Summary
Vertebral injuries consist of fractures, subluxations, dislocations, and ligamentous injuries with or without consequent nerve root and/or spinal cord injury. They are usually caused by high-energy blunt trauma, but pathological fractures may occur. During the initial evaluation, it is imperative to determine if the injury is stable and whether neurological injury has occurred. Spinal motion restrictions are maintained until these questions are resolved. Clinical decision rules are used to determine whether imaging studies are needed; CT spine is the most common initial diagnostic test. Stable vertebral injuries are often managed conservatively with external spinal immobilization, analgesics, and physical therapy. Most unstable vertebral injuries require surgical immobilization. Expert consultation (e.g., with orthopedics, spine surgery, neurosurgery) is usually necessary to determine definitive management.
The primary focus of this article is the thoracolumbar spine. See “Cervical spine injuries” for details on the cervical spine.
For injuries involving the spinal cord, see “Spinal cord injuries.”
Epidemiology
- Common in older women (osteoporotic fractures) and young men (traumatic injuries) [1]
- Location: ∼ 50% in the cervical spine and ∼ 50% in the thoracic, lumbar, and sacral spine [2]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
Trauma
- Blunt trauma: e.g., motor vehicle crashes (MVCs), falls
- Penetrating trauma: e.g., gunshot wounds
| Vertebral injuries by mechanism [2][3] | |
|---|---|
| Mechanism of injury | Types of vertebral injury |
| Flexion |
|
| Flexion rotation |
|
| Extension |
|
| Shear |
|
| Compression (axial loading) |
|
Atlanto-occipital dislocation can be caused by various injury mechanisms, including flexion, flexion rotation, and extension. [2][3]
Pathological fractures
- Osteoporosis (most common)
- Malignancy (e.g., bone metastases)
- Infection (e.g., Pott disease)
Initial management
The following initial steps apply to all levels of vertebral injury. For further details on cervical spine injuries, see “Initial management of C-spine injury.”
Primary survey [4][5]
- If indicated, manage the airway with manual in-line C-spine stabilization.
- Maintain spinal motion restrictions until unstable vertebral injury is excluded.
- Begin management of urgent concurrent injuries, if present (e.g., TBI management, management of trauma).
- Treat neurogenic shock, if present.
Secondary survey [4][5]
- Palpate the entire spine using log roll.
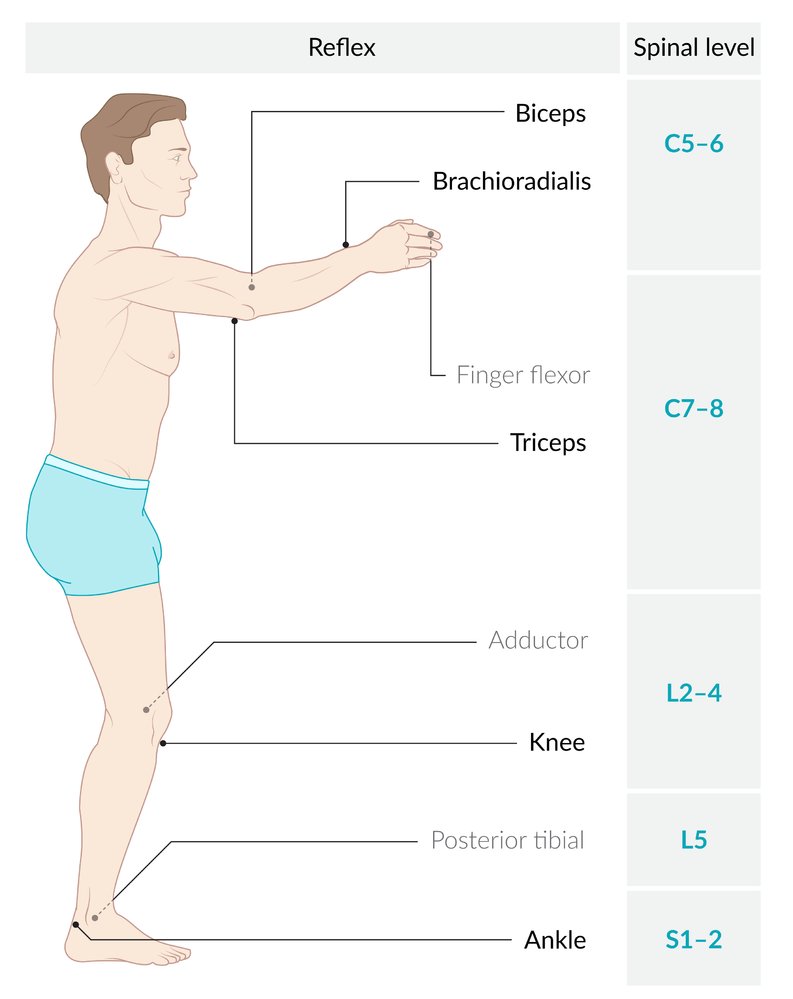
- Perform a focused neurological examination, e.g., segmental motor testing, deep tendon reflexes, identifying sensory level.
- Assess rectal tone on digital rectal examination.
- Begin acute management for spinal cord injury, if suspected.
- Continue management of concurrent injuries.



Initial diagnostics [4][5]
- If applicable, use clinical decision rules to guide decisions on obtaining imaging studies (see “Diagnostics of vertebral injuries” for details).
- When indicated, obtain diagnostics for spinal injuries, e.g., CT spine for adults with blunt trauma.
Urgent consults
- Consult a spine surgeon for known or suspected vertebral or spinal cord injury.
- Consult neurosurgery for concomitant TBI.
- Consult trauma surgery for polytrauma and other multisystem injuries.
For unstable spinal injuries, urgent surgical intervention is typically indicated to minimize the risk of irreversible neurological injury.
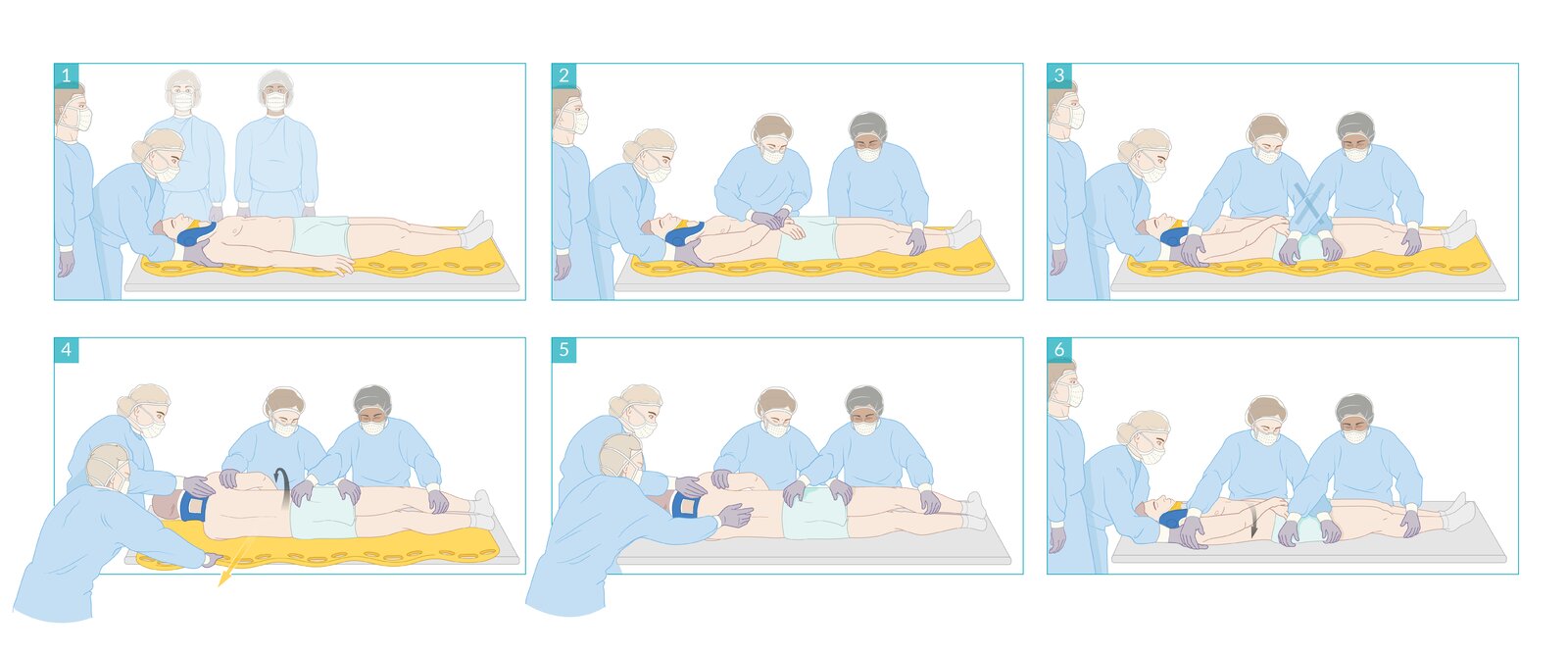
A maneuver used to reposition patients between the supine and lateral decubitus positions while maintaining spinal immobilization. Helpful for posterior body examination, preventing aspiration during emesis, and for transfers (e.g., off stretchers). Requires synchronized movement of multiple trained health providers.
(1) One provider maintains manual in-line cervical stabilization of the patient's head and neck.
(2) Other providers position the patient's limbs securely by crossing their arms over the torso and approximating the legs.
(3) Two providers support the patient's weight evenly by crossing their arms over the patient's pelvis as shown.
(4) In synchrony, all three providers roll the patient into the decubitus position while maintaining full spinal alignment.
(5) The position is maintained by all three providers until the examination and/or intervention is complete.
(6) In synchrony, all three providers roll the patient back into the supine position while maintaining full spinal alignment.
© AMBOSS
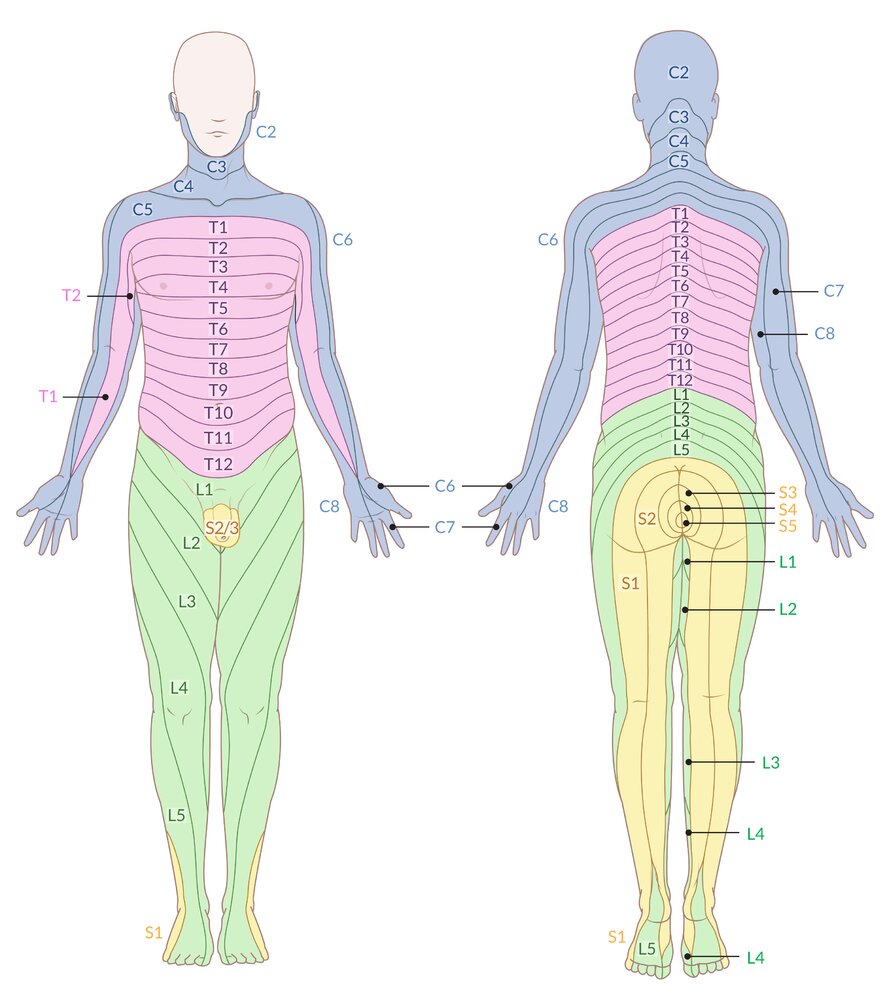
Schematic representation of the body's dermatomes (i.e., areas of skin that are innervated by a single sensory spinal root)
Note: Nearly all dermatome maps refer to publications by Head and Campbell (1900), Foerster (1933), or Keegan and Garrett (1948), which differ significantly in some areas. After careful review of the current literature, this illustration has been based on Keegan and Garrett's work, as it is most likely to be based on valid methodology and correlates with established clinical findings.
© AMBOSS
© AMBOSS
Classification
Vertebral injury stability [3][6][7]
Determining stability typically requires clinical and radiographic assessment of spinal bones, ligaments, and nervous system by a spine specialist. [8]
-
Mechanical instability
- Determined by assessing the integrity of spinal bones and ligaments (especially those of the posterior spinal column)
- If more than one of the following structures are involved, mechanical instability is likely: [6]
- Anterior spinal column
- Middle spinal column
- Posterior spinal column
- Imaging signs of mechanical instability include: [8]
- Significant vertebral body height loss (i.e., > 50%) [8]
- Significant kyphosis (e.g., > 15–35°) [8][9]
- Neurological instability: determined by the ASIA scale
- Mixed instability: a combination of mechanical and neurological instability

Stable vertebral injuries
-
Characteristics
- No risk of displacement, deformity, or progressive neurological injury
- No independently mobile vertebrae or fracture fragments
-
Typical examples
- Vertebral fractures limited to the anterior spinal column, e.g., anterior wedge fractures
- Isolated transverse process fractures
- Isolated spinous process fractures (e.g., Clay-shoveler fracture)
- Isolated laminar or articular processes fractures (e.g., spondylolysis)
- Unilateral cervical facet dislocation [10]
Unstable vertebral injuries
-
Characteristics
- At risk of displacement, deformity, and progressive neurological injury
- Independently mobile vertebrae or fracture fragments
-
Typical examples
-
Vertebral fractures involving the posterior spinal column, e.g.:
- Most burst fractures (including Jefferson fracture)
- Other severe compression fractures
- Flexion-distraction injuries
- Vertebral fracture-dislocations
- Flexion teardrop fracture
- Atlanto-occipital dislocation [11]
- Bilateral cervical facet dislocation [10]
- Type II odontoid fractures [12][13]
-
Vertebral fractures involving the posterior spinal column, e.g.:
AO Spine classification [14][15][16]
AO Spine Upper Cervical Injury Classification System [14][17]
-
Class
- Class I: occipital condyle and craniocervical junction injuries
- Class II: C1 ring and C1–2 joint injuries
- Class III: C2 and C2–3 joint injuries
-
Type
- Type A: bone injury only
- Type B: ligament injury with or without bone injury but with anatomical integrity intact
- Type C: significant translation of spine, loss of anatomical integrity
AO Spine Subaxial and Thoracolumbar Injury Classification Systems [15][16]
This is a simplified version; additional subclassification is based on fracture characteristics, neurological complications, and patient modifiers. [18][19]
- Class A: compression injuries of the vertebral body without ligament damage
- Class B: distraction injuries of the anterior tension band or the posterior tension band
- Class C: displacement or translational injury




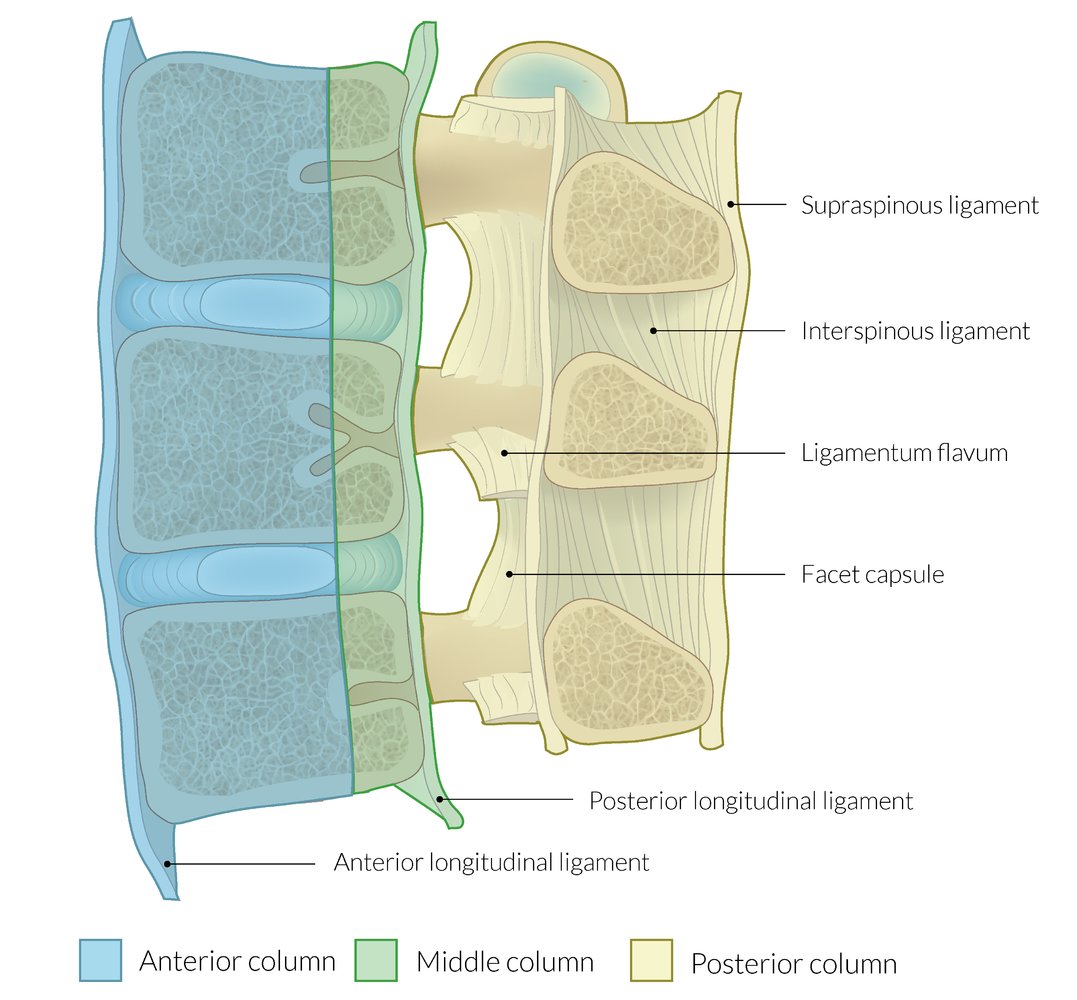
Anterior column = anterior longitudinal ligament, anterior ⅔ of the vertebral body, and anterior ⅔ of the intervertebral disc
Middle column = posterior longitudinal ligament, posterior ⅓ of the vertebral body, and posterior ⅓ of the intervertebral disc
Posterior column = all structures dorsal to the posterior longitudinal ligament
A thoracolumbar injury that simultaneously affects ≥ 2 columns is an unstable injury.
© AMBOSS
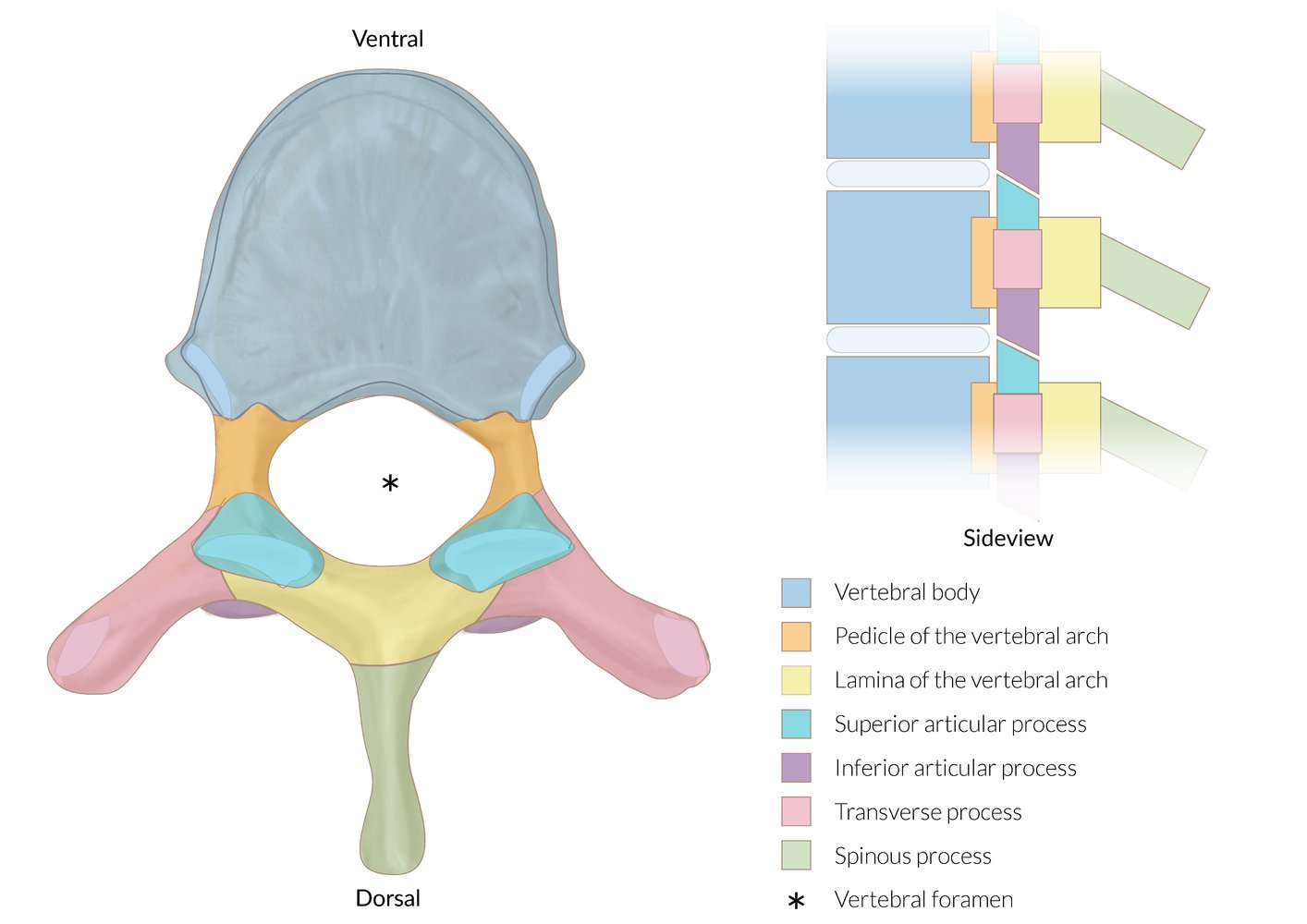
The most important vertebral structures are illustrated here by way of a lumbar vertebra.
© AMBOSS
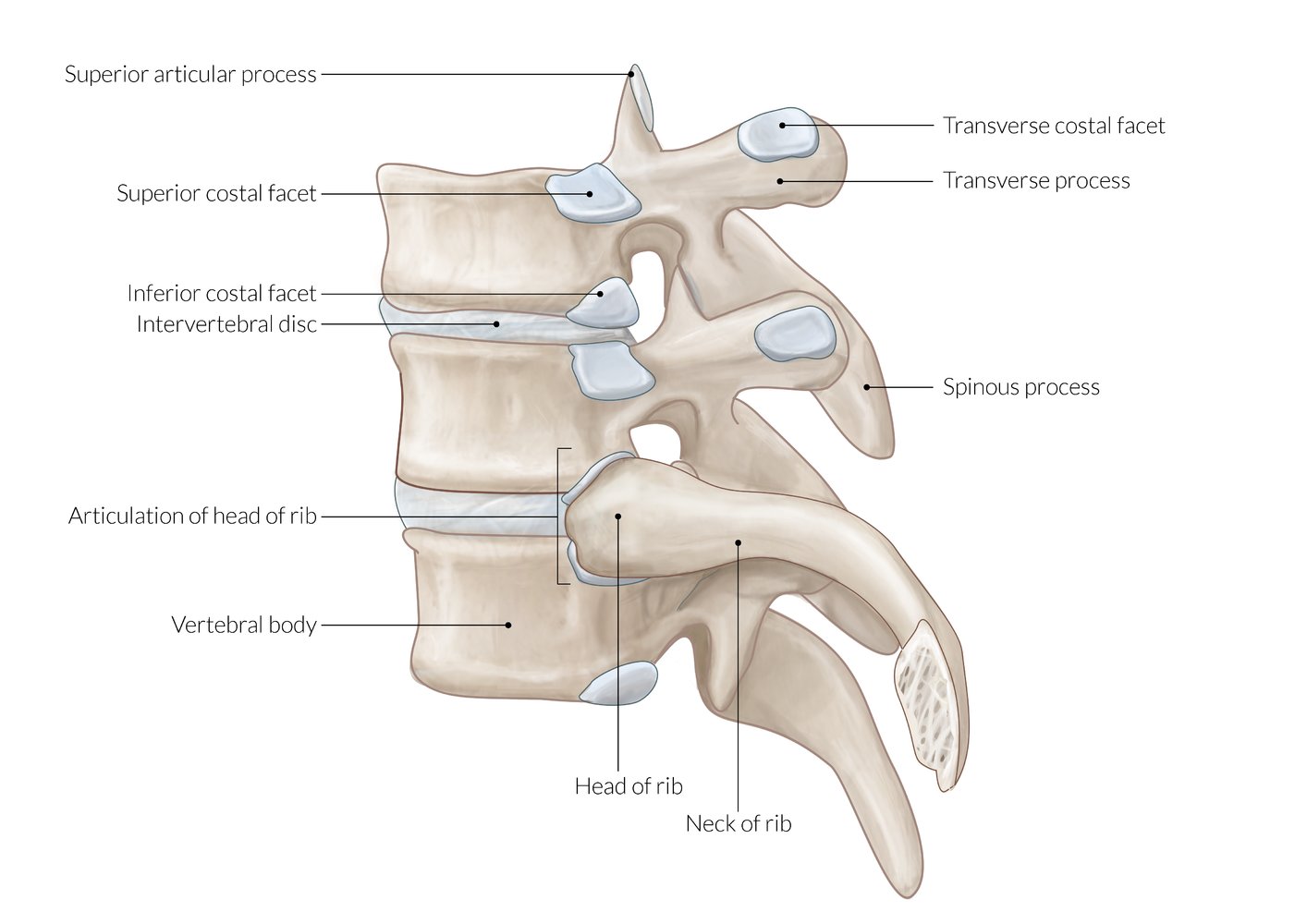
Lateral view
© AMBOSS
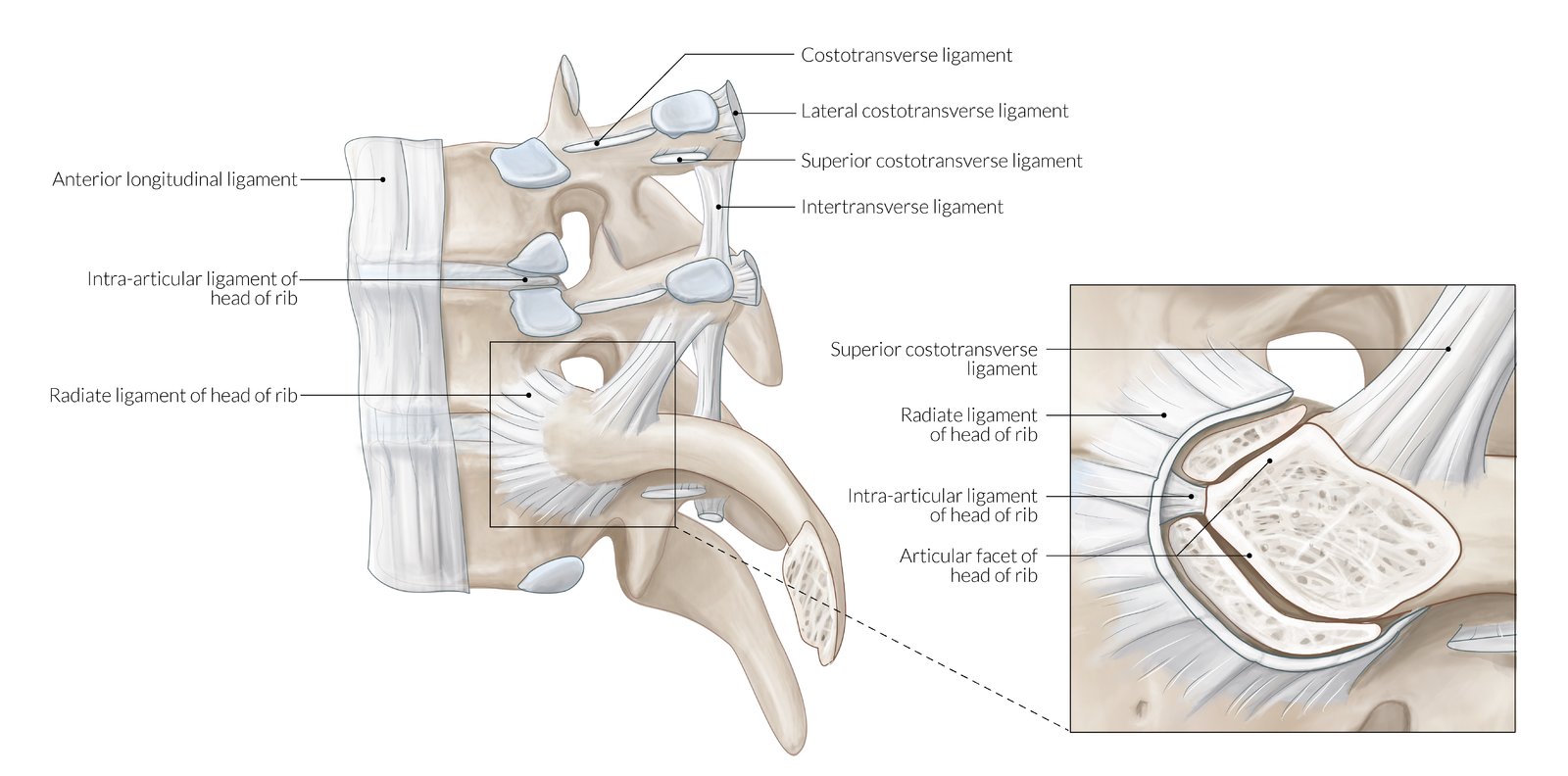
Lateral view
© AMBOSS

Click on the overlay icon below the taskbar on the left to toggle the overlay on and off.
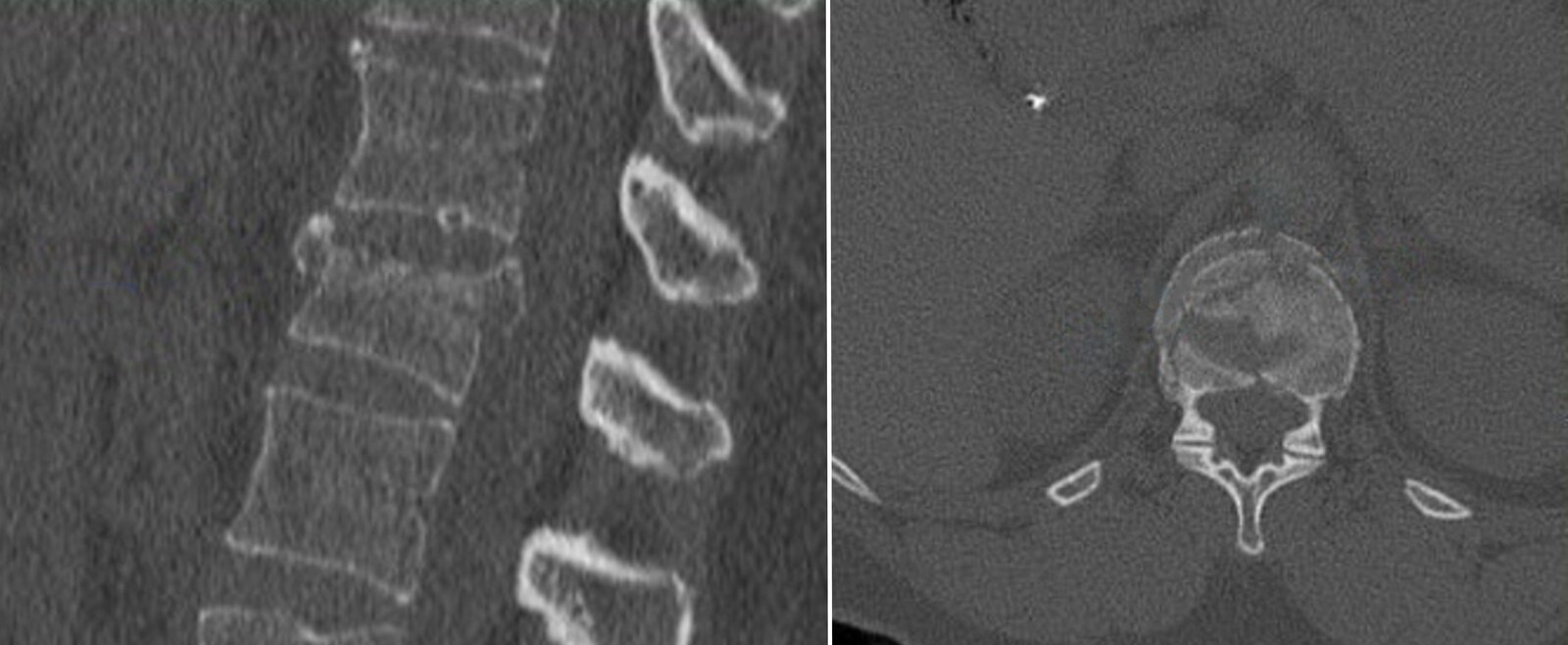
CT thoracic spine (T10–L2; bone window (axial plane, coronal plane, sagittal plane); 3D reformation) of a patient with history of a hyperflexion injury
Anterior wedging and compression of the superior endplate of the T12 vertebral body is accompanied by fractures thorugh the anterior and lateral cortices (green overlay). No retropulsed bone fragments are seen and the posterior elements appear intact.
Schmorl nodes are identified at the inferior endplates of T11, T12, and L1.
Created by: Markus Le Blanc. Organization providing image: Radiologie Frechen-Erftstadt.
Clinical features
-
Vertebral injury
- Localized pain
- Tenderness with pressure, percussion, and/or compression
- Palpable unevenness or disruption of vertebral process alignment
- Paravertebral hematoma
- Kyphosis (secondary to ventral vertebral compression)
-
Neurological injury: clinical features of spinal cord injury and/or nerve root injuries
- Paralysis, weakness, numbness, paresthesias, and/or abnormal proprioception
- Hyperreflexia and/or hyporeflexia
- Urinary retention or urinary incontinence
- Spinal shock
- Concomitant traumatic injuries: e.g., traumatic pneumothorax, traumatic hemothorax, blunt abdominopelvic trauma, blunt cerebrovascular injury (BCVI)
Diagnosis
Approach [4][20][21]
See “Diagnostics for cervical spine injuries” for details on C-spine injuries.
-
Indications for imaging
- C-spine: See ”NEXUS criteria” and “Canadian C-Spine Rule.”
- T- and L-spine: See ”Indications for T- and L-spine imaging.”
-
First-line study (if indicated)
- Children: x-rays of the spine
- Adults with blunt trauma: CT spine
- Adults with penetrating trauma: CTA or MRA of neck, thorax, and/or abdomen
Do not delay urgent interventions (e.g., intubation, fluid resuscitation) to obtain spine imaging in patients with hemodynamic or respiratory instability.
Following blunt trauma, use clinical decision rules to determine the need for C-spine imaging and avoid unnecessary radiation exposure. [22]
X-rays of the spine [4][20]
- Not routinely recommended in adults, often the initial study in children [4][20][23]
- Views
- Thoracolumbar and sacral spine: anteroposterior (AP) and lateral
- C-spine: AP, lateral, swimmer's view, and odontoid view [24]
- See also “C-spine X-rays” and “C-spine x-rays in children.”



CT imaging [4][21]
-
CT spine without IV contrast
- Initial imaging study of choice after blunt trauma in adults
- Obtain CT imaging of the whole spine if an injury at any level of the spine is identified. [21]
- CTA head and neck: in patients meeting the expanded Denver screening criteria for BCVI



MRI spine [4][21]
-
General principles
- Typically used as an adjunct to CT spine
-
Highest sensitivity for soft tissue injuries of the spine
- Neurological: spinal cord injuries or nerve root injuries
- MSK: disc or ligamentous injuries
-
Indications
- Soft tissue injury suggested by clinical or CT findings
- Discordant clinical and CT findings [4]
- Concern for unstable vertebral injuries [4][21]
-
Patients with altered mental status, negative CT, and grossly intact motor function: not routinely indicated [4][21][25][26]
- Follow local protocols.
- See “C-spine clearance” for further details.


X-ray cervical spine (lateral view)
The C1–C6 vertebrae are properly aligned, and the vertebral body and disc space heights are normal, but C7 is not sufficiently visualized through the superimposed shoulders.
To complete the evaluation of the cervical spine, a swimmer's view or CT scan could be performed to completely visualize the C7 vertebra and its articulation with T1.
Blue line: anterior vertebral line; green line: posterior spinous line; red line: posterior vertebral line; yellow line: spinolaminar line
Source: © IMPP

X-ray lumbar spine (lateral view)
There is a chronic compression deformity (red dimension line) of the L4 vertebral body, with displacement (red overlay) toward the spinal canal beyond the posterior vertebral lines of L3 and L5 (white dotted line). Exuberant anterior osteophyte formation is visible at L3–4 (red dotted lines).
Source: © IMPP

X-ray lumbar spine (lateral view)
There is marked compression of the L3 vertebral body (green overlay). Additional radiographic findings include diffuse osteopenia, multiple endplate compression deformities (examples indicated by dashed lines), and extensive atherosclerotic calcification of the abdominal aorta (A) and iliac arteries.
Our great thanks to Dr. Kissig (Center for Diagnostic and Interventional Radiology, Hedwigshöhe, St. Hedwig, Berlin, and St. Josefs Hospital, Potsdam) for kindly providing this image. Further notes: -mirrored
CT thoracic spine (T12 level; left: sagittal plane; right: axial plane; bone window)
A compression fracture of the superior endplate (red overlay and lines) is accompanied by cortical disruption and retropulsion (arrow) into the spinal canal.
Burst fractures result from high-energy axial compression forces accompanied by varying degrees of flexion and/or rotation. They can be stable or unstable fractures.
Source: “Figures 1 and 2, in: A Smart Technique to Remove Ruptured Inflatable Bone Tamp From the Vertebral Body in Balloon Kyphoplasty” by Papaioannou I , Mousafeiris VK, Pantazidou G, Repantis T, Korovessis P, Cureus, licensed under CC BY 4.0. Modifications: images combined and cropped, arrows removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
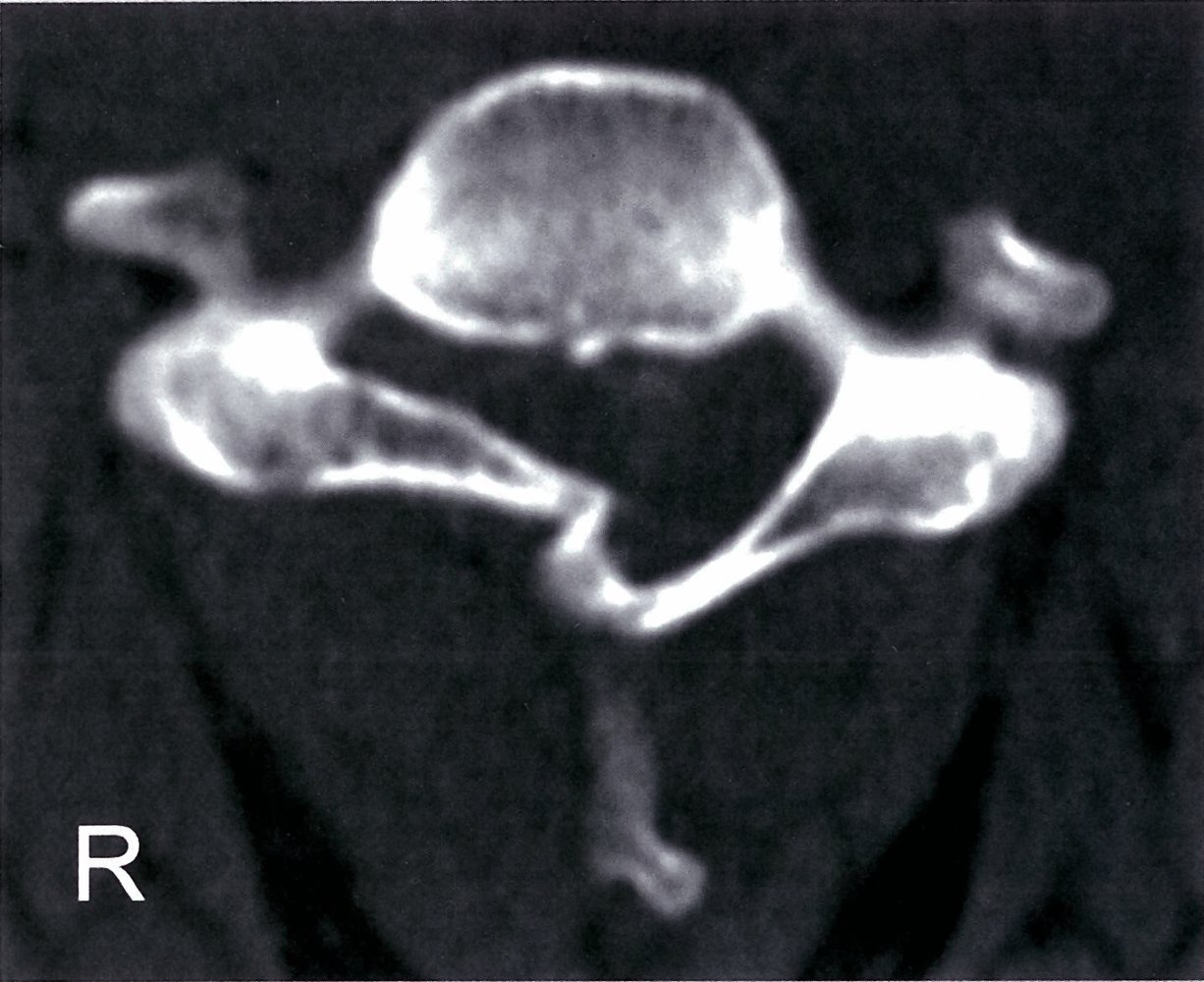
CT cervical spine (bone window; axial plane)
There is a fracture deformity of the right vertebral arch (green overlay) with depression causing narrowing of the spinal canal.
Source: © IMPP
Click on the overlay icon below the taskbar on the left to toggle the overlay on and off.
CT thoracic spine (T10–L2; bone window (axial plane, coronal plane, sagittal plane); 3D reformation) of a patient with history of a hyperflexion injury
Anterior wedging and compression of the superior endplate of the T12 vertebral body is accompanied by fractures thorugh the anterior and lateral cortices (green overlay). No retropulsed bone fragments are seen and the posterior elements appear intact.
Schmorl nodes are identified at the inferior endplates of T11, T12, and L1.
Created by: Markus Le Blanc. Organization providing image: Radiologie Frechen-Erftstadt.

CT lumbar spine (sagittal plane)
There is a T12 burst fracture (red overlay) with retropulsion of fragments into the spinal canal and a dorsal L1 fracture with extension into the T12–L1 disc space (green overlay).
S: sacrum
Source: © IMPP

MRI lumbar spine (left: STIR image; right: T1-weighted; sagittal plane)
Compression deformities of the T8, T10, and L4 vertebrae (green overlays) are visible. The T8 and T10 fractures are hyperintense on the STIR image, indicating that they are recent. The compressed superior endplate of L4 is iso- to hypointense, indicating an old or chronic deformity. The hypointense appearance of the L2–3 intervertebral disc (green circle) on the STIR image indicates disc degeneration.
Source: © IMPP
Differential diagnoses
- See “Back pain.”
- See “Weakness and paralysis.”
The differential diagnoses listed here are not exhaustive.
Management
See also “Initial management of vertebral injuries.”
General principles
- Definitive treatment should be guided by a spine surgeon and depends on: [4]
- Injury characteristics
- Degree of neurological involvement
- Patient factors
- For cervical spine injuries, see “Definitive management of C-spine injuries.”
Conservative management [4][27][28]
- Indications: : typically used for stable vertebral injuries
-
Measures:
- Acute pain management
- External immobilization (orthotic bracing): e.g., halo vest, rigid cervical collar, thoracolumbar brace [4][29]
- Physiotherapy [29]
Surgical management
-
Surgical immobilization (spondylodesis) [27][28][30]
- Indications: unstable vertebral injury; or neurological injury
- Technique [30]
- Decompression of neural elements
- Realignment of the spine
- Fusion of two or more vertebral bodies via internal fixation to stabilize the spine
- Minimally invasive procedures: See “Vertebral augmentation” for compression fractures.



Disposition [3]
- Patients with identified fractures and/or unstable ligamentous injuries are usually admitted.
- Patients with only soft tissue injuries may be discharged with analgesics and return precautions.
- Perform fall risk assessment for all falls in older adults.
- Consider discharge and follow-up in consultation with a spine specialist for patients with all of the following:
- Minor uncomplicated fractures
- Adequate symptom control
- Minimal functional impairment
- Low risk of complications

X-ray cervical spine (AP view)
Anterior monosegmental spondylodesis has been performed at the C6–C7 level (blue overlay).
A typical anatomical arrangement is shown, in which the transverse process of C7 (white dashed line) angles inferiorly and the transverse process of T1 (black dashed line) angles superiorly.
Source: © IMPP

X-ray cervical spine (lateral view)
Anterior monosegmental spondylodesis has been performed at the C6–C7 level.
Arrow: tip of the spinous process of the vertebra prominens (C7); Blue overlay: fusion plate and screws
Source: © IMPP
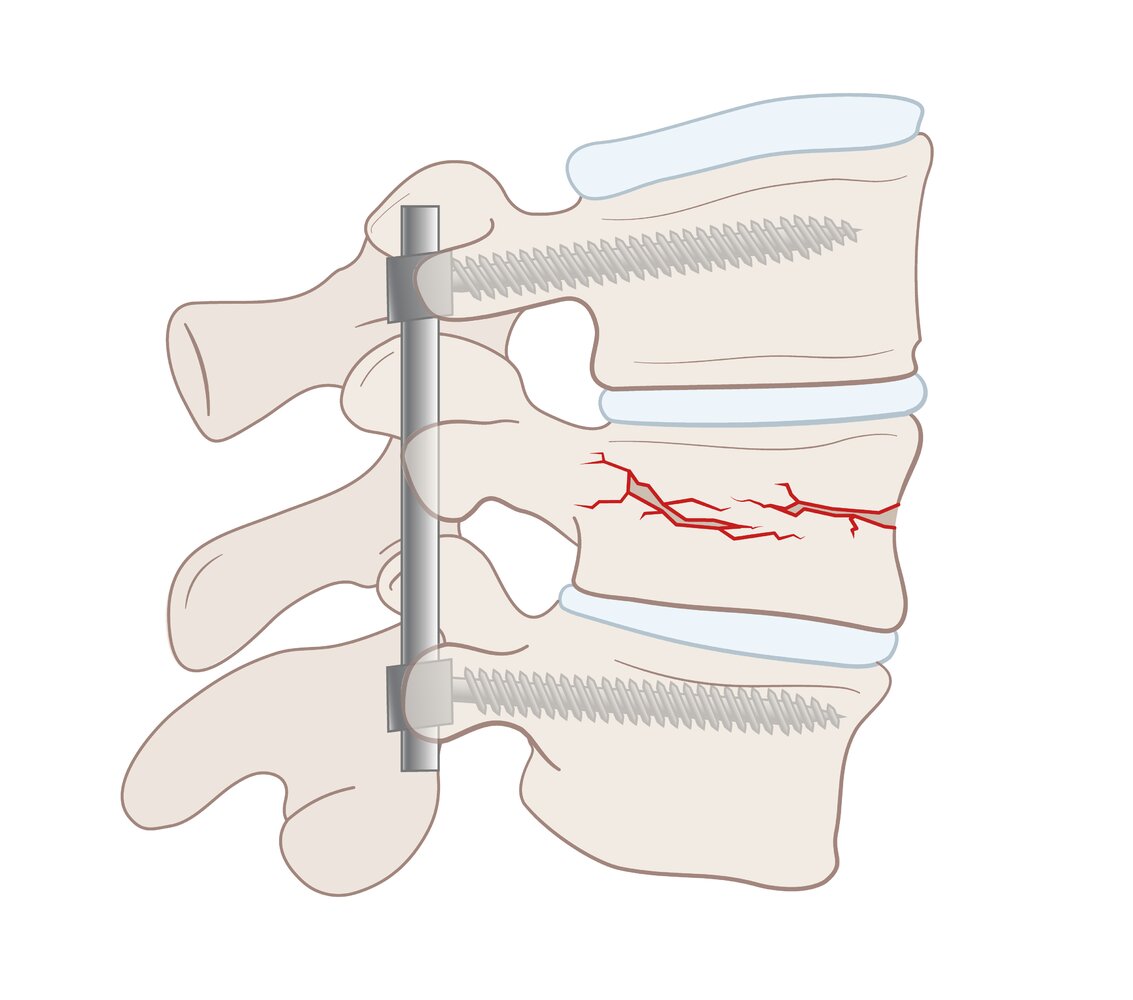
Internal fixation is a method of immobilizing a fracture using devices (e.g., screws, rods, plates, etc.) that are placed completely inside the body (in contrast to external fixation, in which the devices are secured outside the skin).
© AMBOSS
Cervical spine injuries
See “Cervical spine injuries” for information on the following:
Upper cervical spine injuries
- Occipital condyle fractures
- Atlanto-occipital dislocation
- Atlantoaxial dislocation
- Atlas (C1) fractures (including Jefferson fracture)
- Axis (C2) fractures (including odontoid process fracture, hangman's fracture, and extension teardrop fracture)
Lower cervical spine injuries
- Flexion teardrop fracture
- Clay-shoveler fracture
- Cervical facet dislocation
Thoracic and lumbar spine injuries
Diagnostics
-
Indications for imaging the thoracic and/or lumbar spine [31][32][33]
- Thoracolumbar pain or tenderness
- Neurological deficits
- Multiple concurrent or distracting injuries
- Glasgow coma scale score < 15 or intoxication
- Cervical spine fracture [21]
- Other: head injury, age > 60 years, high-risk injury mechanism [34]
- Imaging: typically CT spine, see “Diagnostics of vertebral injuries” for details
Management [28][35][36]
-
Initial management
- See “Initial management of vertebral injuries.”
- Identify and treat concomitant life- or limb-threatening injuries.
- Injuries at or below L1: conus medullaris syndrome or cauda equina syndrome
- T-spine injuries: blunt chest trauma, e.g., rib fractures, pneumothorax, cardiac contusion
- L-spine injuries: blunt abdominopelvic trauma, e.g., intraabdominal hemorrhage, splenic injury, diaphragmatic injury
- Any penetrating thoracic trauma or penetrating abdominal trauma
-
Definitive management: depends on injury stability and score based on the AO Spine classification
- Stable vertebral injuries without neurological deficits: conservative treatment with external orthosis (optional), early mobilization, and close follow-up [28]
- Unstable vertebral injuries and/or spinal cord injury: Surgical immobilization is usually required.
Vertebral compression fracture
Background
- Definition: collapse of the vertebral body with ≥ 20% reduction in its height [37][38]
-
Epidemiology [39]
- Most common in adults > 65 years old, especially those with osteoporosis
- ♀ > ♂
- Mechanism: usually caused by axial loading with flexion
-
Morphology
- Wedge fracture: Collapse is most prominent in the anterior vertebral body. [38]
- Vertebra plana: severe compression fracture with uniform loss of height across the vertebral body [40]
- Codfish vertebra: biconcave vertebral body [41]

Etiology
- Pathological fractures: e.g., due to osteoporosis (most common cause) or bone metastasis
- Trauma
Risk factors [37]
- Osteopenia or osteoporosis
- Older age
- Female sex
- History of inactivity, falls, or prior vertebral compression fractures
- Chronic systemic corticosteroid use
- Low body weight
- Alcohol consumption and/or smoking
- Vitamin D deficiency
Red flags for malignancy-related compression fractures [42]
- Fracture without trauma in individuals aged < 50 years
- History of malignancy
- Weight loss
- Persistent pain
Clinical features [37][42][43]
- Often asymptomatic [37]
-
Pain
- Midline and localized to a spinal segment (bandlike)
- Sudden onset after minor trigger, e.g., sneezing, coughing, turning in bed
- Exacerbated by rotation, movement, standing
- Localized midline tenderness
- Thoracic kyphosis and lumbar lordosis
- Loss of height [38]
- See also “Clinical features of vertebral fractures.”
Diagnostics [42][44]
-
X-ray spine (AP and lateral views)
- Usual initial study
- Typically shows wedge-shaped vertebral body with loss of height
-
CT spine or MRI spine
- Indicated for new and/or symptomatic compression fractures
- MRI spine is often chosen to discriminate between osteoporosis and a neoplastic etiology.
- Dual-energy x-ray absorptiometry: indicated for bone mineral density assessment in patients with suspected fragility fractures
Management [44][45][46]
Approach [29][37][42]
- All patients: Begin initial management of vertebral injuries.
- Unstable vertebral injuries and/or neurological impairment: typically require spondylodesis
- Stable vertebral injuries: usually conservative management, vertebral augmentation in select cases
- Burst fractures: usually unstable (see “Vertebral burst fractures”)
-
Osteoporotic fractures
- 3-month trial of conservative management for most patients
- Vertebral augmentation for severe symptoms or significant deformity
- Underlying radiosensitive malignancy: radiotherapy
Compression fractures involving only the anterior spinal column (most common) are usually stable. [29]
Conservative management [29]
-
Acute pain management
- NSAIDs or acetaminophen: first-line [47]
- Opioids: limited second-line use at minimal effective doses to avoid opioid adverse effects.
- Other: antidepressants, calcitonin, bisphosphonates, teriparatide [29]
- Orthotic bracing [29]
- Physical therapy [29][48]
- Treatment of osteoporosis: e.g., bisphosphonates for osteoporosis
Consult a spine specialist if symptoms do not resolve within 4–8 weeks. [39][44]
Vertebral augmentation [29][46][49]
-
Indications
- Progressive pain or kyphosis despite conservative treatment
- Acute compression fracture with severe pain and/or functional limitation
- Acute compression fracture with significant kyphosis and/or loss of vertebral body height
-
Procedures
- Vertebroplasty: percutaneous injection of bone cement into the fractured vertebra
- Kyphoplasty: reexpansion of vertebral body with an inflatable balloon followed by injection of bone cement
Compression fractures are the most common type of vertebral fracture. Most are stable vertebral injuries and can be managed conservatively. [42]




Complications [37][42][43]
- Loss of mobility
- Reduced lung function
- Decreased appetite and early satiety
- Chronic pain
- Reduced quality of life
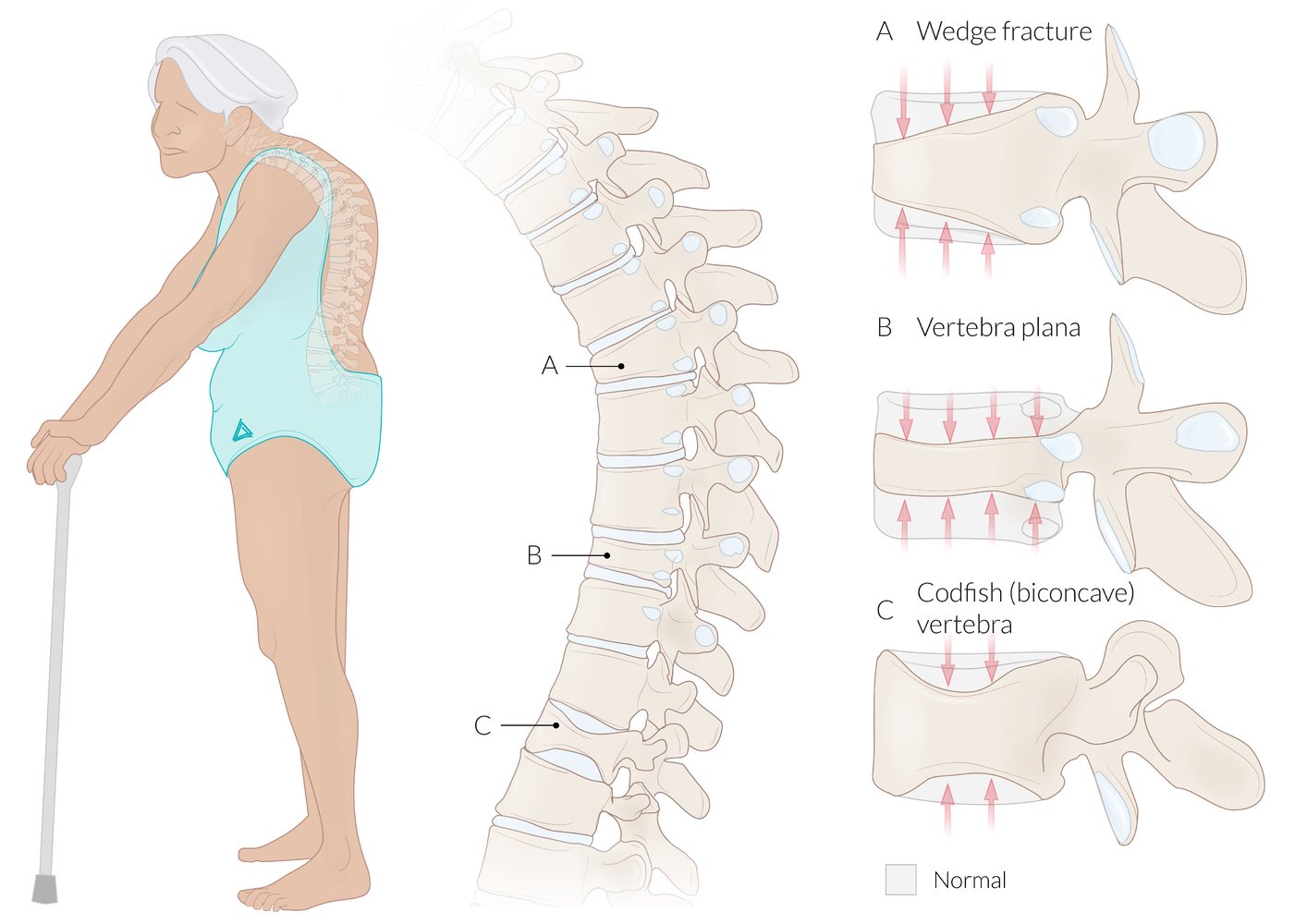
(A) Wedge fracture: characterized by a loss of height, predominantly of the anterior part of the vertebral body. Wedge fractures are common in individuals with osteoporosis, and they can lead to a kyphotic deformity of the spine (gibbus) if multiple vertebrae are involved.
(B) Vertebra plana: an advanced compression fracture where there is a loss of height of the entire vertebral body, both anteriorly and posteriorly. Vertebra plana is also referred to as a pancake or coin-on-edge vertebra.
(C) Codfish vertebra: characterized by loss of height of the central part of the vertebral body, resulting in a biconcave vertebral body that resembles fish vertebrae.
© AMBOSS
Click on the overlay icon below the taskbar on the left to toggle the overlay on and off.
CT thoracic spine (T10–L2; bone window (axial plane, coronal plane, sagittal plane); 3D reformation) of a patient with history of a hyperflexion injury
Anterior wedging and compression of the superior endplate of the T12 vertebral body is accompanied by fractures thorugh the anterior and lateral cortices (green overlay). No retropulsed bone fragments are seen and the posterior elements appear intact.
Schmorl nodes are identified at the inferior endplates of T11, T12, and L1.
Created by: Markus Le Blanc. Organization providing image: Radiologie Frechen-Erftstadt.
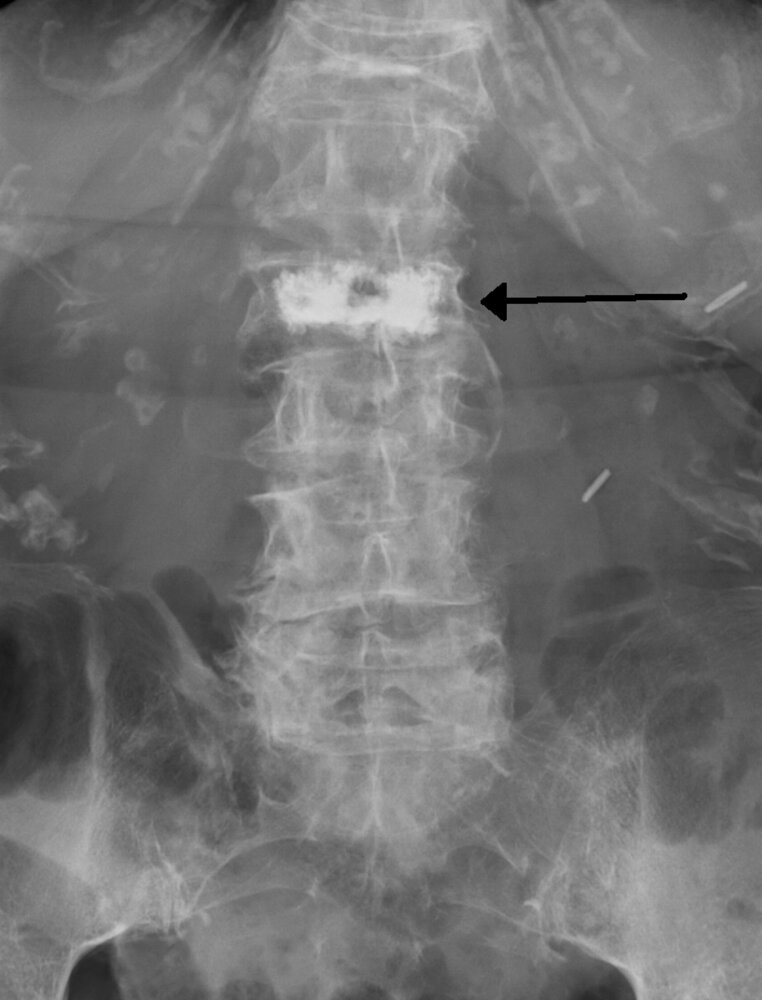
X-ray of the lumbar spine (AP view; post-vertebroplasty)
There is a compression fracture of the L2 vertebral body, which has been treated with vertebroplasty. The injected bone cement is identifiable as increased radiopacity within the vertebral body of L2 (black arrow). There is no evidence of leakage of bone cement injected during the procedure.
Source: “VertcementX” by James Heilman, MD, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}
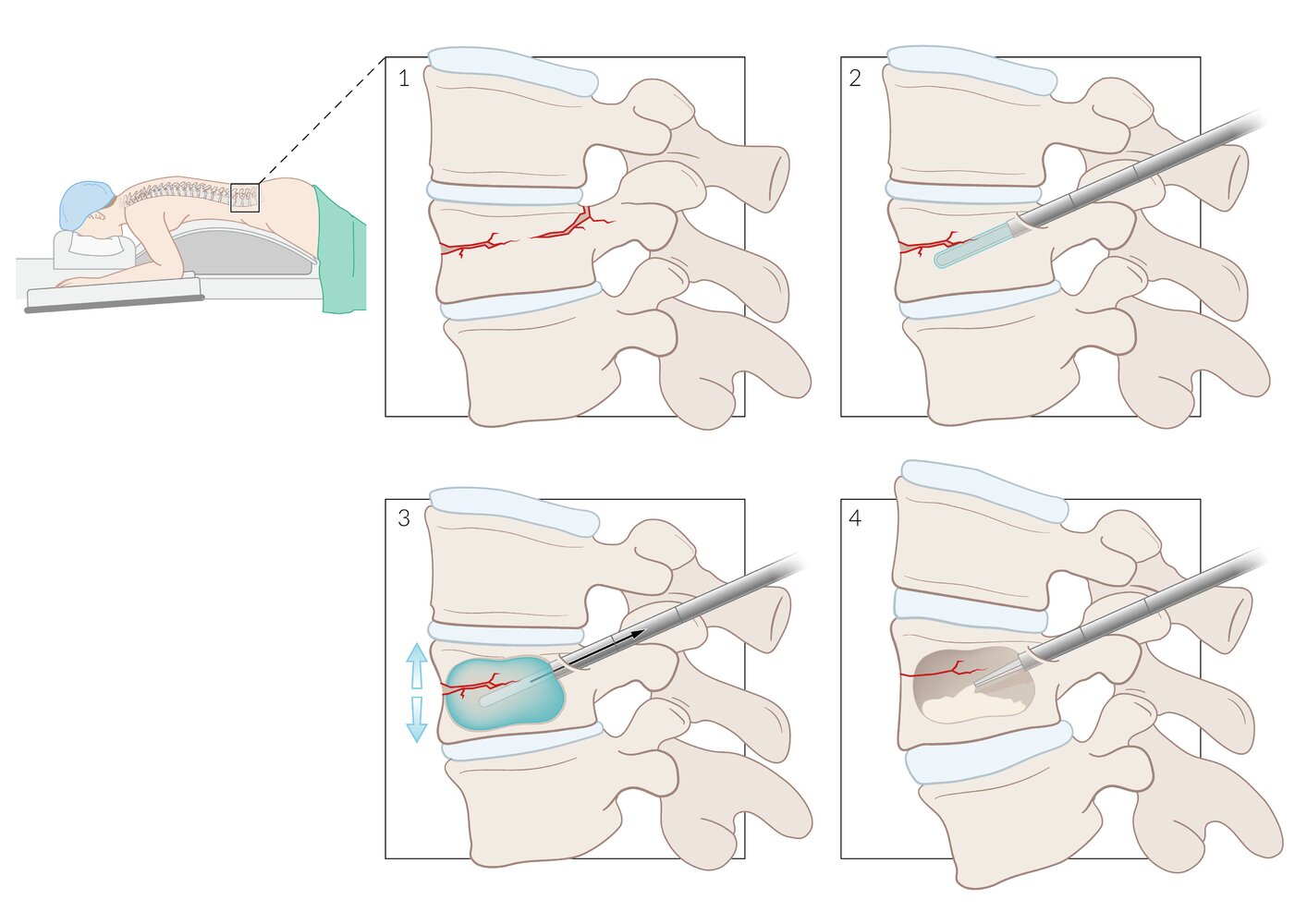
Kyphoplasty is indicated in stable vertebral compression fractures (1) with progressive pain or kyphosis despite conservative treatment.
Procedure:
2) A trochar with an inflatable balloon is inserted into the vertebral body.
3) The balloon is inflated, expanding the vertebral body.
4) The hollow space created is filled with bone cement.
© AMBOSS

X-ray thoracic spine (lateral view; left: pre-intervention; right: post-intervention) of postmenopausal patient with osteoporosis
Thoracic vertebral body compression deformities (left) are present in the setting of diffuse osteopenia. Following vertebral augmentation, high-density cement is visible at three levels (right).
Wedge compression of the middle augmented vertebra (right) was not present on the initial radiograph.
Blue lines: cobb angles
Source: © IMPP
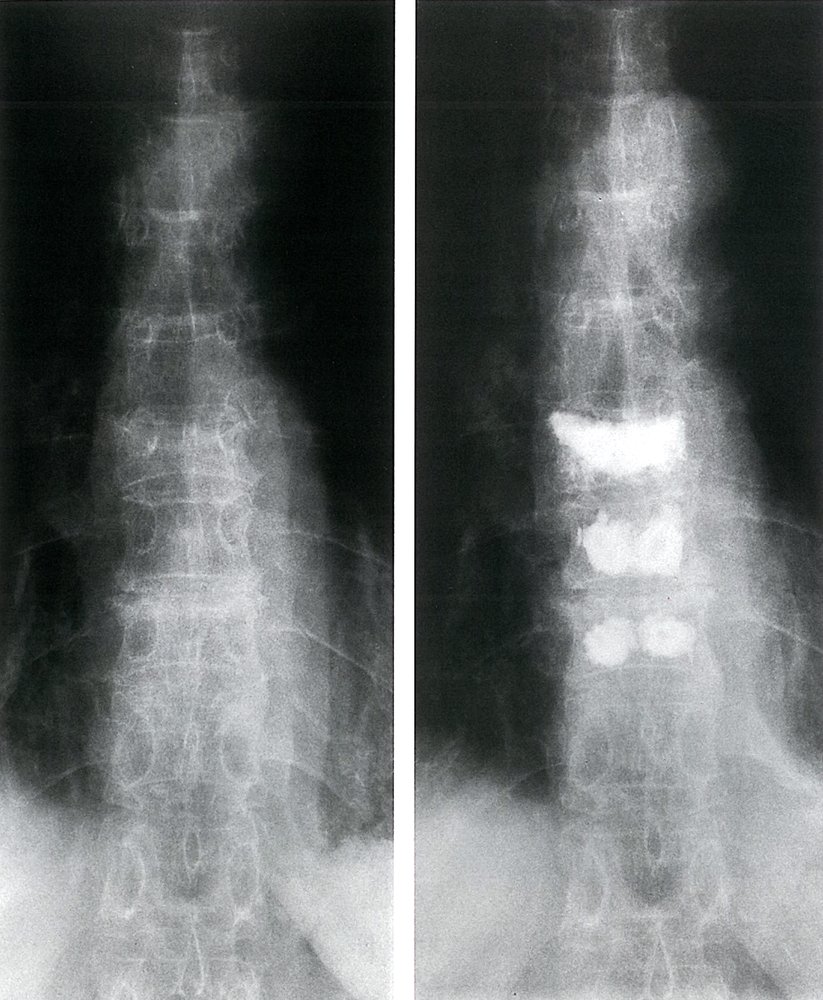
X-ray thoracic spine (AP view; left: before kyphoplasty; right: after kyphoplasty) of a 65-year-old woman
Osteoporotic vertebral body fractures (red overlay and outlines) are present on the radiograph performed prior to kyphoplasty. A T9 compression deformity is not conspicuous on the initial radiograph. Following kyphoplasty, the T8, T9, and T10 vertebrae show opaque (white) areas representing the bone cement (polymethyl methacrylate) injected during the procedure.
Source: © IMPP
Vertebral burst fracture
For cervical burst fractures, see “Jefferson fracture.”
-
Description [50][51][52]
- A type of vertebral compression fracture with displacement of a posterior segment of the vertebral body (middle spinal column) into the spinal canal
- Commonly caused by severe axial loading injuries that disrupt the anterior spinal column and middle spinal column, e.g., MVCs, high-energy falls, sports injuries, and combat injuries
-
Clinical features
- See “Clinical features of vertebral fractures.”
- Clinical features of spinal cord injury are common.
-
Diagnosis: See “Diagnostics of vertebral injuries.” [50][51][52]
- Most occur between T10 and L2, primarily at the thoracolumbar junction.
- Findings include:
- Anterior wedging of the vertebral body
- Increased distance between the vertebral pedicles
- Retropulsion of the posterior vertebral body with narrowing of the spinal canal
-
Management [8][50][53][54]
- Initial management: See “Initial management of vertebral injuries.”
- Definitive management
- Neurologically intact and stable vertebral injury (e.g., kyphosis ≤ 35°): conservative management
- Neurological deficit or unstable vertebral injury (e.g., kyphosis > 35°): surgical management (e.g., spondylodesis)
Burst fractures often involve the posterior spinal column as well as the middle spinal column, making them more likely to be unstable vertebral injuries. [50][53]
CT thoracic spine (T12 level; left: sagittal plane; right: axial plane; bone window)
A compression fracture of the superior endplate (red overlay and lines) is accompanied by cortical disruption and retropulsion (arrow) into the spinal canal.
Burst fractures result from high-energy axial compression forces accompanied by varying degrees of flexion and/or rotation. They can be stable or unstable fractures.
Source: “Figures 1 and 2, in: A Smart Technique to Remove Ruptured Inflatable Bone Tamp From the Vertebral Body in Balloon Kyphoplasty” by Papaioannou I , Mousafeiris VK, Pantazidou G, Repantis T, Korovessis P, Cureus, licensed under CC BY 4.0. Modifications: images combined and cropped, arrows removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Flexion distraction injuries
-
Description [3][55]
- An unstable vertebral injury involving the middle spinal column and posterior spinal column
- Caused by forceful spinal flexion against a stabilized vertebral segment, e.g., seatbelt restraint in an MVC [55]
- Chance fracture: a type of flexion-distraction injury characterized by fracture of the posterior vertebral body, spinous process, and/or pedicles with or without posterior ligamentous complex injury
-
Clinical features: See “Clinical features of vertebral fractures.” [55]
- Kyphosis
- Seatbelt abrasions on the abdomen
- Clinical features of common concurrent injuries, e.g., blunt abdominal trauma, spinal cord injury
-
Diagnosis: See “Diagnostics of vertebral injuries.” [3][55]Management [55]
- Begin initial management of vertebral injuries.
- Manage concurrent blunt abdominal trauma.
- Consult spine surgery for surgical stabilization.
- Most occur at the thoracolumbar junction between T11 and L1.
- The following bony structures can be distracted, burst, or compressed on imaging (e.g., CT spine):
- Spinous process
- Vertebral laminae
- Transverse processes
- Vertebral pedicles
- Vertebral body
- Ligamentous injury (e.g., to the posterior ligament complex) may be seen on MRI.
Obtain abdominal imaging and consider trauma surgery consultation in patients with flexion-distraction injuries. [55]


Chest X-ray (lateral view)
Two fractured vertebral bodies (T9 and T10, green overlay) as a result of the seatbelt during a motor vehicle collision are visible. The posterior edges of the affected vertebral bodies (red outlines, showing multiple interruptions) are involved as well.
This is the typical appearance of a Chance fracture.
Source: “PchancefracCT” by James Heilman, MD, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
Isolated transverse process fracture
- Definition: fracture of the transverse process in the absence of fractures in other parts of the involved vertebra [56]
- Mechanism: avulsion fracture caused by high-energy blunt trauma [56][57]
-
Clinical features [56][57]
- Localized pain
- Clinical features of vertebral fractures from concomitant vertebral injuries
- Signs of associated injuries (common)
- Cervical: head injury, brachial plexopathy, and/or BCVI
- Thoracolumbar: blunt chest injuries and/or blunt abdominopelvic trauma
-
Diagnosis: See “Diagnostics of vertebral injuries.” [56][57]
- Can affect any spinal level, frequently occurs at multiple levels concomitantly
- X-ray spine: often identified on lateral view
- CT spine: more sensitive than x-ray for detection of transverse process fractures
- CTA neck: for fractures extending into the transverse foramina or signs of vertebral artery dissection
-
Management: conservative management [56][57]
- Early mobilization and physical therapy
- Analgesics
- Bracing and orthotics are not routinely recommended.
Isolated transverse process fractures are typically stable vertebral injuries.
Other vertebral injuries
Vertebral fracture-dislocation
- Ligament disruption and displacement of a vertebra and/or vertebral fragments
- Typically an unstable vertebral injury that requires surgical fixation
Vertebral facet dislocation
- Typically occur in the C-spine (see “Cervical facet dislocation”)
-
Facet joint dislocations of the thoracolumbar spine are rare. [58][59]
- Consult spine surgery as they may be unstable vertebral injuries.
- Can be associated with flexion-distraction injuries
Complications
-
Spinal cord injury
- Severe injury of the spinal cord → respiratory depression
- Spinal contusion/concussion to spinal shock → neurological deficits
- Injuries of the cervical spine may result in a retropharyngeal hematoma → dysphagia.
- Vessel injury: dissection or thrombotic blockage of the vertebral artery
- Posttraumatic deformation of the spine: loss of height, scoliosis, or kyphosis
-
Gibbus
- A hump or kyphotic deformity in the spine (usually thoracolumbar spine)
- Common causes include vertebral fracture and spondylodiscitis (especially Pott's disease).

")




 with gibbus deformity")
We list the most important complications. The selection is not exhaustive.

Back of a child with tuberculous spondylitis (Pott disease)
There is kyphosis of the upper thoracic spine showing the characteristically sharp angulation of a gibbus deformity (red arrow).
Gibbus deformities can result from infections, metabolic diseases, and congenital diseases.
Source: “Figure 130, in: Atlas of Paediatric HIV Infection” by Oladokun RE; Lehloenya RJ; Hlela C; et al, Openbooks, licensed under CC BY-ND 4.0.
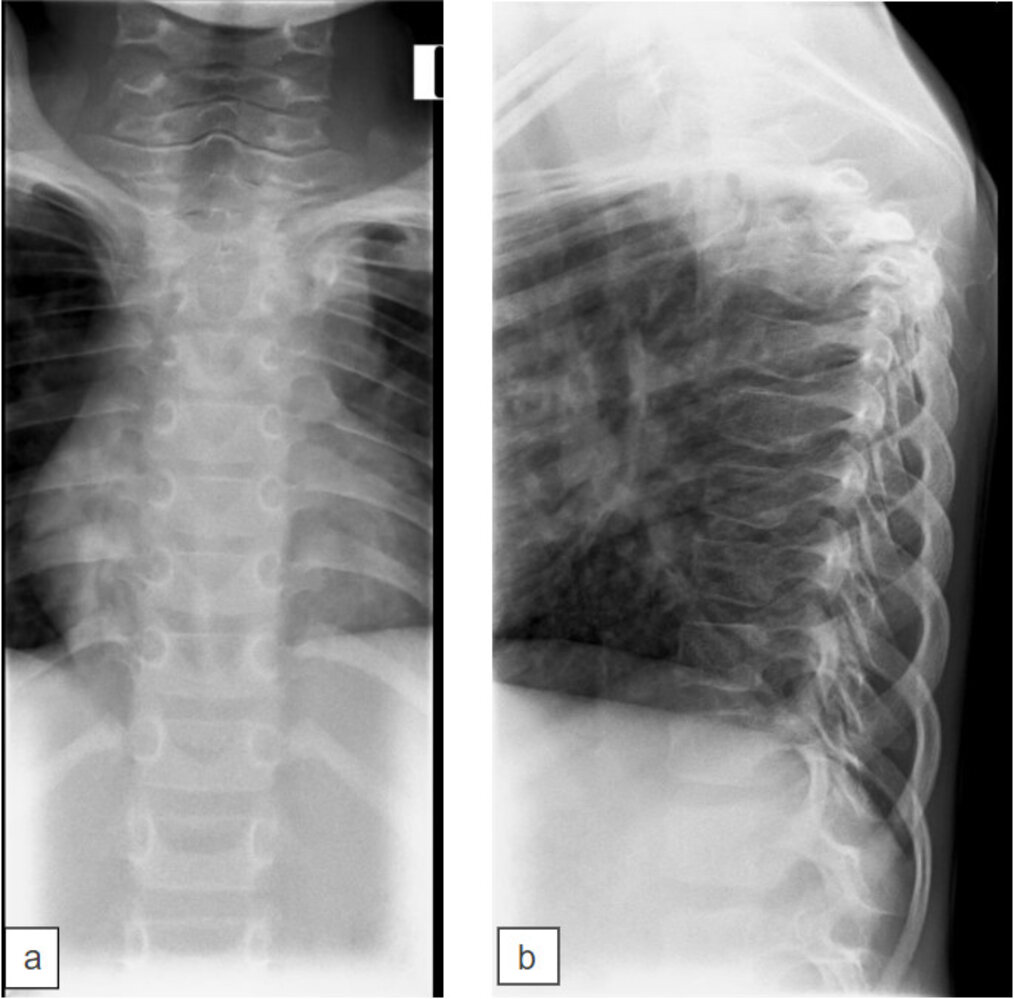
X-ray thoracic spine (a: AP view; b: lateral view) of a child with history of tuberculosis
A markedly angulated short-segment thoracic spine kyphosis (gibbus deformity) has resulted from tuberculous spondylitis involving the T4–T6 vertebrae (a: circle, b: green overlay). The left mediastinal convexity (dashed line) on the anteroposterior (AP) view proved to represent an accompanying paraspinal mass.
Gibbus deformities can be the consequence of various infections, metabolic diseases, or congenital diseases.
Source: “Figure 131a and b, in: Atlas of Paediatric HIV Infection” by Oladokun RE; Lehloenya RJ; Hlela C; et al, Openbooks, licensed under CC BY-ND 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
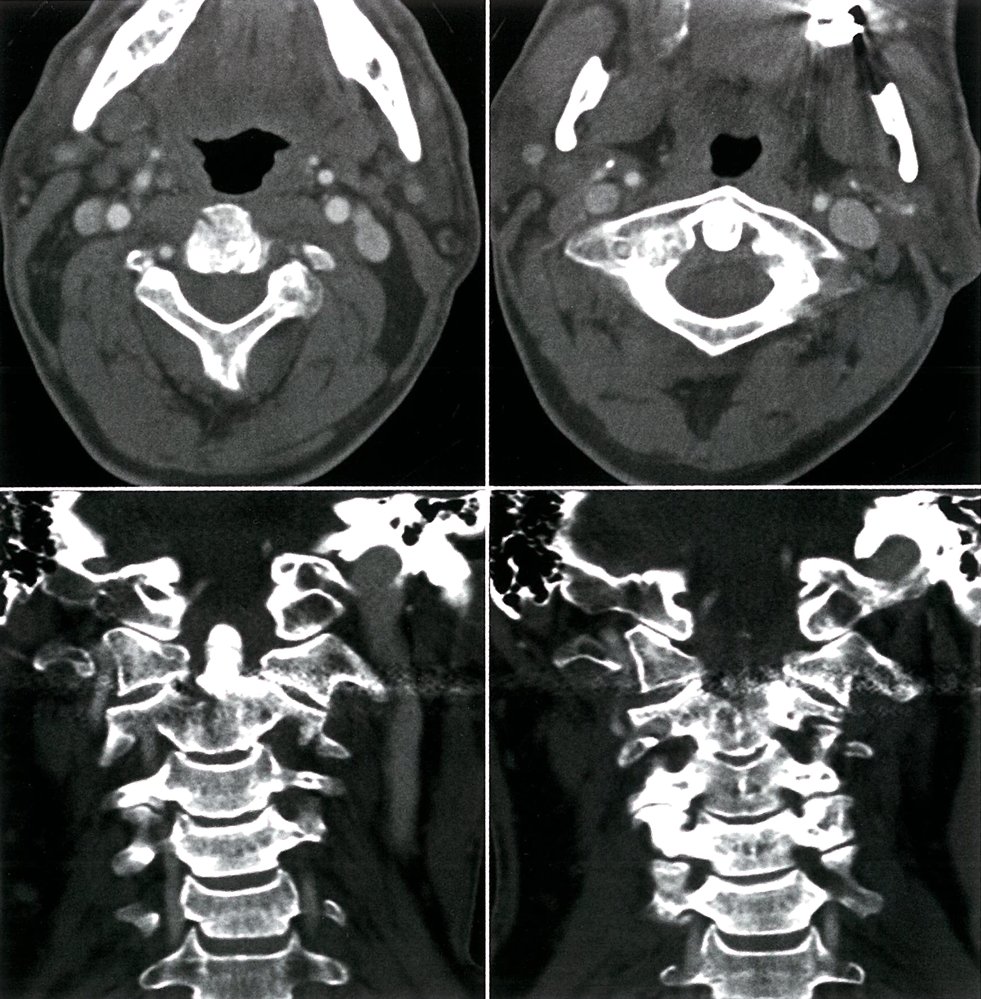
CT angiography of the cervical spine with contrast, axial and coronal view: burst fracture of C2 with pedicle involvement; absence of contrast from the left vertebral artery above C5, indicating its occlusion
Source: © IMPP
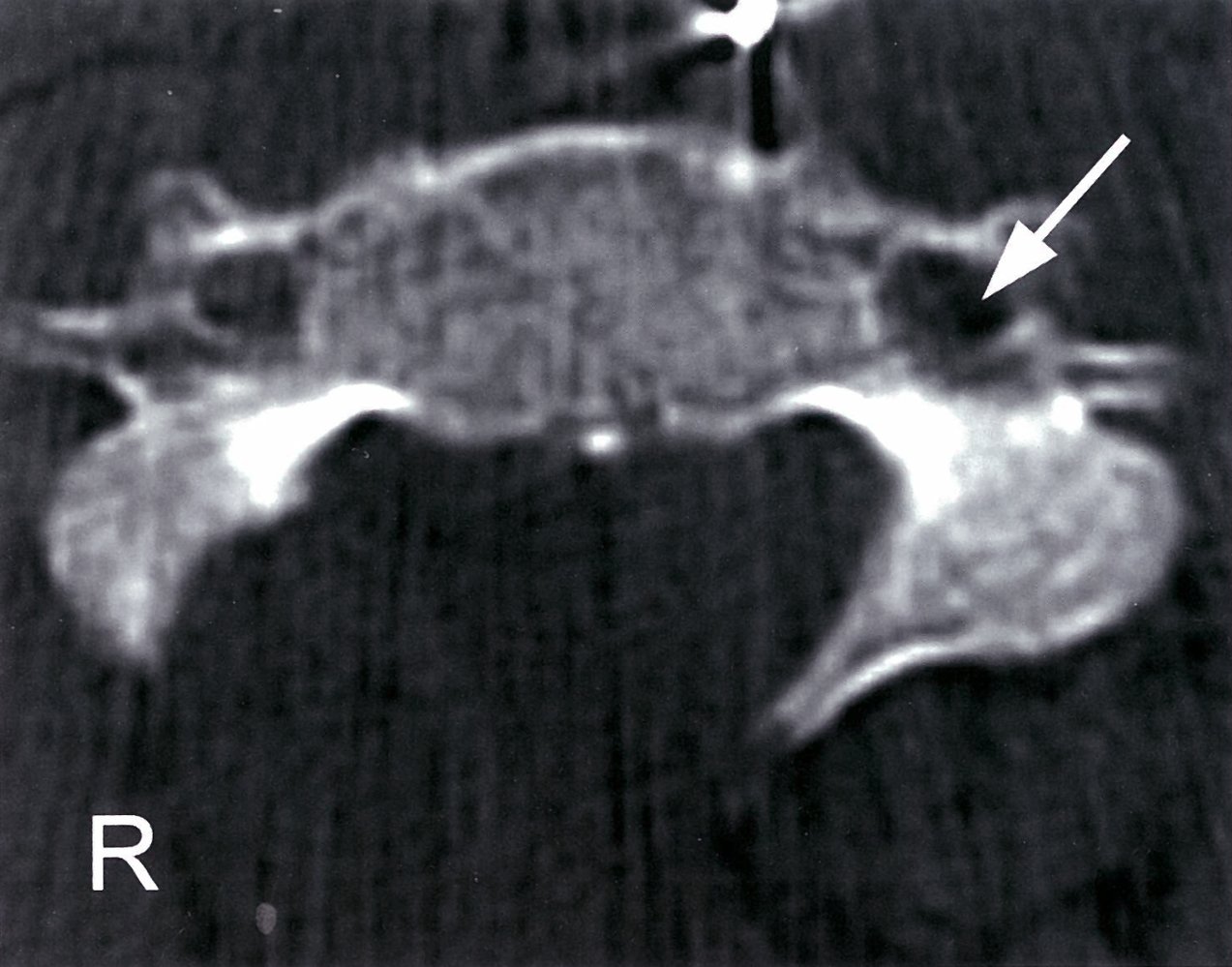
CT scan, axial section at level of 4th cervical vertebra
The white arrow points to the transverse foramen, which the vertebral artery passes through. After arising from the subclavian artery, the
vertebral artery passes back behind the internal carotid artery. At the 6th cervical vertebra, it enters the transverse foramen, which is located in the transverse process. At the first cervical spine, the vertebral artery curves backwards and joins the vertebral artery from the other side to form the basilar artery, entering the cranium via the foramen magnum.
Source: © IMPP
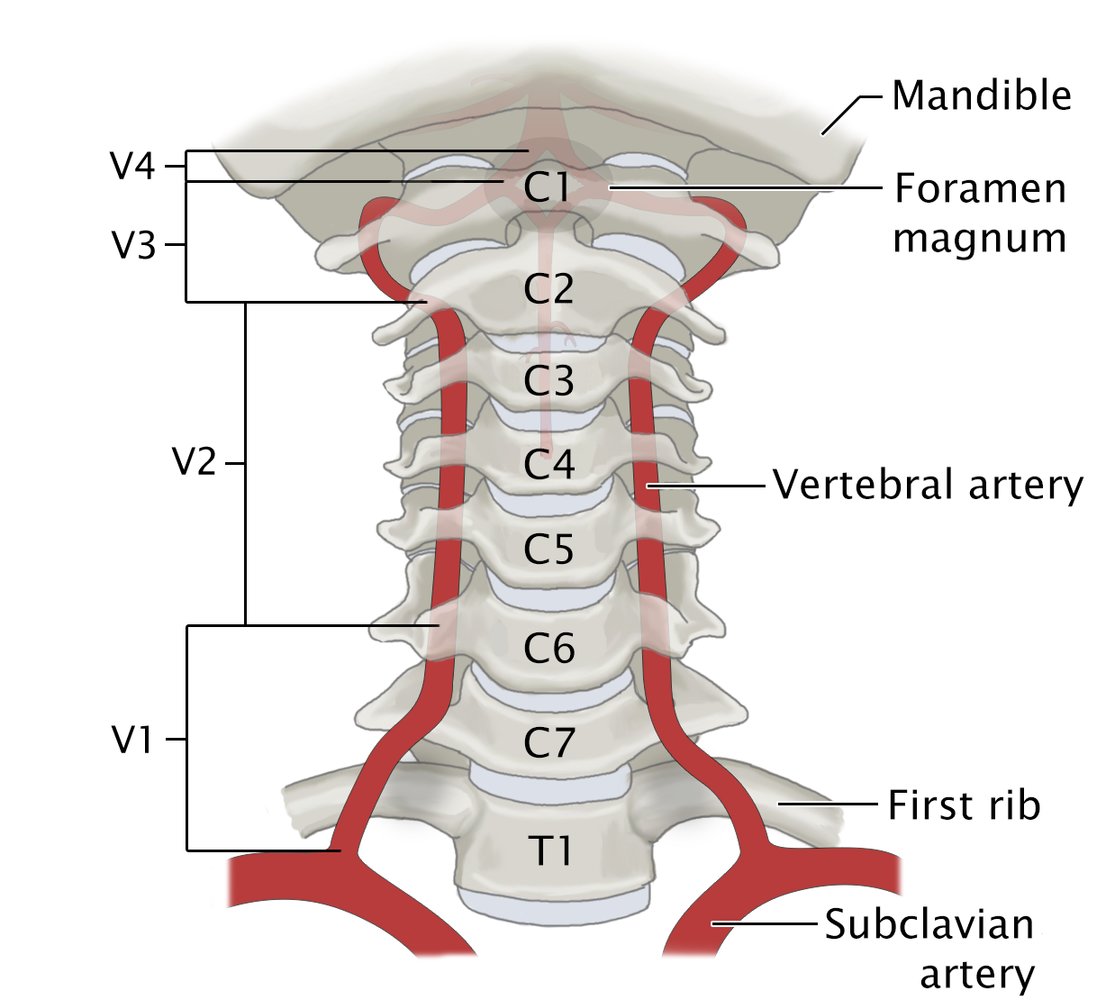
The vertebral artery can be divided into four segments:
V1: preforaminal segment from the subclavian artery to the transverse foramen of C6
V2: foraminal segment through the transverse foramen of C6 to C2
V3: atlanto-axial segment from the exit point of the transverse foramen of C2 to the point of entry in the foramen magnum
V4: intradural segment from the foramen magnum to the transition in the basilar artery
© AMBOSS

MRI cervical spine (T2-weighted; sagittal view) in a patient with a previous C4 vertebral body fracture
There is subtle increased signal within the spinal cord extending from the level of the 3rd to 5th cervical vertebral bodies; this segment of the cord also appears swollen. This represents myelopathy. High signal is shown within the soft tissues surrounding the spinous processes of the 2nd to 6th cervical vertebrae. The patient underwent surgery for a C4 cervical spine fracture prior to this MRI, and this soft tissue high signal is likely related to this. Some of the signal may also be due to the initial traumatic event that resulted in the C4 fracture.
Myelopathy is a broad term meaning disease of the spinal cord. It can be due to various causes, one of the most common being compression of the cord due to trauma, as seen here.
Source: © IMPP
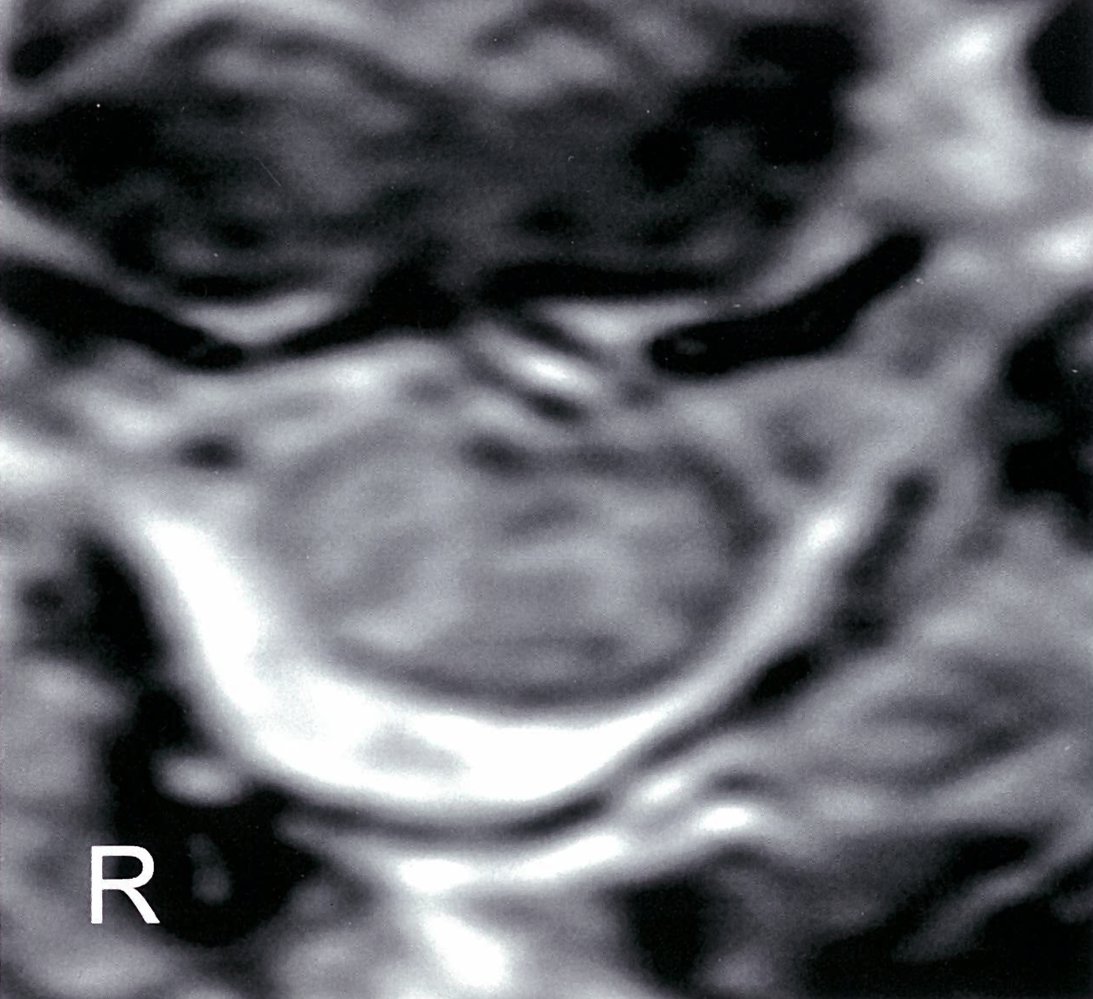
MRI cervical spine (T2-weighted; axial view) of a patient with a vertebral body fracture
Multiple regions of hyperintense signal are visible within the grey and white matter of the spinal cord, indicating myelopathy. In this patient, the myelopathy was caused by direct trauma.
Source: © IMPP
Special patient groups
Deviations in the initial management of vertebral injuries may be necessary for different age groups.
Vertebral injuries in children [60][61]
- Cervical spine injuries (most common): See “C-spine injuries in children.”
-
Thoracolumbar spine injuries [23][60]
- Most common in children > 9 years of age, uncommon in young children
- Often involve vertebral compression fractures and/or burst fractures
-
Diagnostics for vertebral injuries
- X-ray spine (anterior and lateral views): preferred initial study; lower radiation exposure than CT
- CT and/or MRI spine: Consider in consultation with specialists for patients with neurological deficits or abnormal x-ray findings.
- Related injuries: See ”Spinal cord injury without radiographic abnormality (SCIWORA).”
Vertebral injuries in older adults [4][62]
-
Common injuries
- Upper cervical spine injuries
- Vertebral compression fractures
- Concurrent incomplete spinal cord injuries, especially acute cervical central cord syndrome
-
High injury risk
- Significant injuries can be caused by minimal or low-energy trauma.
- High prevalence of risk factors for vertebral injuries, e.g.:
- Falls in older adults
- Osteopenia and osteoporosis
- Stiff spine
- Underlying malignancy
-
Higher risk of missed vertebral fractures
- Lower rates of reported pain and detectable tenderness [63]
- Lower accuracy of clinical decision rules to guide imaging [64]
Maintain a low threshold for imaging in older adults with suspected vertebral injury, even with minimal trauma. [4][62]
External Resources
References
- Bigdon SF, Saldarriaga Y, Oswald KAC, et al. "Epidemiologic analysis of 8000 acute vertebral fractures: evolution of treatment and complications at 10-year follow-up". J Orthop Surg. 17(1). (2022)
- Parizel PM, Van der zijden T, Gaudino S, et al. "Trauma of the spine and spinal cord: imaging strategies". Eur Spine J. 19(Suppl 1). :S8-17. (2009)
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904
- DENIS F. "The Three Column Spine and Its Significance in the Classification of Acute Thoracolumbar Spinal Injuries". Spine. 8(8). :817-831. (1983)
- Denis F. "Spinal instability as defined by the three-column spine concept in acute spinal trauma.". Clin Orthop Relat Res. :65-76. (1984)
- Cahueque M, Cobar A, Zuñiga C, Caldera G. "Management of burst fractures in the thoracolumbar spine". J Orthop. 13(4). :278-281. (2016)
- Sadiqi S, Verlaan JJ, Lehr AM, et al. "Measurement of kyphosis and vertebral body height loss in traumatic spine fractures: an international study". Eur Spine J. 26(5). :1483-1491. (2016)
- Lee JY, Nassr A, Eck JC, Vaccaro AR. "Controversies in the treatment of cervical spine dislocations". Spine J. 9(5). :418-423. (2009)
- Theodore N, Aarabi B, Dhall SS, et al. "The Diagnosis and Management of Traumatic Atlanto-occipital Dislocation Injuries". Neurosurgery. 72(supplement 2). :114-126. (2013)
- Ryken TC, Hadley MN, Aarabi B, et al. "Management of Isolated Fractures of the Axis in Adults". Neurosurgery. 72(supplement 2). :132-150. (2013)
- Anderson Ld, D'Alonzo RT. "Fractures of the odontoid process of the axis". J Bone Joint Surg Am. 56(8). :1663-74. (1974)
- Vaccaro AR, Lambrechts MJ, Karamian BA, et al. "Global Validation of the AO Spine Upper Cervical Injury Classification". Spine. 47(22). :1541-1548. (2022)
- Canseco JA, Schroeder GD, Paziuk TM, et al. "The Subaxial Cervical AO Spine Injury Score". Global Spine J. 12(6). :1066-1073. (2020)
- Schnake KJ, Schroeder GD, Vaccaro AR, Oner C. "AOSpine Classification Systems (Subaxial, Thoracolumbar)". J Orthop Trauma. 31(4). :S14-S23. (2017)
- Vaccaro AR, Karamian BA, Levy HA, et al. "Update on Upper Cervical Injury Classifications". Clin Spine Surg. 35(6). :249-255. (2021)
- Vaccaro AR, Lehman RA, Hurlbert RJ, et al. "A New Classification of Thoracolumbar Injuries". Spine. 30(20). :2325-2333. (2005)
- Vaccaro AR, Hulbert RJ, Patel AA, et al. "The Subaxial Cervical Spine Injury Classification System". Spine. 32(21). :2365-2374. (2007)
- "Best practice guidelines spine injury". https://www.facs.org/media/k45gikqv/spine_injury_guidelines.pdf. [2022-03-01]
- Beckmann NM, West OC, Nunez D, et al. "ACR Appropriateness Criteria® Suspected Spine Trauma". J Am Coll Radiol. 16(5). :S264-S285. (2019)
- "ACS TQIP Best Practices in Imaging Guidelines 2018". https://www.facs.org/media/oxdjw5zj/imaging_guidelines.pdf. [2018-10-01]
- Zileli M, Osorio-Fonseca E, Konovalov N, et al. "Early Management of Cervical Spine Trauma: WFNS Spine Committee Recommendations.". Neurospine. 17(4). :710-722. (2020)
- Kadom N, Palasis S, Pruthi S, et al. "ACR Appropriateness Criteria® Suspected Spine Trauma-Child". J Am Coll Radiol. 16(5). :S286-S299. (2019)
- McAllister AS, Nagaraj U, Radhakrishnan R. "Emergent Imaging of Pediatric Cervical Spine Trauma". RadioGraphics. 39(4). :1126-1142. (2019)
- Patel MB, Humble SS, Cullinane DC, et al. "Cervical spine collar clearance in the obtunded adult blunt trauma patient". J Trauma Acute Care Surg. 78(2). :430-441. (2015)
- Dion PM, Lapierre M, Said H, et al. "Rethinking cervical spine clearance in obtunded trauma patients: An updated systematic review and meta-analysis". Injury. 55(3). :111308. (2024)
- Oner C, Rajasekaran S, Chapman JR, et al. "Spine Trauma—What Are the Current Controversies?". J Orthop Trauma. 31(4). :S1-S6. (2017)
- Patel A, Joaquim A. "Thoracolumbar spine trauma: Evaluation and surgical decision-making". J Craniovertebr Junction Spine. 4(1). :3. (2013)
- Genev IK, Tobin MK, Zaidi SP, et al. "Spinal Compression Fracture Management". Global Spine J. 7(1). :71-82. (2017)
- Okereke I, Mmerem K, Balasubramanian D. "The Management of Cervical Spine Injuries – A Literature Review". Orthop Res Rev. Volume 13. :151-162. (2021)
- Kalanjiyam GP, Kanna RM, Rajasekaran S. "Pediatric spinal injuries– current concepts". J Clin Orthop Trauma. 38. :102122. (2023)
- Sayama C, Chen T, Trost G, Jea A. "A review of pediatric lumbar spine trauma". Neurosurg Focus. 37(1). :E6. (2014)
- Sunder A, Chhabra HS, Aryal A. "Geriatric spine fractures – Demography, changing trends, challenges and special considerations: A narrative review". J Clin Orthop Trauma. 43. :102190. (2023)
- Healey CD, Spilman SK, King BD, Sherrill JE, Pelaez CA. "Asymptomatic cervical spine fractures". J Trauma Acute Care Surg. 83(1). :119-125. (2017)
- "ACS Trauma Quality Improvement Program Best practices guideline in imaging". https://www.facs.org/media/oxdjw5zj/imaging_guidelines.pdf. [2018-01-01]
- Hsu JM, Joseph T, Ellis AM. "Thoracolumbar fracture in blunt trauma patients: guidelines for diagnosis and imaging". Injury. 34(6). :426-433. (2003)
- Holmes JF, Panacek EA, Miller PQ, Lapidis AD, Mower WR. "Prospective evaluation of criteria for obtaining thoracolumbar radiographs in trauma patients". J Emerg Med. 24(1). :1-7. (2003)
- Inaba K, Nosanov L, Menaker J, et al. "Prospective derivation of a clinical decision rule for thoracolumbar spine evaluation after blunt trauma: An American Association for the Surgery of Trauma Multi-Institutional Trials Group Study.". J Trauma Acute Care Surg. 78(3). :459-65; discussion 465-7. (2015)
- Jo AS, Wilseck Z, Manganaro MS, Ibrahim M. "Essentials of Spine Trauma Imaging: Radiographs, CT, and MRI". Sem Ultrasound, CT and MR. 39(6). :532-550. (2018)
- Wood KB, Li W, Lebl DS, Ploumis A. "Management of thoracolumbar spine fractures". The Spine Journal. 14(1). :145-164. (2014)
- Anandasivam NS, Ondeck NT, Bagi PS, et al. "Spinal fractures and/or spinal cord injuries are associated with orthopedic and internal organ injuries in proximity to the spinal injury". N Am Spine Soc J. 6. :100057. (2021)
- Hachem LD, Ahuja CS, Fehlings MG. "Assessment and management of acute spinal cord injury: From point of injury to rehabilitation". J Spinal Cord Med. 40(6). :665-675. (2017)
- Cho N, Alkins R, Khan OH, Ginsberg H, Cusimano MD. "Unilateral Lumbar Facet Dislocation: Case Report and Review of the Literature". World Neurosurg. 123. :310-316. (2019)
- Manaster B, Osborn A. "CT patterns of facet fracture dislocations in the thoracolumbar region". AJR Am J Roentgenol. 148(2). :335-340. (1987)
- Lopez AJ, Scheer JK, Smith ZA, Dahdaleh NS. "Management of flexion distraction injuries to the thoracolumbar spine". J Clin Neuroscience. 22(12). :1853-1856. (2015)
- McCarthy J, Davis A. "Diagnosis and Management of Vertebral Compression Fractures.". Am Fam Physician. 94(1). :44-50. (2016)
- Lenchik L, Rogers LF, Delmas PD, Genant HK. "Diagnosis of Osteoporotic Vertebral Fractures: Importance of Recognition and Description by Radiologists". Am J Roentgenol. 183(4). :949-958. (2004)
- Madassery S. "Vertebral Compression Fractures: Evaluation and Management". Semin Intervent Radiol. 37(02). :214-219. (2020)
- Angelini A, Mosele N, Gnassi A, et al. "Vertebra Plana: A Narrative Clinical and Imaging Overview among Possible Differential Diagnoses". Diagnostics. 13(8). (2023)
- P G Ntagiopoulos, D-A Moutzouris, S Manetas. "The "fish-vertebra" sign". Emerg Med J. 24(9). :674-675. (2007)
- Alsoof D, Anderson G, McDonald CL, et al. "Diagnosis and Management of Vertebral Compression Fracture". Am J Med. 135(7). :815-821. (2022)
- Alexandru D, So W. "Evaluation and Management of Vertebral Compression Fractures". Perm J. 16(4). :46-51. (2012)
- Shah LM, Jennings JW, Kirsch CFE, et al. "ACR Appropriateness Criteria® Management of Vertebral Compression Fractures". J Am Coll Radiol. 15(11). :S347-S364. (2018)
- "AAOS CLINICAL PRACTICE GUIDELINE SUMMARY The Treatment of Symptomatic Osteoporotic Spinal Compression Fractures". https://journals.lww.com/jaaos/fulltext/2011/03000/the_treatment_of_symptomatic_osteoporotic_spinal.7.aspx. [2011-03-01]
- Hirsch JA, Beall DP, Chambers MR, et al. "Management of vertebral fragility fractures: a clinical care pathway developed by a multispecialty panel using the RAND/UCLA Appropriateness Method". Spine J. 18(11). :2152-2161. (2018)
- Tanna NK, Ong T. "Pharmacological options for pain control in patients with vertebral fragility fractures". Osteoporos Sarcopenia. 8(3). :93-97. (2022)
- Kendler DL, Bauer DC, Davison KS, et al. "Vertebral Fractures: Clinical Importance and Management". Am J Med. 129(2). :221.e1-221.e10. (2016)
- Beall DP, Phillips TR. "Vertebral augmentation: an overview". Skeletal Radiol. 52(10). :1911-1920. (2022)
- Abudou M, Chen X, Kong X, Wu T. "Surgical versus non-surgical treatment for thoracolumbar burst fractures without neurological deficit". Cochrane Database Syst Rev. (2013)
- Atlas S, Regenbogen V, Rogers L, Kim K. "The radiographic characterization of burst fractures of the spine". Am J Roentgenol. 147(3). :575-582. (1986)
- Lehman RA, Paik H, Eckel TT, et al. "Low lumbar burst fractures: a unique fracture mechanism sustained in our current overseas conflicts". Spine J. 12(9). :784-790. (2012)
- Roblesgil-Medrano A, Tellez-Garcia E, Bueno-Gutierrez LC, et al. "Thoracolumbar Burst Fractures: A Systematic Review and Meta-Analysis on the Anterior and Posterior Approaches". Spine Surg Rel Res. 6(2). :99-108. (2022)
- Bakhsheshian J, Dahdaleh NS, Fakurnejad S, Scheer JK, Smith ZA. "Evidence-based management of traumatic thoracolumbar burst fractures: a systematic review of nonoperative management". Neurosurg Focus. 37(1). :E1. (2014)
- Nagasawa DT, Bui TT, Lagman C, et al. "Isolated Transverse Process Fractures: A Systematic Analysis". World Neurosurg. 100. :336-341. (2017)
- Peterson A, Behrens J, Salari P, Place H. "Isolated thoracic and lumbar transverse process fractures: Do they need spine surgeon evaluation? a high volume level I trauma center experience with cost analysis". N Am Spine Soc J. 15. :100242. (2023)