Summary
Vulvar cancer is a rare carcinoma that predominantly occurs after menopause. Major risk factors include HPV infection, smoking, vulvar intraepithelial neoplasia, and cervical intraepithelial neoplasia. Clinical features include local pruritus, plaques or masses, and, less frequently, vulvar bleeding. Suspicious lesions must be biopsied for histological analysis and to rule out differential diagnoses. Imaging studies and clinical evaluation, including a complete pelvic examination, are required for tumor staging. Surgical resection (radical vulvectomy) is the first-line treatment for locoregional disease; advanced stages may require radiotherapy and/or palliative chemotherapy.
Vaginal cancer is closely related to vulvar cancer in terms of etiology and histology, but it occurs inside the vagina (typically the posterior third of the vaginal wall) rather than in the vulva.
Vulvar cancer
Epidemiology [1]
- Incidence: rare (∼ 0.7% of female cancers) [1]
-
Age [2]
- HPV-related vulvar cancer: 35–65 years
- Non-HPV related types (e.g., associated with lichen sclerosus): 55–85 years
Risk factors [1]
- Infection with HPV 16, 18, 31, and 33 [1]
- Precursor lesions, e.g., lichen sclerosus, vulvar or cervical intraepithelial neoplasia (VIN/CIN)
- Tobacco smoking
- Immunosuppression
Classification [3][4]
-
Malignant lesions
-
Squamous cell carcinoma (SCC) and subtypes: > 80% of cases [1]
- Verrucous (warty) carcinoma
- Basaloid carcinoma
- Keratinizing carcinoma
- Paget disease of the vulva: an adenocarcinoma characterized by localized pruritus and eczematous lesions (e.g., erythematous patches with white scaling, crusting, ulcerations)
- Other
- Basal cell carcinoma
- Melanoma
- Sarcoma
- Langerhans cell histiocytosis
-
Squamous cell carcinoma (SCC) and subtypes: > 80% of cases [1]
-
Precursor lesions
- Nonneoplastic epithelial disorders (vulvar dermatoses), e.g.:
- Lichen sclerosus
- Squamous cell hyperplasia
- Vulvar intraepithelial neoplasia (VIN)
- Nonneoplastic epithelial disorders (vulvar dermatoses), e.g.:
Unlike Paget disease of the breast, which is always associated with underlying carcinoma, Paget disease of the vulva has a low likelihood (< 15%) of underlying carcinoma.


Clinical features [1][4]
- May initially be asymptomatic
- Local pruritus, possibly with burning sensation and pain
- Plaques, growths of various shapes, often wart-like lesions or ulcers
- Patches of discoloration (reddish, blackish, or whitish)
- Vulvar bleeding or discharge (less common)
- Dysuria, dyspareunia
- Inguinal lymphadenopathy

Diagnostics [1][4][5]
General principles [1][4]
All suspected vulvar cancer requires specialist consultation (e.g., gynecologic or surgical oncologist).
- Pelvic examination and colposcopy
- Biopsy of all suspicious lesions with histological analysis and tumor grading is necessary for diagnostic confirmation. [6]
- Additional studies are required for:
- Tumor staging (e.g., FIGO or TNM staging)
- Identification of comorbidities (e.g., HPV, HIV infection)
Staging [1][4][5]
- Biopsy with histological analysis: all suspicious lesions
-
Imaging studies: considered in consultation with a multidisciplinary team
- MRI pelvis, CT abdomen and chest with IV contrast: to evaluate primary tumor size and local extension
- Chest imaging, FDG-PET/CT scan: to identify distant metastasis if there is local extension (e.g., to the urethra, vagina, bladder mucosa) or lymph node involvement
- Ultrasound, FNA, or core biopsy of inguinofemoral lymph nodes: to identify lymph node involvement
- FIGO or TNM classification: helps establish prognosis and appropriate management
Biopsy is necessary if bladder or rectal involvement is suspected. [4]
Identification of comorbidities [1]
-
Screening for HPV-related cancers (e.g., cervicovaginal or oropharyngeal) [1]
- Pap smear
- HPV testing
- HIV screening (if HIV status is unknown)
HPV-related vulvar tumors have a higher prevalence of multifocal lesions and concurrent cervical neoplasia compared to HPV-negative tumors. [5]
Management of vulvar SCC [1][4]
Therapy is guided by tumor grading, tumor staging, and patient performance status and preferences. [1]
Locoregional disease [1][5]
-
Surgical therapy [5]
- Radical; or simple partial vulvectomy: first line [1]
- Surgical sentinel lymph node biopsy (SLNB): to determine the need for lymphadenectomy in selected patients [1][5]
- Inguinofemoral lymphadenectomy is recommended in: [1][5]
- Positive SLNB
- Tumors ≥ 4 cm [5]
- Multifocal invasive disease
- Post-treatment reconstructive surgery should be offered. [5]
-
Radiotherapy (RT): alone, post-surgical, or with chemotherapy [4]
- Vulvar RT: if surgical therapy is not feasible or if there are positive surgical margins after excision [4]
- Inguinofemoral RT: may be considered for inguinofemoral metastases
Vulvar RT is a third-line option due to associated significant morbidity (e.g., vaginal stenosis, pain, vulvar atrophy). [1]
Metastatic disease [1][4]
Treatment is primarily palliative. Options include:
- Chemoradiotherapy: platinum-based regimens (e.g., cisplatin) ± anti-PD-1 antibodies ± bevacizumab [1]
- Radiation therapy alone
- Surgical resection of large lesions
High-quality evidence for chemotherapy regimens to treat vulvar cancer is lacking. [4]
Supportive care
- HPV vaccination reduces recurrence rates after surgical therapy. [1]
- Pretreatment counseling should be offered to patients receiving chemoradiotherapy.
- A multidisciplinary care team is required for the management of complications. [1]
Complications [1]
Complications may include:
- Urinary incontinence
- Lymphedema
- Sexual dysfunction
- Reduced quality of life
- Anxiety disorders and mood disorders
Prognosis [4]
- Operable tumors without lymph node involvement: 90% overall survival [4]
- Lymph node involvement: ∼ 50% overall survival [4]
- Distant metastatic disease: ∼ 20% overall 5-year survival [1]
Lymph node involvement is the most important factor in determining prognosis. [4]
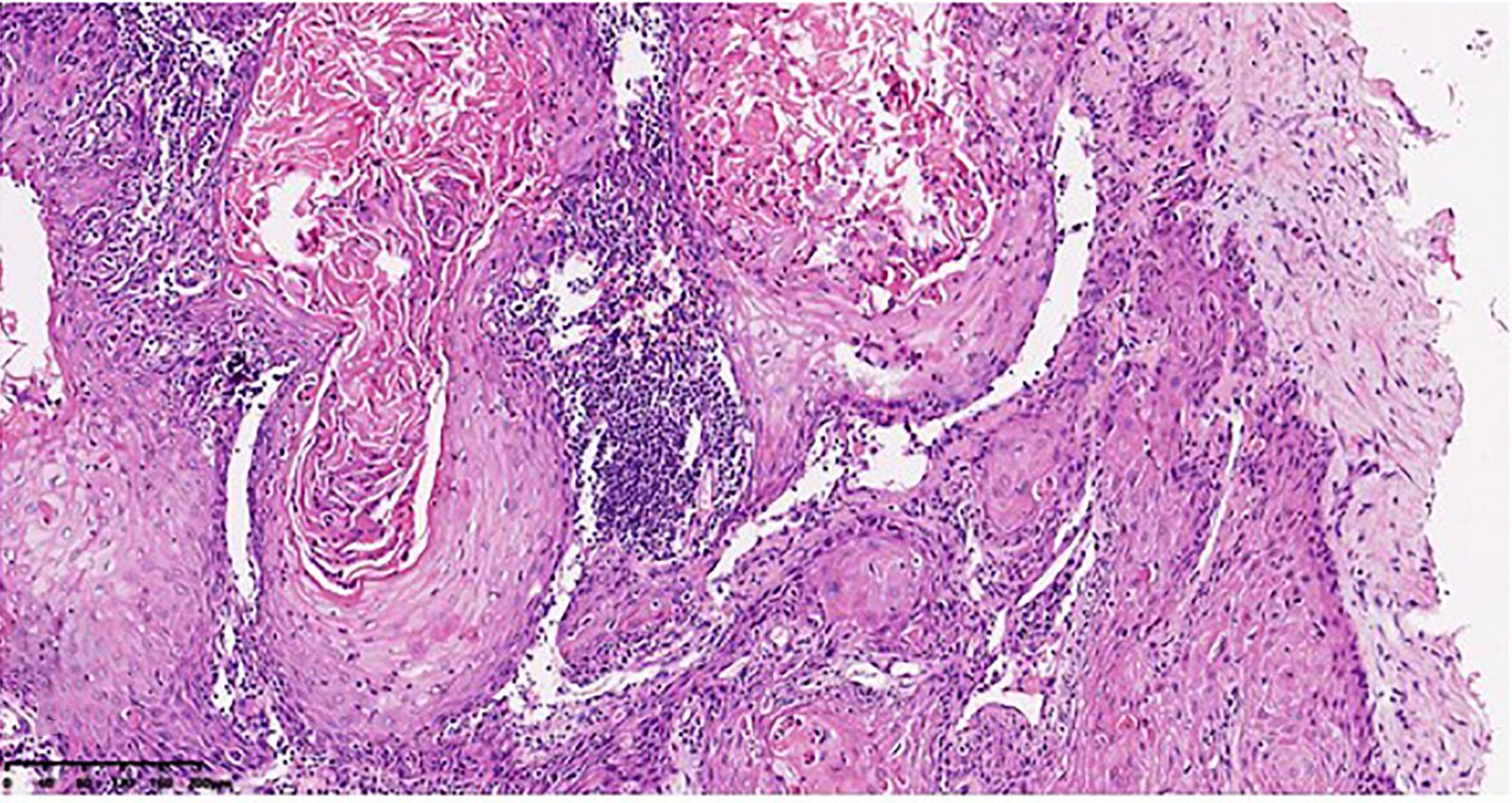
Photomicrograph of a vulvar tissue specimen (H&E stain; high magnification)
Squamous epithelium (example indicated by yellow overlay) with central keratinization (blue overlay) can be seen. It displays slightly irregular borders to the stroma, indicating infiltrative growth (black line). The epithelium shows mostly normal layering with only mild cellular atypia, e.g., enlarged nuclei (example indicated by arrowhead).
These histological features are suggestive of vulvar verrucous carcinoma, a low-grade subtype of squamous cell carcinoma.
Source: “Fig 1B, In: Pembrolizumab in FIGO IVB Verrucous Carcinoma of the Vulva: A Case Report” by Wang Y, Lin R, Zhang B et al., frontiers in Oncology, licensed under CC BY 4.0. Modifications: image cropped & removal of the letter B. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

Raised erythematous, squamous lesions are visible on the labia majora and minora of this patient.
Histologic examination was performed to confirm diagnosis.
Source: “Figure 1, in: Paget's Disease of the Vulva in Premenopausal Woman Treated with Only Surgery: A Case Report” by Hamid Asmouki, Rachid Oumouloud, Abderrahim Aboulfalah, Abderraouf Soummani, and Abdelouahed Marrat, Case Reports in Oncological Medicine, licensed under CC BY 3.0.

The labia minora and majora are difficult to identify due to the destructive, ulcerative, and exophytic growth of the tumor. The affected region shows a livid discoloration with bloody lesions.
These findings are suggestive of a squamous cell carcinoma of the vulva. Diagnosis was confirmed by biopsy.
Source: “Figure 5, in: A Clinical and Pathological Overview of Vulvar Condyloma Acuminatum, Intraepithelial Neoplasia, and Squamous Cell Carcinoma” by B. Léonard, F. Kridelka, K. Delbecque et al., Hindawi - BioMed Research International, licensed under CC BY 3.0.
Precursor lesions
Vulvar dermatoses
Vulvar dermatoses are not inherently precancerous, but some (e.g., lichen sclerosus) do increase the risk of squamous cell carcinoma.
-
Subtypes
- Lichen sclerosus: epidermal atrophy and loss of vulvar architecture
- Lichen simplex chronicus: squamous cell hyperplasia
- Other dermatoses, e.g., genital lichen planus (hypertrophied skin with purple lesions)
- Etiology: unclear
- Epidemiology: postmenopausal women and, less commonly, prepubescent girls
-
Clinical features
- Parchment-like, thin, shiny vulvar skin
- Narrow, atrophic vaginal introitus resulting in dyspareunia
- Burning pain, pruritus, bleeding vulvar ulcers
- Lichen simplex chronicus is characterized by chronic pruritus, which provokes persistent scratching of the vulva and so causes lichenification of the skin.
- Diagnosis: Colposcopy and biopsy of suspicious lesions are required to rule out malignancy.
-
Histology
- Epidermal atrophy, localized hyperkeratosis, degeneration of the basement membrane
- Loss of collagenous and elastic connective tissue
- Presence of an inflammatory infiltrate
-
Therapy
- Without atypical cellular morphology: local therapy with glucocorticoid-containing creams
- In the event of malignancy: surgical resection of the lesion
Vulvar intraepithelial neoplasia (VIN)
- Definition: precancerous lesion caused by dysplasia of squamous cells
-
Classification [7]
-
VIN, usual type (most common)
- Associated with HPV
- Commonly multifocal
-
VIN, differentiated type
- Associated with lichen sclerosus and other dermatoses
- Commonly unifocal
- VIN, unclassified type
-
VIN, usual type (most common)
- Diagnosis: tissue biopsy
- Treatment: : depending on severity, excision or ablation may become necessary
- Prognosis: may progress to vulvar carcinoma despite treatment (in < 10% of cases)

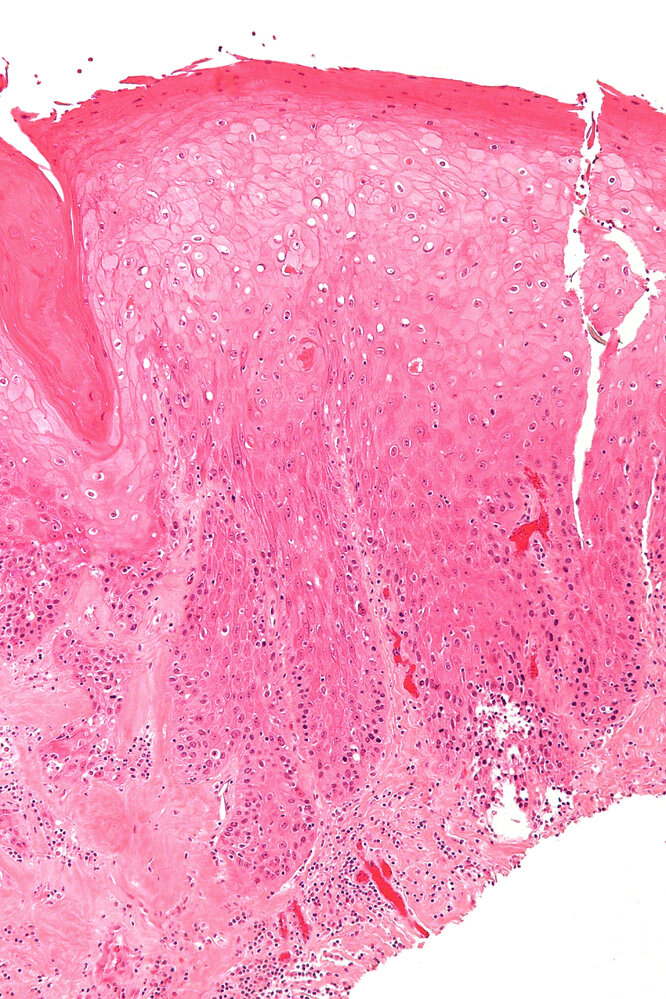
Photomicrograph of a vulvar tissue sample (H&E stain; 100x magnification)
The epidermis shows basal cell atypia as well as a characteristic elongation and anastomosis of rete ridges. The stratum spongiosum appears thickened (acanthosis). The retention of nuclei in the stratum corneum is called parakeratosis.
These histopathological findings are typical of differentiated vulvar intraepithelial neoplasia (dVIN), a precancerous lesion of the vulvar epithelium that often develops in association with chronic inflammatory dermatoses such as lichen sclerosus and lichen simplex chronicus.
Source: “Differentiated vulvar intraepithelial neoplasia - intermed mag.jpg” by Nephron, Wikimedia commons, licensed under CC BY-SA 3.0.
{kind=link}
Vaginal cancer
Overview
- Localization: The upper third of the posterior vaginal wall is the most common site of vaginal carcinoma.
- Etiology: same as vulvar neoplasia (e.g., HPV 16 and 18)
Classification
-
Squamous cell carcinoma
- Most common type
- Usually occurs secondary to cervical squamous cell carcinoma, primary carcinoma is rare
-
Clear cell adenocarcinoma
- Usually occurs secondary to vaginal adenosis (the presence of glandular columnar epithelium within the upper two-thirds of the vaginal wall)
- Seen in daughters of women who received diethylstilbestrol during pregnancy
-
Sarcoma botryoides [8]
- Rare, highly malignant embryonal rhabdomyosarcoma that arises most commonly, but not exclusively in the genitourinary system
- Epidemiology: peak incidence in childhood (< 4 years) [9]
- Pathology
- Gross: clear, polypoid masses that resemble a bunch of grapes protruding through the vagina
- Microscopy: pleomorphic spindle-shaped cells
- Immunohistochemical staining: desmin positive


Clinical features
- Vaginal bleeding
- Leukoplakia, vaginal ulceration with contact bleeding
- Malodorous discharge
- Possibly urinary frequency
Diagnosis
- Pelvic examination
- Colposcopy: if abnormal cytology results without a clearly visible lesion during pelvic examination
- Biopsy of mass to determine histopathology
Treatment
-
Radiotherapy
- Indicated in squamous cell carcinomas
- Preserves external genitalia
- Surgical therapy
Senile vaginitis should also be considered in patients presenting with vaginal pruritus, burning, and pain.
Photomicrograph of a vulvar tissue specimen (H&E stain; high magnification)
Squamous epithelium (example indicated by yellow overlay) with central keratinization (blue overlay) can be seen. It displays slightly irregular borders to the stroma, indicating infiltrative growth (black line). The epithelium shows mostly normal layering with only mild cellular atypia, e.g., enlarged nuclei (example indicated by arrowhead).
These histological features are suggestive of vulvar verrucous carcinoma, a low-grade subtype of squamous cell carcinoma.
Source: “Fig 1B, In: Pembrolizumab in FIGO IVB Verrucous Carcinoma of the Vulva: A Case Report” by Wang Y, Lin R, Zhang B et al., frontiers in Oncology, licensed under CC BY 4.0. Modifications: image cropped & removal of the letter B. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

Intraoperative photograph showing the mucosal surface of the (opened) urinary bladder of a young child
Several clusters of grape-like masses of varying sizes can be seen protruding into the lumen of the bladder.
These features are characteristic of sarcoma botryoides, a rhabdomyosarcoma that typically arises from the genitourinary tract and is most commonly seen in children < 8 years of age.
Source: © IMPP
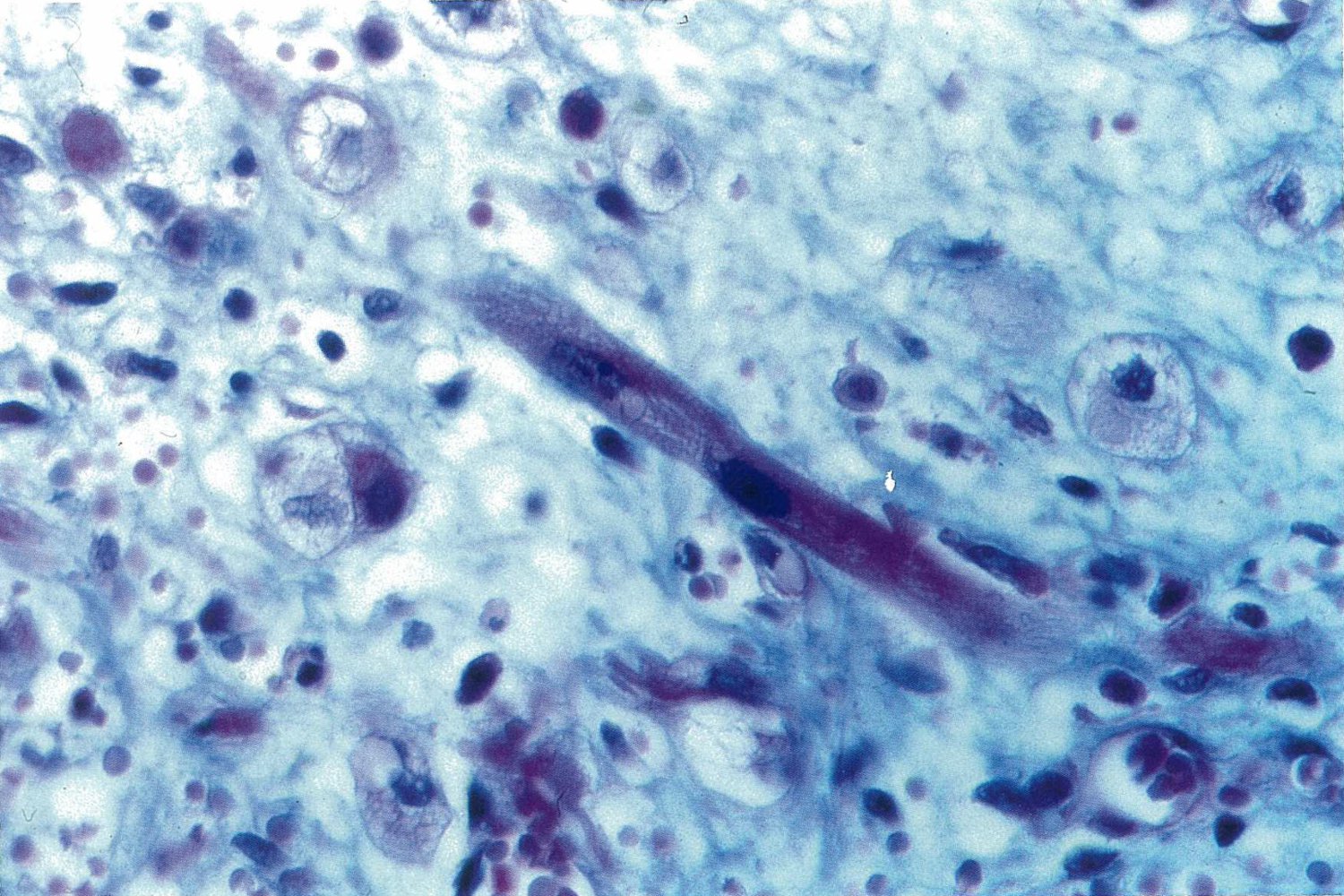
Photomicrograph of a section from a bladder tumor biopsy from a child (H&E stain; approx. 550x magnification)
The spindle-shaped cell (yellow overlay) with transverse striations and two nuclei (red overlay) is a skeletal muscle cell. The surrounding hypercellular stroma and the numerous mitotic figures indicate that this tumor is malignant.
Sarcoma botryoides is a type of rhabdomyosarcoma that almost exclusively affects the bladder and vagina of infants. The presence of skeletal muscle cells in a pediatric bladder tumor tissue is a common feature of sarcoma botryoides.
Source: © IMPP
Prevention of vulvar and vaginal cancer
- There are no screening tests for vulvar or vaginal cancers in asymptomatic individuals.
- Encourage uptake of the HPV vaccine. [10]
- Protects against the HPV subtypes associated with vulvar and vaginal cancer [11]
- See the “ACIP immunization schedule” for scheduling details.
- Counsel on safer sex practices, but advise that condoms only offer partial protection. [12][13]
- Offer support with smoking cessation. [14][15]
External Resources
References
- Qualman SJ, Bowen J, Parham DM, et al. "Protocol for the examination of specimens from patients (children and young adults) with rhabdomyosarcoma.". Arch Pathol Lab Med. 127(10). :1290-7. (2003)
- Ognjanovic S, Linabery AM, Charbonneau B, Ross JA. "Trends in childhood rhabdomyosarcoma incidence and survival in the United States, 1975-2005". Cancer. 115(18). :4218-4226. (2009)
- "Reducing Risk for Vaginal and Vulvar Cancers". https://web.archive.org/web/20240724100314/https://www.cdc.gov/vaginal-vulvar-cancers/prevention/index.html. [2023-11-01]
- Athanasiou A, Bowden S, Paraskevaidi M, et al. "HPV vaccination and cancer prevention". Best Practice & Research Clinical Obstetrics & Gynaecology. 65. :109-124. (2020)
- Markowitz LE, Schiller JT. "Human Papillomavirus Vaccines". J Infect Dis. 224(Supplement_4). :S367-S378. (2021)
- "Vulvar cancer". https://web.archive.org/web/20240724101224/https://www.cancer.org/cancer/types/vulvar-cancer/causes-risks-prevention/prevention.html. [2020-07-21]
- Olawaiye AB, Cuello MA, Rogers LJ. "Cancer of the vulva: 2021 update". Int J Gynaecol Obstet. 155(S1). :7-18. (2021)
- Baral SK, Biswas P, Kaium MdA, et al. "A Comprehensive Discussion in Vaginal Cancer Based on Mechanisms, Treatments, Risk Factors and Prevention". Front Oncol. 12. (2022)
- Chargari C, Wasserman J, Gabro A, et al. "Vulvar Carcinoma: Standard of Care and Perspectives". J Clin Oncol. 42(8). :961-972. (2024)
- Alkatout I, Günther V, Schubert M, et al. "Vulvar cancer: epidemiology, clinical presentation, and management options". Int J Womens Health. :305. (2015)
- Bornstein J, Bogliatto F, Haefner HK, et al. "The 2015 International Society for the Study of Vulvovaginal Disease (ISSVD) Terminology of Vulvar Squamous Intraepithelial Lesions". J Low Genit Tract Dis. 20(1). :11-14. (2016)
- "Vulvar Cancer Treatment (PDQ®)–Health Professional Version". https://web.archive.org/web/20240226083916/www.cancer.gov/types/vulvar/hp/vulvar-treatment-pdq. [2024-02-16]
- Oonk MHM, Planchamp F, Baldwin P, et al. "European Society of Gynaecological Oncology Guidelines for the Management of Patients with Vulvar Cancer - Update 2023". Int J Gynecol Cancer. 33(7). :1023-1043. (2023)
- Stewart DB, Gaertner WB, Glasgow SC, et al. "The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for Anal Squamous Cell Cancers". Dis Colon Rectum. 61(7). :755-774. (2018)
- Preti M. "VIN usual type—from the past to the future". ecancermedicalscience. 9. (2015)