Summary
Vasculitides are a heterogeneous group of rare autoimmune diseases characterized by blood vessel inflammation (vasculitis). Inflammation can lead to ischemia, necrosis, and/or hemorrhage, with subsequent end-organ damage. Vasculitides are either primary (idiopathic) or secondary to an underlying disease (e.g., HBV infection, cancer, systemic lupus erythematosus) or drug use. Vasculitides are further classified based on the size of the affected vessels: small-, medium-, or large-vessel vasculitis, or variable vessel vasculitis. Diagnosing vasculitides is often challenging, as symptoms are usually nonspecific; vasculitides should be considered in patients presenting with constitutional symptoms and signs of multisystem disease (e.g., palpable purpura, pulmonary infiltrates, unexplained ischemic events). Laboratory studies, imaging, and histopathology are often required to confirm the diagnosis. Management should involve a multidisciplinary team (e.g., rheumatology, ophthalmology, neurology) and aims to promptly prevent the progression of vascular inflammation with immunosuppressive therapy to avoid organ damage and death. Treatment of the underlying cause (e.g., with antiviral drugs) and/or symptomatic management (e.g., with NSAIDs) is often necessary.
General principles
Etiology [1]
- Primary (idiopathic)
-
Secondary to another disease or drug use, e.g.:
- Infectious diseases
- Viral infection: e.g., HBV, HCV, HIV
- Infectious endocarditis
- Tuberculosis
- Syphilis
- Drugs: e.g., hydralazine, cocaine
- Malignancy: e.g., multiple myeloma, lymphoproliferative disorders
- Autoimmune diseases: e.g., systemic lupus erythematosus (SLE), Sjogren syndrome, sarcoidosis, IBD
- Infectious diseases
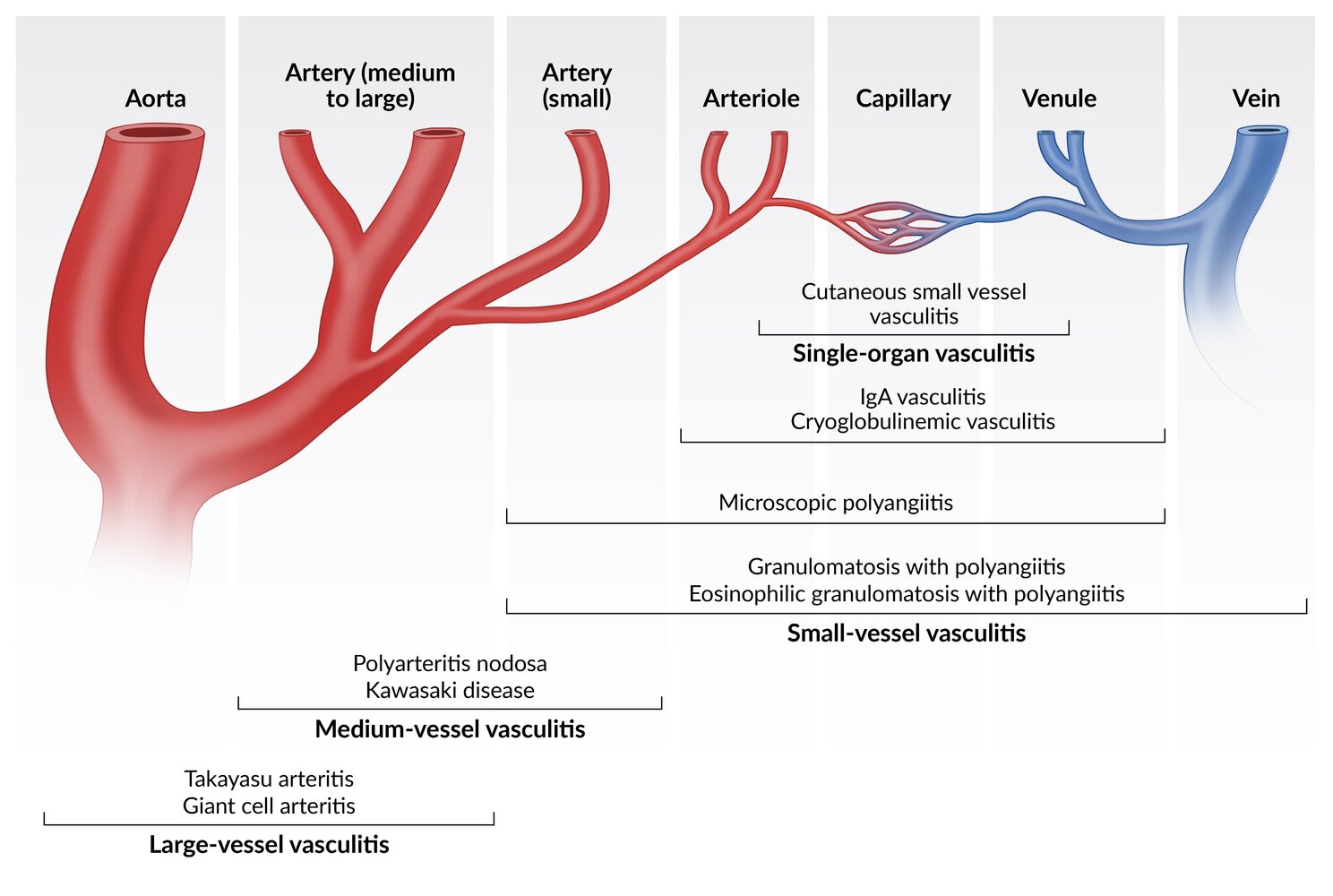
Classification [2]
- Based on the 2012 Chapel Hill Consensus Nomenclature
- Classification is based on the size of the vessel predominantly affected:
- Large-vessel vasculitis
- Medium-vessel vasculitis
-
Small-vessel vasculitis
- ANCA-associated vasculitis of small vessels
- Non-ANCA-associated vasculitis of small vessels
- Variable vessel vasculitis

Approach to management [1]
Vasculitis should be suspected in patients with constitutional symptoms and multisystemic inflammatory disease. Specific manifestations depend on the vessels affected.
- Tailor the approach to the suspected disease and/or affected organ or system.
- Rule out other (more common) diagnoses (e.g., infections, cancer, other autoimmune diseases).
- Assess for secondary causes of vasculitis (see “Etiology”).
- Consult a rheumatologist and/or other specialists as required.
- Start management based on disease severity and the affected organ or system.
Most patients with vasculitis present with nonspecific features (e.g., constitutional symptoms, elevated inflammatory markers).
Initial evaluation
- Perform a thorough history and physical examination; ≥ 1 of the following clinical features are usually found in patients with vasculitis :
- Typical cutaneous lesions (e.g., palpable purpura, livedo reticularis, digital gangrene)
- Pulmonary-renal syndromes (e.g., asthma, hemoptysis, glomerulonephritis)
- Limb claudication, asymmetric pulses and/or blood pressure measurements, bruits
- Temporal headache, visual loss, mononeuritis multiplex
- Findings suggestive of vasculitis on routine studies include:
- CBC: anemia of chronic disease, thrombocytosis, eosinophilia
- Inflammatory markers: ↑ ESR, ↑ CRP
- Infectious diseases workup: positive hepatitis B testing or hepatitis C testing
- Autoimmune diseases workup: negative ANAs and aPL antibodies
- Chest x-ray: lung involvement (e.g., ground glass opacity, nodular lesions)
Vasculitis has a wide variety of signs and symptoms; there is no single typical presentation.
Additional evaluation
Consider further diagnostics guided by clinical suspicion to:
- Determine the extent of the disease, e.g.:
- Urine studies and chest CT to evaluate for kidney and lung involvement
- Nerve conduction studies, electromyography, and creatine kinase levels
- Establish the type of vasculitis: e.g., ↓ ANCAs and ↑ cryoglobulins indicates cryoglobulinemic vasculitis
- Confirm the diagnosis: with imaging (e.g., MRA, CTA) or histological studies
Management
- Immunosuppressive therapy is generally indicated.
- Surgical therapy may be required in specific cases (e.g., those with limb ischemia).
-
Supportive care
- Provide pain management.
- Prevent complications of glucocorticoid therapy.
- Monitor adverse effects of immunosuppressants.
- Consider PCP prophylaxis.
© AMBOSS
Large-vessel vasculitis
| Overview of large-vessel vasculitides | |||
|---|---|---|---|
| Clinical features | Diagnostics | Management | |
| Giant cell arteritis [3] |
|
|
|
| Takayasu arteritis [3][5] |
|
|
|






© AMBOSS

The superficial temporal artery is prominent, which is suggestive of giant cell arteritis.
Source: © IMPP
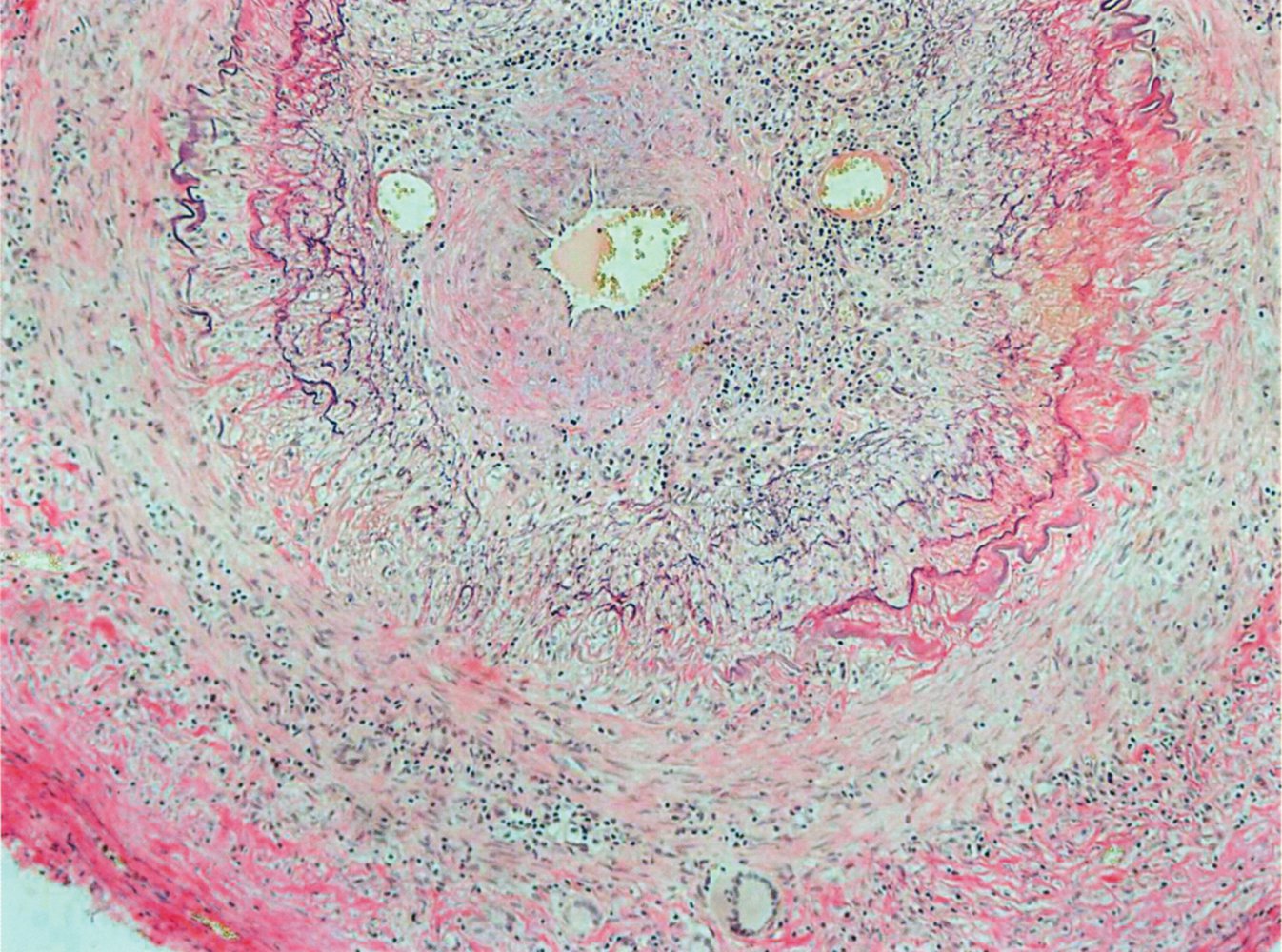
Temporal artery biopsy specimen (Van Gieson stain)
The vessel lumen is narrowed as the tunica intima is thickened and inflamed (yellow overlay). Disruption of the internal elastic lamina (examples indicated by arrowheads) is also visible.
These histological changes are typically seen in temporal arteritis.
Blue overlay: lymphocytic inflammation; dashed overlay: giant cells
Source: © IMPP

Angiography thoracic aorta (left anterior oblique view) of a patient with Takayasu arteritis
Stenoses (examples indicated by white arrows) are seen in the innominate (I), left common carotid (C), and left subclavian (S) arteries. An injection catheter is seen in the dilated ascending aorta (green overlay).
Source: "File:Takayasu Arteritis.jpg", Justin Ly, Wikimedia Commons licensed under Public Domain
{kind=link}
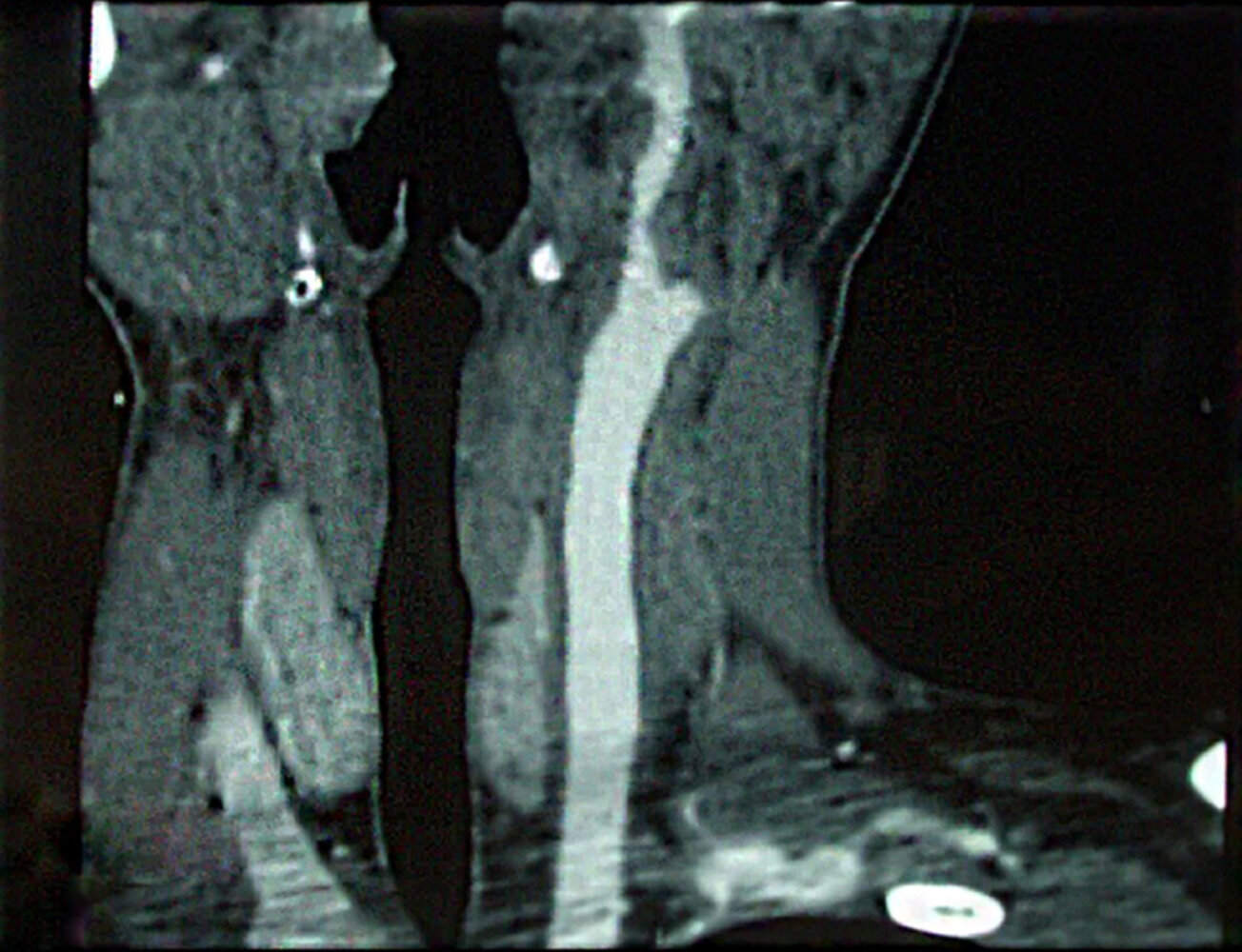
CT angiography neck (left carotid artery) of a patient with Takayasu arteritis
The external carotid artery shows a 50–60% stenosis (arrowheads). Mural thickening (green overlay) and irregularity of the left common carotid artery are also present.
Source: “First case of childhood Takayasu arteritis with renal artery aneurysms” by Tahar Gargah, Mouna Ben Harrath, Haythem Bachrouche et al., Pediatric Rheumatology, licensed under CC BY 2.0. Modifications: Arrows and bracket removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
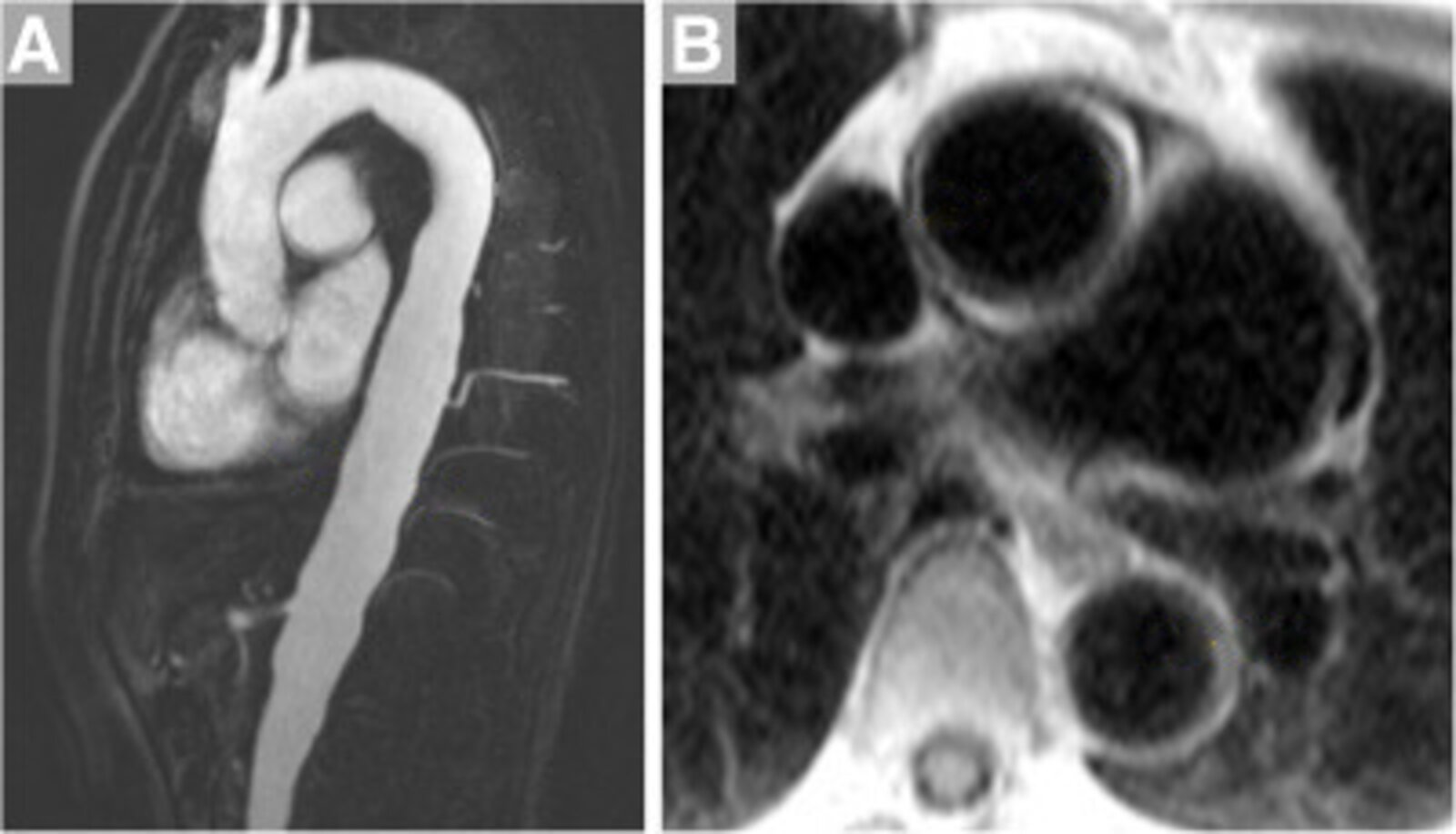
MRI angiography aorta (A: with contrast; sagittal plane. B: inversion recovery dark blood sequence; axial plane)
The descending aorta shows luminal dilatation and irregularity (A: green overlay), with multiple areas of wall thickening (B: examples indicated by red dimension lines).
These features are characteristic of Takayasu arteritis.
© AMBOSS. This image was adapted from the image “Figure 4, in: CMR in inflammatory vasculitis” by Raman SV, Aneja A, Jarjour WN, Journal of Cardiovascular Magnetic Resonance, licensed under CC BY 2.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Medium-vessel vasculitis
| Overview of medium-vessel vasculitides | |||
|---|---|---|---|
| Clinical features | Diagnostics | Management | |
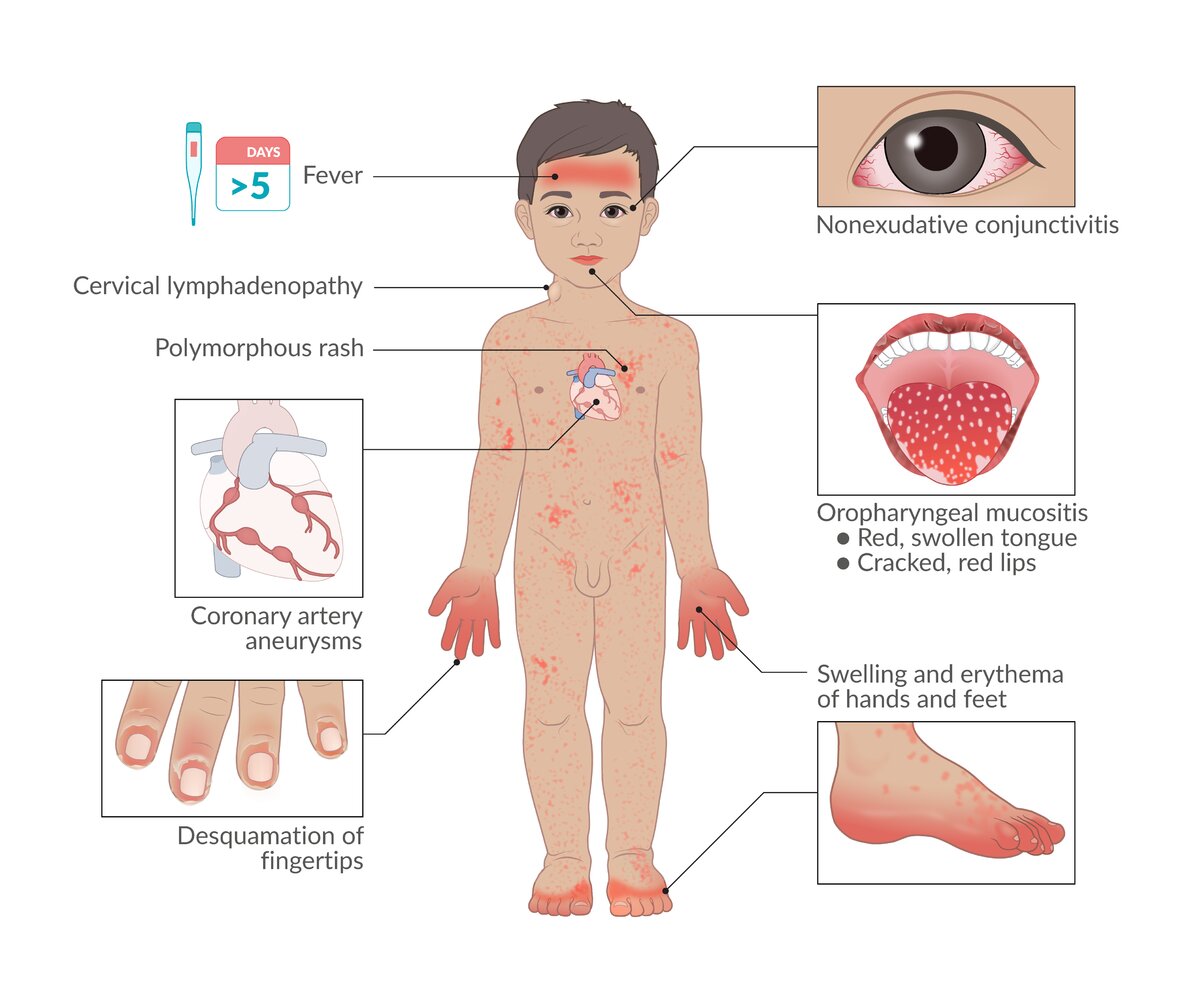
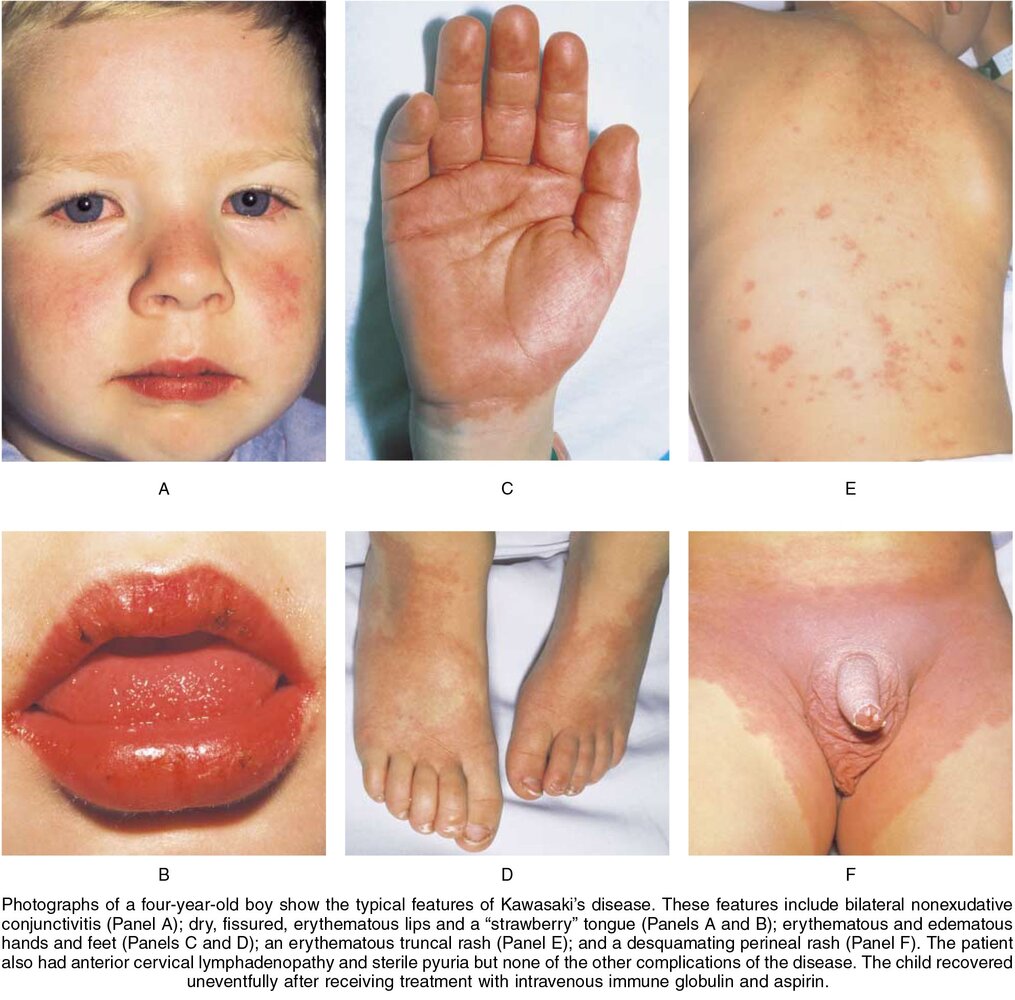
| Kawasaki disease |
|
|
|
| Polyarteritis nodosa |
|
|
|






© AMBOSS
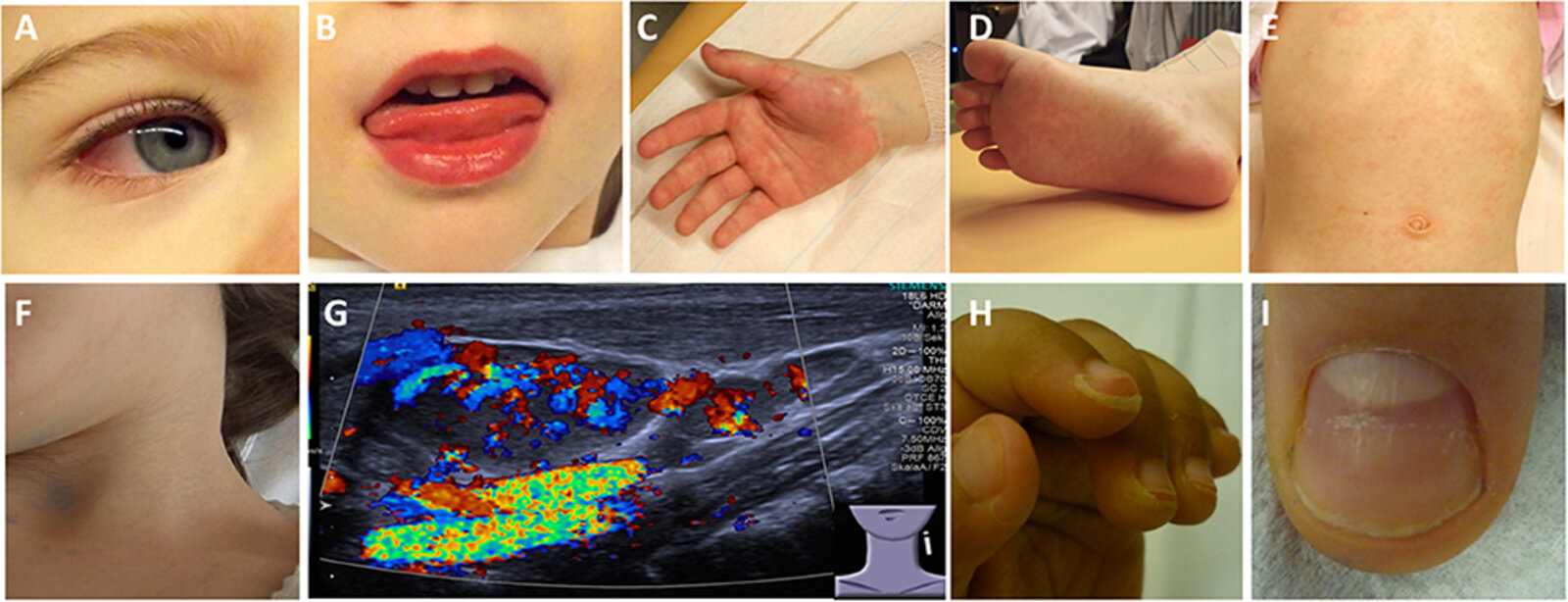
(A) Bilateral, nonpurulent conjunctivitis
(B) Stomatitis with bright red lips
(C) Erythema and edema of the hands
(D) Erythema and edema of the feet
(E) Truncal rash
(F) Cervical lymphadenopathy
(G) Ultrasound of an enlarged cervical lymph node: increased perfusion
(H) Desquamation of fingertips
(I) Deep grooves in the nail (Beau lines)
Source: “Figure 2, in: Kawasaki Disease” by C. M. Hedrich, A. Schnabel, T. Hospach, Frontiers in Pediatrics, licensed under CC BY 4.0.
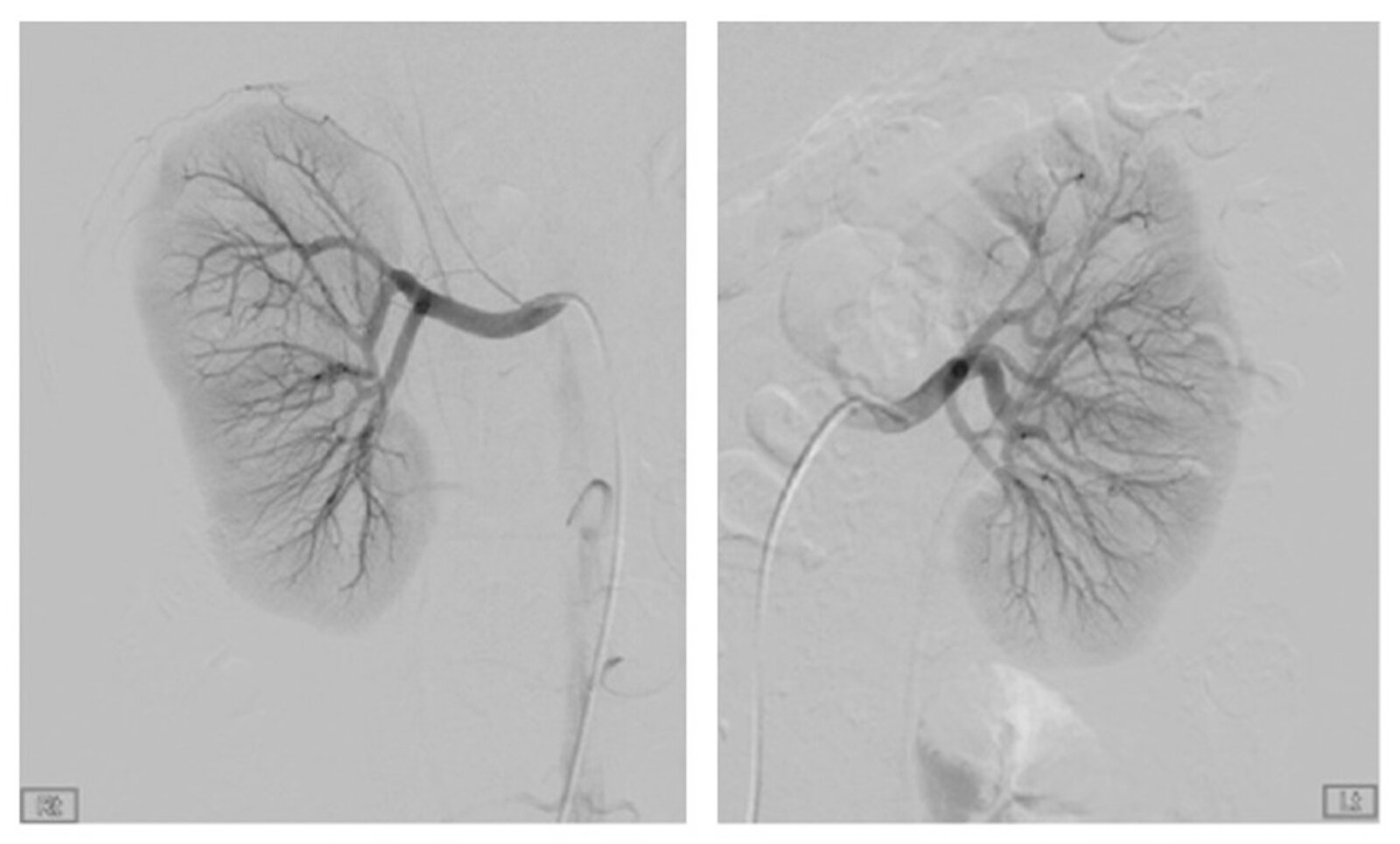
Angiography abdominal (kidneys; arterial phase) of a patient with polyarteritis nodosa
Selective contrast injections of the right and left renal arteries show microaneurysms in both kidneys (examples indicated by arrows).
Source: “Figure 2, in: Bilateral Spontaneous Perirenal Hemorrhage due to Initial Presentation of Polyarteritis Nodosa” by Hyung-Il Choi, Yang-Gyun Kim, Se-Yun Kim, Da Wun Jeong, Ki-Pyo Kim, Kyung-Hwan Jeong, Sang-Ho Lee, and Ju-Young Moon, Case Reports in Medicine, licensed under CC BY 3.0. Modifications: increased size. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
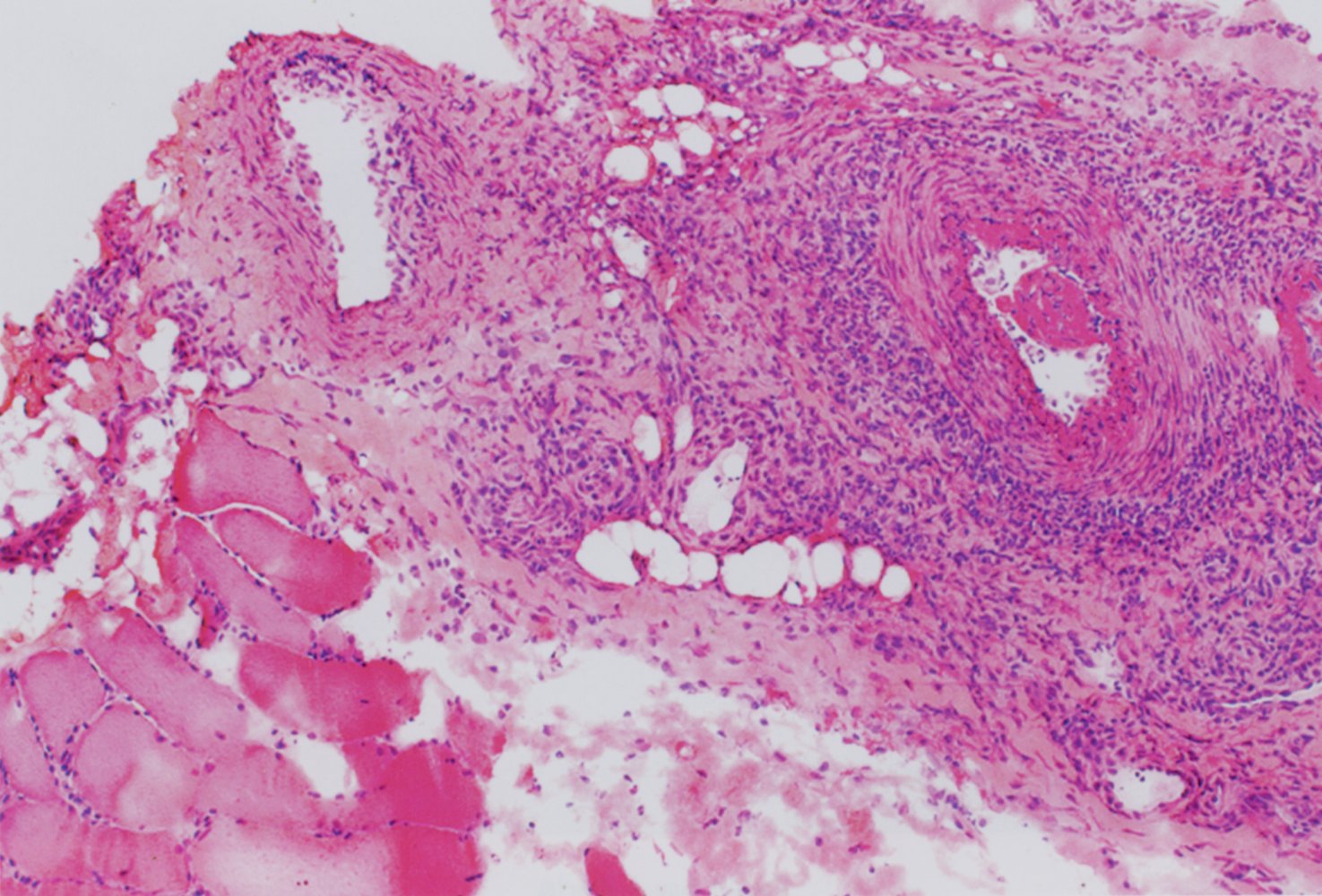
Photomicrograph of a muscle biopsy specimen (H&E stain; medium power magnification)
The artery (top right) shows a transmural inflammatory infiltrate (blue overlay), fibrinoid necrosis (yellow overlay; identifiable as the eosinophilic region within the arterial wall), and an intraluminal thrombus (blue hatched overlay). The skeletal muscle fibers (bottom left) appear normal.
Transmural necrotizing inflammation of small- and medium-sized arteries is a characteristic feature of polyarteritis nodosa.
Source: © IMPP
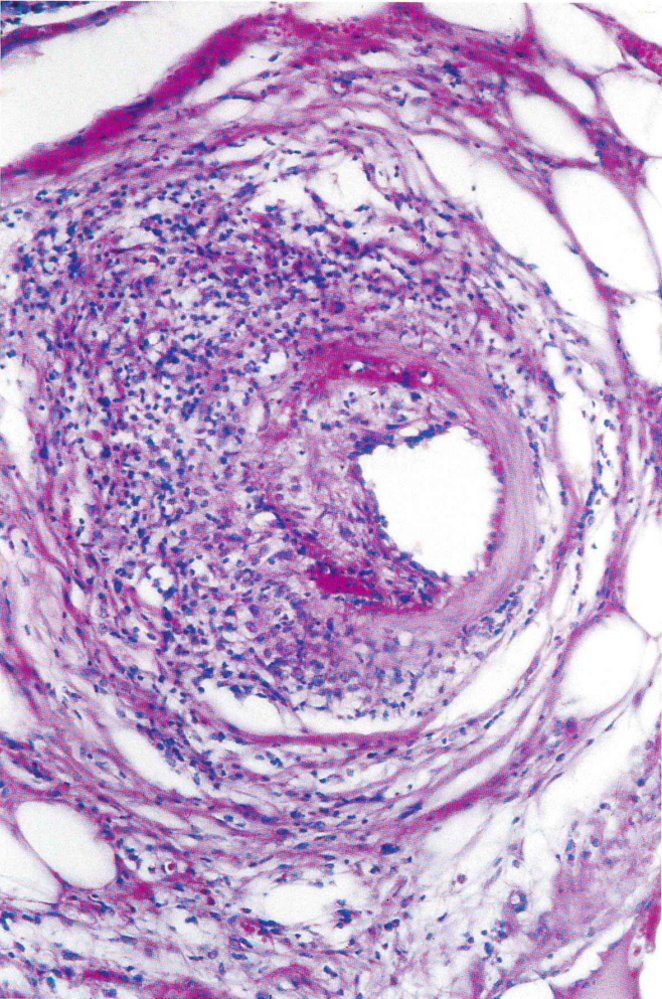
Photomicrograph of a muscle biopsy sample with a medium-sized arterial vessel (H&E stain; low magnification)
There is transmural inflammation of the arterial wall with leukocytic infiltration and fibrinoid necrosis.
These findings are characteristic of polyarteritis nodosa.
Source: © IMPP
Small-vessel vasculitis
ANCA-associated small-vessel vasculitis
| Overview of ANCA-associated small-vessel vasculitides | |||
|---|---|---|---|
| Clinical features | Diagnostics | Management | |
| Granulomatosis with polyangiitis |
|
|
|
| Eosinophilic granulomatosis with polyangiitis |
|
|
|
| Microscopic polyangiitis |
|
|
|
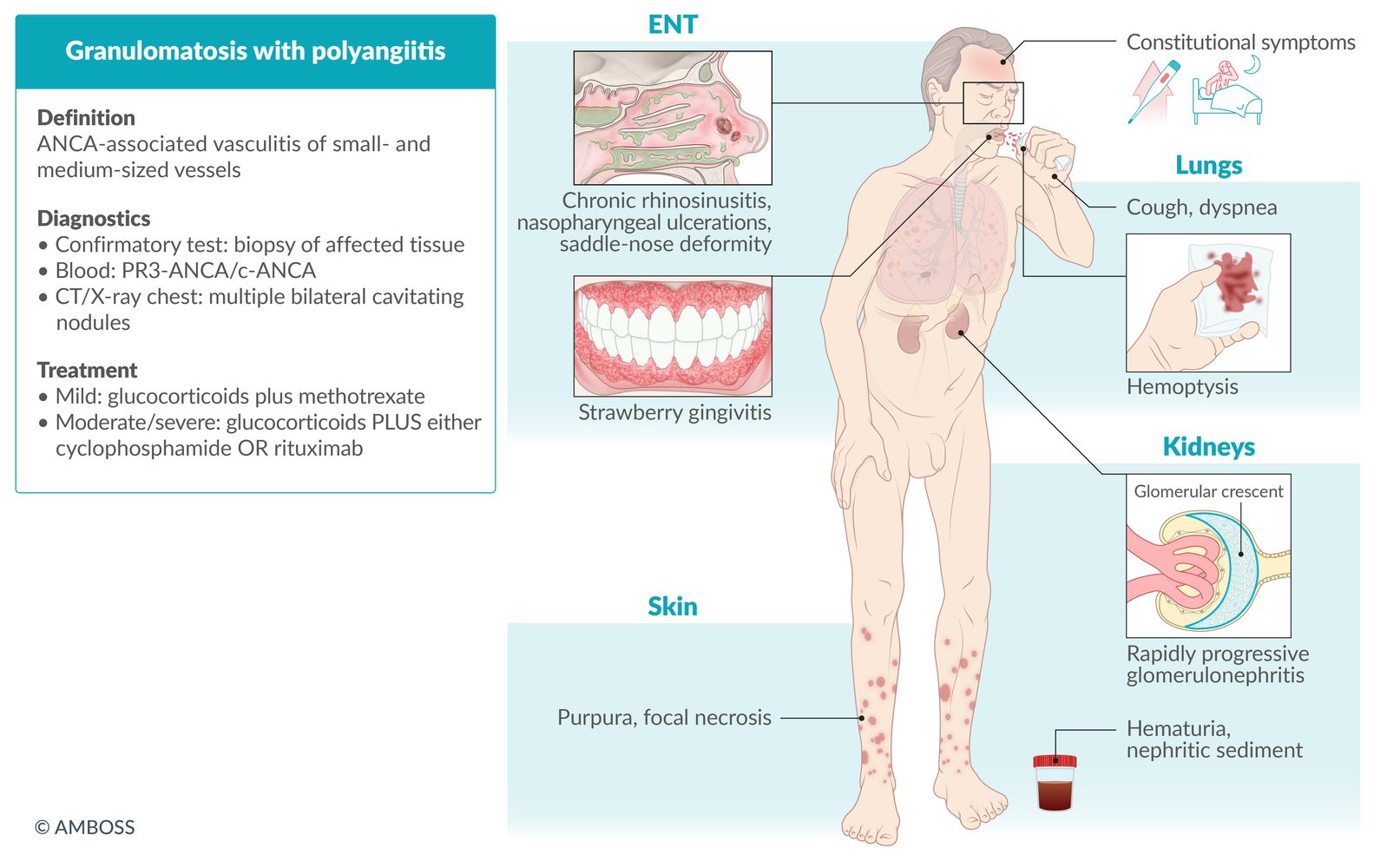
Granulomatosis with polyangiitis is the 'C' disease: Curvy nose (saddle nose deformity), Chronic sinusitis, Cough, Conjunctivitis and Corneal ulceration, Cardiac arrhythmias, non-Caseating granulomas on biopsy, cANCA, Corticosteroids and Cyclophosphamide as treatment.


")


Non-ANCA-associated small-vessel vasculitis
| Overview of non-ANCA-associated small-vessel vasculitides | |||
|---|---|---|---|
| Clinical features | Diagnostics | Management | |
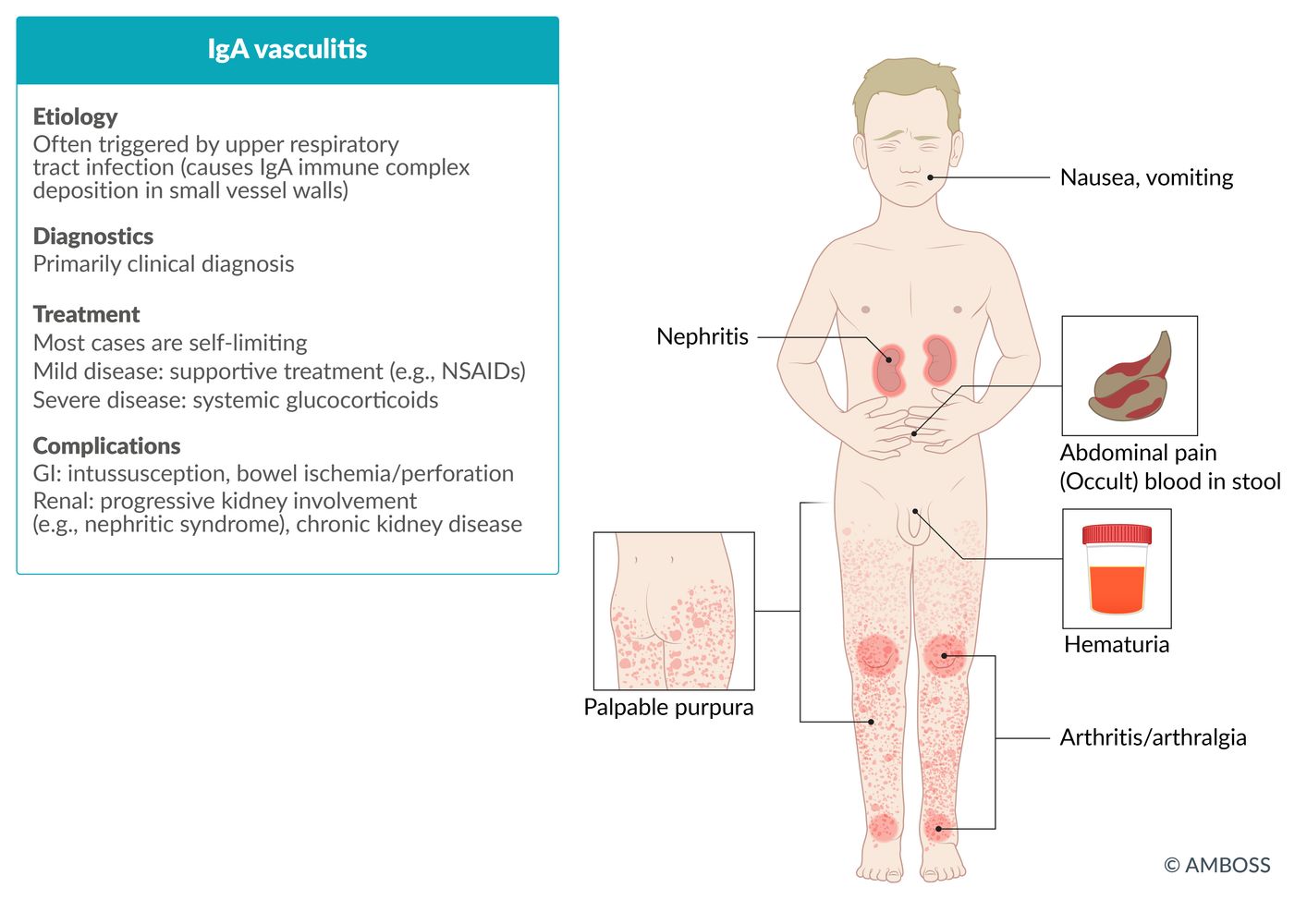
| IgA vasculitis |
|
|
|
| Cryoglobulinemic vasculitis |
|
|
|
| Cutaneous small-vessel vasculitis [7][8] |
|
|
|




© AMBOSS
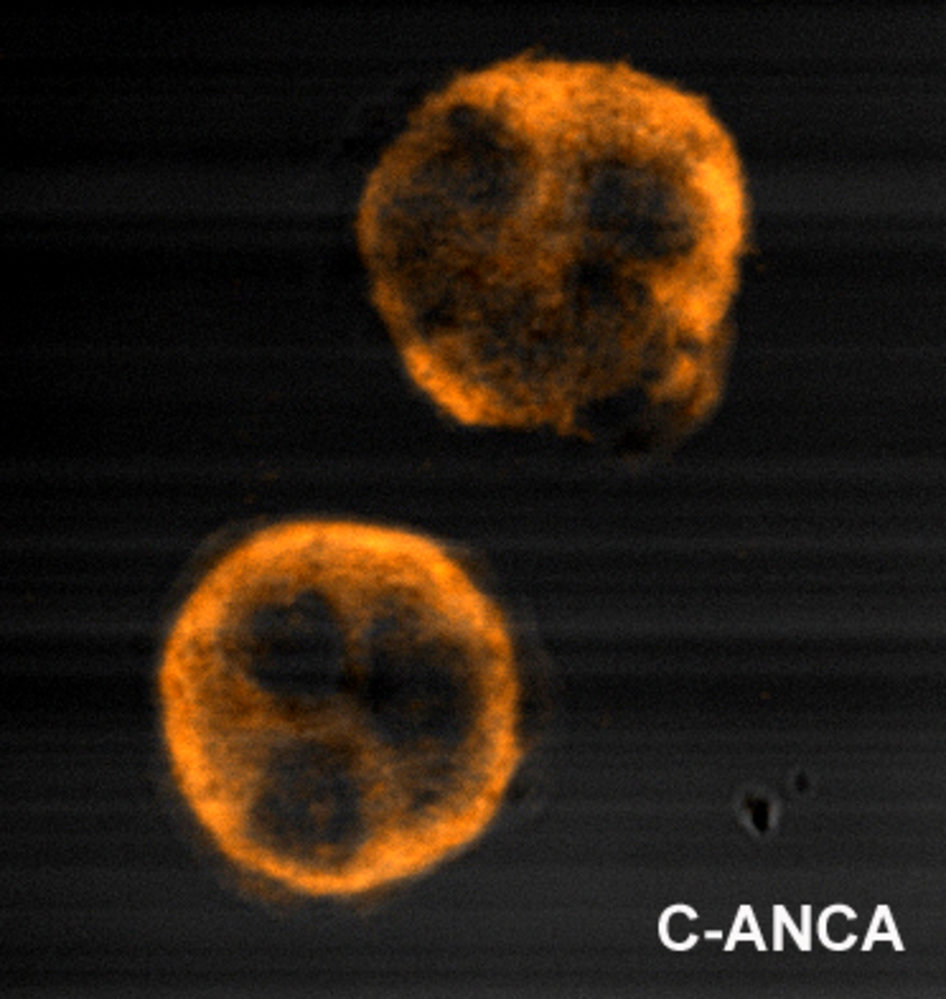
Indirect immunofluorescence of c-ANCA on ethanol-fixed neutrophils (high magnification)
Fluorescently labeled antibodies bind to c-ANCA, forming an extensive, granular pattern of fluorescence within the entire cytoplasm. The unlabeled areas in the center of the neutrophils are the lobulated nuclei. Alternative fluorescence patterns include the perinuclear ANCA (p-ANCA) pattern and the abnormal ANCA (a-ANCA) pattern. Fluorescence patterns are associated with specific antigens and, therefore, the pattern can help determine the underlying disease.
The c-ANCA pattern often suggests the presence of autoantibodies against proteinase 3, which is a characteristic finding in granulomatosis with polyangiitis.
Source: "Immunofluorescence pattern produced by binding of ANCA to ethanol-fixed neutrophils, from a person with GPA", Malittle, Wikimedia licensed under Public Domain
{kind=link}

Photograph of a macroscopic preparation of a lung
Round, solitary and nodular changes (green overlay) with centrally necrotic cavities (arrows) can be recognized in the left lung.
These pathological changes are typically seen in granulomatosis with polyangiitis.
Source: “Wegener's granulomatosis” by Yale Rosen, Flickr, licensed under CC BY-SA 2.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 2.0.
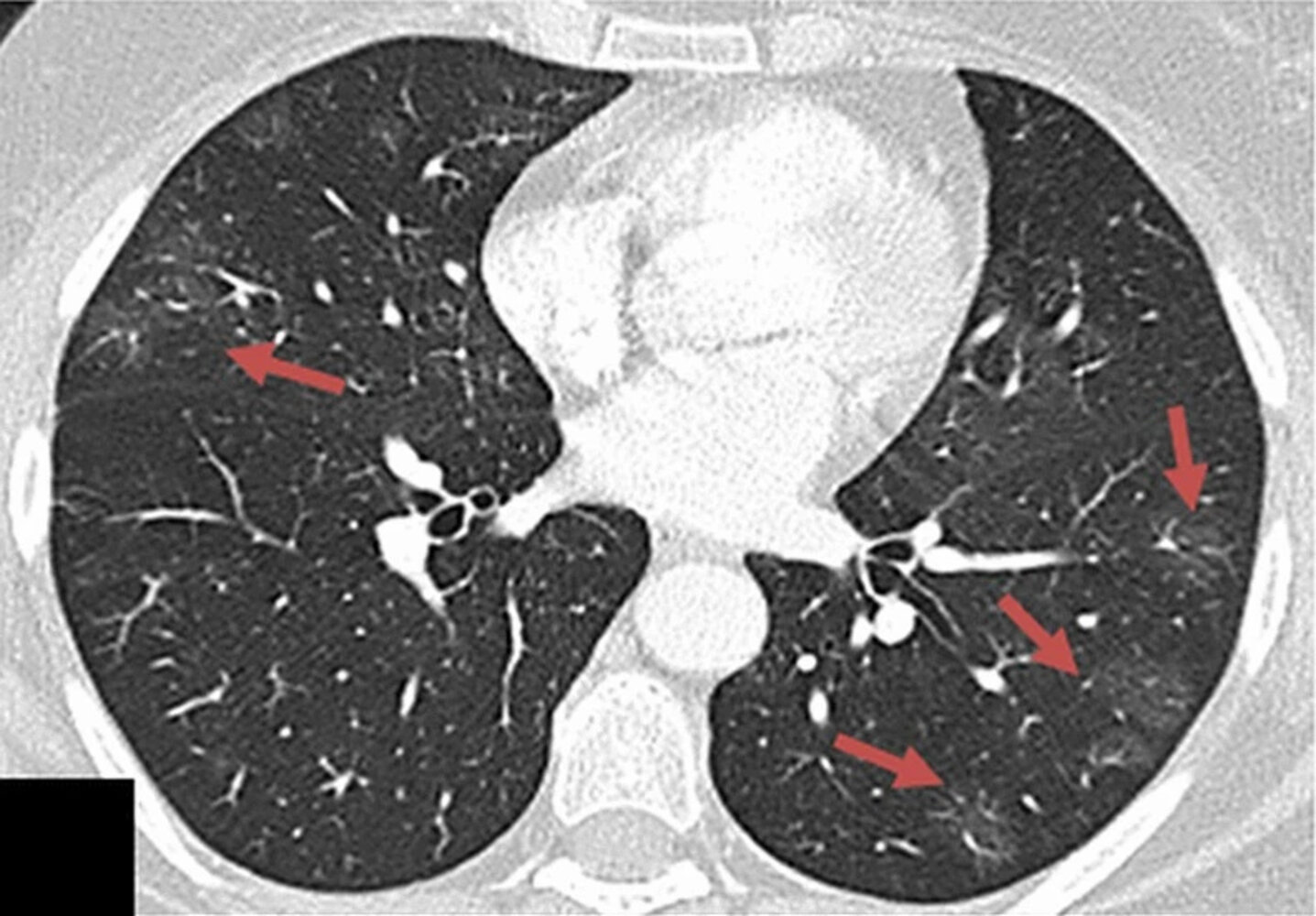
CT chest (high resolution; axial plane; lung window) of a patient with symptoms of asthma and eosinophilia
Scattered ground-glass opacities (examples indicated by red arrows) are present in both lungs, especially in the periphery.
In conjunction with the clinical symptoms, the CT findings are compatible with eosinophilic granulomatosis with polyangiitis (Churg-Strauss syndrome).
Eosinophilic granulomatosis with polyangiitis frequently manifests with peripheral or randomly distributed ground-glass or consolidative opacities. Bronchial wall thickening, septal thickening, and nodules may also be seen.
Source: “Fig. 6C, in: COVID-19 pneumonia: the great radiological mimicker” by Duzgun SA, Durhan G, Demirkazik FB, Akpinar MG, Ariyurek OM, Insights Imaging, licensed under CC BY 4.0. Modifications: Image was cropped.
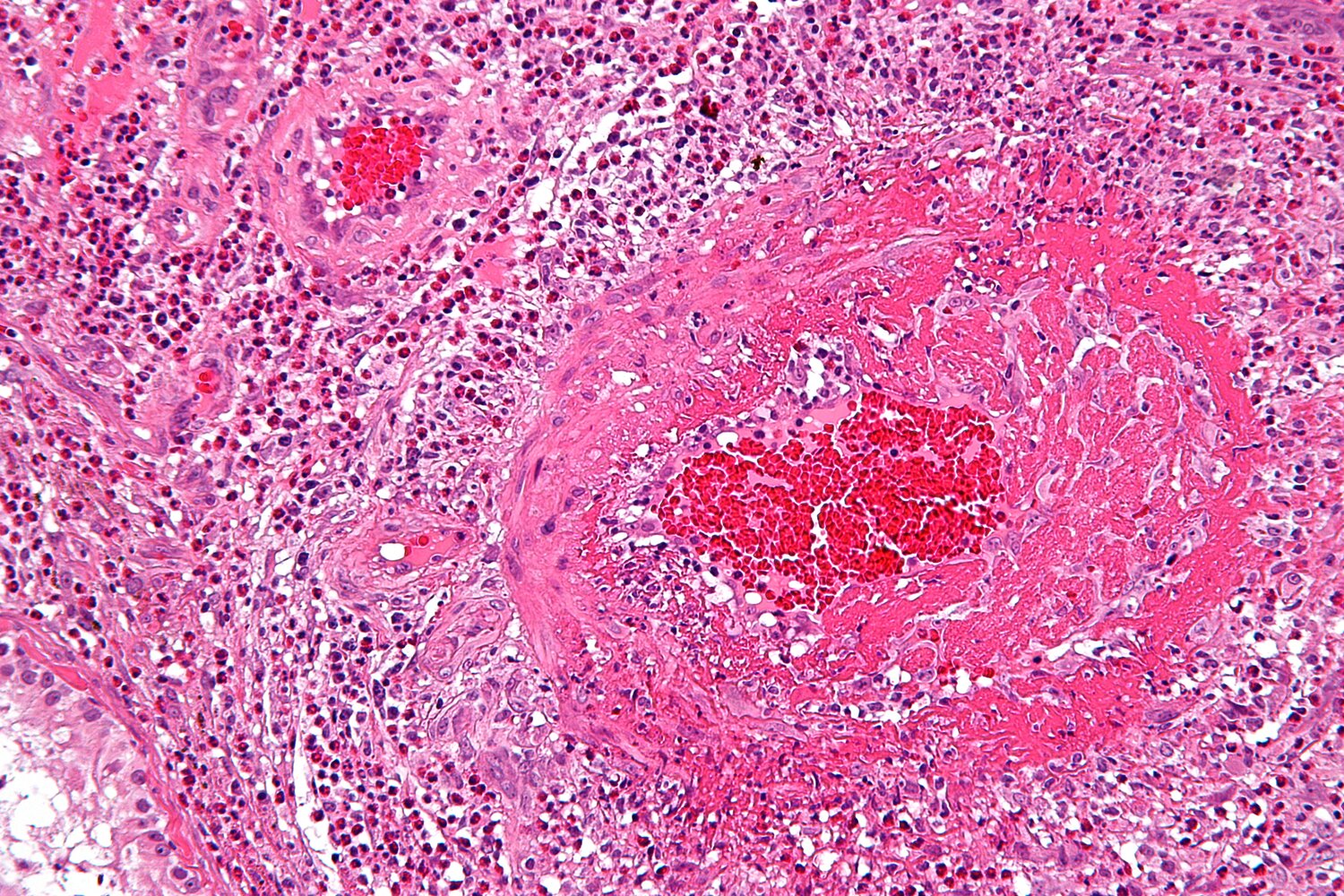
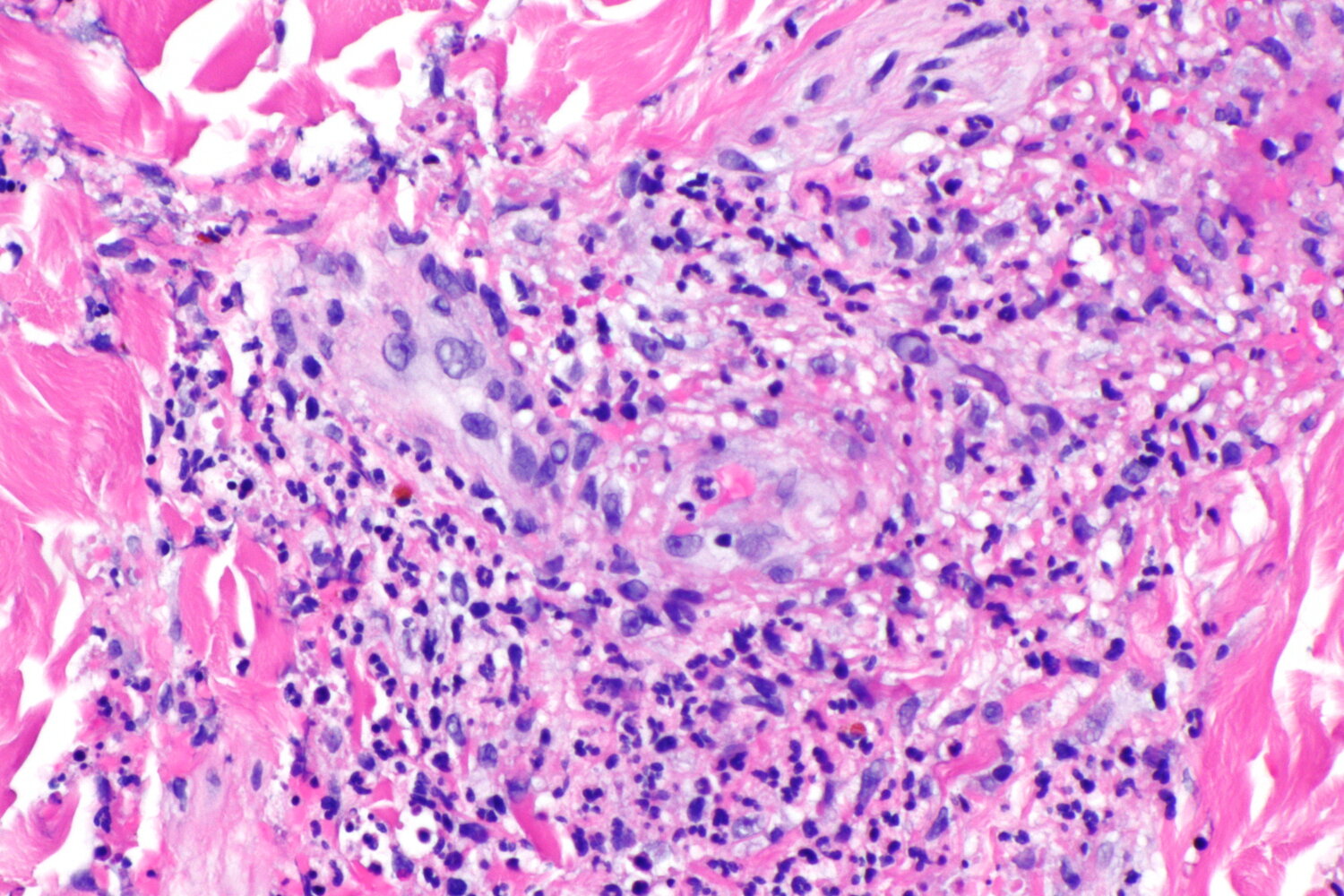
Photomicrograph of eosinophilic vasculitis (H&E stain; high magnification)
Two blood vessels (white outlines) with necrotizing vasculitis with eosinophil infiltration of the media (indicated by arrows in the detail) are visible. Extravascular accumulations of eosinophils cause the characteristic tissue eosinophilia (examples indicated by arrowheads).
These findings are consistent with eosinophilic granulomatosis with polyangiitis.
Source: “Churg-Strauss syndrome - high mag” by Michael Bonert ("Nephron"), Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
© AMBOSS

Maculopapular, reddish, non-blanching, palpable skin lesions (purpura) are seen on both the distal right arm and leg. On the lower leg, the lesions are partially confluent and present with scaling and erosion.
Source: "Purpura2", Okwikikim, Wikimedia Commons licensed under Public Domain
{kind=link}
Photomicrograph of a skin tissue sample (H&E stain; high magnification)
There is focal neutrophilic inflammation (neutrophils indicated by arrowheads) neighboring a small blood vessel (marked by blue line) of the skin with the typical appearance of fragmented neutrophilic nuclei (leukocytoclasia, examples marked by arrows).
These findings are suggestive of small-vessel leukocytoclastic vasculitis (leukocytoclastic vasculitis).
Source: “Leukocytoclastic vasculitis -- high mag.jpg” by Nephron, Libre Pathology, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}

Variable vessel vasculitis
| Overview of variable vessel vasculitides | |||
|---|---|---|---|
| Clinical features | Diagnostics | Management | |
| Behcet disease |
|
|
|
| Cogan syndrome [2][9] |
|
|
|
Differential diagnoses
- Infectious diseases
-
Thrombotic disorders, e.g.:
- Antiphospholipid syndrome
- Thrombotic thrombocytopenic purpura
- Sickle cell disease
- Thromboangiitis obliterans
- Amyloidosis
- Scurvy
- Ergotamines
The differential diagnoses listed here are not exhaustive.
References
- Younger DS. "Overview of the Vasculitides". Neurol Clin. 37(2). :171-200. (2019)
- Espígol-Frigolé G, Prieto-González S, Alba MA, et al. "Advances in the Diagnosis of Large Vessel Vasculitis". Rheumatic Disease Clinics of North America. 41(1). :125-140. (2015)
- Kim ESH, Beckman J. "Takayasu arteritis: challenges in diagnosis and management.". Heart. 104(7). :558-565. (2018)
- Bardi M, Diamantopoulos AP. "EULAR recommendations for the use of imaging in large vessel vasculitis in clinical practice summary". Radiol Med (Torino). 124(10). :965-972. (2019)
- Suresh E. "Diagnostic approach to patients with suspected vasculitis". Postgrad Med J. 82(970). :483-488. (2006)
- Jennette JC, Falk RJ, Bacon PA, et al. "2012 Revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides". Arthritis & Rheumatism. 65(1). :1-11. (2012)
- Micheletti RG, Pagnoux C. "Management of cutaneous vasculitis". Presse Med. 49(3). :104033. (2020)
- Goeser MR, Laniosz V, Wetter DA. "A Practical Approach to the Diagnosis, Evaluation, and Management of Cutaneous Small-Vessel Vasculitis". Am J Clin Dermatol. 15(4). :299-306. (2014)
- A. Greco, A. Gallo, M. Fusconi, et al. "Cogan's syndrome: An autoimmune inner ear disease". Autoimmun Rev. 12(3). :396-400. (2013)