Summary
Vulvovaginitis refers to a large variety of conditions that result in inflammation of the vulva and vagina. The causes may be infectious (e.g., bacterial vaginosis in most cases) or noninfectious. Physiologically, the normal vaginal flora (mainly lactobacilli) keeps the pH levels of the vaginal fluids low, thus preventing the overgrowth of pathogenic and opportunistic organisms. Disruption of that flora (e.g., due to sexual intercourse) predisposes to infection and inflammation. Diagnosis of infectious vulvovaginitis is based on histology examination of vaginal discharge. Treatment consists of administration of antibiotics or antifungals (depending on the pathogen).
For information on vulvovaginal atrophy caused by declining estrogen levels, see “Menopause.”
Infectious vulvovaginitis
Etiology [1]
-
Common causes of infectious vulvovaginitis
- Bacterial vaginosis
- Vulvovaginal candidiasis
- Trichomoniasis
- Aerobic vaginitis
-
Other causes of infectious vulvovaginitis (see respective articles for more information)
- Enterobius vermicularis (especially in prepubescent individuals)
- Scabies (seven-year itch)
- Pediculosis pubis (crabs, pubic lice)
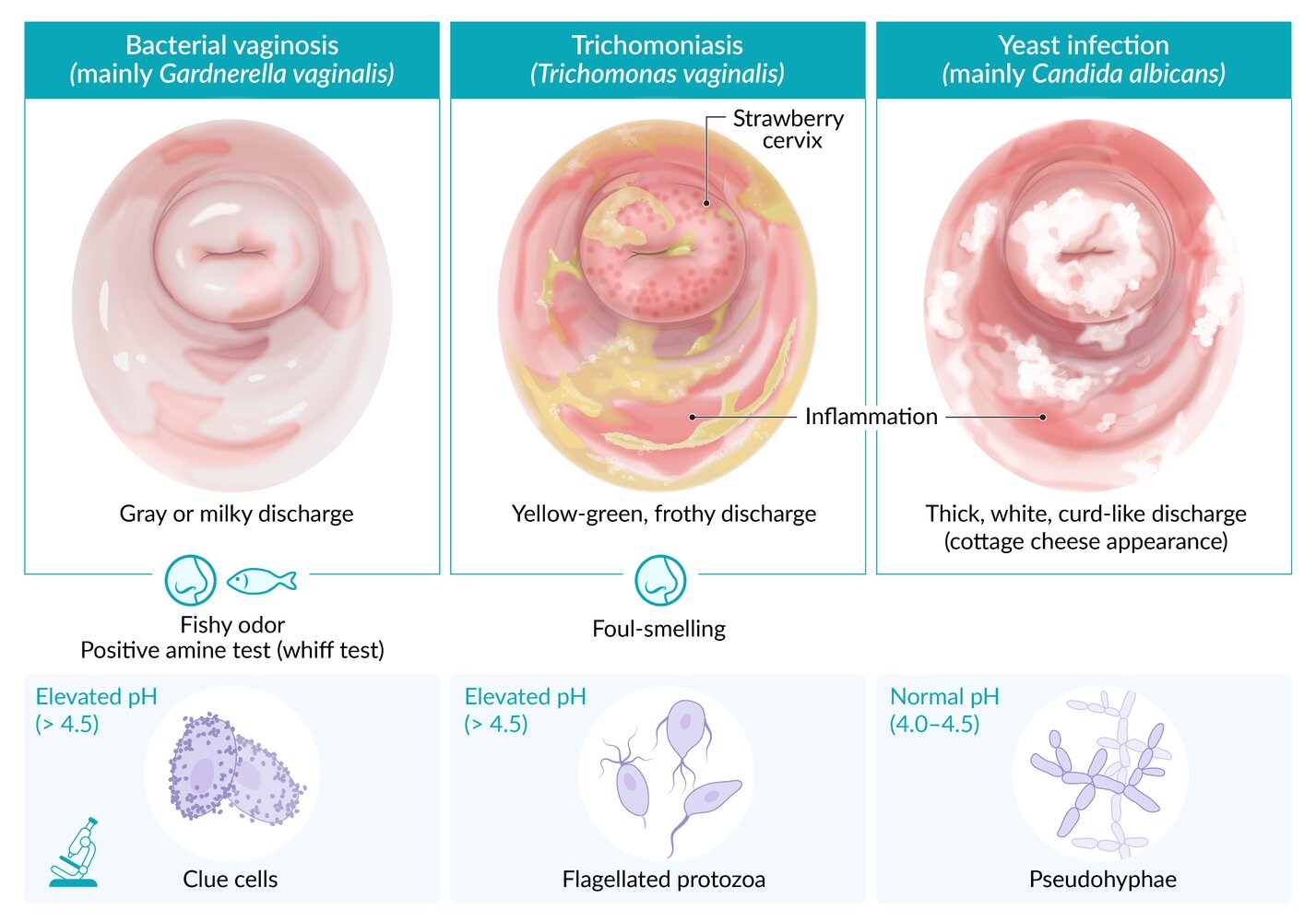
Differential diagnoses of infectious causes of vaginal discharge [1]
See the relevant articles and sections for details, including dosages.
| Overview | |||||
|---|---|---|---|---|---|
| Features | Bacterial vaginosis | Trichomoniasis | Vaginal yeast infection | Gonorrhea | Chlamydia infections |
| Pathogen |
|
|
|
|
|
| Discharge |
|
|
|
|
|
| |||||
| Vaginal inflammation |
|
|
|
|
|
| Cervicitis |
|
|
|
|
|
| Vaginal pH |
|
|
|
||
| Microscopy findings |
|
|
|
|
|
| Treatment |
|
|
|
|
|
Partner therapy is recommended in most cases of STIs, particularly chlamydia, trichomoniasis, and gonorrhea. Bacterial vaginosis and vaginal yeast infection do not require treatment of the partner(s).

© AMBOSS
Bacterial vaginosis
Bacterial vaginosis is the most common vaginal infection (22–50% of all cases). [2][3]
Pathogen [1]
Bacterial vaginosis is a polymicrobial infection caused by overgrowth of species including Gardnerella vaginalis (a pleomorphic, gram-variable rod), Atopobium vaginae, Prevotella spp., and Mobiluncus spp.
Pathophysiology
- Decreased concentrations of Lactobacillus acidophilus lead to overgrowth of Gardnerella vaginalis and other anaerobes.
- Vaginal epithelial inflammation does not occur because there is no immune response.
Risk factors [1]
- Sexual intercourse (primary risk factor, but it is not considered an STI)
- Intrauterine devices
- Vaginal douching
- Pregnancy
- Uncircumcised male partner
Clinical features
- Commonly asymptomatic
- Increased vaginal discharge, usually gray or milky with a fishy odor
- Pruritus and pain are uncommon.

Diagnosis [1]
Several methods can be used to confirm bacterial vaginosis from a vaginal swab.
-
Amsel criteria: A clinical diagnosis is made if ≥ 3 of the following criteria are met. [4]
-
Clue cells
- Vaginal epithelial cells with a stippled appearance and fuzzy borders due to bacteria adhering to the cell surface
- Identified on a vaginal wet mount preparation
- Vaginal pH > 4.5
- Positive amine test (sometimes referred to as the “whiff test”): Adding 1–2 drops of 10% potassium hydroxide to a sample of infected vaginal discharge emits a characteristic amine (fishy) odor. [5][6]
- Thin, homogeneous gray-white or yellow discharge that adheres to the vaginal walls
-
Clue cells
- Nugent score based on Gram stain (a score of 7–10 is consistent with bacterial vaginosis)
- Point-of-care assays
- NAAT
Culture of G. vaginalis is not recommended for diagnosis because of low specificity. [1]
Think DAMP for diagnosis of bacterial vaginosis: Discharge (gray or milky), Amine odor (positive whiff test), Microscopy (clue cells on vaginal wet mount preparation), pH > 4.5.



Management [1]
- Perform STI testing to rule out concurrent infection.
-
Antibiotic therapy is only indicated in symptomatic individuals. [1][2]
-
First-line in nonpregnant and pregnant patients ; [1]
- Oral metronidazole
- OR intravaginal metronidazole
- OR intravaginal clindamycin
-
Alternatives
- Nonpregnant and pregnant patients: oral clindamycin [1]
- Nonpregnant patients: oral tinidazole OR oral secnidazole [1]
-
First-line in nonpregnant and pregnant patients ; [1]
- A test-of-cure is not necessary if symptoms resolve.
- For recurrent infection (i.e., 3 confirmed infections in one year), consider: [1][2]
- Using an alternative agent
- Longer treatment duration
- Suppressive therapy with intravaginal metronidazole
- Treatment of male sexual partners (see "Prevention of reinfection") [7]
Prevention of reinfection
- Advise abstinence or use of condoms during treatment. [1]
-
Treatment of partners is not routinely recommended, as the effect on reinfection prevention is unclear. [1]
- Initial symptomatic infection: Use shared decision-making to determine whether to treat partners. [7]
- Recurrent infection
- Offer topical and oral antimicrobial therapy to male partners. [7]
- Use shared decision-making for same-sex partners. [7]
There is insufficient evidence to recommend screening for, or treating, asymptomatic bacterial vaginosis in pregnant and nonpregnant individuals. [1][8]
Complications [1]
- Adverse pregnancy outcomes: preterm delivery, spontaneous abortion, postpartum endometritis
- Increased risk of acquiring an STI, including HIV
- Reinfection
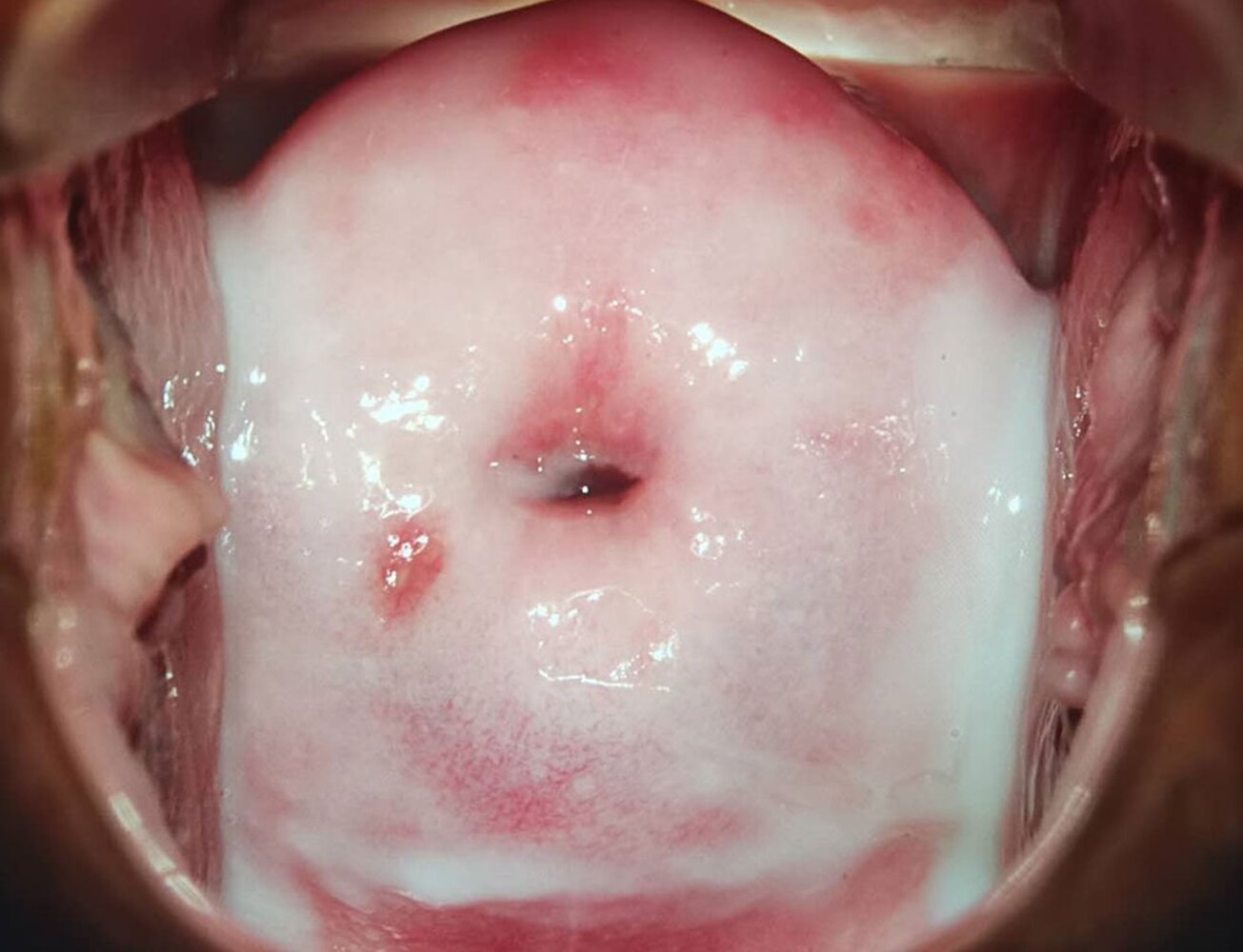
Speculum view of the cervix with thin gray and milky discharge
Source: “Figure 1A, in: The Female Vaginal Microbiome in Health and Bacterial Vaginosis” by X. Chen, Y. Lu, T. Chen et al., Frontiers in Cellular and Infection Microbiology, licensed under CC BY 4.0. Modifications: Image cropped. Original image was made up of 4 images.
© AMBOSS
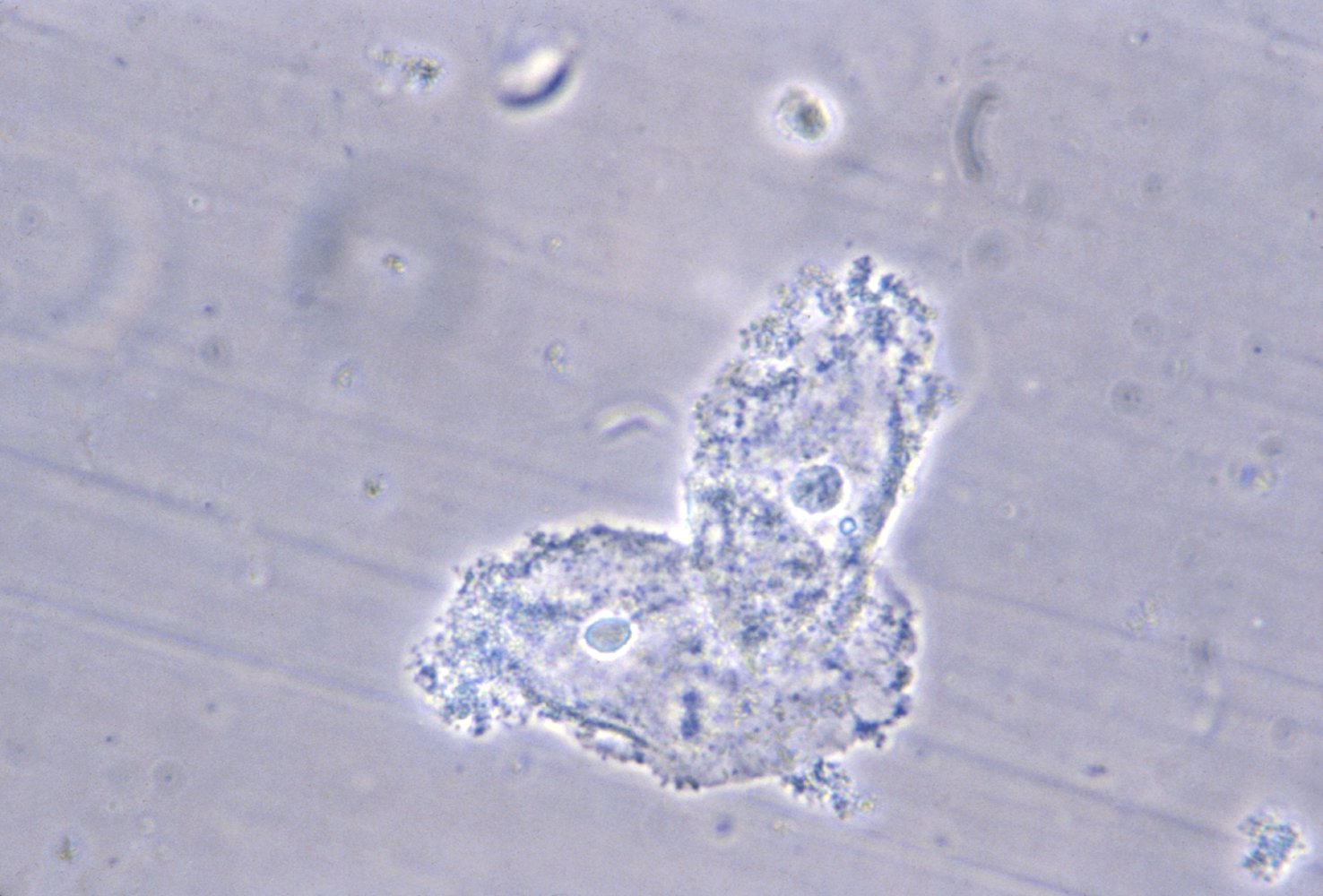
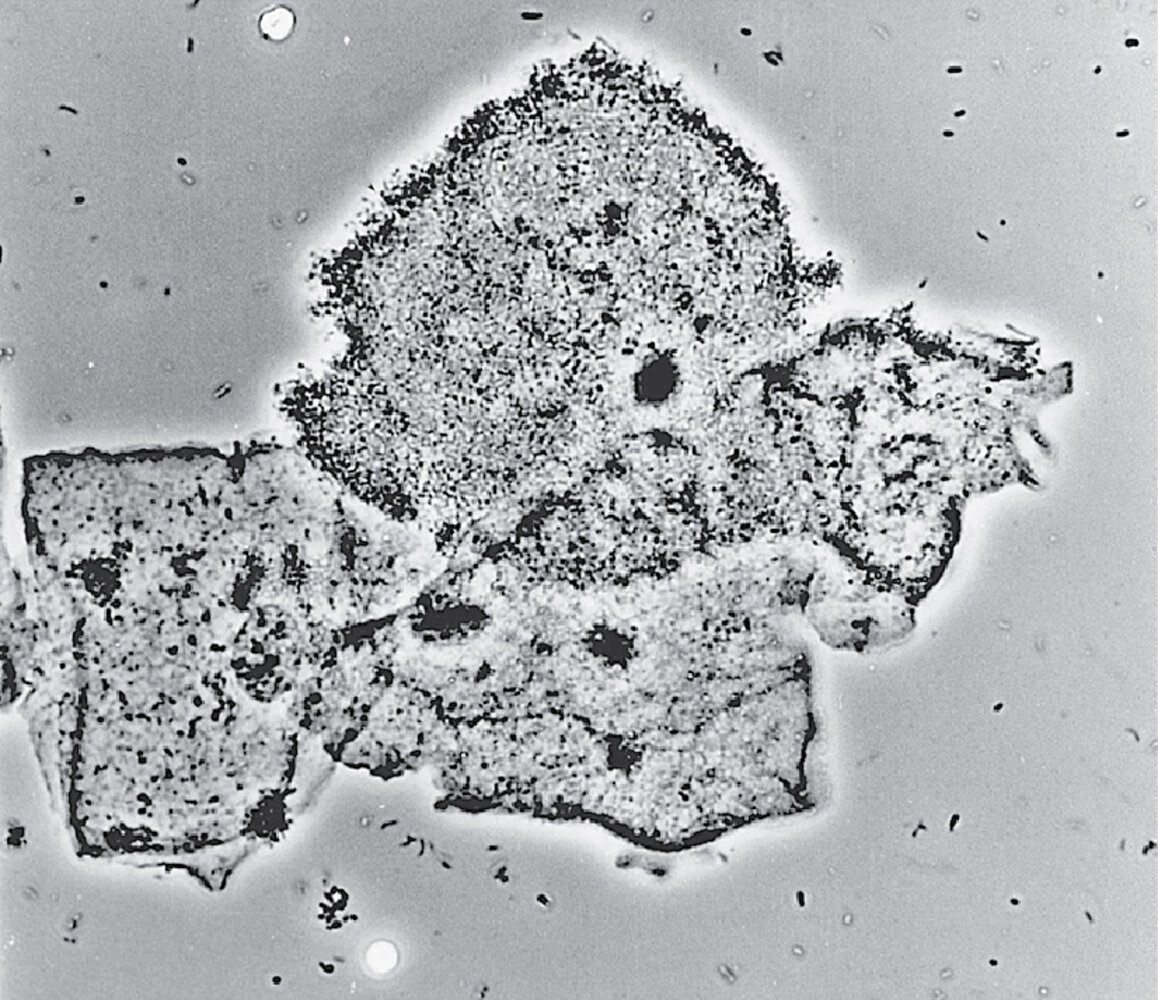
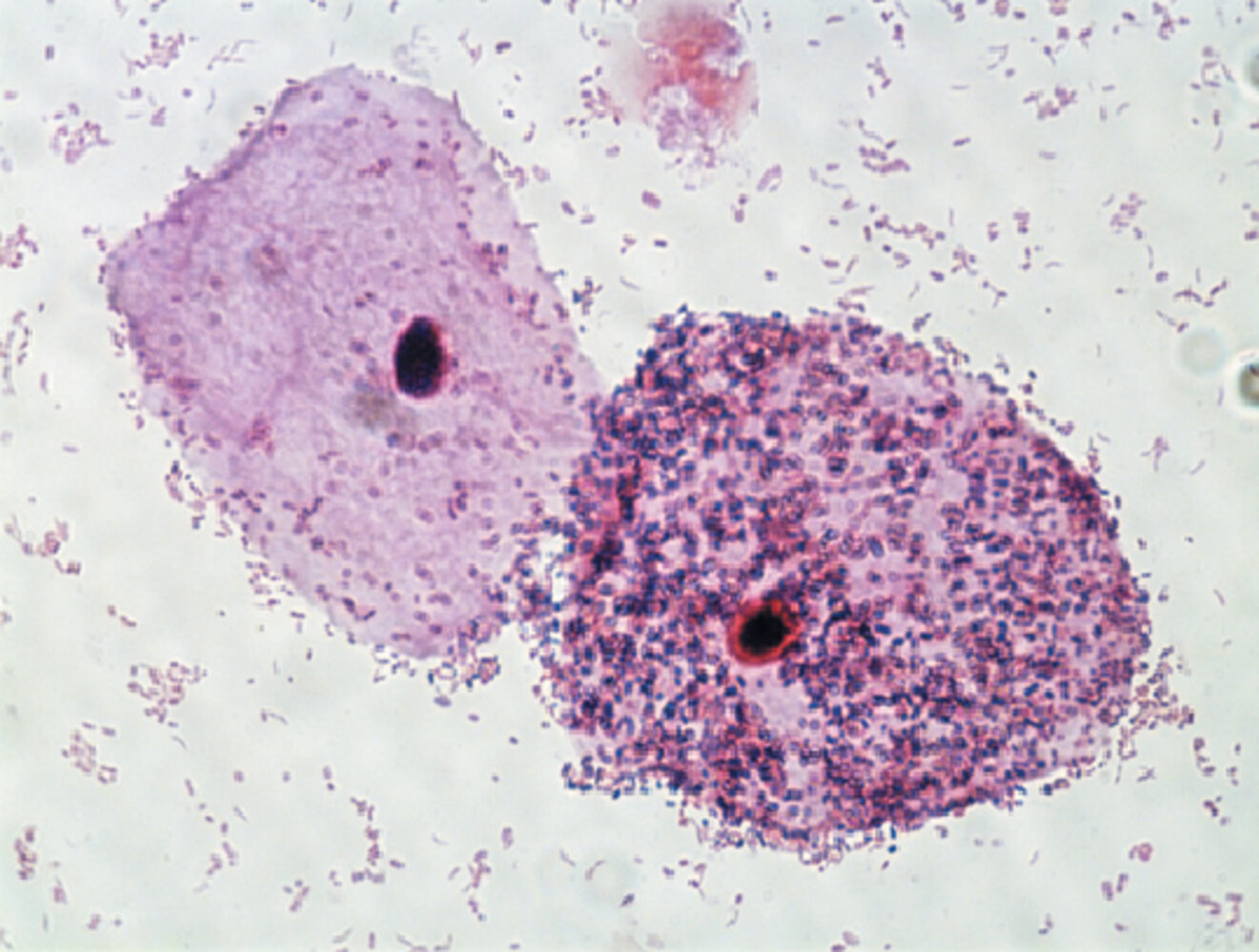
Photomicrograph of a vaginal smear specimen (vaginal wet mount; medium power magnification)
Squamous cells with a stippled appearance and fuzzy borders can be seen (clue cells) due to bacteria adhering to the cell surface.
The presence of clue cells is one of the four Amsel criteria (besides thin, white, yellow, homogeneous discharge; vaginal fluid pH of > 4.5; and a fishy odor after adding 10% potassium hydroxide solution to wet mount) for the diagnosis of bacterial vaginosis. Gardnerella vaginalis is the most common cause of this condition.
Source: "ID#: 3720", CDC/ M. Rein, Centers for Disease Control and Prevention licensed under Public Domain
Vulvovaginal candidiasis
- Epidemiology: second most common cause of vulvovaginitis (17–39% of all cases) [2]
- Pathogen: primarily Candida albicans (in immunosuppressed patients also Candida glabrata)
-
Pathophysiology: overgrowth of C. albicans
- Can be precipitated by the following risk factors:
- Pregnancy
- Immune deficiency: both systemic (e.g., poorly controlled diabetes mellitus, HIV, immunosuppression) and local (e.g., topical corticosteroids)
- Antimicrobial treatment (e.g., after systemic antibiotic treatment)
- Can be precipitated by the following risk factors:
-
Clinical features
- White, crumbly, and sticky vaginal discharge that may appear like cottage cheese and is typically odorless
- Erythematous vulva and vagina
- Vaginal burning sensation, severe pruritus, dysuria, dyspareunia
-
Diagnosis [1][2]
-
Diagnosis is confirmed by the presence of symptoms and either of the following:
- Budding yeast, hyphae, and/or pseudohyphae on a vaginal wet mount with potassium hydroxide (KOH) or saline
- Fungus on vaginal culture
- Additional findings: vaginal pH within normal range (i.e., 4–4.5)
-
Diagnosis is confirmed by the presence of symptoms and either of the following:
-
Classification [1]
-
Complicated vulvovaginal candidiasis is characterized by presence of ≥ 1 of the following:
- Recurrent infection (i.e., ≥ 3 episodes of vulvovaginal candidiasis within 1 year)
- Severe symptoms
- Causative organism other than C. albicans
- Diabetes mellitus or immune deficiency
- Uncomplicated vulvovaginal candidiasis is an infection with no features of complicated vulvovaginal candidiasis.
-
Complicated vulvovaginal candidiasis is characterized by presence of ≥ 1 of the following:
-
Treatment: only indicated in symptomatic patients [1]
-
Uncomplicated vulvovaginal candidiasis
- Nonpregnant individuals: topical azole (e.g., miconazole , clotrimazole ) OR single-dose oral fluconazole (adults only) [1][2]
- Pregnant individuals: 7-day course of a topical azole (e.g., miconazole , clotrimazole )
-
Complicated vulvovaginal candidiasis
- Adults: See “Treatment of complicated vulvovaginal candidiasis”
- Children: Consult a specialist.
-
Uncomplicated vulvovaginal candidiasis
| Treatment of complicated vulvovaginal candidiasis [1][2] | |
|---|---|
| Recurrent infection |
|
| Severe symptoms |
|
| Causative organism other than C. albicans |
|
Obtain a vaginal culture in all patients with complicated vulvovaginal candidiasis. [1]
Oral fluconazole is not recommended for use in pregnant patients because of a possible association with spontaneous abortions and fetal malformations. [1]




Vaginal cavity of a woman presenting with vaginal pruritus and white odorless vaginal discharge
White, cottage cheese-like discharge can be seen adhering loosely to the vaginal walls, which have patchy areas of inflammation.
Source: “Speculum_exam_in_candidal_vulvovaginitis” by Mikael Häggström, Wikimedia Commons, licensed under CC BY 1.0.
{kind=link}
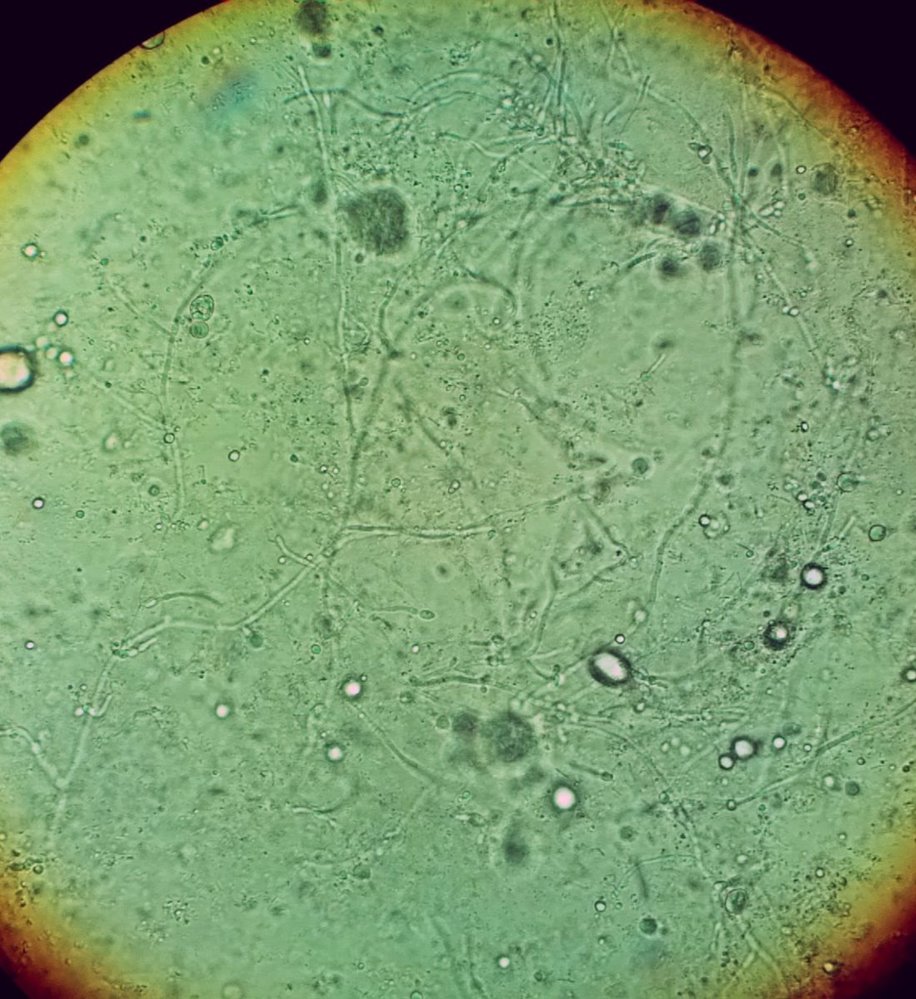
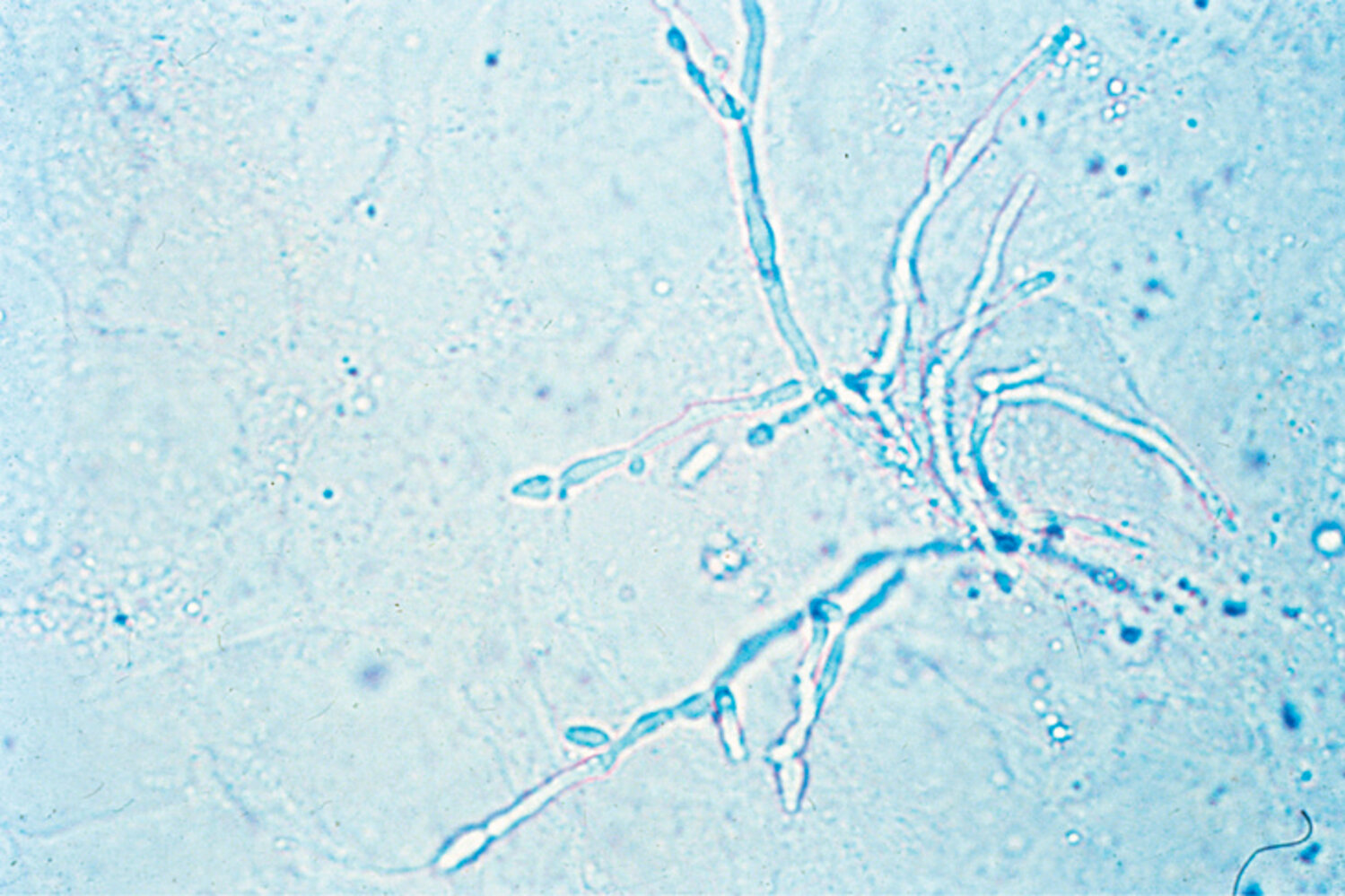
Vaginal wet mount after potassium hydroxide (KOH) preparation (microscopy) that shows Candida albicans forming multiple pseudohyphae (thin filamentous structures; examples indicated by blue overlay).
The prominent grey and white circles are optical artifacts.
White circles: examples of budding yeast
Source: “Vaginal wet mount in candidal vulvovaginitis.jpg” by Mikael Häggström, Wikimedia Commons, licensed under CC0 1.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
{kind=link}
© AMBOSS
Trichomoniasis
- Epidemiology: 4–35% of all cases [2]
-
Pathogen: Trichomonas vaginalis
- Anaerobic, motile protozoan with flagella
- Does not encyst and, therefore, does not survive well outside the human body [9]
- Transmission: : sexual
-
Clinical features
- Foul-smelling, frothy, yellow-green, purulent discharge
- Vulvovaginal pruritus, burning sensation, dyspareunia, dysuria, strawberry cervix (erythematous mucosa with petechiae)
-
Diagnosis [1][10]
- Saline vaginal wet mount (initial test): motile trophozoites with multiple flagella
- If the wet mount is inconclusive, perform a culture or nucleic acid amplification testing (NAAT).
- pH of vaginal discharge > 4.5
- Routine screening in asymptomatic (nonpregnant and pregnant) patients is not recommended.
-
Treatment [1]
- First-line in nonpregnant and pregnant patients: oral metronidazole
- Alternative in HIV-negative nonpregnant patients: oral tinidazole
-
Concurrent treatment of sexual partners:
- Female sexual partners: same as treatment for the primary patient
- Male sexual partners: single-dose oral metronidazole ; alternative: single-dose oral tinidazole
- Check for other sexually transmitted infections.
- Screen patients for repeat infection after 3 months of treatment.
- Complications: adverse pregnancy outcomes, e.g., preterm delivery, intrauterine growth restriction
“After sex, Burn the Foul, Green Tree:” burning sensation and foul-smelling, yellow-green discharge are the features of trichomoniasis.



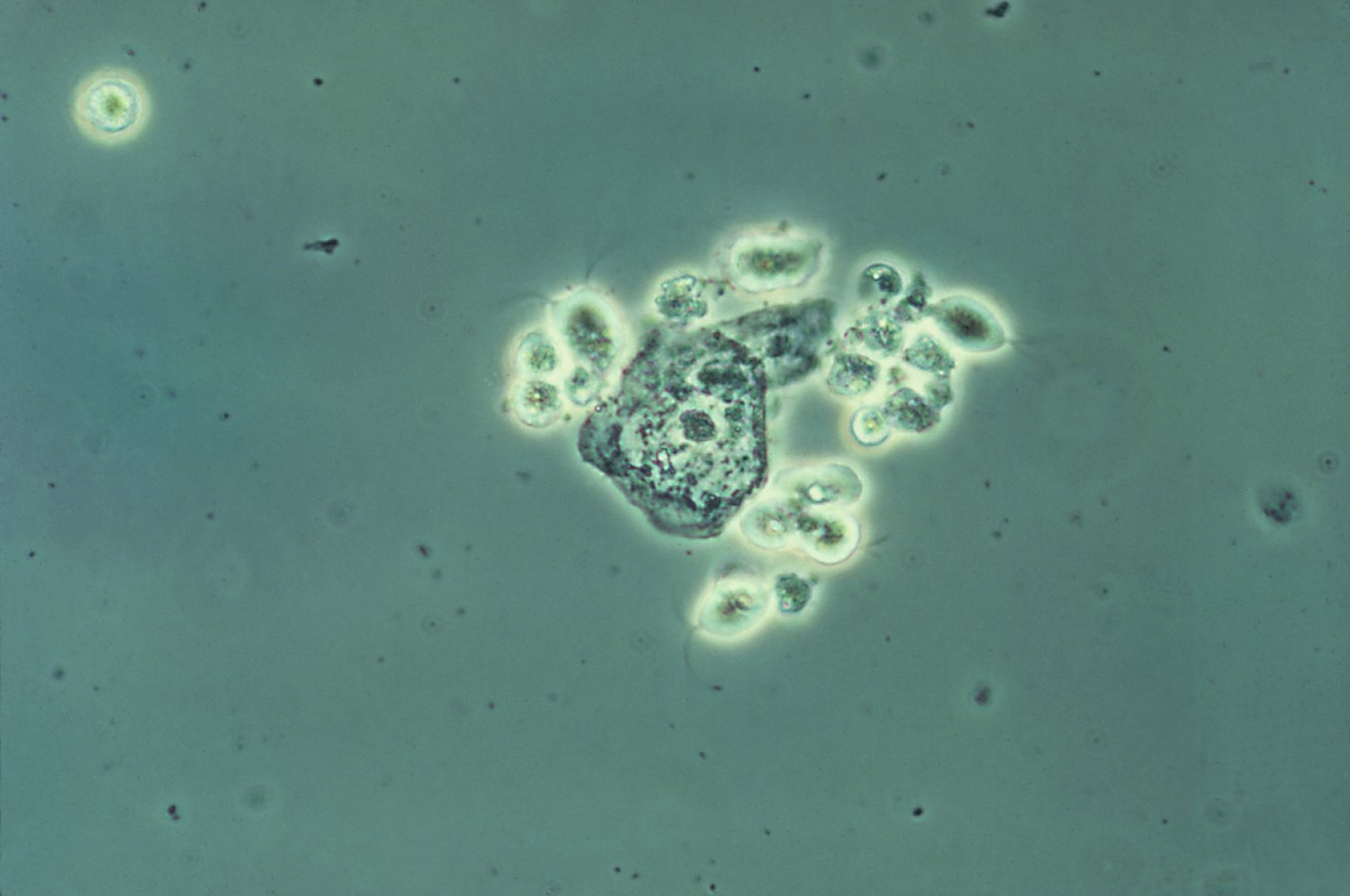
Phase contrast photomicrograph of vaginal discharge (high magnification)
These parasites with flagella (blue overlay) are Trichomonas vaginalis, the causative pathogen of trichomonal vaginitis.
In the center, two squamous epithelial cells can be seen.
Source: "ID#: 5238", CDC, Centers for Disease Control and Prevention (CDC) licensed under Public Domain
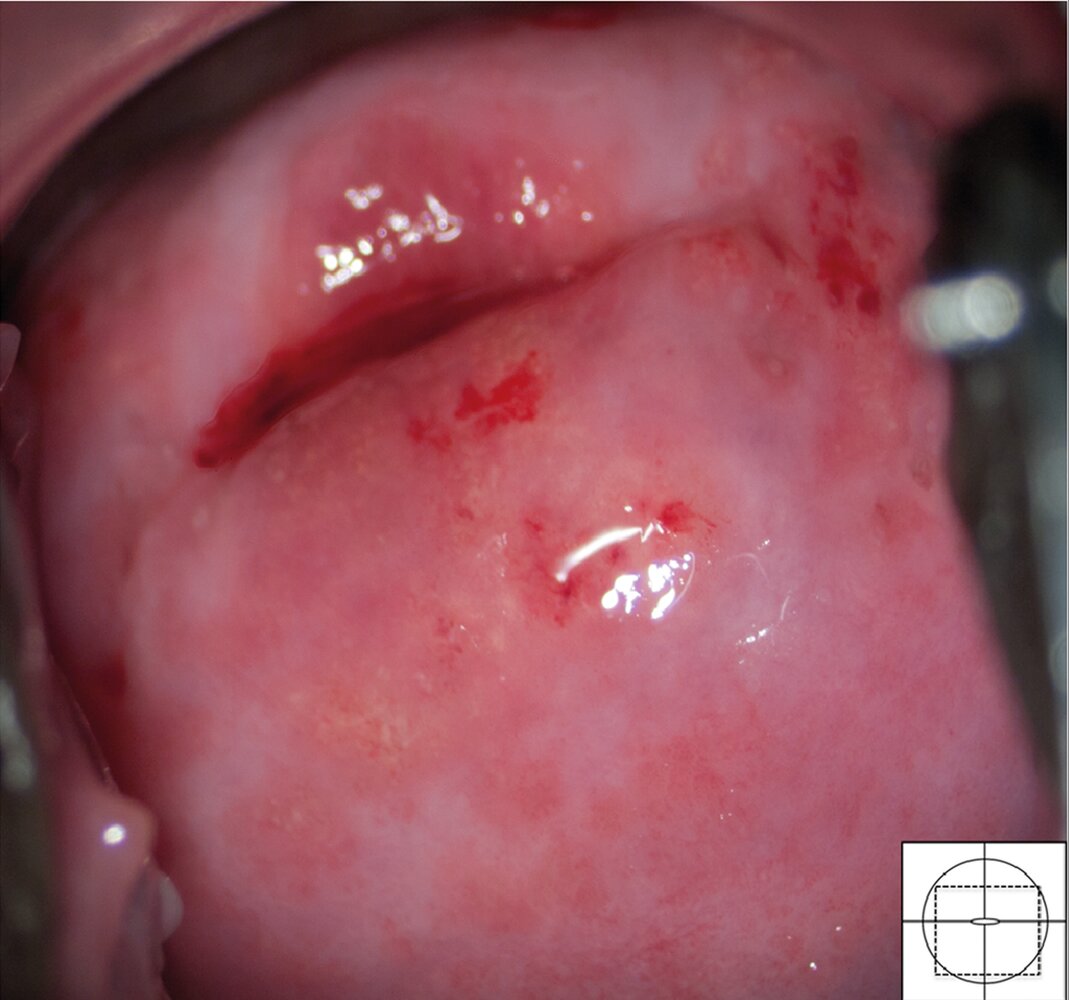
Colposcopy image of the ectocervix in a patient with trichomoniasis and schistosomiasis coinfection
The ectocervical mucosa is diffusely erythematous and multiple well-defined punctate hemorrhages (examples indicated by arrowheads) are visible (strawberry cervix). This finding is characteristic of trichomoniasis.
There are also clusters of small, sandy-colored lesions (sandy patches; examples indicated by yellow overlay), which are consistent with schistosomiasis (Schistosoma haematobium).
Dashed Line: squamocolumnar junction
Source: “Fig. 24, in: The Colposcopic Atlas of Schistosomiasis in the Lower Female Genital Tract Based on Studies in Malawi, Zimbabwe, Madagascar and South Africa” by Norseth HM, Ndhlovu PD, Kleppa E, et al, PLoS Negl Trop Dis, licensed under CC BY 4.0. Modifications: dashed line removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

Photomicrograph of trichomonas vaginalis trophozoites (Giemsa stain; high magnification)
The protozoan appears oval-shaped with flagella (examples indicated by arrowheads) and a nucleus (green overlay) located at the anterior end.
Source: “Figure 3, in: Prevalence of Trichomonas vaginalis Among Females Visiting Some Selected Hospitals in Makurdi, Benue State Nigeria” by I. I. Marsoon, O. M. Enyanwu, International Journal of Microbiology and Biotechnology, licensed under CC BY 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
© AMBOSS
Noninfectious vulvovaginitis
| Differential diagnoses of noninfectious vulvovaginitis | ||||
|---|---|---|---|---|
| Features | Genitourinary syndrome of menopause | Aerobic vaginitis | Allergic vulvovaginitis | Mechanical vulvovaginitis |
| Etiology |
|
|
|
|
| Clinical features |
|
|
|
|
| Diagnosis |
|
|
|
|
| Treatment |
|
|
|
|
Aerobic vaginitis
- Definition: an inflammatory vaginitis of noninfectious origin with microbiome disturbance and secondary bacterial infection
-
Epidemiology
- Approx. 8% of all cases of chronic vaginitis [11]
- More common in perimenopausal or postmenopausal individuals
-
Pathogen [12]
- Gram-negative: Escherichia coli is the most common
- Gram-positive: Streptococcus agalactiae, Staphylococcus aureus, and Enterococcus faecalis
- Pathophysiology: lower concentrations of Lactobacillus species in the vaginal flora → increase in vaginal pH → overgrowth of aerobic pathogens may trigger vaginal immune reaction [13]
-
Clinical features
- Copious, yellow (purulent), odorless vaginal discharge
- Vaginal inflammation, redness, and swelling
- Dyspareunia, burning sensation, itching
-
Diagnosis
- Negative amine test
- Vaginal pH > 4.5
- Leukocytes on microscopy
- Increased parabasal cells
- Culture
-
Treatment: Adapt treatment according to the severity of each of the three disease components (infection, atrophy, and inflammation).
-
Antibiotics
- Kanamycin OR quinolones (e.g., moxifloxacin) [14]
- Ampicillin for GBS or Enterococcus faecalis infection
- Local steroids
- Local estrogens [14]
- Oral probiotics reduce the risk of remission and relapse. [15]
-
Antibiotics
- Complications: Aerobic vaginitis is related to an increased risk of preterm delivery and to other severe pregnancy-related complications (e.g., ascending chorioamnionitis, PROM, miscarriage). [13]
Allergic vulvovaginitis
- Epidemiology: may affect all age groups, but are especially common in prepubescent girls
- Etiology: allergies (e.g., to laundry or cleaning detergents, textile fibers, sanitary napkins)
- Clinical features: pruritus, redness, swelling, burning sensation
- Diagnosis: Special allergy diagnostics (e.g., prick/puncture, intradermal test) may be indicated if symptoms persist despite treatment.
-
Treatment
- Avoid irritants
- Soothing lotions, ice packs, and sitz baths (e.g., containing chamomile)
- Cortisone creams if needed
Mechanical vulvovaginitis
-
Etiology
- Pruritus (e.g., due to atopic dermatitis, psoriasis, psychosomatic conditions)
- Friction of tight clothes, obesity
- Individuals suffering from postmenopausal estrogen deficiency or lichen sclerosis are especially at high risk.
- Clinical features: pruritus, redness, swelling, sometimes dysuria, and/or dyspareunia
- Diagnosis: special dermatological or rheumatological tests to find the cause of pruritus
-
Treatment
- Depends on the cause
- Soothing lotions/creams, ice packs, and sitz baths (e.g., containing chamomile)
Special patient groups
Vulvovaginitis in prepubertal children
Vulvovaginitis is the most common gynecological condition in prepubertal children. [16]
Etiology
-
Noninfectious vulvovaginitis (most common) [16][17][18]
- Mucocutaneous irritation (e.g., from urine or fecal matter, synthetic underwear)
- Use of perfumed products (e.g., soaps, bubble baths)
- Vaginal foreign body [17][19]
-
Infectious vulvovaginitis [16][17]
- Skin flora: e.g., Staphylococcus epidermidis, Streptococcus viridans
- Respiratory tract infections: e.g., group A streptococci, Haemophilus influenzae
- Enteric infections: e.g., E. coli, Shigella
- STI: due to child sexual abuse [18]
- E. vermicularis
- C. albicans (rare) [17][18]
Prepubertal children are predisposed to vulvovaginitis because they have thin vulvar and vaginal mucosa, underdeveloped labia, and an alkaline vaginal pH due to an absence of estrogenization. [16][17]
Clinical features [17]
-
Vulvovaginal
- Frequent touching or rubbing of the genital area by the child
- Burning and/or pruritus
- Localized erythema
- Vaginal discharge (e.g., bloody, purulent, foul-smelling)
- Visible foreign body in selected patients
-
Urinary
- Increased frequency
- Burning and/or dysuria
- Urinary incontinence in previously toilet-trained children
Severe genital pain and watery, gray vaginal discharge suggest the presence of a button battery in the genital tract. [17]
Diagnosis [16][17][19]
Vulvovaginitis in prepubertal children is primarily a clinical diagnosis.
- Perform a comprehensive physical examination, including:
- Evaluation for signs of precocious puberty
- Examination of the vulvovaginal area
- Screening for (or referral to a specialist to screen for) child sexual abuse, if suspected
- Consider targeted diagnostics as needed, e.g.: [16][18][19]
- Urinalysis
- STI testing: for suspected child sexual abuse
- Vaginal culture, wet mount: for suspected infectious vulvovaginitis
- Imaging (e.g., x-ray, transabdominal or transvaginal ultrasound, MRI): for suspected vaginal foreign body not visualized on examination [19]
- Refer to a specialist (e.g., pediatric gynecology) in case of diagnostic uncertainty or persistent symptoms.
If child sexual abuse is suspected (e.g., vaginal foreign body, clinical features of child sexual abuse, STIs), refer to a specialist for examination, if feasible. [19]
Differential diagnosis
- Precocious puberty [16][17]
- Urogenital [17]
- Urinary tract infection in children and adolescents
- Ectopic ureter
- Voiding dysfunction (e.g., overactive bladder, external bladder sphincter dyssynergia) [20]
- Dermatological [17]
- Lichen sclerosis
- Allergic vulvovaginitis
- Atopic dermatitis
- Psoriasis
Treatment [16][17]
- Improved hygiene and toilet practices
- Avoidance of tight clothing, synthetic underwear, and products that cause local irritation
- Symptomatic management of vulvovaginal irritation
- Sitting in a tub of warm water or sitz bath
- Applying a fragrance-free emollient after drying the area completely
- Consider a low-potency topical corticosteroid in patients with severe discomfort. [16]
- Treat the underlying cause.
-
Removal of vaginal foreign body ; [16][17][19]
- Gentle irrigation with saline or water
- If foreign body cannot be removed, refer to a specialist for removal under general anesthesia.
-
Targeted antimicrobial therapy for infectious vulvovaginitis[16][17]
- Skin flora or respiratory tract organisms: ampicillin, amoxicillin
-
Enteric organisms
- E.coli: azithromycin
- Proteus vulgaris: trimethoprim/sulfamethoxazole
- Enterobius vermicularis: mebendazole
-
Removal of vaginal foreign body ; [16][17][19]
Infectious vulvovaginitis in pregnancy
- Screening asymptomatic pregnant individuals for infectious vulvovaginitis is not routinely recommended. [1]
- The etiology, clinical features, diagnosis, and treatment of symptomatic pregnant patients are similar to those in nonpregnant adults; see "Infectious vulvovaginitis" for details.
Infectious vulvovaginitis during pregnancy is associated with adverse pregnancy outcomes (e.g., spontaneous abortion, premature rupture of membranes, chorioamnionitis, neonatal infection, postpartum endometritis).
External Resources
- 2025 ACOG Clinical Practice Update: Concurrent Sexual Partner Therapy to Prevent Bacterial Vaginosis Recurrence
- 2021 CDC Sexually Transmitted Infections Treatment Guidelines
- 2020 (reaffirmed 2025) ACOG Practice Bulletin No. 215: Vaginitis in Nonpregnant Patients
- 2018 AFP Article on Diagnosis and Treatment of Vaginitis
References
- Workowski KA, Bachmann LH, Chan PA, et al. "CDC Sexually Transmitted Infections Treatment Guidelines 2021". MMWR Recomm Rep. 70(4). :1-187. (2021)
- American College of Obstetricians and Gynecologists. "Vaginitis in Nonpregnant Patients". Obstetrics & Gynecology. 135(1). :e1-e17. (2020)
- Koumans EH, Sternberg M, Bruce C, et al. "The Prevalence of Bacterial Vaginosis in the United States, 2001–2004; Associations With Symptoms, Sexual Behaviors, and Reproductive Health". Sex Transm Dis. 34(11). :864-869. (2007)
- Amsel R, Totten PA, Spiegel CA, et al. "Nonspecific vaginitis". Am J Med. 74(1). :14-22. (1983)
- Silverberg B, Moyers A, Hinkle T, Kessler R, Russell NG. "2021 CDC Update: Treatment and Complications of Sexually Transmitted Infections (STIs)". Venereology. 1(1). :23-46. (2022)
- Brotman RM. "Vaginal microbiome and sexually transmitted infections: an epidemiologic perspective". J Clin Invest. 121(12). :4610-4617. (2011)
- American College of Obstetricians and Gynecologists. "Concurrent Sexual Partner Therapy to Prevent Bacterial Vaginosis Recurrence". Obstet Gynecol. (2025)
- Owens DK, Davidson KW, et al. "Screening for Bacterial Vaginosis in Pregnant Persons to Prevent Preterm Delivery". JAMA. 323(13). :1286. (2020)
- Krieger H, Kimmig P. "[Survival ability of Trichomonas vaginalis in mineral baths].". Gesundheitswesen. 57(12). :812-9. (1995)
- Miller JM, Binnicker MJ, Campbell S, et al. "A Guide to Utilization of the Microbiology Laboratory for Diagnosis of Infectious Diseases: 2018 Update by the Infectious Diseases Society of America and the American Society for Microbiology". Clin Infect Dis. 67(6). :e1-e94. (2018)
- Zuckerman A, Romano M. "Clinical Recommendation: Vulvovaginitis". J Pediatr Adolesc Gynecol. 29(6). :673-679. (2016)
- Romano ME. "Prepubertal Vulvovaginitis". Clin Obstet Gynecol. 63(3). :479-485. (2020)
- Vilano SE, Robbins CL. "Common prepubertal vulvar conditions". Curr Opin Obstet Gynecol. 28(5). :359-365. (2016)
- Lehembre-Shiah E, Gomez-Lobo V. "Vaginal Foreign Bodies in the Pediatric and Adolescent Age Group: A Review of Current Literature and Discussion of Best Practices in Diagnosis and Management". J Pediatr Adolesc Gynecol. 37(2). :121-125. (2024)
- Romero P, Rodríguez E, Muñoz M, et al. "Voiding Dysfunction: Another Etiology of Vulvovaginitis in Young Girls". J Pediatr Adolesc Gynecol. 24(4). :189-191. (2011)
- Nyirjesy P, Peyton C, Weitz MV, Mathew L, Culhane JF. "Causes of chronic vaginitis: analysis of a prospective database of affected women.". Obstet Gynecol. 108(5). :1185-91. (2006)
- Donders GG, Vereecken A, Bosmans E, et al. "Definition of a type of abnormal vaginal flora that is distinct from bacterial vaginosis: aerobic vaginitis.". BJOG. 109(1). :34-43. (2002)
- Donders G, Bellen G, Rezeberga D. "Aerobic vaginitis in pregnancy". BJOG. 118(10). :1163-1170. (2011)
- Donders GG, Ruban K, Bellen G. "Selecting anti-microbial treatment of aerobic vaginitis". Curr Infect Dis Rep. 17(5). :477. (2015)
- Heczko PB, Tomusiak A, Adamski P, et al. "Supplementation of standard antibiotic therapy with oral probiotics for bacterial vaginosis and aerobic vaginitis: a randomised, double-blind, placebo-controlled trial". BMC Womens Health ;15:115.. 15. :115. (2015)