Summary
Urinary tract infections (UTIs) are infections of the bladder, urethra, ureters, or kidneys that are most commonly caused by bacteria, especially E. coli. Infections of the bladder or urethra are called lower UTIs, whereas infections involving the kidneys or ureters are called upper UTIs. Because women have a shorter urethra and anal and genital regions that are closer in proximity, they are at higher risk of contracting UTIs than men. Other risk factors include sexual intercourse, indwelling urinary catheters, pregnancy, and abnormalities of the urinary tract. UTIs in otherwise healthy, nonpregnant, premenopausal women are considered uncomplicated. UTIs in men or individuals with other risk factors for treatment failure or serious outcomes, such as functional or anatomical abnormalities of the urinary tract, are considered complicated. Clinical findings depend on which part of the urinary tract is affected. Lower UTIs manifest with dysuria, suprapubic pain, urinary urgency, and increased urinary frequency, whereas upper UTIs additionally cause fever and flank pain. Diagnosis is usually clinical and can be supported with findings of pyuria and bacteriuria on urinalysis. A urine culture may be required for patients with a complicated lower UTI or equivocal urinalysis findings. Imaging is rarely required but may be indicated to rule out underlying factors (e.g., urinary tract obstruction, anatomical abnormalities). First-line empiric antibiotic therapy options for uncomplicated lower UTIs include oral nitrofurantoin, trimethoprim/sulfamethoxazole, or fosfomycin for up to 7 days. For complicated lower UTIs, broad-spectrum antibiotic therapy should be given for 7–14 days and treatable underlying factors should be addressed. Recurrent UTIs are common in women and antibiotic prophylaxis may be indicated. Catheter-associated urinary tract infections (CAUTIs) are among the most common healthcare-associated infections; they are frequently caused by resistant bacteria and are treated with catheter removal or replacement in addition to antibiotic therapy. Pregnant women should be screened and treated both for UTIs and for asymptomatic bacteriuria. For the management of upper UTIs, see “Pyelonephritis.”
See also “UTI in children and adolescents.”
Etiology
Pathogens
Bacteria
- Infection ascends from the urethra to the bladder.
- Can ascend further to the ureters and the renal pelvises (see “Pyelonephritis”)
-
Bacteria that cause UTI
- Escherichia coli: leading cause of UTI (approx. 80%) [1]
- Staphylococcus saprophyticus: 2nd leading cause of UTI in sexually active women
- Klebsiella pneumoniae: 3rd leading cause of UTI
-
Proteus mirabilis
- Produces ammonia, giving the urine a pungent or irritating smell
- Associated with struvite stone formation
- Nosocomial bacteria: Serratia marcescens, Enterococci spp., and Pseudomonas aeruginosa are associated with increased drug resistance.
- Enterobacter species
- Ureaplasma urealyticum
Viruses
- Immunocompromised patients and children are particularly susceptible to viral UTIs. [2]
- Adenovirus, cytomegalovirus, and BK virus are commonly involved in hemorrhagic cystitis. [3]
Fungi [4]
- Yeast: rare (usually Candida species) [5]
- Disseminated fungal infections (e.g., Blastomyces dermatitidis, Cryptococcus neoformans)
Predisposing factors
Host-dependent factors
-
Structural or functional abnormalities of the urinary tract ; [6]
- Prevent bladder emptying and/or result in urinary stasis
- Examples include:
- Benign prostatic hyperplasia
- Congenital malformations causing vesicoureteral reflux
- Urinary bladder diverticulum
- Neurogenic bladder
- Urinary tract calculi
-
Sex
- Female individuals: anatomically predisposed because the urethra is shorter and anal and genital regions are in close proximity → bacteria spreading from the anal region → colonization of vagina → ascending UTIs [7]
- Male individuals: higher risk in uncircumcised male infants [8]
- Pregnancy: hormonal changes during pregnancy → urinary stasis and vesicoureteral reflux → increased risk of UTIs
- Postmenopause: ↓ estrogen → ↓ vaginal lactobacilli → ↑ vaginal pH → ↑ colonization by E. coli [7]
- Chronic constipation: common cause of UTIs in children
-
Prior conditions
- Previous UTI [7]
- History of kidney surgery
- Immunosuppression
- Diabetes mellitus
- Medication: recent use of antibiotics
Other factors
-
Sexual intercourse
- Postcoital cystitis (honeymoon cystitis): a lower urinary tract infection that occurs in women after recent sexual activity, which can cause irritation of the urethral meatus and facilitate bacterial entry into the urethra (e.g., from the genital and/or anal region).
- Diaphragm and spermicide use
-
Catheter-associated urinary tract infection (CAUTI)
- Caused by indwelling urinary catheters
- Most common cause of nosocomial urinary tract infection
")
")
SEEK PP = S - S. saprophyticus, E - E. coli, E - Enterococcus, K - Klebsiella, P - Proteus, P - Pseudomonas are the bacteria commonly associated with UTIs.
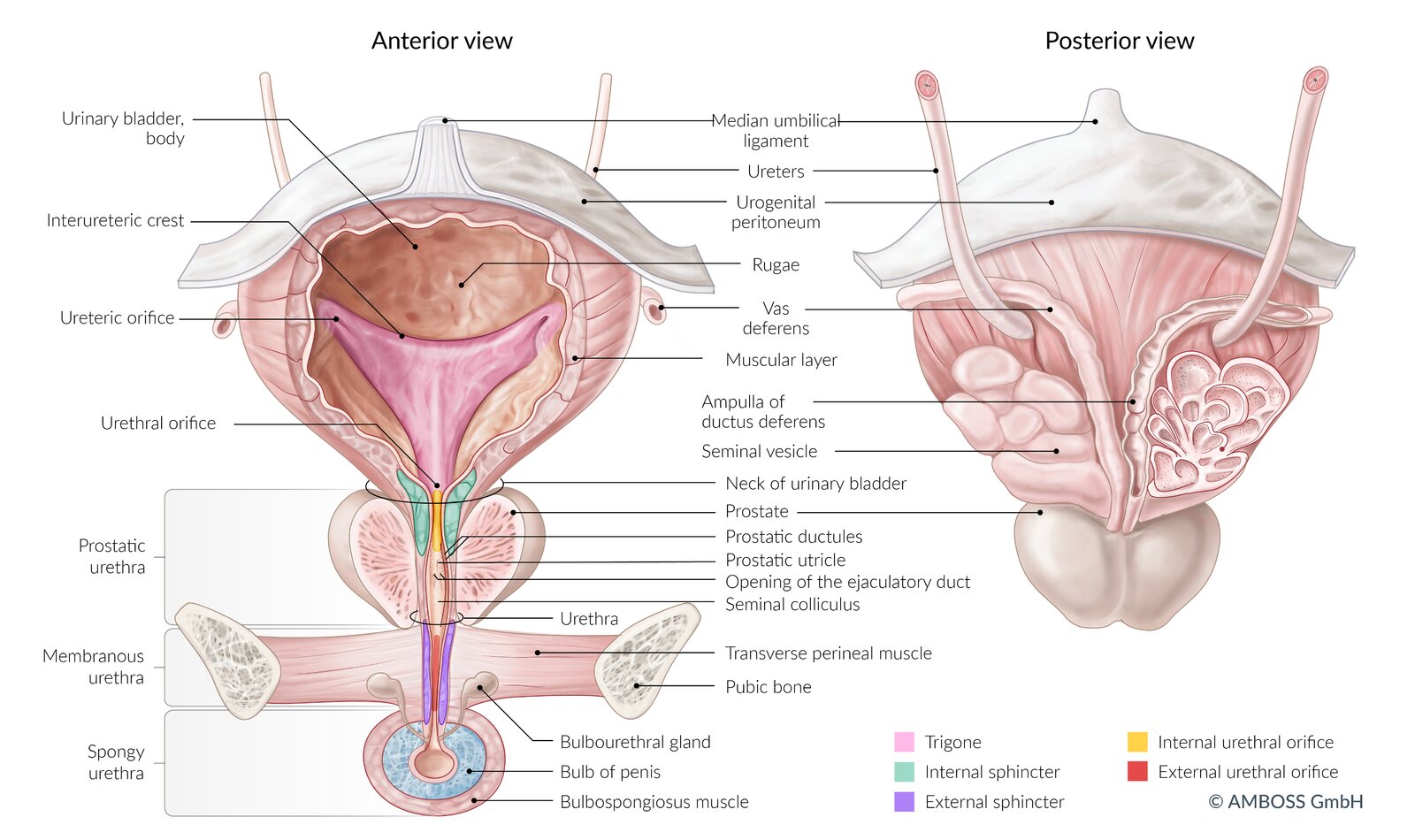
Left: ventral view of the bladder, urethra, prostate, and penis (coronal section)
Right: dorsal view of the bladder, seminal vesicles, terminal ureters, and prostate
The coronal section of the seminal vesicle and vas deferens is depicted on the right.
© AMBOSS
© AMBOSS
Classification
Urinary tract infections are classified and treated based on location, severity, source of infection, and frequency. The presence of symptoms distinguishes UTI from asymptomatic bacteriuria, which only requires treatment in a select subset of patients.
| Classification of urinary tract infections [9] | ||
|---|---|---|
| Details | ||
| By clinical presentation [10] | Asymptomatic bacteriuria (ASB) |
|
| Urinary tract infection (UTI) |
|
|
| By location [11] | Lower UTI |
|
| Upper UTI |
|
|
| By severity [12][13][14] | Uncomplicated UTI |
|
| Complicated UTI (cUTI) |
|
|
| Urosepsis |
|
|
| By source of infection [16][17] | Community-acquired UTI |
|
| Healthcare-associated UTI |
|
|
| By frequency [10] | Recurrent UTI |
|
Clinical features
-
Clinical features of lower UTI [19][20]
-
Irritative lower urinary tract symptoms (LUTS)
- Increased urinary frequency
- Urinary urgency
- Dysuria
- Hematuria
- Suprapubic tenderness
-
Irritative lower urinary tract symptoms (LUTS)
-
Clinical features of upper UTI (pyelonephritis) [21]
- Symptoms of lower UTI
- Fever
- Flank pain
- Costovertebral angle tenderness
- Fatigue/malaise
- Nausea and vomiting
- See “Clinical features” in “Pyelonephritis.”
-
Additional features (special patient groups) [19]
- Male individuals: pain in the prostatic/perineal area
- Children: See “Clinical features of pediatric UTI.”
- Older adults: delirium/acute confusion [22]
In patients with fever and/or flank pain, which are usually absent in lower UTIs, consider a more serious infection (e.g., pyelonephritis).
Dysuria without urgency or frequency may suggest vaginitis or sexually transmitted urethritis rather than cystitis, especially if accompanied by abnormal vaginal or urethral discharge. [9]
Diagnosis
In the following section, “UTI” refers to both upper and lower UTIs, while “lower UTI” typically refers to cystitis with or without urethritis (see “Classification” for details).
Approach [9][23]
Symptomatic, uncomplicated lower UTIs can be diagnosed clinically. In all other patients, urinalysis is the most important initial diagnostic test.
-
Uncomplicated lower UTI in women
- Typical symptoms : Treatment may be initiated without further diagnostics.
- Atypical or unclear symptoms: Perform urinalysis using a urine dipstick test and/or microscopy.
- Positive urinalysis (proof of pyuria and bacteriuria): Initiate treatment.
- Negative urinalysis but persisting suspicion: Obtain urine culture.
-
Complicated lower UTI in women
- Obtain urinalysis and urine culture.
- Consider the need for further diagnostics, depending on history and clinical presentation.
-
Lower UTI in men
- Obtain urinalysis and urine culture.
- First febrile UTI: Perform CT or ultrasound of the urinary tract.
- Consider referral to urology (e.g., in case of unclear diagnosis, hematuria, voiding difficulties, or recurrent UTI)
- Concomitant prostatitis: See “Diagnostics” in “Prostatitis.”
- Upper UTI: See “Diagnostics” in “Pyelonephritis.”
UTI is primarily a clinical diagnosis that is supported by typical findings on urinalysis. Urine culture is indicated in select cases to determine the causative pathogen and adapt antibiotic treatment.
Investigate isolated urethritis (i.e., without concomitant cystitis) for causes other than lower UTI (e.g., STI, reactive arthritis); see “Diagnostics for urethritis.”
Laboratory studies [24]
Urinalysis [24][25]
- Indications: best initial test for all patients
- Procedure: visual, chemical (dipstick), and microscopic examination of urine
-
Specimen collection method
- Clean-catch midstream sample: thought to reduce contamination with vaginal or skin flora
- Straight catheterization of the bladder: may be considered if the risk of contamination is high
- Suprapubic aspiration: no contamination if performed correctly but rarely used due to its invasive nature
-
Typical urinalysis findings of UTI [9]
-
Pyuria: presence of white blood cells (WBCs) in the urine
- Positive leukocyte esterase: an enzyme produced by WBC
- ≥ 5 WBC/HPF or ≥ 8–10 WBC/mm3 [24][25]
-
Bacteriuria: presence of bacteria in the urine [26]
- Positive urinary nitrites: indicate bacteria that convert nitrates to nitrites (most commonly gram-negative bacteria; e.g., E.coli)
- Direct visualization by Gram stain (seldom performed)
-
Pyuria: presence of white blood cells (WBCs) in the urine
-
Other findings
- Leukocyte casts may indicate pyelonephritis.
- Micro- or macroscopic hematuria may be present.
- Alkaline urine (pH > 8); and struvite crystals in sediment: indicate urease-producing organisms (e.g., Proteus, Klebsiella, Staphylococcus saprophyticus) [19][27]
- The presence of squamous epithelial cells can be a sign of contamination.
Urine culture [9][14][24]
-
Indications
- Suspicion for complicated UTI or healthcare-associated UTI
- Suspicion for pyelonephritis or urosepsis
-
Suspicion for uncomplicated cystitis with either of the following:
- History of recurrent UTIs [10]
- Equivocal urinalysis
- Atypical symptoms
- Concern for multiresistant pathogens, e.g., due to recent antibiotic use [15]
- Age ≥ 65 years [28]
- Follow-up cultures for test of cure in the following cases:
- Nonresolving symptoms despite antibiotic treatment
- Anatomic or functional abnormalities of the urinary tract
- Continued pathological findings on urinalysis
-
Interpretation
- Cultures are considered positive if either of the following is present:
- Significant bacteriuria: defined as ≥ 105CFU/mL in a clean-catch specimen [9][29]
- Any organisms in a specimen obtained by suprapubic aspiration [24][30]
- Cultures are considered positive if either of the following is present:
-
Typical colony findings
- E. coli: intensely pink on MacConkey agar
- Klebsiella pneumoniae: viscous colonies
- Serratia marcescens: often red in appearance
- Proteus mirabilis: swarming motility pattern
- Pseudomonas aeruginosa: blue-green pigment
In patients with complicated or recurrent urinary tract infections, a urine culture should be obtained prior to initiating antibiotic treatment. False negative results are possible if a culture is obtained after the patient has received antibiotics.
In patients with lower abdominal pain and sterile pyuria, consider bladder or ureteral irritation from an intraabdominal or pelvic infection unrelated to the urinary tract (e.g., appendicitis, diverticulitis). [31][32]
Additional diagnostics [9][15][23]
- Pregnancy test: indicated in women of childbearing age
-
Testing for sexually transmitted infections (STIs)
- Indicated in patients with STI risk factors and/or symptoms of an STI
- At-risk patients should be tested for Chlamydia trachomatis and Neisseria gonorrhoeae.
-
Blood tests
- Not routinely performed in patients with lower UTI
- May be indicated to assess concomitant conditions (e.g., diabetes mellitus) and exclude differential diagnoses
Imaging [14][15][33]
Imaging is generally not indicated or helpful for the diagnosis of lower UTI, but it may be performed in select patients to rule out complicating factors (e.g., urinary tract obstruction) or if complicated pyelonephritis or urosepsis are suspected. For imaging indications and findings in upper UTI, see “Diagnostics” in “Pyelonephritis.”
-
Indications may include:
- Suspected urinary tract obstruction
- Severe illness (e.g., septic shock)
- Early recurrence of UTI (within two weeks of appropriate treatment)
- Persistent bacteriuria despite treatment
- Recurrent complicated UTI
- Men with febrile UTI
-
Modalities
-
CT abdomen and pelvis with or without IV contrast
- Most sensitive for initial imaging
- Noncontrast CT is useful to diagnose urolithiasis.
- IV contrast is indicated if complications (e.g., abscess) or other causes of obstruction are suspected.
-
Ultrasound of the kidneys and bladder
- Perform if there are contraindications to contrast or radiation.
- Useful for detecting hydronephrosis and measuring postvoid residual volume if an obstruction is suspected
- Additional modalities include MRI abdomen and pelvis, voiding cystourethrography, and retrograde cystography.
-
CT abdomen and pelvis with or without IV contrast
Imaging is not routinely necessary for patients with uncomplicated lower UTI.
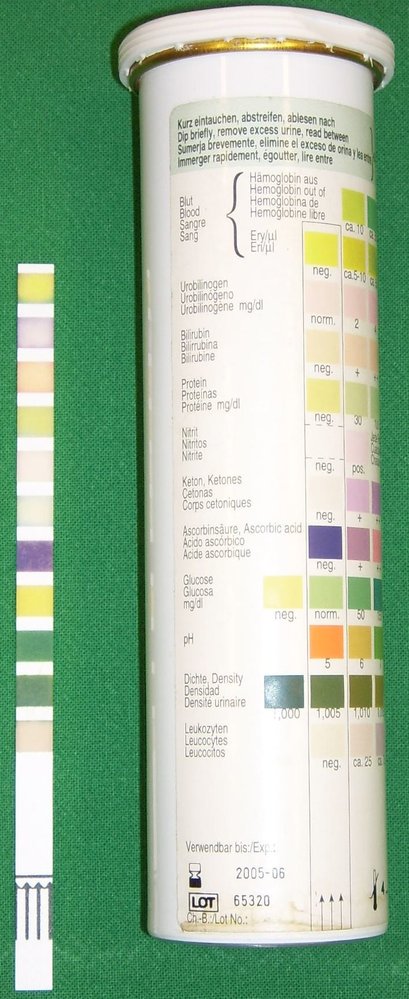
Left: test strip following immersion in urine
Right: test strip packaging with instructions on how to interpret findings
Source: “Urine Quicktest” by Uwe Gille, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}
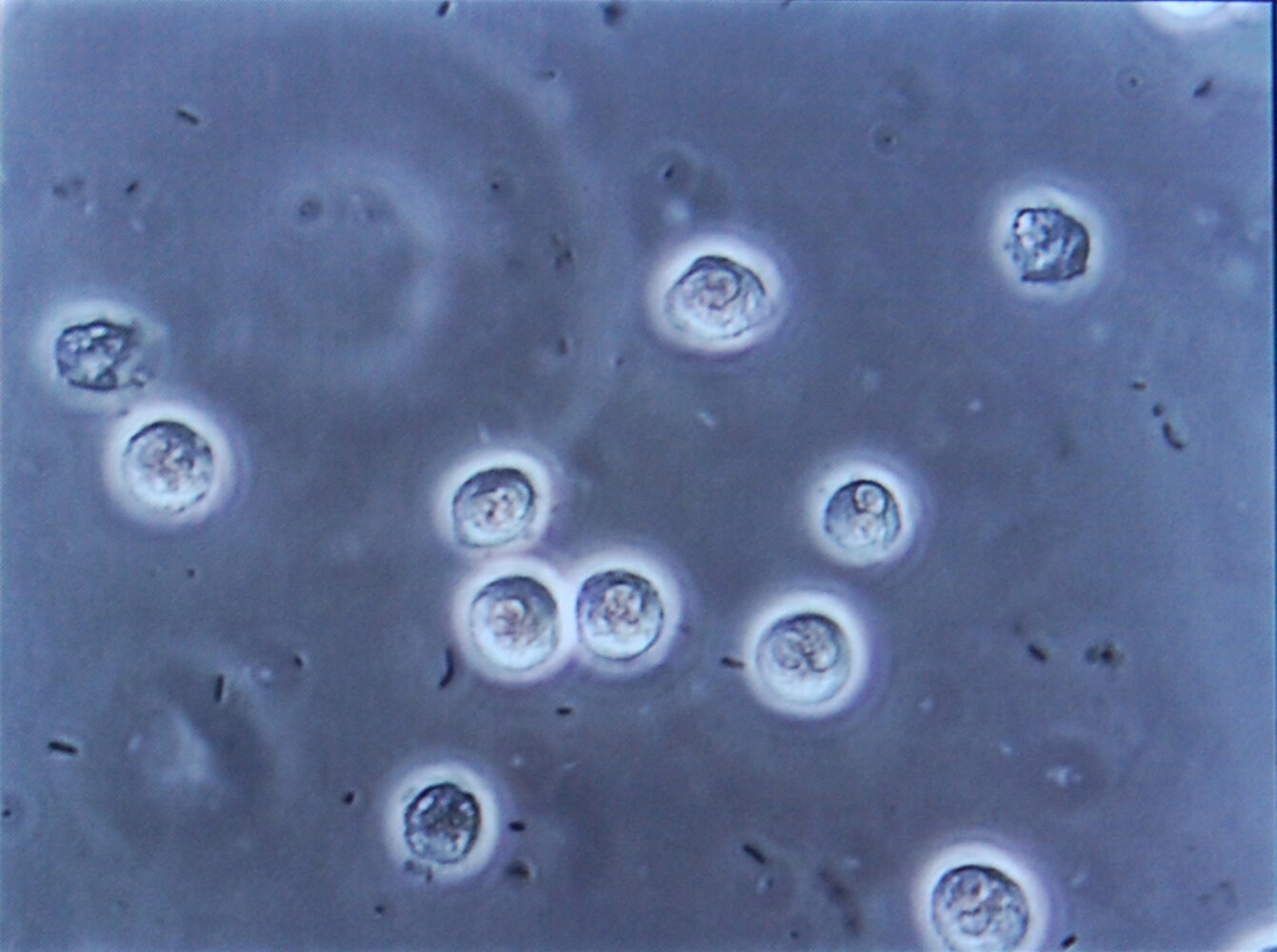
Photomicrograph of a urine specimen (high magnification)
Multiple white blood cells (large, light-colored structures) and bacteria (small black structures) are visible.
The presence of white blood cells (pyuria) and bacteria (bacteriuria) in the urine is characteristic of urinary tract infection.
Source: “Bacteriuria pyuria 4” by Steven Fruitsmaak, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}
Differential diagnoses
Asymptomatic bacteriuria (ASB) [26][34][35]
-
Description
- Presence of ≥ 100,000 CFU/mL in at least two voided urine samples in patients with no symptoms of UTI (e.g., dysuria, frequency, urgency, suprapubic pain)
- Bacteriuria typically resolves spontaneously in healthy, nonpregnant women without any side effects.
- Women with asymptomatic bacteriuria are more likely to develop future UTIs than women with no bacteriuria.
-
Epidemiology
-
Prevalence
- Occurs in 1–5% of healthy, premenopausal women and in 2–10% of pregnant women
- Occurs in 9–25% of older adults and individuals with diabetes, indwelling catheters, or spinal cord injuries
-
Prevalence
- Etiology: E. coli is the most common causative organism.
-
Risk factors
- Age ≥ 65 years
- Diabetes mellitus
- Spinal cord injury
- Indwelling urethral catheter
- Pregnancy
-
Diagnosis: urinalysis with microscopy
- Mid-stream urine sample: bacterial growth ≥ 100,000 CFU/mL in two consecutive samples in women or in one sample in men
- Catheterized urine sample: bacterial growth ≥ 100 CFU/mL in one sample in women or men
-
Management
- Treatment is recommended in:
- Individuals undergoing endourological procedures with possible mucosal trauma [36]
- Pregnant women: See “Treatment of ASB and lower UTIs in pregnant women” below.
-
Treatment is not recommended in:
- Healthy, nonpregnant women
- Older adults and individuals with diabetes, indwelling catheters, or spinal cord injuries
- Treatment is recommended in:
Other differential diagnoses
- Interstitial cystitis
- Vaginitis
- Pelvic inflammatory disease (PID)
- Prostatitis [37]
- Urethritis with sexually transmitted infections (e.g., Neisseria gonorrhoeae, Chlamydia trachomatis), Candida, or irritants
- Tuberculous cystitis (see “Urogenital tuberculosis”)
- Drug-induced cystitis (e.g., cyclophosphamide, NSAIDs) or radiation-induced cystitis
- Hemorrhagic cystitis
- Trauma
- Structural abnormalities of the urethra (e.g., diverticula, strictures)
- Other diseases of the bladder (e.g., urolithiasis, bladder cancer, foreign objects)
The differential diagnoses listed here are not exhaustive.
Treatment
In the following section, “UTI” refers to both upper and lower UTIs, while “lower UTI” typically refers to cystitis with or without urethritis (see “Classification” for details).
General principles [9][14][23][38]
-
Antibiotic treatment is recommended for all patients with symptomatic UTI.
- The optimal therapy depends on disease severity, local resistance patterns, and patient characteristics (e.g., allergies).
- Initial treatment is with an empiric regimen, which is maintained for uncomplicated cystitis.
- In unclear or complicated cases, the regimen may subsequently have to be adjusted based on urine culture data.
- Consider the need for supportive treatment.
- Phenazopyridine, a urinary analgesic, can be used for symptomatic relief for a maximum of 2 days.
- Oral analgesia, e.g., with NSAIDs, can provide additional relief.
- For the treatment of upper UTI, see “Treatment of pyelonephritis.”
Consider empiric treatment of STIs in patients with isolated urethritis, prostatitis, or suspected pelvic inflammatory disease (see “Treatment of PID”).
Uncomplicated lower UTI [14][38][39]
- Management can typically be done in the outpatient setting with oral therapy.
- Treatment duration depends on the chosen antibiotic agent.
- Symptom relief can be expected to occur after an average of 36 hours. [29]
- Persistent symptoms despite antibiotic therapy suggest complicated UTI and/or indicate the need to change the empiric therapy.
Empiric antibiotic treatment of uncomplicated lower UTIs
-
First-line treatment
- Nitrofurantoin for 5 days
- Trimethoprim/sulfamethoxazole (TMP/SMX) for 3 days
- Fosfomycin (single dose)
-
Second-line treatment: beta-lactam antibiotics for 5–7 days
- Aminopenicillins plus beta-lactamase inhibitors, e.g., amoxicillin/clavulanic acid
- Oral cephalosporins, e.g., cefpodoxime , cefdinir , or cefaclor
- Alternatives: Consider fluoroquinolones, e.g., ciprofloxacin for 3 days for patients with previous infections with bacteria resistant to other drug classes. [39]
Complicated lower UTI [9][14][40][41]
- There are few recommendations for the empiric antibiotic treatment of complicated lower UTI.
- Empiric antibiotic therapy should have broad-spectrum activity against the expected uropathogens.
- Because UTIs in men can involve the prostate, antibiotics should be able to penetrate prostate tissue (e.g., fluoroquinolones, TMP/SMX).
- In addition to antibiotic therapy, complicating factors (e.g., obstruction) should be treated, if possible.
-
For UTI in men, referral to urology may be warranted especially in the following cases:
- Treatment failure or recurrent UTIs
- Hematuria
- Voiding difficulties or acute urine retention [23]
- Suspected acute bacterial prostatitis
- Hospitalization and initial intravenous treatment may be necessary in the following cases: [15]
- Severe systemic symptoms, e.g., signs of shock
- Inability to tolerate oral antibiotics
- Severe comorbidities, e.g., immunocompromise or heart failure
Antibiotic treatment of complicated lower UTIs [14][40]
- Antibiotic therapy must be adapted to culture results and is commonly given for 7–14 days.
- Options for the initial empiric treatment of complicated lower UTIs include:
- Fluoroquinolones PO or IV: e.g., ciprofloxacin or levofloxacin
-
Beta lactams
- Second-generation or third-generation cephalosporins: e.g., ceftriaxone
- Extended-spectrum penicillins: e.g., ampicillin/sulbactam
- Aminoglycosides (e.g., gentamicin ): treatment option if fluoroquinolones or beta lactams are contraindicated or as an addition to beta lactams
-
Reasonable options if the pathogen is susceptible include: [42]
- Nitrofurantoin
- TMP/SMX
- Fosfomycin (multiple doses) [42][43]
Treatment regimens for UTI in men should include antibiotics that are able to penetrate prostate tissue (e.g., fluoroquinolones or TMP/SMX). Fosfomycin or nitrofurantoin are generally not adequate.
Management of complicating factors
- Nephrolithiasis: In UTI with renal obstruction, urgent urology consultation is required for drainage. [44]
-
Indwelling medical devices (e.g., ureteral stents, percutaneous nephrostomy tubes) [45][46]
- Management of infections may require exchange or removal of the device, especially when it is obstructed.
- Urology should be consulted urgently for further management.
- Other treatable factors should be addressed: e.g., optimal blood sugar control for diabetics.
Recurrent UTI [10][47]
Recurrent UTIs are common in women and are defined as ≥ 3 episodes of symptomatic, culture-proven UTI in one year or ≥ 2 episodes in 6 months. Management involves the implementation of preventive measures and antibacterial prophylaxis in addition to the antibiotic treatment of acute episodes.
Acute management
Whenever possible, obtain a urine culture for every episode prior to initiating antibiotic therapy.
-
Choice of antibiotic
- First recurrence: See “Antibiotic treatment for uncomplicated lower UTIs” and “Antibiotic treatment for complicated lower UTIs” for initial empiric regimens.
- Frequent recurrences
- Regimens should be tailored to the patient and prior culture results.
- Consider increased antibiotic resistance to standard agents.
- Antibiotics must be adapted to the current culture results once available.
-
Self-initiated treatment
- May be considered for motivated women who have documented recurrent UTIs.
- Patients are given a prescription to fill when symptoms start.
- Reevaluation is required if no improvement occurs within 48 hours.
- Follow-up: Consider test of cure with repeat urine culture only if symptoms persist beyond 7 days.
Antibiotic prophylaxis [10]
- Indication: may be considered in all women with recurrent uncomplicated UTIs
-
Continuous prophylaxis
- Typically taken for 3–12 months with periodic reassessment
- Regimens
- Trimethoprim (TMP) daily
- TMP/SMX daily
- Cephalexin daily
- Nitrofurantoin daily
- Fosfomycin every 10 days
-
Intermittent or postcoital prophylaxis
- Recommended for women who have recurrent UTIs associated with sexual activity
- Substances
- TMP/SMX
- Cephalexin
- Nitrofurantoin
Nonantibiotic prophylaxis [48]
- There is insufficient high-quality data to support the use of cranberry products for preventing UTIs. [49][50]
- Topical estrogen therapy may be considered in peri- and postmenopausal women.
- Behavioral modifications (e.g., increased fluid intake, postcoital voiding) may be helpful.
Candiduria [51]
- Candida isolated from the urine rarely indicates systemic infection, but it may be a marker for greater mortality in severely ill patients.
- Predisposing factors should be treated in all cases of candiduria, e.g., by removing indwelling catheters whenever possible.
- Indications for antifungal treatment include symptomatic cystitis or pyelonephritis, neutropenia, or a planned urologic procedure.
- Commonly used antifungals include fluconazole and amphotericin B.
- Consult the infectious disease service for assistance with appropriate antifungal treatment.
Complications
-
General
- Pyelonephritis
- Perinephric abscess
- Urosepsis
- Emphysematous pyelonephritis
-
In male individuals
- Urethral stricture
- Epididymitis
- Prostatitis
- Orchitis
-
In pregnant women [52]
- Increased risk of preterm labor and birth [53]
- Hypertension and preeclampsia
- Chorioamnionitis
We list the most important complications. The selection is not exhaustive.
Prevention
-
Behavioral modifications [54]
- Increased fluid intake
- Timely bladder voiding
- Postcoital voiding
- Adequate genital hygiene
-
Clean intermittent catheterization
- Indicated for individuals with neurogenic bladder
- Reduces incidence of catheter-associated UTIs
- Prophylaxis: indicated for recurrent urinary tract infections (see ”Chemoprophylaxis” in “Recurrent UTI” for details)
Catheter-associated UTI (CAUTI)
Overview [14][16]
-
Definitions
- Catheter-associated UTI (CAUTI): symptomatic UTI occurring in a patient with an indwelling urinary catheter OR within 48 hours after removal of a urinary catheter
- Catheter-associated asymptomatic bacteriuria (CAASB): bacteriuria (≥ 105CFU/mL) without symptoms in a patient with an indwelling urinary catheter OR within 48 hours after removal of a urinary catheter
- Epidemiology: CAUTIs are among the most common healthcare-associated infections. [16]
-
Microbiology
- Causative organisms are likely to have antibiotic resistance.
- In patients with long-term catheterization (≥ 30 days), UTIs are typically polymicrobial.
-
Clinical features
- Infection is commonly asymptomatic or presents with atypical symptoms.
- Possible symptoms include fever, pelvic or flank pain, hematuria, altered mental status, and lethargy.
- Catheter obstruction may result from colonization with urease-producing organisms, especially Proteus spp.
Diagnostics
A urine culture, ideally obtained prior to antibiotic treatment, is always required to diagnose CAUTI.
- Indications: features consistent with potential infection
- Specimen collection: ideally from the sampling port of a newly inserted device using aseptic technique
-
Diagnostic criteria
-
Significant bacteriuria thresholds in catheterized patients [16]
- CAASB: ≥ 105CFU/mL without symptoms
- CAUTI: ≥ 103CFU/mL with symptoms of UTI
- Pyuria is usually present but is not diagnostic of CAUTI in isolation.
-
Significant bacteriuria thresholds in catheterized patients [16]
To reduce false-positive results, avoid sampling urine for culture from previously inserted catheters or collection bags, as these sites are frequently colonized by bacteria within a few hours of catheter insertion. [55]
Treatment
-
Catheter removal or replacement
- Remove if no longer necessary.
- Replace if still necessary and present for > 2 weeks.
-
Antibiotic therapy
- Guided by culture results and local resistance patterns
- See “Antibiotic treatment of complicated lower UTIs” and “Empiric antibiotic therapy of complicated pyelonephritis” for potential empiric regimens.
- Duration: typically 7–14 days depending on the resolution of symptoms
- Prevention: See “Prevention of catheter-associated urinary tract infections.”
Special patient groups
See also “Urinary tract infections in children and adolescents.”
UTI in older adults [56]
- UTI is very common in advanced age, both in individuals who live in long-term care facilities and those who do not.
- Symptoms of UTI are more commonly atypical (e.g., back pain, pelvic pain, constipation, urinary incontinence, and altered mental status).
- Management principles are generally the same as outlined above.
- Preventative strategies include increased fluid intake and increasing mobility (see also “Prevention” above).
UTI in pregnancy [57]
Pathophysiology
- Pregnancy may increase the risk of recurrent bacteriuria and UTIs.
-
Factors involved
- Increased progesterone levels → urinary stasis and ureteral smooth muscle relaxation and dilation → vesicoureteral reflux
- Gravid uterus → ↑ pressure on the bladder and compression of ureters → vesicoureteral reflux
- Relative immunosuppression
Asymptomatic bacteriuria in pregnancy [14][34]
- See “Asymptomatic bacteriuria” for diagnostic criteria.
- Screening is recommended for all pregnant women in the first trimester.
- Treatment is always required, as evidence suggests that it reduces the risk of pyelonephritis and fetal complications.
Treatment of ASB and lower UTIs in pregnancy [14][58]
Although UTI in pregnancy is generally considered complicated, treatment regimens for ASB and lower UTI in pregnancy may include those typically used for uncomplicated UTI and should be adapted to the patient's individual risk and urine culture results. [14][34]
- Upper UTIs generally require hospitalization and intravenous treatment; see “Pyelonephritis in pregnancy.”
-
Empiric antibiotics for ASB and lower UTI considered appropriate during pregnancy include:
- Fosfomycin
-
Beta-lactam antibiotics for 5–7 days
- Oral cephalosporins (e.g., cefpodoxime )
- Aminopenicillins plus beta-lactamase inhibitors (e.g., amoxicillin/clavulanic acid )
-
Antibiotics that are potentially appropriate during specific stages of pregnancy include:
- Nitrofurantoin for 5 days: Avoid close to the delivery date.
- TMP/SMX for 3 days: Avoid during the first trimester and past 32 weeks' gestation.
- Antibiotics that should be avoided include fluoroquinolones and aminoglycosides.
-
Follow-up culture should be considered a week after treatment for ASB and UTI.
- Negative culture: no further treatment required unless new UTI symptoms develop
- Positive culture: indicates persistent bacteriuria; antibiotic therapy based on the culture results
Asymptomatic bacteriuria in pregnancy is a risk factor for pyelonephritis and should be treated.
Related One-Minute Telegram
- One-Minute Telegram 127-2025-2/3: A new oral option for UTIs?
- One-Minute Telegram 43-2022-3/3: Is fosfomycin effective in treating multidrug-resistant E. coli?
- One-Minute Telegram 32-2021-3/3: Are seven days of antibiotics sufficient to treat UTI in men?
Interested in the newest medical research, distilled down to just one minute? Sign up for the One-Minute Telegram in “Tips and links” below.
External Resources
- Sign up for the One-Minute Telegram
- 2022 AUA/CUA/SUFU Updates to Recurrent Uncomplicated Urinary Tract Infections in Women
- 2019 IDSA Clinical Practice Guideline for the Management of Asymptomatic Bacteriuria
- 2019 AUA/CUA/SUFU Guideline on Recurrent Uncomplicated Urinary Tract Infections in Women
- 2010 IDSA/ESCMID Guidelines for the Treatment of Acute Uncomplicated Cystitis and Pyelonephritis in Women
- 2009 IDSA Guidelines for the Management of CAUTI
- EAU Guidelines for the Management of Urological Infections
- US Preventive Services Task Force Recommendations (Asymptomatic Bacteriuria in Adults)
References
- Ronald A. "The etiology of urinary tract infection: traditional and emerging pathogens". Am J Med. 113(1). :14-19. (2002)
- "Medical Student Curriculum: Pediatric Urinary Tract Infections". https://www.auanet.org/education/auauniversity/for-medical-students/medical-students-curriculum/medical-student-curriculum/pediatric-uti. [2016-07-01]
- Paduch DA. "Viral lower urinary tract infections". Curr Urol Rep. 8(4). :324-35. (2007)
- Kauffman CA. "Diagnosis and Management of Fungal Urinary Tract Infection". Infect Dis Clin North Am. 28(1). :61-74. (2014)
- Kauffman CA. "Candiduria". Clin Infect Dis. 41(Supplement_6). :S371-S376. (2005)
- Fischer C. "Master the Boards USMLE Step 2 CK". Kaplan Publishing. (2013). ISBN: 9781609787608
- Ahmad Nikibakhsh. "Clinical Management of Complicated Urinary Tract Infection". InTech. (2011). ISBN: 9789533073934
- Shapiro E. "American academy of pediatrics policy statements on circumcision and urinary tract infection". Rev Urol. 1(3). :154-6. (1999)
- Flores-Mireles et al. "Urinary tract infections: epidemiology, mechanisms of infection and treatment options". Nature Reviews Microbiology. 13(5). :269-284. (2015)
- Hooton TM, Gupta K. "Acute Uncomplicated Cystitis in Women". UpToDate. UpToDate. https://www.uptodate.com/contents/acute-uncomplicated-cystitis-in-women. [2017-12-06]
- Hooton TM, Gupta K. "Acute Complicated Urinary Tract Infection (Including Pyelonephritis) in Adults". UpToDate. UpToDate. https://www.uptodate.com/contents/acute-complicated-urinary-tract-infection-including-pyelonephritis-in-adults. [2018-03-16]
- Kuswardhani RAT, Sugi YS. "Factors Related to the Severity of Delirium in the Elderly Patients With Infection". Gerontology and Geriatric Medicine. 3. :233372141773918. (2017)
- Jameson JL, Fauci AS, Kasper DL, et al. "Harrison's Principles of Internal Medicine, Twentieth Edition (Vol.1 & Vol.2)". McGraw-Hill Education / Medical. (2018). ISBN: 9781259644030
- Gupta K. "Urinary Tract Infection". Ann Intern Med. 156(5). :ITC3. (2012)
- Wilson ML, Gaido L. "Laboratory Diagnosis of Urinary Tract Infections in Adult Patients". Clin Infect Dis. 38(8). :1150-1158. (2004)
- Simerville JA, Maxted WC, Pahira JJ. "Urinalysis: a comprehensive review". Am Fam Physician. 71(6). :1153-62. (2005)
- Colgan R, Nicolle LE, McGlone A, Hooton TM. "Asymptomatic bacteriuria in adults". Am Fam Physician. 74(6). :985-90. (2006)
- Brown PD. "Management of Urinary Tract Infections Associated with Nephrolithiasis". Curr Infect Dis Rep. 12(6). :450-454. (2010)
- "2021 EAU Guideline on Urological Infections". https://web.archive.org/web/20210611080346/https://uroweb.org/guideline/urological-infections/. [2021-03-01]
- Anger J, Lee U, Ackerman AL, et al. "Recurrent Uncomplicated Urinary Tract Infections in Women: AUA/CUA/SUFU Guideline". J Urol. 202(2). :282-289. (2019)
- Walls R, Hockberger R, Gausche-Hill M. "Rosen's Emergency Medicine". Elsevier Health Sciences. (2018). ISBN: 9780323354790
- Mody L, Juthani-Mehta M. "Urinary Tract Infections in Older Women". JAMA. 311(8). :844. (2014)
- Colgan, Williams. "Diagnosis and Treatment of Acute Uncomplicated Cystitis". American Family Physician. (2011)
- Doern CD, Richardson SE. "Diagnosis of Urinary Tract Infections in Children". J Clin Microbiol. 54(9). :2233-2242. (2016)
- Hooker JB, Mold JW, Kumar S. "Sterile Pyuria in Patients Admitted to the Hospital With Infections Outside of the Urinary Tract". J Am Board Fam Med. 27(1). :97-103. (2014)
- Goonewardene S, Persad R. "Sterile pyuria: a forgotten entity". Ther Adv Urol. 7(5). :295-298. (2015)
- Venkatesan AM, Oto A, Allen BC, et al. "ACR Appropriateness Criteria® Recurrent Lower Urinary Tract Infections in Females". J Am Coll Radiol. 17(11). :S487-S496. (2020)
- Nicolle LE, Gupta K, Bradley SF, et al. "Clinical Practice Guideline for the Management of Asymptomatic Bacteriuria: 2019 Update by the Infectious Diseases Society of America". Clin Infect Dis. (2019)
- "Guidelines on Urological infections 2019". https://uroweb.org/wp-content/uploads/EAU-Guidelines-on-Urological-infections-2019.pdf. [2019-03-01]
- "Asymptomatic Bactetiuria". https://www.aafp.org/afp/2020/0715/p99.html. [2020-07-15]
- Le T, Bhushan V, Chen V, King M. "First Aid for the USMLE Step 2 CK". McGraw-Hill Education. (2015). ISBN: 9780071844574
- Gupta K, Hooton TM, Naber KG, et al. "International Clinical Practice Guidelines for the Treatment of Acute Uncomplicated Cystitis and Pyelonephritis in Women: A 2010 Update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases". Clin Infect Dis. 52(5). :e103-e120. (2011)
- Lee RA, Centor RM, Humphrey LL, et al. "Appropriate Use of Short-Course Antibiotics in Common Infections: Best Practice Advice From the American College of Physicians". Ann Intern Med. (2021)
- Murphy JE, Lee MW-L. "PSAP 2018 Book 1: Infectious Diseases". American College of Clinical Pharmacy. (2018). ISBN: 9781939862600
- Levison ME, Kaye D. "Treatment of Complicated Urinary Tract Infections With an Emphasis on Drug-Resistant Gram-Negative Uropathogens". Curr Infect Dis Rep. 15(2). :109-115. (2013)
- Bennett JE, Dolin R, Blaser MJ. "Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases". Elsevier. (2019). ISBN: 9780323482554
- Derington CG, Benavides N, Delate T, Fish DN. "Multiple-Dose Oral Fosfomycin for Treatment of Complicated Urinary Tract Infections in the Outpatient Setting". Open Forum Infect Dis. 7(2). (2020)
- Assimos D, Krambeck A, Miller NL et al. "Surgical Management of Stones: American Urological Association/Endourological Society Guideline, PART II". J Urol. 196(4). :1161-1169. (2016)
- Dyer RB, Chen MY, Zagoria RJ, et al. "Complications of Ureteral Stent Placement". RadioGraphics. 22(5). :1005-1022. (2002)
- Huang S, Philip A, Richter M, et al. "Prevention and Management of Infectious Complications of Percutaneous Interventions". Semin Intervent Radiol. 32(02). :078-088. (2015)
- Kodner CM, Thomas Gupton EK. "Recurrent urinary tract infections in women: diagnosis and management". Am Fam Physician. 82(6). :638-43. (2010)
- Bixler BR, Anger JT. "Updates to Recurrent Uncomplicated Urinary Tract Infections in Women: AUA/CUA/SUFU Guideline". J Urol. 208(4). :754-756. (2022)
- Ruth G Jepson, Gabrielle Williams, Jonathan C Craig. "Cranberries for preventing urinary tract infections". Cochrane Database of Systematic Reviews. (2012)
- Luís Â, Domingues F, Pereira L. "Can Cranberries Contribute to Reduce the Incidence of Urinary Tract Infections? A Systematic Review with Meta-Analysis and Trial Sequential Analysis of Clinical Trials". J Urol. 198(3). :614-621. (2017)
- Pappas PG, Kauffman CA, Andes DR et al. "Clinical Practice Guideline for the Management of Candidiasis: 2016 Update by the Infectious Diseases Society of America". Clin Infect Dis. 62(4). :e1-e50. (2015)
- Loh K, Sivalingam N. "Urinary tract infections in pregnancy". Malaysian family physician : the official journal of the Academy of Family Physicians of Malaysia. 2(2). :54-7. (2007)
- Verma I, Avasthi K, Berry V. "Urogenital infections as a risk factor for preterm labor: a hospital-based case-control study". J Obstet Gynaecol India. 64(4). :274-8. (2014)
- Ghouri F, Hollywood A, Ryan K. "A systematic review of non-antibiotic measures for the prevention of urinary tract infections in pregnancy". BMC Pregnancy Childbirth. 18(1). :99. (2018)
- Rowe TA, Juthani-Mehta M. "Diagnosis and Management of Urinary Tract Infection in Older Adults". Infect Dis Clin North Am. 28(1). :75-89. (2014)
- Schnarr J, Smaill F. "Asymptomatic bacteriuria and symptomatic urinary tract infections in pregnancy". Eur J Clin Invest. 38. :50-57. (2008)
- Bookstaver PB, Bland CM, Griffin B, et al. "A Review of Antibiotic Use in Pregnancy". Pharmacotherapy. 35(11). :1052-1062. (2015)
- Katz MH, Doherty GM. "Current Diagnosis and Treatment Surgery, 15th Edition". McGraw-Hill Education / Medical. (2020). ISBN: 9781260122213
- Hooton TM. "Uncomplicated Urinary Tract Infection". N Engl J Med. 366(11). :1028-1037. (2012)
- Colgan R, Williams M. "Diagnosis and treatment of acute uncomplicated cystitis". Am Fam Physician. 84(7). :771-6. (2011)
- Hooton TM, Bradley SF, Cardenas DD, et al. "Diagnosis, Prevention, and Treatment of Catheter-Associated Urinary Tract Infection in Adults: 2009 International Clinical Practice Guidelines from the Infectious Diseases Society of America". Clin Infect Dis. 50(5). :625-663. (2010)
- Cardoso T, Almeida M, Friedman ND, et al. "Classification of healthcare-associated infection: a systematic review 10 years after the first proposal". BMC Med. 12(1). (2014)
- Magill SS, Edwards JR, Bamberg W, et al. "Multistate point-prevalence survey of health care-associated infections". N Engl J Med. 370(13). :1198-1208. (2014)
- Miller JM, Binnicker MJ, Campbell S, et al. "A Guide to Utilization of the Microbiology Laboratory for Diagnosis of Infectious Diseases: 2018 Update by the Infectious Diseases Society of America and the American Society for Microbiology". Clin Infect Dis. 67(6). :e1-e94. (2018)