Summary
Valvular heart diseases (VHDs) comprise a group of conditions that affect the heart valves. Valvular defects are either acquired or congenital and manifest as stenosis and/or insufficiency (regurgitation) of the valves. Acquired defects, which are primarily found in the left heart, are the most common form of VHD and often occur secondary to infections (postinflammatory), degenerative processes, or underlying heart disease. The type of valvular disease determines the type of cardiac stress and subsequent symptoms. Valvular stenosis leads to a greater pressure load and concentric hypertrophy, while insufficiencies are characterized by volume overload and eccentric hypertrophy of the preceding heart cavities. Diagnostic procedures typically include ECGs, chest x-ray, and echocardiograms. Management consists of medical therapy for symptoms (e.g., due to heart failure) as well as interventional or surgical procedures to repair, reconstruct, or replace valves.
Epidemiology
-
Aortic stenosis
- Most common valve defect in industrialized countries
- Mostly degenerative
- Degenerative stenosis usually becomes symptomatic after the age of 75 and is most common in men.
- Aortic stenosis in young people is usually secondary to congenital defects (e.g., bicuspid aortic valve).
-
Aortic regurgitation
- Age of onset: 40–60 years
- Severity increases with age
- Mitral stenosis: symptom onset between 20 and 39 years [1]
-
Mitral regurgitation
- Overall prevalence of 0.6 to 2.4 %
- Second most common valve defect
- More common in women
- Tricuspid valve defects: occur in < 1% of the population
- Pulmonary valve defects: rare outside of congenital conditions
Epidemiological data refers to the US, unless otherwise specified.
Etiology
Valvular heart defects may either be acquired or congenital. Acquired defects are more common and typically occur secondary to infections (postinflammatory), degenerative processes, or heart disease.
| Etiology of valvular heart conditions [2][3] | |||
|---|---|---|---|
| Valve stenosis | Valve regurgitation | ||
| Left heart | Mitral valve |
|
|
| Aortic valve |
|
|
|
| Right heart | Tricuspid valve |
|
|
| Pulmonary valve |
|
|
|
Clinical features
All valvular defects can eventually lead to symptoms of heart failure as a result of excessive strain on the ventricles.
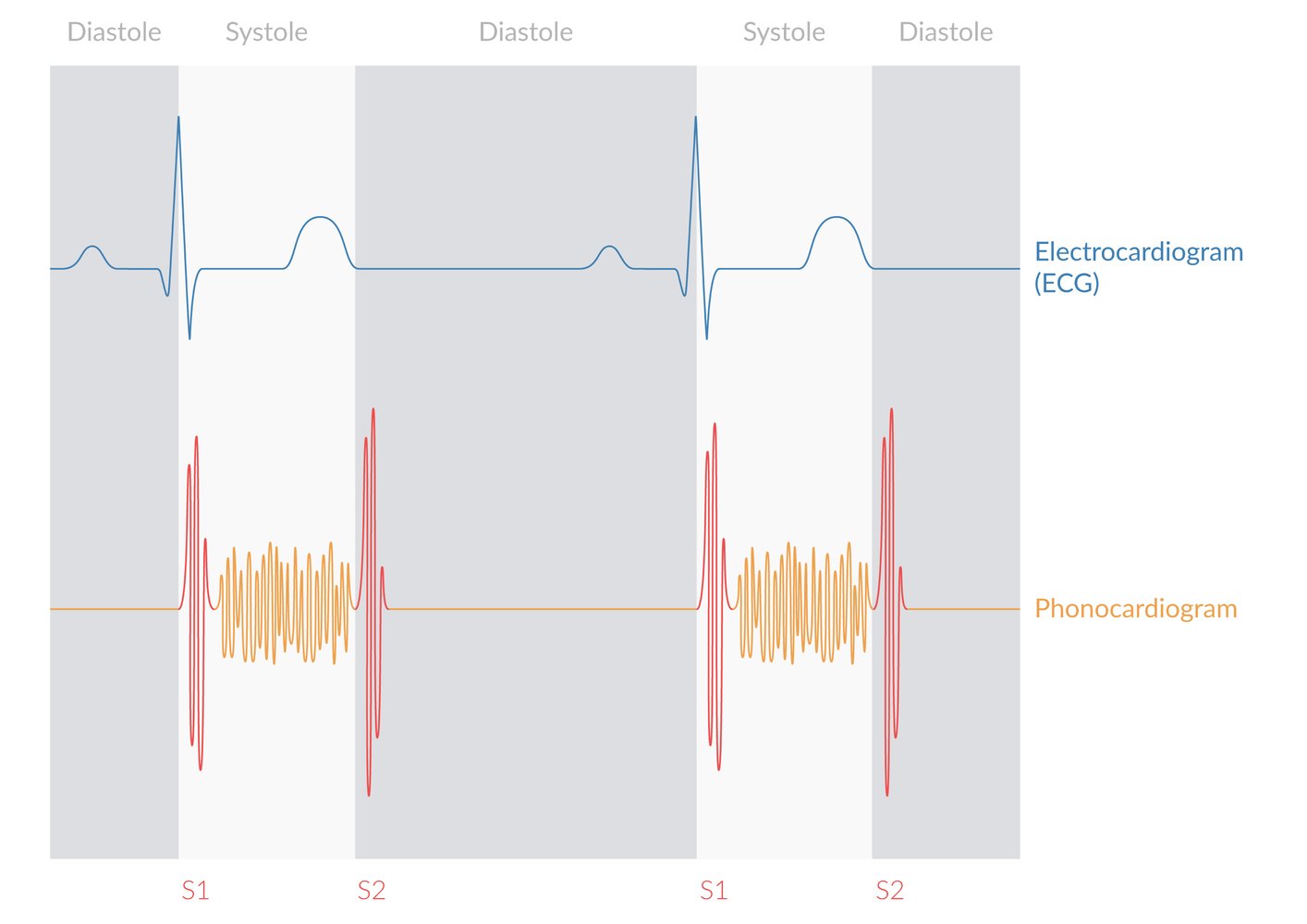
Physical examination
- Complete heart examination: see cardiovascular examination and auscultation of the heart for details.
| Auscultation in valvular defects | |||
|---|---|---|---|
| Maximum point | Murmur | Characteristics | |
| Aortic stenosis |
|
|
|
| Aortic regurgitation |
|
|
|
| Mitral stenosis |
|
|
|
| Mitral valve prolapse |
|
|
|
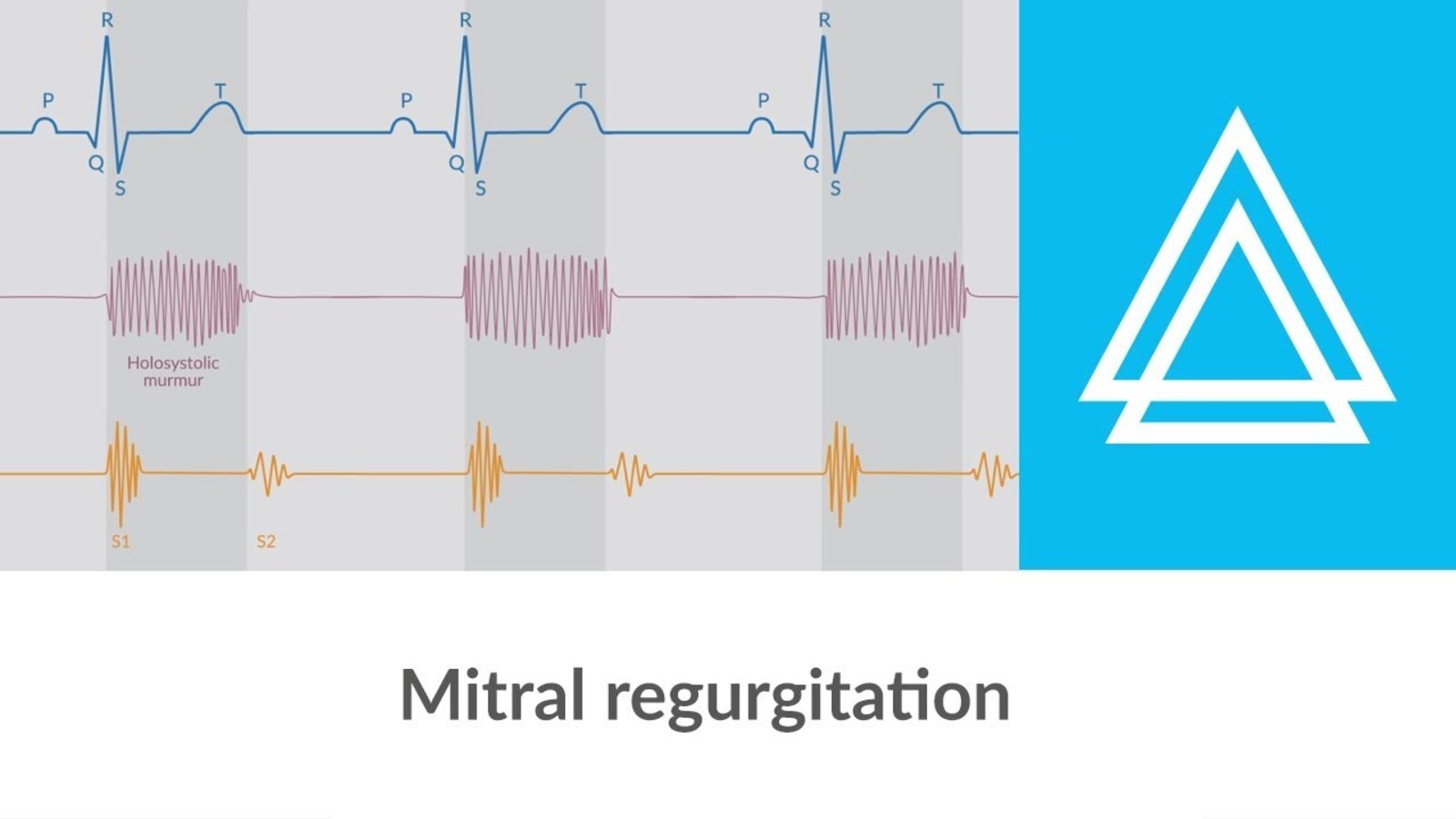
| Mitral regurgitation |
|
|
|
| Pulmonary stenosis |
|
|
|
| Pulmonary regurgitation |
|
|
|
| Tricuspid stenosis (extremely rare) |
|
|
|
| Tricuspid regurgitation |
|
|
|












References:[4][5]
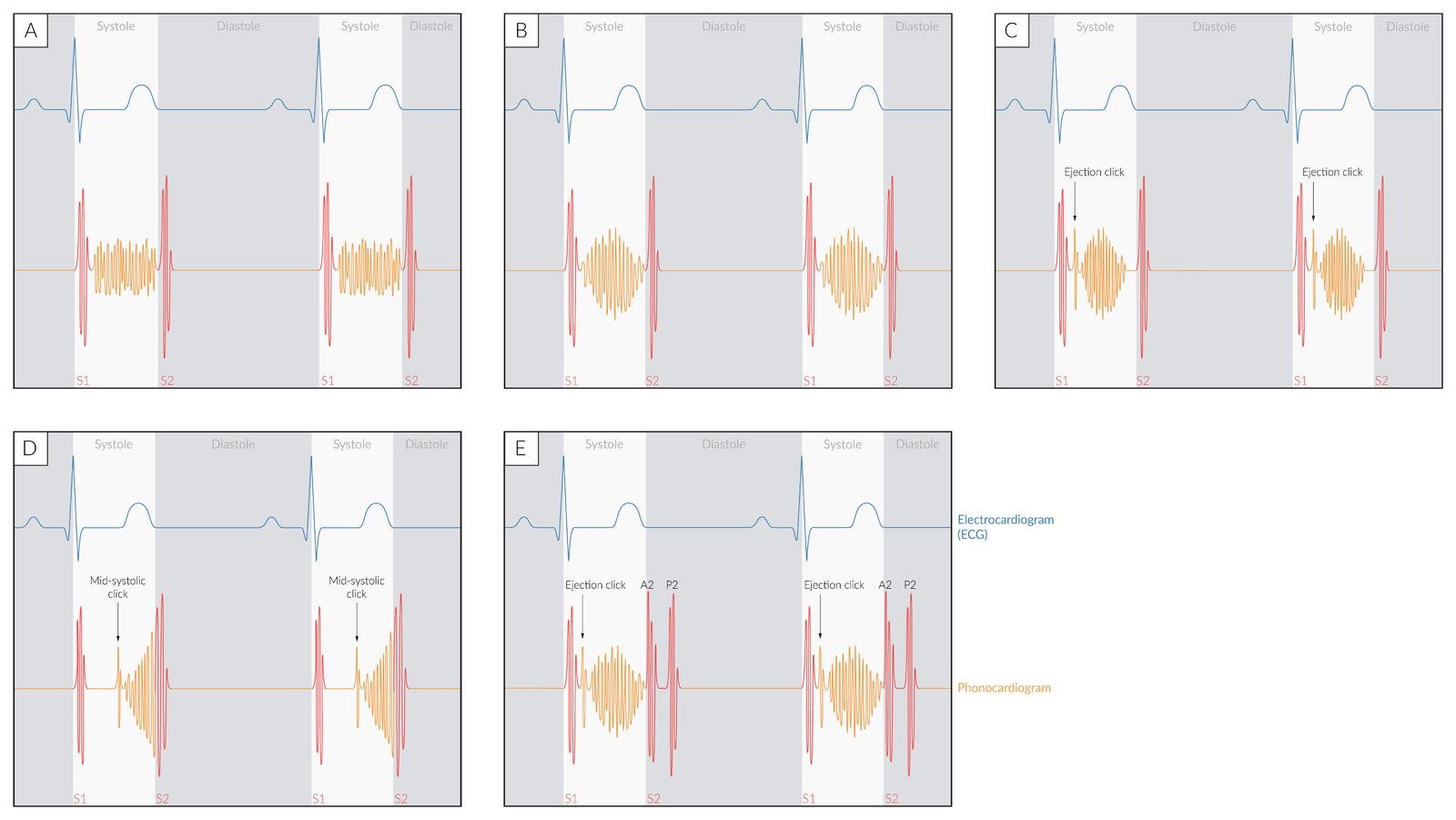
Systolic murmurs (orange waveform) occur in:
(A) Mitral/tricuspid regurgitation and/or ventricular septal defect (holosystolic murmur)
(B) Aortic/pulmonary stenosis (crescendo-decrescendo murmur)
(C) Aortic/pulmonary stenosis with an ejection click
(D) Mitral valve prolapse (midsystolic click followed by crescendo murmur)
(E) Pulmonary stenosis with a split second heart sound
© AMBOSS
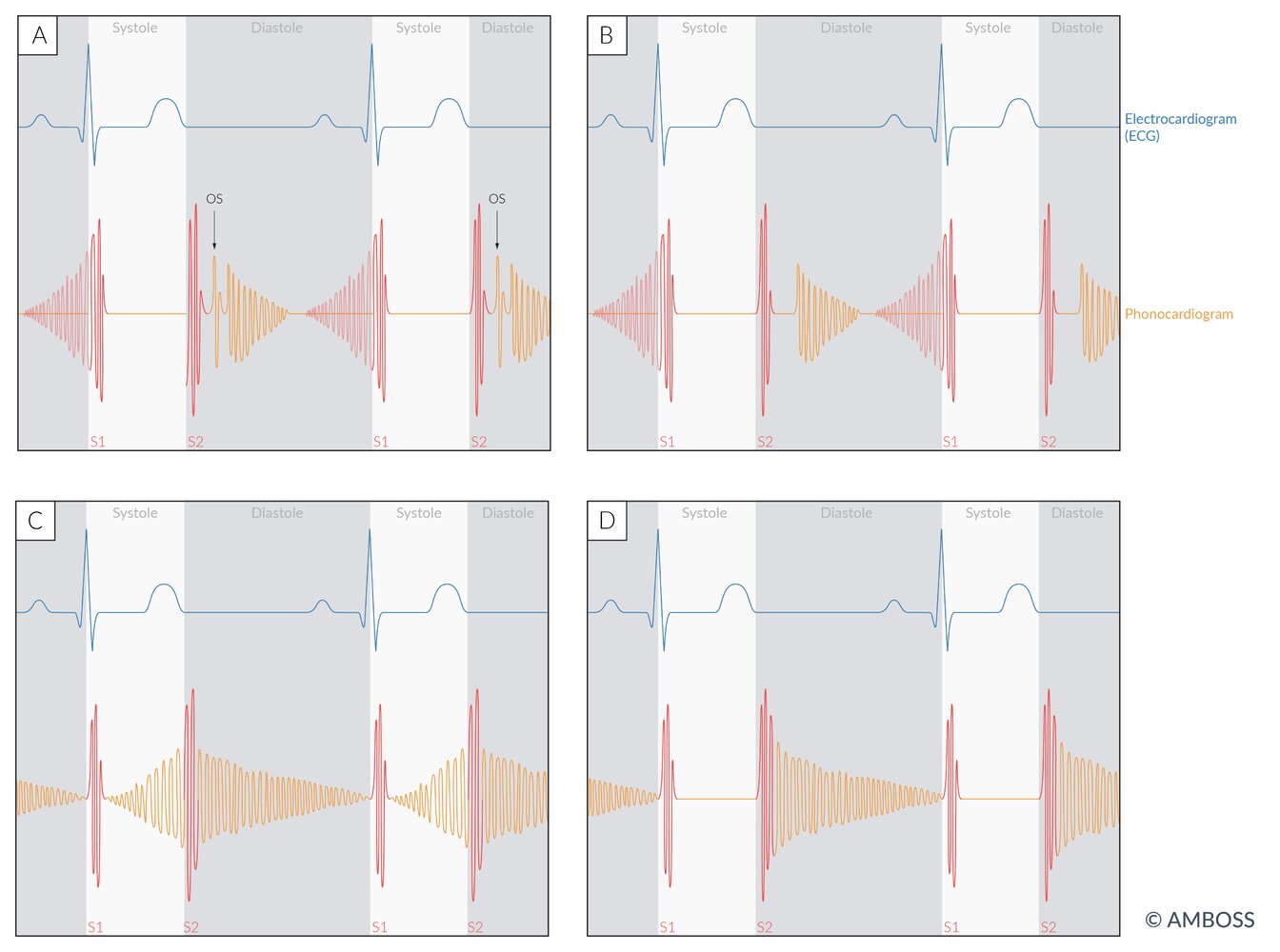
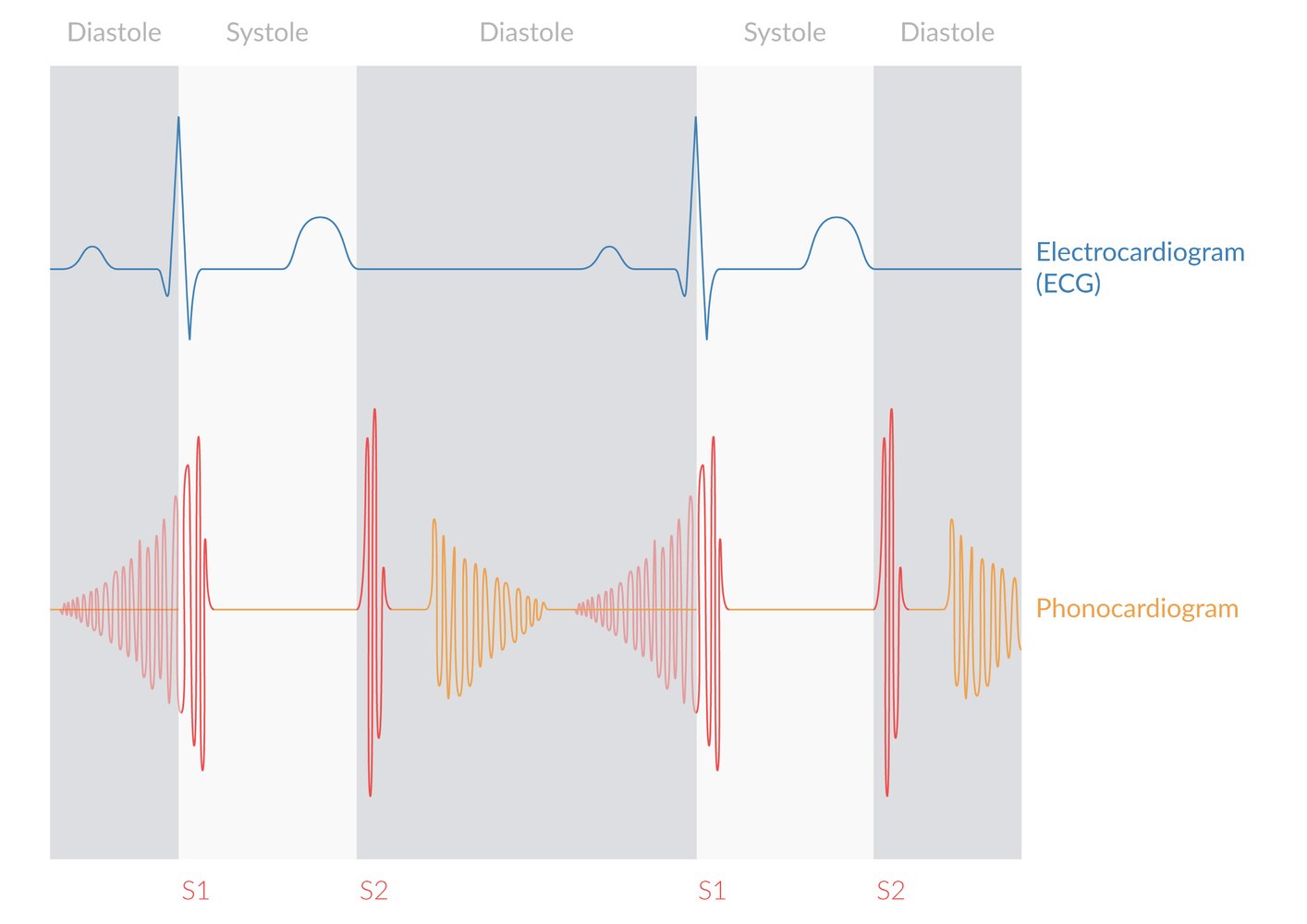
Diastolic murmurs (orange waveform) occur in:
(A) Mitral stenosis (decrescendo murmur with OS)
(B) Tricuspid stenosis (mid-diastolic decrescendo murmur)
(C) Patent ductus arteriosus (continuous crescendo-decrescendo murmur)
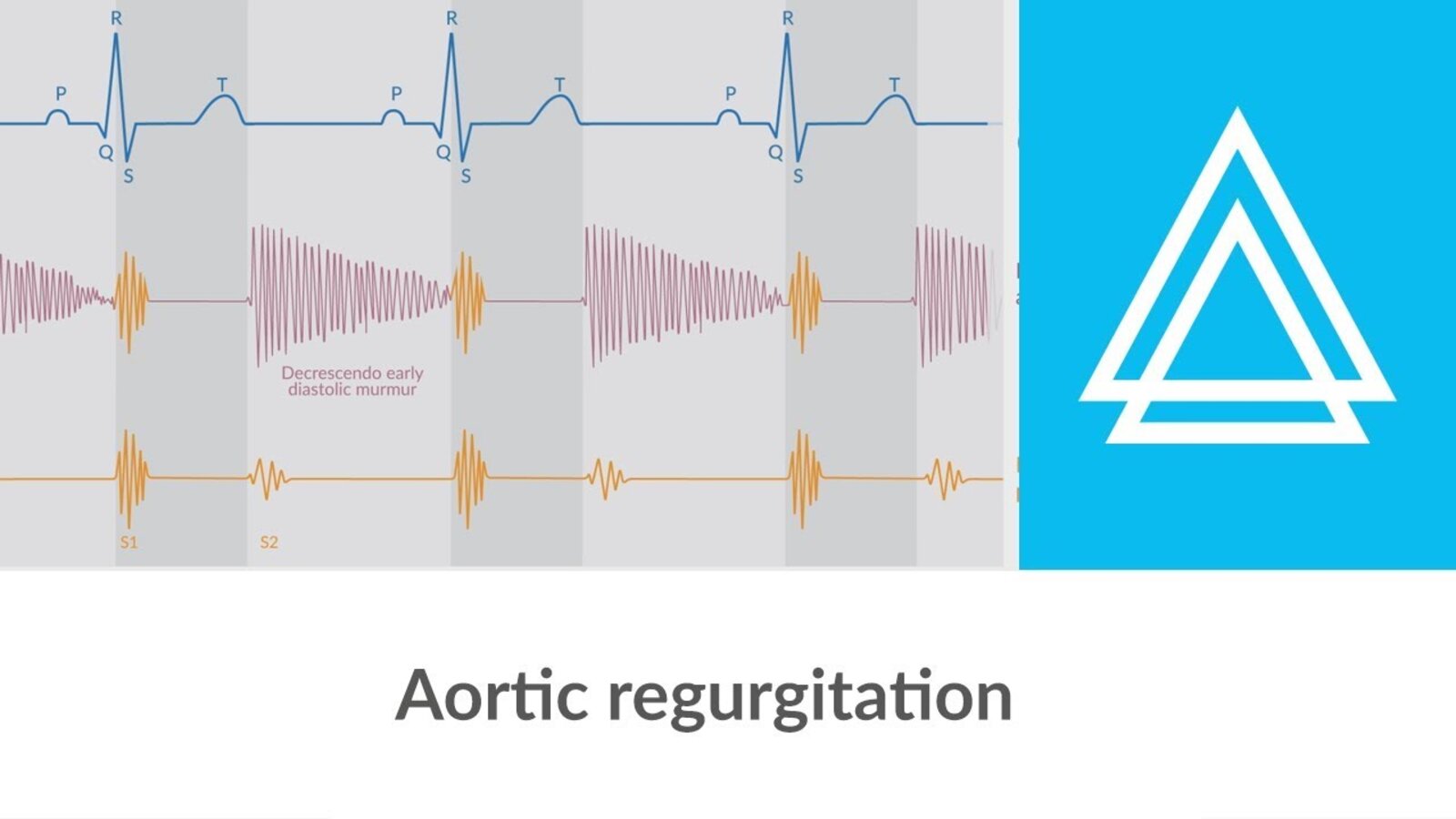
(D) Aortic and pulmonary regurgitation (decrescendo murmur)
Note that patent ductus arteriosus produces a continuous murmur heard in both systole and diastole.
OS: opening snap
© AMBOSS
© AMBOSS
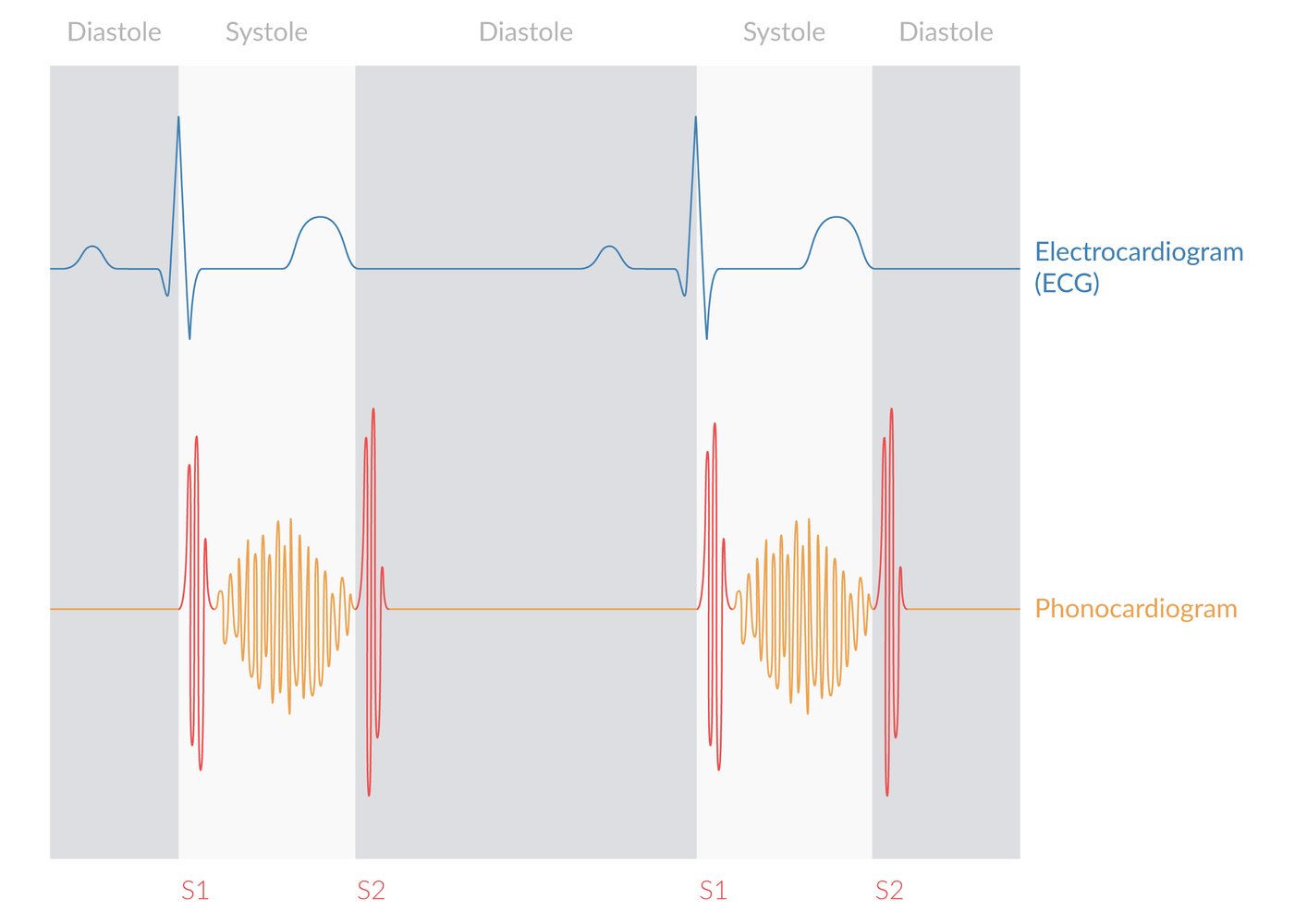
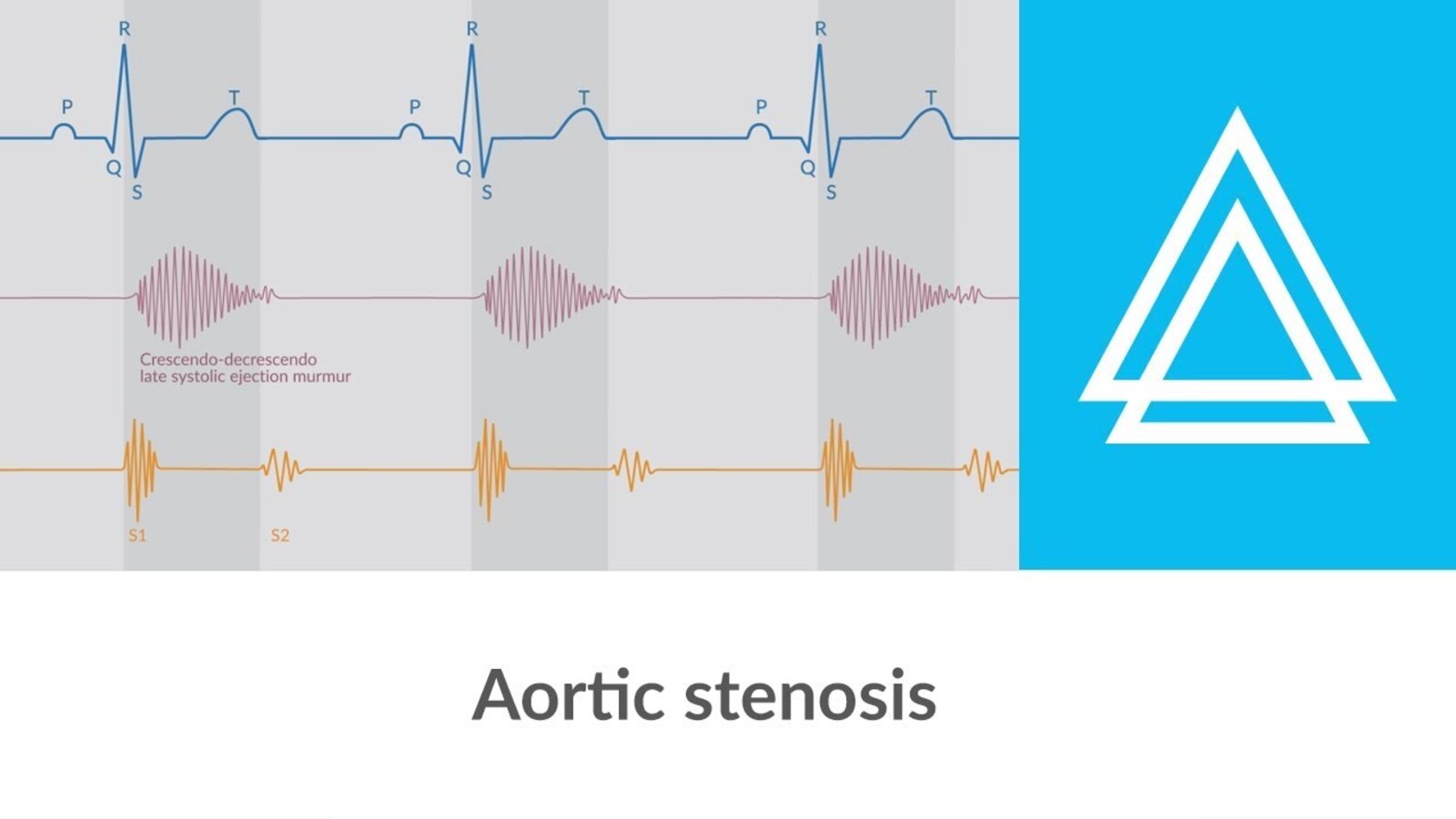
A crescendo-decrescendo late systolic murmur is depicted. In the case of aortic stenosis, the murmur may radiate to the carotid arteries.
© AMBOSS
© AMBOSS
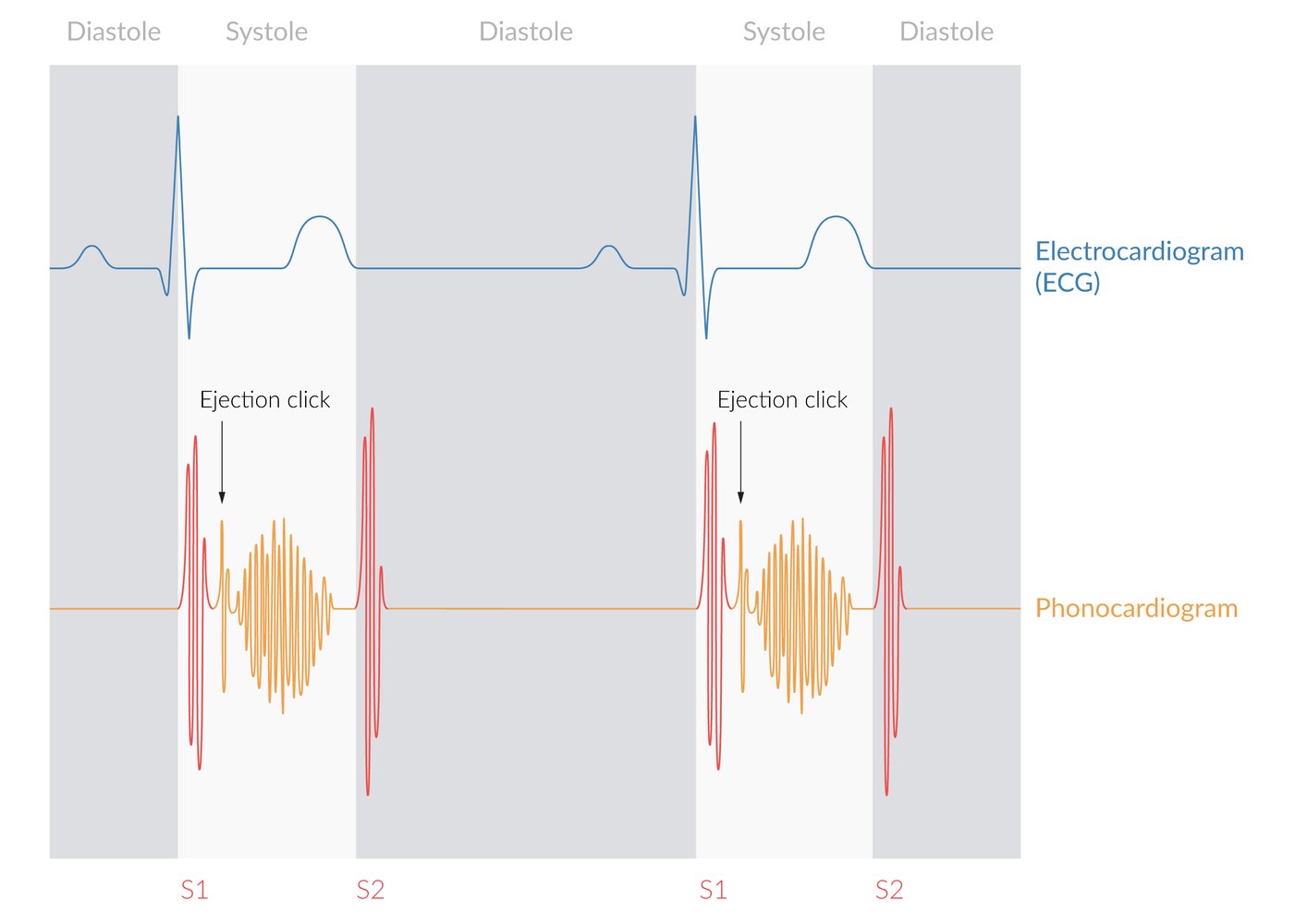
Crescendo-decrescendo ejection murmur with an ejection click
In aortic stenosis, there is usually radiation into the carotids.
© AMBOSS
© AMBOSS
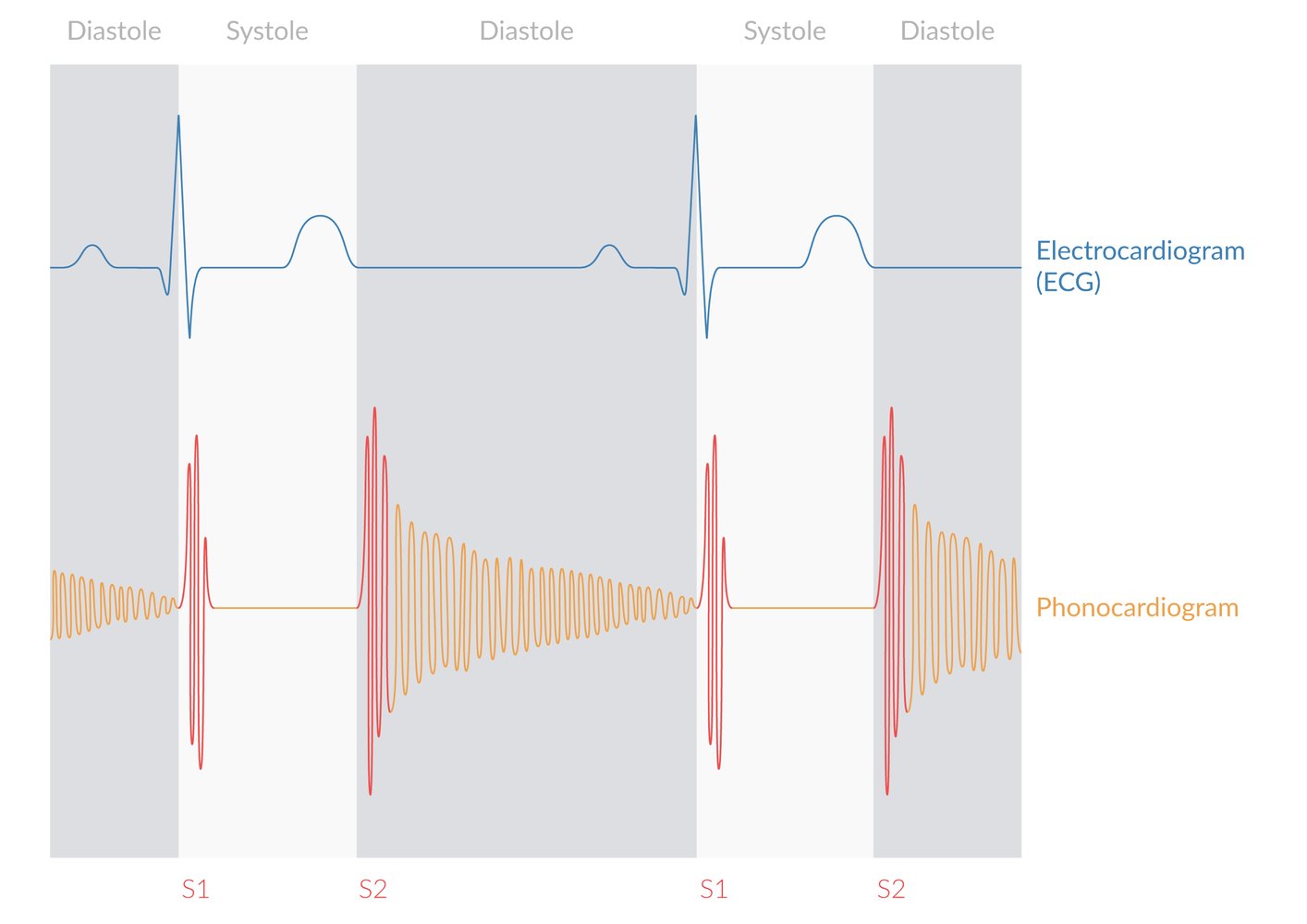
Early-diastolic decrescendo murmur (directly after the second heart sound), consistent with aortic regurgitation and/or pulmonary regurgitation.
© AMBOSS
© AMBOSS

© AMBOSS
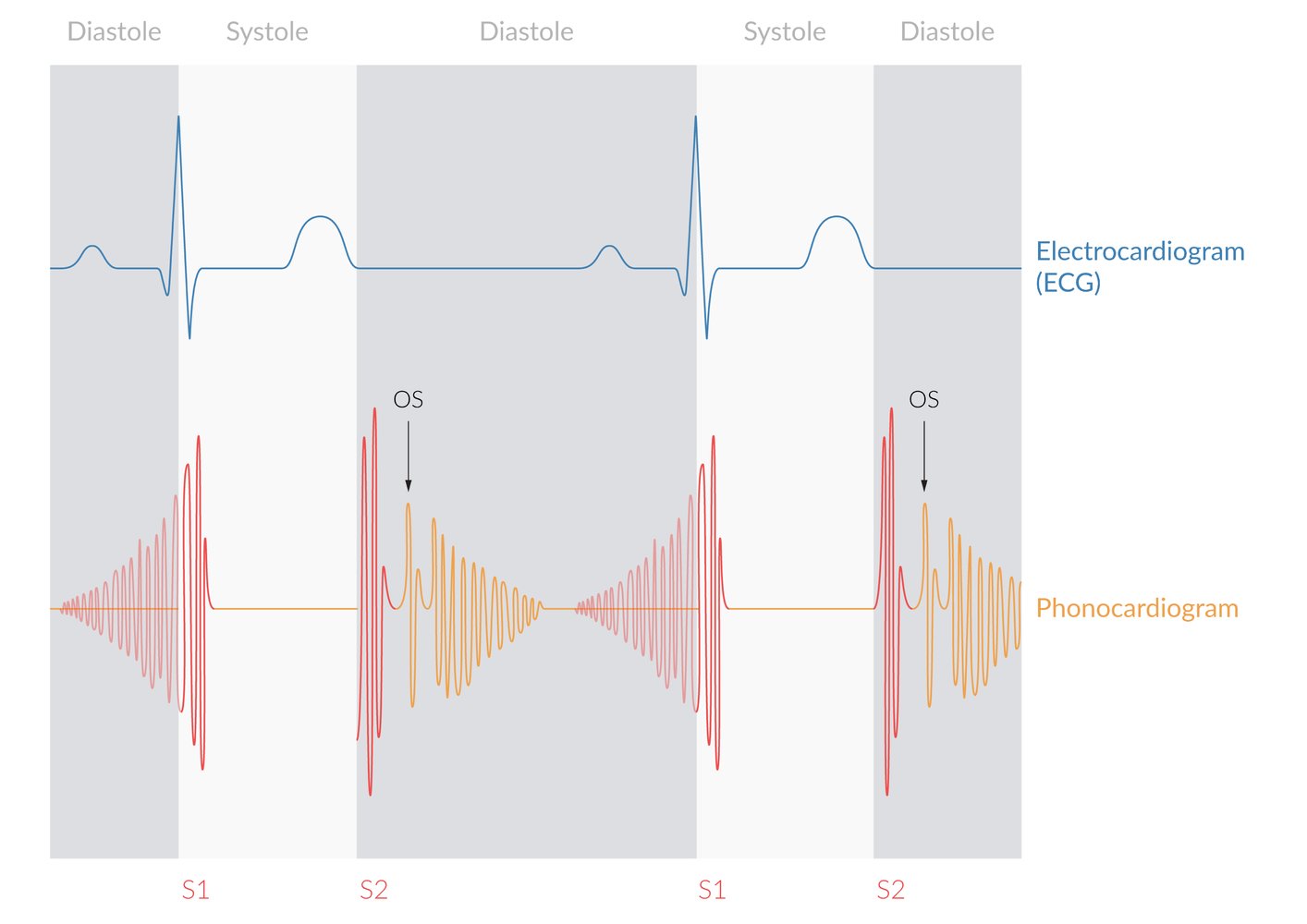
Delayed decrescendo diastolic murmur. A presystolic crescendo murmur and/or mitral valve opening snap (OS) may also be present.
© AMBOSS
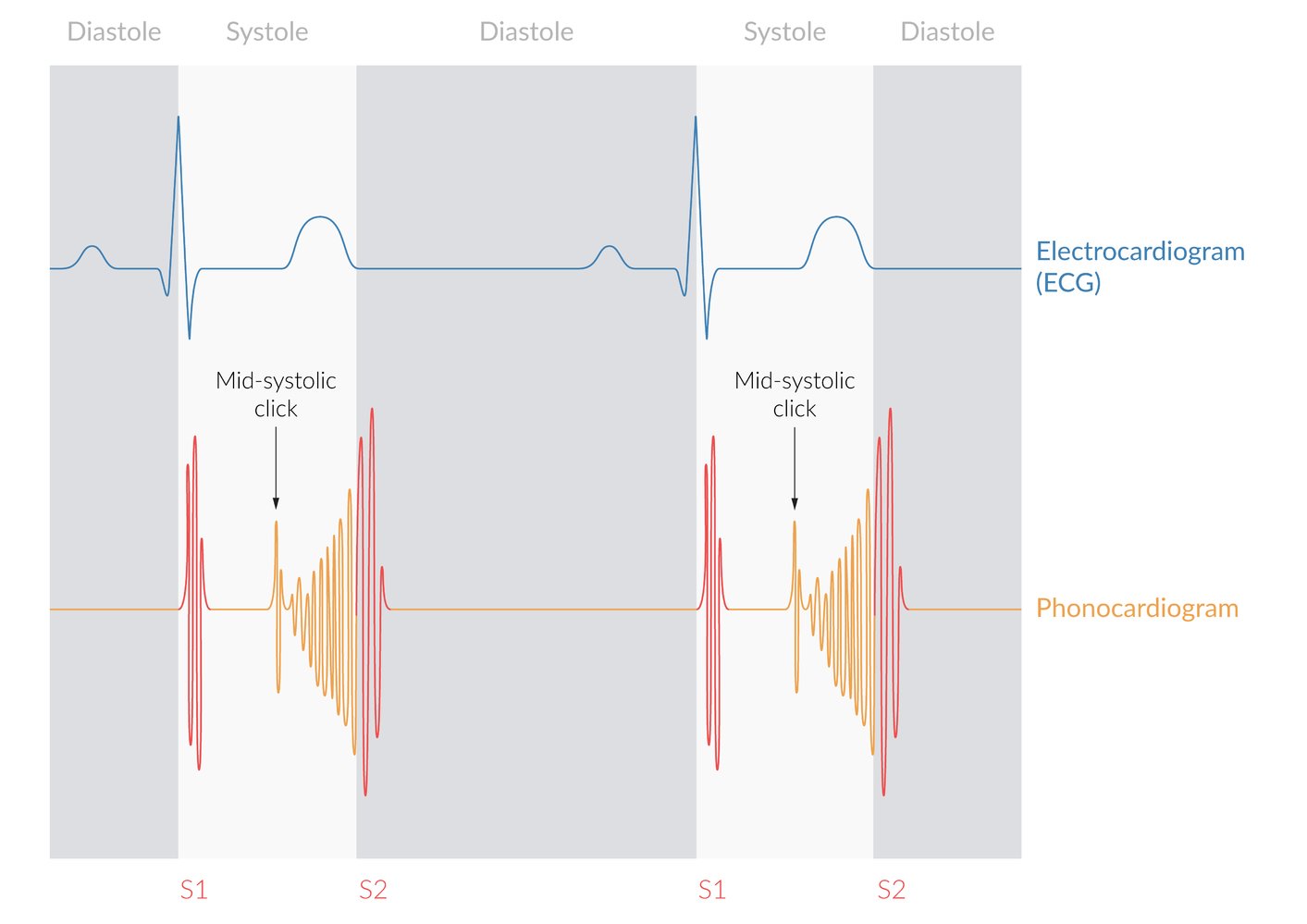
High-frequency, mid-systolic click with a late systolic crescendo murmur.
© AMBOSS
© AMBOSS
Holosystolic murmur (often referred to as “pansystolic murmur” in the case of a ventricular septal defect)
© AMBOSS
© AMBOSS
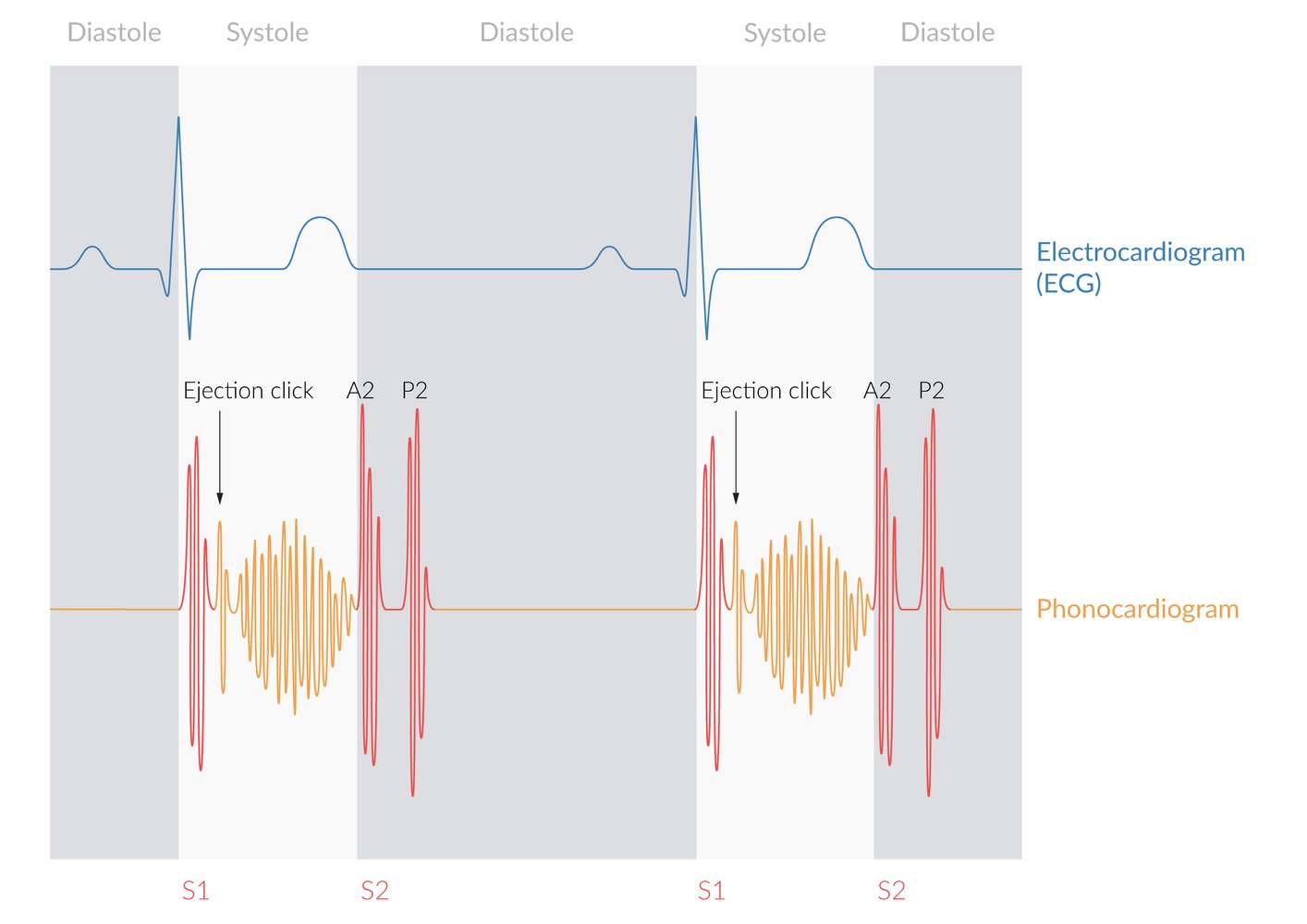
Crescendo-decrescendo murmur with ejection click and widely split second heart sound
© AMBOSS
Delayed diastolic murmur with a decrescendo, possible presystolic crescendo
© AMBOSS
© AMBOSS
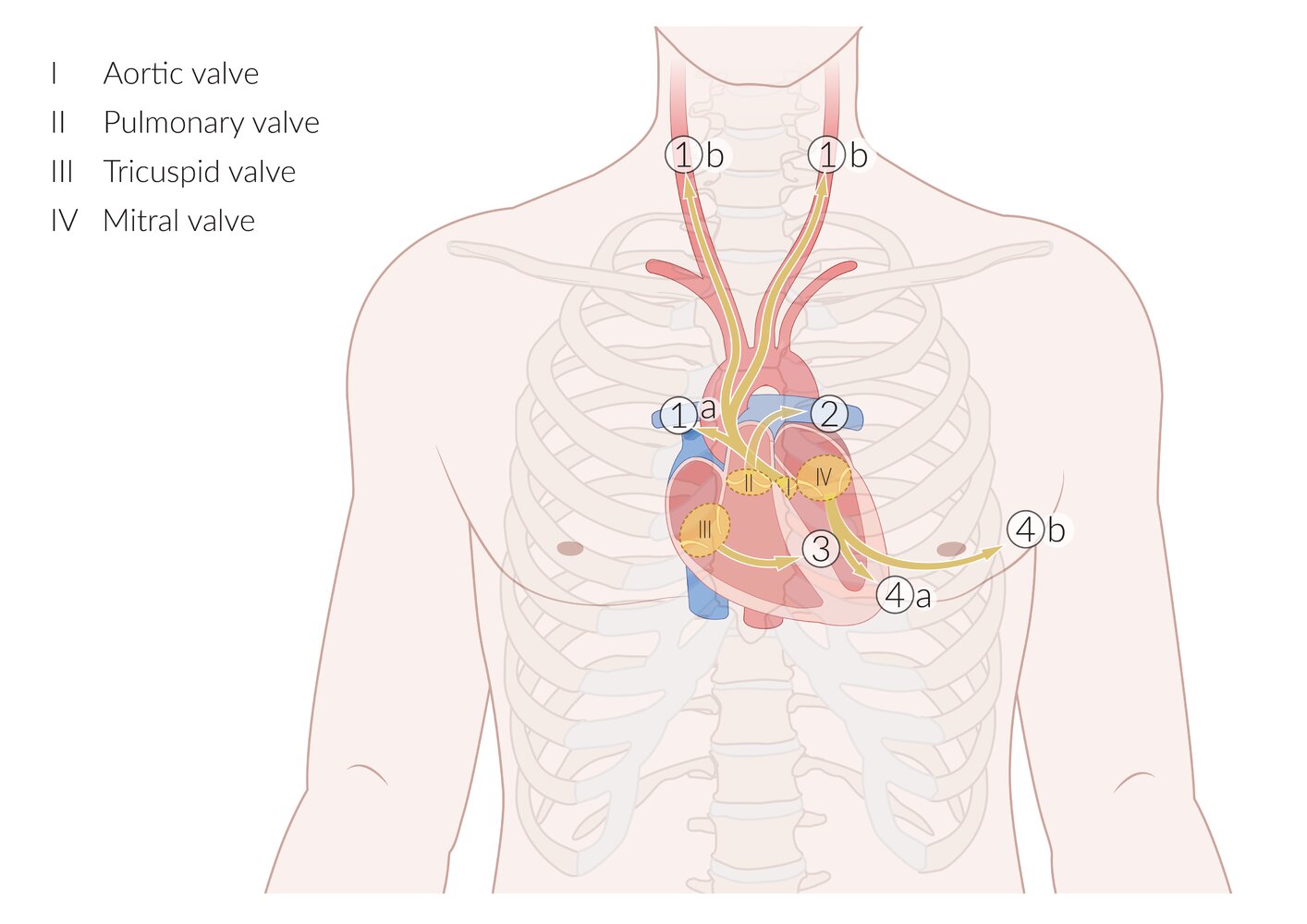
I–IV: anatomical locations of heart valves
1. Aortic area: 2nd right parasternal intercostal space (ICS)
- Ideal site for auscultation of aortic valve murmurs (1a). The murmur of aortic stenosis also radiates to the carotid arteries (1b).
2. Pulmonary area: 2nd left parasternal ICS
- Ideal site for auscultation of pulmonary valve murmurs
3. Tricuspid area: 4th left parasternal ICS
- Ideal site for auscultation of tricuspid valve murmurs
4. Mitral area: 5th left ICS in the midclavicular line (over the cardiac apex)
- Ideal site for auscultation of mitral valve murmurs (4a). The murmur of mitral regurgitation also radiates to the left axilla (4b).
© AMBOSS
© AMBOSS
Management
This section provides a general overview of various management strategies for valvular heart diseases (VHDs). See the respective articles on aortic stenosis, aortic regurgitation, mitral stenosis, and mitral regurgitation for the management of acutely decompensated VHD, and for further details on the management of chronic VHD.
Approach [6]
- Perform a thorough initial evaluation, including TTE and assessment of symptoms and comorbidities.
- Consider the need for advanced studies to identify symptom etiology and further characterize valvular lesions.
- Classify the disease according to severity.
- Refer patients with indications for interventional treatment (e.g., those with severe and/or symptomatic VHD):
- Valve repair vs. prosthetic heart valve replacement
- Surgical vs. transcatheter approach
- Refer patients without indications for valve intervention at diagnosis to a cardiologist for monitoring.
- Offer supportive care to all patients.
Acutely decompensated VHD (e.g., presenting as cardiogenic shock, acute heart failure, or acute arrhythmia symptoms) requires urgent management and cardiology consultation.
The approach to management depends on the type and severity of VHD, the patient's individual risk profile (e.g., comorbidities, age, and fitness level), evaluation of risks and benefits of each procedure, and shared decision-making.
Diagnostics
Minimum diagnostic workup [6]
- ECG: to assess cardiac rhythm and check for signs of ventricular hypertrophy
- TTE: to assess cardiac structure, valve morphology, and hemodynamics
- Consider chest x-ray to assess for pulmonary congestion or lung pathology.

Advanced studies [6]
- Transesophageal echocardiography (TEE): for more precise estimations of valve anatomy and/or to identify possible complications
- Cardiac MRI: to assess for structural heart disease
- Cardiac catheterization: to assess valve hemodynamics and cardiac pressures
- Exercise stress testing: Consider in patients with unclear symptom history.
")
Classification [6]
- Valvular disease is classified into four stages (A-D) depending on the severity of disease.
- Classification is based on:
- Presence of symptoms
- Valve anatomy and hemodynamics
- Effects on cardiac chambers and pulmonary circulation (e.g., LVEF, chamber dilation, right ventricular function)
- For more information, see:
- AHA staging for aortic valve stenosis
- AHA staging for chronic aortic valve regurgitation
- AHA staging for mitral valve stenosis
- AHA staging for mitral valve regurgitation
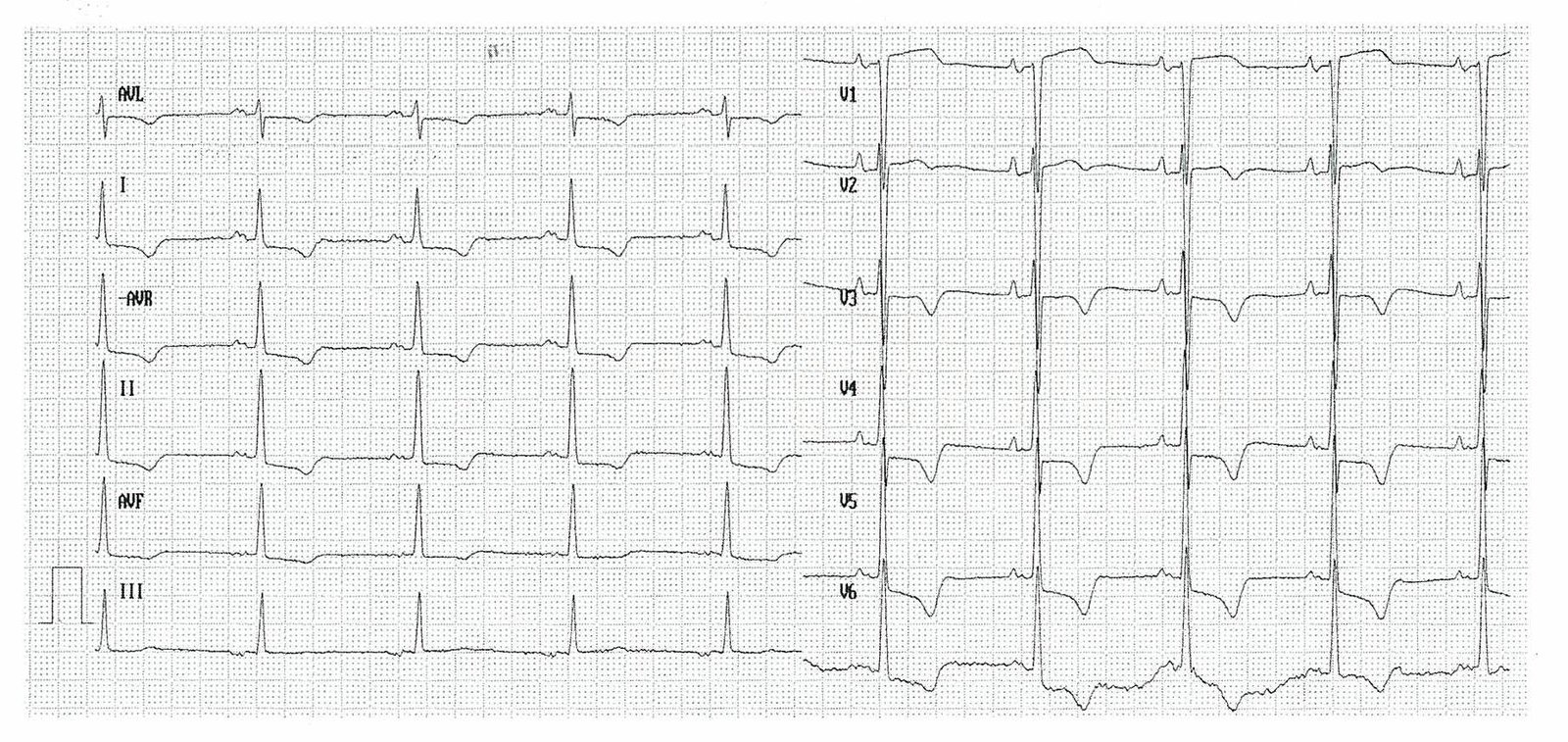
12-lead ECG (paper speed: 25 mm/s)
– Heart rate: ∼55/min
– Regular sinus rhythm
– Normal cardiac axis: positive (+) QRS complex polarity in leads I, II, and III
– Broad and bifid P waves (P): referred to as “P mitrale” and suggestive of left atrial enlargement
– SV2 (S) + RV5 (R) >3.5 mV: meets Sokolow-Lyon criteria for left ventricular hypertrophy
– Left ventricular strain pattern: ST depression (ST) with T-wave inversion (T) in left-sided leads I and V4–V6
Positive Sokolow-Lyon criteria and left ventricular strain pattern are characteristic of left ventricular hypertrophy.
Source: © IMPP
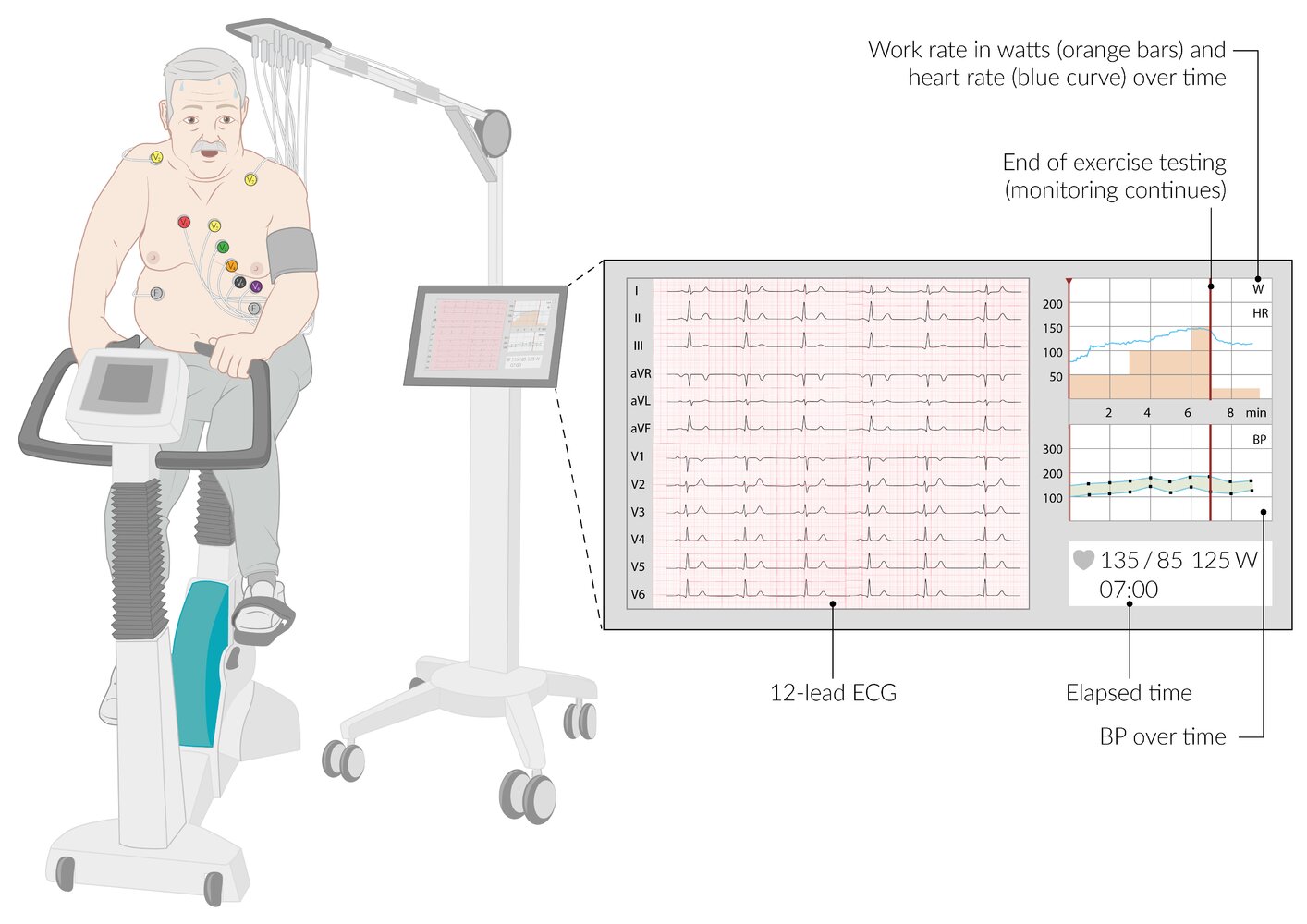
While the patient exercises, their blood pressure, heart rate, and 12-lead ECG are continuously recorded. Exercise intensity can be adjusted by altering the resistance and/or rate of pedaling, and the patient's work rate is calculated in watts. The test continues until the protocol is complete or there is an indication for early test termination.
© AMBOSS
Medical treatment
Supportive care [6]
- Screen for and manage other traditional atherosclerotic cardiovascular disease risk factors.
- Manage complications, e.g., treatment of heart failure.
- Consider indications for endocarditis prophylaxis before procedures that may cause bacteremia.
- Secondary prevention of rheumatic fever if indicated (see “Prevention” in “Acute rheumatic fever”)
- Prevention of thromboembolism if indicated (e.g., anticoagulant therapy after heart valve replacement)
Monitoring for disease progression [6]
Monitor all patients without indications for intervention at diagnosis.
- Repeat patient history and physical examination annually.
- Obtain TTE follow-up at fixed intervals depending on the type and severity of valve defect.
- Consider advanced studies and/or referral for valve intervention depending on findings.
Interventional treatment
Valve repair [6]
-
Valve reconstruction
-
Annuloplasty [7]
- A ring-shaped device is attached to the outside of the valve opening to reestablish the shape and function of the valve.
- Commonly used to treat mitral valve regurgitation [8]
- Leaflet repair: involves the use of a clip device; may be performed in patients with mitral valve regurgitation
-
Annuloplasty [7]
-
Valvuloplasty
- A procedure performed in patients with valvular stenosis (e.g., aortic valve stenosis or mitral stenosis) to separate fused or calcified valve leaflets.
- Approach
- Percutaneous balloon valvuloplasty: A balloon is advanced into the target valve (either transfemorally or transapically) and inflated, opening the stenotic valve.
- Open commissurotomy: open surgical procedure to separate fused and/or calcified leaflets
Prosthetic heart valve replacement [6]
| Overview of prosthetic heart valve replacement options [6] | ||
|---|---|---|
| Mechanical prosthetic valve | Biological prosthetic valve | |
| Indications |
|
|
| Advantages |
|
|
| Disadvantages |
|
|
The choice of mechanical vs. bioprosthetic valve replacement should be based on shared-decision making, patient age and preference, presence of comorbidities (e.g., conditions that increase the patient's surgical risk), and ability to take anticoagulation.



Replacement route
The approach depends on the type of valve (e.g., mechanical vs. bioprosthetic) and the patient's surgical risk.
- Surgical heart valve replacement: may be done in conjunction with a CABG in suitable patients who require both procedures
-
Transcatheter aortic valve replacement (TAVR)
- A minimally invasive, percutaneous procedure that utilizes an endovascular technique to replace the aortic valve.
- A collapsible replacement valve is inserted via a catheter and placed over the native valve.
- Once the replacement valve is expanded, it displaces the old valve and assumes its function.
- Transcatheter mitral valve replacement
Complications of heart valve intervention [6][9]
-
Patient-prosthesis mismatch
- Caused by implantation of a prosthetic valve with a functional area that is too small for the cardiac demand of the patient
- Leads to left ventricle hypertrophy and impaired exercise capacity
- Increased risk of other cardiac events (e.g., arrhythmia, MI) and increased mortality
-
Prosthetic valve thrombosis [10][11]
- Etiology
- Mechanical valves are more prone to thrombosis than biological prosthetic valves.
- Ιnsufficient anticoagulatory therapy after valve replacement
- Clinical features
- Signs of acute heart failure due to valve dysfunction (e.g., dyspnea, fatigue, peripheral edema)
- New murmur consistent with valve obstruction and/or regurgitation
- Thromboembolic event (e.g., TIA)
- Diagnostics
- First-line imaging: transthoracic or transesophageal echocardiography [11]
- If echocardiography is negative: cardiac CT to assess leaflet anatomy and motility
- Treatment: anticoagulation and fibrinolysis, surgical valve replacement
- Etiology
- Prosthetic valve dysfunction: e.g., paravalvular leak
- Prosthetic valve stenosis or regurgitation: Clinical presentation is similar to native valve disease.
- Cardiac complications: e.g., prosthetic valve endocarditis, heart failure, pericarditis, high-grade AV block, atrial fibrillation [6]
- Vascular complications: e.g., bleeding, femoral artery dissection, hemolytic anemia in patients with a mechanical valve , thromboembolism [6]
- Other: e.g., stroke, acute kidney injury
Preoperative risk assessment [6]
- Prior to any valve procedure, preoperative testing includes:
- Coronary angiography to assess coronary anatomy
- CT imaging
- Dental examination to assess the risk of infection
- Additional evaluations may be required prior to open surgery: Refer for preoperative testing for high-risk surgery.
Post-procedure follow-up [6]
- Monitor patients for recurrent or persistent symptoms and complications of heart valve intervention.
- Obtain TTE to evaluate valve and cardiac function.
- 1–3 months after valve procedure [6]
- At fixed intervals thereafter depending on type of valve replacement
Anticoagulant therapy after heart valve replacement [6]
-
Mechanical valve replacement
- Lifelong anticoagulation with a vitamin K antagonist (VKA) to a target INR [6]
-
Bridging anticoagulation is recommended when VKA is interrupted (e.g., for surgery) for patients with:
- Aortic valve replacement and additional risk factors for thromboembolism
- Mitral valve replacement
-
Biological valve replacement
- Anticoagulation with VKA for 3–6 months after intervention
- Low-dose aspirin after discontinuing VKA can be beneficial.
- In patients with atrial fibrillation and a bioprosthetic valve replacement > 3 months prior, a non-vitamin K oral anticoagulant (NOAC) may be considered based on the CHA2DS2-VASc score.
Insufficient anticoagulation increases the risk of thromboembolism, while excessive anticoagulation with VKA increases bleeding risk significantly. In patients with a mechanical valve and uncontrollable hemorrhage, anticoagulation reversal may be indicated.

Mechanical valves are constructed entirely of non-biological materials (here a pyrolitic carbon valve with a dacron cuff).
Source: © IMPP
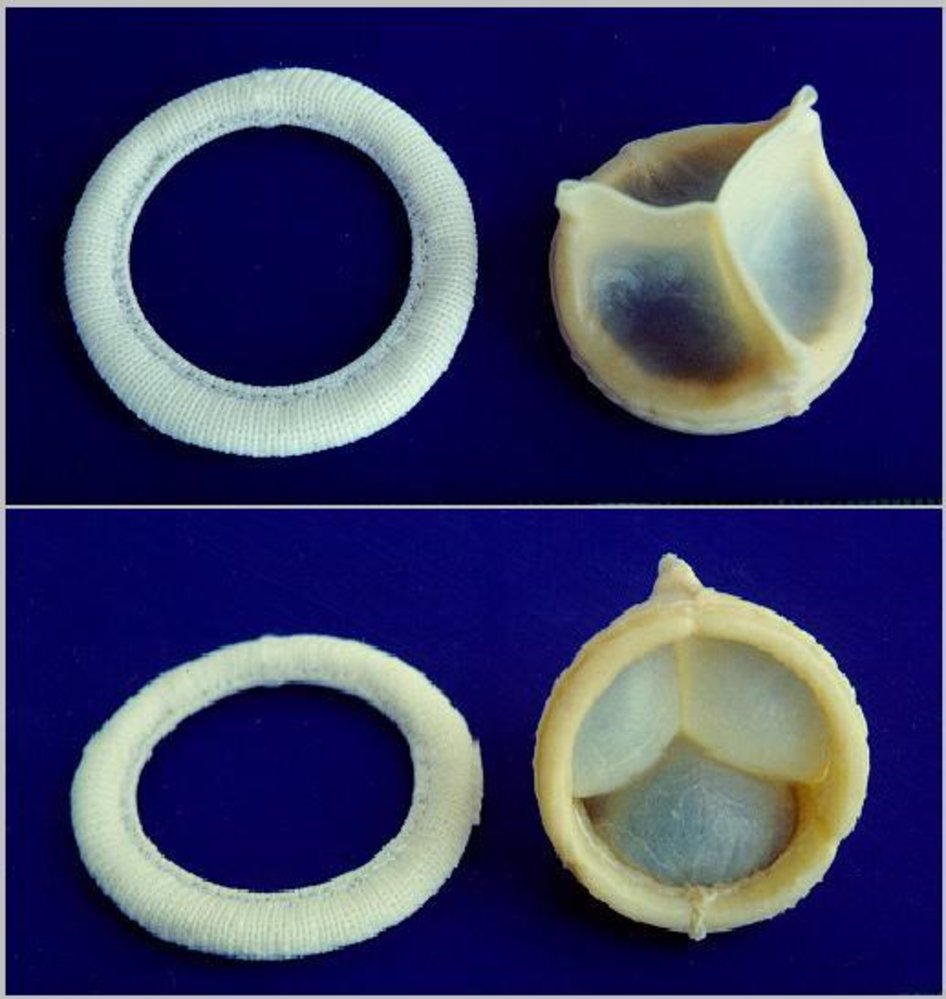
Photographic image of a bioprosthetic heart valve
This particular bioprosthetic heart valve is a replacement for an aortic valve (it features three leaflets).
Source: “BiologicalValves” by Robertolyra, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}
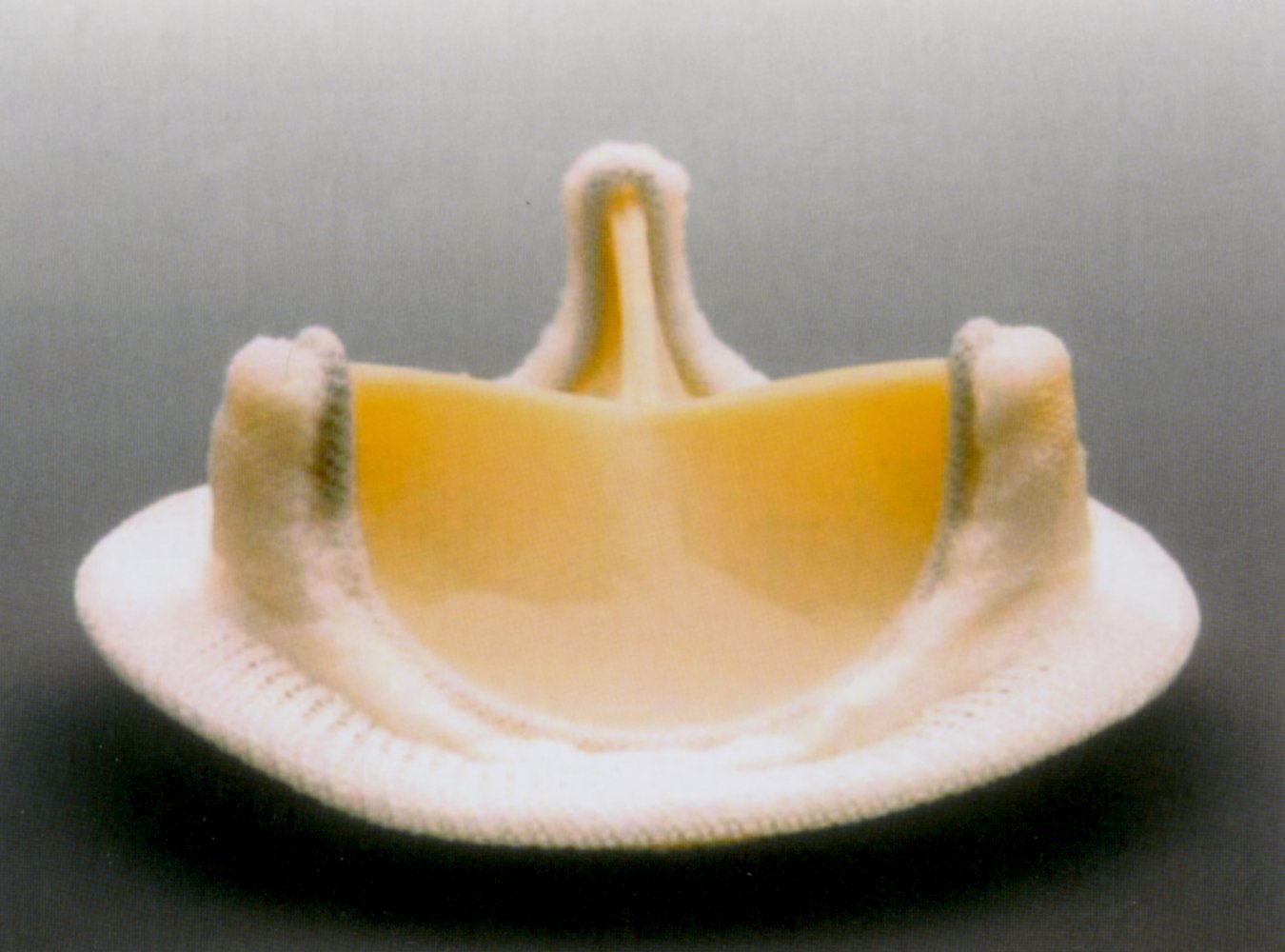
A stented bioprosthetic valve, consisting of xenograft material (most commonly porcine aortic valve leaflets or bovine pericardium) mounted on a manufactured supporting stent.
Source: © IMPP
Special patient groups
VHD and pregnancy [6][12][13]
- The hemodynamic demands of pregnancy increase the risk of cardiovascular morbidity and mortality in individuals with VHD.
- Refer patients with VHD to a cardiologist for pre-pregnancy counseling and risk assessment; and follow-up during pregnancy and postpartum.
- Management of VHD in pregnancy should involve a multidisciplinary care team (e.g., cardiology, maternal-fetal medicine, anesthesiology).
Contraception [12][14][15]
The CDC offers an app to guide contraceptive method selection based on the US Medical Eligibility Criteria for Contraceptive Use and the US Selected Practice Recommendations for Contraceptive Use. See “Tips and Links.”
- Offer contraception counseling and tailor contraceptive choice, in consultation with cardiology, based on the following: [12]
- Patient preference
- Contraception contraindications
- Type and severity of the cardiac condition
- Risks and benefits of the contraceptive agent on the cardiac condition
- Choice of reversible contraception: [12][13][14]
- Progestin-only contraception is generally preferred for patients with VHD.
- IUDs are recommended for patients with high-risk cardiac conditions.
Avoid combined hormonal contraceptives in individuals with VHD who are at high risk for thromboembolism (e.g., patients with complex valvular pathology). [12][15]
Planning pregnancy [6][12]
- Counsel patients on the risks to the pregnant individual and fetus.
- Counsel individuals at high risk to avoid pregnancy and consider reproductive alternatives (e.g., surrogacy, adoption).
- Offer genetic counseling to patients with genetic causes of VHD (e.g., Marfan syndrome). [16]
- Refer to cardiology for appropriate evaluation and optimization of management of VHD before pregnancy, including: [6]
- Cardiac testing (e.g., TTE, exercise stress testing)
- Consideration for prosthetic valve replacement before pregnancy
- Adjusting medications to avoid teratogenicity: See "Pregnancy restrictions on heart failure medications.”
During pregnancy [6][12]
Refer all patients to an obstetrician specializing in complex pregnancies and a cardiologist specializing in VHDs for multidisciplinary care.
- Offer elective pregnancy termination, when appropriate, to patients with high-risk conditions (e.g., severe mitral stenosis, severe symptomatic aortic stenosis). [12]
- Refer to specialists to:
- Review pregnancy restrictions on heart failure medications and switch to safer agents if feasible.
- Determine disease-specific management, e.g.:
- Anticoagulation (e.g., in patients with mechanical heart valves)
- Intrapartum antibiotics in patients with indications for endocarditis prophylaxis
- See “Management of high-risk pregnancies” for considerations related to delivery.
ACE inhibitors, angiotensin receptor blockers, and warfarin are contraindicated during pregnancy. Do not change or discontinue current medications without specialist consultation and careful consideration of the type and severity of the cardiac condition and the risks and benefits of continuing the medication. [6][13]
External Resources
- CDC contraception app
- 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease
- 2020 AHA Scientific Statement on Cardiovascular Considerations in Caring for Pregnant Patients
- 2020 ACOG Committee Opinion on Gynecologic Considerations for Adolescents and Young Women With Cardiac Conditions
- 2019 (reaffirmed in 2021) ACOG Practice Bulletin on Pregnancy and Heart Disease
References
- Iung B, Vahanian A. "Epidemiology of Acquired Valvular Heart Disease". Can J Cardiol. 30(9). :962-970. (2014)
- Lincoln J, Garg V. "Etiology of Valvular Heart Disease". Circulation Journal. 78(8). :1801-1807. (2014)
- Waller BF. "Etiology of pure tricuspid regurgitation.". Cardiovasc Clin. 17(2). :53-95. (1987)
- Kasper DL, Fauci AS, Hauser SL, et al. "Harrison's Principles of Internal Medicine". McGraw-Hill Education. (2015). ISBN: 9780071802161
- Nishimura RA, Otto CM, Bonow RO, et al. "2017 AHA/ACC Focused Update of the 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease". J Am Coll Cardiol. 70(2). :252-289. (2017)
- Otto CM, Nishimura RA, Bonow RO, et al. "2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines". Circulation. 143(5). (2020)
- Acker MA, Parides MK, Perrault LP, et al. "Mitral-valve repair versus replacement for severe ischemic mitral regurgitation". N Engl J Med. 370(1). :23-32. (2014)
- Mazine A, Badiwala M, Cohen G. "Year in review". Curr Opin Cardiol. 31(2). :154-161. (2016)
- Vesey JM, Otto CM. "Complications of prosthetic heart valves". Curr Cardiol Rep. 6(2). :106-111. (2004)
- Dürrleman N, Pellerin M, Bouchard D, et al. "Prosthetic valve thrombosis: twenty-year experience at the Montreal Heart Institute.". J Thorac Cardiovasc Surg. 127(5). :1388-92. (2004)
- Dangas GD, Weitz JI, Giustino G, Makkar R, Mehran R. "Prosthetic Heart Valve Thrombosis". J Am Coll Cardiol. 68(24). :2670-2689. (2016)
- The American College of Obstetricians and Gynecologists. "ACOG Practice Bulletin No. 212: Pregnancy and Heart Disease". Obstetrics & Gynecology. 133(5). :e320-e356. (2019)
- Mehta LS, Warnes CA, Bradley E, et al. "Cardiovascular Considerations in Caring for Pregnant Patients: A Scientific Statement From the American Heart Association". Circulation. 141(23). (2020)
- American College of Obstetricians and Gynecologists’ Committee on Adolescent Health Care. "Gynecologic Considerations for Adolescents and Young Women With Cardiac Conditions". Obstet Gynecol. 136(5). :e90-e99. (2020)
- Nguyen AT, Curtis KM, Tepper NK, et al. "U.S. Medical Eligibility Criteria for Contraceptive Use, 2024". MMWR Recomm Rep. 73(4). :1-126. (2024)
- Isselbacher EM, Preventza O, Hamilton Black J, et al. "2022 ACC/AHA Guideline for the Diagnosis and Management of Aortic Disease: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines". Circulation. 146(24). (2022)