Summary
Vaccination is a very effective measure for providing immunity to many infectious diseases. The discovery of vaccines played a central part in the eradication of smallpox and helped significantly reduce the incidence of potentially severe diseases such as poliomyelitis and measles. Live vaccines (attenuated, i.e., noninfective pathogens), inactivated vaccines (subunits or complete pathogens), viral vector vaccines, and nucleic acid vaccines (DNA, RNA, mRNA, or viral replicons) are used to achieve active immunization, which enables the host's immune system to build up a sustained immune response to specific pathogens. The immune response may be measured and quantified by assessing the antibody titer. In the event of potential disease (e.g., after exposure to high-risk pathogens), if the immune system is unable to produce sufficient antibodies fast enough, passive immunization can offer immediate short-term protection via direct injection of pooled antibodies for many conditions. Modern vaccines are usually well-tolerated, and adverse events are rare. However, the intervals between vaccine administration and possible contraindications must be considered. Vaccine hesitancy is an ambivalence or resistance toward receiving vaccination, which may influence the uptake of vaccinations. Vaccine hesitancy can be addressed by empathetically addressing patients' vaccine-related concerns and using motivational interviewing techniques.
For ACIP vaccination recommendations, see “Immunization schedule.”
Definitions
-
Vaccine
- A product (e.g., dead or weakened organism) that provides immunity from a disease
- May be administered through injection, orally, or nasally
- Vaccination: administration of a vaccine that induces an active immune reaction in form of cellular and/or humoral response, providing immunity against a pathogen
-
Immunization
- The process by which a person becomes protected from a disease
- Vaccines and recovering from some infections cause immunization.
References:[1]
Aims of routine immunization
-
Herd immunity
- Once a certain percentage of the population has received immunization, nonvaccinated individuals (e.g., children too young to receive vaccination) will also be protected.
- Mass vaccination: Vaccination of a large number of people in the shortest possible time after the outbreak of an epidemic, with the goal of herd immunity.
-
Eradication of disease
- High immunization rates over prolonged periods of time can achieve eradication of certain diseases. [2]
- To date, only two diseases have been eradicated by human efforts: smallpox (1980) and rinderpest (2011).
- Lower incidence and associated risks: The Haemophilus influenzae type b (Hib) vaccine has decreased the number of cases of invasive Hib disease (e.g., pneumonia, bacteremia, meningitis, epiglottitis, infectious arthritis) in children younger than 5 by more than 99%. [3]
Passive immunization
-
Mechanism of action
- Injection of preformed antibodies induces a rapid humoral response against a specific pathogen
- Provides only temporary protection, as antibodies have a half-life of ∼ 3 weeks and their titers decrease over time.
-
Examples
- Antitoxins
- Humanized monoclonal antibodies
- Maternal immunoglobulins that are transmitted via breast milk (IgA) or cross the placenta (IgG) to provide passive immunity
- Intravenous immunoglobulins to provide temporary passive immunity to a specific pathogen (e.g., CMV)
-
Indications
-
Acute, post-exposure elimination of a pathogen
- Viruses: rubella, rabies, hepatitis B
- Toxins: tetanus, botulinum, diphtheria
- Rhesus incompatibility prevention
-
Acute, post-exposure elimination of a pathogen
- Application: Vaccines are available for intramuscular as well as for intravenous injection .
-
Combination
-
Simultaneous vaccination
- Two different passive vaccines may be administered simultaneously.
- An inactivated active and a passive vaccine may be administered simultaneously (e.g., in acute hepatitis A, hepatitis B, rabies, or tetanus infection). [4]
- After transfusion of certain blood products and/or immunoglobulin therapy, live vaccines should be delayed depending on the estimated amount of IgG in the transfusion. [5][6]
-
Simultaneous vaccination
“Passive immunization Helps Beat The Disease Rapidly:” HBV, Botulinum, Tetanus, Diphtheria, and Rabies are indications for passive immunization.
Active immunization
-
General information
- In active immunity, the body's immune system reacts to the presence of antigens by producing antibodies.
- In general, a combination of different active vaccinations is possible.
- Slow onset, but immunity usually lasts for years or even a lifetime.
- Besides vaccines and toxoids, natural infections lead to active immunization as well.
-
Classification
- Live attenuated vaccines
-
Inactivated vaccines
- Whole vaccines
-
Subunit vaccines
- Protein-based (subunit and toxoid vaccines)
- Polysaccharide-based
- Viral vector vaccines
- Nucleic acid vaccines (DNA, RNA, mRNA, or viral replicons)
Current vaccination recommendations for the US can be found in the “Immunization schedule.”

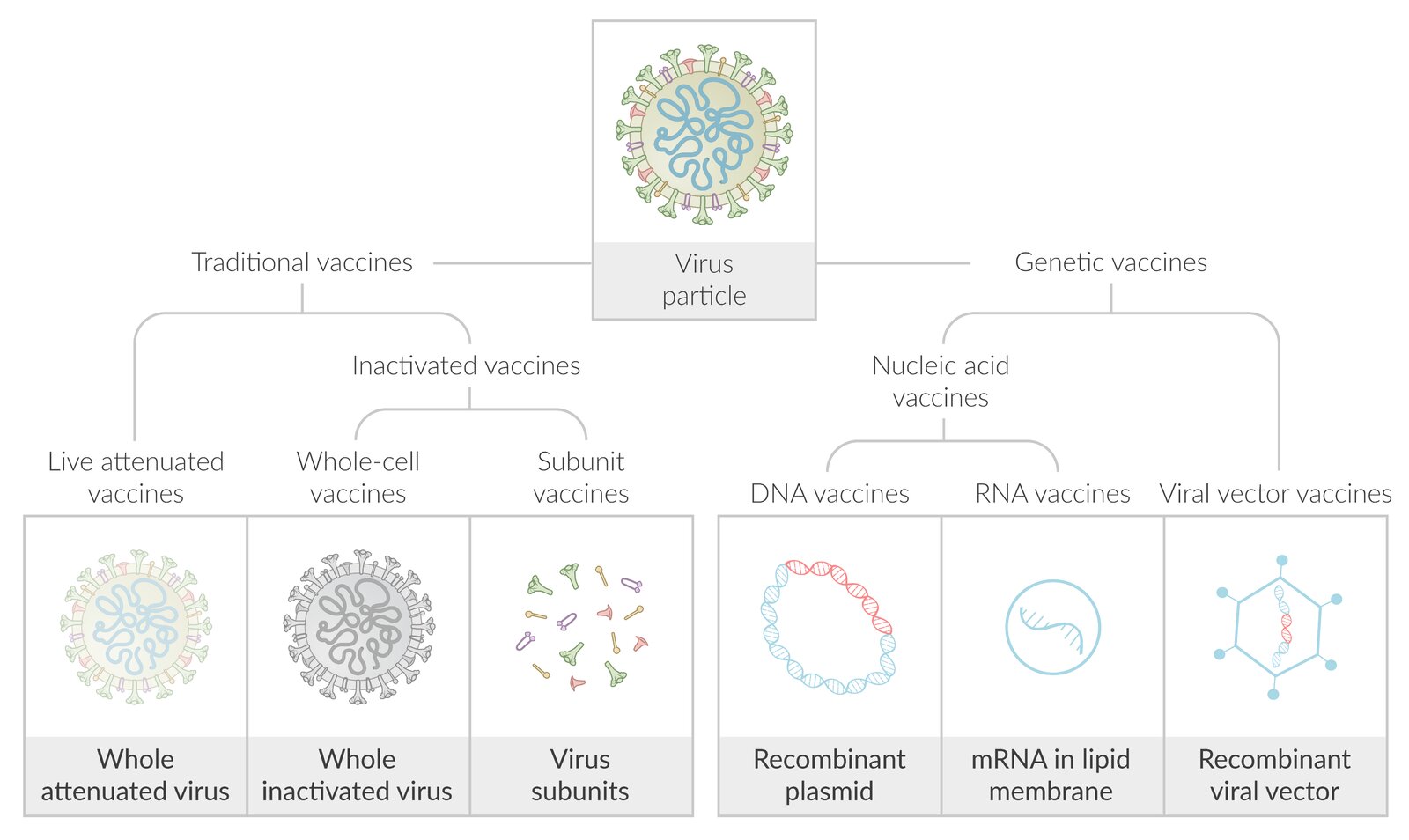
This diagram illustrates vaccine types based on the example of antiviral vaccines.
Traditional vaccines are either live attenuated or inactivated. Live attenuated vaccines contain modified whole virus particles capable of replication, but not of causing disease. Inactivated vaccines contain either the whole inactivated virus particles or their subunits.
Gene-based vaccines contain only the genetic information of the pathogen. This information, which is transmitted either directly in the form of nucleic acid (DNA in a recombinant plasmid or mRNA in a lipid envelope) or by means of a recombinant viral vector, induces endogenous antigen production in the host cells.
© AMBOSS
Live attenuated vaccines
- Definition: Modified functioning virus or bacterium that can replicate in the patient's body but does not cause disease.
-
Mechanism of action
- Similar to an infection with a “wild” pathogen and induces a cellular and humoral immune response.
- Specific B-cells against an antigen are formed, which induces a potent, lifelong immune response
-
Administration
- Oral vaccine or subcutaneous/intramuscular injection in children > 12 months
- Not indicated in children < 9 months; (the rotavirus vaccine is an exception, which is first given at 6 weeks of age)
- Second dose usually recommended to “catch” nonresponders (not as a boost)
- Multiple live vaccines can be given simultaneously, but if given at different times they should be at least 4 weeks apart to avoid possible interference.
- May be administered simultaneously with inactivated vaccines
-
Available vaccines
- MMR: prevents measles, mumps and rubella infections
- Varicella: against varicella-zoster virus (VZV)
- Zoster: prevents reactivation of latent VZV (i.e., shingles)
- Yellow fever
- Rotavirus
- Influenza (intranasal)
- Smallpox
- Adenovirus
- Oral polio, Sabin (no longer available in the US)
- BCG
- Typhoid (oral, Ty21a)
-
Special considerations
- Very rarely, live attenuated vaccines may become virulent again and are thus often contraindicated in immunodeficient individuals and pregnant women .
- HIV-positive individuals can be vaccinated with live attenuated vaccines (e.g., MMR and varicella) if their CD4 cell count is ≥ 200/mm3.
- Adenovirus vaccine is given in its nonattenuated form to military recruits.
“TYler And Paul Burnt their INFamous ROasted YELLOW-RUBy CHICKEN MEAt Very MUch”: TYphoid, Adenovirus, Polio, BCG, INFluenza, ROtavirus, YELLOW fever, RUBella, CHICKENpox, MEAsles, Varicella, and MUmps are live attenuated vaccines.
 and subcutaneous (SC) injection")
References:[7][8]
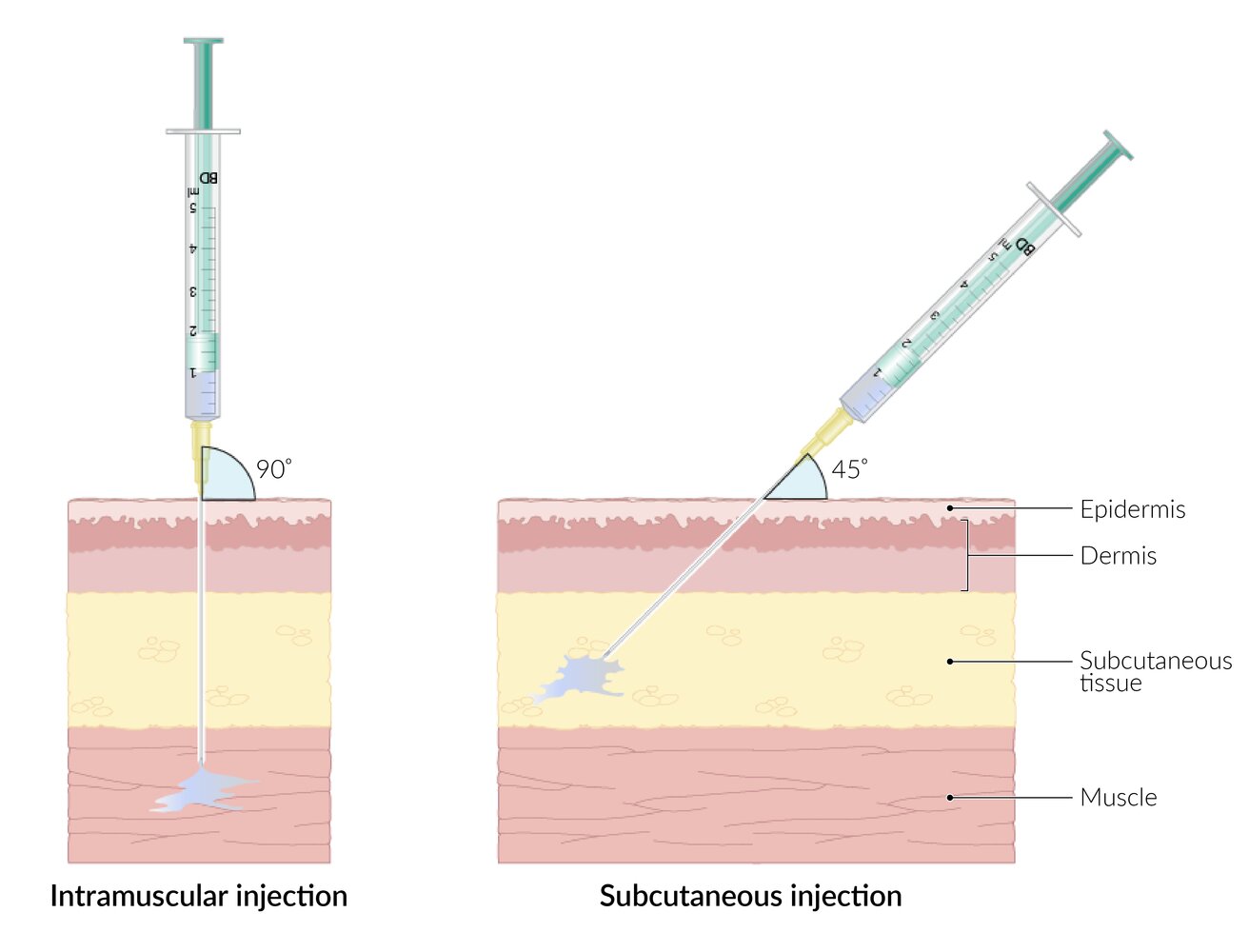
For IM injection, the needle is inserted at 90° to the skin to ensure the medication is delivered directly into muscle tissue. Muscles commonly used include the deltoid and vastus lateralis.
For SC injection, the needle is inserted at a 45° angle to deliver the medication into the subcutaneous tissue. Sites for injection should have sufficient subcutaneous tissue and no bony prominences, major nerves, or large blood vessels, e.g., the dorsal upper arm.
Choice of technique depends on the medication to be administered and the desired speed of effect: muscle tissue has greater vascularization than subcutaneous tissue; therefore, medications usually act more quickly if given IM rather than SC.
© AMBOSS
Inactivated vaccines
| Overview of inactivated vaccines | ||||
|---|---|---|---|---|
| Whole vaccines | Subunit vaccines | |||
| Protein-based | Polysaccharide-based | |||
| Characteristics |
|
|
|
|
| Available vaccines |
|
|
|
|
| Mechanism of action |
|
|
||
| Special considerations |
|
|
||
| Administration |
|
|||
“Beware of Hepatitis A on your TRIP:” Hepatitis A, Typhoid fever, Rabies, Influenza, and Poliomyelitis.
References:[9][10]
Viral vector vaccines
- Definition: an unrelated virus (e.g., adenovirus, vesicular stomatitis virus, influenza virus) is modified to be used as a nonpathogenic vector that delivers genetic code to cells containing instructions for the production of the desired antigen. [11]
-
Mechanism of action
- There are two types of viral vector vaccines: replicating and nonreplicating
- Nonreplicating vector vaccines: enter the cells and induce the production of vaccine antigens, but cannot produce new viral particles
- Replicating vector vaccines
- Enter the cells, inducing the production of new viral particles
- New viral particles go on to infect other host cells, leading to the production of further viral and vaccine antigens
- Induce both humoral and cellular immune responses
- There are two types of viral vector vaccines: replicating and nonreplicating
- Administration: usually injected intramuscularly, but can also be administered intranasally, intradermally, and orally
-
Available vaccines
- Ebola virus vaccine (rVSV-ZEBOV; Ervebo)
- COVID-19 vaccine (Janssen COVID-19 vaccine, Vaxzevria, Sputnik V vaccine)
-
Special considerations
- Preexisting immunity to the virus that serves as the vector may affect the effectiveness of a vaccine. [12]
- Less strict storage and handling conditions than nucleic acid vaccines
- Viral vectors are genetically stable and lack a viral genome and nonstructural proteins. Therefore, they do not interact or integrate into the host's DNA and are nonpathogenic.

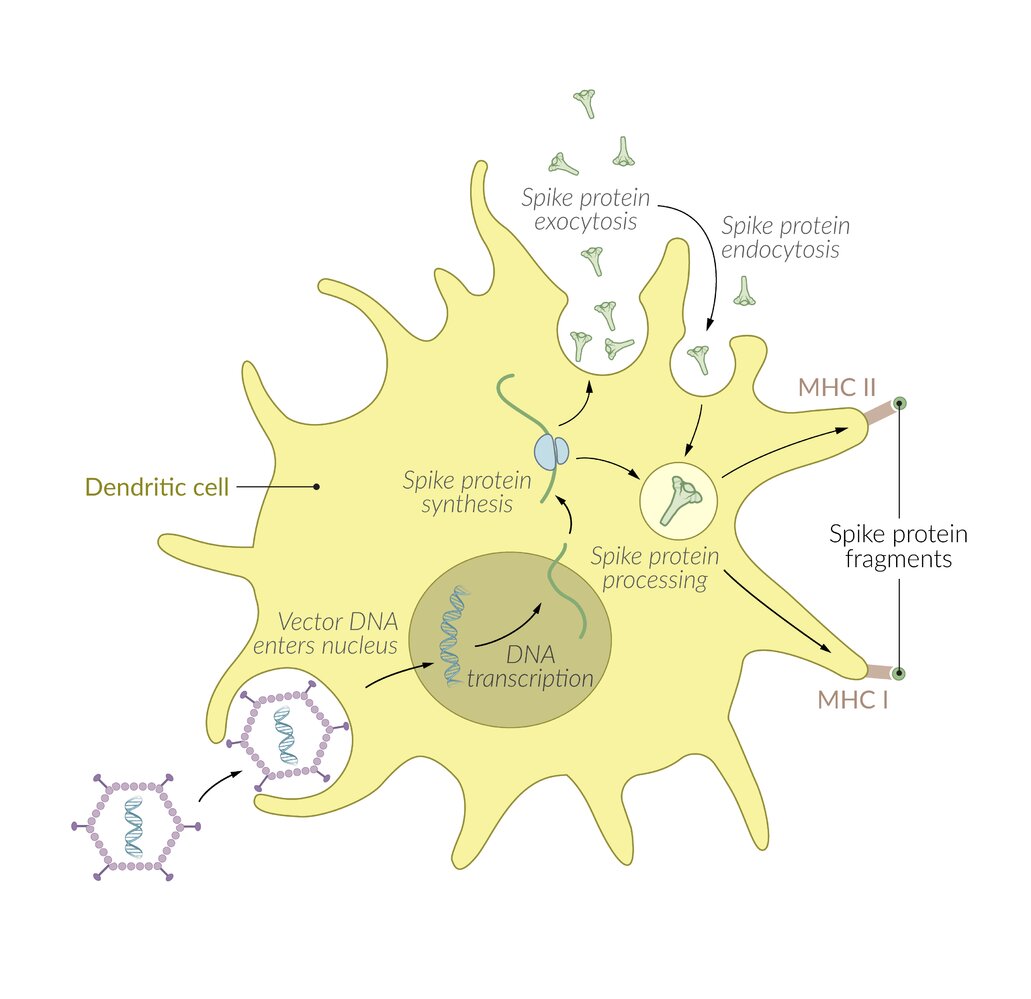
The vector-based COVID-19 vaccines are based on various recombinant adenoviruses (e.g., the chimpanzee adenovirus in AZD1222 by AstraZeneca, or the human adenovirus type 26 in Ad26.COV2.S by Janssen).
The recombinant DNA of the vector virus codes for the spike protein of SARS-CoV-2, which is synthesized by the host cell. The spike protein is then either processed and presented via MHC-I molecules or exocytosed. Exocytosed spike proteins are taken up by phagocytes (esp. dendritic cells in muscle) and presented via MHC-II molecules. Presentation of the spike protein fragments via MHC-I and MHC-II leads to the development of a specific immune response against the spike protein.
© AMBOSS
Nucleic acid vaccines
RNA vaccines [13][14]
- Definition: a vaccine based on mRNA that delivers genetic code containing instructions for the production of the desired antigen to cells
-
Mechanism of action
- Two types of mRNA vaccines: nonreplicating and self-amplifying
- Nonreplicating mRNA vaccines: contain the sequence of the desired antigen and the 5′ and 3′ untranslated regions
- Self-amplifying mRNA vaccines: contain the sequence of the desired antigen and the viral replication machinery (e.g., RNA polymerase) that enables intracellular RNA amplification
- Both types induce humoral as well as cellular immune responses.
- Two types of mRNA vaccines: nonreplicating and self-amplifying
-
Administration
- Injected intramuscularly or intradermally
- Require multiple doses
- Available vaccines: COVID-19 vaccines (e.g., Comirnaty, Spikevax) contain modified mRNA embedded in lipid nanoparticles that encodes for the spike protein mRNA sequence of SARS-CoV-2
-
Special considerations
- mRNA is a nonintegrating platform that is degraded by normal cellular processes. Due to its transitory nature, mRNA does not interact or integrate into the DNA and bears no risk of insertional mutagenesis. (e.g., COVID-19 vaccines are safe to use during pregnancy)
- There is no potential risk of infection as mRNA is nonpathogenic.
- Require strict cold-chain
- Different techniques can be used to deliver the vaccine (e.g., injection of naked mRNA or encapsulated within nanoparticles or polyplex)

DNA vaccines [15]
- Definition: A specific antigen-coding DNA sequence is introduced using a genetically engineered plasmid to induce endogenous antigen production in the host.
-
Mechanism of action
- After entering the cells, the vaccine antigen is expressed from the DNA construct.
- Induce both humoral and cellular immune responses
-
Administration
- Intramuscularly or intradermally
- Require multiple doses
- Available vaccines: No DNA vaccines have been approved for human use in the United States.
-
Special considerations
- Potential advantages observed in animal models are improved vaccine stability and the use of nonpathogenic agents.
- In order to properly deliver the vaccine and ensure cellular uptake, injection needs to be followed by electroporation.
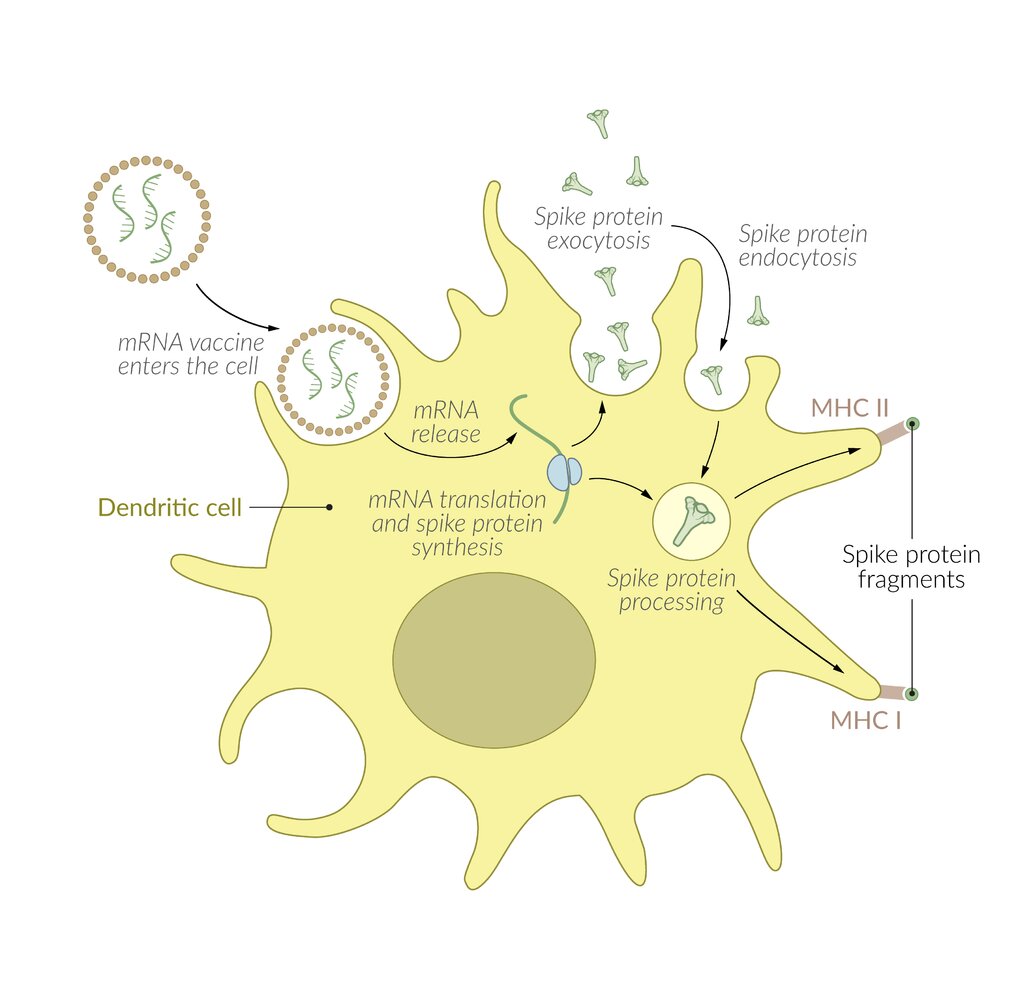
The mRNA-based COVID-19 vaccines contain mRNA coding for the spike protein of the SARS-CoV-2 virus. To increase stability and enhance uptake into cells, the mRNA strands are encapsulated in lipid nanoparticles.
Within the cell, the mRNA causes transient, local expression of the spike protein, which is then either processed and presented via MHC-I molecules or exocytosed. Exocytosed spike proteins are taken up by phagocytes (especially dendritic cells in the muscle) and presented via MHC-II molecules. Presentation of the spike protein fragments via MHC-I and MHC-II leads to the development of a specific immune response against the spike protein.
© AMBOSS
Vaccine administration


© AMBOSS
For IM injection, the needle is inserted at 90° to the skin to ensure the medication is delivered directly into muscle tissue. Muscles commonly used include the deltoid and vastus lateralis.
For SC injection, the needle is inserted at a 45° angle to deliver the medication into the subcutaneous tissue. Sites for injection should have sufficient subcutaneous tissue and no bony prominences, major nerves, or large blood vessels, e.g., the dorsal upper arm.
Choice of technique depends on the medication to be administered and the desired speed of effect: muscle tissue has greater vascularization than subcutaneous tissue; therefore, medications usually act more quickly if given IM rather than SC.
© AMBOSS
Adverse effects of vaccination
Common adverse effects [16][17][18]
- Affects ∼ 1/3
- Usually begin within the first 48–72 hours after administration and last 1–2 days
- Symptoms
- Local swelling, redness, and pain at the injection site
- Low-grade fever (postvaccination fever)
- Headaches
- Fatigue
- Flu-like symptoms
- Live attenuated vaccine: can cause mild form of the disease, usually appearing within 1–3 weeks of administration :usually caused by replication of the attenuated vaccine strain
Rare adverse effects [16][17][18]
-
Cardiovascular complications: observed in young men who received mRNA vaccines (COVID-19 vaccines) [19]
- Pericarditis
- Myocarditis
- Myocardial ischemia
- Serious allergic reaction (generally < 1 per million doses)
- Live attenuated vaccine: attenuated course of the disease following immunization (e.g., vaccine-related measles)
- Vaccine injury (∼ 1/1,000,000): permanent injury from a vaccination or a vaccine-related complication (e.g., encephalopathy, seizures, brachial neuritis)
There is no link between autism and vaccines or their ingredients. [20][21]
Contraindications for vaccination
Precautions
-
General precautions
- A precaution is a condition in the recipient that might increase the risk for serious adverse reactions or interfere with a vaccine's ability to produce immunity.
- Generally, vaccination should be deferred when a precaution is present, except when the benefits of protection outweigh the risks.
- Acute moderate or severe illness (with or without fever)
-
Special precautions
- Rotavirus vaccine: uncorrected GI tract malformation (e.g., Meckel's diverticulum)
- Egg protein-containing vaccines: allergic reactions other than urticaria (e.g., angioedema, bronchospasm) to egg products
- Pertussis vaccine: progressive or unstable neurologic disorders (e.g., uncontrolled epilepsy, infantile spasms, progressive encephalopathy) [22]
-
Tetanus toxoid-containing vaccines
- Development of Guillain-Barré syndrome within 6 weeks of a previous dose
- Arthus reaction after a previous dose [22]
Contraindications [23]
-
General contraindications
- Vaccines are generally contraindicated in recipients with conditions that increase the risk for severe vaccine reactions or in whom the vaccine may exacerbate the condition.
- Previous severe adverse reactions (e.g., anaphylaxis)
- Severe adverse reactions to a vaccine component (e.g., egg protein in yellow fever vaccine, yeast in hepatitis B vaccine)
-
Contraindications to live vaccines
-
Rotavirus vaccine
- Severe combined immunodeficiency (SCID)
- History of intussusception [24]
- Pertussis vaccines: risk of encephalopathy (e.g., prolonged seizures, decreased level of consciousness, coma) within 7 days following a previous dose
-
Live, attenuated virus vaccinations [22]
- Pregnant individuals
- Immunodeficient individuals (e.g., individuals receiving chemotherapy or long-term immunosuppressive therapy, individuals with congenital immunodeficiencies, patients with HIV and severe immunocompromise)
- Individuals receiving IVIG therapy (e.g., for Kawasaki disease)
-
Rotavirus vaccine
-
False contraindications [25][26]
- Fever within 48 hours
- Current or recent mild illness (e.g., rhinorrhea, otitis media, mild diarrhea)
- Current or recent antibiotic therapy (exception is oral live typhoid vaccine )
- Current or recent low-dose and/or short-term steroid use (i.e., < 2 mg/kg/day or < 20 mg/day, < 14 days)
- Previous mild or moderate localized cutaneous reaction (e.g., swelling, redness, soreness) following any vaccination
-
Preterm infants
- Should be immunized according to chronological age, not gestational age
- The exception is the hepatitis B vaccine: vaccination should be delayed by a month or until hospital discharge for infants weighing < 2 kg born to HBsAg-negative mothers.
- Adjustment according to weight: no dose adjustment is needed
All children should be immunized with the standard doses of vaccines according to their chronological age; doses should not be adjusted to weight or height.
Special patient groups
Immunizations during pregnancy, vaccinations in preterm infants, and vaccinations in individuals with HIV are detailed in the “Immunization schedule” article.
Pathogens affecting unvaccinated children
| Pathogens affecting unvaccinated and underimmunized individuals | |||||
|---|---|---|---|---|---|
| Disease | Clinical features | Treatment | |||
| Measles virus |
|
|
|
||
| Rubella virus |
|
|
|
||
| Varicella zoster virus |
|
|
|
||
| Mumps virus |
|
|
|
||
| Corynebacterium diphtheriae |
|
|
|
||
| Haemophilus influenzae type b |
|
|
|
||
|
|
|
|
||
| Streptococcus pneumoniae |
|
||||
| Neisseria meningitidis |
|
||||
| Poliovirus |
|
|
|
||
| Clostridium tetani |
|
|
|
||
| Bordetella pertussis |
|
|
|
||
| Hepatitis A virus |
|
|
|
||
| Hepatitis B virus |
|
||||
Vaccine hesitancy
Overview [27][28]
- Vaccine hesitancy is a state of feeling ambivalent about or resistant to receiving vaccinations.
-
Vaccine hesitancy may lead to:
- Delay of vaccinations
- Cautious acceptance of vaccinations
- Refusal of some or all vaccinations
- Individuals may express vaccine hesitancy for themselves and/or their children.
Approach [27][29][30]
Follow the key principles of communication and counseling with all patients.
- Presume individuals have no vaccine hesitancy, and make a strong recommendation for vaccination.
- If the individual declines, inquire sensitively about and address vaccine-related concerns.
-
If the individual continues to express hesitancy:
- Use motivational interviewing techniques to facilitate further discussion.
- Continue to definitively recommend adherence to the standard immunization schedule.
- Consider sharing personal or family experience with vaccines.
- If the individual refuses vaccination:
- Affirm their autonomy.
- Document the individual's decision. [31]
- Continue to build trust over time and revisit the conversation at a later date.
- Consider dismissal of the patient from the practice only after careful consideration of implications for patient's health and care. [27]
Vaccine hesitancy is a complex issue with no single effective solution. Engage with the individual regarding their concerns and social and cultural context. [32]
Discuss vaccines with the use of evidence-based information, e.g., vaccine information statements for individual vaccines, and leaflets and infographics provided by the American Academy of Pediatrics and CDC. See “Tips and links.”
Vaccine-related concerns [27][33][34]
| Addressing patient concerns about vaccination [27][33][34] | ||
|---|---|---|
| Concern | Patient counseling topics and strategies | |
| Simultaneous vaccination [35] |
|
|
| Safety of vaccine components [36][37] |
|
|
| Adverse effects of vaccination |
|
|
| Fear and pain of needles [27][43] |
|
|
| Autism |
|
|
| Natural immunity is preferable to vaccination |
|
|
| Vaccine efficacy |
|
|
| Getting illness from vaccines |
|
|
Unapproved delayed or alternate immunization schedules put individuals at risk for vaccine-preventable conditions and complications. [27]
Refusal of vaccines may lead to exclusion from school. Check with local state and health departments. [50]

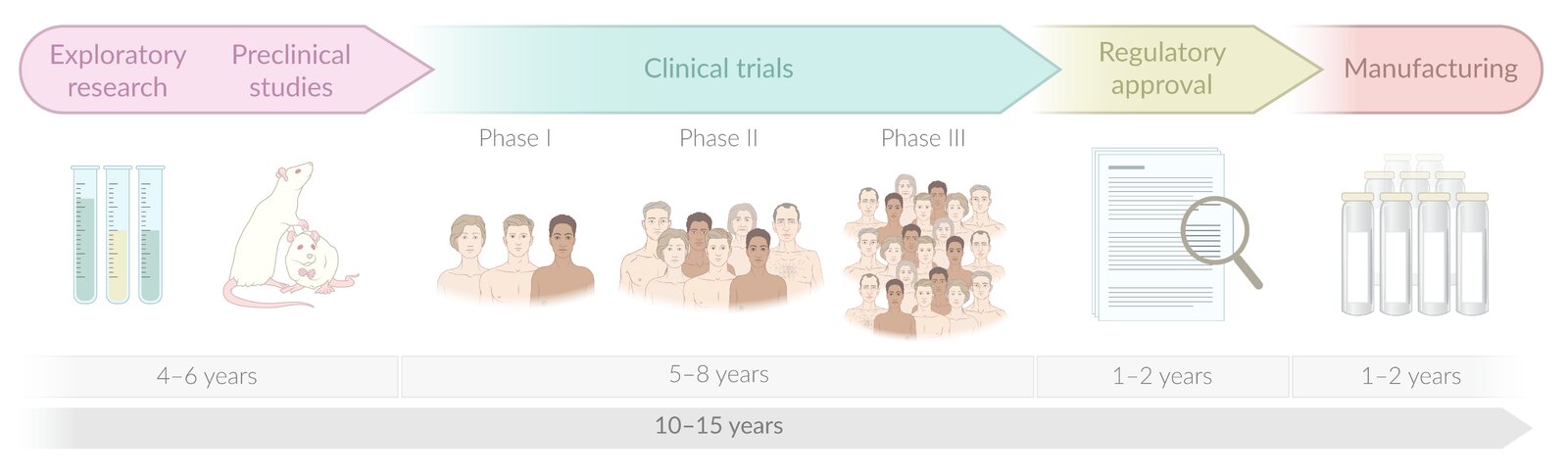
In standard vaccine development, individual study phases (exploratory, preclinical, and clinical phases) are performed sequentially. The application for regulatory approval (in the US to the FDA) is submitted on the basis of the complete study data after the clinical trials are finished. Manufacturing begins only once approval has been granted.
© AMBOSS
Related One-Minute Telegram
- One-Minute Telegram 128-2025-1/3: No observed link between aluminum-adsorbed vaccines and chronic childhood diseases
- One-Minute Telegram 119-2025-1/3: Want to increase vaccination rates? Talk to your patients!
- One-Minute Telegram 9-2020-1/3: SARS-CoV-2 vaccine candidate shows promising results in phase 1–2 trial
Interested in the newest medical research, distilled down to just one minute? Sign up for the One-Minute Telegram in “Tips and links” below.
External Resources
References
- Van Riel D, de Wit E. "Next-generation vaccine platforms for COVID-19". Nat Mater. 19(8). :810-812. (2020)
- Barrett JR, Belij-Rammerstorfer S, Dold C, et al. "Phase 1/2 trial of SARS-CoV-2 vaccine ChAdOx1 nCoV-19 with a booster dose induces multifunctional antibody responses". Nat Med. 27(2). :279-288. (2020)
- "Possible Side-Effects from Vaccines". https://web.archive.org/web/20240702114104/https://www.cdc.gov/vaccines/vac-gen/side-effects.htm. [2016-12-02]
- "Information Sheet: Observed Rate of Vaccine Reactions: Measles, Mumps and Rubella Vaccines"
- Offit PA, Bell LM. "Vaccines". John Wiley & Sons. (2003). ISBN: 9780471420040
- Fazlollahi A, Zahmatyar M, Noori M, et al. "Cardiac complications following mRNA COVID‐19 vaccines: A systematic review of case reports and case series". Rev Med Virol. (2021)
- Hviid A, Hansen JV, Frisch M, Melbye M. "Measles, Mumps, Rubella Vaccination and Autism". Ann Intern Med. 170(8). :513. (2019)
- "Vaccines Do Not Cause Autism". https://web.archive.org/web/20240701171841/https://www.cdc.gov/vaccinesafety/concerns/autism.html. [2015-11-23]
- "Epidemiology and Prevention of Vaccine-Preventable Diseases - Pertussis". https://web.archive.org/web/20170311032559/https://www.cdc.gov/vaccines/pubs/pinkbook/pert.html#contraindications. [2015-09-29]
- "Vaccine Recommendations and Guidelines of the ACIP - Contraindications and Precautions". https://web.archive.org/web/20170913010854/https://www.cdc.gov/vaccines/hcp/acip-recs/general-recs/contraindications.html. [2017-01-30]
- "Rotavirus". https://web.archive.org/web/20200806205921/https://www.cdc.gov/vaccines/pubs/pinkbook/rota.html. [2016-11-15]
- Opri R, Zanoni G, Caffarelli C, et al. "True and false contraindications to vaccines". Allergol Immunopathol (Madr). 46(1). :99-104. (2018)
- "WHO - VACCINE SAFETY AND FALSE CONTRAINDICATIONS TO VACCINATION". https://www.euro.who.int/__data/assets/pdf_file/0009/351927/WHO-Vaccine-Manual.pdf. [2017-01-01]
- Leentvaar-Kuijpers A, Coutinho RA, Brulein V, Safary A. "Simultaneous passive and active immunization against hepatitis A". Vaccine. 10. :S138-S141. (1992)
- "ACIP Vaccine Recommendations and Guidelines Timing and Spacing of Immunobiologics General Best Practice Guidelines for Immunization". https://web.archive.org/web/20230426141911/https://www.cdc.gov/vaccines/hcp/acip-recs/general-recs/timing.html. [2023-04-07]
- AAP Committee on Infectious Diseases. "Red Book: 2021–2024 Report of the Committee on Infectious Diseases". American Academy of Pediatrics. (2021). ISBN: 9781610025218
- "Polio Elimination in the United States". https://web.archive.org/web/20210326071449/https://www.cdc.gov/polio/what-is-polio/polio-us.html. [2019-10-25]
- "CDC - Haemophilus Influenzae Type b (Hib) VIS". https://web.archive.org/web/20210416213403/https://www.cdc.gov/vaccines/hcp/vis/vis-statements/hib.html. [2019-10-29]
- "Vaccine Basics". https://web.archive.org/web/20240725155429/https://www.hhs.gov/immunization/basics/index.html. [2017-03-23]
- Songul Yalcin S, Engur Karasimav D, Yurdakok K. "Measles vaccine failure in 9-month-old infants". Çocuk Enfeksiyon Dergisi/Journal of Pediatric Infection. 9(4). :153-160. (2016)
- Baicus A. "History of polio vaccination". World J Virol. 1(4). :108. (2012)
- "Neonatal Immunology". https://www.immunology.org/public-information/bitesized-immunology/immune-development/neonatal-immunology. [2018-01-01]
- Foged C, Rades T, Perrie Y, Hook S. "Subunit Vaccine Delivery". Springer. (2014). ISBN: 9781493914173
- Park KS, Sun X, Aikins ME, Moon JJ. "Non-viral COVID-19 vaccine delivery systems". Adv Drug Deliv Rev. 169. :137-151. (2021)
- Pardi N, Hogan MJ, Porter FW, Weissman D. "mRNA vaccines — a new era in vaccinology". Nature Reviews Drug Discovery. 17(4). :261-279. (2018)
- "DNA vaccines". https://www.who.int/teams/health-product-policy-and-standards/standards-and-specifications/vaccines-quality/dna. [2021-01-01]
- O’Leary ST, Opel DJ, Cataldi JR, et al. "Strategies for Improving Vaccine Communication and Uptake". Pediatrics. 153(3). (2024)
- MacDonald NE. "Vaccine hesitancy: Definition, scope and determinants". Vaccine. 33(34). :4161-4164. (2015)
- Loehr J, Savoy M. "Strategies for Addressing and Overcoming Vaccine Hesitancy". Am Fam Physician. 94(2). :94-6. (2016)
- "CDC: Talking with Parents about Vaccines for Infants". https://web.archive.org/web/20240109151947/https://www.cdc.gov/vaccines/hcp/conversations/preparing-for-parent-vaccine-questions.html. [2018-04-11]
- "Documenting Parental Refusal to Have Their Children Vaccinated: American Academy of Pediatrics"
- Jarrett C, Wilson R, O'Leary M, et al. "Strategies for addressing vaccine hesitancy - A systematic review". Vaccine. 33(34). :4180-90. (2015)
- Miller E, Wodi AP. "Epidemiology and Prevention of Vaccine-Preventable Diseases". Centers for Disease Control and Prevention. (2021). ISBN: 0017066115
- "Preparing for Questions Parents May Ask about Vaccines". https://web.archive.org/web/20240524200658/https://www.cdc.gov/vaccines/hcp/conversations/preparing-for-parent-vaccine-questions.html. [2018-04-11]
- "Multiple Vaccinations at Once". https://web.archive.org/web/20240102110045/https://www.cdc.gov/vaccinesafety/concerns/multiple-vaccines-immunity.html. [2020-08-14]
- "CDC Appendix B for the Pink Book: Vaccine excipient summary". https://web.archive.org/web/20240404105018/https://www.cdc.gov/vaccines/pubs/pinkbook/downloads/appendices/b/excipient-table-2.pdf. [2021-11-11]
- "Common Ingredients in U.S. Licensed Vaccines". https://web.archive.org/web/20240524194236/https://www.fda.gov/vaccines-blood-biologics/safety-availability-biologics/common-ingredients-fda-approved-vaccines. [2019-04-04]
- "Thimerosal and Vaccines". https://www.fda.gov/vaccines-blood-biologics/safety-availability-biologics/thimerosal-and-vaccines. [2018-02-01]
- "Manual for the Surveillance of Vaccine-Preventable Diseases; Chapter 21: Surveillance for Adverse Events Following Immunization Using the Vaccine Adverse Event Reporting System (VAERS)". https://web.archive.org/web/20240403145034/https://www.cdc.gov/vaccines/pubs/surv-manual/chpt21-surv-adverse-events.html. [2024-02-22]
- "CDC: How Vaccines are Developed and Approved for Use". https://web.archive.org/web/20240403144659/https://www.cdc.gov/vaccines/basics/test-approve.html. [2023-03-30]
- "Fainting (Syncope) after Vaccination". https://web.archive.org/web/20240524201154/https://www.cdc.gov/vaccinesafety/concerns/fainting.html. [2020-08-25]
- Klein NP, Fireman B, Yih WK, et al. "Measles-Mumps-Rubella-Varicella Combination Vaccine and the Risk of Febrile Seizures". Pediatrics. 126(1). :e1-e8. (2010)
- Edwards KM, Hackell JM. "Countering Vaccine Hesitancy". Pediatrics. 138(3). (2016)
- Centers for Disease Control and Prevention. "Epidemiology and Prevention of Vaccine-Preventable Diseases". Public Health Foundation. (2021). ISBN: 9780990449119
- "CDC: Healthcare Providers/Professionals - Administer the Vaccine(s)". https://web.archive.org/web/20240527100339/https://www.cdc.gov/vaccines/hcp/admin/administer-vaccines.html. [2021-09-08]
- Davidson M. "Vaccination as a cause of autism-myths and controversies". Dialogues Clin Neurosci. 19(4). :403-407. (2017)
- Niewiesk S. "Maternal antibodies: clinical significance, mechanism of interference with immune responses, and possible vaccination strategies". Front Immunol. 5. :446. (2014)
- Phadke VK, Bednarczyk RA, Salmon DA, Omer SB. "Association Between Vaccine Refusal and Vaccine-Preventable Diseases in the United States: A Review of Measles and Pertussis". JAMA. 315(11). :1149-58. (2016)
- Roush SW. "Historical Comparisons of Morbidity and Mortality for Vaccine-Preventable Diseases in the United States". JAMA. 298(18). :2155. (2007)
- "School Vaccination Requirements and Exemptions". https://web.archive.org/web/20240311134643/https://www.cdc.gov/phlp/docs/school-vaccinations.pdf. [2017-10-12]
- "Epidemiology and Prevention of Vaccine-Preventable Diseases - Principles of Vaccination". https://web.archive.org/web/20180626235906/https://www.cdc.gov/vaccines/pubs/pinkbook/prinvac.html. [2016-11-15]