied into a sterile urine collection cup. The cup is then placed in a specimen transport bag and sent to the laboratory.
Note: In older children and/or children with thicker abdominal walls, additional subcutaneous infiltration of local anesthetic is preferred over a topical anesthetic alone. This is performed between steps 4 and 5 using a sterile technique.
© AMBOSS
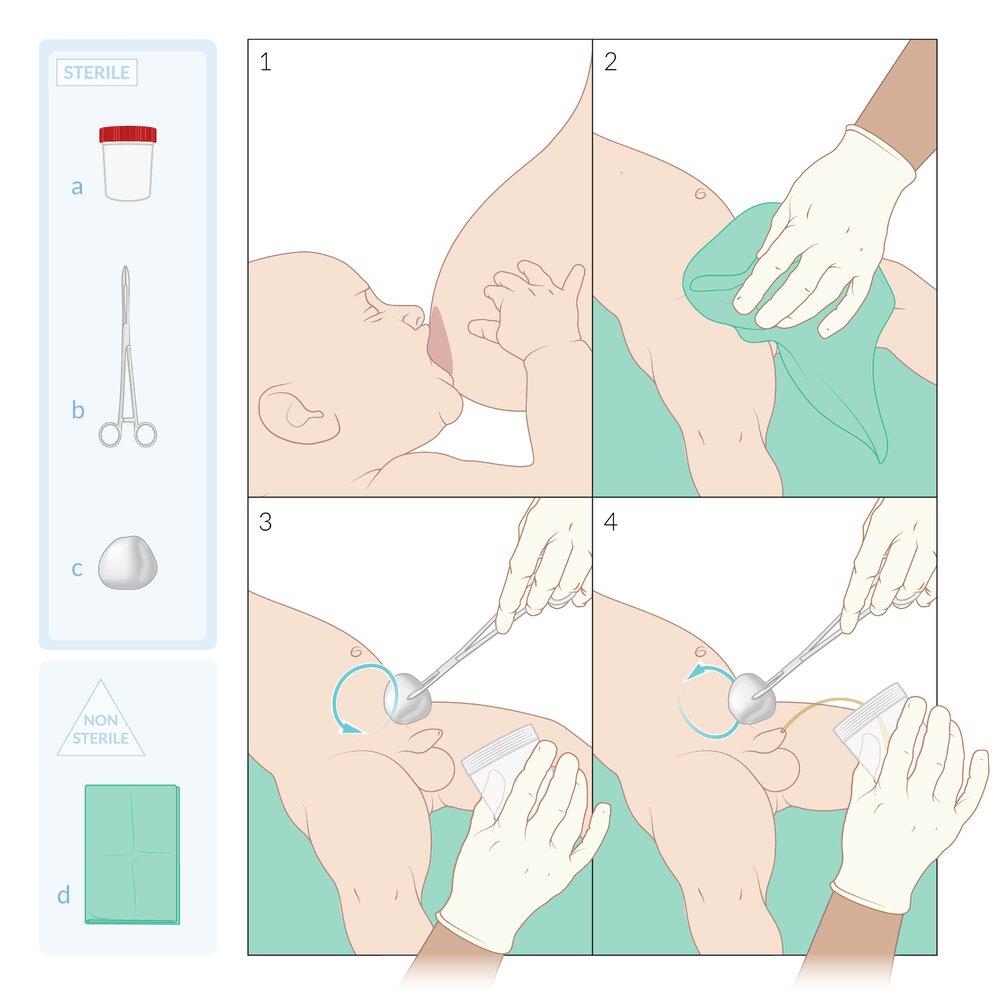
Illustration depicting a voiding stimulation technique to accelerate the collection of a clean-catch (i.e., midstream) urine sample in an infant. It is also known as the Quick-Wee method.
Sterile materials: (a) urine collection cup; (b) forceps; (c) surgical swab
Nonsterile materials: (d) towel, cloth, or urine towelette
1) The caregiver may offer a bottle or breastfeed before the procedure.
2) The urethral opening (and perineum, if female) is cleaned, first with an antiseptic and then with sterile water.
3) Using a cold saline-soaked gauze held with forceps, the suprapubic area is gently rubbed in a circular motion while holding the collection cup (no pressure is required: the cold and wet stimulus is thought to trigger cutaneous voiding reflexes).
4) Urine is collected without skin contact to avoid contamination.
© AMBOSS
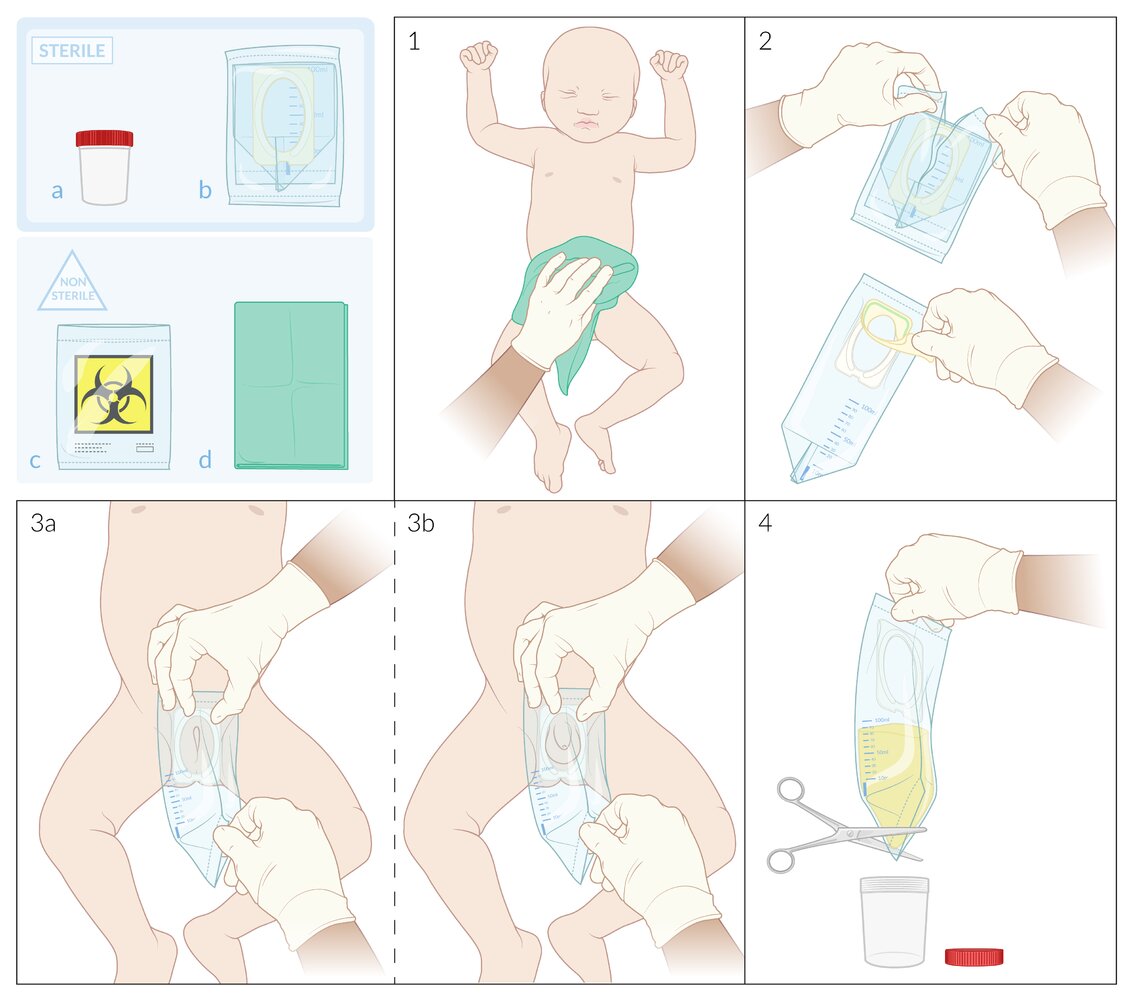
Sterile equipment: (a) urine collection cup; (b) urine collection bag (e.g., U-bag)
Nonsterile equipment: (c) specimen transport bag; (d) towel, cloth, or urine towelette
1) The urethral opening and perineum are cleaned, first with an antiseptic and then with sterile water.
2) The urine collection bag is opened and the adhesive sticker removed without touching the adhesive collar underneath.
3) The adhesive collar is applied to the skin of the genital area by pressing on the nonadhesive side of the collection bag and gently pulling down on the bag to open it. To prevent leakage and contamination, it is essential to ensure the adhesive has fully adhered around the entire collar without skin folds or gaps. The urethral opening and labia of female children (3a) and the penis and scrotum of male children (3b) must be inside the opening of the bag.
4) After the child has urinated, the bag is held above a sterile urine collection cup and opened, either via a dedicated mechanism (e.g., by pulling the blue square tab on a U-bag) or by cutting the bottom corner with sterile scissors. The urine is drained into a sterile cup without the bag touching the cup. The cup is then sealed with its lid, placed inside the specimen transport bag, and sent to the laboratory.
© AMBOSS
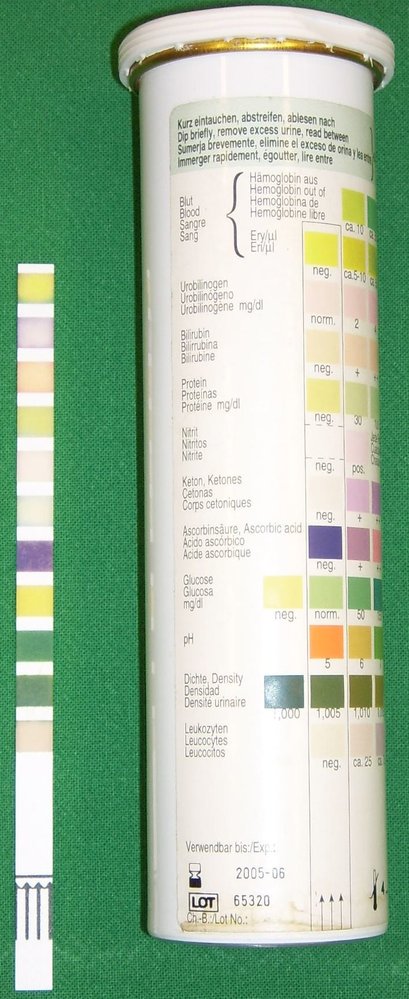
Left: test strip following immersion in urine
Right: test strip packaging with instructions on how to interpret findings
Source: “Urine Quicktest” by Uwe Gille, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}
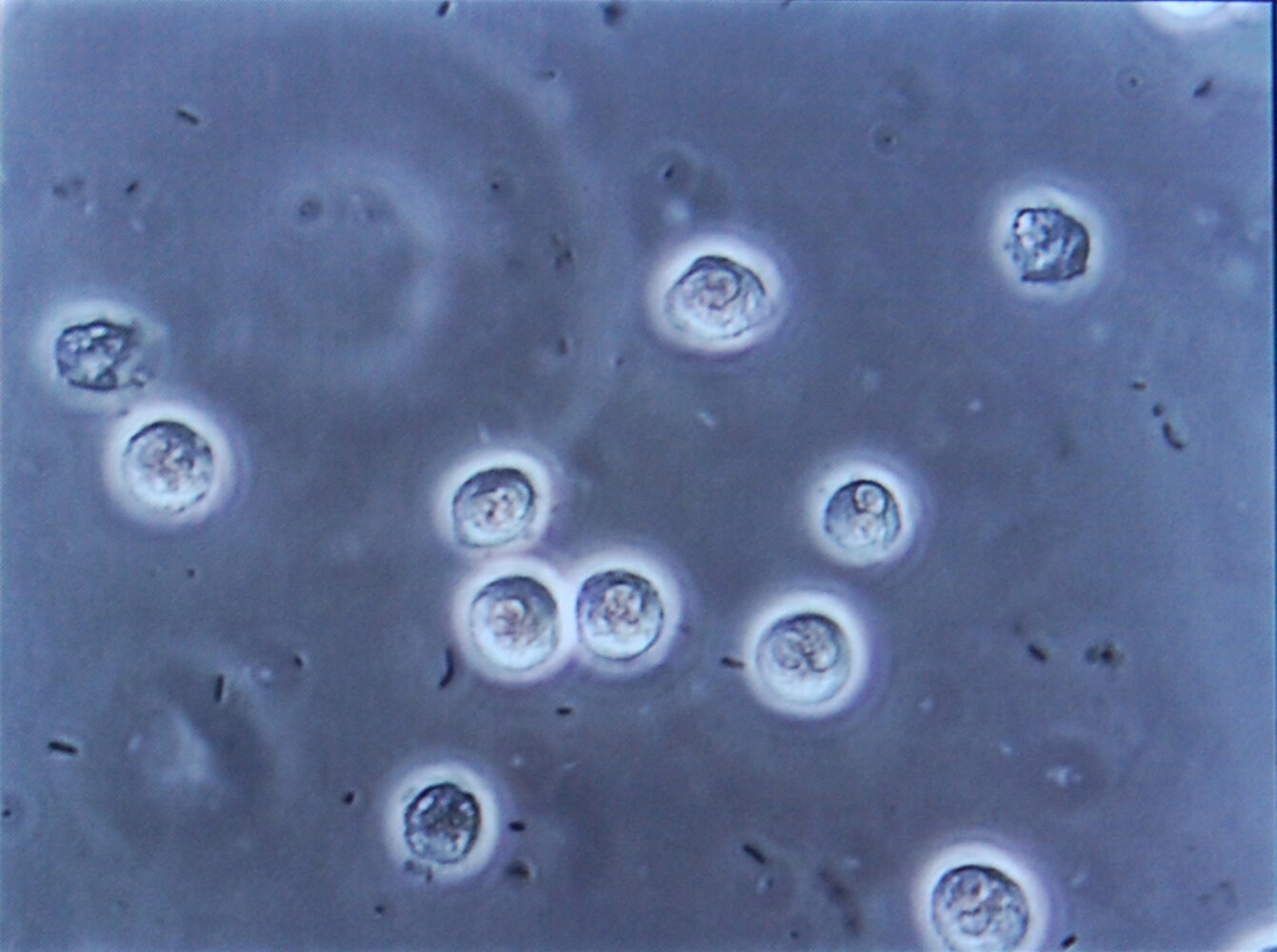
Photomicrograph of a urine specimen (high magnification)
Multiple white blood cells (large, light-colored structures) and bacteria (small black structures) are visible.
The presence of white blood cells (pyuria) and bacteria (bacteriuria) in the urine is characteristic of urinary tract infection.
Source: “Bacteriuria pyuria 4” by Steven Fruitsmaak, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}

Ultrasound left kidney (longitudinal plane)
There is hypoechoic dilation (green overlay) of the renal pelvis (RP) and visible calyces. The thickness of the renal parenchyma is normal.
This appearance is characteristic of hydronephrosis grade II (illustration).
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.

Ultrasound left kidney (longitudinal plane)
The calyces (green overlay) are dilated and have lost their normal cup-shaped appearance. Flattening of papillae and blunting of fornices can be seen. Where visible, the renal cortical parenchyma is not thinned.
RP: renal parenchyma; Arrowheads: hyperechoic renal sinus
Source: “Ultrasonographic picture taken from a patient with left ureteral stone with hydronephrosis, created in Taiwan” by morning2k, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}

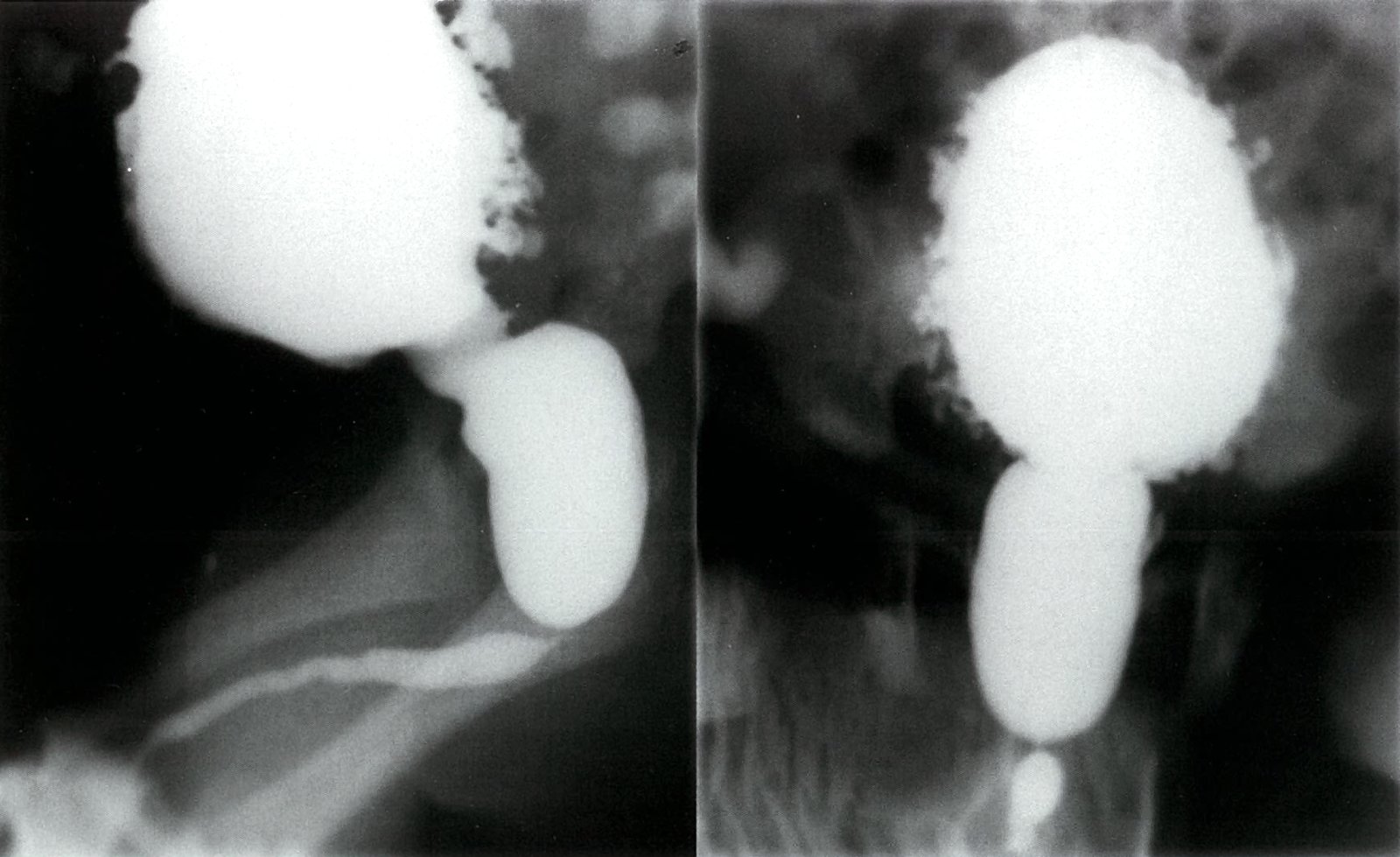
Contrast-filled, ballooning of the renal pelvicalyceal system (left > right) can be seen, as well as a dilated ureter with numerous kinks. This finding indicates grade V vesicoureteral reflux.
Source: © IMPP
Contrast-filled, ballooning of the renal pelvicalyceal system (left > right) can be seen, as well as a dilated ureter with numerous kinks. This finding indicates grade V vesicoureteral reflux.
Source: © IMPP
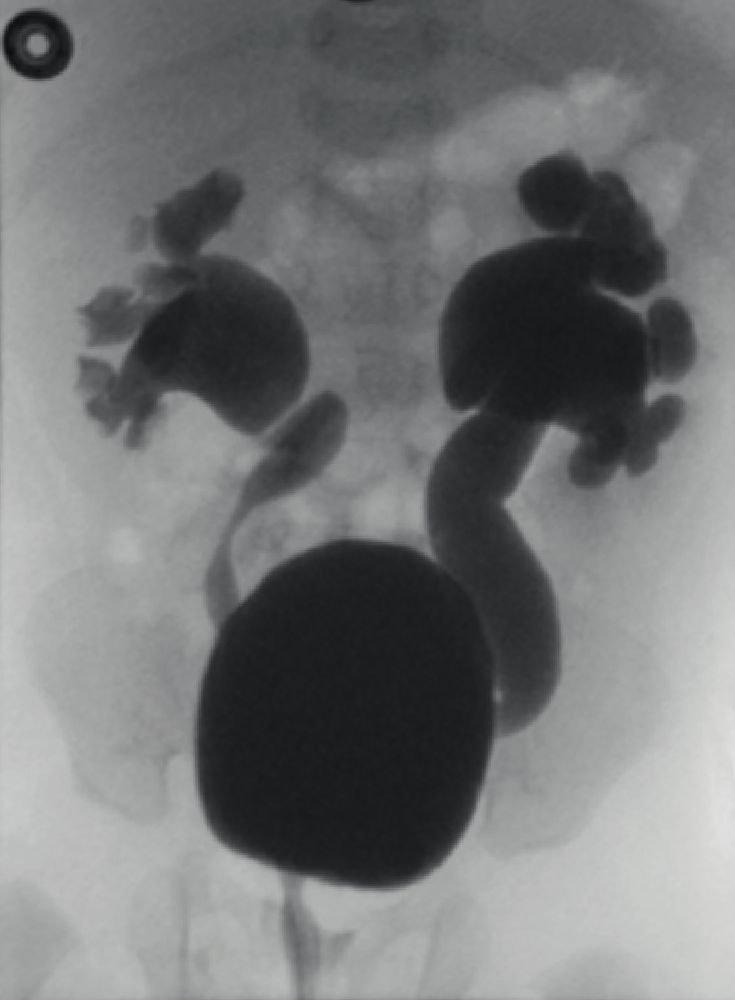
Voiding cystourethrogram (AP view)
Bilateral vesicoureteral reflux (VUR) has resulted in dilatation of the ureters and pelvicalyceal systems. The right ureter is tortuous and moderately dilated, with blunting of calyceal fornices (example indicated by arrow) but preserved papillary impressions (green line; grade IV VUR). The left ureter is markedly dilated with loss of the fornices and papillary impressions (grade V VUR).
B: bladder
Source: © IMPP

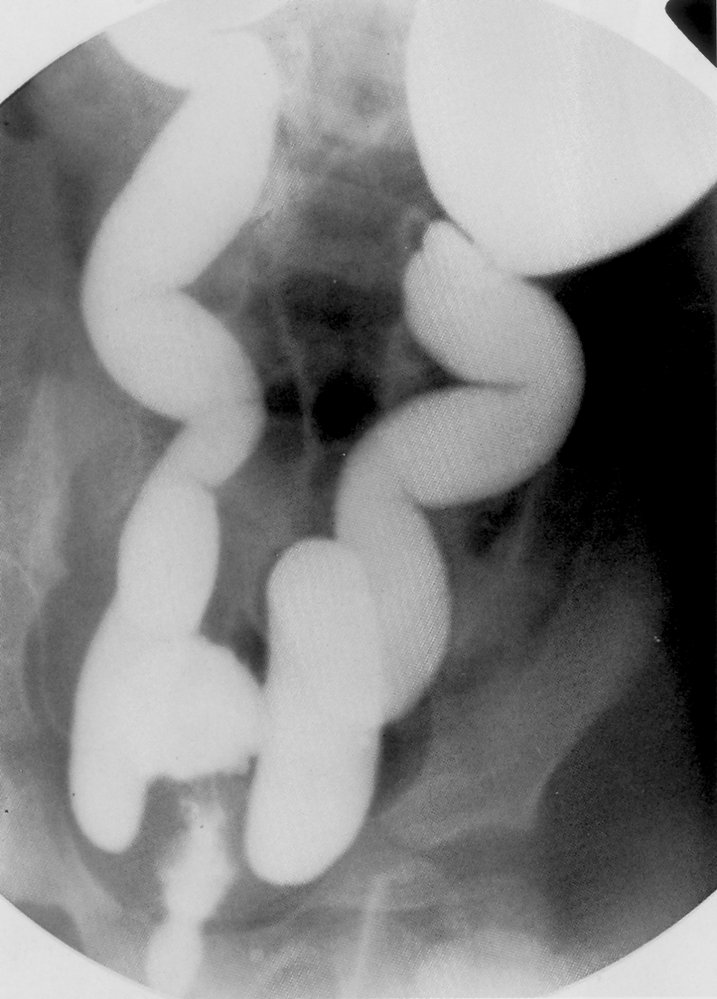
Fluoroscopy (voiding cystourethrogram; supine; frontal view)
Reflux of contrast (vesicoureteral reflux; green overlay) from the bladder (B) into the right ureter is seen, without dilation of the ureter. The proximal collecting system and kidney are not visible on this image.
U: urethra
Source: © IMPP
This voiding cystourethrogram shows a contrast-filled bladder (B) and urethra (U) that demonstrates pronounced stenosis (S) in the proximal region. The urethra is significantly dilated proximal to the stenosis. Multiple diverticula can be seen in the region of the bladder.
Source: © IMPP
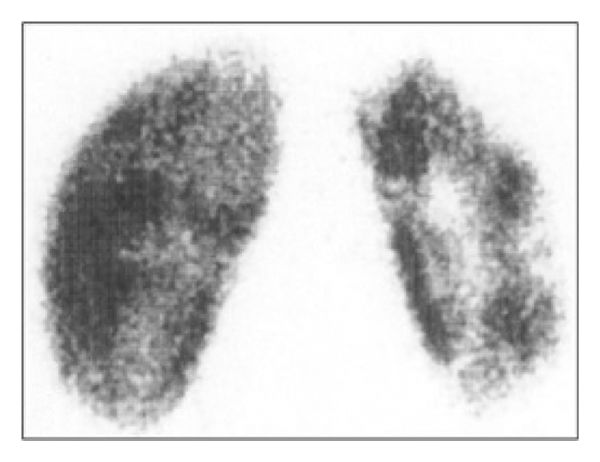
Nuclear Medicine 99m-Tc DMSA renal scan (99m-Technetium dimercaptosuccinic acid; posterior view) of a patient with severe vesicoureteral reflux
There is abnormal tracer uptake. Multiple parenchymal defects are visible throughout the small right kidney (indicated by arrowheads).
99m-Tc DMSA binds to the proximal convoluted tubules. A DMSA scan can be used to evaluate renal size, shape, and position and to detect areas of parenchymal scarring.
Source: “Figure 2 (c), in: Correlation of Renal Scarring to Urinary Tract Infections and Vesicoureteral Reflux in Children” by Hamdy Aboutaleb, Tamer A. Abouelgreed, Hala El-Hagrasi, Diaa Bakry Eldib, Mohamed A. Abdelaal, and Mohamed Amin El Gohary, Hindawi, licensed under CC BY 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Treatment
Approach [2][3]
- Start empiric antibiotics for pediatric UTI while awaiting urine culture results.
- Assess for admission criteria.
-
Adjust treatment when culture results become available.
- Negative culture: Stop antibiotics and consider differential diagnoses of pediatric UTI.
- Confirmed UTI: Alter treatment as needed based on antibiotic sensitivities.
- Provide supportive treatment (e.g., analgesia, supportive care for pediatric fever).
- If fever persists for > 72 hours, consider urgent imaging for pediatric UTI to rule out renal abscess and/or acute urinary tract obstruction. [3]
- Educate patients and caregivers on prevention of pediatric UTI.
- Refer patients to a specialist (e.g., urology, nephrology) for any of the following:
- CAKUT
- Chronic complications of pediatric UTI
- Management of persistent risk factors for pediatric UTI (e.g., bowel and bladder dysfunction) [2][10]
Admission criteria for pediatric UTI [3][12]
- IV antibiotics required (for indications, see “Empiric antibiotics for pediatric UTI”)
- Consider admitting patients with any of the following:
- Age 1–2 months [16]
- Significant renal tract anomalies [12]
- Barriers to follow-up
Antibiotic therapy
- Follow local guidelines and protocols if available.
- Always check local resistance patterns before initiating treatment.
| Empiric antibiotics for pediatric UTI [2][3][19] | |||
|---|---|---|---|
| Indications | Recommended antibiotics | Duration [2] | |
| IV |
|
|
|
| Oral |
|
|
|
|
|
|
|
Avoid empiric antibiotic monotherapy with amoxicillin or other penicillins because of resistance. [3]
Repeat urine culture is not necessary unless symptoms persist. [3]
Differential diagnoses
- Vulvovaginitis (e.g., from poor hygiene, irritation) [20][21]
- Appendicitis or mesenteric lymphadenitis [21][22]
- Diabetes mellitus or arginine vasopressin disorders (may cause urinary frequency) [20]
- Genital injury [23]
- Sexually transmitted infections [20]
Consider sexual assault in all pediatric patients presenting with genital injury or sexually transmitted infections; in adolescents, screen for signs of human trafficking.
The differential diagnoses listed here are not exhaustive.
Complications
-
Acute [2][3]
- Dehydration and hypovolemia
- Pediatric sepsis
- Renal abscess
- Acute kidney injury
-
Chronic [2][3]
- Recurrent UTIs
- Renal scarring (from recurrent APN) can result in:
- Chronic kidney disease
- Hypertension in children
We list the most important complications. The selection is not exhaustive.
Prevention
- Educate caregivers on nonspecific symptoms of pediatric UTI and the need to seek early treatment.
- Promptly identify and treat any underlying conditions, including:
- Bladder and bowel dysfunction (see “Constipation in children and adolescents”) [2][10]
- CAKUT (e.g., hydronephrosis, vesicoureteral reflux)
- Encourage children to urinate regularly. [10]
- Consider recommending an increase in fluid intake. [24]
- Uncircumcised boys: Encourage daily gentle retraction of the foreskin for cleaning. [10]
- Discuss antibiotic prophylaxis for recurrent UTIs with a specialist; use is controversial. [2][10]
- Long-term antibiotic use is associated with a high risk of resistance.
- Trials have shown limited or no benefit. [25][26]
- Use is typically limited to patients with high-risk CAKUT and young infants [10]
- Some evidence suggests that probiotics and cranberry supplements may prevent recurrence, but further research is required. [27]
UTI 1-year recurrence rates are as high as 30%. Children with a history of UTIs should be seen within 48 hours if they experience an unexplained fever or symptoms of a pediatric UTI. [2][3][28]
External Resources
References
- Mattoo TK, Shaikh N, Nelson CP. "Contemporary Management of Urinary Tract Infection in Children". Pediatrics. 147(2). (2021)
- Leung AKC, Wong AHC, Leung AAM, et al. "Urinary Tract Infection in Children". Recent Pat Inflamm Allergy Drug DIscov. 13(1). :2-18. (2019)
- Karmazyn BK, Alazraki AL, Anupindi SA, et al. "ACR Appropriateness Criteria ® Urinary Tract Infection—Child". J Am Coll Radiol. 14(5). :S362-S371. (2017)
- Okarska-Napierała M, Wasilewska A, Kuchar E. "Urinary tract infection in children: Diagnosis, treatment, imaging – Comparison of current guidelines". J Pediatr Urol. 13(6). :567-573. (2017)
- Santos JD, Lopes RI, Koyle MA. "Bladder and bowel dysfunction in children: An update on the diagnosis and treatment of a common, but underdiagnosed pediatric problem". Can Urol Assoc J. 11(1-2Suppl1). :S64-S72
- Veauthier B, Miller MV. "Urinary Tract Infections in Young Children and Infants: Common Questions and Answers". Am Fam Physician. 102(5). :278-285. (2020)
- Schmidt B, Copp HL. "Work-up of Pediatric Urinary Tract Infection". Urol Clin North Am. 42(4). :519-526. (2015)
- Shapiro E. "American academy of pediatrics policy statements on circumcision and urinary tract infection". Rev Urol. 1(3). :154-6. (1999)
- Olson P, Dudley AG, Rowe CK. "Contemporary Management of Urinary Tract Infections in Children". Current Treatment Options in Pediatrics. (2022)
- "AAFP policy on Neonatal Circumcision". https://web.archive.org/web/20220913194032/https://www.aafp.org/about/policies/all/neonatal-circumcision.html
- Kaufman J, Temple-Smith M, Sanci L. "Urinary tract infections in children: an overview of diagnosis and management". BMJ Paediatr Open. 3(1). :e000487. (2019)
- Chang PW, Schroeder AR, Lucas BP, McDaniel CE. "Impact of Diagnostic Criteria on UTI Prevalence in Young Infants With Jaundice: A Meta-analysis". Hosp Pediatr. 12(4). :425-440. (2022)
- Chandra T, Bajaj M, Iyer R, et al. "ACR Appropriateness Criteria® Urinary Tract Infection-Child: 2023 Update". Journal of the American College of Radiology. 21(6). :S326-S342. (2024)
- Pantell RH, Roberts KB, Adams WG, et al. "Evaluation and Management of Well-Appearing Febrile Infants 8 to 60 Days Old". Pediatrics. 148(2). (2021)
- Shaikh N, Hoberman A, Hum SW, et al. "Development and Validation of a Calculator for Estimating the Probability of Urinary Tract Infection in Young Febrile Children". JAMA Pediatr. 172(6). :550. (2018)
- Gorelick MH, Hoberman A, Kearney D, Wald E, Shaw KN. "Validation of a decision rule identifying febrile young girls at high risk for urinary tract infection". Pediatr Emerg Care. 19(3). :162-164. (2003)
- Committee on Infectious Disease, American Academy of Pediatrics. "Red Book: 2024-2027 Report of the Committee on Infectious Diseases, 33rd Edition". American Academy of Pediatrics. (2024). ISBN: 9781610027373
- Fasugba O, Mitchell BG, McInnes E, et al. "Increased fluid intake for the prevention of urinary tract infection in adults and children in all settings: a systematic review". J Hosp Infect. 104(1). :68-77. (2020)
- Williams G, Craig JC. "Long-term antibiotics for preventing recurrent urinary tract infection in children". Cochrane Database Syst Rev. (2019)
- Williams G, Hodson EM, Craig JC. "Interventions for primary vesicoureteric reflux". Cochrane Database Syst Rev. 2019(2). (2019)
- Meena J, Thomas CC, Kumar J, Raut S, Hari P. "Non-antibiotic interventions for prevention of urinary tract infections in children: a systematic review and meta-analysis of randomized controlled trials". Eur J Pediatr. 180(12). :3535-3545. (2021)
- American Academy of Pediatrics. "Reaffirmation of AAP Clinical Practice Guideline: The Diagnosis and Management of the Initial Urinary Tract Infection in Febrile Infants and Young Children 2-24 Months of Age". Pediatrics. 138(6). :e20163026-e20163026. (2016)
- "Contributor Disclosures - Urinary tract infections in children and adolescents. All of the relevant financial relationships listed for the following individuals have been mitigated: Alexandra Willis (copyeditor, was previously employed by OPEN Health Communications). None of the other individuals in control of the content for this article reported relevant financial relationships with ineligible companies. For details, please review our full conflict of interest (COI) policy:"
- Bergelson J, Zaoutis T, Shah SS. "Pediatric Infectious Diseases E-Book". Elsevier Health Sciences. (2008). ISBN: 9780323076333
- Marcdante K, Kliegman RM. "Nelson Essentials of Pediatrics E-Book". Elsevier Health Sciences. (2018). ISBN: 9780323528061
- Walls R, Hockberger R, Gausche-Hill M. "Rosen's Emergency Medicine". Elsevier Health Sciences. (2018). ISBN: 9780323354790
- Fan SM, Grigorian A, Chaudhry HH, et al. "Female pediatric and adolescent genitalia trauma: a retrospective analysis of the National Trauma Data Bank". Pediatr Surg Int. 36(10). :1235-1241. (2020)
- Shaikh K, Osio V, Leeflang M, Shaikh N. "Procalcitonin, C-reactive protein, and erythrocyte sedimentation rate for the diagnosis of acute pyelonephritis in children". Cochrane Database Syst Rev. 2020(9). (2020)