Summary
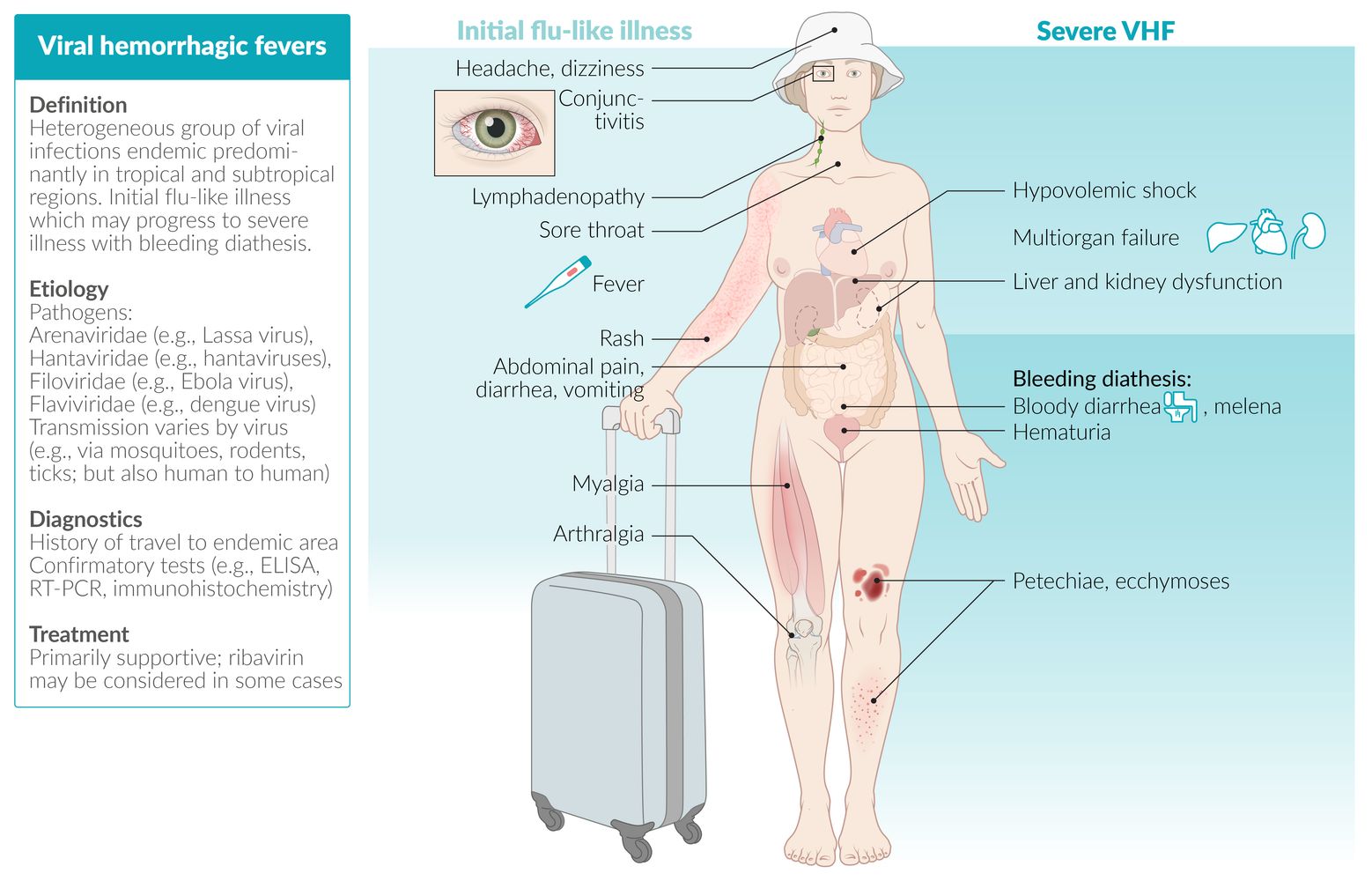
Viral hemorrhagic fevers (VHFs) are a group of viral infections caused by viruses from five different families: Arenaviridae, Bunyaviridae, Filoviridae, Flaviviridae, and Paramyxoviridae. The most well-known VHFs are Lassa fever, Hantavirus syndromes, Ebola virus disease, Dengue hemorrhagic fever, and yellow fever. Transmission of VHFs occurs via contact with their animal or insect reservoirs or vectors (e.g., rodents, mosquitoes, ticks). Human-to-human transmission is also possible, e.g., via bodily fluids. VHFs predominantly occur in tropical and subtropical regions. Clinical features of VHFs vary but often include an initial nonspecific flu-like illness that progresses to multisystem hemorrhage. VHFs are diagnosed via antibody detection (e.g., IgG, IgM), PCR, or immunohistochemistry. Treatment is typically supportive, but antivirals may be used in some cases (e.g., ribavirin in Lassa fever). Case fatality rates vary greatly between VHFs but can be up to 90%. Vaccines are licensed internationally for yellow fever only, so prevention primarily consists of infection control measures.
Etiology
-
Pathogens are enveloped RNA viruses from the following families:
- Arenaviridae
- Bunyaviridae
- Filoviridae
- Flaviviridae
- Paramyxoviridae
-
Transmission
-
Reservoir hosts or vectors such as rodents, mosquitoes, and ticks
- Direct contact
- Inhalation of infected particles
- Contact with infectious material
-
Human-to-human transmission
- Airborne droplets
- Contact with blood or other bodily fluids
-
Reservoir hosts or vectors such as rodents, mosquitoes, and ticks
Overview
| Overview of common viral hemorrhagic fevers | |||||||
|---|---|---|---|---|---|---|---|
| Family | Virus | Disease(s) | Geography | Transmission | Incubation period | Case fatality rate | Vaccine |
| Arenaviridae | Lassa virus | Lassa fever |
|
|
|
|
|
| Hantaviridae | Hantaviruses (especially Sin Nombre virus for HCPS) | Hantavirus cardiopulmonary syndrome (HCPS) |
|
|
|
|
|
| Hemorrhagic fever with renal syndrome (HFRS) |
|
|
|
||||
| Nairoviridae | Crimean Congo hemorrhagic fever virus | Crimean-Congo hemorrhagic fever |
|
|
|
|
|
| Phenuiviridae | Rift valley fever virus | Rift valley fever |
|
|
|
|
|
| Filoviridae | Ebola virus | Ebola virus disease |
|
|
|
|
|
| Marburg virus | Marburg hemorrhagic fever |
|
|
|
|
|
|
| Flaviviridae | Dengue virus | Severe dengue (Dengue hemorrhagic fever) |
|
|
|
|
|
| Yellow fever virus | Yellow fever |
|
|
|
|
|
|



Colorized electron micrographs
Single filamentous virus particles (yellow) can be seen in the first and second image. The third image shows several filamentous viral particles.
The Ebola virus is a member of the family Filoviridae, named after the filamentous shape of the viruses it contains.
Source: "IDs 10815, 17776, 17775", CDC/ National Institute of Allergy and Infectious Diseases (NIAID)/Frederick A. Murphy, Centers for Disease Control and Prevention (CDC) licensed under Public Domain Further notes: The image actually is a merged image of three CDC Images (10815, 17776, 17775)
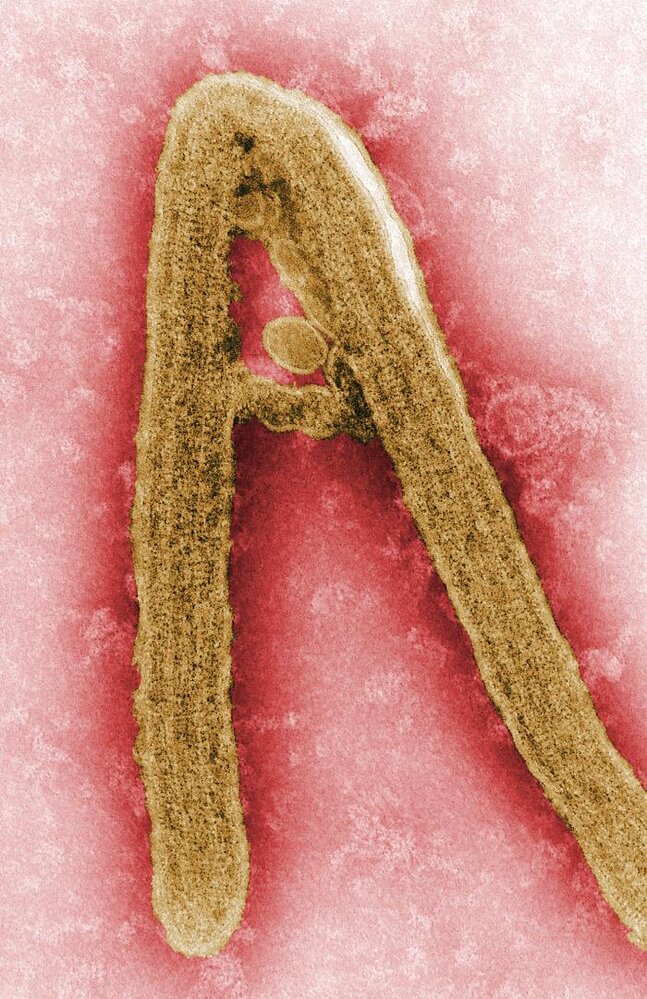
Colorized electron micrograph of a Marburg virus
The linear virus appears in yellow and has a characteristic filamentous shape.
Source: "ID#10813", CDC/ Frederick Murphy, Public Health Image Library licensed under Public Domain
Clinical features
Clinical features of VHFs vary depending on which virus is involved. Onset may be acute (e.g., Ebola virus disease) or insidious (e.g., Lassa fever) and often includes the following:
-
Initial flu-like illness
- Headache, dizziness
- Conjunctivitis
- High fever
- Lymphadenopathy
- Sore throat
- Myalgia, arthralgia
- Rash
- Weakness, fatigue, prostration [15]
- Gastrointestinal symptoms (abdominal pain, diarrhea; , nausea, vomiting) [15][16]
-
Severe VHF with bleeding diathesis: develops in a variable number of cases, depending on the causative pathogen
-
Diffuse hemorrhage including:
- Bloody diarrhea, hematuria, hematemesis, melena
- Mucosal bleeding
- Petechiae, ecchymoses
- Hypovolemic shock and multiorgan failure
- Sepsis
- DIC
- Meningoencephalitis
-
Diffuse hemorrhage including:


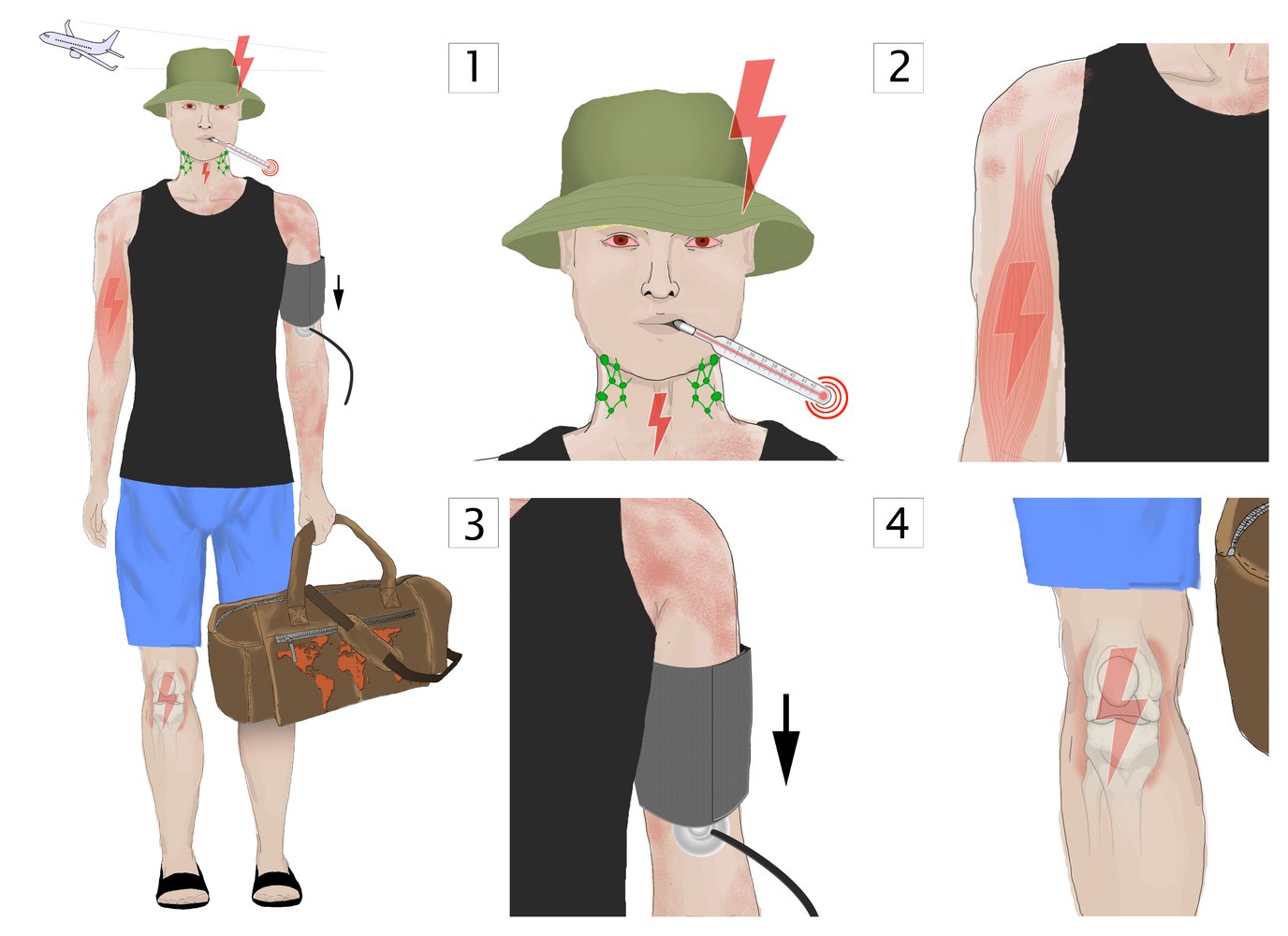
Symptoms of viral hemorrhagic fevers resemble those of the flu, which is why the patient's travel history is of great importance. The most common symptoms are: (1) headaches, conjunctivitis, high fever (up to 41°C), lymphadenopathy, sore throat; (2) myalgias; (3) mild hypotension and exanthema; (4) and arthralgias.
© AMBOSS

Diffuse macules and papules are seen on the back, left shoulder, and left arm.
This is the typical appearance of the rash caused by the Marburg virus.
Source: "ID#: 6571", CDC/ Dr. J. Lyle Conrad, Centers for Disease Control and Prevention (CDC) licensed under Public Domain
© AMBOSS
Diagnosis
-
Approach
- Diagnosis of VHF during the early stages is difficult because the symptoms are nonspecific.
- If clinical and laboratory features are consistent with the condition, further studies should be conducted to confirm the diagnosis.
-
Medical history
- A detailed travel history to endemic regions is essential!
- History of exposure to a potential source of infection (e.g., rodents, mosquitoes, ticks)
-
General laboratory studies
- CBC
- Electrolytes, BUN/creatinine, liver function tests
- Urinalysis
- Coagulation studies
-
Confirmatory tests
- Generally performed by specialized reference laboratories; presumptive positive results must be confirmed by the CDC. [15]
- Serology: IgM and/or rising levels of IgG antibodies detected using enzyme-linked immunosorbent assay (ELISA) or other diagnostic assays [17][18]
- Reverse transcription-polymerase chain reaction (RT-PCR) [19]
- Immunohistochemistry [19]
Differential diagnoses
- Malaria
- Meningococcal septicemia or other types of sepsis
- Leptospirosis
- Typhoid fever
- Q fever
- Influenza
- Shigellosis
- Rickettsial infection (e.g., Rocky Mountain spotted fever)
- Acute leukemia
- Idiopathic thrombocytopenic purpura
- Thrombotic thrombocytopenic purpura
The differential diagnoses listed here are not exhaustive.
Treatment
-
Supportive treatment
- Management of fluids and electrolyte balance
- Maintenance of blood pressure and oxygenation
- Analgesics for pain and fever
- Blood products in patients with severe thrombocytopenia, coagulopathy, hemorrhage
-
Medical treatment
- Treat patients with ebola with atoltivimab/maftivimab/odesivimab OR ansuvimab. [20]
- Ribavirin may be used in Lassa fever and Crimean-Congo fever. [21][22]
Aspirin and NSAIDs should be avoided in VHFs because they are associated with an increased risk of bleeding!
Prevention
Immunization
- See “Vaccine” in “Overview of viral hemorrhagic fevers” above.
Prevention [15][23][24]
- Avoid contact with blood, body fluids, or tissue from infected reservoirs or humans
- Avoid travel to endemic areas
- In suspected cases
- Immediate notification of local health authorities and the CDC of any suspected cases of VHF
- Strict isolation of infected patients and their contacts with disinfection and sterilization measures
- Wear appropriate personal protective equipment (e.g., impermeable gown, gloves, respiratory protection, rubber boots).
Reportable disease [25]
- Probable, suspected, or confirmed cases of VHFs are notifiable conditions to local and state health authorities, as well as the CDC National Notifiable Disease Surveillance System.
Hantavirus infection
There are two notable syndromes that can develop from a hantavirus infection: hantavirus cardiopulmonary syndrome (HCPS) and hemorrhagic fever with renal syndrome (HFRS)
- Epidemiology: See “Overview of viral hemorrhagic fevers” above.
-
Clinical features
- History of rodent or rodent urine exposure (e.g., picnicking in a park)
- Prodromal/febrile phase (∼ 2–7 days upon onset of illness): clinical features of VHF (see above)
- Syndrome-specific features
-
HCPS: Cardiopulmonary phase (∼ 2–7 days following prodromal/febrile phase) with lung infiltration (pulmonary edema) and, in severe cases, development of acute respiratory distress syndrome (ARDS)
- Dry cough
- In severe cases: rapidly developing shock, coagulopathy, pulmonary edema
- Tachycardia, hypotension
- Dyspnea
-
HFRS: group of clinical syndromes of acute interstitial nephritis occurring mainly in Europe and Asia [18]
- Signs of renal failure
- Hypotension
-
HCPS: Cardiopulmonary phase (∼ 2–7 days following prodromal/febrile phase) with lung infiltration (pulmonary edema) and, in severe cases, development of acute respiratory distress syndrome (ARDS)
-
Diagnostics: If clinical and laboratory features are consistent with the condition, further studies should be conducted to confirm the diagnosis.
-
Laboratory studies
- HCPS: triad of left shift, thrombocytopenia, abundance of immunoblasts
-
HFRS
- CBC: thrombocytopenia, leukocytosis
- BMP: ↑ serum creatinine
-
Urinalysis
- Proteinuria
- Hematuria
- Confirmatory studies [18][19][26]
- Serology: IgM and/or rising levels of IgG antibodies detected using enzyme-linked immunosorbent assay (ELISA) or other diagnostic assays
- Reverse transcription-polymerase chain reaction (RT-PCR)
- Immunohistochemistry
-
Laboratory studies
-
Management [18][27][28]
- Supportive care (e.g., ICU admission, early intubation, supplementary oxygen)
- For HFRS: ribavirin
- Prognosis: See case fatality rate in “Overview of viral hemorrhagic fevers” above.
References
- "CDC - Viral Hemorrhagic Fevers". https://web.archive.org/web/20210318074601/https://wwwnc.cdc.gov/travel/yellowbook/2020/travel-related-infectious-diseases/viral-hemorrhagic-fevers. [2019-06-24]
- Cobo F. "Viruses Causing Hemorrhagic Fever. Safety Laboratory Procedures.". The open virology journal. 10. :1-9. (2016)
- "CDC - Hantavirus". https://web.archive.org/web/20210416052756/https://www.cdc.gov/hantavirus/technical/hps/diagnostics.html. [2020-03-11]
- "CDC - Hemorrhagic Fever with Renal Syndrome (HFRS)". https://web.archive.org/web/20210410125757/https://www.cdc.gov/hantavirus/hfrs/index.html. [2017-01-18]
- "CDC - Hantavirus Pulmonary Syndrome (HPS)". https://web.archive.org/web/20210322143116/https://wwwn.cdc.gov/nndss/conditions/hantavirus-pulmonary-syndrome/case-definition/2015/. [2015-01-01]
- "CDC: Clinical Guidance for Ebola Disease". https://web.archive.org/web/20260318023126/https://www.cdc.gov/ebola/hcp/clinical-guidance/index.html#cdc_clinical_guidance_prevent_key-preventing-infection
- "CDC - Lassa Fever - Treatment". https://web.archive.org/web/20210419140055/https://www.cdc.gov/vhf/lassa/treatment/index.html. [2014-03-25]
- "Clinical guidelines - Diagnosis and treatment manual". https://medicalguidelines.msf.org/en/viewport/CG/english/clinical-guidelines-16686604.html. [2025-06-01]
- "CDC - Ebola (Ebola Virus Disease) - Prevention and Vaccine". https://web.archive.org/web/20210318021906/https://www.cdc.gov/vhf/ebola/prevention/index.html. [2021-02-26]
- "Infection Control for Viral Haemorrhagic Fevers"
- "CDC - National Notifiable Diseases Surveillance System (NNDSS)". https://web.archive.org/web/20210330023654/https://wwwn.cdc.gov/nndss/conditions/notifiable/2017/. [2017-01-01]
- "CDC - Lassa Fever". https://web.archive.org/web/20210326072351/https://www.cdc.gov/vhf/lassa/index.html. [2019-01-31]
- "CDC - Hantaviruses". https://web.archive.org/web/20210410130401/https://www.cdc.gov/hantavirus/technical/hanta/virology.html. [2012-08-29]
- Avšič-Županc T, Saksida A, Korva M. "Hantavirus infections". Clinical Microbiology and Infection. 21. :e6-e16. (2019)
- Jonsson CB, Figueiredo LT, Vapalahti O. "A global perspective on hantavirus ecology, epidemiology, and disease.". Clin Microbiol Rev. 23(2). :412-41. (2010)
- Mertens M, Schmidt K, Ozkul A, Groschup MH. "The impact of Crimean-Congo hemorrhagic fever virus on public health.". Antiviral Res. 98(2). :248-60. (2013)
- Dowall SD, Carroll MW, Hewson R. "Development of vaccines against Crimean-Congo haemorrhagic fever virus.". Vaccine. 35(44). :6015-6023. (2017)
- "CDC - Rift Valley Fever (RVF)". https://web.archive.org/web/20210331034730/https://www.cdc.gov/vhf/rvf/. [2020-02-25]
- "2014-2016 Ebola Outbreak in West Africa". https://web.archive.org/web/20210401205323/https://www.cdc.gov/vhf/ebola/history/2014-2016-outbreak/index.html. [2019-03-08]
- "CDC - Ebola (Ebola Virus Disease) - Case Counts". https://web.archive.org/web/20210326152807/https://www.cdc.gov/vhf/ebola/history/2014-2016-outbreak/case-counts.html. [2020-02-19]
- "CDC - Marburg hemorrhagic fever (Marburg HF)". https://web.archive.org/web/20210320122301/https://www.cdc.gov/vhf/marburg/about.html. [2014-12-03]
- Guzman MG, Halstead SB, Artsob H, et al. "Dengue: a continuing global threat". Nature Reviews Microbiology. 8(S12). :S7-S16. (2010)
- World Health Organization. "Dengue: Guidelines for Diagnosis, Treatment, Prevention and Control 2009". WHO. (2009)
- Moraes GH, de Fátima Duarte E, Duarte EC. "Determinants of mortality from severe dengue in Brazil: a population-based case-control study.". Am J Trop Med Hyg. 88(4). :670-6. (2013)
- "CDC - Yellow Fever". https://web.archive.org/web/20210406000952/https://www.cdc.gov/globalhealth/newsroom/topics/yellowfever/index.html. [2018-09-14]
- "CDC - Hantavirus - Diagnostics". https://web.archive.org/web/20210416052756/https://www.cdc.gov/hantavirus/technical/hps/diagnostics.html. [2020-03-11]
- "CDC - Hantavirus - Diagnosis & Treatment". https://web.archive.org/web/20210416055455/https://www.cdc.gov/hantavirus/hps/diagnosis.html. [2012-08-29]
- Moreli ML, Marques-Silva AC, Pimentel VA, da Costa VG. "Effectiveness of the ribavirin in treatment of hantavirus infections in the Americas and Eurasia: a meta-analysis.". Virusdisease. 25(3). :385-9. (2014)